

This article provides a summary of the changes along with the updated recommendations (Table 1) made by Health Canada's Steering Committee on Clinical Practice Guidelines for the Care and Treatment of Breast Cancer to the article “Clinical Practice Guidelines for the Care and Treatment of Breast Cancer: 3. Mastectomy or lumpectomy? The choice of operation for clinical stages I and II breast cancer,” originally published in 19981 (the 2002 update can be found online at www.cmaj.ca/cgi/content/full/158/3/DC1).
Table 1
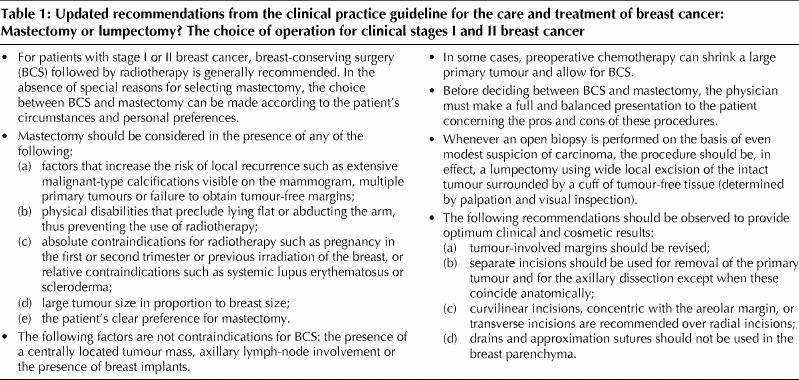
In the 1998 guideline, breast-conserving surgery (BCS) followed by radiotherapy was recommended, and the choice between BCS and mastectomy was to be made according to the patient's circumstances and personal preferences. This recommendation was based on the results of 6 randomized trials that showed no difference in survival between patients who received BCS plus radiotherapy and those who underwent mastectomy.1 In the 2002 update, results of longer follow-up from 2 of these trials are presented. There continues to be no difference in survival between BCS and mastectomy patients. In the National Surgical Adjuvant Breast Project (NSABP) B-06 trial, after an average of 12 years of follow-up, the survival was 62% in the BCS and breast irradiation group and 60% in the mastectomy group.2 In the European Organization for Research and Treatment of Cancer (EORTC) trial, at 10 years of follow-up, the survival was 65% in the BCS and radiation therapy group and 66% in the mastectomy group.3 Hence, our 1998 recommendation concerning the type of surgery has not changed.
In the 1998 guideline, the importance of having tumour-free margins following BCS was discussed. The steering committee feels that this point needs emphasizing. In the update, data from 2 randomized trials is included showing that positive margins following lumpectomy and breast irradiation is a predictor of local breast cancer recurrence. In the EORTC trial involving women who underwent lumpectomy, the local recurrence rate was 14% among women with positive margins compared with 8% among those with negative margins.4 In the Milan II trial, the corresponding rates were 17% and 9%.5 Finally, data from 2 NSABP randomized trials involving women with ductal carcinoma in situ who had lumpectomy provide supporting evidence that positive margins even in cases of noninvasive breast cancer are associated with an increased risk of local breast cancer recurrence. In the NSABP B-17 trial6 breast irradiation was compared with no radiation, and in the NSABP B-24 trial breast irradiation plus tamoxifen was compared with breast irradiation plus placebo.7 In both of these studies the presence of positive margins was associated with an approximate two-fold increase in the rates of local breast cancer recurrence. Hence, the steering committee reaffirms its recommendations that tumour-involved margins should be re-excised and that mastectomy be considered if margins remain positive after re-excision.
The role of preoperative (neo-adjuvant) chemotherapy for shrinking large tumours to allow BCS has been clarified sufficiently to allow for a new recommendation. In the NSABP B-18 trial over 1500 women with early breast cancer were randomly assigned to receive chemotherapy consisting of 4 cycles of adriamycin and cyclophosphamide either preoperatively or postoperatively.8,9 No difference was detected in disease-free or overall survival between the 2 groups. Sixty-seven percent of women in the preoperative chemotherapy group underwent lumpectomy compared with 60% in the postoperative chemotherapy group. Among the patients with tumours > 5 cm in diameter, the rates of lumpectomy were 22% and 8%, respectively. There was a trend for a higher rate of local breast cancer recurrence among the lumpectomy patients who received preoperative chemotherapy than among those who received postoperative chemotherapy (10.7% v. 7.6%, p = 0.12). In the EORTC 10902 trial 698 women with breast cancer were randomly assigned to receive 4 cycles of fluorouracil, epirubicin and cyclophosphamide either preoperatively or postoperatively.10 No difference was detected in overall survival between the 2 groups. In the preoperative chemotherapy group 57 patients (23%) who were scheduled to undergo mastectomy had their cancer downstaged and had BCS.
Additional experience with BCS has led to some refinements in surgical technique with respect to incision placement. In addition, it has become evident that the proportion of women eligible for BCS has increased. It is estimated that 80% of women with clinically detected tumours and nearly all women with mammographically identified tumours may be eligible for BCS.
Footnotes
The patient version of these guidelines has also been updated and can be found online at www.cma.ca/cmaj/XXXXX
Drs. Scarth, Cantin and Levine contributed equally to the writing and revising of this commentary.
Competing interests: None declared.
Correspondence to: Dr. Mark Levine, Rm. 9, Wing 90, Main floor, Henderson Hospital, 711 Concession St., Hamilton ON L8V 1C3; fax 905 389-9288
References
- 1.Steering Committee on Clinical Practice Guidelines for the Care and Treatment of Breast Cancer. Clinical practice guidelines for the care and treatment of breast cancer. CMAJ 1998;158(Suppl 3):S71-81. Available: www .cmaj .ca /cgi /content/full/158/3/DC1 [PubMed]
- 2.Fisher B, Anderson S, Redmond CK, Wolmark M, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1995;333:1456-61. [DOI] [PubMed]
- 3.Van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 Trial. J Natl Cancer Inst 2000;92:1143-50. [DOI] [PubMed]
- 4.Van Dongen JA, Bartelink H, Fentiman IS, Lerut T, Mignolet F, Olthuis G, et al. Factors influencing local relapse and survival and results of salvage treatment after breast conserving therapy in operable breast cancer: EORTC Trial 10801, breast conservation compared with mastectomy in TNM stage I and II breast cancer. Eur J Cancer 1992;28A:801-5. [DOI] [PubMed]
- 5.Veronesi U, Luini A, Galimberti V, Zurrida S. Conservation approaches for the management of stage I/II carcinoma of the breast: Milan Cancer Institute trials. World J Surg 1994;18:70-5. [DOI] [PubMed]
- 6.Fisher ER, Dignam J, Tan-Chiu E, Constantino J, Fisher B, Paik S, et al. Pathologic findings from the NSABP eight-year update of protocol B-17: intraductal carcinoma. Cancer 1999;86:429-38. [DOI] [PubMed]
- 7.Fisher B, Dignam J, Wolmark N, Wickerham DL, Fisher ER, Mamounas E, et al. Tamoxifen in treatment of intraductal breast cancer: NSABP B-24 randomised controlled trial. Lancet 1999;353:1993-2000. [DOI] [PubMed]
- 8.Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 1998;16:2672-85. [DOI] [PubMed]
- 9.Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative chemotherapy in patients with operable breast cancer: nine-year results from National Surgical Adjuvant Breast and Bowel Project B-18. J Natl Cancer Inst Monogr 2001;30:96-102. [DOI] [PubMed]
- 10.Van der Hage JA, van de Velde CJH, Julien JP, Tubiana-Hulin M, Vandervelden C, Duchateau L, et al. Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer Trial 10902. J Clin Oncol 2001;19:4224-37. [DOI] [PubMed]