

Abstract
Introduction
The aim of this study was to investigate the cardiovascular safety of romosozumab in postmenopausal women with osteoporosis. Romosozumab, a monoclonal antibody targeting sclerostin, has been shown to increase bone mineral density and reduce the risk of osteoporotic fractures. However, in previous studies, romosozumab therapy was identified as a potential risk factor for cardiovascular events, particularly in patients with predisposing cardiovascular disease.
Methods
A systematic literature search was performed in the Cochrane Library, Embase, PubMed, and Web of Science databases to identify randomized controlled trials (RCTs) comparing the safety and efficacy of romosozumab versus alendronate, teriparatide, denosumab, or placebo in postmenopausal women with osteoporosis. Contrast-based network meta-analysis was performed using a random-effects model. The pooled estimates are presented as risk ratios with 95% confidence intervals.
Results
Of the 5282 articles retrieved, 25 RCTs were included in this review (n = 24,942), and 18 randomized controlled trials (n = 16,777) were included in the network meta-analysis. The results indicated no significant differences in cardiovascular mortality rate between romosozumab and placebo. Regarding the risk of major cardiovascular events, no significant differences were found in the direct evidence or the network meta-analysis with placebo as the reference.
Conclusion
Romosozumab might be a safe option for treating postmenopausal women with osteoporosis. The cardiovascular concerns associated with this treatment seem less significant than previously suggested, although additional real-world data are required to confirm this conclusion.
Supplementary Information
The online version contains supplementary material available at 10.1007/s40264-024-01475-9.
Key Points
| Romosozumab did not significantly increase the risk of cardiovascular events, mortality, or adverse events compared to placebo and other anti-osteoporotic drugs. |
| Age and daily calcium supplementation might not affect the influence of medications on the risk of cardiovascular events and mortality. |
| Romosozumab might be a safe anti-osteoporotic therapy for postmenopausal women. |
Introduction
Osteoporosis is a major public health concern among older adults, notably postmenopausal women. This demographic is highly susceptible to osteoporotic fractures, which lead to significant physical disability and impose a considerable financial burden [1]. Postmenopausal women represent the predominant demographic within the osteoporotic population, primarily due to the physiological effect of aging and reduced estrogen secretion following menopause. These factors contribute significantly to accelerated bone loss and diminished bone strength [2]. Effective management of osteoporosis and prevention of its consequences are crucial for this population. Currently available non-pharmacologic therapies for postmenopausal osteoporosis include calcium supplementation, vitamin D supplementation, exercise, and daily activity management [3]. However, pharmacologic intervention is recommended for patients who are at a high risk of fracture despite non-pharmacologic treatment [4]. The choice of anti-osteoporotic medications is guided by the type of osteoporosis, fracture risk, age, comorbidities, and safety profile. Among these, cardiovascular risk is an important factor in treatment decision making. Postmenopausal women are at an increased risk of cardiovascular disease due to the effects of aging and the loss of hormone protection. Reduced estrogen production changes body fat composition and plasma lipid levels, increases the risk of metabolic syndrome, and raises blood pressure [5, 6]. Therefore, due caution should be exercised while prescribing anti-osteoporotic drugs if their use increases the risk of cardiovascular disease.
Several anti-osteoporotic medicines are available for preventing or treating postmenopausal osteoporosis, including selective estrogen receptor modulators, bisphosphonates, receptor activator of nuclear factor kappa-B (RANK) ligand inhibitors, and teriparatide [3]. Recently, romosozumab, a novel therapy with a unique mechanism, has garnered significant attention [7]. This monoclonal antibody targets sclerostin, a protein released primarily by osteocytes that downregulates the Wnt signal pathway and bone formation [8]. By inhibiting sclerostin, romosozumab increases bone formation while decreasing bone resorption, resulting in a considerable increase in bone mineral density (BMD) [9]. Romosozumab has been shown to improve BMD more quickly and effectively than traditional antiresorptive medications [10]. However, concerns have been raised about its potential to increase cardiovascular calcification, as sclerostin is believed to inhibit vascular calcification [11, 12]. The ARCH trial, a large study comparing romosozumab to alendronate, found an increased risk of cardiovascular events, including cardiovascular death, heart attack, and stroke [13]. Although similar outcomes were not observed in studies comparing romosozumab to placebo or teriparatide, the drug’s use was restricted due to safety concerns. The US Food and Drug Administration (FDA) has contraindicated romosozumab in patients with recent myocardial infarction or stroke and recommends cautious use in those with a higher cardiovascular risk. Several authors have proposed explanations for the findings of the ARCH study, and one of these is the cardioprotective effect of bisphosphonates [14–16]. Currently, there is no consensus on the impact of romosozumab on cardiovascular health. Recent studies have suggested that anti-sclerostin antibodies pose a low risk to cardiac health, but the findings should be interpreted with caution due to small sample sizes [17, 18].
This study aimed to compare the incidence of cardiovascular events and cardiovascular-related mortality associated with the use of romosozumab versus some commonly used medications such as alendronate, denosumab, teriparatide, and raloxifene in postmenopausal osteoporotic women using network meta-analysis. While most of these medications have been compared with each other in previous trials, this synthesis includes placebo in the evidence network because placebo-controlled trials are the gold standard for establishing cause-and-effect relationships, rather than comparator trials.
Methods
This study followed the guidance outlined in the Cochrane Handbook for Systematic Reviews of Interventions and adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [19].
Eligibility Criteria
Randomized controlled trials (RCTs) that utilized either parallel or crossover designs for randomization were eligible for inclusion in this study. The inclusion criteria were as follows: (a) studies that exclusively recruited postmenopausal women, and (b) compared the efficacy of monotherapy of alendronate, romosozumab, teriparatide, or placebo. Studies that lacked randomization or solely compared different doses or combinations of the above-mentioned drugs were excluded from the analysis. Studies that enrolled males or patients without osteoporosis were also excluded from the review. In the case of post hoc analyses or repetitive data, only the most relevant references were included for pooled analysis to avoid inappropriate overweighting of duplicate data. Studies with insufficient follow-up duration (< 6 months) were excluded to minimize time-related bias. Articles that were retracted by journals were also excluded to ensure the quality and reliability of the pooled results.
Source and Search Strategy
The Cochrane Library (the Cochrane Database of Reviews and Cochrane CENTRAL), Embase, PubMed, and Web of Science databases were searched for relevant studies using relevant keywords such as "osteoporosis," "postmenopausal," "alendronate," " romosozumab," "teriparatide," and "placebo," with keyword sets combined using the Boolean operator OR within each concept. To enhance search sensitivity, all keywords related to anti-osteoporotic drugs were combined using the Boolean operator OR. The Boolean operator AND was used to establish connections between keyword sets for postmenopausal, osteoporosis, and anti-osteoporotic drugs.
No filters for publication year, article type, accessibility (full-text), or language were applied. The search strategies were developed in a primary database (PubMed) and are described in detail in Table S1 of the Supplement. The final search included studies published until December 2022, followed by independent (SHC and YNK) evidence selection according to the eligibility criteria.
Data Extraction
Two researchers independently extracted and verified trial information, details of the anti-osteoporotic drugs used, and outcome data. The extracted information included the study characteristics (first author’s name, publication year, study location), participant characteristics (age of participants, history of fractures, prior osteoporotic treatment), and intervention details (duration of the intervention, dosage of the anti-osteoporotic drug, and any supplemental treatments). The outcomes of interest were overall adverse events, cardiovascular events, and cardiovascular mortality. Since the outcomes of interest involved event data, the number of events and sample size for each group were also extracted for subsequent analysis.
Quality Evaluation
Two researchers (SHC and YNK) independently evaluated the quality of the included studies using the Cochrane Risk of Bias 2 tool, adhering to the guidelines outlined in the Cochrane Handbook of Systematic Reviews of Interventions [20]. The study design and methods were examined to identify potential bias due to (a) the randomization process, (b) deviation from intended interventions, (c) missing outcome data, (d) outcome measurement, and (e) selection of the reported results. Concerning the evaluation of deviation from intended interventions, the researchers’ effect of interest was adherence. Any disagreement during the risk of bias assessment was resolved by consensus after involving another member of the research team.
Certainty of synthesis was evaluated using the Confidence in Network Meta-analysis (CINeMA) approach, which assesses six domains: (a) within-study bias, (b) reporting bias, (c) indirectness, (d) imprecision, (e) heterogeneity, and (f) incoherence [21]. Within-study bias and indirectness were evaluated proportionally based on each study’s contribution to the evidence network. This evaluation incorporated the overall bias evaluated by RoB 2 and considerations of indirectness. The threshold for determining imprecision and heterogeneity followed a standard criterion, typically set at a value of 0.8 [21].
Statistics
All data included in this study were quantitatively synthesized using the random-effects model and the frequentist approach was applied to the conventional network meta-analysis using R-package netmeta version 2.8-2. Since all outcomes were based on dichotomous variables, the pooled effects are presented using risk ratios (RR) and 95% confidence intervals (CI). To assess heterogeneity, I2 statistics with corresponding p values were used. If I2 exceeded 50%, indicating high heterogeneity, the pooled effects were interpreted with caution. The separation of indirect from direct evidence (SIDE) method and the design-by-treatment interaction model were used to detect consistency model incoherence. To detect asymmetric publication bias, a comparison-adjusted funnel plot with regression intercept test was used for pooled analysis.
Network meta-regression was conducted to explore the role of age, given its significant impact on many health and clinical outcomes. Network meta-regression was also used to explore the risk of cardiovascular mortality and events associated with medications, adjusting for daily calcium supplementation (minimum mg/day), to mitigate any potential effect of calcium supplementation while examining the potential association between medication use and calcification risks, such as aortic calcification [11, 12]. The Bayesian approach is a mature approach for network meta-regression, and this study performed Bayesian network meta-regression using R-package gemtc version 1.0–2 with 50,000 simulation iterations. When the trace plot showed poor convergence, the analysis was re-conducted by 100,000 simulation iterations. The quality of the network meta-regression was evaluated using trace and density, shrinkage, residual deviance, and leverage. The significance of age in the network meta-regression was based on 95% credible interval (CrI). All analyses were carried out using R version 4.2.2 via RStudio version 2022.07.2 for Microsoft Windows.
Results
A total of 5282 articles were retrieved from databases, including the Cochrane database (k = 66), Cochrane CENTRAL Register of Controlled Trials (k = 1439), Embase (k = 1009), PubMed (k = 549), and Web of Science (k = 2219). No additional reference was identified after a manual screening of reference lists. Endnote functions and manual screening were used to remove duplicates (k = 2236). Then, 3004 records were excluded as being irrelevant (k = 2176), non-clinical studies (k = 82), non-female study population (k = 358), non-RCTs (k = 378), retracted articles (k = 7), and protocol-related issues (k = 3). Full texts of the 42 remaining articles were retrieved for eligibility review. Of these, 17 were excluded after a full-text review (Table S2). Finally, 25 articles qualified for our eligibility criteria (Fig. 1) [10, 13, 22–44]. The 25 studies, involving 24,942 patients with osteoporosis, examined cardiovascular outcomes following treatment with anti-osteoporosis medications such as alendronate, denosumab, raloxifene, romosozumab, and teriparatide.
Fig. 1.

Flow chart illustrating the study selection process for network meta-analysis. CDSR Cochrane Database of Systemic Reviews, k number of references, RCT randomized controlled trial
Characteristics
These trials were conducted across America, Asia, and Europe, underscoring the global significance of the research. Notably, 11 of the 25 studies were multicenter studies, harnessing the collaborative efforts of institutions from around the world. The recruited postmenopausal women exhibited a wide age range (50–90 years), representing a broad spectrum of individuals within the target population. The selected studies encompassed a substantial temporal range, ranging from 1996 to 2021, providing a comprehensive overview of advancements and progress in the field over the past few decades. Eighteen RCTs of 25 studies (n = 16,777) were included in quantitative synthesis due to adequate data availability [10, 13, 22, 24–29, 31–37, 43, 44]. The characteristics of each trial, including study design, patient demographics, intervention duration, and supplementary treatments are summarized in Table 1. The results of the risk of bias assessment for the included studies are provided in Table S3.
Table 1.
Characteristics of randomized controlled trials in this synthesis
| Author | Year | Location | All patients with fracture | Previous osteoporotic treatment | Intervention | Duration | Daily supplement treatment | Patients Number | Age (y) | CV AE | CV death |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Devogelaer | 1996 | Worldwide | X | X | Placebo | 24M | 500 mg calcium | 205 | 62.7±7.2 | Not report | 0 |
| Alendronate 5 mg/d | 104 | 61.2±6.8 | 0 | ||||||||
| Alendronate 10 mg/d | 102 | 63.2±6.6 | 0 | ||||||||
| Alendronate 20 mg/d | 105 | 63±6.6 | 0 | ||||||||
| Tucci | 1996 | USA | X | X | Placebo | 3y | 500 mg calcium | 192 | 64.2±7.4 | Not report | 0 |
| Alendronate 5 mg/d | 98 | 66.5±6.9 | 0 | ||||||||
| Alendronate10 mg/d | 94 | 63.9±6.4 | 0 | ||||||||
| Alendronate 20 mg/d | 94 | 63.8±6.8 | 0 | ||||||||
| Felsenberg (FOSIT trail) | 1998 | Worldwide | X | X | Placebo | 12M | 500 mg calcium | 222 | 63.3±7.5 | Not report | 1 |
| Alendronate | 218 | 64.1±6.7 | |||||||||
| Black (Fracture Intervention Trial) | 2000 | USA | X | X | Alendronate | 51M | 500 mg calcium + 250 IU vitamin D | 1841 | 69.8 | Not report | Not report |
| Placebo | 1817 | 70 | |||||||||
| Kung | 2000 | China | X | X | Alendronate 10 mg/d | 12M | Calcium 500 mg | 35 | 64±5 | 1 | Not report |
| placebo | 35 | 65±4 | |||||||||
| Lau | 2000 | China | X | X | Alendronate 10 mg/d | 12M | Calcium 500 mg daily | 41 | 74±0.7 | 0 | Not report |
| placebo | 37 | 74±0.7 | 0 | ||||||||
| Neer (fracture prevention trial) | 2001 | Worldwide | Vertebral fracture | X | Placebo | 21M | 500–1000 mg of calcium and 600–800 IU of vitamin D | 448 | 69.0±6.8 | Not report | Not report |
| Teriparatide 20 μg/d | 444 | 69.1±6.7 | |||||||||
| Teriparatide 40 μg/d | 434 | 69.6±6.8 | |||||||||
| Body | 2002 | Worldwide | X | X | 40 μg teriparatide oral placebo | 24M | 1000 mg of calcium + 400 to 1200 IU of vitamin D | 73 | 65±9 | 1 | 1 |
| Placebo + oral 10 mg alendronate | 73 | 66±8 | 0 | 0 | |||||||
| Author | Year | Location | All patients with fracture | Previous osteoporotic treatment | Intervention | Duration | Daily supplement treatment | Patients Number | Age | CV AE | CV death |
| Alan | 2003 | Worldwide | Vertebral fracture | X | Placebo | 21M | 1000 mg of calcium and 400 to 1200 IU of vitamin D | 1637 | 70.7 | Not report | Not report |
| Teriparatide 20 μg/d | |||||||||||
| Teriparatide 40 μg/d | |||||||||||
| Cryer | 2005 | USA | X | X | Alendronate 70 mg/wk | 6M | 1000 mg calcium in diet or 500 mg supplement | 224 | 64.6±10 | Not report | 0 |
| Placebo | 230 | 65.8±9.9 | 0 | ||||||||
| Gallagher | 2005 | Worldwide | Vertebral fracture | X | Placebo | 21M | 1000 mg calcium + 400 to 1200 IU of vitamin D | 544 | 69 ± 7 | Not report | Not report |
| Teriparatide 20 mg/d | 541 | 70±7 | |||||||||
| Ho | 2005 | China | X | X | Alendronate | 12M | Calcium 500 mg | 29 | 60.6±5.5 | 0 | 0 |
| Placebo | 29 | 62±4.0 | 0 | 0 | |||||||
| McClung | 2005 | USA | X | X | Alendronate 10 mg/day | 18M | 1000 mg calcium and 400 IU vitamin D | 101 | 66.6±8.5 | Not report | Not report |
| Teriparatide 20 μg/day | 102 | 65.3±8.4 | |||||||||
| Brown | 2009 | Worldwide | X | X | Denosumab 60 mg Q6M | 12M | >500 mg calcium daily + vitamin D | 594 | 64.1±8.6 | Not report | 1 |
| Alendronate 70 mg/week | 595 | 64.6±8.3 | |||||||||
| Not report | 0 | ||||||||||
| Eastell | 2009 | Europe | X | Use of anti-resorptive drug not excluded | Teriparatide 20 mg/day | 12M | 500mg calcium + 400 to 800 IU of vitamin D | 304 | 69.2±7.2 | 12 | 0 |
| Raloxifene 60 mg/day | 97 | 69.4±7.0 | 2 | 0 | |||||||
| No treatment | 102 | 69.1±8.6 | 2 | 0 | |||||||
| Kendler | 2009 | Worldwide | X | X | Alendronate 70 mg/week | 12M | Calcium 1000mg+Vit D > 400 IU/d | 251 | 68.2±7.7 | 0 | 0 |
| Denosumab 60 mg Q6M | 253 | 66.9±7.8 | 1 | 1 | |||||||
| Author | Year | Location | All patients with fracture | Previous osteoporotic treatment | Intervention | Duration | Daily supplement treatment | Patients Number | Age | CV AE | CV death |
| Miyauchi | 2010 | Japan | X | Conditionally included | Teriparatide 20 μg/day | 24M | 610 mg of calcium and 400–800 IU of vitamin D | 136 | 69.2±6.3 | Not report | Not report |
| Placebo | 67 | 70.4±5.4 | |||||||||
| Seeman | 2010 | Worldwide | X | Conditionally included | Placebo | 12M | Calcium >500 mg/d + vitamin D | 82 | 60.8±5.2 | Not reported | 0 |
| Alendronate 70 mg QW | 82 | 60.7±5.2 | 0 | ||||||||
| Denosumab 60 mg Q6M | 83 | 60.3±5.9 | 0 | ||||||||
| Henriksen | 2013 |
Denmark Estonia |
X | X | Placebo | 24W | 500 mg calcium + > 400 IU vitamin D | 29 | 65.8±6.2 | Not report | 0 |
| Oral rhPTH | 29 | 68.0±3.6 | 0 | ||||||||
| Teriparatide | 31 | 66.4±7.1 | 0 | ||||||||
| Tsai (DATA study) | 2013 | USA | X | X | Teriparatide 20 μg/day | 12M |
Total daily intakes of 1200 mg calcium Vit D > 50 nmol |
31 | 65.5±7.9 | 1 | 0 |
| Denosumab 60 mg Q6M | 33 | 66.3±8.3 | 0 | 0 | |||||||
| Combined treatment | 30 | 65.9±9.0 | 0 | 0 | |||||||
| Cosman (FRAME trial) | 2016 | Worldwide | X | X | Placebo | 24M | 500–1000 mg calcium + 600 to 800 IU vitamin D | 3591 | 70.8±6.9 | 41 | 15 |
| Romosozumab 210 mg/month | 3589 | 70.9±7.0 | 44 | 17 | |||||||
| Ishibashi | 2017 | Japan | X | Conditionally included | Placebo | 12M | >500 mg calcium + > 600 IU vitamin D | 63 | 67.8±7.2 | 0 | 0 |
| Romosozumab 70 mg/M | 63 | 66.5±6.3 | 0 | 0 | |||||||
| Romosozumab 140 mg/M | 63 | 68.4±6.0 | 0 | 0 | |||||||
| Romosozumab 210 mg/M | 63 | 68.3±5.9 | 0 | 0 | |||||||
| Langdahl (STRUCTURE trial) | 2017 | America Europe | X | Oral bisphosphonate therapy | Romosozumab 210 mg/M | 12M | 500–1000 mg of calcium and 600–800 IU of vitamin D | 218 | 71.8±7.4 | 2 | 0 |
| Teriparatide 20 μg/day | 218 | 71.2±7.7 | 0 | 0 | |||||||
| Author | Year | Location | All patients with fracture | Previous osteoporotic treatment | Intervention | Duration | Daily supplement treatment | Patients Number | Age | CV AE | CV death |
| Saag (ARCH trial) | 2017 | Worldwide | Fragile fracture | X | Alendronate 70 mg/week | 12M | 500–1000 mg calcium and 600–800 IU vitamin D | 2047 | 74.2±7.5 | 38 | 12 |
| Romosozumab 210 mg/M | 2046 | 74.4±7.5 | 50 | 17 | |||||||
| Baek | 2020 | Korean | X | After washout period | Romosozumab 210 mg/M | 6M | 500–1000 mg calcium + 600 to 800 IU of vitamin D | 34 | 66.7±7.6 | 1 | 0 |
| Placebo | 33 | 68.4±7.2 | 0 | 0 |
| Author | Year | Intervention | Vertebral fracture | Fracture number | Vertebral fracture degree |
|---|---|---|---|---|---|
| Devogelaer | 1996 | Placebo | NA | ||
| Alendronate 5 mg/d | NA | ||||
| Alendronate 10 mg/d | NA | ||||
| Alendronate 20 mg/d | NA | ||||
| Tucci | 1996 | Placebo | NA | ||
| Alendronate 5 mg/d | NA | ||||
| Alendronate 10 mg/d | NA | ||||
| Alendronate 20 mg/d | NA | ||||
| Felsenberg (FOSIT trail) | 1998 | Placebo | NA | ||
| Alendronate | |||||
| Black (Fracture Intervention Trial) | 2000 | Alendronate | 1022 | NA | |
| Placebo | 1005 | NA | |||
| Kung | 2000 | Alendronate 10 mg/d | 12 | NA | |
| Placebo | 14 | NA | |||
| Lau | 2000 | Alendronate 10 mg/d | 4 | NA | |
| Placebo | 1 | NA | |||
| Neer (fracture prevention trial) | 2001 | Placebo | 448 | 2.3±1.8 | NA |
| Teriparatide 20 μg/d | 444 | 2.3±1.8 | NA | ||
| Teriparatide 40 μg/d | 434 | 2.3±1.8 | NA | ||
| Body | 2002 | 40 μg teriparatide oral placebo | NA | ||
| Placebo + oral 10 mg Alendronate | NA | ||||
| Alan | 2003 | Placebo | 1637 | NA | NA |
| Teriparatide 20 μg/d | |||||
| Teriparatide 40 μg/d | |||||
| Cryer | 2005 | Alendronate 70 mg/wk | 0 | ||
| Placebo | 0 | ||||
| Gallagher | 2005 | Placebo | 544 | 2.6±1.7 | 1.9±0.7 |
| Teriparatide 20 mg/d | 541 | 2.5±1.7 | 1.9±0.7 | ||
| Ho | 2005 | Alendronate | 12 | NA | NA |
| Placebo | 10 | NA | NA | ||
| McClung | 2005 | Alendronate 10 mg/d | NA | ||
| Teriparatide 20 μg/d | NA | ||||
| Brown | 2009 | Denosumab 60 mg Q6M | NA | ||
| Alendronate 70 mg/wk | NA | ||||
| Eastell | 2009 | Teriparatide 20 mg/d | NA | ||
| Raloxifene 60 mg/d | NA | ||||
| No treatment | NA | ||||
| Kendler | 2009 | Alendronate 70 mg/wk | NA | ||
| Denosumab 60 mg Q6M | NA | ||||
| Miyauchi | 2010 | Teriparatide 20 μg/d | 54 | 35/10/9 | NA |
| Placebo | 29 | 18/8/5 | NA | ||
| Author | Year | Intervention | Vertebral fracture | Fracture number | Vertebral fracture degree |
| Miyauchi | 2010 | Teriparatide 20 μg/d | 54 | 35/10/9 | NA |
| Placebo | 29 | 18/8/5 | NA | ||
| Seeman | 2010 | Placebo | 0 | ||
| Alendronate 70 mg QW | 0 | ||||
| Denosumab 60 mg Q6M | 0 | ||||
| Henriksen | 2013 | Placebo | NA | ||
| Oral rhPTH | NA | ||||
| Teriparatide | NA | ||||
| Tsai (DATA study) | 2013 | Teriparatide 20 μg/d | NA | ||
| Denosumab 60 mg Q6M | NA | ||||
| Combined treatment | NA | ||||
| Cosman (FRAME trial) | 2016 | Placebo | 645 | 496/149 | 378/263/4 |
| Romosozumab 210 mg/M | 672 | 506/166 | 378/293/1 | ||
| Ishibashi | 2017 | Placebo | 0 | ||
| Romosozumab 70 mg/M | 0 | ||||
| Romosozumab 140 mg/M | 0 | ||||
| Romosozumab 210 mg/M | 0 | ||||
| Langdahl (STRUCTURE trial) | 2017 | Romosozumab 210 mg/M | NA | ||
| Teriparatide 20 μg/d | NA | ||||
| Saag (ARCH trial) | 2017 | Alendronate 70 mg/wk | 1964 | NA | 73/570/1321 |
| Romosozumab 210 mg/M | 1969 | NA | 68/532/1369 | ||
| Baek | 2020 | Romosozumab 210 mg/M | NA | ||
| Placebo | NA |
CV AE cardiovascular adverse events, d days, IU international units, M month, NA not applicable, Q6M every six months, QW every week, rhPTH recombinant human parathyroid hormone, wk week
Cardiovascular Outcomes
A total of 13 RCTs (n = 14,304) had available information regarding cardiovascular mortality, and these studies contributed to a five-node consistency model involving alendronate (n = 3221), denosumab (n = 286), romosozumab (n = 6076), teriparatide (n = 349), and placebo (n = 4372) (Fig. 2A). Besides, eight direct comparisons existed among the four medications and placebo without significant heterogeneity (Table S4). Based on available data, the incidence of cardiovascular death was approximately 500 per 100,000 individuals, and the values approximated the incidence in the placebo group (Fig. S1). Pooled results with placebo as the reference did not identify any significant finding (Fig. 3A), while alendronate exhibited a slight reduction trend among all treatments (Table 2). The results of the network meta-analysis for cardiovascular mortality showed no evidence of inconsistency, as confirmed by the SIDE method and design-by-treatment interaction model (Table S5). Besides, no significant asymmetry was observed in the comparison-adjusted funnel plot for the synthesis of cardiovascular mortality (Fig. 4A). Concerning the influence of age within the network evidence of cardiovascular mortality, as evidenced by representative simulations (Fig. S2), the majority of shrinkage occurred within an acceptable threshold in terms of shrink factor 1.1 (Fig. S3), with deviance leverage consistently remaining around 2 (Figs S4 and S5). Age exhibited no significant influence on the result of network evidence (log RR = −0.267; Table S6). Furthermore, no discernible association was observed between age and the risk of cardiovascular mortality as influenced by the administered medications (Fig. S6), a trend observed consistently at the age of 60 years (Table S7) and 70 years (Table S8). With acceptable convergence and shrinkage (Figs S7 to S10), no significant difference in cardiovascular mortality risk was observed between medications and placebo after adjusting for calcium supplementation in the consistency model (Tables S9 and S10).
Fig. 2.

Network graphs for A cardiovascular death, B cardiovascular event, and C adverse event. Structure of the network evidence shows most pairwise comparisons consisting of direct evidence. The purple shade refers to a three-arm trial comparing teriparatide, raloxifene, and placebo
Fig. 3.
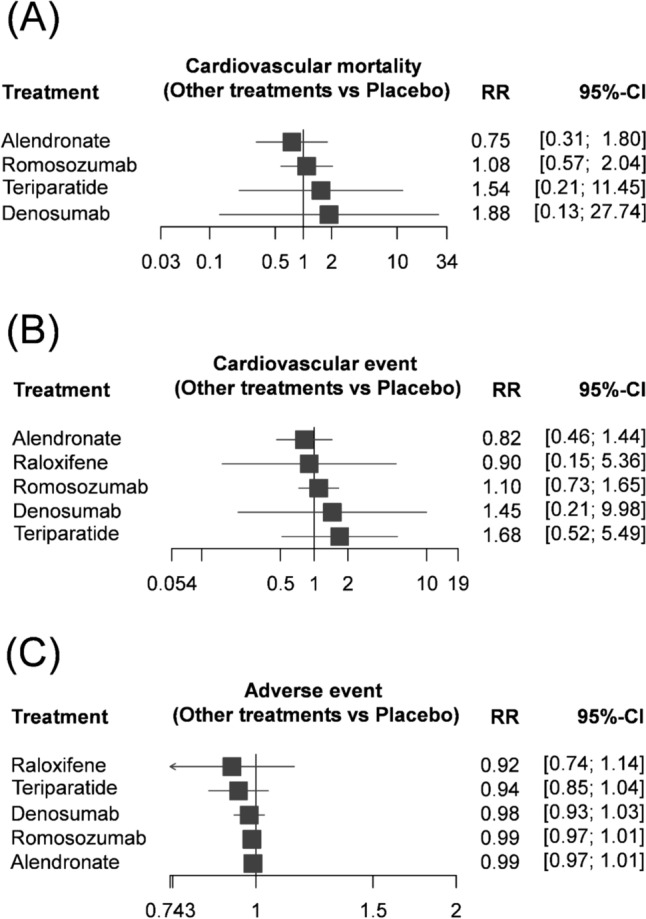
Forest plots of A cardiovascular death, B cardiovascular event, and C adverse event. The anti-osteoporosis drugs in this study did not result in significantly higher rates of cardiovascular death, cardiovascular events, or adverse events. CI confidence interval, RR risk ratio
Table 2.
League table of network meta-analysis findings. Risk ratio (95% confidence interval)
| Cardiovascular death | |||||
|---|---|---|---|---|---|
| Romosozumab | |||||
| – | Raloxifene | ||||
| 0.58 (0.04–8.16) | – | Denosumab | |||
| 0.70 (0.10–5.03) | – | 1.22 (0.08–18.72) | Teriparatide | ||
| 1.44 (0.73–2.86) | – | 2.50 (0.19–33.38) | 2.05 (0.29–14.52) | Alendronate | |
| 1.08 (0.57–2.04) | – | 1.88 (0.13–27.74) | 1.54 (0.21–11.45) | 0.75 (0.31–1.80) | Placebo |
| Cardiovascular event | |||||
|---|---|---|---|---|---|
| Romosozumab | |||||
| 1.22 (0.20–7.37) | Raloxifene | ||||
| 0.76 (0.11–5.11) | 0.62 (0.05–7.18) | Denosumab | |||
| 0.65 (0.20–2.17) | 0.54 (0.12–2.34) | 0.86 (0.11–6.44) | Teriparatide | ||
| 1.34 (0.89–2.02) | 1.10 (0.18–6.85) | 1.77 (0.27–11.69) | 2.06 (0.60–7.09) | Alendronate | |
| 1.10 (0.73–1.65) | 0.90 (0.15–5.36) | 1.45 (0.21–9.98) | 1.68 (0.52–5.49) | 0.82 (0.46–1.44) | Placebo |
| Adverse event | |||||
|---|---|---|---|---|---|
| Romosozumab | |||||
| 1.07 (0.86–1.33) | Raloxifene | ||||
| 1.01 (0.96–1.06) | 0.94 (0.76–1.17) | Denosumab | |||
| 1.05 (0.95–1.16) | 0.98 (0.80–1.20) | 1.04 (0.93–1.16) | Teriparatide | ||
| 1.00 (0.98–1.01) | 0.93 (0.75–1.15) | 0.99 (0.94–1.03) | 0.95 (0.86–1.05) | Alendronate | |
| 0.99 (0.97–1.01) | 0.92 (0.74–1.14) | 0.98 (0.93–1.03) | 0.94 (0.85–1.04) | 0.99 (0.97–1.01) | Placebo |
Fig. 4.

Funnel plots of A cardiovascular death, B cardiovascular event, and C adverse event. NS non-significant
Another important outcome was cardiovascular event. Twelve trials had relevant information to form a six-node consistency model with a total of 14,556 postmenopausal women. The model consisted of alendronate (n = 3027), denosumab (n = 879), raloxifene (n = 97), romosozumab (n = 6076), teriparatide (n = 622), and placebo (n = 3855) (Fig. 2B). This six-node consistency model was based on 10 direct comparisons with very low heterogeneity (I2 < 25%; Table S11). The direct evidence did not own any significant finding, and the network meta-analysis with placebo as reference also showed no significant difference in the risk of cardiovascular event among the six intervention groups (Fig. 3B and Table 2). The network meta-analysis of cardiovascular events showed no significant inconsistency according to the SIDE method and design-by-treatment interaction model (Table S12), and the comparison-adjusted funnel plot for the synthesis of cardiovascular event showed no major asymmetry (Fig. 4B). In testing the influence of age on the network model of cardiovascular events, as demonstrated by representative simulations (Fig. S11), the bulk of shrinkage was observed within 1.05 (Fig. S12), and deviance leverage remained within acceptable parameters, typically below 3 (Figs S13 and S14). Age itself did not exert a significant effect on the network evidence (log RR = −1.529; 95% CrI −10.744–3.223; Table S13). Moreover, there was no association between age and the risk of cardiovascular events influenced by the administered medications (Fig. S15), a trend consistently observed at the age of 60 years (Table S14) and 70 years (Table S15). With acceptable convergence and shrinkage in the network meta-regression of cardiovascular events by dosage of calcium supplementation (Figs S16 to S19), no significant finding was observed (Tables S16 and S17).
Other Adverse Event
Information on other adverse events was available for all 17 RCTs (n = 16,514), and a six-node consistency model was formed using alendronate (n = 4101), denosumab (n = 879), raloxifene (n = 97), romosozumab (n = 6076), teriparatide (n = 622), and placebo (n = 4739 (Fig. 2B). This network meta-analysis was based on 10 direct comparisons with very low heterogeneity (I2 < 25%), and the direct evidence did not show any significant difference in the overall adverse event rate between each pairwise comparison (Table S18). Similarly, network meta-analysis revealed no significant difference in any comparison (Fig. 3C and Table 2). The network meta-analysis of the overall adverse events showed no major inconsistency according to the SIDE method and design-by-treatment interaction model (Table S19), and the comparison-adjusted funnel plot for the synthesis of overall adverse events showed no significant asymmetry (Fig. 4C). In evaluating the influence of age on the network model of adverse events, as illustrated by representative simulations (Fig. S20), there was acceptable shrinkage (Fig. S21), with deviance leverage consistently below 3, thus falling within acceptable thresholds (Figs S22 and S23). Age showed no significant impact on the network evidence (log RR = −0.110; 95% CrI −1.842–0.096; Table S20). Furthermore, there was no apparent association between age and the risk of adverse events influenced by the administered medications (Fig. S24), a trend consistently observed across both 60- (Table S21) and 70-year-olds (Table S22).
Certainty of Evidence
The certainty of evidence for cardiovascular mortality, cardiovascular events, and adverse events is presented in Tables S23 to S25. For cardiovascular mortality, evidence was generally rated as low confidence due to concerns regarding within-study bias and imprecision across several comparisons of osteoporosis treatments. Similarly, evidence pertaining to cardiovascular events varied from low to moderate confidence, with primary concerns related to within-study bias and imprecision. Evidence regarding overall adverse events consistently received a moderate confidence rating, with the main issues attributed to within-study bias and imprecision. These evaluations provide a comprehensive overview of the strengths and limitations of the available evidence.
Discussion
This study found that romosozumab, denosumab, teriparatide, and alendronate have similar effects on major cardiovascular events and cardiovascular mortality, with no significant increase in cardiovascular risk compared to the placebo group. Specifically, the pooled cardiovascular mortality rate for romosozumab was 548 per 100,000, which falls within the global range of cardiovascular disease mortality rates for females aged 50–74 years (366–611 per 100,000) between 1990 and 2021 [45]. This suggests that the anti-osteoporotic agents may have little impact on cardiovascular death in patients. The present evidence appears to be unaffected by age.
Romosozumab, a humanized monoclonal antibody, is an anti-osteoporotic medication that inhibits sclerostin, a protein essential for normal bone metabolism. Sclerostin inhibits bone formation by decreasing osteoblastic activity [46]. Romosozumab accelerates bone stock accumulation by simultaneously increasing bone formation and reducing bone resorption by inhibiting sclerostin [9]. However, since sclerostin also inhibits vascular calcification [11, 12], inhibiting sclerostin may potentially have harmful effects. Research in animal models suggests a protective effect of sclerostin against arterial calcification and aortic aneurysm [47, 48]. However, large trials have yielded conflicting evidence in this regard [10, 13]. The ARCH trial found a significant increase in serious cardiac incidents and cardiac ischemia. However, the FRAME placebo-controlled trial found no significant risk of cardiac incidents or ischemia. Additionally, a subgroup analysis of the Asian population showed no significant effect on cardiovascular events [49]. Several hypotheses have been proposed to explain the phenomenon. Some authors attributed the differences purely to chance, whereas the potential cardiovascular protective effect of bisphosphonates is another likely explanation [50]. For decades, the impact of bisphosphonates on the cardiovascular system has remained uncertain, with some meta-analyses finding no potential benefit [51, 52]. The precise effect of alendronate on cardiovascular safety remains unclear due to inadequate evidence. Our study found no evidence that alendronate reduces cardiovascular events or mortality through either direct or indirect comparisons. One potential explanation is that the cardiovascular effects of alendronate balance each other out, leading to no significant increase or decrease in risk. This balance could occur when mechanisms that increase risk and those that offer protection operate simultaneously in patients, effectively offsetting each other.
Our synthesis included denosumab, a RANK ligand inhibitor that inhibits osteoclastic activity. RANK ligands, produced by osteoblasts or endothelial cells, bind to RANK receptors on osteoclast precursors or vascular smooth muscle cells (VSMCs), contributing to osteoclast maturation and bone resorption in bone tissue [53]. In vascular calcification, VSMCs undergo a phenotypic transformation into osteochondrogenic cells, promoting the deposition of mineralized matrix [53]. These mechanisms suggest that the cardiovascular effects of denosumab may be mediated via this pathway [54]. However, previous RCTs, including the Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) trial, which involved 7868 women treated with denosumab, found no significant differences in cardiovascular events, stroke, coronary heart disease, peripheral vascular disease, or atrial fibrillation [55]. Our study’s comparison of denosumab with other therapies yielded similar results, consistent with earlier research findings.
Calcium and vitamin D supplements are often used as adjuvant treatments in osteoporosis trials, but their impact on the cardiovascular system should be considered. High-dose calcium supplementation may lead to arterial and soft tissue calcification, and the effect of regular dosage of calcium on cardiovascular morbidity is still being studied. The study and meta-analysis by Bolland et al found that calcium may increase the risk of ischemic heart disease [56, 57], but subsequent trials and meta-analyses yielded inconsistent results [58–60]. Therefore, the effect of calcium supplementation on cardiovascular health remains uncertain. However, a daily intake of 1000 mg of calcium has been shown to reduce fracture risk without increasing the risk of cardiovascular events [61]. Since all studies in our review included calcium supplementation (500–1000 mg) as an adjuvant therapy, we hypothesized its effect might be overlooked. Similar concerns prevail regarding vitamin D treatment. Vitamin D can impact the cardiovascular system by affecting blood calcium and myocardial calcification [54]. This theoretical effect, however, was not observed in prior trials [58, 62]. Meta-analysis of data from multiple studies also found no evidence of a harmful effect of vitamin D on cardiovascular health [63]. Although some studies incorporated vitamin D supplements in their study protocol, we considered that its effect was likely negligible and did not need to be discussed independently in our meta-analysis.
Some limitations of this synthesis should be considered before clinical application. First, variability in the definition of osteoporosis across RCTs and lack of information on the severity of osteoporosis may have impacted the results. Second, this study only compared romosozumab with some commonly used mono-therapies since the main concerns regarding the risk of cardiac events have been raised from the romosozumab versus alendronate comparison. Further research on other medications or medication strategies is warranted. Third, many studies did not report the risk of specific cardiac events, limiting the ability to provide detailed information for individual cardiac events of interest. We recommend that future relevant trials should separately report different cardiac events. Fourth, there was limited availability of data to differentiate between patients with and without ≥ grade 2 vertebral fractures. Therefore, the present study cannot analyze the specific impact of vertebral fracture severity on medication outcomes in detail. Future studies should provide detailed information on vertebral fracture severity. Last, determining the cardiovascular risk level is a complex matter, and the present synthesis cannot provide clear recommendations based on risk levels. Real-world evidence also underscores the complexities of using romosozumab in individuals at cardiovascular risk [64, 65], as romosozumab may not be advisable for patients at high risk [65, 66].
Conclusions
The current evidence implies that romosozumab may be a safe option for postmenopausal women with osteoporosis, as it does not appear to significantly increase the risk of cardiovascular complications or mortality. This finding might help alleviate concerns about cardiovascular risk associated with romosozumab use. However, further observation in real-world practice is necessary to confirm these results and ensure the long-term safety of romosozumab in this patient population.
Supplementary Information
Below is the link to the electronic supplementary material.
Declarations
Funding
Open Access funding enabled and organized by National Yang Ming Chiao Tung University.
Conflict of interest
Shih-Hao Cheng, William Chu, Wen-Hsiang Chou, Woei-Chyn Chu, Yi-No Kang declare that they have no conflict of interest.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Data in this study are available to other researchers upon reasonable request to corresponding author Y.N.K.
Code availability
Not applicable.
Author contributions
Shih-Hao Cheng: conceptualization, data curation, investigation, interpretation, validation, writing—original draft. William Chu: interpretation, supervision, validation. Wen-Hsiang Chou: supervision. Woei-Chyn Chu: interpretation, supervision, validation, writing—review and editing. Yi-No Kang: formal analysis, visualization, writing—review and editing. All authors read and approved the final version.
Footnotes
Woei Chyn Chu and Yi No Kang: Equal contribution.
Contributor Information
Woei-Chyn Chu, Email: wchu@nycu.edu.tw.
Yi-No Kang, Email: academicnono@gmail.com.
References
- 1.Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22(3):465–75. [DOI] [PubMed] [Google Scholar]
- 2.Black DM, Rosen CJ. Clinical Practice. Postmenopausal Osteoporosis. N Engl J Med. 2016;374(3):254–62. [DOI] [PubMed] [Google Scholar]
- 3.Camacho PM, Petak SM, Binkley N, Diab DL, Eldeiry LS, Farooki A, et al. American Association of Clinical Endocrinologists/American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis-2020 Update. Endocr Pract. 2020;26(Suppl 1):1–46. [DOI] [PubMed] [Google Scholar]
- 4.Kanis JA, Harvey NC, McCloskey E, Bruyere O, Veronese N, Lorentzon M, et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos Int. 2020;31(1):1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.El Khoudary SR, Aggarwal B, Beckie TM, Hodis HN, Johnson AE, Langer RD, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation. 2020;142(25):e506–32. [DOI] [PubMed] [Google Scholar]
- 6.Rosano GM, Vitale C, Marazzi G, Volterrani M. Menopause and cardiovascular disease: the evidence. Climacteric. 2007;10(Suppl 1):19–24. [DOI] [PubMed] [Google Scholar]
- 7.Lim SY, Bolster MB. Profile of romosozumab and its potential in the management of osteoporosis. Drug Des Dev Ther. 2017;11:1221–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rauner M, Taipaleenmaki H, Tsourdi E, Winter EM. Osteoporosis treatment with anti-sclerostin antibodies-mechanisms of action and clinical application. J Clin Med. 2021;10(4):787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chavassieux P, Chapurlat R, Portero-Muzy N, Roux JP, Garcia P, Brown JP, et al. Bone-forming and antiresorptive effects of romosozumab in postmenopausal women with osteoporosis: bone histomorphometry and microcomputed tomography analysis after 2 and 12 months of treatment. J Bone Miner Res. 2019;34(9):1597–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cosman F, Crittenden DB, Adachi JD, Binkley N, Czerwinski E, Ferrari S, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med. 2016;375(16):1532–43. [DOI] [PubMed] [Google Scholar]
- 11.Turk JR, Deaton AM, Yin J, Stolina M, Felx M, Boyd G, et al. Nonclinical cardiovascular safety evaluation of romosozumab, an inhibitor of sclerostin for the treatment of osteoporosis in postmenopausal women at high risk of fracture. Regul Toxicol Pharmacol. 2020;115:104697. [DOI] [PubMed] [Google Scholar]
- 12.Zheng J, Wheeler E, Pietzner M, Andlauer TFM, Yau MS, Hartley AE, et al. Lowering of circulating sclerostin may increase risk of atherosclerosis and its risk factors: evidence from a genome-wide association meta-analysis followed by Mendelian randomization. Arthritis Rheumatol. 2023;75(10):1781–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Saag KG, Petersen J, Brandi ML, Karaplis AC, Lorentzon M, Thomas T, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med. 2017;377(15):1417–27. [DOI] [PubMed] [Google Scholar]
- 14.Wu ST, Chen JF, Tsai CJ. The impact of bisphosphonates on mortality and cardiovascular risk among osteoporosis patients after cardiovascular disease. J Formos Med Assoc. 2021;120(11):1957–66. [DOI] [PubMed] [Google Scholar]
- 15.Casula M, Olmastroni E, Galimberti F, Tragni E, Corrao G, Scotti L, et al. Association between the cumulative exposure to bisphosphonates and hospitalization for atherosclerotic cardiovascular events: a population-based study. Atherosclerosis. 2020;301:1–7. [DOI] [PubMed] [Google Scholar]
- 16.Rodriguez AJ, Ernst MT, Nybo M, Prieto-Alhambra D, Ebeling PR, Hermann AP, et al. Oral bisphosphonate use reduces cardiovascular events in a cohort of Danish patients referred for bone mineral density. J Clin Endocrinol Metab. 2020;105(10):3215–25. [DOI] [PubMed] [Google Scholar]
- 17.Kobayakawa T, Suzuki T, Nakano M, Saito M, Miyazaki A, Takahashi J, et al. Real-world effects and adverse events of romosozumab in Japanese osteoporotic patients: a prospective cohort study. Bone Rep. 2021;14: 101068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kobayakawa T, Miyazaki A, Saito M, Suzuki T, Takahashi J, Nakamura Y. Denosumab versus romosozumab for postmenopausal osteoporosis treatment. Sci Rep. 2021;11(1):11801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88: 105906. [DOI] [PubMed] [Google Scholar]
- 20.Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898. [DOI] [PubMed] [Google Scholar]
- 21.Nikolakopoulou A, Higgins JPT, Papakonstantinou T, Chaimani A, Del Giovane C, Egger M, et al. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17(4): e1003082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Baek KH, Chung YS, Koh JM, Kim IJ, Kim KM, Min YK, et al. Romosozumab in postmenopausal korean women with osteoporosis: a randomized, double-blind, placebo-controlled efficacy and safety study. Endocrinol Metab (Seoul). 2021;36(1):60–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, et al. Fracture risk reduction with alendronate in women with osteoporosis: the fracture intervention trial. J Clin Endocrinol Metab. 2000;85(11):4118–24. [DOI] [PubMed] [Google Scholar]
- 24.Body JJ, Gaich GA, Scheele WH, Kulkarni PM, Miller PD, Peretz A, et al. A randomized double-blind trial to compare the efficacy of teriparatide [recombinant human parathyroid hormone (1–34)] with alendronate in postmenopausal women with osteoporosis. J Clin Endocrinol Metab. 2002;87(10):4528–35. [DOI] [PubMed] [Google Scholar]
- 25.Brown JP, Prince RL, Deal C, Recker RR, Kiel DP, de Gregorio LH, et al. Comparison of the effect of denosumab and alendronate on BMD and biochemical markers of bone turnover in postmenopausal women with low bone mass: a randomized, blinded, phase 3 trial. J Bone Miner Res. 2009;24(1):153–61. [DOI] [PubMed] [Google Scholar]
- 26.Cryer B, Binkley N, Simonelli C, Lewiecki EM, Lanza F, Chen E, et al. A randomized, placebo-controlled, 6-month study of once-weekly alendronate oral solution for postmenopausal osteoporosis. Am J Geriatr Pharmacother. 2005;3(3):127–36. [DOI] [PubMed] [Google Scholar]
- 27.Devogelaer JP, Broll H, Correa-Rotter R, Cumming DC, De Deuxchaisnes CN, Geusens P, et al. Oral alendronate induces progressive increases in bone mass of the spine, hip, and total body over 3 years in postmenopausal women with osteoporosis. Bone. 1996;18(2):141–50. [DOI] [PubMed] [Google Scholar]
- 28.Eastell R, Nickelsen T, Marin F, Barker C, Hadji P, Farrerons J, et al. Sequential treatment of severe postmenopausal osteoporosis after teriparatide: final results of the randomized, controlled european study of forsteo (EUROFORS). J Bone Miner Res. 2009;24(4):726–36. [DOI] [PubMed] [Google Scholar]
- 29.Felsenberg D, Alenfeld F, Beck O, Hammermeister C, Gowan W, Grp FS. Placebo-controlled multicenter study of oral alendronate in postmenopausal osteoporotic women. Maturitas. 1998;31(1):35–44. [DOI] [PubMed] [Google Scholar]
- 30.Gallagher JC, Genant HK, Crans GG, Vargas SJ, Krege JH. Teriparatide reduces the fracture risk associated with increasing number and severity of osteoporotic fractures. J Clin Endocrinol Metab. 2005;90(3):1583–7. [DOI] [PubMed] [Google Scholar]
- 31.Henriksen K, Andersen JR, Riis BJ, Mehta N, Tavakkol R, Alexandersen P, et al. Evaluation of the efficacy, safety and pharmacokinetic profile of oral recombinant human parathyroid hormone [rhPTH(1–31)NH(2)] in postmenopausal women with osteoporosis. Bone. 2013;53(1):160–6. [DOI] [PubMed] [Google Scholar]
- 32.Ho AYY, Kung AWC. Efficacy and tolerability of alendronate once weekly in Asian postmenopausal osteoporotic women. Ann Pharmacother. 2005;39(9):1428–33. [DOI] [PubMed] [Google Scholar]
- 33.Ishibashi H, Crittenden DB, Miyauchi A, Libanati C, Maddox J, Fan M, et al. Romosozumab increases bone mineral density in postmenopausal Japanese women with osteoporosis: a phase 2 study. Bone. 2017;103:209–15. [DOI] [PubMed] [Google Scholar]
- 34.Kendler DL, Roux C, Benhamou CL, Brown JP, Lillestol M, Siddhanti S, et al. Effects of denosumab on bone mineral density and bone turnover in postmenopausal women transitioning from alendronate therapy. J Bone Miner Res. 2010;25(1):72–81. [DOI] [PubMed] [Google Scholar]
- 35.Kung AWC, Yeung SSC, Chu LW. The efficacy and tolerability of alendronate in postmenopausal osteoporotic Chinese women: a randomized placebo-controlled study. Calcif Tissue Int. 2000;67(4):286–90. [DOI] [PubMed] [Google Scholar]
- 36.Langdahl BL, Libanati C, Crittenden DB, Bolognese MA, Brown JP, Daizadeh NS, et al. Romosozumab (sclerostin monoclonal antibody) versus teriparatide in postmenopausal women with osteoporosis transitioning from oral bisphosphonate therapy: a randomised, open-label, phase 3 trial. Lancet. 2017;390(10102):1585–94. [DOI] [PubMed] [Google Scholar]
- 37.Lau EMC, Woo J, Chan YH, Griffith J. Alendronate prevents bone loss in Chinese women with osteoporosis. Bone. 2000;27(5):677–80. [DOI] [PubMed] [Google Scholar]
- 38.McClung MR, San Martin J, Miller PD, Civitelli R, Bandeira F, Omizo M, et al. Opposite bone remodeling effects of teriparatide and alendronate in increasing bone mass. Arch Intern Med. 2005;165(15):1762–8. [DOI] [PubMed] [Google Scholar]
- 39.Miyauchi A, Matsumoto T, Sugimoto T, Tsujimoto M, Warner MR, Nakamura T. Effects of teriparatide on bone mineral density and bone turnover markers in Japanese subjects with osteoporosis at high risk of fracture in a 24-month clinical study: 12-Month, randomized, placebo-controlled, double-blind and 12-month open-label phases. Bone. 2010;47(3):493–502. [DOI] [PubMed] [Google Scholar]
- 40.Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, et al. Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–41. [DOI] [PubMed] [Google Scholar]
- 41.Oglesby AK, Minshall ME, Shen W, Xie S, Silverman SL. The impact of incident vertebral and non-vertebral fragility fractures on health-related quality of life in established postmenopausal osteoporosis: results from the teriparatide randomized, placebo-controlled trial in postmenopausal women. J Rheumatol. 2003;30(7):1579–83. [PubMed] [Google Scholar]
- 42.Seeman E, Cheung A, Shane E, Thomas T, Boyd S, Boutroy S, et al. Relationship between baseline remodelling intensity and changes in HR-pQCT parameters at the radius in postmenopausal women treated with denosumab or alendronate. Osteoporos Int. 2010;21:S362–3. [Google Scholar]
- 43.Tsai JN, Uihlein AV, Lee H, Kumbhani R, Siwila-Sackman E, McKay EA, et al. Teriparatide and denosumab, alone or combined, in women with postmenopausal osteoporosis: the DATA study randomised trial. Lancet. 2013;382(9886):50–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tucci JR, Tonino RP, Emkey RD, Peverly CA, Kher U, Santora AC 2nd. Effect of three years of oral alendronate treatment in postmenopausal women with osteoporosis. Am J Med. 1996;101(5):488–501. [DOI] [PubMed] [Google Scholar]
- 45.Institute for Health Metrics and Evaluation (IHME). GBD Compare. Seattle: IHME, University of Washington; 2021.
- 46.Compton JT, Lee FY. A review of osteocyte function and the emerging importance of sclerostin. J Bone Jt Surg Am. 2014;96(19):1659–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Krishna SM, Seto SW, Jose RJ, Li J, Morton SK, Biros E, et al. Wnt signaling pathway inhibitor sclerostin inhibits angiotensin ii-induced aortic aneurysm and atherosclerosis. Arterioscler Thromb Vasc Biol. 2017;37(3):553–66. [DOI] [PubMed] [Google Scholar]
- 48.Shao JS, Cheng SL, Pingsterhaus JM, Charlton-Kachigian N, Loewy AP, Towler DA. Msx2 promotes cardiovascular calcification by activating paracrine Wnt signals. J Clin Investig. 2005;115(5):1210–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lau EMC, Dinavahi R, Woo YC, Wu CH, Guan J, Maddox J, et al. Romosozumab or alendronate for fracture prevention in East Asian patients: a subanalysis of the phase III, randomized ARCH study. Osteoporos Int. 2020;31(4):677–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Cummings SR, McCulloch C. Explanations for the difference in rates of cardiovascular events in a trial of alendronate and romosozumab. Osteoporos Int. 2020;31(6):1019–21. [DOI] [PubMed] [Google Scholar]
- 51.Kranenburg G, Bartstra JW, Weijmans M, de Jong PA, Mali WP, Verhaar HJ, et al. Bisphosphonates for cardiovascular risk reduction: a systematic review and meta-analysis. Atherosclerosis. 2016;252:106–15. [DOI] [PubMed] [Google Scholar]
- 52.Kim DH, Rogers JR, Fulchino LA, Kim CA, Solomon DH, Kim SC. Bisphosphonates and risk of cardiovascular events: a meta-analysis. PLoS One. 2015;10(4): e0122646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tsang HG, Rashdan NA, Whitelaw CB, Corcoran BM, Summers KM, MacRae VE. Large animal models of cardiovascular disease. Cell Biochem Funct. 2016;34(3):113–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Fuggle NR, Cooper C, Harvey NC, Al-Daghri N, Brandi ML, Bruyere O, et al. Assessment of cardiovascular safety of anti-osteoporosis drugs. Drugs. 2020;80(15):1537–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–65. [DOI] [PubMed] [Google Scholar]
- 56.Bolland MJ, Barber PA, Doughty RN, Mason B, Horne A, Ames R, et al. Vascular events in healthy older women receiving calcium supplementation: randomised controlled trial. BMJ. 2008;336(7638):262–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Bolland MJ, Avenell A, Baron JA, Grey A, MacLennan GS, Gamble GD, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ. 2010;29(341): c3691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Harvey NC, D’Angelo S, Paccou J, Curtis EM, Edwards M, Raisi-Estabragh Z, et al. Calcium and Vitamin D supplementation are not associated with risk of incident ischemic cardiac events or death: findings from the UK Biobank cohort. J Bone Miner Res. 2018;33(5):803–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Manson JE, Allison MA, Carr JJ, Langer RD, Cochrane BB, Hendrix SL, et al. Calcium/vitamin D supplementation and coronary artery calcification in the Women’s Health Initiative. Menopause. 2010;17(4):683–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Yang C, Shi X, Xia H, Yang X, Liu H, Pan D, et al. The evidence and controversy between dietary calcium intake and calcium supplementation and the risk of cardiovascular disease: a systematic review and meta-analysis of cohort studies and randomized controlled trials. J Am Coll Nutr. 2020;39(4):352–70. [DOI] [PubMed] [Google Scholar]
- 61.Prentice RL, Pettinger MB, Jackson RD, Wactawski-Wende J, Lacroix AZ, Anderson GL, et al. Health risks and benefits from calcium and vitamin D supplementation: Women’s Health Initiative clinical trial and cohort study. Osteoporos Int. 2013;24(2):567–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Barbarawi M, Kheiri B, Zayed Y, Barbarawi O, Dhillon H, Swaid B, et al. Vitamin D supplementation and cardiovascular disease risks in more than 83,000 individuals in 21 randomized clinical trials: a meta-analysis. JAMA Cardiol. 2019;4(8):765–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Mineta K, Nishisho T, Okada M, Kamada M, Sairyo K. Real-world effects, safety, and predictors of the effectiveness of romosozumab in primary and secondary osteoporosis: an observational study. Bone. 2024;186:117164. [DOI] [PubMed] [Google Scholar]
- 65.Stokar J, Szalat A. Cardiovascular safety of romosozumab vs PTH analogs for osteoporosis treatment: a propensity score matched cohort study. J Clin Endocrinol Metab. 2024. 10.1210/clinem/dgae173. [DOI] [PubMed] [Google Scholar]
- 66.Farr JN. Cardiovascular safety and romosozumab—the plot thickens. J Clin Endocrinol Metab. 2024. 10.1210/clinem/dgae313. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.