

Abstract
Purpose:
To assess and quantify teprotumumab’s effect on thyroid eye disease (TED)-related strabismus by change in measured horizontal and vertical deviations, and change in extraocular motility.
Methods:
We reviewed a series of patients with TED-related strabismus treated with teprotumumab. Exclusion criteria included age under 18 years, strabismus of alternate etiology, or TED-related reconstructive surgery during the treatment course. Primary outcomes were absolute (prism diopters) and relative (%) differences in horizontal and vertical deviations in primary position at distance, as well as change in ductions of the more affected eye. Secondary outcomes included incidence and timing of strabismus surgery post-teprotumumab.
Results:
Thirty-one patients were included, with mean age 63 years and TED duration 10 months. After teprotumumab, there was 6 PD (39%) mean reduction in vertical deviation (p<0.001), without significant change in mean horizontal deviation (p=0.75). Supraduction, abduction, adduction, and infraduction significantly improved in the more restricted eye (p<0.01, p<0.01, p=0.04, p=0.01, respectively). Thirty-five percent of patients underwent strabismus surgery post-treatment, at an average 10 months after last infusion.
Conclusions:
Teprotumumab produced a statistically significant reduction in vertical but not horizontal strabismus angles in primary position at distance. Extraocular motility in all four ductions also improved. A substantial minority of patients still required strabismus surgery following teprotumumab.
Précis:
In this series of 31 patients with thyroid eye disease-related strabismus treated with teprotumumab, we report significant reduction in vertical deviations and improvement in extraocular motility, though a substantial minority of patients required post-treatment strabismus surgery.
Introduction
The pathophysiology of thyroid eye disease (TED) involves autoimmune-mediated upregulation of the thyroid-stimulating hormone receptor and insulin-like growth factor-1 receptor (IGF-1R) complex on orbital fibroblasts, ultimately leading to expansion of orbital fat and extraocular muscle volume, among other cellular and biochemical changes.1–4 Clinically this process manifests heterogeneously with features including proptosis, orbital inflammation, restrictive myopathy, and/or eyelid retraction.5 Particularly disabling aspects of TED include resultant strabismus and diplopia. 6
Despite the diversity in both medical and surgical therapy for TED, one of the most challenging features to manage is a resultant strabismus. In the active stage of disease, non-surgical treatment modalities include prism, monocular occlusion, and botulinum toxin muscle injections.7,8 Strabismus surgery is typically performed after stabilization of disease-related changes and any planned orbital intervention. However, achieving an optimal outcome can be challenging due to the variable inflammation and fibrosis of involved muscles.8
In January 2020, the US Food and Drug Administration approved teprotumumab (Tepezza, Horizon Pharmaceuticals, Deerfield, IL), a monoclonal antibody targeting IGF-1R, for treatment of TED following a phase III clinical trial that demonstrated efficacy in reducing proptosis, clinical activity score, and diplopia in patients with active TED.9 Several post-approval studies have since demonstrated proptosis reduction and diplopia improvement in patients with chronic disease, after retreatment following recurrence, and with partial teprotumumab treatment.10–13 These studies have largely reported changes in diplopia using the subjective Bahn-Gorman diplopia score, rather than quantifying alignment. The few studies that have reported motility suggest that teprotumumab treatment can reduce restriction, albeit without concomitant reduction in measured strabismus.14, 15 This study aimed to quantify the effect of teprotumumab on TED-related ocular alignment and extraocular motility.
Methods
Cohort Assembly:
This is a cross sectional cohort study comprised of adult patients with TED-related strabismus in primary position treated with teprotumumab. Approval was obtained by the Institutional Review Boards at the University of California, San Diego and University of California, Los Angeles. This report adheres to the ethical principles outlined in the Declaration of Helsinki as amended in 2013 and is HIPAA compliant.
Patients were identified from the pool of those presenting to the oculoplastic divisions of both participating institutions from September 2019 to December 2021, with a diagnosis of TED. Inclusion criteria were age ≥18 years, completion of ≥ 3 teprotumumab infusions, pre-treatment horizontal and/or vertical strabismus in primary position at distance and motility restriction secondary to TED. Exclusion criteria included strabismus of alternate etiology or TED-related reconstructive surgery (orbital decompression, strabismus, or eyelid surgery) during the teprotumumab course.
Study Design and Statistical Analysis:
Demographics, clinical examinations, laboratory reports, operative reports, and radiographic reports were extracted from electronic medical records. Pre-teprotumumab demographic variables of interest included age, sex, smoking history (none versus current or previous), time from patient reported TED onset in months, TED stage (active versus inactive) and history of TED-related surgery (including orbitotomy, orbital decompression, strabismus surgery and/or eyelid surgery).
Vertical and horizontal strabismus deviations were recorded in prism diopters (PD) as measured in primary position at distance. Alternate prism cover testing was completed by an ophthalmologist or certified orthoptist before (pre-) and after last teprotumumab infusion (post-). Where available, a mid-treatment measurement between the third and sixth infusions was recorded. The absolute differences (measured in prism diopters, PD) and relative differences (percent increase or decrease) in vertical and horizontal deviations pre- and post-teprotumumab were calculated. Extraocular motility limitation was scored using a standard 5-point, 0 to −4 scale (where 0 represents full motility and −4 represents inability to pass midline) for abduction, adduction, supraduction, and infraduction of each eye. The eye with the numerically largest negative sum of ductions in the four directions pre-treatment was considered the more affected eye.
Absolute differences were compared via paired t-test and relative differences compared via one-sample t-test, with p-values of <0.05 indicating statistical significance. A mixed effects linear regression model was fitted for vertical and horizontal deviations over time. Multivariable analyses considered age, sex, smoking history, and TED phase as covariates, though none of these variables conferred statistical significance. To evaluate change in ductions the difference in score between the post- and pre-teprotumumab time points was calculated and the Wilcoxon signed rank test applied. The incidence of post-teprotumumab strabismus surgery and time to strabismus surgery from last infusion measured in months were calculated.
Statistical analyses were performed using R Statistical Software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism 9.0.0 (GraphPad Software LLC; San Diego, California). Mixed effects models were fitted using the lme4 and lmerTest packages.16,17
Results
Thirty-one patients met inclusion criteria. Of these, 55% (17) were female. Mean time from reported TED onset to pre-treatment examination was 10 ± 10 months, and 61% (19) had active disease, of whom 1 patient was experiencing reactivation. Thirteen percent of patients had prior history of TED-related surgery including orbital decompression, strabismus surgery, and/or eyelid surgery (Table 1). One active TED patient had undergone orbitotomy with biopsy for diagnosis. Six patients completed less than 8 infusions. One patient received 3 infusions due to exacerbated colitis, 1 patient received 7 infusions due to infusion-related drug rash, 1 patient received 4 infusions due to an episode of infusion-related hypotension, and 3 patients received 6–7 infusions due to supply unavailability. Two patients received a total of 10 infusions each. Mean time from last infusion to post-teprotumumab examination was 49 ± 40 days.
Table 1:
Demographic and clinical characteristics (N=31)
| Age (years) | 63 ± 10 |
| Sex (% female) | 55 |
| TED onset (months) | 10 ± 10 |
| TED stage (%) | |
| Active | 61 |
| Inactive | 16 |
| Not reported | 23 |
| Smoking history (%) | |
| Yes | 39 |
| No | 61 |
| Prior TED-related surgery (%) | 13 |
| Orbitotomy with biopsy (n) | 1 |
| Orbital decompression (n) | 3 |
| Strabismus surgery (n) | 2 |
| Eyelid surgery (n) | 2 |
Table 2 presents changes in measured vertical deviation pre, mid-, and post-teprotumumab. There was a significant absolute decrease in vertical strabismus of 6 ± 6 PD (p<0.0001) post teprotumumab, representing a 39 ± 50% percent decrease (p=0.002). When controlling for age, sex, smoking history, and TED phase in a multivariable mixed effects model, mean vertical deviation remained significantly improved post-treatment (Figure 1). Figures 2 and 3 depict representative patients with restrictive hypotropia in primary position that decreased post-treatment.
Table 2:
Vertical deviation (prism diopters) pre-, mid-, and post-teprotumumab
| Descriptive Statistics | Absolute Difference | Relative Difference | |||
|---|---|---|---|---|---|
| (N) Mean ± SD | (N) Mean ± SD | 1 p | 2 Mean ± SD | 3 p | |
|
| |||||
| Pre | (24) 17 ± 12 | Ref | - | Ref | - |
| Mid | (15) 14 ± 12 | ||||
| Post | (24) 11 ± 12 | -6 ± 6 | <0.0001 | -39 ± 50% | 0.002 |
Paired sample t-test
Relative differences were calculated for 22 patients because 2 patients had reversal of direction of their deviation
One-sample t-test to null H0 = mean of 0
Figure 1:

Vertical deviations pre-, mid-, and post-teprotumumab with multivariable mixed effects model controlling for age, sex, TED phase, and smoking history with mean and its 95% confidence interval overlaid (N=17).
Figure 2:

TED with left hypotropia (A) in primary position with improvement in deviation post teprotumumab (B).
Figure 3:

TED with left hypotropia (A) with improvement in vertical deviation in sursumversion (top) and primary position (bottom) post- teprotumumab (B).
Three patients (3/24, 12.5%) with solely vertical deviations exhibited complete resolution to orthotropia post-teprotumumab. Two additional patients with both vertical and horizonal deviations experienced resolution of the vertical component and improvement but not resolution of the horizontal component. Pre-treatment vertical deviations in these groups measured between 5–10 PD. Two patients exhibited a reversal of the angle of their vertical deviation, one case of 5 PD left hypotropia to 1 PD right hypotropia, and another of 1 PD right hypotropia to a 5 PD left hypotropia. No patient developed a new vertical deviation post-teprotumumab.
Table 3 presents changes to mean horizontal deviation pre, mid-, and post-teprotumumab. The absolute measured change of −0.5 ±7 prism diopters, did not reach significance (p=0.75). A multivariable mixed effects model controlling for age, sex, smoking history, and TED phase demonstrated a similar lack of significant effect (Figure 4). Two patients who had a small angle horizontal deviation between 2–6 PD before treatment had resolution of their horizontal deviation. Both of these patients had a concurrent larger vertical deviation that improved but did not completely resolve. Six patients without horizontal deviation at baseline developed new horizontal deviation of between 2–10 prism diopters post-teprotumumab.
Table 3:
Horizontal deviation (prism diopters) pre-, mid, and post-teprotumumab.
| Descriptive Statistics | Absolute Difference | Relative Difference | |||
|---|---|---|---|---|---|
| (N) Mean ± SD | Mean ± SD | 1 p | 2 Mean ± SD | 3 p | |
|
| |||||
| Pre | (26) 12 ± 14 | Ref | - | Ref | - |
| Mid | (19) 8 ± 7 | ||||
| Post | (26) 11 ± 10 | -0.5 ± 7 | 0.75 | 1 ± 76% | 0.96 |
Paired sample t-test
Relative differences were calculated for 20 patients because 6 patients had pre values of 0
One-sample t-test to null H0 = mean of 0
Figure 4:

Horizontal deviations pre-, mid, and post-teprotumumab with multivariable mixed effects model controlling for age, sex, TED phase, and smoking history with mean and its 95% confidence interval overlaid (N=19).
Median [95% confidence interval] change in supraduction, abduction, infraduction, and adduction was 1.0 [0.0,1.0], 0.0 [0.0,1.0], 0.0 [0.0,0.5], and 0.0 [0.0,0.5], respectively (Figure 5). These were all significant (p<0.01, p<0.01, p=0.01, p=0.04 respectively).
Figure 5:
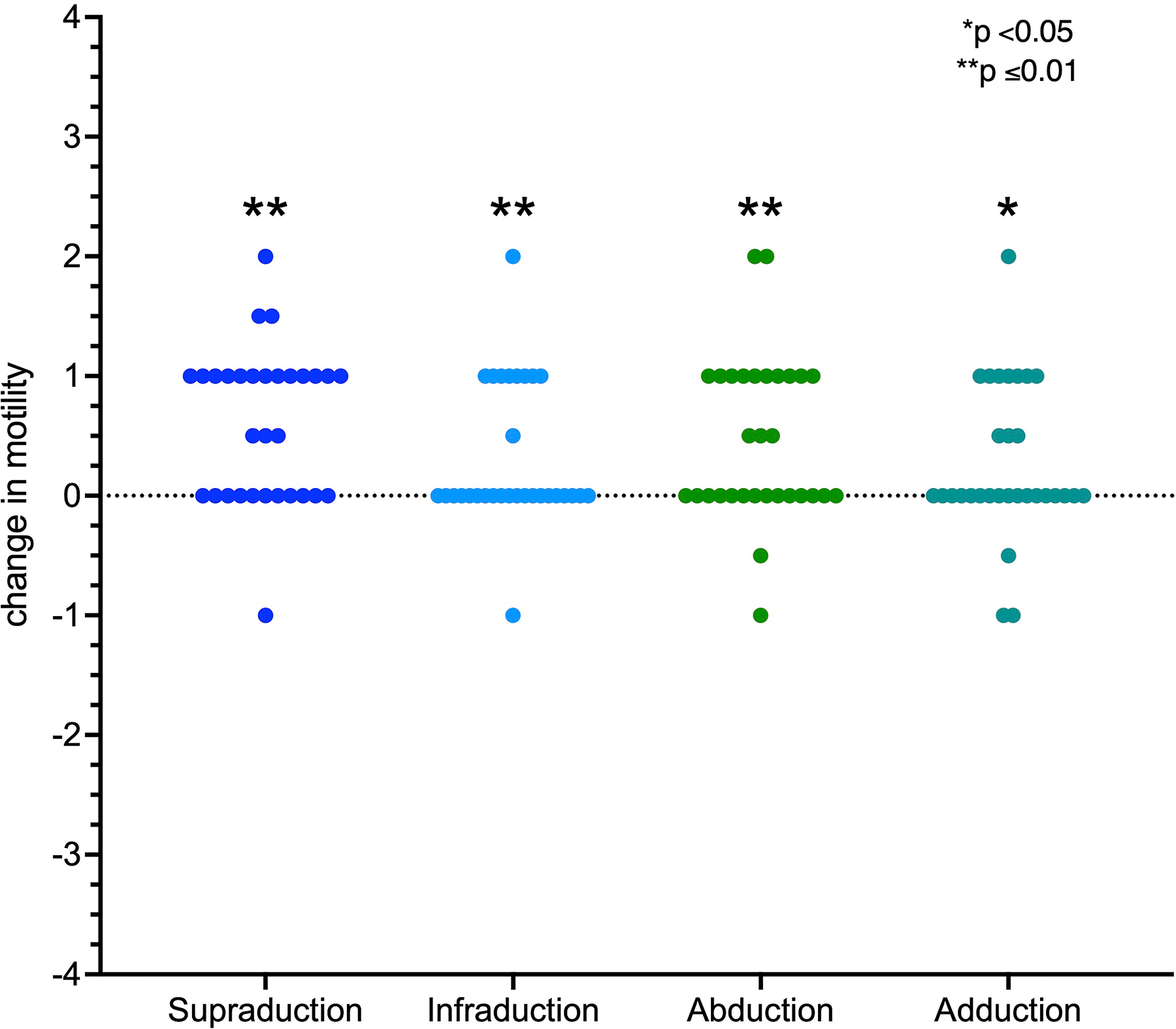
Changes in ductions (post versus pre teprotumumab) in the more affected eye (N=31).
Of the 31 patients with TED-related strabismus, 11 (35%) underwent strabismus surgery following completion of treatment with teprotumumab. Mean time to strabismus surgery from last infusion was 10 ± 7 months. In the patients who underwent strabismus surgery, mean change in vertical deviation during the interval between teprotumumab completion and strabismus surgery was +1 ± 4 PD, and the mean change horizontal deviation was +2 ± 5 PD. Four patients who underwent a post-teprotumumab orbital decompression were excluded from this analysis.
Discussion
Strabismus surgery in TED is commonly reserved for patients in the quiescent phase of disease who demonstrate stability in the angle of deviation for at least 6 months.8,18–21 Surgery is mostly effective in reducing strabismus, however, due to the variable inflammation and fibrosis of involved muscles, reoperation rates can be high with reports of between 17% and 45%.8, 22–25 Teprotumumab has been shown in clinical trials and post-approval studies to have a positive effect on diplopia, however little evidence exists to its effect on alignment in primary position.
The present investigation demonstrated that teprotumumab was associated with a significant reduction in vertical deviations of approximately 6 prism diopters or 39%. Horizontal deviations were not reliably affected. Of all patients presenting with primary position strabismus, approximately 10% (n=3) experienced complete resolution to orthophoria. These were all small angle (5–10 PD) vertical deviations. After therapy, 35% of the patients in this study underwent strabismus surgery.
This modest effect on TED-related primary position strabismus appears to be somewhat discordant with previously reported data on diplopia. Both the phase III OPTIC trial and several post-approval studies have utilized the Bahn-Gorman diplopia scale as a surrogate for teprotumumab’s effect on TED-related strabismus.9 12, 13 This approach is problematic because it is a non-linear symptom-based scale, in that the degree of disability is significantly greater for patients with the highest score (diplopia in primary position) than any other level. For example, the patient experience of change in diplopia from primary position to gaze evoked diplopia only is likely more dramatic than from intermittent diplopia to none. This distinction is not consistently made in the Bahn-Gorman scale data reported; thus it is not possible to discern how much of the diplopia improvement represented diplopia in primary position. Additionally, this scale is uninformative regarding the type and degree of deviation responsive to IGF-1R inhibition.
These strabismus findings are further somewhat incongruous with findings from this study and others suggesting a consistently positive effect of teprotumumab on motility. For instance, improvement in ductions was first reported by Diniz et al. and later corroborated by two additional groups. 14 Ugradar et al added that the greatest improvement is in sursumversion.15 Reshef et al. further described clinic-radiologic correlations, reporting a reduction in composite motility restriction and total EOM cross sectional area.26 Little information on strabismus was offered in either of the latter two studies. Interestingly, a similar pattern of significant improvement in supraduction in TED patients treated with orbital radiation has been previously reported. 27 These studies taken together tend to support the contention that the more commonly involved muscles (inferior and medial rectus) tend to experience consistent size reduction and motility improvement, though they do not offer significant insight into the motility – strabismus relationship.
The dissociation between improvement in motility without similarly consistent improvements in strabismus is curious, yet consistent with previous reports.14, 15, 26 It is not completely clear how these results can be reconciled. It is possible that the improvements in motility may occur without altering the relative size and strength imbalance between agonists and antagonist EOMs so that strabismus persists. Perhaps there is an element of central processing that is unforgiving to biomechanically modified extraocular muscles or that the muscles recover some aspect of their elasticity yet remain abnormally active. Further investigation is warranted in this area.
Of note, this study has several limitations. It was retrospective and non-comparative. The findings were additionally not correlated with radiological changes in extraocular muscle cross-sectional area or volume as has been previously reported. 28–30 This investigation also did not examine teprotumumab’s effect on secondary gaze incomitance, forced ductions, or spring back testing and concurrent effect on proptosis. Lastly, this study examined a heterogenous, though predominantly active TED patient population.
The key findings of this study have several potential implications for treatment of TED-related strabismus. Overall, the effect of teprotumumab on primary position strabismus is small but significant. Patients with predominantly vertical strabismus are more likely to experience reduction in strabismus angle with teprotumumab, and approximately 10% of those with small angle deviations may even experience resolution. Horizontal deviations are less likely to change. Similarly, teprotumumab treatment appears to have a modest, consistent, and positive effect on motility. Given these findings, strabismus surgery is likely to remain an important part of the rehabilitation pathway for patients affected by TED-related strabismus.
Acknowledgements:
Ashley Shirriff, BS – data collection, Jason Zhou, BS – statistics support
Financial Support:
Research reported in this publication is supported by the National Center for Advancing Translational Science (NCATS) of the National Institutes of Health under the UCLA Clinical and Translational Science Institute grant number UL1TR001881, and an unrestricted grant to the Departments of Ophthalmology from Research to Prevent Blindness (New York, NY).
Footnotes
Proprietary interest statement:
Shira L. Robbins – royalties, Elsevier Publishing
Bobby S. Korn – consultant, Horizon Therapeutics; royalties, Elsevier Publishing
Daniel B Rootman – consultant, Horizon Therapeutics
Don O. Kikkawa – consultant, Horizon Therapeutics; consultant, Immunovant; royalties, Elsevier Publishing
Meeting presentation: Preliminary results were presented as an oral presentation at the American Society of Ophthalmic Plastic and Reconstructive Surgery fall scientific symposium in September 2022.
References
- 1.Bahn RS, Heufelder AE. Pathogenesis of Graves’ ophthalmopathy. N Engl J Med 1993;329 (20):1468–1475. [DOI] [PubMed] [Google Scholar]
- 2.Yoon JS, Kikkawa DO. Thyroid eye disease: From pathogenesis to targeted therapies. Taiwan J Ophthalmol 2022;12(1):3–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Douglas RS, Gupta S. The pathophysiology of thyroid eye disease: implications for immunotherapy. Curr Opin Ophthalmol 2011;22:385–390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Garrity JA, Bahn RS. Pathogenesis of graves ophthalmopathy: implications for prediction, prevention, and treatment. Am J Ophthalmol 2006;142:147–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bartley GB. The epidemiologic characteristics and clinical course of ophthalmopathy associated with autoimmune thyroid disease in Olmsted County, Minnesota. Trans Am Ophthalmol Soc 1994;92:477–588. [PMC free article] [PubMed] [Google Scholar]
- 6.Jellema HM, Merckel-Timmer E, Kloos R, et al. Quality of life improves after strabismus surgery in patients with Graves’ orbitopathy. Eur J Endocrinol 2014;170(5):785–9 [DOI] [PubMed] [Google Scholar]
- 7.Granet DB, Hodgson N, Godfrey KJ, et al. Chemodenervation of extraocular muscles with botulinum toxin in thyroid eye disease. Graefes Arch Clin Exp Ophthalmol 2016;254:999–1003. [DOI] [PubMed] [Google Scholar]
- 8.Akbari MR, Mirmohammadsadeghi A, Mahmoudzadeh R, Veisi A. Management of Thyroid Eye Disease-Related Strabismus. J Curr Ophthalmol 2020. Mar 23;32(1):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med 2020;382 (4):341–352. [DOI] [PubMed] [Google Scholar]
- 10.Ozzello DJ, Kikkawa DO, Korn BS. Early experience with teprotumumab for chronic thyroid eye disease. Am J Ophthalmol Case Rep 2020;19:100744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ozzello DJ, Dallalzadeh LO, Liu CY. Teprotumumab for chronic thyroid eye disease. Orbit 2022;41:539–546. [DOI] [PubMed] [Google Scholar]
- 12.Douglas RS, Kahaly GJ, Ugradar S, et al. Teprotumumab Efficacy, Safety, and Durability in Longer-Duration Thyroid Eye Disease and Re-treatment: OPTIC-X Study. Ophthalmology 2022;129(4):438–449. [DOI] [PubMed] [Google Scholar]
- 13.Ho TC, Maamari RN, Kossler AL, et al. Outcomes of Patients With Thyroid Eye Disease Partially Treated With Teprotumumab. Ophthalmic Plast Reconstr Surg 2023. Mar-Apr 01;39(2):150–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Diniz SB, Cohen LM, Roelofs KA, et al. Early experience with the clinical use of teprotumumab in a heterogenous thyroid eye disease population. Ophthalmic Plast Reconstr Surg 2021;37:583–591. [DOI] [PubMed] [Google Scholar]
- 15.Ugradar S, Kang J, Kossler AL, et al. Teprotumumab for the treatment of chronic thyroid eye disease. Eye 2022;36(8):1553–1559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bates D, Maechler M, Bolker B, Walker S. Fitting Linear Mixed-Effects Models Using lme4. Journal of Statistical Software 2015; 67(1): 1–48. [Google Scholar]
- 17.Kuznetsova A, Brockhoff PB, Christensen RHB. lmerTest Package: Tests in Linear Mixed Effects Models. Journal of Statistical Software 2017; 82(13): 1–26. [Google Scholar]
- 18.Nardi M Squint surgery in TED – Hints and fints, or why Graves’ patients are difficult patients. Orbit 2009;28:245–50. [DOI] [PubMed] [Google Scholar]
- 19.Long JC. Surgical management of tropias of thyroid exophthalmos. Arch Ophthalmol 1966;75:634–8. [DOI] [PubMed] [Google Scholar]
- 20.Lee YH, Oh SY, Hwang JM. Is 6 months of stable angle of strabismus enough to perform surgery in patients with strabismus related to thyroid ophthalmopathy? Br J Ophthalmol 2010;94:955–6. [DOI] [PubMed] [Google Scholar]
- 21.Jellema HM, Saeed P, Mombaerts I, et al. Objective and subjective outcomes of strabismus surgery in Graves’ orbitopathy: A prospective multicentre study. Acta Ophthalmol 2017;95:386–91. [DOI] [PubMed] [Google Scholar]
- 22.Rajendram R, Bunce C, Adams GG, et al. Smoking and strabismus surgery in patients with thyroid eye disease. Ophthalmology 2011;118:2493–7. [DOI] [PubMed] [Google Scholar]
- 23.Flanders M, Hastings M. Diagnosis and surgical management of strabismus associated with thyroid-related orbitopathy. J Pediatr Ophthalmol Strabismus 1997;34:333–40. [DOI] [PubMed] [Google Scholar]
- 24.Volpe NJ, Mirza-George N, Binenbaum G. Surgical management of vertical ocular misalignment in thyroid eye disease using an adjustable suture technique. J Pediatr Ophthalmol Strabismus 2012;16:518–22. [DOI] [PubMed] [Google Scholar]
- 25.Yan J, Zhang H. The surgical management of strabismus with large angle in patients with Graves’ ophthalmopathy. Int Ophthalmol 2008;28:75–82. [DOI] [PubMed] [Google Scholar]
- 26.Reshef ER, Marsiglia M, Bouhadjer K, et al. Reduction in Extraocular Muscle Cross-sectional Area and Correlation with Extraocular Motility and Diplopia Following Teprotumumab for Thyroid Eye Disease. Ophthalmic Plast Reconstr Surg 2023:e002337. [DOI] [PubMed] [Google Scholar]
- 27.Mourits MP, van Kempen-Harteveld ML, García MB, et al. Radiotherapy for Graves’ orbitopathy: randomised placebo-controlled study. Lancet 2000;355(9214):1505–9. [DOI] [PubMed] [Google Scholar]
- 28.Jain AP, Gellada N, Ugradar S, et al. Teprotumumab reduces extraocular muscle and orbital fat volume in thyroid eye disease. Br J Ophthalmol 2022;106:165–171. [DOI] [PubMed] [Google Scholar]
- 29.Tran C, Pham CM, Simmons BA, et al. Echographic assessment of extraocular muscle response to teprotumumab. Ophthalmic Plast Reconstr Surg 2022;38:336–339. [DOI] [PubMed] [Google Scholar]
- 30.Nugent RA, Belkin RI, Neigel JM, et al. Graves orbitopathy: correlation of CT and clinical findings. Radiology 1990;177:675–682 [DOI] [PubMed] [Google Scholar]