

Abstract
Erectile Dysfunction (ED) is the leading cause of sexual dysfunction affecting hundreds of millions of men worldwide, and has been described as an important public health problem. The association of five novel anthropometrics related to obesity, lipids and glucose with ED remains unclear. To investigate the association of lipid accumulation products index (LAP), triglyceride glucose index (TyG), waist triglyceride index (WTI), weight-adjusted-waist index (WWI) and a body shape index (ABSI) with ED. Cross-sectional data from the NHANES were used. Participants were adults aged 20–85 y from 2001 to 2004. The analysis of logistic regressions, smooth curve fitting, subgroup analyses and generalized addition model were performed to examine the relationship between five novel anthropometric indicators and the prevalence of ED. An overall 1413 adult men were included in the study. After adjusting for confounding factors, the results of multiple regression analysis showed, ED positively correlated with LAP(OR = 1.0031, P < 0.05), TyG(OR = 1.2981, P < 0.05), WTI(OR = 1.4220, P < 0.05), WWI(OR = 1.6043, P < 0.001), and ABSI(OR = 1.6211, P < 0.05). Smoothed curve fitting and subgroup analyses proved the stability of the relationship. This cross-sectional study showed a positive correlation between these five novel anthropometric indicators (LAP, TyG, WTI, WWI, ABSI) and ED. Further studies are needed to explore their association better and the underlying mechanisms.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-024-80878-1.
Keywords: Erectile dysfunction, Anthropometric indice, Lipid accumulation products index (LAP), Triglyceride glucose index (TyG), Waist triglyceride index (WTI), Weight-adjusted-waist i ndex (WWI), A body shape index (ABSI), NHANES.
ndex (WWI), A body shape index (ABSI), NHANES.
Subject terms: Sexual dysfunction, Erectile dysfunction
Introduction
Erectile dysfunction (ED), defined as the inability to achieve or maintain an erection sufficient for satisfactory sexual intercourse1, is a common condition predominantly affecting men over the age of 402. It is estimated that more than 30% of men between the ages of 40 and 70 suffer from ED3,4, and the incidence of erectile dysfunction in men under the age of 40 is also on the rise5. ED is the leading cause of sexual dysfunction affecting hundreds of millions of men worldwide, and has been described as an important public health problem. The prevalence of ED, closely linked to age, health status, and emotional well-being6.
The current therapeutic landscape for ED includes a variety of treatments such as transrectal thermotherapy (TRT), PDE5 inhibitors, intracorporeal injections, vacuum constriction devices (VCDs), intraurethral prostaglandin suppositories, and surgically implanted prosthetic devices7. Despite the availability of these oral and surgical interventions, the efficacy in restoring erectile function often falls short of natural recovery. Therefore, identifying risk factors for ED, including metabolic abnormalities, obesity, cardiovascular disease, sedentary lifestyle, and chronic alcohol consumption, is imperative for its prevention8,9. Given the rising prevalence of ED, particularly among younger men, its prevention should be a public health priority.
Obesity is a key risk factor associated with a myriad of common diseases such as hypertension, diabetes, cardiovascular diseases, cancer, psychiatric disorders, and impaired sexual function10,11. Body mass index (BMI) is the standard metric for assessing obesity. However, BMI has limitations in evaluating body fat distribution and metabolic health, as it does not differentiate between muscle and fat mass and fails to accurately reflect central obesity risks12. Consequently, several novel metrics have been proposed as more reliable indicators for assessing obesity. These include the lipid accumulation product (LAP), the triglyceride and glucose index (TyG), the waist triglyceride index (WTI), the waist weight corrected index (WWI), and the body shape index (ABSI). LAP, combining blood lipid data with waist circumference measurements, is thought to more accurately represent the risk of central obesity and metabolic syndrome13. TyG, a non-invasive marker, assesses insulin resistance by considering triglyceride levels and fasting glucose levels14. WTI15and WWI16 specifically focus on waist circumference relative to triglyceride levels and body weight, emphasizing the significance of central obesity in metabolic health. ABSI17 offers a novel perspective on body shape and health risks by correlating waist circumference with height and weight.
Emerging evidence suggests a strong association between obesity and an increased likelihood of ED. Studies by Filo et a.l18 and Zhang et al.19. have demonstrated that men over 40 with abdominal obesity and those with a BMI ≥ 30 kg/m², respectively, show a heightened prevalence of ED. Two other studies have shown that weight loss can improve erectile dysfunction20,21. Additionally, prior research has established a link between ED and indicators such as TyG22, WWI23, and ABSI24. The primary objective of the current study is to investigate the association of LAP and WTI with ED, in addition to previously studied metrics, to investigate the association of five novel anthropometric indices with ED.
Materials and methods
Study population
The NHANES was a survey conducted by the US Centers for Disease Control and Prevention (CDC) to monitor the health and nutrition statuses of the adults and children in the US. The survey was approved by the Institutional Review Board of the National Center for Health Statistics (NCHS), and all participants gave informed consent. NHANES used “stratified multistage probability sampling” to obtain a nationally representative sample. The details of survey administration and methods can be accessed on the NHANES website (http://www.cdc.gov/nchs/nhanes.htm, accessed on 18 March 2023).
In our analysis, we utilized NHANES data from two independent waves (2001–2002 and 2003–2004) because questionnaire information regarding ED was available only in those years. And the data related to the five novel anthropometric indices and erectile dysfunction and covariates are all measured at the same time. The study population was limited to those ≥ 20 years of age as the age under 20 years was not interviewed about erectile function. We excluded those participants with a history of prostate cancer because treatment for prostate cancer might be a potential iatrogenic cause of ED. Exclusion criteria were as follows: age<20 years (n = 5347); missing information on ED (n = 838); missing waist circumference(n = 112); missing lipid data (n = 2029); missing blood glucose data (n = 4); missing weight data (n = 2); missing height data (n = 16); missing alcohol intake data (n = 373); missing hypertension data(n = 25); missing smoking status data(n = 1); missing marital status data(n = 2); missing education data (n = 1); missing activity data (n = 27); discrete values for triglycerides (> 2740 mg/dl) (n = 3). Finally, a total of 1413 cases were included in this study, including 284 ED patients and 1129 non-ED controls. As shown in Fig. 1, according to the exclusion criteria, a total of 1413 survey individuals aged from 20 to 85 years were enrolled in our study.
Fig. 1.
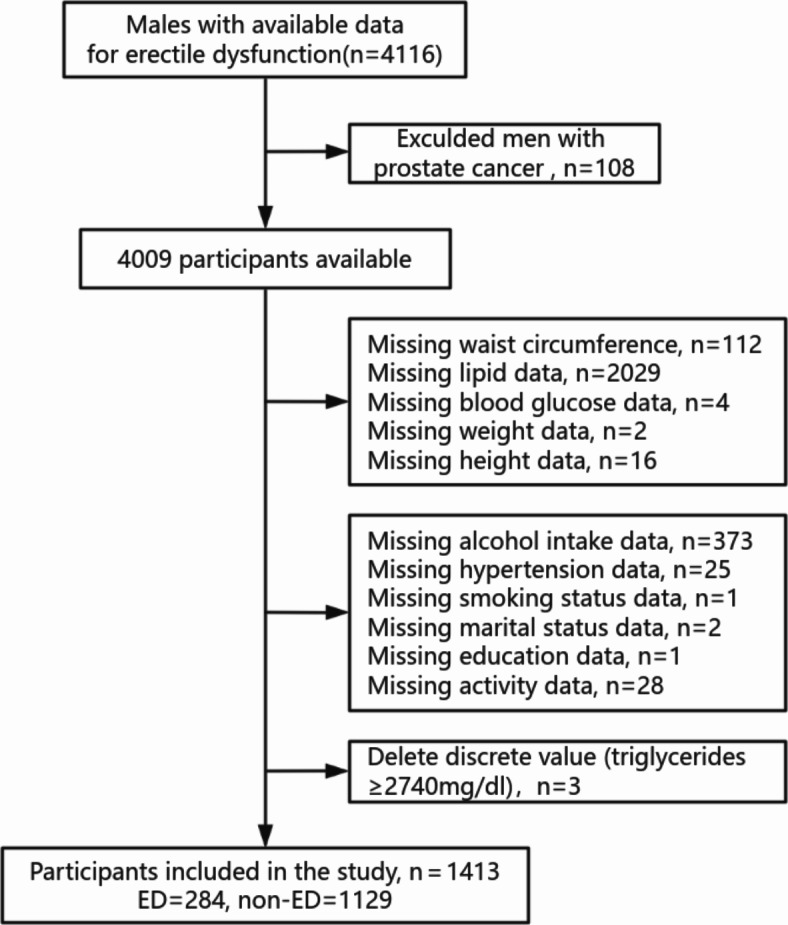
Flowchart of the sample selection from NHANES 2001–2004.
Anthropometric indexes measurement
Each participant had a home interview and finished a physical examination at a mobile examination center (MEC). Participants were required to fast at least 9 h before the health examination25. Height and weight were measured at the MEC by a standardized protocol. BMI was calculated by dividing the weight in kilograms by the square of the height in meters and then rounding to the nearest 1/10 cm. WC was measured by an inelastic ruler with a minimum scale of one millimeter at the end of a normal exhalation, and when standing naturally with legs opened about 25–30 cm apart. Placed the ruler at the midpoint of the connecting line between the upper edge of the top of the iliac crest and the lower edge of the 12th rib (usually the natural narrowest part of the waist) and horizontally circled the abdomen, and then rounded to 0.1 cm26 After at least 5 min of rest at the MEC, using a standardized mercury sphygmomanometer to measure blood pressure in a sitting position27.
LAP, TyG, WTI, WWI and ABSI were calculated by using the following formulas24,28–30:
 |
Erectile dysfunction definition
We assessed erectile function with the following question from the Massachusetts Male Aging Study31,32: “Many men experience problems with sexual intercourse. How would you describe your ability to get and keep an erection adequate for satisfactory intercourse?” Response options were available as “always or almost always able,” “usually able,” “sometimes able” and “never able.” ED was defined as “sometimes able” or “never able” to keep an erection adequate for satisfactory intercourse as previously validated Participants who responded “almost always able” or “usually able” to maintain an erection were defined as not having ED.
Covariates
Based on clinical professional knowledge and previous literature results33,34, covariates including age, race, marital status, education, alcohol consumption status, poverty income ratio, smoking status, history of diabetes, history of hypertension, history of hypercholesterolemia, physical activity, cardiovascular disease, and were selected for analysis.
The results of race were classified as Mexican American, Non-Hispanic White, Non-Hispanic Black, and other races.
Educational attainment was divided into less than high school, high school, and more than high school.
The marital status was divided into cohabitation and solitude. If participants responded that they were “widowed”, “divorced”, “separated”, or “never married”, we categorised the participants as solitude. And those who answered “married” and “living with partner” were classified as cohabitation.
The poverty income ratio (PIR) is an index of the household income to poverty ratio, which reflects social economic status35, and a higher PIR indicated a better family income status. In this study, PIR was stratified as 0–2, 2–4, and ≥ 4 according to the original value36.
Drinking Alcohol intake was divided into 3 categories: no alcohol consumption (< 1 lifetime drink), light alcohol consumption (1 or 2 drinks/day), and heavy alcohol consumption (≥ 3 drinks/day).
In the NHANES, self-reported smoking status can be assessed by the following two survey question: “Have you smoked at least 100 cigarettes in your entire life?” and “Do you now smoke cigarettes every day, some days or not at all?” According to the National Health Interview Survey, smoking status can be categorized into three groups: never smoker (smoked less than 100 cigarettes in the lifetime, or has never smoked), former smoker (smoked at least 100 cigarettes in the lifetime and responded that now do not smoke), current smoker (smoked at least 100 cigarettes in the lifetime and responded that now smoke cigarettes every day or some days37.
The participants underwent multiple blood pressure measurements. A mean of multiple measurements ≥ 140/90 mm/Hg, a previous diagnosis of hypertension, or the prescription of hypertension lowering medication were considered hypertensive.
The participants with a previous diagnosis of diabetes, or Glucose level ≥ 126 mg/dl were considered diabetic.
Cardiovascular disease was defined as self-reported history of one of the following conditions: coronary heart disease, myocardial infarction, congestive heart failure, and stroke.
Physical activity status was evaluated based on responses to questions regarding whether the participants engaged in moderate or vigorous activity during the past 30 days.
Hypercholesterolemia was defined as a total cholesterol level of 240 mg/dL or higher, a prior diagnosis of “high cholesterol,” or self-reported taking a cholesterol-lowering medication38.
Statistical analysis
In the study, according to the official recommendations of the NHANES website and the guidelines provided by the Centers for Disease Control and Prevention (CDC)23,39,40, appropriate weighting methodology were used to account for complex sampling design to provide nationally representative results.
In the baseline characteristics table of the subjects, the participants were categorized into “ED” group and “non-ED” group. Differences between the two groups were tested using the survey-weighted Chi-square test (svytable) or survey-weighted linear regression (svyglm), with categorical data expressed as weighted percentages and non-normal continuous variables expressed as weighted medians (interquartile range, IQR). Logistic regression analyses were used to assess the relationship between anthropometric indicators (LAP, TyG, WTI, WWI, ABSI) and ED prevalence. And three models were constructed to adjust for confounders: crude model 1 was the unadjusted version. Minimally model 2 was adjusted for age, race, education, marital status, PIR. And fully model 3 was adjusted for alcohol intake, smoking status, hypertension, diabetes, hypercholesterolemia, coronary artery disease, vigorous activity, and moderate activity, which were added to Model 2. Based on the results of the above analyses, we further assessed the differences in ED risk between different quartile groups by converting LAP, TyG, WTI, WWI, and ABSI into categorical variables (quartile method).
In the fully adjusted model, smoothed curve fitting and generalized additive models are further used to test whether there is a linear correlation between five novel anthropometric indicators and ED. the subgroup analyses and interaction tests were performed to ensure the robustness of the result. Finally, the association of five novel anthropometric indicators for ED was assessed using receiver operating characteristic (ROC) curves and area under the curve (AUC). All statistical significance was set to P < 0.05. All statistical analyses were conducted using Empower Stats (http://www.empowerstats.com, X&Y Solutions, Inc.) and statistical software packages R (http://www.R-project.org; The R Foundation).
Result
Baseline characteristics of the subjects
The baseline characteristics of the included population and the weighted analysis of the study population characteristics for the total sample are detailed in Table 1. 284 of 1413individuals had a history of ED. The average age of included subjects was 40.81 (39.91 ,41.70) years for the non-ED group and 56.84 (55.06 ,58.62) years for the ED group. Males with ED may be older, less educated, less physical activity, be former smokers, be light drinker, and have diabetes, hypertension, and CVD (all p < 0.05). In addition, all of the anthropometric indexes in the ED group, including LAP, TyG, WTI, WWI, ABSI were significantly increased.
Table 1.
Weighted distributions of characteristics of participants.
| Characteristic | Erectile Dysfunction | P-value | |
|---|---|---|---|
| ED (n = 284) | non-ED (n = 1129) | ||
| Age, mean (95% CI) (years) | 56.84 (55.06 ,58.62) | 40.81 (39.91 ,41.70) | < 0.0001 |
| Race (%) | 0.8333 | ||
| Mexican American | 8.36 (5.55 ,12.39) | 8.24 (6.16 ,10.94) | |
| Non-Hispanic White | 76.76 (67.97 ,83.71) | 74.20 (68.48 ,79.20) | |
| Non-Hispanic Black | 7.66 (4.98 ,11.60) | 9.45 (7.24 ,12.26) | |
| Other | 7.23 (2.84 ,17.19) | 8.10 (5.57 ,11.64) | |
| Education (%) | 0.0087 | ||
| Less than high school | 23.49 (18.25 ,29.70) | 13.95 (12.07 ,16.06) | |
| High school | 25.56 (19.44 ,32.83) | 27.95 (25.12 ,30.97) | |
| More than high school | 50.95 (41.81 ,60.02) | 58.10 (55.35 ,60.80) | |
| Marital status (%) | 0.0542 | ||
| Cohabitation | 75.32 (67.61 ,81.70) | 67.80 (63.58 ,71.75) | |
| Solitude | 24.68 (18.30 ,32.39) | 32.20 (28.25 ,36.42) | |
| PIR (%) | 0.8649 | ||
| <2 | 26.87 (21.72 ,32.73) | 24.98 (22.08 ,28.13) | |
| 2.0 ≤ PIR < 4.0 | 27.90 (20.52 ,36.71) | 28.63 (24.65 ,32.96) | |
| ≥ 4.0 | 45.23 (36.57 ,54.19) | 46.39 (42.23 ,50.60) | |
| Alcohol intake (%) | 0.0312 | ||
| Nondrinker | 9.38 (5.87 ,14.66) | 7.75 (4.47 ,13.13) | |
| Light drinker | 60.93 (51.89 ,69.28) | 49.51 (44.74 ,54.29) | |
| Heavy drinker | 29.69 (22.07 ,38.63) | 42.74 (39.33 ,46.22) | |
| Smoking status (%) | < 0.0001 | ||
| Nonsmoker | 26.64 (21.26 ,32.82) | 45.17 (41.12 ,49.27) | |
| Former smoker | 46.65 (41.82 ,51.55) | 26.02 (23.10 ,29.18) | |
| Current smoker | 26.70 (21.60 ,32.51) | 28.81 (26.17 ,31.60) | |
| Hypertension (%) | < 0.0001 | ||
| Yes | 46.22 (40.08 ,52.48) | 20.37 (17.52 ,23.55) | |
| No | 53.78 (47.52 ,59.92) | 79.63 (76.45 ,82.48) | |
| Diabetes (%) | < 0.0001 | ||
| Yes | 17.81 (13.04 ,23.83) | 3.46 (2.39 ,4.99) | |
| No | 80.12 (73.75 ,85.26) | 95.66 (93.95 ,96.91) | |
| Borderline | 2.07 (0.64 ,6.52) | 0.87 (0.42 ,1.82) | |
| Hypercholesterolemia (%) | 0.7284 | ||
| Yes | 14.97 (9.29 ,23.22) | 16.06 (13.67 ,18.78) | |
| No | 85.03 (76.78 ,90.71) | 83.94 (81.22 ,86.33) | |
| Coronary Artery Disease (%) | < 0.0001 | ||
| Yes | 18.02 (13.49 ,23.66) | 4.67 (3.39 ,6.39) | |
| No | 81.98 (76.34 ,86.51) | 95.33 (93.61 ,96.61) | |
| Vigorous activity (%) | < 0.0001 | ||
| Yes | 24.91 (18.38 ,32.82) | 43.40 (39.69 ,47.19) | |
| No | 75.09 (67.18 ,81.62) | 56.60 (52.81 ,60.31) | |
| Moderate activity (%) | 0.0129 | ||
| Yes | 50.27 (42.76 ,57.77) | 59.59 (56.09 ,63.01) | |
| No | 49.73 (42.23 ,57.24) | 40.41 (36.99 ,43.91) | |
| LAP | 88.58 (74.78 ,102.38) | 64.85 (60.11 ,69.59) | 0.0021 |
| TyG | 9.06 (8.95 ,9.17) | 8.74 (8.70 ,8.79) | < 0.0001 |
| WTI | 8.99 (8.89 ,9.09) | 8.73 (8.68 ,8.77) | < 0.0001 |
| WWI | 11.12 (11.02 ,11.23) | 10.56 (10.51 ,10.60) | < 0.0001 |
| ABSI | 8.41 (8.34 ,8.47) | 8.09 (8.06 ,8.13) | < 0.0001 |
For continuous variables: survey-weighted mean (95% CI), P-value was by survey-weighted linear regression (svyglm). For categorical variables: survey-weighted percentage (95% CI), P-value was by survey-weighted Chi-square test (svytable). ED erectile dysfunction. PIR Poverty to income ratio. LAP Lipid Accumulation Products Index. TyG Triglyceride Glucose Index. WTI Waist Triglyceride Index. WWI Weight-adjusted-waist Index. ABSI A Body Shape Index.
Association between LAP, TyG, WTI, WWI, ABSI and ED
The association between five novel anthropometric indices and ED is seen in Table 2. We used the multivariable logistic regression to examine the relationship between novel anthropometric indices and ED in crude, minimally adjusted, as well as fully adjusted models, and found a positive connection. And the results were stable in the minimally adjusted model (adjusting for age, race, education, marital status, and PIR) and fully adjusted model (adjusting for Model 2 + alcohol intake, smoking status, hypertension, diabetes, hypercholesterolemia, coronary artery disease, vigorous activity and moderate activity), which was demonstrated in the Table 2. After adjusting for all covariates, we observed a positive association between the prevalence of erectile dysfunction ED and the five novel anthropometric indices. Specifically, for every one-unit increase in the LAP index, the odds of ED increased by 0.31%, with an odds ratio (OR) of 1.0031 (95% confidence interval [CI]: 1.0008 to 1.0054). For the TyG index, a one-unit increase was associated with an OR of 1.2981 (95% CI: 1.0024 to 1.6810), indicating a nearly three-fold increase in the odds of ED. The WTI showed an OR of 1.4220 (95% CI: 1.0826 to 1.8678) for a one-unit increase, suggesting a 42.20% increase in the odds of ED. The WWI had an OR of 1.6043 (95% CI: 1.2190 to 2.1114), indicating a 60.43% increase in the odds of ED for each one-unit increase. Lastly, for the ABSI, an OR of 1.6211 (95% CI: 1.0330 to 2.5440) was found for a one-unit increase, reflecting a 62.11% increase in the odds of ED. Furthermore, we categorized the continuous LAP, TyG, WTI, WWI, and ABSI variables into quartiles to investigate their potential nonlinear relationship with ED. The results demonstrate that this linear relationship is stable, as demonstrated in supplementary Table 1. And we have supplemented the relative risk (RR) values to provide a more comprehensive analysis (supplementary Table 2).
Table 2.
Association between LAP, TyG, WTI, WWI, ABSI (continuous variable) and ED.
| Exposure | Crude model 1 | Minimally adjusted model 2 | Fully adjusted model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P | |
| LAP | 1.0029 (1.0012, 1.0046) | 0.0006 | 1.0033 (1.0014, 1.0053) | 0.0009 | 1.0031 (1.0008, 1.0054) | 0.0090 |
| TyG | 1.6515 (1.3757, 1.9827) | < 0.0001 | 1.4125 (1.1386, 1.7523) | 0.0017 | 1.2981 (1.0024, 1.6810) | 0.0479 |
| WTI | 1.5508 (1.2788, 1.8807) | < 0.0001 | 1.4662 (1.1577, 1.8568) | 0.0015 | 1.4220 (1.0826, 1.8678) | 0.0114 |
| WWI | 3.6221 (2.9251, 4.4852) | < 0.0001 | 1.8468 (1.4236, 2.3959) | < 0.0001 | 1.6043 (1.2190, 2.1114) | 0.0007 |
| ABSI | 7.3231(5.2161, 10.2810) | < 0.0001 | 1.9770 (1.2819, 3.0491) | 0.0020 | 1.6211 (1.0330, 2.5440) | 0.0356 |
Crude Model 1: no -adjusted model.
Minimally adjusted model 2: age, race, education, marital status and PIR were adjusted.
Fully adjusted model 3: Model 2 + alcohol intake, smoking status, hypertension, diabetes, hypercholesterolemia, coronary artery disease, vigorous activity and moderate activity were adjusted.
OR, Odds ratio. Cl, confidence interval.
Additionally, upon full adjustments, we further investigated the relationship between LAP, TyG, WTI, WWI, ABSI, and the risk of ED using smoothed curve fitting, revealing a positive linear relationship, as illustrated in Fig. 2.
Fig. 2.

Smooth curve fitting for (a) Lipid Accumulation Products Index (LAP), (b) Triglyceride Glucose Index (TyG), (c) Waist Triglyceride Index (WTI), (d) Weight-adjusted-waist Index (WWI), (e) A Body Shape Index (ABSI) and ED. The area between the upper and lower blue dotted lines is on behalf of 95% CI. The red dotted line indicates that the positivelinear association between LAP, TyG, WTI, WWI, ABSI and ED are proven by generalized additive model.
Subgroup analyses for ED association with LAP, TyG, WTI, WWI, ABSI quartile
We performed subgroup analyses and interaction tests to ensure the robustness of the relationship between LAP, TyG, WTI, WWI, ABSI, and ED among different age subgroups (Table 3). The results showed that the relationship between the fourth quartile of LAP, TyG, WTI, WWI, ABSI, and ED was nearly consistent among different age subgroups. Compared with the lowest quartile (Q1), the fourth quartile (Q4) of WTI was associated with an increased risk of ED among those with age < 40 year (OR,4.90; 95% CI: 1.39, 17.26), the fourth quartile (Q4) of WWI and ABSI were associated with an increased risk of ED among those with age ≥ 40 year (OR,3.68; 95% CI: 1.79, 7.60;OR,2.63; 95% CI: 1.37, 5.04). Furthermore, the relationship between LAP, TyG, WTI, WWI, ABSI, and ED was not affected by the interaction among different subgroups (P values for interaction > 0.05).
Table 3.
Subgroup analyses for ED association with LAP, TyG, WTI, WWI, ABSI (categorical variable) in two subgroups of < 40, and ≥ 40years.
| Subgroup | Total (N) | ED (N) | LAP quartile | P for interaction | |||
|---|---|---|---|---|---|---|---|
| Q1 (-0.92-24.42) | Q2 (24.51–48.50) | Q3 (48.62–79.25) | Q4 (79.46-706.99) | ||||
| Age, years | 0.8108 | ||||||
| <40 | 571 | 34 | Ref | 1.07 (0.35, 3.30) | 0.95 (0.30, 2.99) | 2.39 (0.81, 7.04) | |
| ≥40 | 842 | 250 | Ref | 1.13 (0.66, 1.94) | 1.04 (0.60, 1.79) | 1.54 (0.90, 2.65) | |
| Subgroup | Total (N) | ED (N) | TYG quartile | P for interaction | |||
| Q1 (7.15–8.32) | Q2 (8.32–8.73) | Q3 (8.74–9.18) | Q4 (9.18–12.12) | ||||
| Age, years | 0.3004 | ||||||
| <40 | 571 | 34 | Ref | 3.33 (1.02, 10.80) | 4.31 (1.28, 14.46) | 3.00 (0.79, 11.39) | |
| ≥40 | 842 | 250 | Ref | 1.40 (0.84, 2.35) | 1.33 (0.79, 2.23) | 0.97 (0.57, 1.66) | |
| Subgroup | Total (N) | ED (N) | WTI quartile | P for interaction | |||
| Q1 (7.09–8.26) | Q2 (8.26–8.72) | Q3 (8.72–9.15) | Q4 (9.15–11.40) | ||||
| Age, years | 0.0933 | ||||||
| <40 | 571 | 34 | Ref | 4.69 (1.46, 15.05) | 2.08 (0.53, 8.12) | 4.90 (1.39, 17.26) | |
| ≥40 | 842 | 250 | Ref | 1.07 (0.64, 1.80) | 1.04 (0.62, 1.75) | 1.37 (0.82, 2.32) | |
| Subgroup | Total (N) | ED (N) | WWI quartile | P for interaction | |||
| Q1 (8.54–10.20) | Q2 (10.20-10.74) | Q3 (10.75–11.22) | Q4 (11.22–12.85) | ||||
| Age, years | 0.9966 | ||||||
| <40 | 571 | 34 | Ref | 1.08 (0.38, 3.07) | 1.80 (0.59, 5.54) | 3.28 (0.98, 11.00) | |
| ≥40 | 842 | 250 | Ref | 1.21 (0.56, 2.60) | 1.84 (0.89, 3.78) | 3.68 (1.79, 7.60) | |
| Subgroup | Total (N) | ED (N) | ABSI quartile | P for interaction | |||
| Q1 (6.82–7.87) | Q2 (7.87–8.16) | Q3 (8.16–8.47) | Q4 (8.48–9.68) | ||||
| Age, years | 0.2967 | ||||||
| <40 | 571 | 34 | Ref | 1.63 (0.63, 4.24) | 1.47 (0.51, 4.20) | 1.21 (0.22, 6.77) | |
| ≥40 | 842 | 250 | Ref | 0.84 (0.41, 1.73) | 1.52 (0.79, 2.94) | 2.63 (1.37, 5.04) | |
The model was adjusted for race, education, marital status, PIR, alcohol intake, smoking status, hypertension, diabetes, hypercholesterolemia, coronary artery disease, vigorous activity and moderate activity were adjusted.
Comparison of AUC values between LAP and other indexes
The ROC analysis was conducted to evaluate the discriminative power of the LAP, TyG, WTI, WWI, ABSI for ED in individuals. The results showed that WWI and ABSI had a stronger ability to identify ED than other anthropometric indexes, the ROC of the WWI was 0.744 (95% CI: 0.718–0.770), with a sensitivity of 0.66 and a specificity of 0.72; meanwhile, the ROC of the ABSI was 0.734 (95% CI: 0.707–0.761), with a sensitivity of 0.824 and a specificity of 0.683, as demonstrated in supplementary Fig. 1 and supplementary Table 2.
Discussion
This is the largest population-based study to examine the relationship between LAP, TyG, WTI, WWI, ABSI, and ED in a nationally representative sample. This original study, to the best of our knowledge, is the first to comprehensively analyze the relationship between these five indicators and ED. The study included 1,413 participants, aged 20–85 years, categorized into 284 individuals with ED and 1,129 without. This finding is consistent with previous data in the literature. Based on a review of 98 meta-analyses41, 20–40% of men aged 30–49 years had ED, 60% of men aged 50–59 years had ED, and up to 80% of men aged 60 years and older had ED. These data suggest that the prevalence of ED increases significantly with age, further supporting the importance of age as a risk factor for ED. In the unadjusted Model 1, the indices LAP, TyG, WTI, WWI, and ABSI demonstrated positive correlations with ED. As the values of these indices increased, so did the risk of ED in adult men. This correlation persisted in the minimally adjusted Model 2 and the fully adjusted Model 3, confirming a positive association between the indices and ED. Previous studies reported that ED primarily affects men over 40, compared to a 5% prevalence among males under 406,42. Consequently, this study stratified the population into two age groups: 20–40 years and over 40 years, for a stratified analysis.According to the age stratification, after adjusting for potential covariates, the positive correlation between these five indicators and ED remained significant, validating the stability of the study’s results. These findings further support the hypothesis that these body size and metabolism-related indicators can provide important clinical and epidemiological information for ED risk assessment.
After adjusting for confounding factors, the results of multiple regression analysis showed, ED positively correlated with WWI(OR = 1.6043, P < 0.001), and ABSI(OR = 1.6211, P < 0.05). Traditional body surface measurement indicators have been pointed out to have certain limitations in evaluating obesity, such as BMI not reflecting fat distribution, while WC and wait-to-hip ratio (WHR) cannot better evaluate individuals with different heights, while WWI and ABSI seem to be better. The results of related studies have shown that WWI is highly predictive of cardiometabolic morbidity and mortality23. The results of a study showed that WWI is effective in predicting the prevalence of ED, and the ROC value of WII for with the diagnosis of ED was 0.745, which is much higher than the predictive value of BMI (ROC value of 0.528) and WC (ROC value of 0.609)23. ABSI adds height as a variable compared to WWI. The ABSI was proposed as a new measure of abdominal obesity in 2012, and the results of the study showed a positive correlation between the values and the accumulation of abdominal adipose tissue24. Lin et al. showed that the diagnostic value of ABSI for ED was higher than the remaining five markers included in the study.
The results of our study showed that WWI and ABSI had a stronger ability to identify ED than LAP, TyG and WTI. The ROC of the WWI was 0.744 (95% CI: 0.718–0.770), with a sensitivity of 0.66 and a specificity of 0.72; meanwhile, the ROC of the ABSI was 0.734 (95% CI: 0.707–0.761), with a sensitivity of 0.824 and a specificity of 0.683.
ABSI showed a ROC value of 0.750, a sensitivity of 0.722 and a specificity of 0.66024. People with high WWI and high ABSI may increase the risk of ED, which may be attributed to central obesity. Central obesity is a risk factor for erectile dysfunction. ABSI is positively correlated with visceral adiposity, as are visceral fat thickness and area estimated by ultrasound43. ABSI can also be used as an indicator of abdominal obesity and insulin resistance in men44. Similarly, correlative evidence suggests that WWI is significantly and positively associated with abdominal fat45. In a cross-sectional descriptive study, a complete urological, medical and hormonal evaluation of 216 men with a mean age of 61 years showed that 74.7% of patients with abdominal obesity (AO) had varying degrees of ED, and 53.0% of patients with AO were diagnosed with metabolic syndrome (MetS)16. Obesity is associated with hormonal changes such as decreased testosterone levels and increased oestrogen levels, which may interfere with the normal process of erection. Thus, people with central obesity may possess higher WWI and ABSI values than those with non-neutral obesity, with a correspondingly higher risk of ED.
The three markers, LAP, TyG and WTI, are mainly associated with lipids and blood glucose, the results of the multiple regression analysis in this study showed that, ED positively correlated with LAP(OR = 1.0031, P < 0.05), TyG(OR = 1.2981, P < 0.05), WTI(OR = 1.4220, P < 0.05). Elevated blood lipids are considered a risk factor for atherosclerosis, which can lead to erectile dysfunction. atherogenic index of plasma is positively associated with the development of ED46. There have been studies confirming that TyG index, which is an indicator of insulin resistance, and atherogenic indices, such as atherogenic index of plasma (AIP), were significantly associated with ED, AIP and the TyG index seem to important in the evaluation of ED47 .Related studies have shown that TyG may provide a broader basis for assessing the relationship between MetS and obesity and lipid-related markers. As a result, TyG-related factors have also recently been suggested as a method of assessing metabolic disorders. TyG provides an excellent criterion for identifying patients with prediabetes/diabetes, while most studies have also shown a significant correlation between TyG and prediabetes/diabetes48,49. Multiple research results had shown that LAP and WTI were highest discriminatory ability for MetS29,50. Previous studies have shown varying degrees of association between erectile dysfunction and many MetS components, including obesity, hypertension, hyperglycaemia, dyslipidaemia, body mass index, elevated cholesterol and HDL cholesterol51. The relationship between LAP and WTI and ED in the US population has been studied for the first time, both are obtained from WC and TG calculations, and they were all positively correlated with ED. Previous studies have shown that LAP can be used as a predictor of diabetes and cardiovascular disease risk52. Our results showed that the ROC of LAP was 0.606 (95% CI: 0.576–0.635) with a sensitivity of 0.585 and a specificity of 0.578.The ROC of the TyG was 0.607 (95% CI: 0.577–0.637), with a sensitivity of 0.629 and a specificity of 0.544. The ROC of the WTI was 0.589 (95% CI: 0.559–0.619), with a sensitivity of 0.625and a specificity of 0.516. There is a positive correlation between the degree of obesity and the prevalence of inflammation, and the inflammatory response is associated with reduced nitric oxide activity, which can lead to endothelial damage and dysfunction, indirectly contributing to ED. In summary, LAP, TyG, WTI, WWI and ABSI were positively correlated with ED, which was of great significance for assessing the risk of ED occurrence.
Our study presents several limitations that warrant consideration. Firstly, due to the cross-sectional design of the NHANES, we are unable to establish a causal relationship between the five novel anthropometric indices and the risk of ED. Secondly, the reliance on self-reported questionnaires introduces the possibility of recall bias, which may impact the accuracy of the data collected. Thirdly, inherent to cross-sectional studies, there remains the possibility of residual and unmeasured confounders that cannot be entirely excluded from our analysis. Consequently, it is imperative to interpret the conclusions of this study with caution, recognizing these limitations in the interpretation of the results.
Conclusion
This cross-sectional study reveals the relationship between these five novel anthropometric indicators and This cross-sectional study showed a positive correlation between these five novel anthropometric indicators (LAP, TyG, WTI, WWI, ABSI) and ED. Further studies are needed to explore their association better and the underlying mechanisms.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Author contributions
N.X., H.Z. and H.X.wrote the main manuscript text; N.X. and H.Z. prepared figures and tables; Q.W., X.X. and Y.C. conducted the data collection and collation;S.W. reviewed and revised the manuscript text. All authors reviewed the manuscript.
Funding
This work was funded by Guangdong Basic and Applied Basic Research Foundation (No. 2022A1515220178), Science and Technology Innovation project of Foshan Science and Technology Bureau (No. 2016AG100531),Guangdong TCM anti-aging Engineering Technology Research Center (No. 2022E040) and Scientific Research Project of Guangdong Provincial Bureau of Traditional Chinese Medicine (No. 20221371). The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Data availability
The datasets used in this study are freely available from the National Health and Nutrition Examination Survey (NHANES) (http://www.cdc.gov/nchs/nhanes.htm).
Declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the National Centre for Health Statistics.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Yafi, F. A. et al. Erectile dysfunction. Nat. Rev. Dis. Primers2, 16003 (2016). [DOI] [PMC free article] [PubMed]
- 2.Shamloul, R. & Ghanem, H. Erectile dysfunction. Lancet381, 153–165 (2013). [DOI] [PubMed] [Google Scholar]
- 3.Laumann, E. O., Paik, A. & Rosen, R. C. Sexual dysfunction in the United StatesPrevalence and Predictors. JAMA281, 537–544 (1999). [DOI] [PubMed]
- 4.Feldman, H. A., Goldstein, I., Hatzichristou, D. G., Krane, R. J. & McKinlay, J. B. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol.151, 54–61 (1994). [DOI] [PubMed] [Google Scholar]
- 5.Nguyen, H. M. T., Gabrielson, A. T. & Hellstrom, W. J. G. Erectile Dysfunction in Young Men—A review of the prevalence and risk factors. Sex. Med. Rev. 5, 508–520 (2017). [DOI] [PubMed]
- 6.Pastuszak, A. W. Current diagnosis and management of Erectile Dysfunction. Curr. Sex. Health Rep.6, 164–176 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mobley, D. F., Khera, M. & Baum, N. Recent advances in the treatment of erectile dysfunction. Postgrad. Med. J. 93, 679–685 (2017). [DOI] [PubMed]
- 8.Kloner, R. A. Erectile dysfunction in the cardiac patient. Curr. Urol. Rep.4, 466–471 (2003). [DOI] [PubMed] [Google Scholar]
- 9.Sasayama, S. et al. Men’s Health Study. Circ. J.67, 656–659 (2003). [DOI] [PubMed] [Google Scholar]
- 10.Larsen, S., Wagner, G. & Heitmann, B. Sexual function and obesity. Int. J. Obes.31, 1189–1198 (2007). [DOI] [PubMed] [Google Scholar]
- 11.De Lorenzo, A. et al. Why primary obesity is a disease? J. Transl. Med.17, 169 (2019). [DOI] [PMC free article] [PubMed]
- 12.Oliveros, E., Somers, V. K., Sochor, O., Goel, K. & Lopez-Jimenez, F. The Concept of Normal Weight obesity. Prog. Cardiovasc. Dis.56, 426–433 (2014). [DOI] [PubMed] [Google Scholar]
- 13.Rico-Martín, S. et al. Effectiveness of body roundness index in predicting metabolic syndrome: A systematic review and meta-analysis. Obesity Rev. 21, e13023 (2020). [DOI] [PubMed]
- 14.Mazidi, M., Kengne, A-P., Katsiki, N., Mikhailidis, D. P. & Banach, M. Lipid accumulation product and triglycerides/glucose index are useful predictors of insulin resistance. J. Diabetes Complicat.32, 266–270 (2018). [DOI] [PubMed] [Google Scholar]
- 15.Liu, P. J., Lou, H. P. & Zhu, Y. N. Sreening for metabolic syndrome using an Integrated continuous index consisting of Waist circumference and triglyceride: A preliminary cross-sectional Study. DMSO 13, 2899–2907 (2020). [DOI] [PMC free article] [PubMed]
- 16.Park, Y. et al. A novel adiposity index as an integrated predictor of cardiometabolic disease morbidity and mortality. Sci. Rep.8, 16753 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Krakauer, N. Y. & Krakauer, J. C. A new body shape index predicts Mortality Hazard independently of body Mass Index. PLoS ONE. 7, e39504 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fillo, J., Levcikova, M., Ondrusova, M., Breza, J. & Labas, P. Importance of different grades of abdominal obesity on Testosterone Level, Erectile Dysfunction, and clinical coincidence. Am. J. Mens Health. 11, 240–245 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhang, X., Yang, B., Li, N. & Li, H. Prevalence and risk factors for Erectile Dysfunction in Chinese Adult males. J. Sex. Med.14, 1201–1208 (2017). [DOI] [PubMed] [Google Scholar]
- 20.Collins, C. E. et al. Improvement in erectile function following weight loss in obese men: The SHED-IT randomized controlled trial. Obesity Res. Clin. Practice7, e450–e454 (2013). [DOI] [PubMed]
- 21.Wing, R. R. et al. Effects of Weight loss intervention on erectile function in older men with type 2 diabetes in the look AHEAD Trial. J. Sex. Med.7, 156–165 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li, L. et al. A higher TyG index is related with a higher prevalence of erectile dysfunction in males between the ages 20–70 in the United States, according to a cross-sectional research. Front. Endocrinol.13, (2022). [DOI] [PMC free article] [PubMed]
- 23.Cao, S. et al. Relationship between weight-adjusted-waist index and erectile dysfunction in the United State: results from NHANES 2001–2004. Front. Endocrinol. 14 (2023). [DOI] [PMC free article] [PubMed]
- 24.Lin, W. & Lin, M. E. Novel anthropometric measures are positively associated with erectile dysfunction: A cross-sectional study. Int. Urol. Nephrol.10.1007/s11255-023-03840-6 (2023). [DOI] [PubMed] [Google Scholar]
- 25.Curtin, L. et al. (ed, R.) The National Health and Nutrition Examination Survey: Sample design, 1999–2006. Vital Health Stat. 2155 1–39 (2012). [PubMed] [Google Scholar]
- 26.Bawadi, H., Abouwatfa, M., Alsaeed, S., Kerkadi, A. & Shi, Z. Body shape index is a stronger predictor of diabetes. Nutrients, 11(5), 1018. 10.3390/nu11051018 [DOI] [PMC free article] [PubMed]
- 27.Seventh Report of the Joint National Committee on the Prevention. Detection, evaluation, and treatment of high blood pressure (JNC7). (2003). [DOI] [PubMed]
- 28.Ke, B., Sun, Y., Dai, X., Gui, Y. & Chen, S. Relationship between weight-adjusted waist circumference index and prevalence of gallstones in U.S. adults: A study based on the NHANES 2017–2020. Front. Endocrinol. 14 (2023). [DOI] [PMC free article] [PubMed]
- 29.Li, Y. et al. Association between four anthropometric indexes and metabolic syndrome in US adults. Front. Endocrinol. 13, (2022). [DOI] [PMC free article] [PubMed]
- 30.Li, H. et al. The triglyceride glucose index was U-shape associated with all-cause mortality in population with cardiovascular diseases. Diabetol Metab. Syndr. 15, 181 (2023). [DOI] [PMC free article] [PubMed]
- 31.Cole, S. R., Chu, H., Nie, L. & Schisterman, E. F. Estimating the odds ratio when exposure has a limit of detection. Int. J. Epidemiol. 38, 1674–1680 (2009). [DOI] [PMC free article] [PubMed]
- 32.O’Donnell, A. B., Araujo, A. B., Goldstein, I. & McKinlay, J. B. The validity of a single-question self-report of erectile dysfunction. J Gen. Int. Med. 20, 515–519 (2005). [DOI] [PMC free article] [PubMed]
- 33.Zhou, H. et al. The association of various physical activities with erectile dysfunction: NHANES 2001–2004. Sex. Med. 11, qfad036 (2023). [DOI] [PMC free article] [PubMed]
- 34.Zhong, L., Zhan, X. & Luo, X. Higher systemic immune-inflammation index is associated with increased risk of erectile dysfunction: result from NHANES 2001–2004. Medicine102, e35724 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Office of the Assistant Secretary for Planning and Evaluation. [Cited 2021 Nov 17]. https://aspe.hhs.gov/topics/poverty-economic-mobility/poverty-guidelines
- 36.Ahluwalia, N., Raghavan, R., Zhang, G., Talegawkar, S. A. & Jacques, P. F. Vitamin D status and prevalence of metabolic syndrome by race and hispanic origin in US adults: Findings from the 2007–2014 NHANES. Am. J. Clin. Nutr.116, 1400–1408 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Liu, C., Gao, Y., Ji, J., Sun, C. & Chen, M. Association between inflammatory indexes and erectile dysfunction in U.S. adults: National Health and Nutrition Examination Survey 2001–2004. Sex. Med. 11(4), (2023). 10.1093/sexmed/qfad045 (2023). [DOI] [PMC free article] [PubMed]
- 38.Wang, W. et al. The Association between 2, 4-Dichlorophenoxyacetic Acid and Erectile Dysfunction. Front. Public Health10, (2022). [DOI] [PMC free article] [PubMed]
- 39.Sun, H., Huang, J., Tang, H. & Wei, B. Association between weight-adjusted-waist index and urge urinary incontinence: A cross-sectional study from NHANES 2013 to 2018. Sci. Rep.14, 478 (2024). [DOI] [PMC free article] [PubMed]
- 40.Huang, L., Liu, H., Li, L., Wang, S. & Sun, G. Correlation between visceral fat metabolism score and erectile dysfunction: A cross-sectional study from NHANES 2001–2004. Front. Endocrinol.14 (2023). [DOI] [PMC free article] [PubMed]
- 41.Allen, M. S. & Walter, E. Erectile dysfunction: An umbrella review of meta-analyses of risk-factors, treatment, and prevalence outcomes. J. Sex. Med.16 (4), 531–541 (2009). [DOI] [PubMed] [Google Scholar]
- 42.Wang, W. et al. Research advances in stem cell therapy for erectile dysfunction. BioDrugs38, 353–367 (2024). [DOI] [PMC free article] [PubMed]
- 43.Bouchi, R. et al. Indirect measure of visceral adiposity ‘A body shape index’ (ABSI) is associated with arterial stiffness in patients with type 2 diabetes. BMJ Open Diabetes Res. Care4, e000188 (2016). [DOI] [PMC free article] [PubMed]
- 44.Inverse relationship between. A body shape index (ABSI) and fat-free mass in women and men: Insights into mechanisms of sarcopenic obesity - Clinical Nutrition. https://www.clinicalnutritionjournal.com/article/S0261-5614(14)00092-2/fulltext [DOI] [PubMed]
- 45.Kim, N. H., Park, Y., Kim, N. H. & Kim, S. G. Weight-adjusted waist index reflects fat and muscle mass in the opposite direction in older adults. Age Ageing50, 780–786 (2021). [DOI] [PubMed]
- 46.Guo, L., Nan, Y. & Yao, L. Association between atherogenic indexes and erectile dysfunction: A cross-sectional analysis of the National Health and Nutrition Examination Survey 2001–2004. Int. Urol. Nephrol. 56, 2877–2885 (2024). [DOI] [PubMed]
- 47.Sambel, M. et al. Can atherogenic indices and the triglyceride-glucose index be used to predict erectile dysfunction? Sex. Med.11, qfad069 (2023). [DOI] [PMC free article] [PubMed]
- 48.Ahn, N. et al. Visceral adiposity index (VAI), lipid accumulation product (LAP), and product of triglycerides and glucose (TyG) to discriminate prediabetes and diabetes. Sci. Rep.9, 9693 (2019). [DOI] [PMC free article] [PubMed]
- 49.Alves, L. F., Cruz, J. O., Souza, C. & de Oliveira, C. C. A. L., Performance of adiposity indicators in predicting metabolic syndrome in older adults. Arch. Endocrinol. Metabol. 65(5), 588–595 (2021). [DOI] [PMC free article] [PubMed]
- 50.Alfawaz, H. A. et al. Sex-specific cut-offs of seven adiposity indicators and their performance in Predicting metabolic syndrome in arab adults. J. Clin. Med. 12, 7280 (2023). [DOI] [PMC free article] [PubMed]
- 51.Raheem, O. A., Su, J. J., Wilson, J. R. & Hsieh, T. C. The association of erectile dysfunction and cardiovascular disease: A systematic critical review. Am. J Men’s Health, 11(3), 552–563 (2017). [DOI] [PMC free article] [PubMed]
- 52.Kahn, H. S. The ‘lipid accumulation product’ performs better than the body mass index for recognizing cardiovascular risk: A population-based comparison. BMC Cardiovasc. Disorders5, 26 (2005). [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets used in this study are freely available from the National Health and Nutrition Examination Survey (NHANES) (http://www.cdc.gov/nchs/nhanes.htm).