

Abstract
Background:
Athletes with decreased baseline neurocognitive function may experience noncontact anterior cruciate ligament (ACL) injury in unanticipated athletic situations. Many ACL injury prevention programs (IPPs) focus on improving closed-skill movements (eg, planned landing). However, the more open-skill movements (eg, unplanned reactive movements) required in unpredictable sports scenarios are commonly absent from ACL IPPs, and the acute effects of open-skill training on neurocognitive function remain unclear.
Purpose:
To investigate the acute effects of unplanned versus planned training on neurocognitive function and knee biomechanics associated with ACL injury risk during the side-step cutting motion.
Study Design:
Controlled laboratory study.
Methods:
A total of 32 adult recreational athletes (16 female, 16 male) were randomly assigned to either an unplanned training (UT) group or a control (CON) group. The UT group performed unplanned hop-landing training while the CON group performed planned hop-landing training. Both before and after the training, neurocognitive function was evaluated using the Trail Making Test–part B and Stroop Color and Word Test. Additionally, unanticipated and anticipated side-step cutting tasks were performed while 3-dimensional kinematic and kinetic data for the dominant leg were collected. Neurocognitive test scores and biomechanical variables relevant to ACL injury were analyzed using 2-way repeated-measures analysis of variance to determine the main effects of training, group, and training × group interaction.
Results:
Trail Making Test–part B and Stroop Color and Word Test scores significantly improved from pre- to posttraining in both groups (P < .001 for both). There was a significant training × group interaction for peak knee abduction angle during the unanticipated side-step cutting task (pre- vs posttraining: –8.81°± 7.23° vs −7.40°± 7.24° [UT group]; –8.23°± 9.40° vs −9.99°± 9.83° [CON group]; P = .02) and for peak vertical ground-reaction force during the anticipated side-step cutting task (pre- vs posttraining: 3.86 ± 0.59 vs 4.08 ± 0.74 percentage body weight [%BW] [UT group]; 3.70 ± 0.62 vs 3.34 ± 0.62 %BW [CON group]; P = .04).
Conclusion:
Study findings showed a significant training × group interaction for knee abduction angle during the unanticipated side-step cutting task with unplanned training and for vertical ground-reaction force during the anticipated side-step cutting task with planned training.
Clinical Relevance:
Designing ACL IPPs based on the sport type (ie, open skill or closed skill) may contribute to better preparation.
Keywords: ACL, injury prevention, biomechanics, neurocognitive functioning, open skill
Anterior cruciate ligament (ACL) injury is one of the most severe and complex knee injuries during sports and physical activity. This injury can lead to prolonged rehabilitation, 14 high medical costs, 18 high reinjury rates, 60 and an increased risk of osteoarthritis. 2 Therefore, preventing ACL injuries may dramatically improve the long-term health and quality of life of athletes.
Many ACL injury prevention programs (IPPs) have been developed and shown efficacy in reducing the incidence of ACL injury.35,50 However, ACL injury incidence rates continue to rise in some sports (eg, soccer, basketball). 1 Several factors such as motivation, time requirements, and compliance were identified as barriers to the implementation of ACL IPPs. 10 Therefore, the development of more ecologically valid and time-efficient training would be required to promote the more widespread use of ACL IPPs.
Open skills include active decision making and reactions in a dynamic and unpredictable environment (eg, basketball, soccer), while closed skills are movements that follow set patterns in a predictable and relatively unchanging environment (eg, running, cycling). 32 In open-skill sports, where ACL injuries most frequently occur,16,24,46 athletes are required to perform higher-level neurocognitive processes and multitask under unanticipated situations.9,40,49 Indeed, several studies have reported the potential relationship between neurocognitive function and ACL injury risk.27,31,34,57 Swanik et al 57 found that athletes with noncontact ACL injuries demonstrated significantly lower neurocognitive performance compared with controls. Herman and Barth 34 reported that athletes with lower baseline neurocognitive performance demonstrated higher biomechanical risk for ACL injury during an unanticipated drop vertical jump. Grooms et al 31 assessed changes in biomechanics and neural mechanisms during sport-specific landing before and after a 6-week neuromuscular training program; functional magnetic resonance imaging data suggested that changes in brain activity may have been related to the adaptation of injury risk–reducing movement mechanics. Therefore, future ACL injury prevention training may need to focus on changes in neurocognitive functions as well as improved lower-limb biomechanics during sport-related movements.
Neurocognitive functions generally include “high-order” and “low-order” abilities.5,22 Executive functions, referring to high-order neurocognitive functions, enable us to plan and execute actions while staying focused, resisting temptation, and addressing novel and unanticipated challenges. 22 Previous studies have found that executive functions can affect high-risk biomechanics associated with ACL injury during unanticipated situations.25,27 Core executive functions are subdivided into working memory, cognitive flexibility, and inhibitory control.22,45 Working memory and cognitive flexibility are crucial for creative thinking and the ability to adapt rapidly and flexibly to altered circumstances. 22 Inhibitory control encompasses the capacity to manage automatic impulses (eg, self-control to resist temptations and acting impulsively) as well as interference control (eg, selective attention and cognitive inhibition). 22 Pen-and-paper or verbal-based neurocognitive tests have been used as practical and simple assessment tools for executive functions.
Current general ACL IPPs focus on improving closed-skill exercises such as landing from a jump in planned environments. 35 Typically, ACL IPPs that contain more open-skill movements demanded in unplanned sports scenarios have not been established. To replicate sports scenarios and to make prevention training more efficient in a limited time frame, it is necessary to incorporate an open-skill structure.26,27 In addition, open-skill exercises (cognitive demands and challenges of complex motor movements) may improve neurocognitive function, specifically executive function, compared with closed-skill exercises. 32 While a systematic review by Gu et al 32 indicated that open-skill (versus closed-skill) exercises offer superior executive function benefits in childhood and later adulthood, evidence regarding young adults remains relatively limited. Investigation of the effects of open-skill training on neurocognitive function and unanticipated athletic movements simultaneously could provide insight into the neuromotor mechanisms underlying the biomechanical changes. Furthermore, even though many sports teams perform ACL IPPs as warm-up exercises to optimize training sessions, 10 the acute effects of open-skill training for ACL injury prevention have not been assessed.
Therefore, there were 2 purposes for this study. First, we investigated the acute effect of unplanned versus planned training on neurocognitive function. It was hypothesized that unplanned training would significantly improve neurocognitive function compared with planned training. Second, we examined the acute effect of unplanned versus planned training on knee biomechanics associated with ACL injury risk (eg, knee flexion and abduction) during unanticipated cutting motions. It was hypothesized that unplanned training would significantly improve knee biomechanics (ie, increased knee flexion and decreased knee abduction) compared with planned training.
Methods
Participants
The study protocol received ethics committee approval from our institution, and informed consent was obtained from all participants. Adult recreational athletes from the University of Essex and the surrounding area were recruited through flyers and university advertisements. Inclusion criteria were (1) age >18 years and (2) participation in jumping/cutting sports (eg, basketball, soccer, volleyball, lacrosse) at least once a week, with ≥1 year of experience in these sports. Exclusion criteria were (1) concussion within the past 6 months, (2) neurocognitive impairment that would inhibit motor learning (eg, impaired processing speed), 6 (3) any disorder of the peripheral sensory system, (4) current injury in the lower back or lower limbs, (5) history of surgery in the lower back or lower limbs, (6) being color-blind, (7) previously having taken the Stroop Color and Word Test (SCWT) or the Trail Making Test–part B (TMT-B), which were used in this study for neurocognitive testing, and/or (8) taking medication that might affect neurocognitive ability (eg, anticholinergic drugs, psychotropics, and opioids 33 ). The study was conducted from October 2022 to March 2023.
An a priori power analysis using G*Power (Version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf) was performed based on a previous study 37 ; the alpha level and beta error were set at .05 and 0.8, respectively. Effect sizes of 0.90 for knee flexion and 0.75 for knee abduction were used to determine the sample sizes. The sample sizes (n = 10 based on knee flexion data and n = 13 based on knee abduction data) were calculated to obtain a statistically significant effect. To allow for potential dropout, a total of 32 healthy and physically active adults were enrolled in this study.
The 32 participants were randomly assigned in a single-blind manner, with a 1:1 allocation ratio stratified by sex, to either the unplanned training (UT) group (n = 16; 8 male/8 female) or a matched control (CON) group (n = 16; 8 male/8 female). Randomization was conducted by an Excel spreadsheet (Microsoft Corp) with random permuted block sizes 1 and 2. Participants were blinded by not being informed as to which group they were allocated.
Study Protocol
All participants wore athletic shorts, sports bra (for women), and athletic shoes they normally wore in sports activities. Participants in the UT group performed unplanned hop-landing training, while participants in the CON group performed planned hop-landing training. Both before and after completing their respective training protocols, each participant completed (1) neurocognitive assessments and (2) the unanticipated and anticipated side-step cutting movements as part of the experimental tasks. All baseline testing and the training intervention were performed during a single day, with the entire experimental protocol requiring approximately 2 hours to complete. The overall study protocol is shown in Figure 1.
Figure 1.
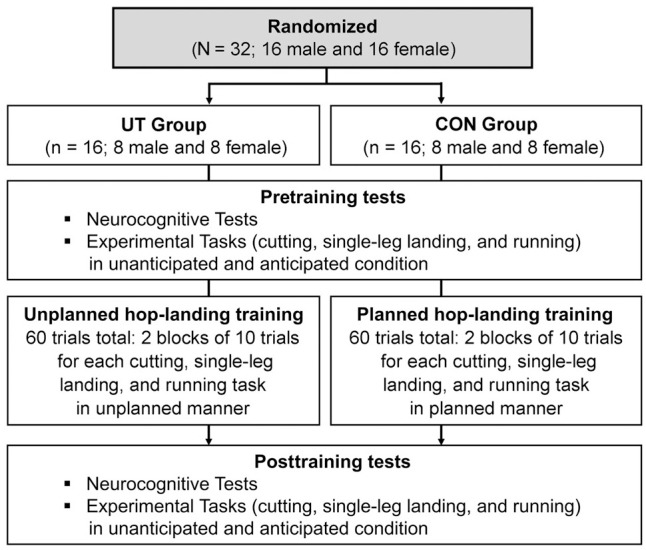
Flowchart of the study protocol. CON, control; UT, unplanned training.
Neurocognitive Testing
Cognitive flexibility, working memory, and inhibitory control were assessed as high-order neurocognitive functions (also referred to as executive functions 22 ). Cognitive flexibility and working memory were tested with the TMT-B 53 using pen and paper. The TMT-B was conducted by linking both disordered numbers (1-13) and letters (A-L) in alternating and ascending order (ie, 1-A-2-B-3-C-4-D, etc), and the score was recorded as the time in seconds required to complete the task. Inhibitory control was tested with the SCWT, 28 which consisted of a list of printed color names that were different from the color in which they were printed. Participants were given 45 seconds to state aloud the ink color rather than the printed word, and the score was recorded as the number of correct responses. A previous meta-analysis 54 revealed that retest effects on cognitive ability were largest from the first to the second test and would have reached a plateau after the third test. Therefore, before the pretraining tests, sufficient explanation was given to each participant and ≥3 practices were conducted until the participant became familiar with the tests.
Experimental Tasks
Before the experimental task, the participants warmed up with a 2-minute jog at a self-selected pace followed by 3 minutes of dynamic quadriceps and hamstring stretching. 59
Three motions were selected as experimental tasks: 45° side-step cutting, single-leg landing, and running forward. For both the unanticipated and the anticipated conditions, the participants hopped down to the center of a force plate from a 30-cm high box using the dominant leg (Figure 2A) and performed 1 of the 3 tasks after receiving a cue via a visual light stimulus (Swift NEO wireless timing system; Swift Performance). The dominant leg was defined as the leg with which the participants preferred to kick a ball, 13 and the box was placed at a distance 50% of their standing height away from the center of the force plate. Three lights were placed at 1-m height from the floor in the directions of the tasks (in front of participants and at 45° to the left and right), 2.5 m away from the center of the force plate.
Figure 2.

A right leg–dominant participant performing the experimental tasks. After hopping off from the (A) start position, the participant performed either the (B) cutting, (C) single-leg landing, or (D) running task upon receiving the visual cue.
The instructions for each experimental task were as follows: (1) for cutting, when a light placed at 45° from the nondominant leg side lit up, the participant performed a side-step cutting movement toward that direction (Figure 2B); (2) for single-leg landing, when none of the lights were lit, the participant performed a single-leg landing on the dominant leg and kept the landing position for 3 seconds (Figure 2C); and (3) for running, when the light placed in front of the box lit up, the participant took a step with the nondominant leg to the front of the force plate and continued to run forward as fast as possible (Figure 2D). We categorized deviations from the provided instructions, such as shifting the initial landing position within the force plate or making contact with the force plate using the free leg or hands, as “errors” and excluded them from the analysis. Each participant performed all of the experimental tasks in both the unanticipated and the anticipated conditions.
Before beginning the experimental tasks, all participants completed up to 5 practice trials for each task under each condition. These practice trials allowed the participants to become familiarized with the tasks, minimizing potential performance changes from pre- to posttraining due to task habituation. The participants were required to perform 3 successful trials for each task.
In the unanticipated condition, the visual light stimulus cued 1 of the 3 tasks randomly via a wireless sensor (Swift NEO wireless timing system) triggered when hopping off from the box. The wireless sensor was placed at both sides of the box's front edge. Each of the 3 tasks was presented almost the same number of times throughout the experiment; randomization was done automatically via the Swift NEO system.
In the anticipated condition, 1 of the 3 visual light stimuli was turned on in advance, then the participants performed the task after they sufficiently recognized the task to be performed. Once 1 of the 3 tasks had been successfully completed 3 times, the other remaining tasks were performed (eg, cutting 3 times, then single-leg landing 3 times, and finally running 3 times). Before the experiment, the order of the 3 tasks in the anticipated condition was randomized for each participant in an Excel (Microsoft Corp) spreadsheet.
Hop-Landing Training Intervention
After the baseline data collection, both groups performed the training intervention. The same movements as in the experimental tasks (detailed in the next section) were performed during the training: 2 blocks of 10 trials for each 45° side-step cutting, single-leg landing, and running task (60 trials total) regardless of success or error. We categorized deviations from the provided instructions as “errors” and excluded them from the analysis. The definition of errors during training was the same as the definition of errors in the experimental tasks, detailed in the next section. Moreover, the number of training errors was recorded to provide a clear depiction of the breakdown in the training process.
In addition, perceived exertion before, during the interval between training blocks, and after the training was assessed using the Borg scale to determine the participants’ perceived exertion. 11 The Borg scale is strongly correlated with heart rate and is considered a practical and valid tool for monitoring training intensity. 55 During the interval between blocks, participants were evaluated using the Borg scale every minute and rested until their Borg rating returned to a level similar to pretraining. Each participant was then allowed a minimum 5-minute interval. By verifying that there was no significant change in the Borg scale, we excluded a confounding factor (participant fatigue) that could affect the neurocognitive function and biomechanics after training. 4
The UT group performed each movement in an unplanned manner (ie, the participants did not know the direction of movement beforehand, and when the light system was triggered, they received the cue), whereas the CON group performed each movement in a planned manner (ie, the participants knew the direction of movement beforehand).
Participants focused on the movement with an external focus of attention, and they were given the following verbal instructions for each task before training and in the interval between blocks: for cutting, “While changing direction, take 1 step toward the gates on the nondominant leg side from the center of the force plate and run through the gates”; for single-leg landing, “Land softly, being gentle as you can when making contact with the ground and hold that position for 3 seconds”; and for running, “Run straight through the gates in front of you immediately after landing.” Neither the UT nor the CON group was provided with any feedback about task performance or outcome.
Marker Placement
For the experimental tasks, 44 retroreflective markers were attached to the trunk and lower extremities of participants according to Kettlety et al 38 (Figure 3). A 3-dimensional motion analysis system (Vicon MX; Vicon) was used to capture the task motions with a 200-Hz sampling rate through 14 infrared cameras. Data regarding ground-reaction forces (GRFs) were obtained at 1000 Hz from a force platform (model 9281C; Kistler Instruments Inc) that was synchronized with the kinematic data. A static calibration trial was collected by having participants stand on a force plate with both feet parallel to the anterior-posterior axis of the laboratory. After the static calibration trial, the calibration markers were removed for the experimental tasks.
Figure 3.
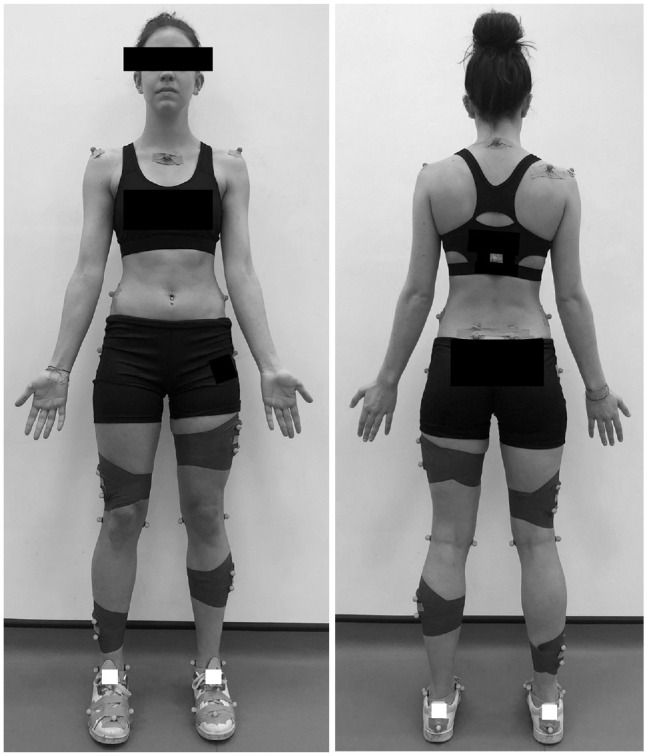
Marker placement for the experimental tasks. Four tracking clusters each with 4 markers (16 markers) were placed bilaterally on the thigh and shank. Additional tracking markers (18 markers) were attached to the manubrium, 7th cervical vertebra, right scapula, 10th thoracic vertebrae, and bilaterally to the following locations: acromion, posterior superior iliac spine, lateral iliac spine, 2nd metatarsophalangeal joint, 5th distal metatarsal, 1st proximal metatarsal, and posterior calcaneus. Ten additional calibration markers were attached bilaterally to the following anatomical landmarks: greater trochanters, lateral and medial knee joint lines, and lateral and medial malleoli.
Based on the static trials, a kinematic model including the trunk, pelvis, and bilateral thigh, shank, and foot segments was created for each participant using Visual 3D software (C-Motion).
Unanticipated and Anticipated Side-Step Cutting Task
In this study, only the cutting task was analyzed for the knee kinematic and kinetic evaluation, as change of direction when running represented the most common mechanism of noncontact ACL injury. 20 The mean of the 3 successful cutting tasks in each of the unanticipated and anticipated conditions was used for all biomechanical analyses. Biomechanical risk factors for noncontact ACL injury have been reported to include a nearly extended knee at initial contact (IC), followed by a combination of high GRFs, knee abduction, and tibial internal rotation.19,39 Therefore, the dependent variables used in this study were knee angles and internal moments, specifically knee flexion at IC, knee abduction and internal rotation at peak stance (PS), and vertical GRF (vGRF) at PS.
Data Processing
Joint angles were calculated within the Visual 3D kinematic model using a Cardan angle (x-y-z), 30 and a standard inverse dynamics analysis was conducted to synthesize the trajectory and vGRF data for internal moment estimation. Joint kinematics and kinetics were smoothed at 15 Hz using a fourth-order Butterworth filter. 41 The dependent variables (ie, knee flexion, knee abduction, knee internal rotation, and vGRF) were calculated at IC and PS. As described in a previous study, 12 IC was defined as the time point when vGRF was higher than 10 N. PS was defined as the time point when the maximum (knee internal rotation and vGRF) or minimum (knee abduction) value of a dependent variable was evident between IC and 50% of stance phase,13,17 as ACL injury tends to occur within this time frame. 29 The data for the cutting tasks were normalized to 100% of the stance phase, which was defined as the time from when the vGRF first exceeded 10 N until it fell below 10 N.13,17 GRF data were normalized to body mass (percentage of body weight [%BW]), and joint moments were normalized to mass × height (N·m/kg).
Statistical Analysis
All statistical analyses were conducted using the open-source statistical software JASP 0.17.1. 51 The Shapiro-Wilk test was performed to determine the normality of data, with alpha set a priori at .05. Due to skewed distributions in the data, the Mann-Whitney U test was used to compare the differences in participant characteristics and the number of training errors between groups, with descriptive statistics presented as medians with interquartile ranges. Neurocognitive test scores, kinematic and kinetic data, and Borg scale ratings for perceived exertion were subjected to a 2-way repeated-measures analysis of variance (ANOVA) to determine the main effect of training (pre- vs posttraining), group (UT vs CON), and any interaction effects (training × group), with results presented as means with standard deviations. If a significant interaction effect was detected, pairwise comparisons with Bonferroni post hoc adjustment were performed to compare each dependent variable between pre- and posttraining within each group. If the sphericity assumption was violated in the repeated-measures ANOVA, degrees of freedom were Greenhouse-Geisser adjusted. A Bonferroni-adjusted alpha value of .0063 per test (.05/8) was also applied.
Results
Participant Characteristics, Training Errors, and Perceived Exertion
Participant characteristics and training errors are summarized in Table 1. There were no significant differences between groups in age, height, mass, or playing experience. The UT group demonstrated a significantly larger total number of training errors compared with the CON group (P = .003). The training errors were almost always caused by single-leg landing.
Table 1.
Participant Characteristics and Training Errors a
| Characteristics | UT Group (n = 16) | CON Group (n = 16) | P |
|---|---|---|---|
| Age, y | 21.00 (20.00-23.00) | 21.50 (19.75-22.25) | .95 |
| Height, m | 1.77 (1.63-1.85) | 1.75 (1.68-1.78) | .69 |
| Mass, kg | 71.25 (60.63-78.10) | 66.57 (61.20-75.86) | .70 |
| Playing experience, mo | 95.00 (75.50-156.00) | 145.50 (108.75-192.00) | .15 |
| Training errors, n | |||
| Cutting task (n = 20) | 0.00 (0.00-1.25) | 0.00 (0.00-0.00) | − |
| Single-leg landing task (n = 20) | 6.00 (4.00-7.25) | 3.00 (1.75-4.75) | .02 b |
| Running task (n = 20) | 0.50 (0.00-1.00) | 0.00 (0.00-0.00) | − |
| Total (n = 60) | 6.00 (5.00-10.75) | 3.00 (1.75-4.75) | .003 b |
Data are shown as median (interquartile range). Dashes indicate areas not applicable. CON, control; UT, unplanned training. Dashes indicate areas where the statistical analysis was not applicable.
Statistically significant difference between groups.
Repeated-measures ANOVA for the Borg scale revealed that the sphericity assumption was violated; to account for this violation, degrees of freedom were Greenhouse-Geisser adjusted. No significant training × group interaction was found (P = .304); however, the main effect of time was significant for the Borg scale (P < .001). Post hoc tests with Bonferroni correction showed that the Borg scale ratings at any time point (pretraining, interval between training blocks, and posttraining) were statistically significantly higher than at the resting state for both the UT and the CON groups (P < .001 for all); however, there was no significant difference in Borg scale when comparing the pretraining, interval between training blocks, and posttraining time points (Figure 4).
Figure 4.
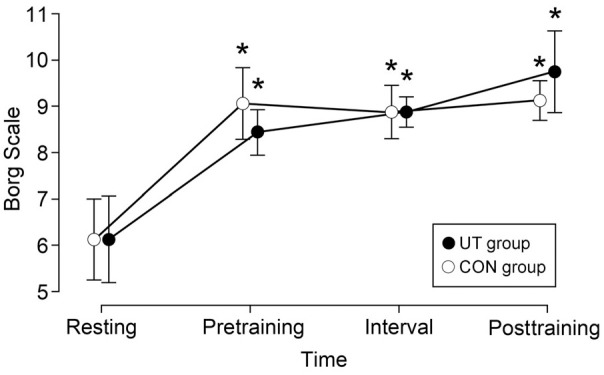
Borg scale ratings for perceived exertion in participants during rest, before training, between training blocks, and after training. Error bars represent SDs. *Statistically significant difference compared with resting. CON, control; UT, unplanned training.
Neurocognitive Test Scores
There was no significant training × group interaction for either the TMT-B or the SCWT score. However, a significant main effect of training was observed for both scores (P < .001 for both) (Table 2).
Table 2.
Pre- and Posttraining Neurocognitive Test Scores a
| Pre | Post | Test Within: Training × Group | Test Within: Training | Test Between: Group | ||||
|---|---|---|---|---|---|---|---|---|
| F (1, 32) | P | F (1, 32) | P | F (1, 32) | P | |||
| TMT-B, s | 0.57 | .46 | 28.71 | <.001 b | 1.06 | .31 | ||
| UT group | 38.56 ± 22.51 | 30.31 ± 8.87 | ||||||
| CON group | 45.53 ± 22.51 | 34.57 ± 17.36 | ||||||
| SCWT, n | 0.38 | .54 | 114.64 | <.001 b | 0.60 | .45 | ||
| UT group | 65.06 ± 11.36 | 74.75 ± 12.09 | ||||||
| CON group | 61.56 ± 10.38 | 72.44 ± 9.91 | ||||||
Data are presented as mean ± SD unless otherwise indicated. CON, control; Post, posttraining; Pre, pretraining; SCWT, Stroop Color and Word Test; TMT-B, Trail Making Test–part B; UT, unplanned training.
Significant main effect of training (P < .05).
Changes in Unanticipated Side-Step Cutting Biomechanics
The pre- and posttraining kinematic and kinetic variables during the unanticipated side-step cutting task are summarized in Appendix Table A1. There was a significant training × group interaction for knee abduction angle at PS: in posttraining compared with pretraining, the UT group displayed decreased knee abduction angles and the CON group displayed increased knee abduction angles (pre- vs posttraining: –8.81°± 7.23° vs −7.40°± 7.24° [UT group]; –8.23°± 9.40° vs −9.99°± 9.83° [CON group]; P = .02) (Figure 5A). Bonferroni post hoc test showed that there was no significant difference in knee abduction angle at PS from pre- to posttraining in either the UT or the CON groups.
Figure 5.

Significant interaction effects of (A) knee abduction (–) angle at peak stance (PS) during unanticipated side-step cutting tasks and (B) vertical ground-reaction force (vGRF) at PS during the anticipated side-step cutting task. BW, body weight; CON, control; UT, unplanned training.
There was a significant main effect of training for knee flexion moment at IC (pre- vs posttraining: –0.07 ± 0.11 vs −0.13 ± 0.17 N·m/kg [UT group]; –0.09 ± 0.13 vs −0.11 ± 0.12 N·m/kg [CON group]; P = .02) and in vGRF at PS (4.32 ± 0.85 vs 4.24 ± 0.66 %BW [UT group]; 4.25 ± 0.81 vs 3.85 ± 0.99 %BW [CON group]; P = .02). There was no significant main effect of group.
Changes in Anticipated Side-Step Cutting Biomechanics
The pre- and posttraining kinematic and kinetic variables during the anticipated side-step cutting task are summarized in Appendix Table A2. There was a significant training × group interaction for vGRF at PS: in posttraining compared with pretraining, the UT group displayed increased vGRF and the CON group displayed decreased vGRF (pre- vs posttraining: 3.86 ± 0.59 vs 4.08 ± 0.74 %BW [UT group]; 3.70 ± 0.62 vs 3.34 ± 0.62 %BW [CON group]; P = .04) (Figure 5B). Bonferroni post hoc test showed that there was no significant difference in vGRF at PS from pre- to posttraining in either group.
There was a significant main effect of training for knee flexion angle at IC (pre- vs posttraining: –13.64°± 5.11° vs −12.86°± 4.13° [UT group]; –16.99°± 3.72° vs −15.51°± 4.01° [CON group]; P = .03) and for knee flexion moment at IC (–0.11 ± 0.09 vs −0.14 ± 0.16 N·m/kg [UT group]; –0.10 ± 0.13 vs −0.16 ± 0.13 N·m/kg [CON group]; P = .01). A significant main effect of group was observed for knee flexion angle at IC (P = .04) and for vGRF at PS (P = .03).
Discussion
In the current study, neurocognitive function improved in both the UT and the CON groups after training. However, the UT group showed more beneficial changes to knee abduction angle at PS during the unanticipated side-step cutting task compared with the CON group. On the other hand, the CON group showed more beneficial changes to vGRF at PS during the anticipated side-step cutting task compared with the UT group. The findings of the current study partly supported our hypotheses that unplanned hop-landing training would significantly improve neurocognitive function and biomechanical risk factors for noncontact ACL injury during the unanticipated side-step cutting task when compared with planned training. To the best of our knowledge, this is the first report on the acute effects of unplanned (open-skill) versus planned (closed-skill) training on the neurocognitive function and knee biomechanics of the side-step cutting motion.
Acute Effects of Unplanned Versus Planned Hop-Landing Training on Neurocognitive Function
In the current study, both groups showed improvement in neurocognitive function after training; however, there was no significant training × group interaction or main effect of group (Table 2). The neurocognitive procedures used in the current study were designed to assess executive functions (ie, cognitive flexibility, working memory, inhibitory control), which are considered representative of high-order neurocognitive function. 22 Executive functions enable individuals to complete goal-oriented behavior and decision making in complex situations such as open-skill sports. 27 Open-skill exercises are, therefore, more likely to impose higher cognitive demands and loads compared with closed-skill exercises, 32 and participants must adapt to a constantly changing environment.8,44 Furthermore, multisensory stimuli in open-skill exercises could potentially enhance neural connectivity between the cerebellum, which is critical for complex movements, and the dorsolateral prefrontal cortex, which is critical for executive function, thereby resulting in substantial coactivation of these regions.8,21 In their systematic review, Gu et al 32 suggested that long-term (minimum 6-week) open-skill exercise intervention may improve executive function compared with closed-skill exercises. On the other hand, the current study only examined the acute (short-term) effects of unplanned (open-skill) training versus planned (closed-skill) training on neurocognitive function. Therefore, future research will be required to evaluate the effects of long-term unplanned training interventions on neurocognitive function.
Potential pathways through which exercise facilitates executive function include the cognitive demands required to execute complex movements and the physiological changes in the brain induced by aerobic exercise. 8 Considering that in the current study, both the UT and the CON groups improved neurocognitive function (ie, executive function) after training, the improvement may have been induced by aerobic exercise with the training, not the cognitive demands of the training. Byun et al 15 showed that acute light-intensity exercise (30% peak oxygen uptake [VO2 peak] for 10 minutes) led to improved executive function. It is postulated that the exercise-induced arousal state and arousal-related cortical activation would enhance neurocognitive performance.23,52,61 In the current study, the Borg scale at pretraining, interval between training blocks, and posttraining was significantly higher compared with the resting state in both study groups (P < .001 for all). In addition, the values were <11, which is considered light-intensity perceived exertion. 11 Therefore, an aerobic exercise state induced by the light-intensity training may have then caused arousal-related cortical activation and improved neurocognitive function in both the UT and the CON groups.
Acute Effects of Unplanned Versus Planned Hop-Landing Training on Knee Biomechanics Associated With Noncontact ACL Injury During the Side-Step Cutting Motion
In the current study, there was a significant group × training interaction for knee abduction angle at PS during the unanticipated side-step cutting task (P = .02). Specifically, in the UT group, this variable changed beneficially after the training. Biomechanically, there is a consensus that most noncontact ACL injuries involve knee abduction. 20 Therefore, unplanned training may be useful to improve ACL injury–related biomechanics during unanticipated movements. On the other hand, there was a significant group × training interaction for vGRF at PS during the anticipated side-step cutting task (P = .04). Specifically, for the CON group, this variable changed beneficially after the training. It has been reported that knee abduction combined with greater GRF could induce ACL strain. 43 The results of the current study suggest that planned training may improve anticipated movement patterns, as seen in sports that require closed skills (eg, gymnastics, track and field).
Athletes with lower baseline neurocognitive abilities may demonstrate higher biomechanical risk factors for ACL injury in unanticipated athletic situations.27,31,34,57 Thus, the level of neurocognitive function may affect biomechanics during unanticipated movements. In the current study, while both groups showed significant improvement in TMT-B and SCWT scores after the training (P < .001 for both), only the UT group demonstrated a significant improvement in the biomechanics associated with ACL injury during the unanticipated cutting task. Therefore, factors other than executive function may have been related to the posttraining biomechanical changes.
Changes in the neurosubstrates of the brain may correspond to improvements in movement capability; the acquisition of task-oriented motor skills involves a complex neural network including the cerebellum and basal ganglia as well as the executive functions.21,42 For example, to refine movements based on deviations between actual and predicted sensory consequences (ie, supervised learning), the cerebellum is thought to play an important role. 36 Repeating the same task in the same manner consistently, known as constant practice, can enhance specific task performance. 48 On the other hand, executive functions, which entail the ability to develop novel and intricate motor plans through trial and error, 22 may be improved by more diverse and flexible training programs.32,48 The results of the current study showed that participants improved in cutting tasks under conditions corresponding to their training: unplanned training improved unanticipated cutting, while planned training improved anticipated cutting. Thus, other neural networks such as the cerebellum may have supported motor control and motor learning through repetitive practice, thereby enhancing future movements. To clarify this hypothetical theory, a wider range of neurocognitive functions and athletic movements needs to be assessed in future studies.
In contrast, unfavorable changes, defined as changes in a direction linked to increased tensile forces imposed on the ACL,19,39 were observed after the training: increased vGRF at PS during the anticipated cutting task in the UT group and increased knee abduction angle at PS during the unanticipated cutting task in the CON group. In the later stages of learning a particular motor skill, motor control strategies may be refined, resulting in unconscious motion-dependent performance. 48 Typically, unplanned conditions do not allow athletes enough time to successfully develop a motor program compared with planned conditions.3,47 Moreover, Mornieux et al 47 found that unanticipated side-step cutting generated significantly higher vGRF compared with the anticipated condition. In the UT group, the participants may have performed the cutting movements with higher vGRF than participants who underwent planned training, resulting in an unconsciously higher vGRF during anticipated cutting tasks. In the CON group, the planned training may have automated closed-skill movements, requiring conscious and higher cognitive effort during reactive and unanticipated cutting tasks.32,47 This may have resulted in delays in decision making and altered whole-body motor control, potentially leading to a negative impact on movements. The results of the current study suggest that there is a need to design the training approach based on the specific demands of the sport (ie, open skill or closed skill).
The training protocol in the current study consisted of the same movements as in the experimental tasks. Benjaminse et al 7 found that a simple jump-landing task training (2 blocks each of 10 trials), identical to the baseline assessment, significantly improved lower extremity biomechanics during the jump-landing task. Following their jump-landing assessment, these authors also observed a significant improvement in biomechanics associated with ACL injury during the transfer test (45° unanticipated side-step cutting motion). 7 Considering these facts, any biomechanical improvements observed by training on the same tasks as those in the baseline assessment may potentially translate to more sport-specific movements. However, as the CON group in the current study did not demonstrate any improvement even in the unanticipated experimental cutting tasks, transfer effects to more sports-specific open-skill movements may be challenging. On the other hand, considering that knee biomechanics improved in the UT group during the unanticipated experimental cutting tasks, unplanned hop-landing training could potentially transfer to open-skill performance in actual sports. However, the results of the current study provided only fundamental insight, and the evidence was limited. Thus, future studies should investigate the transfer to unpredictable sport-specific movements, along with identifying the underlying neurocognitive mechanisms.
Limitations
The current study has some limitations. First, the study population included recreational athletes of both sexes and was not controlled according to specific sports. Therefore, the acute effects of unplanned training may have differed depending on participant sex, type of sport, and also level of skill. Second, multiple ACL injury risk factors (eg, neuromuscular, anatomic, and hormonal factors 56 ) were not assessed in the current study. Investigation of these factors would provide a better understanding of their relationship to ACL injury risk. Third, it was difficult to measure the time from the visual light stimulus cue to IC due to the limitations of the wireless sensor system. As Mornieux et al 47 demonstrated that the reduction of time from visual information to IC increases the biomechanical risk for noncontact ACL injury during unanticipated situations, the time from visual light stimulus cue to IC may have affected the side-step cutting movement data. Fourth, the training in the current study involved the same movements as those used in the experimental tasks; thus, although the study findings offer fundamental insights into the usefulness of unplanned training for unanticipated movements, its transferability to more sport-specific movements has yet to be demonstrated. 7 Therefore, there is a need to develop future studies for practical use in a real sports environment. Finally, we did not assess whether the improvement resulting from the training persisted over time. Welling et al 58 showed that the motor learning effects of simple jump-landing training persisted after 1 week (ie, retention). For future studies, it would be useful to include a retention test.
Future studies should perform a more detailed screening and assessment of the above factors before introducing ACL IPPs. Additionally, development of the training that can be adapted to each sex, sport type, and level of skill may be required.
Conclusion
Study findings showed a significant training × group interaction for knee abduction angle during the unanticipated side-step cutting task with unplanned training and for vGRF during the anticipated side-step cutting task with planned training. Designing ACL IPPs based on the sport type (ie, open skill or closed skill) may contribute to better preparation for those sports.
Acknowledgments
The authors thank all participants involved in this study and members of the laboratory. In particular, they appreciated the support of Mr Christopher Spice, technical manager at the University of Essex.
Appendix Table A1.
Pre- and Posttraining Kinematic and Kinetic Variables During the Unanticipated Side-Step Cutting Task a
| Variable | Pre | Post | Test Within: Training × Group | Test Within: Training | Test Between: Group | |||
|---|---|---|---|---|---|---|---|---|
| F (1, 32) | P | F (1, 32) | P | F (1, 32) | P | |||
| Kinematic | ||||||||
| IC knee flexion (–) angle, deg | 0.23 | .63 | 1.72 | .20 | 2.90 | .10 | ||
| UT group | −13.03 ± 5.28 | −12.62 ± 3.68 | ||||||
| CON group | −15.81 ± 4.30 | −14.92 ± 4.35 | ||||||
| PS knee abduction (–) angle, deg | 6.56 | .02 b | 0.08 | .78 | 0.12 | .73 | ||
| UT group | −8.81 ± 7.23 | −7.40 ± 7.24 | ||||||
| CON group | −8.23 ± 9.40 | −9.99 ± 9.83 | ||||||
| PS knee internal rotation (+) angle, deg | 0.78 | .38 | 2.15 | .15 | 1.05 | .31 | ||
| UT group | 10.89 ± 5.02 | 11.20 ± 6.29 | ||||||
| CON group | 12.50 ± 5.79 | 13.77 ± 6.61 | ||||||
| Kinetic | ||||||||
| IC knee flexion (–) moment, N·m/kg | 1.15 | .29 | 5.89 | .02 c | 9.67×10–34 | ≥.999 | ||
| UT group | −0.07 ± 0.11 | −0.13 ± 0.17 | ||||||
| CON group | −0.09 ± 0.13 | −0.11 ± 0.12 | ||||||
| PS knee abduction (–) moment, N·m/kg | 0.14 | .71 | 0.46 | .50 | 0.17 | .68 | ||
| UT group | −0.59 ± 0.25 | −0.57 ± 0.23 | ||||||
| CON group | −0.56 ± 0.20 | −0.55 ± 0.15 | ||||||
| PS knee internal rotation (+) moment, N·m/kg | 0.03 | .87 | 1.33 | .26 | 0.23 | .64 | ||
| UT group | 0.02 ± 0.03 | 0.02 ± 0.02 | ||||||
| CON group | 0.03 ± 0.03 | 0.02 ± 0.02 | ||||||
| PS vGRF (%BW) | 2.53 | .12 | 5.85 | .02 c | 0.70 | .41 | ||
| UT group | 4.32 ± 0.85 | 4.24 ± 0.66 | ||||||
| CON group | 4.25 ± 0.81 | 3.85 ± 0.99 | ||||||
Data are presented as mean ± SD unless otherwise indicated. BW, body weight; CON, control; IC, initial contact; Post, posttraining; Pre, pretraining; PS, peak stance; UT, unplanned training; vGRF, vertical ground-reaction force.
Significant interaction effect (P < .05).
Significant main effect of training (P < .05).
Appendix Table A2.
Pre- and Posttraining Kinematic and Kinetic Variables During the Anticipated Side-Step Cutting Task a
| Variable | Pre | Post | Test Within: Training × Group | Test Within: Training | Test Between: Group | |||
|---|---|---|---|---|---|---|---|---|
| F (1, 32) | P | F (1, 32) | P | F (1, 32) | P | |||
| Kinematic | ||||||||
| IC knee flexion (–) angle, deg | 0.46 | .50 | 4.99 | .03 b | 4.44 | .04 c | ||
| UT group | −13.64 ± 5.11 | −12.86 ± 4.13 | ||||||
| CON group | −16.99 ± 3.72 | −15.51 ± 4.01 | ||||||
| PS knee abduction (–) angle, deg | 0.07 | .79 | 2.78 | .11 | 0.01 | .93 | ||
| UT group | −7.90 ± 6.71 | −6.88 ± 7.13 | ||||||
| CON group | −7.51 ± 8.31 | −6.77 ± 7.74 | ||||||
| PS knee internal rotation (+) angle, deg | 1.89 | .18 | 0.22 | .65 | 0.80 | .38 | ||
| UT group | 9.53 ± 5.40 | 10.07 ± 6.07 | ||||||
| CON group | 12.50 ± 5.79 | 13.77 ± 6.61 | ||||||
| Kinetic | ||||||||
| IC knee flexion (–) moment, N·m/kg | 0.61 | .44 | 8.87 | .01 b | 0.05 | .83 | ||
| UT group | −0.11 ± 0.09 | −0.14 ± 0.16 | ||||||
| CON group | −0.10 ± 0.13 | −0.16 ± 0.13 | ||||||
| PS knee abduction (–) moment, N·m/kg | 0.02 | .88 | 0.72 | .40 | 6.80×10–5 | .99 | ||
| UT group | −0.59 ± 0.21 | −0.58 ± 0.23 | ||||||
| CON group | −0.60 ± 0.21 | −0.58 ± 0.22 | ||||||
| PS knee internal rotation (+) moment, N·m/kg | 1.10 | .30 | 0.08 | .78 | 0.002 | .97 | ||
| UT group | 0.01 ± 0.03 | 0.01 ± 0.02 | ||||||
| CON group | 0.01 ± 0.02 | 0.01 ± 0.03 | ||||||
| PS vGRF, %BW | 4.50 | .04 d | 0.18 | .68 | 4.99 | .03 c | ||
| UT group | 3.86 ± 0.59 | 4.08 ± 0.74 | ||||||
| CON group | 3.70 ± 0.62 | 3.34 ± 0.62 | ||||||
Data are presented as mean ± SD unless otherwise indicated. BW, body weight; CON, control; IC, initial contact; Post, posttraining; Pre, pretraining; PS, peak stance; UT, unplanned training; vGRF, vertical ground-reaction force.
Significant main effect of training (P < .05).
Significant main effect of group (P < .05).
Significant interaction effect (P < .05).
Footnotes
Final revision submitted May 23, 2024; accepted May 24, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Essex (ref No. ETH2223-0080).
ORCID iDs: Mika Konishi  https://orcid.org/0009-0007-7248-1893
https://orcid.org/0009-0007-7248-1893
Nelson Cortes https://orcid.org/0000-0001-8762-3144
References
- 1. Agel J, Rockwood T, Klossner D. Collegiate ACL injury rates across 15 sports: National Collegiate Athletic Association Injury Surveillance System data update (2004-2005 through 2012-2013). Clin J Sport Med. 2016;26(6):518-523. [DOI] [PubMed] [Google Scholar]
- 2. Ajuied A, Wong F, Smith C, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med. 2014;42(9):2242-2252. [DOI] [PubMed] [Google Scholar]
- 3. Almonroeder TG, Garcia E, Kurt M. The effects of anticipation on the mechanics of the knee during single-leg cutting tasks: a systematic review. Int J Sports Phys Ther. 2015;10(7):918-928. [PMC free article] [PubMed] [Google Scholar]
- 4. Almonroeder TG, Tighe SM, Miller TM, Lanning CR. The influence of fatigue on decision-making in athletes: a systematic review. Sports Biomech. 2020;19(1):76-89. [DOI] [PubMed] [Google Scholar]
- 5. Alvarez JA, Emory E. Executive function and the frontal lobes: a meta-analytic review. Neuropsychol Rev. 2006;16(1):17-42. [DOI] [PubMed] [Google Scholar]
- 6. Babikian T, Asarnow R. Neurocognitive outcomes and recovery after pediatric TBI: meta-analytic review of the literature. Neuropsychology. 2009;23(3):283-296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Benjaminse A, Welling W, Otten B, Gokeler A. Transfer of improved movement technique after receiving verbal external focus and video instruction. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):955-962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Best JR. Effects of physical activity on children's executive function: contributions of experimental research on aerobic exercise. Dev Rev. 2010;30(4):331-351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Boden BP, Torg JS, Knowles SB, Hewett TE. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37(2):252-259. [DOI] [PubMed] [Google Scholar]
- 10. Bogardus RL, Martin RJ, Richman AR, Kulas AS. Applying the socio-ecological model to barriers to implementation of ACL injury prevention programs: a systematic review. J Sport Health Sci. 2019;8(1):8-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Borg G. Borg’s Perceived Exertion and Pain Scales. Human Kinetics; 1998. [Google Scholar]
- 12. Brown SR, Brughelli M, Hume PA. Knee mechanics during planned and unplanned sidestepping: a systematic review and meta-analysis. Sports Med. 2014;44(11):1573-1588. [DOI] [PubMed] [Google Scholar]
- 13. Brown TN, Palmieri-Smith RM, McLean SG. Sex and limb differences in hip and knee kinematics and kinetics during anticipated and unanticipated jump landings: implications for anterior cruciate ligament injury. Br J Sports Med. 2009;43(13):1049-1056. [DOI] [PubMed] [Google Scholar]
- 14. Buckthorpe M. Optimising the late-stage rehabilitation and return-to-sport training and testing process after ACL reconstruction. Sports Med. 2019;49(7):1043-1058. [DOI] [PubMed] [Google Scholar]
- 15. Byun K, Hyodo K, Suwabe K, et al. Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: an fNIRS study. Neuroimage. 2014;98:336-345. [DOI] [PubMed] [Google Scholar]
- 16. Chia L, De Oliveira Silva D, Whalan M, et al. Non-contact anterior cruciate ligament injury epidemiology in team-ball sports: a systematic review with meta-analysis by sex, age, sport, participation level, and exposure type. Sports Med. 2022;52(10):2447-2467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Cortes N, Blount E, Ringleb S, Onate JA. Soccer-specific video simulation for improving movement assessment. Sports Biomech. 2011;10(1):22-34. [DOI] [PubMed] [Google Scholar]
- 18. Curran AR, Park AE, Bach BR, Bush-Joseph CA, Cole BJ, Yao ES. Outpatient anterior cruciate ligament reconstruction: an analysis of charges and perioperative complications. Am J Knee Surg. 2001;14(3):145-151. [PubMed] [Google Scholar]
- 19. Della Villa F, Buckthorpe M, Grassi A, et al. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med. 2020;54(23):1423-1432. [DOI] [PubMed] [Google Scholar]
- 20. Della Villa F, Tosarelli F, Ferrari R, et al. Systematic video analysis of anterior cruciate ligament injuries in professional male rugby players: pattern, injury mechanism, and biomechanics in 57 consecutive cases. Orthop J Sports Med. 2021;9(11):23259671211048182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Diamond A. Close interrelation of motor development and cognitive development and of the cerebellum and prefrontal cortex. Child Dev. 2000;71(1):44-56. [DOI] [PubMed] [Google Scholar]
- 22. Diamond A. Executive functions. Annu Rev Psychol. 2013;64:135-168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Dietrich A, Audiffren M. The reticular-activating hypofrontality (RAH) model of acute exercise. Neurosci Biobehav Rev. 2011;35(6):1305-1325. [DOI] [PubMed] [Google Scholar]
- 24. Gans I, Retzky JS, Jones LC, Tanaka MJ. Epidemiology of recurrent anterior cruciate ligament injuries in National Collegiate Athletic Association sports: the Injury Surveillance Program, 2004-2014. Orthop J Sports Med. 2018;6(6):2325967118777823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Giesche F, Wilke J, Engeroff T, et al. Are biomechanical stability deficits during unplanned single-leg landings related to specific markers of cognitive function? J Sci Med Sport. 2020;23(1):82-88. [DOI] [PubMed] [Google Scholar]
- 26. Gokeler A, Benjaminse A, Della Villa F, Tosarelli F, Verhagen E, Baumeister J. Anterior cruciate ligament injury mechanisms through a neurocognition lens: implications for injury screening. BMJ Open Sport Exerc Med. 2021;7(2):e001091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gokeler A, Tosarelli F, Buckthorpe M, Della Villa F. Neurocognitive errors and noncontact anterior cruciate ligament injuries in professional male soccer players. J Athl Train. 2024;59(3):262-269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Golden CJ. Stroop Color and Word Test: A Manual for Clinical and Experimental Uses. Stoelting Co; 1978. [Google Scholar]
- 29. Griffin LY, Albohm MJ, Arendt EA, et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med. 2006;34(9):1512-1532. [DOI] [PubMed] [Google Scholar]
- 30. Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105(2):136-144. [DOI] [PubMed] [Google Scholar]
- 31. Grooms DR, Kiefer AW, Riley MA, et al. Brain-behavior mechanisms for the transfer of neuromuscular training adaptions to simulated sport: initial findings from the Train the Brain Project. J Sport Rehabil. 2018;27(5):1-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Gu Q, Zou L, Loprinzi PD, Quan M, Huang T. Effects of open versus closed skill exercise on cognitive function: a systematic review. Front Psychol. 2019;10:1707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Hafez G, Malyszko J, Golenia A, et al. ; CONNECT Action Group. Drugs with a negative impact on cognitive functions (part 2): drug classes to consider while prescribing in CKD patients. Clin Kidney J. 2023;16(12):2378-2392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Herman DC, Barth JT. Drop-jump landing varies with baseline neurocognition: implications for anterior cruciate ligament injury risk and prevention. Am J Sports Med. 2016;44(9):2347-2353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Huang YL, Jung J, Mulligan CMS, Oh J, Norcross MF. A majority of anterior cruciate ligament injuries can be prevented by injury prevention programs: a systematic review of randomized controlled trials and cluster–randomized controlled trials with meta-analysis. Am J Sports Med. 2020;48(6):1505-1515. [DOI] [PubMed] [Google Scholar]
- 36. Hull C. Prediction signals in the cerebellum: beyond supervised motor learning. eLife. 2020;9:e54073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Jeong J, Choi DH, Shin CS. Core strength training can alter neuromuscular and biomechanical risk factors for anterior cruciate ligament injury. Am J Sports Med. 2021;49(1):183-192. [DOI] [PubMed] [Google Scholar]
- 38. Kettlety S, Lindsey B, Eddo O, Prebble M, Caswell S, Cortes N. Changes in hip mechanics during gait modification to reduce knee abduction moment. J Biomech. 2020;99:109509. [DOI] [PubMed] [Google Scholar]
- 39. Kiapour AM, Quatman CE, Goel VK, Wordeman SC, Hewett TE, Demetropoulos CK. Timing sequence of multi-planar knee kinematics revealed by physiologic cadaveric simulation of landing: implications for ACL injury mechanism. Clin Biomech (Bristol, Avon). 2014;29(1):75-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Koga H, Nakamae A, Shima Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38(11):2218-2225. [DOI] [PubMed] [Google Scholar]
- 41. Kristianslund E, Krosshaug T, Van den Bogert AJ. Effect of low pass filtering on joint moments from inverse dynamics: implications for injury prevention. J Biomech. 2012;45(4):666-671. [DOI] [PubMed] [Google Scholar]
- 42. Leisman G, Moustafa A, Shafir T. Thinking, walking, talking: integratory motor and cognitive brain function. Front Public Health. 2016;4:94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Levine JW, Kiapour AM, Quatman CE, et al. Clinically relevant injury patterns after an anterior cruciate ligament injury provide insight into injury mechanisms. Am J Sports Med. 2013;41(2):385-395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Ludyga S, Gerber M, Kamijo K, Brand S, Pühse U. The effects of a school-based exercise program on neurophysiological indices of working memory operations in adolescents. J Sci Med Sport. 2018;21(8):833-838. [DOI] [PubMed] [Google Scholar]
- 45. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. 2000;41(1):49-100. [DOI] [PubMed] [Google Scholar]
- 46. Montalvo AM, Schneider DK, Webster KE, et al. Anterior cruciate ligament injury risk in sport: a systematic review and meta-analysis of injury incidence by sex and sport classification. J Athl Train. 2019;54(5):472-482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Mornieux G, Gehring D, Fürst P, Gollhofer A. Anticipatory postural adjustments during cutting manoeuvres in football and their consequences for knee injury risk. J Sports Sci. 2014;32(13):1255-1262. [DOI] [PubMed] [Google Scholar]
- 48. Muratori LM, Lamberg EM, Quinn L, Duff SV. Applying principles of motor learning and control to upper extremity rehabilitation. J Hand Ther. 2013;26(2):94-102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32(4):1002-1012. [DOI] [PubMed] [Google Scholar]
- 50. Padua DA, DiStefano LJ. Sagittal plane knee biomechanics and vertical ground reaction forces are modified following ACL injury prevention programs: a systematic review. Sports Health. 2009;1(2):165-173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Pfadt JM, van den Bergh D, Sijtsma K, Wagenmakers EJ. A tutorial on Bayesian single-test reliability analysis with JASP. Behav Res Methods. 2023;55(3):1069-1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Ramos BP, Arnsten AFT. Adrenergic pharmacology and cognition: focus on the prefrontal cortex. Pharmacol Ther. 2007;113(3):523-536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Sánchez-Cubillo I, Periáñez JA, Adrover-Roig D, et al. Construct validity of the Trail Making Test: role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J Intl Neuropsychol Soc. 2009;15(3):438-450. [DOI] [PubMed] [Google Scholar]
- 54. Scharfen J, Peters JM, Holling H. Retest effects in cognitive ability tests: a meta-analysis. Intelligence. 2018;67:44-66. [Google Scholar]
- 55. Scherr J, Wolfarth B, Christle JW, Pressler A, Wagenpfeil S, Halle M. Associations between Borg's rating of perceived exertion and physiological measures of exercise intensity. Eur J Appl Physiol. 2013;113(1):147-155. [DOI] [PubMed] [Google Scholar]
- 56. Shultz SJ, Schmitz RJ, Benjaminse A, Collins M, Ford K, Kulas AS. ACL Research Retreat VII: an update on anterior cruciate ligament injury risk factor identification, screening, and prevention. J Athl Train. 2015;50(10):1076-1093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Swanik CB, Covassin T, Stearne DJ, Schatz P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am J Sports Med. 2007;35(6):943-948. [DOI] [PubMed] [Google Scholar]
- 58. Welling W, Benjaminse A, Gokeler A, Otten B. Enhanced retention of drop vertical jump landing technique: randomized controlled trial. Hum Mov Sci. 2016;45:84-95. [DOI] [PubMed] [Google Scholar]
- 59. Whyte EF, Moran K, Shortt CP, Marshall B. The influence of reduced hamstring length on patellofemoral joint stress during squatting in healthy male adults. Gait Posture. 2010;31(1):47-51. [DOI] [PubMed] [Google Scholar]
- 60. Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(7):1861-1876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Yanagisawa H, Dan I, Tsuzuki D, et al. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage. 2010;50(4):1702-1710. [DOI] [PubMed] [Google Scholar]