

Abstract
Objective. Sarcoidosis is a granulomatous disease affecting the lungs in over 90% of patients. Qualitative assessment of chest CT by radiologists is standard clinical practice and reliable quantification of disease from CT would support ongoing efforts to identify sarcoidosis phenotypes. Standard imaging feature engineering techniques such as radiomics suffer from extreme sensitivity to image acquisition and processing, potentially impeding generalizability of research to clinical populations. In this work, we instead investigate approaches to engineering variogram-based features with the intent to identify a robust, generalizable pipeline for image quantification in the study of sarcoidosis. Approach. For a cohort of more than 300 individuals with sarcoidosis, we investigated 24 feature engineering pipelines differing by decisions for image registration to a template lung, empirical and model variogram estimation methods, and feature harmonization for CT scanner model, and subsequently 48 sets of phenotypes produced through unsupervised clustering. We then assessed sensitivity of engineered features, phenotypes produced through unsupervised clustering, and sarcoidosis disease signal strength to pipeline. Main results. We found that variogram features had low to mild association with scanner model and associations were reduced by image registration. For each feature type, features were also typically robust to all pipeline decisions except image registration. Strength of disease signal as measured by association with pulmonary function testing and some radiologist visual assessments was strong (optimistic AUC ≈ 0.9, in models for architectural distortion, conglomerate mass, fibrotic abnormality, and traction bronchiectasis) and fairly consistent across engineering approaches regardless of registration and harmonization for CT scanner. Significance. Variogram-based features appear to be a suitable approach to image quantification in support of generalizable research in pulmonary sarcoidosis.
Keywords: sarcoidosis, variograms, radiomics, computed tomography, quantitative imaging, robustness
1. Introduction
Sarcoidosis is a systemic granulomatous disease affecting the lungs in over 90% of patients (Baughman et al 2011). The disease is highly heterogeneous in presentation and prognosis, and etiology and treatment of disease remain under investigation (Baughman and Lower 2015). Sarcoidosis often presents in the lungs as textural changes in the lung parenchyma. In practice, these abnormalities may be qualitatively assessed on chest computed tomography (CT) scans by radiologists to produce visual assessment scores (VAS) for presence and severity of abnormalities with different visual textures. Qualitative visual assessment has been shown to have low inter- and intra-rater reliability (Van den Heuvel et al 2015, Lovinfosse 2022, Benn 2024). Reliable quantification of disease related textures from images could support ongoing efforts to identify meaningful phenotypes of pulmonary sarcoidosis (Schupp 2018, Rubio-Rivas and Corbella 2020, Lin 2022, Desai 2023, Lew et al 2023, Carlson 2024).
A standard approach to quantify texture or spatial structure in images is radiomics (Haralick et al 1973, Van Timmeren et al 2020). In radiomics-based approaches, statistical measures of texture are computed from images and these measures serve as observations of engineered features in later analyses. Previous investigation of whole-lung classical radiomics in sarcoidosis showed consistently strong associations with clinical measures of disease such as pulmonary function testing (PFT) (Ryan et al 2019, Carlson 2024). However, computed radiomic feature values are known to vary substantially on the bases of differences in image acquisition, reconstruction, and processing (Mackin 2015, Rizzo et al 2018, Shiri et al 2020, Van Timmeren et al 2020). Indeed, in radiomics applications, the scanners which were used to obtain images may account for more variability than disease, necessitating harmonization (Mackin 2015, Rizzo et al 2018). Although harmonization or batch correction can be useful to produce meaningful analyses within a single study, harmonization approaches are typically not generalizable beyond the particular application, leaving it difficult to move these measures into less controlled settings such as clinical use. This suggests we might improve upon previous work by identifying alternative approaches to feature engineering which efficiently capture sarcoidosis-relevant textures while disregarding systematic variation due to study factors unrelated to disease.
In this work, we investigate potential clinical relevance and optimality of pipelines for engineering variogram-based features in the study of pulmonary sarcoidosis, with specific interest in exploring phenotyping via unsupervised clustering. Variograms are a common geostatistical tool for measuring and modelling spatial covariance within an image or spatial process as a function of distance between locations (Banerjee et al 2014). Empirical variograms have previously been used as a type of engineered radiomic feature in biomedical imaging to investigate health associations with spatial structures like texture, such as associating age and sex with bony trabecular shadows (Gough et al 1994), investigating chromatin patterns in various tissues (Diaz et al 1997, Muniandy and Stanslas 2008), assessing malignancy of lung nodules (Silva et al 2004), and identifying the presence and location of tumors in the breasts (Ericeira et al 2013). We did not find previous application of variograms in the study of interstitial lung diseases like sarcoidosis, though other measures specifically related to spatial covariance such as Geary’s C and Moran’s I have been considered (Ryan et al 2019). Models for variogram functions typically include overall magnitude of variation and a notion of spatial scale of correlation as parameters, and tend to be more interpretable measures of spatial structure than their classical radiomic counterparts. As variograms are closely related to measures of spatial covariance, variogram features also have the potential to be less sensitive to noise and distortions attributable to image acquisition which happen not to affect the spatial covariance structure in particular.
Use of variogram-based features as engineered radiomic features is historically handled differently from classical radiomics, for which robustness of features to the imaging pipeline is considered fundamentally important (Lambin 2017, Van Timmeren et al 2020, Zwanenburg 2020). While empirical variogram features have long been observed to also differ with image acquisition and pre-processing factors, these features have been valued as a sensitive analytic tool for that reason (Carr and De Miranda 1998, Dai and Khorram 1998, Goodin et al 2004, Luo et al 2022). Investigations of variograms as radiomics routinely consider optimal decisions such as regions and resolutions for computation and standardization of images with respect to image contrast (Gough et al 1994, Diaz et al 1997, Keil et al 2012, Jacob et al 2013, Jacob and Carson 2014). By comparison, relatively little attention has been given to classical radiomics as a sensitive tool for which image processing and feature engineering might be optimized to produce strong signal (Lv et al 2018, Au et al 2021). While robustness of feature computation to variability in image acquisition and processing is desirable in that it supports generalizability of research to new cohorts and contexts, understanding which processing decisions lead to efficient extraction of disease signal is also fundamentally important.
The purpose of this paper is to establish clinical relevance of and identify an appropriate pipeline for variogram-based study of sarcoidosis chest CT phenotypes in future clinical cohorts. To uncover influential decisions in the engineering pipeline, we quantified sensitivity of variogram-based features and clusters to processing specifications under 24 different feature engineering pipelines producing 48 clustering analyses. We further assessed presence and strength of disease-relevant signals of heterogeneity for each clustering analysis to identify pipelines which best supported study of sarcoidosis.
2. Materials and methods
2.1. Data
The Genomic Research in alpha-1 antitrypsin deficiency (AATD) and sarcoidosis (GRADS) study (Moller 2015, Vukmirovic 2021) was a multi-site study in the United States (N = 368) with 10 participating sites. All subjects gave written informed consent according to the site’s institutional review board. Enrolled subjects underwent physical examination, PFT, research chest x-ray (CXR), and high resolution CT imaging.
CXR was performed based on the site’s standard protocol and Scadding Stage was determined by the site radiologist. CT was obtained in accordance with the standardized GRADS protocol (Moller 2015). 3D chest CT scans were obtained as a series of 2D axial images or slices. Scans from this cohort included a complete set of sequentially adjacent axial slices and were obtained using 8 different scanner models.
From the GRADS cohort, N = 337 subjects had CT scans available and of sufficient quality for investigation in this study; that is, inspiratory scans of appropriate resolution and reconstruction lacking artifacts and successfully masked and segmented. See Carlson (2024) for details of original image acquisition, reconstruction, and selection for use in analysis. All images were resampled to have the same resolution (1 × 1 × 1 mm) and centered. Images were then masked and segmented using the lungct package (Ryan et al 2020) in R (2020), producing two binary images indicating presence of left or right lung tissue. For registered analyses, an individual’s 3D lung mask was further registered to a sarcoidosis-specific template lung mask, and the corresponding transformation was then used to register each individual’s CT scan to a template lung. See Ryan et al (2020) for details of masking and registration.
While GRADS CTs were interpreted for many CT abnormalities by a dedicated thoracic chest radiologist determined by GRADS to evaluate sarcoidosis and AATD, we used a simplified visual assessment scoring (VAS) method developed by our radiologists for sarcoidosis. Experienced thoracic radiologists evaluated CT for the presence of the following features: mediastinal and hilar lymphadenopathy, micronodules, ground-glass opacity, consolidation, conglomerate perihilar or peribronchovascular mass, linear or reticular abnormality, fibrotic abnormality, honeycombing, mosaic attenuation, architectural distortion, traction bronchiectasis, bronchial wall thickening, cysts, cavity, emphysema, and air trapping. Definitions of these findings were based on Bankier (2024). For this work, we considered only a subsetted VAS panel for abnormalities deemed present in 15%–85% of the GRADS cohort: mediastinal and hilar lymphadenopathy, micronodules, ground-glass, conglomerate mass, reticular abnormality, fibrotic abnormality, mosaic attenuation, architectural distortion, and traction bronchiectasis. See supplemental figure 16 for example images of features.
PFT was performed according to established criteria per the GRADS protocol (Moller 2015), including post broncho-dilation forced expiratory volume in one second (FEV1), forced vital capacity (FVC), ratio of FEV1 to FVC (FEV1/FVC), and single-breath carbon monoxide diffusing capacity (DLCO). DLCO was corrected for elevation in accordance with (Graham et al 2017).
Collected demographics included age, height, weight, body mass index (BMI), sex, and self-reported primary race and ethnicity. Self-reported primary race and ethnicity were collapsed in this study into a single marker to reduce identifiability of participants with rarer self-reported descriptions and improve power in analyses as follows: all subjects reporting Hispanic ethnicity were reported in this study as Hispanic subjects and all subjects self-reporting ethnicity as non-Hispanic and primary race as white or as black were reported as white subjects or as black subjects respectively. All remaining subjects self-reported a primary race as Asian, American Indian, or Alaska Native, or did not identify a single primary race (identifying as multi-racial, having no primary race, or having unknown primary race), and are reported together as subjects in a combined group.
2.1.1. Cohort descriptive statistical analysis
Covariates comprised of demographics age, height, sex, BMI, and race/ethnicity, PFT outcomes, and presence of VAS outcomes are summarized for the N = 337 individuals in this study, stratified by Scadding stage, and reported with counts and percents for categorical covariates and with means and standard deviations for continuous covariates.
2.2. Feature engineering
2.2.1. Variogram Theory
We discuss variogram theory explicitly in the context of 3D images such as CT scans. In this context, a voxel is a 3D analog of the 2D pixel. To describe the models, we will assume stationarity, meaning the image has the same distribution at every location, and isotropy, meaning the image has the same distribution in every direction. As described below, we can later relax these assumptions for investigation of their impact on estimation.
Under further reasonable assumptions, the variogram function may be understood as where C(h) is the common covariance of the hues of any two voxels separated by a distance h. More generally, let z denote an image meeting the above conditions with hues at observed voxels . If z is observed at any two voxels a distance h apart, we may define
noting this definition to be independent of the specific pair (i, j) by stationarity and isotropy. See Banerjee et al (2014) for more detail. We note that terminology around the variogram is not settled. Some might say semivariogram or semivariance (Banerjee et al 2014) or γ-variance (Bachmaier and Backes 2011), among other terms. We use the term variogram for limited consistency with established literature.
To model variograms, three of the most common families are the exponential, Gaussian, and spherical families. We consider the exponential family as well as the Matérn family, a larger family including the exponential and Gaussian families as special cases. The Matérn family is very flexible, standardly used and recommended, and exhibits many desirable mathematical properties and interpretations (Banerjee et al 2014). The Matérn family has parameters nugget, partial sill, range, and kappa or degrees of freedom. In turn, these parameters may be understood to describe noise, overall variability not attributed to noise, the distance at which image voxels appear to become roughly uncorrelated, and image smoothness. Exponential models are a widely used special case which are more analytically tractable with kappa (image smoothness) set to 0.5.
For a high resolution image of a large region such as chest CT of the lungs, the variogram value is well-estimated empirically using voxel pairs a distance apart. If we expect the assumption of stationarity to be violated by a non-constant mean, empirical variograms may also be computed from residuals obtained by subtracting off an assumed or estimated mean image from the observed image. In absence of statistical models, variogram models are classically fit from empirical variograms using weighted least squares (Cressie 1985).
2.2.2. Application to GRADS
From the chest CT scans, 24 similar datasets were engineered through the use of variograms; see figure 1. Datasets were distinguished through the decisions to a) register images to a template or not, b) assume stationarity or account for linear drift in computation of empirical variograms, c) use empirical variograms or fit variogram model parameters for either exponential or Matérn models, and d) harmonize or not harmonize data for CT scanner effects; details follow. These specific decisions are considered as registration and harmonization are established impediments to generalizability in radiomics-style analyses and stationarity is a strong assumption which should be evaluated. Furthermore, while empirical variograms appear to be used almost exclusively in previous biomedical works (Gough et al 1994, Diaz et al 1997, Silva et al 2004, Ericeira et al 2013), fitting of standard variogram models may allow us to capture the same information with a smaller number of features.
Figure 1.
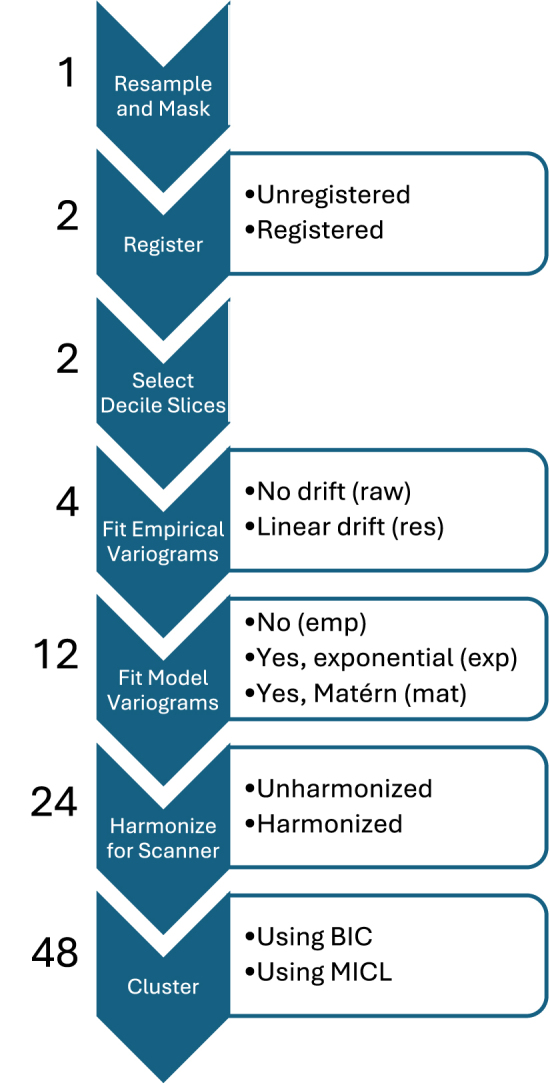
Steps in the image processing, feature engineering, and clustering pipeline. The number of datasets or analyses after completing each step is listed to the left, and steps permitting decisions have decision options listed to the right.
To ensure sufficient data for variogram estimation, all top and bottom axial slices of the left lung and right lung images with fewer than 1000 voxels indicated to be lung tissue by the corresponding mask were removed from consideration. Unregistered images paired with the unregistered mask or registered images paired with the template mask were then used for this study. For unregistered images, this typically produced images with 150–300 axial slices with at most 3.3% of lung voxels removed from consideration. For registered images, this produced 228 (left) and 232 (right) sequential axial slices with 0.3% of lung voxels removed from consideration.
The number of axial slices considered was then substantially reduced to account for the sometimes reduced availability of axial slices in clinically obtained images. Requiring fewer slices supports broader inclusion of participants and potentially more consistent feature extraction. Specifically, for each image, observations for the inner decile axial slices of each lung were extracted, resulting in 18 axial slices per 3D CT image. That is, for each lung, 9 axial slices were selected which broke the masked lung into 10 equal height segments. Decile 1 corresponded with the lowest retained axial slice of the lung while decile 9 corresponded with the uppermost retained axial slice. Decile indices were determined independently for individuals and for right and left lungs. These decile slices were then used for computation of variogram features.
For each axial slice, two empirical variograms were computed under the assumption of either stationarity and isotropy (from raw data) or the same except permitting a linear mean trend (from linear residuals). The variogram function from the gstat package (Gräler et al 2016) in R was used for computation with a cutoff of 25 mm, a formula of HU ~ 1 indicating no drift, and otherwise default settings for variograms from raw data. Default settings estimated variogram values at 15 values from 0 to the cutoff using equal size bins. For variograms from linear residuals, the same function was used with a cutoff of 25 mm, a formula of HU ~ x + y indicating linear drift, and otherwise default settings. This produced four empirical variogram datasets differing by decisions on registration and accounting for drift.
An additional eight engineered datasets were computed from these four by fitting either an exponential or Matérn variogram model to the empirical variograms and using the fit model parameters as features. Models were fit using the fit.variogram function from the gstat package in R with initial psill value given by the maximum empirical variogram value, initial range value 1, and fit.method 2 corresponding with weighted least squares. In each case, the nugget parameter (noise) is set to zero. For computational reasons, parameter kappa is not fit continuously but rather permitted to take one of a list of pre-specified values: seq(0.01,5,0.01). Fit range and psill parameters were then log-transformed to account for skew and standardized. For two subjects, model fit parameters were estimated as negative for some datasets, which is not reasonable. These two subjects were thus removed across all datasets to preserve comparability, resulting in N = 335 subjects with unharmonized engineered feature data.
Finally, from these twelve datasets, another twelve datasets were produced via harmonization. The ez.combat package (Koscik 2021) in R was used with default settings to adjust for CT scanner model while preserving variability associated with Scadding stage, height, age, BMI, and sex. N = 330 subjects had complete Scadding and demographic data for producing harmonized engineered feature data.
In summary, 24 datasets were computed, differing by registration, accounting for drift, data type (empirical, exponential, Matérn), and harmonization; see figure 1. For each dataset, lung-deciles were presumed to correspond across individuals, resulting in balanced datasets with features identified by lung, decile, and value computed, either an empirical variogram value at a specific distance h (p = 270 features) or an estimated parameter value for a specific variogram model parameter (p = 36 features for exponential model, p = 54 features for Matérn model).
2.2.3. Feature robustness and association with scanner
We assessed dataset association with scanner model by regressing each feature in each dataset onto scanner model and reporting dataset distributions of model R squared and F-test p-value.
We also assessed robustness or stability of feature computation for matched pairs of variables across datasets. For a pair of variables from different datasets, the variables were considered matched if they were computed for the same lung-decile and were either (a) both empirical variogram values at the same specified distance or (b) both estimates of the same parameter. For example, the right lung decile 9 empirical variogram values at distance 25 mm would be matched for the (empirical, linear residual, unregistered, unharmonized) dataset and the (empirical, raw data, unregistered, harmonized) dataset, as would the left lung decile 1 estimates of partial sill for the (exponential, linear residual, unregistered, harmonized) dataset and the (Matérn, raw data, registered, unharmonized) dataset.
Following Lv et al (2018), Denzler (2021), for each matched pair of variables, for all available data () we computed the two-way random effects, single measurement intra-class correlation coefficient for consistency (ICC(3,1)) using the icc function from the irr package (Gamer et al 2019) in R with specifications model = ”twoway”, type = ”consistency”, unit = ”single”. In accordance with (Koo and Li 2016, Lv et al 2018, Denzler 2021), we understand ICC values above 0.9 to indicate excellent robustness.
We compute also the Spearman’s correlation coefficient using the cor function in R to investigate monotonicity of association between matched pairs in absence of robustness.
2.3. Clustering analyses
2.3.1. Clustering
Each of the 24 datasets was clustered in two ways (unharmonized data: N = 335; harmonized data: N = 330), producing 48 clustering analyses; see figure 1. Model-based clustering was used, specifically a sparse diagonal Gaussian mixture model assuming homoscedasticity of irrelevant features and selecting sparsity using an information criterion (Celeux and Govaert 1995, Marbac and Sedki 2017). The VarSelCluster function from the VarSelLCM package (Marbac and Sedki 2017, Marbac et al 2020) in R was used to cluster features allowing for between 1 and 8 resultant clusters. One clustering approach used default settings which performs model selection using the Bayesian information criterion (BIC). The other clustering approach used Maximum integrated complete-data likelihood (MICL) for model selection and otherwise default settings. The MICL is a less standard information criterion previously observed to outperform BIC when paired with the VarSelLCM approach (Marbac and Sedki 2017). Features selected as relevant and number of clusters selected in cluster analysis are reported.
As we use empirical and model fit variogram measures which are highly related to measures of covariance as features for clustering, we note that we effectively take a covariance-based clustering approach (Ieva 2016, Hallac et al 2017) similar to that of Marquez et al (2021).
2.3.2. Cluster descriptives and comparisons
Each cluster analysis was compared in turn to covariates scanner model, PFT, and VAS outcomes. Cluster analyses were further compared pairwise to each other to assess sensitivity of clustering results to data processing and analysis decisions. Strength of association was assessed using R squared values when comparing to PFT and bias-corrected Cramér’s V (Bergsma 2013) otherwise. Differences in covariates and in demographics across groupings were assessed and p-values reported via Fisher exact test with simulated p-value from 20 000 replicates for categorical covariates or via F-test p-value for continuous covariates. For these analyses, complete case analyses were performed for each assessment individually.
2.3.3. Cluster associations with clinical outcomes
We assessed strength of association between clusters and clinical outcomes PFT and VAS after adjusting for demographics or for demographics and Scadding stage. Linear regression was used to predict PFT and Firth logistic regression was used to predict VAS. Demographics adjusted for included sex, height, age, and BMI. Note, we exclude self-reported race and ethnicity as an adjustment factor in these analyses. The nature of the relationship between self-reported race and ethnicity and disease presentation in sarcoidosis remains under study (Hena 2020, Sharp et al 2020, Zhou 2021), and adjustment could hide disease signal or compound systematic biases in selection of appropriate pipelines.
For each outcome, two models were fitted without clusters, one with covariates demographics (base model) and one with covariates demographics and Scadding stage (Scadding only model). Then, for each cluster analysis, two more models were fitted, one with covariates demographics and clusters (cluster only model), and one with covariates demographics, clusters, and Scadding stage (full model).
For each model predicting PFT, we reported an R squared value. For each model predicting VAS, we reported an area under the curve (AUC) value obtained from predicting the observed outcomes. Models were fitted to and AUC values were computed for the same data, and so AUC values are ‘optimistic’ training AUC values and understood here as a summary of model fit. For each pair of outcome and cluster analysis, we report likelihood ratio test p-values (PFT) or penalized likelihood ratio test p-values (VAS) for 3 pairs of models: the full and Scadding only models, the cluster only and base models, and the full and cluster only models. Additionally, for each outcome, we report a p-value comparing the Scadding only and base models.
For these analyses, subjects with complete adjustment demographic, Scadding stage, and PFT data (N = 313) were analysed for PFT outcomes and subjects with complete adjustment demographic, Scadding stage, and VAS data (N = 322) were analysed for VAS outcomes.
3. Results
3.1. Cohort descriptives
Subjects were 54% Female and 53 years old on average; see table 1 (N = 337). Subjects predominantly identified as non-Hispanic and White (69%) followed by Non-Hispanic and Black (24%). All PFT and VAS assessments appear to differ substantially by Scadding stage with subjects in stage 0 exhibiting least severe disease and subjects in stage IV exhibiting most severe disease as expected. Inconsistencies between CT-based assessments (VAS) and CXR-based assessments (Scadding) of lymphadenopathy, parenchymal abnormalities, and fibrosis have been previously noted (Zhang 2022), including for this cohort for lymphadenopathy and parenchymal abnormalities (Benn 2024). Inconsistencies included 46% and 32% of subjects in stages II and III having fibrotic abnormalities on CT.
Table 1.
Demographics, post-bronchodilator PFT, and VAS by Scadding for full cohort.
| Scadding Stage | ||||||||
|---|---|---|---|---|---|---|---|---|
| N miss | 0, N = 43 | I, N = 69 | II, N = 97 | III, N = 45 | IV, N = 79 | NA, N = 4 | Overall, N = 337 | |
| Sex | 2 | |||||||
| Female | 27 (62.8%) | 43 (62.3%) | 43 (44.3%) | 23 (51.1%) | 43 (55.1%) | 2 (66.7%) | 181 (54.0%) | |
| Male | 16 (37.2%) | 26 (37.7%) | 54 (55.7%) | 22 (48.9%) | 35 (44.9%) | 1 (33.3%) | 154 (46.0%) | |
| Race/Ethnicity | 3 | |||||||
| White | 33 (76.7%) | 54 (78.3%) | 65 (67.0%) | 30 (68.2%) | 44 (56.4%) | 3 (100.0%) | 229 (68.6%) | |
| Black | 6 (14.0%) | 12 (17.4%) | 22 (22.7%) | 12 (27.3%) | 28 (35.9%) | 0 (0.0%) | 80 (24.0%) | |
| Hispanic | 3 (7.0%) | 3 (4.3%) | 4 (4.1%) | 1 (2.3%) | 5 (6.4%) | 0 (0.0%) | 16 (4.8%) | |
| Combineda | 1 (2.3%) | 0 (0.0%) | 6 (6.2%) | 1 (2.3%) | 1 (1.3%) | 0 (0.0%) | 9 (2.7%) | |
| Age (years) | 2 | 53.04 (9.51) | 51.57 (11.47) | 53.15 (9.29) | 50.62 (10.89) | 55.16 (9.02) | 53.04 (5.86) | 52.94 (9.99) |
| BMI (kg/m2) | 0 | 33.40 (6.46) | 31.81 (6.93) | 29.53 (5.38) | 32.49 (7.35) | 28.29 (5.57) | 31.45 (6.97) | 30.62 (6.42) |
| Height (in) | 0 | 66.67 (4.08) | 66.96 (3.45) | 67.71 (4.23) | 66.49 (4.23) | 66.51 (4.04) | 63.75 (4.19) | 66.93 (4.03) |
| DLCo (ml/min/mmHg) | 18 | 24.45 (7.52) | 23.86 (7.82) | 23.69 (7.39) | 21.54 (8.06) | 17.60 (7.16) | 20.80 (1.74) | 22.08 (7.90) |
| FVC (L) | 11 | 3.69 (1.04) | 3.76 (1.09) | 3.84 (1.12) | 3.58 (1.14) | 3.11 (1.15) | 3.75 (0.80) | 3.60 (1.14) |
| FEV1 (L) | 11 | 2.92 (0.82) | 2.97 (0.91) | 2.90 (0.88) | 2.72 (0.99) | 2.11 (0.89) | 2.68 (0.80) | 2.70 (0.95) |
| FEV/FVC (%) | 11 | 79.77 (9.32) | 78.74 (8.48) | 75.69 (8.26) | 76.14 (12.69) | 68.61 (13.50) | 71.15 (12.58) | 75.18 (11.19) |
| Mediastinal LA | 9 | 12 (27.9%) | 37 (55.2%) | 61 (64.2%) | 12 (27.3%) | 47 (61.8%) | 1 (33.3%) | 170 (51.8%) |
| Hilar LA | 9 | 8 (18.6%) | 27 (40.3%) | 55 (57.9%) | 8 (18.2%) | 42 (55.3%) | 1 (33.3%) | 141 (43.0%) |
| Micronodules | 9 | 14 (32.6%) | 38 (56.7%) | 81 (85.3%) | 32 (72.7%) | 65 (85.5%) | 0 (0.0%) | 230 (70.1%) |
| Conglomerate | 9 | 0 (0.0%) | 2 (3.0%) | 26 (27.4%) | 8 (18.2%) | 53 (69.7%) | 0 (0.0%) | 89 (27.1%) |
| Architectural distortion | 9 | 2 (4.7%) | 8 (11.9%) | 47 (49.5%) | 16 (36.4%) | 73 (96.1%) | 0 (0.0%) | 146 (44.5%) |
| Traction bronchiectasis | 9 | 2 (4.7%) | 4 (6.0%) | 34 (35.8%) | 11 (25.0%) | 71 (93.4%) | 0 (0.0%) | 122 (37.2%) |
| Fibrotic abnormality | 9 | 2 (4.7%) | 5 (7.5%) | 44 (46.3%) | 14 (31.8%) | 74 (97.4%) | 0 (0.0%) | 139 (42.4%) |
| Ground-glass | 9 | 5 (11.6%) | 16 (23.9%) | 36 (37.9%) | 15 (34.1%) | 52 (68.4%) | 0 (0.0%) | 124 (37.8%) |
| Reticular abnormality | 9 | 1 (2.3%) | 11 (16.4%) | 44 (46.3%) | 19 (43.2%) | 60 (78.9%) | 0 (0.0%) | 135 (41.2%) |
| Mosaic attenuation | 9 | 1 (2.3%) | 8 (11.9%) | 14 (14.7%) | 9 (20.5%) | 32 (42.1%) | 0 (0.0%) | 64 (19.5%) |
Includes subjects who both did not identify as Hispanic and also either identified as Asian, American Indian, Alaska Native, or did not identify as a single primary race.
3.2. Feature robustness and association with scanner
Among the 12 unharmonized datasets, use of unregistered images or empirical variogram data was typically associated with stronger associations between features and scanner model; see figure 2. Matérn data were typically least associated with scanner and exhibited near uniform distributions of p-values for association with scanner model consistent with lack of association. R squared values were typically below 0.15. Harmonized datasets exhibited feature R squared values of approximately 0 and p-values biased towards 1 as expected.
Figure 2.

Density histograms of R squared values and p values obtained by regressing each engineered feature onto scanner model, stratified by the 24 engineered datasets (see figure 1 for datasets and acronyms).
Pairs of matched variables from datasets differing only in handling of drift and use of harmonization typically exhibited excellent robustness (ICC); see figure 3, top two rows. Pairs of matched variables differing in use of registration (bottom row) exhibited moderate to good robustness for empirical datasets (ICC) and variable robustness for exponential and for Matérn datasets. Pairs of matched variables from datasets differing in harmonization exhibited slightly reduced ICC but harmonization was not substantially impactful; see supplementary figure 8. Spearman’s correlation was generally consistent with ICC, suggesting non-excellent robustness related to registration was generally not attributable to monotonic transformation; see supplementary figure 9.
Figure 3.

Histograms of intraclass correlation coefficients between matched variable pairs from different engineered datasets, stratified by engineered dataset (see figure 1 for datasets and acronyms). Harmonized and unharmonized data are similar and thus pooled.
Matched variable pairs for which one variable was from Matérn data and the other was from exponential data exhibited differing robustness patterns by parameter; see supplementary figure 10. Patterns for the psill parameter were consistent with patterns described above, with robustness typically excellent unless datasets differed by registration as well. Robustness for the range parameter was highly variable and especially poor when datasets differed by registration, suggesting these data may not be comparable.
3.3. Cluster results, consistency, and association with scanner
The 48 clustering analyses typically resulted in between 6 and 8 clusters; see supplemental table 3. Most cluster analyses selected models which were not sparse; see supplemental figure 11. Analyses of empirical variogram data selected all variables. Analyses of fit Matérn variogram model parameters, especially those using MICL for model selection, tended to be sparser. Partial sill parameters were deemed relevant from all locations by all analyses while range exhibited variable relevance and kappa parameters were typically deemed relevant almost everywhere for analyses using BIC, and relevant at the bottom of the lungs for analyses using MICL. Relevance patterns did not differ substantially between left and right lungs. Analyses of fit exponential variogram model parameters similarly deemed partial sill parameters to be relevant everywhere. Range parameters were deemed relevant everywhere when registration was used in feature engineering and at the tops and bottoms of the lung when it was not. Harmonization and drift were not substantial factors for relevance.
All cluster analyses from harmonized data were not significantly associated with scanner (p > 0.1), as expected; see table 2. Cluster analyses from unharmonized, unregistered data exhibited stronger, more significant associations (p < 0.001) with scanner model than cluster analyses from unharmonized, registered data (p > 0.01), consistent with patterns of associations between variogram features and scanner model. Association strength between clusters from unharmonized, unregistered data and scanner model ranged from 0.15 to 0.3 as measured by Cramér’s V, indicating cluster analyses did differ substantially from scanner model.
Table 2.
For each of the 48 cluster analyses (see figure 1), we report the strength of association between clusters and scanner model using Cramér’s V. In parentheses, we report simulated Fisher’s exact test p-values (20 000 replicates) with * indicating p < 0.001 and - indicating p > 0.1.
| Registered | Unregistered | |||||
|---|---|---|---|---|---|---|
| Data | Drift | IC | Harmonized | Unharmonized | Harmonized | Unharmonized |
| Empirical | Linear | BIC | 0.000 (-) | 0.086 (0.035) | 0.055 (-) | 0.188 (*) |
| Empirical | Linear | MICL | 0.000 (-) | 0.092 (0.034) | 0.000 (-) | 0.163 (*) |
| Empirical | Raw | BIC | 0.062 (-) | 0.078 (0.050) | 0.020 (-) | 0.178 (*) |
| Empirical | Raw | MICL | 0.000 (-) | 0.126 (0.005) | 0.000 (-) | 0.151 (*) |
| Exponential | Linear | BIC | 0.023 (-) | 0.069 (0.059) | 0.000 (-) | 0.271 (*) |
| Exponential | Linear | MICL | 0.065 (-) | 0.052 (-) | 0.000 (-) | 0.279 (*) |
| Exponential | Raw | BIC | 0.057 (-) | 0.083 (0.013) | 0.000 (-) | 0.247 (*) |
| Exponential | Raw | MICL | 0.000 (-) | 0.076 (0.035) | 0.000 (-) | 0.276 (*) |
| Matern | Linear | BIC | 0.000 (-) | 0.000 (-) | 0.000 (-) | 0.189 (*) |
| Matern | Linear | MICL | 0.000 (-) | 0.092 (0.012) | 0.000 (-) | 0.187 (*) |
| Matern | Raw | BIC | 0.000 (-) | 0.076 (0.076) | 0.000 (-) | 0.188 (*) |
| Matern | Raw | MICL | 0.000 (-) | 0.031 (-) | 0.000 (-) | 0.196 (*) |
Pairwise comparisons of cluster analyses using Cramér’s V showed strong consistency across analyses; see figure 4. All comparisons produced values above 0.4, 40% produced values above 0.6, and 15% produced values above 0.7. 70% of comparisons of unregistered analyses produced values above 0.6 while 60% of comparisons of registered analyses produced values above 0.6. 48% of comparisons of unharmonized analyses produced values above 0.6 while 54% of comparisons of harmonized analyses produced values above 0.6.
Figure 4.

Pairwise comparisons by Cramér’s V of 48 cluster analyses (see figure 1 for datasets and acronyms).
Registration was the most influential factor in consistency across the 48 analyses, followed by harmonization and data type (empirical, exponential, or Matérn). Strongest consistency was observed between analyses differing only in handling of drift or selection criterion.
3.4. Clinical outcomes and demographics by clusters
Comparisons of demographics, PFT, and VAS to each of the 48 clustering analyses are summarized; see figure 5 for unadjusted association strength and supplemental figure 12 for corresponding p-values.
Figure 5.

Cramér’s V comparing 48 cluster analyses (see figure 1 for datasets and acronyms) to VAS and linear model r-squared values predicting PFT from each analysis without adjustment.
All analyses produced clusters which differed significantly by DLCO, FEV1, and FVC (p < 0.001) and by BMI and FEV1/FVC (p < 0.05). Most analyses produced clusters which differed significantly by self-reported race and ethnicity indicator (p < 0.001), with analyses from data not harmonized for scanner effects exhibiting stronger association. Most analyses produced clusters which differed significantly by sex (p < 0.05), though no clusters produced from unharmonized empirical variogram data differed significantly by sex. Most analyses produced clusters which did not differ significantly by age and height (p > 0.05), though all analyses from registered exponential data differed significantly by height (p < 0.001).
Most analyses produced clusters which differed significantly (p < 0.001) by each VAS measure except mediastinal lymphadenopathy.
A comparison of cluster analyses with VAS using Cramér’s V showed that clusters tended to capture architectural distortion, conglomerate mass, fibrotic abnormality, and traction bronchiectasis particularly well (typical Cramér’s V ), as well as ground-glass, mosaic attenuation, and reticular abnormality more modestly (typical Cramér’s V ); see figure 5. A comparison of cluster analyses with PFT further suggested strong associations between PFT and clusters. Clusters generally explained 15%–35% of variability observed in FEV1, FVC, and DLCO. Clusters obtained from fitting exponential variogram models to registered data were particularly strongly associated with FEV1 and typically explained 25%–35% of variability. Overall, clusters obtained from registered data exhibited slightly stronger unadjusted associations with PFT outcomes than those from unregistered data.
3.5. Cluster associations with clinical outcomes after adjustment
After adjusting for base demographic factors, clusters exhibited strong associations with PFT; see figure 6 for R squared summaries, supplemental figure 13 for p-value summaries. Clusters typically explained another 10%–15% of variability beyond base adjustment factors.
Figure 6.
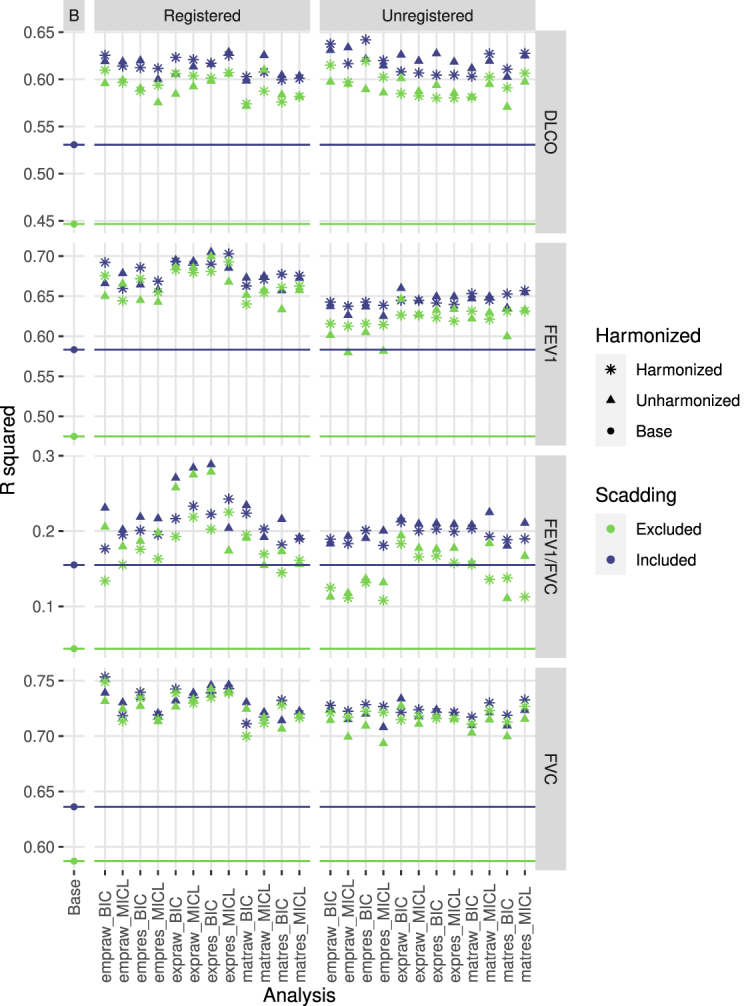
R squared values for various linear models predicting PFT from base adjustment factors, cluster analysis grouping, and Scadding stage, with color indicating inclusion or exclusion of Scadding stage as a variable and shape indicatating whether engineered data were harmonized prior to clustering. For each of 48 cluster analyses (see figure 1 for datasets and acronyms), we fitted a model with base factors and group and a model with base factors, group, and Scadding. Additionally, we fitted a model with base factors and a model with base factors and Scadding, indicated as the base analyses. For reference, horizontal lines indicate R squared values for base models.
Associations with DLCO, FEV1, and FVC were similar compared to each other and across cluster analyses. Scadding stage typically lost significance (p > 0.001 or p ≈ 0.001) in the presence of clusters and clusters were significant () with or without adjusting for Scadding. Clusters alone explained much more variability than Scadding stage alone beyond base adjustment factors. Scadding stage did not explain substantially more variation beyond cluster grouping and base adjustment factors. Clusters from registered data typically exhibited slightly stronger associations, with the effect of registration most pronounced for FEV1.
For FEV1/FVC, clusters produced from registered data exhibited stronger associations more often with or without adjusting for Scadding stage, especially when clusters were produced from unharmonized exponential data. Clusters alone typically explained as much variability as Scadding stage alone beyond base adjustment factors.
Most full models of VAS produced (training) AUC roughly 0.05 greater than Scadding models, while most cluster models produced AUC roughly the same as Scadding models; see figure 7 for AUC summaries, supplemental figure 14 for p-value summaries. Full models of architectural distortion, conglomerate mass, fibrotic abnormality, and traction bronchiectasis all produced AUC around or above 0.9, with full models of ground-glass, micronodules, mosaic attenuation, and reticular abnormality producing AUC around or above 0.8. All models of hilar and mediastinal lymphadenopathy failed to produce AUC above 0.75.
Figure 7.

AUC values for various firth-type logistic models predicting VAS from base adjustment factors, cluster analysis grouping, and Scadding stage, with color indicating inclusion or exclusion of Scadding stage as a variable and shape indicatating whether engineered data were harmonized prior to clustering. For each of 48 cluster analyses (see figure 1 for datasets and acronyms), we fitted a model with base factors and group and a model with base factors, group, and Scadding. Additionally, we fitted a model with base factors and a model with base factors and Scadding, indicated as the base analyses. For reference, horizontal lines indicate AUC values for base models.
AUC values were typically comparable between registered and unregistered analyses, and between harmonized and unharmonized analyses.
Association between clusters and VAS measures was typically significant (p < 0.001) for cluster and full models of architectural distortion, conglomerate mass, fibrotic abnormality, reticular abnormality, and traction bronchiectasis. Associations between clusters and VAS measures were typically significant in cluster models but lost significance after adjustment for Scadding stage in models of ground-glass, hilar adenopathy, micronodules, and mosaic attenuation. Scadding stage typically remained significant in full models of architectural distortion, fibrotic abnormality, hilar and mediastinal lymphadenopathy, micronodules, reticular abnormality, and traction bronchiectasis, while dropping to marginal significance (p ≈ 0.001) in full models of conglomerate mass and ground-glass and losing significance (p > 0.001) in full models of mosaic attenuation.
4. Discussion
In this paper, we investigated potential clinical relevance of variograms-based feature engineering pipelines for quantification of chest CT imaging and phenotyping in the study of sarcoidosis. Factors of interest included feature robustness, consistency of identified phenotypes across approaches, and strength of association between identified phenotypes and clinical measures of disease.
Consistent with the literature, computed variogram-based features were not robust to the decision to register images to a template (frequently ICC ). If the decision on registration was fixed, feature robustness was typically excellent with respect to other decisions (ICC). Even in absence of robust feature computation, however, resulting clusters from each of 48 clustering analyses were surprisingly consistent (typical Cramér’s V ). Mild but statistically significant associations between features and scanner model used in image acquisition were found for all 24 unharmonized datasets, especially empirical and exponential datasets, which persisted through to associations between phenotypes and scanner model. Associations between features and scanner were mild at worst, unlike in radiomics (Mackin 2015, Rizzo et al 2018); see a comparison of variogram- and radiomics-based (Carlson 2024) analyses in the GRADS cohort in the supplement. Registering images before feature extraction appeared to reduce feature and phenotype association with scanner model.
Presence and strength of disease signal were impressively consistent across all 48 approaches considered for processing images, engineering features, and phenotyping/clustering. Associations of variogram-based phenotypes with PFT were observed to be similarly strong compared to previously identified associations of radiomics-based phenotypes with PFT in the GRADS cohort (Carlson 2024); see a comparison of variogram- and radiomics-based analyses in the supplement. Results were also consistent with similar radiomics-based studies of PFT and VAS in lung diseases such as chronic obstructive pulmonary disease (COPD) and interstitial lung diseases (Occhipinti 2019, Schniering 2022). Associations of variogram-based phenotypes with visual assessments of architectural distortion, conglomerate masses, fibrotic abnormalities, and traction bronchiectasis (optimistic AUC ≈ 0.9) establish strong potential relevance of variogram-based approaches in future study of sarcoidosis and quantitative biomarker development. Lowest strength associations between clusters and measures of disease were observed for lymphadenopathy measures (optimistic AUC between 0.65 and 0.75), though we note that lymph nodes were masked out of images for all 48 pipelines.
Consistency in identified clusters and disease signal across approaches suggested that use of unharmonized variogram data from unregistered images, consistent with a simple, expedient, and generalizable processing pipeline, is reasonable for future study of sarcoidosis. Further, the low-dimension variogram-based feature sets considered here are more interpretable and apparently much less influenced by scanner model than radiomics while also showing strong association with disease features. This work suggests variogram-based features are a promising alternative to classic radiomics in sarcoidosis.
4.1. Limitations
The GRADS study enrolled subjects representing clinically pre-defined phenotypes, and so analyses of heterogeneity in a subcohort may not be generalizable to clinical populations. Furthermore, CT scans obtained for the GRADS study using a standardized protocol were more consistent in image acquisition and reconstruction than is typical for clinical populations. Variation in image acquisition protocol could not be assessed. Future investigations should more thoroughly assess pipeline robustness to variation in image acquisition and reconstruction, as well as the highly related factor of image resolution.
5. Conclusion
All feature engineering pipelines and clustering approaches considered produced similar measures of heterogeneity and strong association with sarcoidosis disease signal as measured by PFT and VAS, clearly establishing potential for clinical relevance of variogram-based approaches in future research. While clusters produced from unregistered data were typically more significantly associated with scanner model than those produced from registered data, this association was mild in strength and did not appear to impede detection of disease related signal in subsequent analyses. As such, optimality of pipelines and approaches among those considered might reasonably be selected on other bases, such as simplicity and expediency of pipeline, dimensionality of data produced, robustness of feature computation, and appropriateness of pipelines for clinical cohorts having more variability in CT image metadata such as original reconstructed resolution, convolution kernel used in reconstruction, and retention of axial slices.
In particular, future investigation of variogram-based features in clinical sarcoidosis cohorts might reasonably consider unharmonized, unregistered Matérn data without accounting for drift, corresponding with a balance of simplicity in implementation and robustness of engineered features. In principle, this harmonization- and registration-free pipeline should also be more readily applicable to both research and clinical cohorts without substantial modification. Building and applying a template is typically a time-consuming cohort–specific process with the potential to impede generalizability while harmonization directly impedes generalization to new contexts.
Registered image data do appear slightly more appropriate for establishing clinically relevant phenotypes through clustering as registration seems to reduce association of engineered features and clustering-based phenotypes with scanner model; however, care would need to be taken to ensure templates and registration process were appropriate for application to diverse clinical populations of sarcoidosis patients in support of generalizable research.
Acknowledgments
This work was supported by the National Institutes of Health under Grants R01 HL114587, R01 HL142049, R01 HL152735, and T32 HL007085.
Data from the GRADS study was supported under Grants U01 HL112707, U01 HL112707, U01 HL112694, U01 HL112695, U01 HL112696, U01 HL112702, U01 HL112708, U01 HL112711, U01 HL112712.
This study was reviewed and approved by the National Jewish Health and BRANY Institutional Review Boards (HS3211).
Data availability statement
The data cannot be made publicly available upon publication due to legal restrictions preventing unrestricted public distribution. The data that support the findings of this study are available upon reasonable request from the authors.
Conflict of interest
L A M received grants from the National Institute of Health (R01HL140357, R01HL142049, and R01HL136681), Ann Theodore Foundation, the FSR, Mallinckrodt Pharmaceuticals, and the University of Cincinnati (Mallinckrodt Pharmaceuticals Foundation Grant) and serves on the Scientific Advisory Board for FSR, and Boeringer Ingelheim. R Y was a speaker at Boehringer Ingelhein and Omnicurus CME experts, and is a consultant with IMBIO. W L L, T E F, D A L, J R, A C H, S L, M M M, B Q B, K J C, H J H, and N E C have nothing to declare.
References
- Au R C, Tan W C, Bourbeau J, Hogg J C, Kirby M. Impact of image pre-processing methods on computed tomography radiomics features in chronic obstructive pulmonary disease. Phys. Med. Biol. 2021;66:245015. doi: 10.1088/1361-6560/ac3eac. [DOI] [PubMed] [Google Scholar]
- Bachmaier M, Backes M. Variogram or semivariogram? Variance or semivariance? Allan variance or introducing a new term? Math. Geosci. 2011;43:735–40. doi: 10.1007/s11004-011-9348-3. [DOI] [Google Scholar]
- Banerjee S, Carlin B P, Gelfand A E. Hierarchical Modeling and Analysis for Spatial Data. CRC Press; 2014. [Google Scholar]
- Bankier A A, et al. Fleischner society: glossary of terms for thoracic imaging. Radiology. 2024;310:e232558. doi: 10.1148/radiol.232558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baughman R P, Culver D A, Judson M A. A concise review of pulmonary sarcoidosis. Am. J. Resp. Crit. Care Med. 2011;183:573–81. doi: 10.1164/rccm.201006-0865CI. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baughman R P, Lower E E. Treatment of sarcoidosis. Clin. Rev. Aller. Immunol. 2015;49:79–92. doi: 10.1007/s12016-015-8492-9. [DOI] [PubMed] [Google Scholar]
- Benn B S, et al. Chest computed tomography provides more information than chest x-ray alone in determining extent of physiologic impairment in pulmonary sarcoidosis. Chest. 2024;166:1093–107. doi: 10.1016/j.chest.2024.04.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bergsma W. A bias-correction for Cramér’s V and Tschuprow’s T. J. Korean Stat. Soc. 2013;42:323–8. doi: 10.1016/j.jkss.2012.10.002. [DOI] [Google Scholar]
- Carlson N E, et al. Radiomic profiling of lung CT in a cohort of sarcoidosis cases. MedRxiv. 2024. (available at: www.medrxiv.org/content/early/2024/03/05/2022.10.01.22280365)
- Carr J R, De Miranda F P. The semivariogram in comparison to the co-occurrence matrix for classification of image texture. IEEE Trans. Geosci. Remote Sens. 1998;36:1945–52. doi: 10.1109/36.729366. [DOI] [Google Scholar]
- Celeux G, Govaert G. Gaussian parsimonious clustering models. Pattern Recognit. 1995;28:781–93. doi: 10.1016/0031-3203(94)00125-6. [DOI] [Google Scholar]
- Cressie N. Fitting variogram models by weighted least squares. J. Int. Assoc. Math. Geol. 1985;17:563–86. doi: 10.1007/BF01032109. [DOI] [Google Scholar]
- Dai X, Khorram S. The effects of image misregistration on the accuracy of remotely sensed change detection. IEEE Trans. Geosci. Remote Sens. 1998;36:1566–77. doi: 10.1109/36.718860. [DOI] [Google Scholar]
- Denzler S, et al. Impact of CT convolution kernel on robustness of radiomic features for different lung diseases and tissue types. Br. J. Radiol. 2021;94:20200947. doi: 10.1259/bjr.20200947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desai S R, et al. High-resolution CT phenotypes in pulmonary sarcoidosis: a multinational Delphi consensus study. Lancet Resp. Med. 2023;12:409–18. doi: 10.1016/S2213-2600(23)00267-9. [DOI] [PubMed] [Google Scholar]
- Diaz G, Zucca A, Setzu M D, Cappai C. Chromatin pattern by variogram analysis. Microsc. Res. Tech. 1997;39:305–11. doi: 10.1002/(SICI)1097-0029(19971101)39:33.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- Ericeira D R, Silva A C, De Paiva A C, Gattass M. Detection of masses based on asymmetric regions of digital bilateral mammograms using spatial description with variogram and cross-variogram functions. Comput. Biol. Med. 2013;43:987–99. doi: 10.1016/j.compbiomed.2013.04.019. [DOI] [PubMed] [Google Scholar]
- Gamer M, Lemon J, Singh I F P. irr: various coefficients of interrater reliability and agreement. 2019. R package version 0.84.1. (available at: https://CRAN.R-project.org/package=irr)
- Goodin D G, Gao J, Henebry G M. The effect of solar illumination angle and sensor view angle on observed patterns of spatial structure in tallgrass prairie. IEEE Trans. Geosci. Remote Sens. 2004;42:154–65. doi: 10.1109/TGRS.2003.815674. [DOI] [Google Scholar]
- Gough J, Kent J, O’Higgins P, Ellison L. Variogram methods for the analysis of bony trabecular shadows in plain radiographs. Int. J. Bio-Med. Comput. 1994;35:141–53. doi: 10.1016/0020-7101(94)90063-9. [DOI] [PubMed] [Google Scholar]
- Graham B L, Brusasco V, Burgos F, Cooper B G, Jensen R, Kendrick A, MacIntyre N R, Thompson B R, Wanger J. ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Resp. J. 2017;49:2017. doi: 10.1183/13993003.00016-2016. [DOI] [PubMed] [Google Scholar]
- Gräler B, Pebesma E, Heuvelink G. Spatio-temporal interpolation using gstat. The R Journal. 2016;8:204–18. doi: 10.32614/RJ-2016-014. [DOI] [Google Scholar]
- Hallac D, Vare S, Boyd S, Leskovec J. Toeplitz inverse covariance-based clustering of multivariate time series data. Proc. 23rd ACM SIGKDD Int. Conf. on Knowledge Discovery and Data Mining; 2017. pp. 215–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haralick R M, Shanmugam K, Dinstein I H. Textural features for image classification. IEEE Trans. Syst. Man Cybern. 1973;SMC-3:610–21. doi: 10.1109/TSMC.1973.4309314. [DOI] [Google Scholar]
- Hena K M. Sarcoidosis epidemiology: race matters. Front. Immunol. 2020;11:537382. doi: 10.3389/fimmu.2020.537382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ieva F, et al. Covariance-based clustering in multivariate and functional data analysis. J. Mach. Learn. Res. 2016;17:1–21. (available at: www.jmlr.org/papers/v17/15-568.html) [Google Scholar]
- Jacob R E, Carson J P. Automated measurement of heterogeneity in CT images of healthy and diseased rat lungs using variogram analysis of an octree decomposition. BMC Med. Imaging. 2014;14:1–11. doi: 10.1186/1471-2342-14-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacob R E, Murphy M K, Creim J A, Carson J P. Detecting radiation-induced injury using rapid 3D variogram analysis of CT images of rat lungs. Acad. Radiol. 2013;20:1264–71. doi: 10.1016/j.acra.2013.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keil F, Oros-Peusquens A-M, Shah N J. Investigation of the spatial correlation in human white matter and the influence of age using 3-dimensional variography applied to mp-rage data. Neuroimage. 2012;63:1374–83. doi: 10.1016/j.neuroimage.2012.07.034. [DOI] [PubMed] [Google Scholar]
- Koo T K, Li M Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropract. Med. 2016;15:155–63. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koscik T R. ez.combat: Easy ComBat Harmonization. 2021. R package version 1.0.0. (available at: https://CRAN.R-project.org/package = ez.combat)
- Lambin P, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017;14:749–62. doi: 10.1038/nrclinonc.2017.141. [DOI] [PubMed] [Google Scholar]
- Lew D, Klang E, Soffer S, Morgenthau A S. Current applications of artificial intelligence in sarcoidosis. Lung. 2023;201:445–54. doi: 10.1007/s00408-023-00641-7. [DOI] [PubMed] [Google Scholar]
- Lin N W, et al. Clinical phenotyping in sarcoidosis using cluster analysis. Resp. Res. 2022;23:88. doi: 10.1186/s12931-022-01993-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovinfosse P, et al. Distinction of lymphoma from sarcoidosis on 18f-FDG PET/CT: Evaluation of radiomics-feature–guided machine learning versus human reader performance. J. Nucl. Med. 2022;63:1933–40. doi: 10.2967/jnumed.121.263598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo J, Ma G, Haouchine N, Xu Z, Wang Y, Kapur T, Ning L, Wells W M, Frisken S. On the dataset quality control for image registration evaluation. In: Wang L, Dou Q, Fletcher P T, Speidel S, Li S, editors. Medical Image Computing and Computer Assisted Intervention – MICCAI 2022; Springer; 2022. pp. 36–45. [Google Scholar]
- Lv W, Yuan Q, Wang Q, Ma J, Jiang J, Yang W, Feng Q, Chen W, Rahmim A, Lu L. Robustness versus disease differentiation when varying parameter settings in radiomics features: application to nasopharyngeal pet/ct. Eur. Radiol. 2018;28:3245–54. doi: 10.1007/s00330-018-5343-0. [DOI] [PubMed] [Google Scholar]
- Mackin D, et al. Measuring computed tomography scanner variability of radiomics features. Investigative Radiol. 2015;50:757–65. doi: 10.1097/RLI.0000000000000180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marbac M, Sedki M. Variable selection for model-based clustering using the integrated complete-data likelihood. Stat. Comput. 2017;27:1049–63. doi: 10.1007/s11222-016-9670-1. [DOI] [Google Scholar]
- Marbac M, Sedki M, Patin T. Variable selection for mixed data clustering: application in human population genomics. J. Class. 2020;37:124–42. doi: 10.1007/s00357-018-9301-y. [DOI] [Google Scholar]
- Marquez R G, Scheffler A W, Guhaniyogi R, Dickinson A, DiStefano C, Jeste S. A bayesian covariance based clustering for high dimensional tensors. 2021. (available at: https://tr.soe.ucsc.edu/research/technical-reports/UCSC-SOE-22-07)
- Moller D R, et al. Rationale and design of the genomic research in alpha-1 antitrypsin deficiency and sarcoidosis (GRADS) study. sarcoidosis protocol. Ann. Am. Thoracic Soc. 2015;12:1561–71. doi: 10.1513/AnnalsATS.201503-172OT. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muniandy S, Stanslas J. Modelling of chromatin morphologies in breast cancer cells undergoing apoptosis using generalized cauchy field. Comput. Med. Imaging Graph. 2008;32:631–7. doi: 10.1016/j.compmedimag.2008.07.003. [DOI] [PubMed] [Google Scholar]
- Occhipinti M, et al. Spirometric assessment of emphysema presence and severity as measured by quantitative CT and CT-based radiomics in COPD. Resp. Res. 2019;20:1–11. doi: 10.1186/s12931-019-1049-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Core Team R: a language and environment for statistical computing. 2020. R Foundation for Statistical Computing, Vienna, Austria. (available at: www.R-project.org/)
- Rizzo S, Botta F, Raimondi S, Origgi D, Fanciullo C, Morganti A G, Bellomi M. Radiomics: the facts and the challenges of image analysis. Eur. Radiol. Exp. 2018;2:1–8. doi: 10.1186/s41747-018-0068-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubio-Rivas M, Corbella X. Clinical phenotypes and prediction of chronicity in sarcoidosis using cluster analysis in a prospective cohort of 694 patients. Eur. J. Inter. Med. 2020;77:59–65. doi: 10.1016/j.ejim.2020.04.024. [DOI] [PubMed] [Google Scholar]
- Ryan S M, Fingerlin T E, Mroz M, Barkes B, Hamzeh N, Maier L A, Carlson N E. Radiomic measures from chest high-resolution computed tomography associated with lung function in sarcoidosis. Eur. Resp. J. 2019;54:1900371. doi: 10.1183/13993003.00371-2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan S M, Vestal B, Maier L A, Carlson N E, Muschelli J. Template creation for high-resolution computed tomography scans of the lung in R software. Acad. Radiol. 2020;27:e204–15. doi: 10.1016/j.acra.2019.10.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schniering J, et al. Computed tomography-based radiomics decodes prognostic and molecular differences in interstitial lung disease related to systemic sclerosis. Eur. Resp. J. 2022;59:2004503. doi: 10.1183/13993003.04503-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schupp J C, et al. Phenotypes of organ involvement in sarcoidosis. Eur. Resp. J. 2018;51:1700991. doi: 10.1183/13993003.00991-2017. [DOI] [PubMed] [Google Scholar]
- Sharp M, Eakin M N, Drent M. Socioeconomic determinants and disparities in sarcoidosis. Curr. Opin. Pulmonary Med. 2020;26:568–73. doi: 10.1097/MCP.0000000000000704. [DOI] [PubMed] [Google Scholar]
- Shiri I, Hajianfar G, Sohrabi A, Abdollahi H, Shayesteh S P, Geramifar P, Zaidi H, Oveisi M, Rahmim A. Repeatability of radiomic features in magnetic resonance imaging of glioblastoma: Test–retest and image registration analyses. Med. Phys. 2020;47:4265–80. doi: 10.1002/mp.14368. [DOI] [PubMed] [Google Scholar]
- Silva A C, Carvalho P C P, Gattass M. Analysis of spatial variability using geostatistical functions for diagnosis of lung nodule in computerized tomography images. Pattern Anal. Appl. 2004;7:227–34. doi: 10.1007/s10044-004-0219-0. [DOI] [Google Scholar]
- Van den Heuvel D, De Jong P, Zanen P, Van Es H, Van Heesewijk J, Spee M, Grutters J. Chest computed tomography-based scoring of thoracic sarcoidosis: inter-rater reliability of CT abnormalities. Eur. Radiol. 2015;25:2558–66. doi: 10.1007/s00330-015-3685-4. [DOI] [PubMed] [Google Scholar]
- Van Timmeren J E, Cester D, Tanadini-Lang S, Alkadhi H, Baessler B. Radiomics in medical imaging-“how-to” guide and critical reflection. Insights into Imaging. 2020;11:1–16. doi: 10.1186/s13244-020-00887-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vukmirovic M, et al. Transcriptomics of bronchoalveolar lavage cells identifies new molecular endotypes of sarcoidosis. Eur. Resp. J. 2021;58:2002950. doi: 10.1183/13993003.02950-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Y, et al. Chest high-resolution computed tomography can make higher accurate stages for thoracic sarcoidosis than x-ray. BMC Pulmonary Med. 2022;22:146. doi: 10.1186/s12890-022-01942-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou Y, et al. The impact of demographic disparities in the presentation of sarcoidosis: a multicenter prospective study. Resp. Med. 2021;187:106564. doi: 10.1016/j.rmed.2021.106564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zwanenburg A, et al. The image biomarker standardization initiative: standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology. 2020;295:328–38. doi: 10.1148/radiol.2020191145. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data cannot be made publicly available upon publication due to legal restrictions preventing unrestricted public distribution. The data that support the findings of this study are available upon reasonable request from the authors.