

Abstract
Objective: To evaluate the impact and prognosis of a multidisciplinary discharge preparation service model for patients with chronic heart failure. Methods: A total of 100 patients with chronic heart failure who visited the Wuhan Asia Heart Hospital from January 2022 to September 2023 were included. The patients were divided into an experimental group, receiving a multidisciplinary discharge preparation service, and a control group, receiving conventional treatment. Primary outcomes included New York Heart Association (NYHA) Functional Classification, Left Ventricular Ejection Fraction (LVEF), Serum Uric Acid (SUA) levels, Creatinine Clearance Rate (Ccr), Serum Potassium levels, cardiac death count, and the frequency of heart failure-related hospitalizations. Comparisons between the two groups were conducted to evaluate the effectiveness of the multidisciplinary service model. Results: After 3 months of treatment, both groups showed significant reductions in NYHA scores, with notable differences before and after treatment (t=-2.631, P=0.025). LVEF levels decreased in both groups following 3 months of discharge preparation service (t=-4.741, P=0.003). The experimental group exhibited greater improvements in SUA and Ccr indices. The highest serum potassium level reached approximately 4.68 mmol/L when LVEF > 50%. In the experimental group, there was 1 case of cardiac death and 6 cases of heart failure-related readmission, while the control group had 2 cases of cardiac death and 8 cases of heart failure-related readmission. There were no significant differences between the two groups in terms of hypoglycemia, urinary tract infections, and gastrointestinal adverse reactions (all P > 0.05). Conclusion: The multidisciplinary discharge preparation service model significantly improves the clinical condition of patients with chronic heart failure, reducing the risk of heart failure-related deaths and rehospitalizations.
Keywords: Multidisciplinary involvement, discharge preparation, chronic heart failure, cardiac function
Introduction
In the 21st century, global public health faces significant challenges, with the management and treatment of chronic heart failure (CHF) being particularly prominent. CHF, a prevalent cardiovascular disease, has become a global public health issue [13,23]. It often results in a progressive decline in heart function, adversely affecting patients’ life expectancy [11,12,22,31]. CHF is a complex clinical syndrome characterized by structural or functional cardiac abnormalities, leading to elevated intracardiac pressure and reduced cardiac output. The main symptoms include dyspnea, fatigue, and fluid retention (pulmonary congestion, systemic congestion, and peripheral edema), representing the final stage and primary cause of death for most cardiovascular diseases [2,30]. The high incidence, mortality rate, and poor prognosis of CHF highlight the urgent need for effective clinical management [20]. The incidence of CHF increases with age, ranging from 1% at age 55 to 10% at age 70, with a continuously rising prevalence [20].
Current management strategies for CHF include pharmacological treatment, lifestyle modifications, and surgical interventions. Commonly used medications include diuretics, β-blockers, ACE inhibitors, and angiotensin receptor blockers. Additionally, cardiac rehabilitation and regular follow-up are essential components of patient care, aiming to prevent disease progression and reduce hospitalization rates [2,10]. Despite these interventions, CHF remains a significant challenge for healthcare systems due to its complex nature and the need for individualized care. This necessitates the development of innovative models that can effectively integrate various aspects of patient management.
Discharge Preparation Services (DPS), a key component of Transitional Care, provide patients with comprehensive and continuous care through identification, evaluation, planning, implementation, and assessment. DPS aims to evaluate patient needs and formulate personalized discharge preparation plans based on specific conditions, patient characteristics, and environmental factors, playing a crucial role in patient management [21,34]. Implementing DPS can ensure continuity of care for elderly CHF patients across different living environments, enhance discharge readiness, shorten hospital stays, and reduce readmission rates [1]. Previous studies have shown that multidisciplinary approaches can improve the discharge process and quality of life, making it a promising treatment model [8,24,33]. However, there is a lack of in-depth analysis in the academic community, and existing DPS models often have limitations, such as limited participant engagement, insufficient personalization, and inadequate consideration of the comprehensive needs of CHF patients.
In response to these limitations, there is an urgent need to develop and evaluate new DPS models. This study introduces a novel multidisciplinary DPS model involving a team of professionals from various disciplines collaboratively managing and treating CHF patients. The study aims to explore the application and prognosis of this multidisciplinary DPS model for patients with CHF.
Data and methods
General information
This retrospective study was conducted at Wuhan Asia Heart Hospital from January 2022 to September 2023, involving 100 patients diagnosed with CHF, with 50 patients in each of the experimental and control groups. The inclusion criteria were as follows: (1) Age between 65 and 80 years; (2) Left Ventricular Ejection Fraction (LVEF) below 40%; (3) Heart function classified as Grade II to IV.
The exclusion criteria were: (1) Estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2; (2) Blood pressure below 90/60 mmHg; (3) Severe liver or kidney dysfunction; (4) Acute left heart failure, cardiogenic shock, malignant arrhythmias, high-grade atrioventricular block, or severe heart valve disease; (5) Presence of malignant tumors or autoimmune diseases (Figure 1).
Figure 1.

Flow chart of study. A total of 119 patients were enrolled in the study, with 100 patients ultimately completing the study, achieving a completion rate of 84.0%.
The experimental group received a multidisciplinary DPS involving physicians, nurses, nutritionists, and pharmacists, while the control group received standard DPS. The study was approved by the Medical Ethics Committee of Wuhan Asia Heart Hospital (2024-B036). The sample size was calculated using PASS® version 15.0, with a sample size of 47 being adequate given the 1.3% prevalence of chronic heart failure.
Research methodology
A total of 100 patients were enrolled, with 50 patients each in the experimental and control groups. During the discharge preparation period, the experimental group received a multidisciplinary DPS model, whereas the control group received conventional DPS. Baseline data were collected for both groups, including gender, age, heart function, NYHA classification, comorbidities, and use of heart failure medications. Relevant indicators were collected before and after DPS implementation, including heart function parameters, renal function markers, and NYHA classification. Key composite events during the study, such as readmission rates and cardiogenic deaths, were also recorded [4,32].
Post-discharge quality of life and health outcomes were compared between the two groups, focusing on readmission rates, mortality rates, improvement in heart failure symptoms, treatment adherence, and patient satisfaction levels. Additionally, adverse events during the service period, patient feedback on services, changes in post-discharge quality of life, and physical condition were also assessed. Through comparative analysis, this study aimed to evaluate the effectiveness and benefits of the multidisciplinary DPS model in patients with CHF.
Treatment protocol
Patients in the control group received standard DPS prior to discharge, which included medication guidance, lifestyle modification recommendations, disease monitoring, and treatment planning [5]. These steps aimed to help patients manage their condition effectively, promote recovery, and maintain their health after hospital discharge. Comprehensive guidance and advice enabled patients to understand the nature of their disease, enhance adherence to treatment plans, and reduce complications, thereby improving their quality of life.
The experimental group implemented a multidisciplinary collaborative DPS model [3,15,28], involving a team of specialized physicians, nurses, rehabilitation specialists, nutritionists, pharmacists, and community healthcare providers working together (Table 1). The multidisciplinary nursing team offered coordinated referral services for patients with CHF. The protocol included:
Table 1.
Multidisciplinary collaborative DPS model nursing measures
| Step | Treatment |
|---|---|
| Multidisciplinary Collaborative DPS Care: Involves specialized physicians, nursing staff, rehabilitation physicians, nutritionists, pharmacists, and community nursing personnel. | |
| Content | Specific Measures |
| Establishment of multidisciplinary team | 9 specialized physicians in heart failure |
| 8 heart failure specialized nurses | |
| 2 pharmacists | |
| 2 nutritionists | |
| 2 rehabilitation therapists | |
| 2 social workers | |
| Data Management | Establish data center Collect and record patient information |
| Care Plan | Initial Assessment: Conducted within 24 hours of admission - Multidisciplinary team assesses various needs and selects service recipients |
| Plan Development: Reassessment within 48 hours of admission and plan formulation - Discharge plan developed before discharge | |
| Dietary Management | Nutritionists create meal plans, Attending physician optimizes sodium intake, Nursing staff guide implementation |
| Exercise Management | Rehabilitation physicians develop exercise plans - Community nursing personnel provide exercise videos and guidance |
| Follow-up | 1. Weekly follow-up during the first month post-discharge |
| 2. Bi-weekly follow-up during the second month | |
| 3. Monthly follow-up during the third month | |
| 4. Monthly follow-up within three to six months post-discharge | |
Formation of Multidisciplinary Nursing Subgroups: The team, led by a manager who also served as the director of the heart failure center, consisted of 9 specialized physicians, 8 specialized nurses, 2 pharmacists, 2 nutritionists, 2 rehabilitation therapists, and 2 social workers. Each team member’s responsibilities were clearly defined, and work procedures were established. Treatment, follow-up, and review plans were developed by the specialized physicians, with nurses assisting in follow-up and health education. Pharmacists, nutritionists, rehabilitation therapists, and social workers contributed according to their respective expertise, coordinated by the team manager.
Establishment of a Data Management Center: A data management center was established to implement phased, continuous care plans. Specialized nursing staff collected patient information on CHF, which was meticulously recorded in the national heart failure center’s database to support epidemiological research.
Initial Assessment Upon Admission: Upon admission, an initial assessment was conducted to identify patients at risk of delayed discharge or those requiring continuous care after discharge. Identified candidates underwent a comprehensive assessment within 24-72 hours by senior responsibility nurses or specialized nurses. A phased implementation plan was devised as follows:
Phase One: Within 24 hours of admission, responsibility nurses conducted the initial assessment. The multidisciplinary team evaluated socioeconomic, cultural, living conditions, marital status, lifestyle behaviors, medical and nursing needs (physical function, mental/psychological status, cognitive ability, daily living skills, self-care ability), family support, and community resources available upon discharge. Based on these assessments, high-risk patients were identified, and specific risk factors, symptoms, and gaps in discharge preparation were noted.
Phase Two: Within 48 hours of admission, the selected service recipients were reassessed. Implementation plans were developed based on patient profiles. Post-discharge, if patients were involved in home rehabilitation, community health service centers assisted with rehabilitation. If patients resided in rehabilitation institutions, direct contact was made with the respective institutions to ensure continuity of care. Bed management doctors formulated post-hospital rehabilitation plans and evaluated the need for special medical equipment, such as home respiratory devices or suction apparatus. Communication with patients and their families ensured a clear understanding of post-discharge nursing needs and the fulfillment of any special requirements. Three days before and on the day of discharge, a comprehensive discharge plan was formulated, including the distribution of heart failure health guidance brochures covering diet, exercise, and individualized treatment plans. Patients received on-site education regarding the disease, symptoms, treatment, and prognosis. Nursing staff instructed patients on how to accurately measure their weight, heart rate, and blood pressure, and follow-up actions were advised for any abnormalities.
Follow-Up Care: After discharge, patients were primarily followed up through telephone consultations or home visits over a three-month period. The follow-up schedule included weekly visits during the first month, bi-weekly visits in the second month, and monthly visits in the third month. The primary objectives were to assess medication adherence, dietary compliance, and rehabilitation exercise participation, and to evaluate potential safety and health issues. Nurses reported patient conditions to the multidisciplinary team for evaluation and adjustments in treatment, nutrition, and nursing care. Adjustments were communicated to lower-level healthcare institutions and patients, ensuring collaboration with community personnel for the effective implementation of patient rehabilitation measures. Between three and six months post-discharge, patients were scheduled for monthly follow-ups to assess cardiac function, treatment adherence, and self-management capabilities. Stable patients were invited to participate in lectures and health education sessions.
Dietary Management: Nutritionists designed meal plans based on the patient’s dietary preferences. The attending physician further refined daily sodium intake to optimize the diet plan. Nursing staff communicated the finalized diet plan to the patients and provided guidance for its proper implementation.
Exercise Management: Rehabilitation physicians assessed the patient’s exercise tolerance and developed individualized daily exercise plans, specifying types, duration, and intensity of exercises. Community nursing personnel provided rehabilitation exercise videos and detailed instructions on correct techniques.
Both groups received standard treatment for CHF, which included a low-salt, low-fat diet and comprehensive therapies such as ventricular rate control, cardiac remodeling inhibition, and diuretic therapy. This study aimed to evaluate the effectiveness of a multidisciplinary DPS model for patients with CHF by comparing readmission rates, quality of life, and disease control indicators between the two groups. Feedback, suggestions, and insights from the experimental group regarding the multidisciplinary DPS were collected and analyzed to identify advantages and areas for improvement.
Tests and examination
Cardiac Function Indicators: Changes in heart function before and after receiving the services were evaluated using indicators such as Left Ventricular Ejection Fraction (LVEF), Left Ventricular End-Diastolic Diameter (LVEDD), and the ratio of early mitral inflow velocity to mitral annular early diastolic velocity (E/e).
Renal Function Indicators: Given the frequent occurrence of renal dysfunction in CHF patients, 5 ml of fasting venous blood was collected, and serum creatinine (Scr), serum uric acid (SUA), and creatinine clearance rate (Ccr) were measured using the Beckman A580 automatic biochemical analyzer [25,29].
Readmission Rate: The readmission rate due to acute exacerbation of heart failure was calculated six months after implementing the DPS model, based on follow-up visits and medical record reviews. The readmission rate was calculated as follows: (number of readmissions due to acute heart failure exacerbation/total number of cases) × 100%.
Quality of Life: The quality of life in both groups after receiving the services was assessed using the Minnesota Living with Heart Failure Questionnaire (MLHFQ) [7]. The MLHFQ consists of 21 items that measure quality of life across three domains: physical, emotional, and other domains. Each item is scored on a scale of 0 to 5, with a total score ranging from 0 to 105. Higher scores indicate a poorer quality of life.
Patient Satisfaction: Patient satisfaction and feedback were collected through questionnaire surveys and follow-up interviews.
Adverse Events: Any adverse events during the multidisciplinary DPS, including changes in health status and dissatisfaction with the service in the experimental group, were recorded and analyzed.
Observational indicators
The study compared and analyzed changes in cardiac and renal function parameters, readmission rates, and quality of life between the experimental and control groups before and after receiving the services. Adverse events, including changes in health status and dissatisfaction with the service during and after discharge, were also recorded and statistically analyzed for both groups. Quality of life was the primary outcome, while changes in cardiac and renal function parameters, readmission rates, and adverse events were secondary outcomes. All comparisons and analyses focused on the patients’ overall health outcomes and satisfaction.
Statistical methods
To ensure data accuracy and reliability, statistical analysis was performed using SPSS version 22.0, and figures were generated using Prism version 8.0.2. Means and standard deviations (SD) were used to describe the characteristics of the measurement data, and t-tests were employed for comparison. Categorical data were presented as percentages, and the Chi-square test was used. All test results were considered statistically significant at P < 0.05.
Results
Comparison of baseline characteristics
In the experimental group, there were 30 males and 20 females, with an average age of 70.2±3.1 years. The control group comprised 31 males and 19 females, with an average age of 70.5±2.8 years. There was no significant difference in age and gender distribution between the two groups (P > 0.05). Similarly, there were no significant differences in systolic blood pressure, diastolic blood pressure, or heart rate between the two groups. See Table 2.
Table 2.
Comparison results of general information
| Variables | Experiment group (n=50) | Control group (n=50) | P |
|---|---|---|---|
| Sex (%) | 0.856 | ||
| Male | 30 (60) | 31 (62) | |
| Female | 20 (40) | 19 (38) | |
| Age (years) | 70.2±3.1 | 70.5±2.8 | 0.727 |
| Systolic BP (mmHg) | 125±13 | 126±12 | 0.874 |
| Diastolic BP (mmHg) | 80±9 | 82±8 | 0.612 |
| Average Heart Rate (beats/min) | 78±11 | 79±10 | 0.733 |
| Renal Function Index | / | ||
| Scr (μmol/L) | 79.6±4.6 | 76.9±4.3 | 0.074 |
| SUA (μmol/L) | 453.5±83.5 | 463.2±68.7 | 0.063 |
| Ccr (mL/min) | 39.5±4.8 | 38.3±4.6 | 0.086 |
| Cardiac Function Index (LVEF, LVEDD, E/e) | / | ||
| LVEF (%) | 32.9±2.5 | 35.9±1.9 | 0.051 |
| LVEDD (mm) | 59.6±2.4 | 59.0±3.0 | 0.083 |
| E/e | 16.3±1.6 | 15.8±1.0 | 0.071 |
| NYHA Class (%) | 0.891 | ||
| II | 25 (50) | 26 (52) | |
| III | 20 (40) | 19 (38) | |
| IV | 5 (10) | 5 (10) | |
| Comorbidities (%) | 0.849 | ||
| Hypertension | 45 | 47 | |
| Diabetes | 30 | 28 | |
| Medications for Heart Failure (n/%) | 0.882 | ||
| ACEI/ARB | 30 (60) | 31 (62) | |
| β-blockers | 20 (40) | 19 (38) | |
| Diuretics | 45 (90) | 46 (92) | |
| Cardiac glycosides | 5 (10) | 4 (8) |
Note: LVEF: Left Ventricular Ejection Fraction; LVEDD: Left Ventricular End-Diastolic Diameter; NYHA: New York Heart Association; Scr: Serum creatinine; SUA: Serum uric acid; Ccr: Creatinine clearance rate; ACEI/ARB: Angiotensin converting enzyme inhibitors/Angiotensin receptor antagonist.
In the experimental group, 25 patients were classified as NYHA Class II, 20 as NYHA Class III, and 5 as NYHA Class IV. In the control group, 26 patients were NYHA Class II, 19 were NYHA Class III, and 5 were NYHA Class IV. Regarding comorbidities, 46% of the experimental group had hypertension, and 30% had diabetes, while in the control group, 44% had hypertension and 28% had diabetes. There was no significant difference in the severity of disease between the two groups, indicating comparability.
In terms of medication use, 30 patients in the experimental group were on ACEI/ARB therapy, 20 were on β-blockers, 45 were on diuretics, and 5 were on cardiac glycosides. In the control group, 32 patients were on ACEI/ARB therapy, 19 were on β-blockers, 46 were on diuretics, and 4 were on cardiac glycosides. There was no significant difference in baseline drug treatment between the two groups (P > 0.05).
Comparison of heart failure treatment results
The pre- and post-treatment outcomes for heart failure management in both groups are illustrated in Figure 2. As shown in Figure 1, there was no significant difference in NYHA classification between the experimental group and control group before treatment (t=-4.285, P=0.053). After 3 months of treatment, both groups exhibited a significant reduction in NYHA scores. The changes in NYHA scores were statistically significant in both the experimental and control groups (t=-3.142, P=0.023). There was no significant difference in baseline weight between the experimental and control groups before treatment. After 3 months of treatment, no statistically significant difference in weight change was observed within each group (P > 0.05), nor was there a significant difference in weight change between the experimental and control groups (P > 0.05).
Figure 2.

Comparison of heart failure management outcomes between the two groups. A: Changes in patient New York Heart Association (NYHA) levels before and after treatment. B: Changes in patient weights before and after treatment.
Comparison of cardiac function indicators before and after DPS
The comparison of cardiac function indicators before and after DPS between the two groups is presented in Table 3. Prior to the implementation of the DPS model, there were no statistically significant differences in BNP, LVEF, LVEDD, and E/e levels between the two groups. However, after 3 months of DPS, significant improvements were observed within both groups. Inter-group comparison demonstrated significant differences in BNP (P=0.021), LVEF (P=0.003), LVEDD (P=0.012), and E/e (P=0.011), indicating that the DPS model had a notable effect on these cardiac function parameters.
Table 3.
Comparison of cardiac function indicators before and after discharge preparation services
| Cardiac function indicators | Before | After | ||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Experiment group | Control group | t | P | Experiment group | Control group | t | P | |
| BNP (Pg/ml) | 1135±364 | 1068±264 | -2.114 | 0.062 | 454±161a | 695±136b | -7.082 | 0.021 |
| LVEF (%) | 32.9±2.5 | 35.9±1.9 | -3.248 | 0.051 | 39.8±2.8a | 36.5±1.8b | -4.729 | 0.003 |
| LVEDD (mm) | 59.6±2.4 | 59.0±3.0 | -3.134 | 0.083 | 53.2±2.2a | 55.9±2.5b | -4.335 | 0.012 |
| E/e | 16.3±1.6 | 15.8±1.0 | -3.627 | 0.071 | 10.6±1.6a | 12.7±1.8b | -5.472 | 0.011 |
the statistical comparison before and after treatment within the experimental group (P < 0.05);
the statistical comparison before and after treatment within the control group (P < 0.05).
LVEF: Left Ventricular Ejection Fraction; LVEDD: Left Ventricular End-Diastolic Diameter.
Comparison of renal function
The comparison of renal function indicators between the two groups before and after the implementation of the DPS model is shown in Table 4. Prior to DPS implementation, there were no statistically significant differences in Scr levels within or between the groups (P > 0.05). Similarly, there were no significant differences in SUA and Ccr levels between the two groups. After 3 months of DPS, no statistically significant difference in SUA levels was observed within the control group (P=0.054), while the experimental group showed a significant improvement in SUA levels (P=0.043). Significant changes were observed in Ccr levels between the two groups (P < 0.05). The inter-group comparison indicated that SUA and Ccr levels in the experimental group were significantly lower than those in the control group, with statistical significance (P < 0.05).
Table 4.
Comparison of renal function indicators before and after discharge preparation services
| Renal function indicators | Before | After | ||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Experiment group | Control group | t | P | Experiment group | Control group | t | P | |
| Scr (μmol/L) | 79.6±4.6 | 76.9±4.3 | 0.08 | 0.074 | 76.7±4.6 | 79.6±5.3 | 0.07 | 0.07 |
| SUA (μmol/L) | 453.5±83.5 | 463.2±68.7 | 0.07 | 0.063 | 371.6±72.1a | 452.1±64.8 | 0.035 | 0.035 |
| Ccr (mL/min) | 39.5±4.8 | 38.3±4.6 | 0.07 | 0.086 | 59.1±4.7a | 49.4±4.6b | 0.056 | 0.006 |
the statistical comparison before and after treatment within the experimental group (P < 0.05);
the statistical comparison before and after treatment within the control group (P < 0.05).
Scr: serum creatinine; SUA: serum uric acid; Ccr: creatinine clearance rate.
Figure 3 illustrates the specific changes in renal function during the DPS period for both groups. While Scr levels remained stable in both groups, the experimental group showed greater improvement in SUA and Ccr indicators, suggesting better recovery of renal function.
Figure 3.

Comparison of changes in renal function during discharge preparation services. A: Changes in Scr indicators before and after treatment for patients. B: Changes in SUA indicators of patients before and after treatment. C: Changes in SUA indicators of patients before and after treatment.
Comparison of blood potassium levels and its correlation
The correlation analysis of the multidisciplinary DPS model in patients with CHF is shown in Table 5. After 3 months of DPS, blood potassium levels decreased in both groups. A significant difference in blood potassium levels was observed between the two groups at NYHA Class III and IV before and after the service period (P=0.023).
Table 5.
Comparison of changes in blood potassium levels in the two groups
| Discharge Preparation service stage | After | t | P | |
|---|---|---|---|---|
|
| ||||
| Experiment group | Control group | |||
| Level II | 4.17±0.13 | 4.20±0.21 | -0.677 | 0.500 |
| Level III | 3.84±0.52 | 4.21±0.26 | -2.642 | 0.023 |
| Level IV | 3.25±0.36 | 4.31±0.38 | -3.779 | 0.011 |
Figure 4 illustrates the correlation between LVEF and blood potassium levels. When LVEF is less than 45%, the average blood potassium level is approximately 3.37 mmol/L. As LVEF increases, blood potassium levels also rise. For patients with LVEF greater than 50%, the highest blood potassium level can reach around 4.68 mmol/L. Statistical analysis reveals a significant difference in blood potassium levels between patients with LVEF greater than 50% and those with lower LVEF (P=0.006). This finding indicates a positive correlation between blood potassium levels and LVEF, with higher LVEF values associated with higher blood potassium levels.
Figure 4.
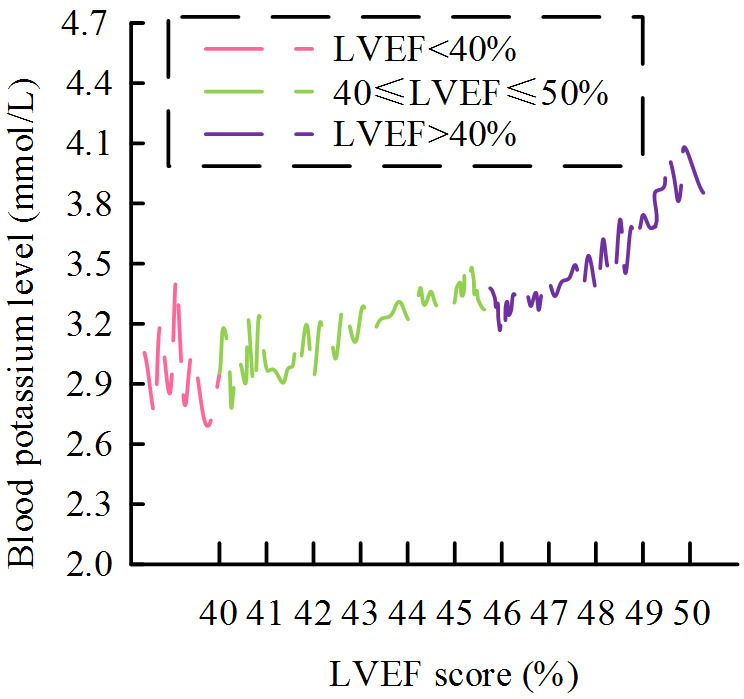
Correlation between Patient blood potassium levels and different left ventricular ejection fractions. LVEF: Left Ventricular Ejection Fraction.
Composite endpoint event results
Cardiogenic deaths and heart failure-related readmissions for both groups are shown in Figure 5. Figure 5A and 5B present the data on composite endpoint events for the experimental and control groups. In the experimental group, there was 1 case of cardiogenic death and 6 cases of heart failure readmission, while the control group had 2 cases of cardiogenic death and 8 cases of heart failure readmission. Statistical analysis indicated no significant difference in composite endpoint events between the experimental and control groups (P=0.08).
Figure 5.
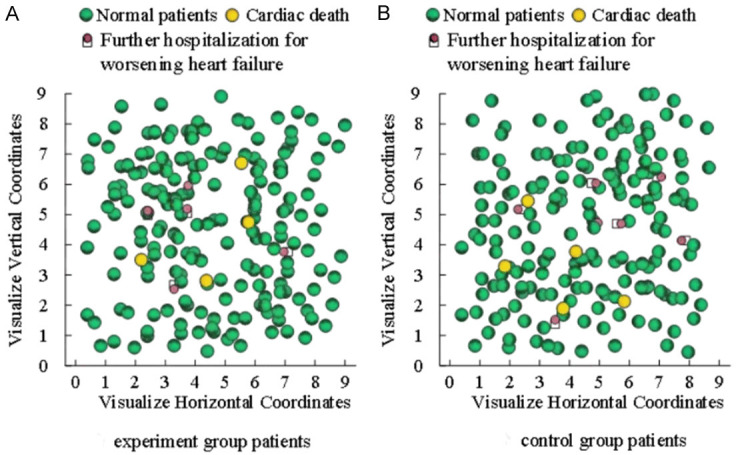
Cardiogenic death and worsening heart failure readmission in two groups of patients. A: Visualization of composite endpoint events for experimental group patients. B: Visualization of composite endpoint events in control group patients.
Comparison of adverse reactions
During the 3-month DPS period, patients underwent regular monitoring, including blood tests, urinalysis, stool analysis, and assessments of liver and kidney function. The incidence of adverse reactions in both groups is shown in Table 6. There were no statistically significant differences in the rates of hypoglycemia, urinary tract infections, or gastrointestinal adverse reactions between the experimental and control groups (P > 0.05).
Table 6.
Comparison of adverse reactions
| Types of adverse reactions | Experiment group (n=50) | Control group (n=50) | P |
|---|---|---|---|
| Hypoglycemic response n (%) | 2 (4.0) | 3 (6.0) | 0.684 |
| Urinary system infection n (%) | 3 (6.0) | 2 (4.0) | 0.687 |
| Gastrointestinal adverse reactions n (%) | 1 (2.0) | 2 (4.0) | 0.665 |
Comparison of clinical efficacy
Figure 6 illustrates the comparison of clinical efficacy between the experimental and control groups. Clinical outcomes were categorized as significant, effective, or ineffective. In the experimental group, 38.0% of patients experienced significant improvement, 48.0% showed effective outcomes, and 14.0% were classified as having no improvement. In the control group, 28.0% of patients experienced significant improvement, 52.0% showed effective outcomes, and 20.0% were classified as having no improvement. Statistical analysis revealed a significant difference in clinical efficacy between the two groups (P=0.001).
Figure 6.

Comparison of clinical efficacy between the two groups. *: P < 0.05.
Discussion
Despite advancements in medical technology that have greatly improved quality of life, the number of patients with CHF continues to rise. The multidisciplinary DPS model is considered one of the most advanced management approaches, integrating expertise from various disciplines to provide comprehensive and personalized medical care [17,26].
The implementation of multidisciplinary DPS for patients with CHF represents a novel medical service model aimed at improving clinical outcomes, enhancing quality of life, and reducing readmission rates. In this model, healthcare professionals develop personalized DPS through comprehensive evaluations to help patients better manage their condition and reduce the likelihood of readmission. Weber et al. suggested that the incidence of newly diagnosed heart failure is particularly high among patients with CHF, especially those with concomitant atrial fibrillation at the time of admission [35]. This underscores the need for more effective management strategies, as patients’ conditions may progress during treatment.
Consistent with these findings, the multidisciplinary collaborative treatment model adopted in this study aims to improve management outcomes for patients with CHF. Similarly, Jiang et al. investigated the effectiveness of nurse-led self-management programs for families managing heart failure and found that the program improved clinical outcomes [14]. This study’s multidisciplinary DPS model also aimed to enhance patient management through collaborative care approaches.
After three months of multidisciplinary DPS, patients with CHF showed significant reductions in their NYHA scores, indicating an improvement in their clinical status. These findings are in line with Koleck et al.’s research, which demonstrated that multidisciplinary DPS significantly improve clinical symptoms and quality of life for heart failure patients [18]. Furthermore, post-discharge services not only significantly alleviate symptoms but also enhance patients’ quality of life. With the use of mobile health applications and connected health devices, patients are better equipped to monitor their condition, thereby improving the effectiveness of self-management and self-care strategies.
In this study, patients demonstrated significant improvement in cardiac function indicators, such as BNP, LVEF, LVEDD, and E/e levels, following the implementation of multidisciplinary DPS, aligning with previous literature. These findings are consistent with those of Chang et al., who reported that nurse-led self-management programs can enhance cardiac function indicators in patients [6]. The results of this study also suggest that DPS significantly improve heart function and reduce the risk of cardiac decompensation, further underscoring the clinical importance of such services for optimizing heart function.
Moreover, the study shows that multidisciplinary DPS have a positive impact on renal function, particularly in the experimental group. This finding aligns with the work of Kindel et al., who highlighted the critical role of renal function in the management and prognosis of heart failure [16]. Therefore, improving renal function may be crucial for enhancing the management effectiveness of patients with CHF a conclusion that is supported by the research of McCarthy et al. [19].
Additionally, the study identified a correlation between blood potassium levels and cardiac function, particularly LVEF levels. When LVEF exceeds 50%, the highest observed blood potassium level was approximately 4.68 mmol/L. This observation is consistent with the findings of Ghadge et al., who reported that blood potassium levels are associated with the severity and prognosis of heart failure, and that effective regulation of blood potassium in heart failure patients may contribute to improved cardiac function [9]. Consequently, monitoring blood potassium levels is essential not only for assessing heart failure severity and prognosis but also for guiding the development of effective treatment plans.
Finally, the comparison of clinical efficacy in this study revealed that multidisciplinary participation in DPS services significantly improved clinical outcomes, which is in line with similar findings in the literature. Sivakumar et al. demonstrated that comprehensive management strategies for heart failure patients can enhance clinical outcomes, reduce mortality, and decrease readmission rates [27]. This underscores the significance of DPS and highlights the pivotal role of multidisciplinary collaboration in the management of CHF.
We analyzed the advantages of the multidisciplinary collaborative discharge preparation nursing model as follows: (1) The team consists of experts from various relevant disciplines, ensuring a stable and cohesive team composition. (2) Communication and discussion among team members lead to comprehensive and optimal solutions, rather than unilateral decisions. Treatment and care plans are made through collaborative discussions, promoting efficient communication and decision-making within the team. (3) Team members collaborate in their respective roles centered around the patient, which alleviates individual workload pressures. For patients, this model addresses previous service gaps, while for the team, discussions, exchanges, and knowledge sharing provide opportunities for continuing education and professional development. The leadership roles of specialized physicians and nurses in heart failure management significantly enhance their expertise and understanding of patient conditions. This improvement in clinical insight and intervention capabilities facilitate the delivery of optimal treatment plans to patients. Furthermore, it allows for the timely identification of warning signs, initiation of remote consultations when necessary, and effective disease management, ultimately reducing readmission rates by controlling the progression of acute heart failure episodes.
This study introduces a multidisciplinary DPS model for managing CHF, combining expertise from various fields to improve clinical outcomes and patient quality of life while reducing readmission rates. The findings highlight the positive impact of this model on cardiac and renal function indicators and emphasize the importance of monitoring blood potassium levels to guide comprehensive treatment plans. The research advances the use of collaborative treatment models in CHF management and provides new insights and theoretical foundations for related disciplines.
This study does have a few limitations. As a retrospective study, it is subject to confounding and selection biases in sample collection. Additionally, the sample size is small and the follow-up period is short. A larger sample size and a randomized controlled trial is needed to better evaluate the efficacy of the multidisciplinary DPS model. These limitations are inherent to retrospective studies but do not undermine the accuracy of the findings. Future research should aim to expand the sample size to eliminate potential random variability, enabling a more accurate assessment of the effectiveness of multidisciplinary DPS models in the management of CHF.
In conclusion, the multidisciplinary DPS model is a comprehensive management approach that provides personalized medical care, making it suitable for managing patients with CHF. The advantages of the multidisciplinary DPS model include the development of personalized treatment plans through comprehensive evaluation, the use of applications and health devices for remote monitoring, and the provision of integrated medical services.
Acknowledgements
This work was supported by the Scientific Research Program of Wuhan Municipal Health Commission (WG20B04).
Disclosure of conflict of interest
None.
References
- 1.Averbuch T, Lee SF, Zagorski B, Mebazaa A, Fonarow GC, Thabane L, Van Spall HGC. Effect of a transitional care model following hospitalization for heart failure: 3-year outcomes of the patient-centered care transitions in heart failure (PACT-HF) randomized controlled trial. Eur J Heart Fail. 2024;26:652–660. doi: 10.1002/ejhf.3134. [DOI] [PubMed] [Google Scholar]
- 2.Bakitas MA, Dionne-Odom JN, Ejem DB, Wells R, Azuero A, Stockdill ML, Keebler K, Sockwell E, Tims S, Engler S, Steinhauser K, Kvale E, Durant RW, Tucker RO, Burgio KL, Tallaj J, Swetz KM, Pamboukian SV. Effect of an early palliative care telehealth intervention vs usual care on patients with heart failure: the ENABLE CHF-PC randomized clinical trial. JAMA Intern Med. 2020;180:1203–1213. doi: 10.1001/jamainternmed.2020.2861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Blot C, Sabbagh C, Rebibo L, Brazier F, Chivot C, Fumery M, Regimbeau JM. Use of transanastomotic double-pigtail stents in the management of grade B colorectal leakage: a pilot feasibility study. Surg Endosc. 2016;30:1869–1875. doi: 10.1007/s00464-015-4404-6. [DOI] [PubMed] [Google Scholar]
- 4.Brathwaite BM, Howell RS, Petrone P, Brathwaite C. Safety of bariatric surgery in patients with congestive heart failure: results of an 11-year retrospective study. Am Surg. 2022;88:1195–1200. doi: 10.1177/0003134821991975. [DOI] [PubMed] [Google Scholar]
- 5.Chai PR, Kaithamattam JJ, Chung M, Tom JJ, Goodman GR, Hasdianda MA, Carnes TC, Vaduganathan M, Scirica BM, Schnipper JL. Formative perceptions of a digital pill system to measure adherence to heart failure pharmacotherapy: mixed methods study. JMIR Cardio. 2024;8:e48971. doi: 10.2196/48971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chang AB, Bell SC, Byrnes CA, Dawkins P, Holland AE, Kennedy E, King PT, Laird P, Mooney S, Morgan L, Parsons M, Poot B, Toombs M, Torzillo PJ, Grimwood K. Thoracic society of australia and new zealand (TSANZ) position statement on chronic suppurative lung disease and bronchiectasis in children, adolescents and adults in australia and New Zealand. Respirology. 2023;28:339–349. doi: 10.1111/resp.14479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cong J, Zhu Y, Du J, Lin L, He Y, Zhang Q, Chye TO, Lv X, Liu W, Wu X, Ma F, Zhao X, Li Y, Long L. Mapping the minnesota living with heart failure questionnaire (MLHFQ) to SF-6Dv2 in Chinese patients with heart failure. Health Qual Life Outcomes. 2022;20:98. doi: 10.1186/s12955-022-02004-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Davidson PM, Newton PJ, Tankumpuan T, Paull G, Dennison-Himmelfarb C. Multidisciplinary management of chronic heart failure: principles and future trends. Clin Ther. 2015;37:2225–2233. doi: 10.1016/j.clinthera.2015.08.021. [DOI] [PubMed] [Google Scholar]
- 9.Ghadge R, Ghorpade R, Joshi S. Multi-disciplinary design optimization of composite structures: a review. Compos Struct. 2022;280:114875. [Google Scholar]
- 10.Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail. 2020;22:1342–1356. doi: 10.1002/ejhf.1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Han H, Zhu T, Guo Y, Ruan Y, Herzog E, He J. Impact of prior bariatric surgery on outcomes of hospitalized patients with heart failure: a population-based study. Surg Obes Relat Dis. 2019;15:469–477. doi: 10.1016/j.soard.2018.12.030. [DOI] [PubMed] [Google Scholar]
- 12.Hirji SA, Sabatino ME, Minhas AMK, Okoh AK, Fudim M, Vaduganathan M, Khan MS. Contemporary nationwide heart transplantation and left ventricular assist device outcomes in patients with histories of bariatric surgery. J Card Fail. 2022;28:330–333. doi: 10.1016/j.cardfail.2021.08.017. [DOI] [PubMed] [Google Scholar]
- 13.Jamaly S, Carlsson L, Peltonen M, Jacobson P, Karason K. Surgical obesity treatment and the risk of heart failure. Eur Heart J. 2019;40:2131–2138. doi: 10.1093/eurheartj/ehz295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jiang Y, Koh KWL, Ramachandran HJ, Nguyen HD, Lim S, Tay YK, Shorey S, Wang W. The effectiveness of a nurse-led home-based heart failure self-management programme (the HOM-HEMP) for patients with chronic heart failure: a three-arm stratified randomized controlled trial. Int J Nurs Stud. 2021;122:104026. doi: 10.1016/j.ijnurstu.2021.104026. [DOI] [PubMed] [Google Scholar]
- 15.Jubic K, Dick E, Moelber C. A multidisciplinary approach to improving the pediatric discharge process. J Nurs Care Qual. 2022;37:206–212. doi: 10.1097/NCQ.0000000000000608. [DOI] [PubMed] [Google Scholar]
- 16.Kindel TL, Higgins RM, Lak K, Gould J, Baumann Kreuziger L, Mohammed A, Gaglianello N, Ishizawar D. Bariatric surgery in patients with advanced heart failure: a proposed multi-disciplinary pathway for surgical care in medically complex patients. Surgery. 2021;170:659–663. doi: 10.1016/j.surg.2021.04.036. [DOI] [PubMed] [Google Scholar]
- 17.Kitsiou S, Gerber BS, Kansal MM, Buchholz SW, Chen J, Ruppar T, Arrington J, Owoyemi A, Leigh J, Pressler SJ. Patient-centered mobile health technology intervention to improve self-care in patients with chronic heart failure: protocol for a feasibility randomized controlled trial. Contemp Clin Trials. 2021;106:106433. doi: 10.1016/j.cct.2021.106433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Koleck TA, Topaz M, Tatonetti NP, George M, Miaskowski C, Smaldone A, Bakken S. Characterizing shared and distinct symptom clusters in common chronic conditions through natural language processing of nursing notes. Res Nurs Health. 2021;44:906–919. doi: 10.1002/nur.22190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McCarthy MJ, Gottlieb JF, Gonzalez R, McClung CA, Alloy LB, Cain S, Dulcis D, Etain B, Frey BN, Garbazza C, Ketchesin KD, Landgraf D, Lee HJ, Marie-Claire C, Nusslock R, Porcu A, Porter R, Ritter P, Scott J, Smith D, Swartz HA, Murray G. Neurobiological and behavioral mechanisms of circadian rhythm disruption in bipolar disorder: a critical multi-disciplinary literature review and agenda for future research from the ISBD task force on chronobiology. Bipolar Disord. 2022;24:232–263. doi: 10.1111/bdi.13165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, Burri H, Butler J, Celutkiene J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A ESC Scientific Document Group. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–3726. doi: 10.1093/eurheartj/ehab368. [DOI] [PubMed] [Google Scholar]
- 21.Metra M, Tomasoni D, Adamo M, Bayes-Genis A, Filippatos G, Abdelhamid M, Adamopoulos S, Anker SD, Antohi L, Bohm M, Braunschweig F, Gal TB, Butler J, Cleland JGF, Cohen-Solal A, Damman K, Gustafsson F, Hill L, Jankowska EA, Lainscak M, Lund LH, McDonagh T, Mebazaa A, Moura B, Mullens W, Piepoli M, Ponikowski P, Rakisheva A, Ristic A, Savarese G, Seferovic P, Sharma R, Tocchetti CG, Yilmaz MB, Vitale C, Volterrani M, von Haehling S, Chioncel O, Coats AJS, Rosano G. Worsening of chronic heart failure: definition, epidemiology, management and prevention. A clinical consensus statement by the heart failure association of the European society of cardiology. Eur J Heart Fail. 2023;25:776–791. doi: 10.1002/ejhf.2874. [DOI] [PubMed] [Google Scholar]
- 22.Mottel BH, Lindsay DA, Frishman WH. Effect of bariatric surgery on cardiovascular function and heart failure outcomes. Cardiol Rev. 2021;29:187–194. doi: 10.1097/CRD.0000000000000338. [DOI] [PubMed] [Google Scholar]
- 23.Murray G, Gottlieb J, Hidalgo MP, Etain B, Ritter P, Skene DJ, Garbazza C, Bullock B, Merikangas K, Zipunnikov V, Shou H, Gonzalez R, Scott J, Geoffroy PA, Frey BN. Measuring circadian function in bipolar disorders: empirical and conceptual review of physiological, actigraphic, and self-report approaches. Bipolar Disord. 2020;22:693–710. doi: 10.1111/bdi.12963. [DOI] [PubMed] [Google Scholar]
- 24.Page K, Marwick TH, Lee R, Grenfell R, Abhayaratna WP, Aggarwal A, Briffa TG, Cameron J, Davidson PM, Driscoll A, Garton-Smith J, Gascard DJ, Hickey A, Korczyk D, Mitchell JA, Sanders R, Spicer D, Stewart S, Wade V National Heart Foundation of Australia. A systematic approach to chronic heart failure care: a consensus statement. Med J Aust. 2014;201:146–150. doi: 10.5694/mja14.00032. [DOI] [PubMed] [Google Scholar]
- 25.Park JJ. Epidemiology, pathophysiology, diagnosis and treatment of heart failure in diabetes. Diabetes Metab J. 2021;45:146–157. doi: 10.4093/dmj.2020.0282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Redeker NS, Yaggi HK, Jacoby D, Hollenbeak CS, Breazeale S, Conley S, Hwang Y, Iennaco J, Linsky S, Nwanaji-Enwerem U, O’Connell M, Jeon S. Cognitive behavioral therapy for insomnia has sustained effects on insomnia, fatigue, and function among people with chronic heart failure and insomnia: the HeartSleep Study. Sleep. 2022;45:zsab252. doi: 10.1093/sleep/zsab252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sivakumar V. Approaches towards tannery modernization and up-gradation: leather Industry 4.0: multi-disciplinary approach. J Am Leather Chem Assoc. 2021:116. [Google Scholar]
- 28.Smith H, Harvey C, Portela A. Discharge preparation and readiness after birth: a scoping review of global policies, guidelines and literature. BMC Pregnancy Childbirth. 2022;22:281. doi: 10.1186/s12884-022-04577-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tinajero MG, Malik VS. An update on the epidemiology of type 2 diabetes: a global perspective. Endocrinol Metab Clin North Am. 2021;50:337–355. doi: 10.1016/j.ecl.2021.05.013. [DOI] [PubMed] [Google Scholar]
- 30.Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Beaton AZ, Boehme AK, Buxton AE, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Fugar S, Generoso G, Heard DG, Hiremath S, Ho JE, Kalani R, Kazi DS, Ko D, Levine DA, Liu J, Ma J, Magnani JW, Michos ED, Mussolino ME, Navaneethan SD, Parikh NI, Poudel R, Rezk-Hanna M, Roth GA, Shah NS, St-Onge MP, Thacker EL, Virani SS, Voeks JH, Wang NY, Wong ND, Wong SS, Yaffe K, Martin SS American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2023 update: a report from the American heart association. Circulation. 2023;147:e93–e621. doi: 10.1161/CIR.0000000000001123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tsui ST, Yang J, Zhang X, Docimo S Jr, Spaniolas K, Pryor AD. Hospitalizations and emergency department visits in heart failure patients after bariatric surgery. Surg Obes Relat Dis. 2021;17:489–497. doi: 10.1016/j.soard.2020.11.014. [DOI] [PubMed] [Google Scholar]
- 32.Val FRD, Cheon O, Menser T, Kash B, Jones SL, Baek J, Bhimaraj A, Estep J, Sherman V, Tariq N. Bariatric surgery in end-stage heart failure: feasibility in successful attainment of a target body mass index. J Card Fail. 2020;26:944–947. doi: 10.1016/j.cardfail.2020.04.020. [DOI] [PubMed] [Google Scholar]
- 33.Van Spall HGC, Lee SF, Xie F, Ko DT, Thabane L, Ibrahim Q, Mitoff PR, Heffernan M, Maingi M, Tjandrawidjaja MC, Zia MI, Panju M, Perez R, Simek KD, Porepa L, Graham ID, Haynes RB, Haughton D, Connolly SJ. Knowledge to action: rationale and design of the patient-centered care transitions in heart failure (PACT-HF) stepped wedge cluster randomized trial. Am Heart J. 2018;199:75–82. doi: 10.1016/j.ahj.2017.12.013. [DOI] [PubMed] [Google Scholar]
- 34.Van Spall HGC, Lee SF, Xie F, Oz UE, Perez R, Mitoff PR, Maingi M, Tjandrawidjaja MC, Heffernan M, Zia MI, Porepa L, Panju M, Thabane L, Graham ID, Haynes RB, Haughton D, Simek KD, Ko DT, Connolly SJ. Effect of patient-centered transitional care services on clinical outcomes in patients hospitalized for heart failure: the PACT-HF randomized clinical trial. JAMA. 2019;321:753–761. doi: 10.1001/jama.2019.0710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Weber C, Hung J, Hickling S, Nedkoff L, Murray K, Li I, Briffa TG. Incidence, predictors and mortality risk of new heart failure in patients hospitalised with atrial fibrillation. Heart. 2021;107:1320–1326. doi: 10.1136/heartjnl-2020-318648. [DOI] [PubMed] [Google Scholar]