

Abstract
Background
Substance‐specific mass media campaigns which address young people are widely used to prevent illicit drug use. They aim to reduce use and raise awareness of the problem.
Objectives
To assess the effectiveness of mass media campaigns in preventing or reducing the use of or intention to use illicit drugs amongst young people.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library 2013, Issue 1), including the Cochrane Drugs and Alcohol Group's Specialised Register; MEDLINE through PubMed (from 1966 to 29 January 2013); EMBASE (from 1974 to 30 January 2013) and ProQuest Dissertations & Theses A&I (from 1861 to 3 February 2013).
Selection criteria
Cluster‐randomised controlled trials, prospective and retrospective cohort studies, interrupted time series and controlled before and after studies evaluating the effectiveness of mass media campaigns in influencing drug use, intention to use or the attitude of young people under the age of 26 towards illicit drugs.
Data collection and analysis
We used the standard methodological procedures of The Cochrane Collaboration.
Main results
We included 23 studies involving 188,934 young people, conducted in the USA, Canada and Australia between 1991 and 2012. Twelve studies were randomised controlled trials (RCT), two were prospective cohort studies (PCS), one study was both a RCT and a PCS, six were interrupted time series and two were controlled before and after (CBA) studies. The RCTs had an overall low risk of bias, along with the ITS (apart from the dimension 'formal test of trend'), and the PCS had overall good quality, apart from the description of loss to follow‐up by exposure.
Self reported or biomarker‐assessed illicit drug use was measured with an array of published and unpublished scales making comparisons difficult. Pooled results of five RCTs (N = 5470) show no effect of media campaign intervention (standardised mean difference (SMD) ‐0.02; 95% confidence interval (CI) ‐0.15 to 0.12).
We also pooled five ITS studies (N = 26,405) focusing specifically on methamphetamine use. Out of four pooled estimates (two endpoints measured in two age groups), there was evidence of a reduction only in past‐year prevalence of methamphetamine use among 12 to 17 years old.
A further five studies (designs = one RCT with PCS, two PCS, two ITS, one CBA, N = 151,508), which could not be included in meta‐analyses, reported a drug use outcome with varied results including a clear iatrogenic effect in one case and reduction of use in another.
Authors' conclusions
Overall the available evidence does not allow conclusions about the effect of media campaigns on illicit drug use among young people. We conclude that further studies are needed.
Keywords: Humans, Illicit Drugs, Mass Media, Australia, Canada, Health Promotion, Health Promotion/methods, Prospective Studies, Randomized Controlled Trials as Topic, Retrospective Studies, Substance‐Related Disorders, Substance‐Related Disorders/prevention & control, United States
Plain language summary
Do media campaigns prevent young people from using illicit drugs?
Media campaigns to prevent illicit drug use are a widespread intervention. We reviewed 23 studies of different designs involving 188,934 young people and conducted in the United States, Canada and Australia. The studies tested different interventions and used several questionnaires to interview the young people about the effects of having participated in the studies brought to them. As a result it was very difficult to reach conclusions and for this reason we are highlighting the need for further studies.
Background
Health promotion, mass media campaigns are initiatives typically undertaken by national authorities which use communication media to disseminate information about, for example, health or threats to it and to persuade people to adopt behavioural changes. Mass media campaigns are implemented via television and radio broadcasts, newspaper or magazine advertisements, billboards and road posters. They can also use colourful advertisements and brochures available for travellers on buses and the metro and, more recently, a broad range of available technology including the Internet, mobile phone short messages and email lists. Media campaigns can be of short or longer duration and sometimes they encompass several consequent rounds of delivery. They can be standalone interventions or be integrated into complex social marketing programmes.
Mass media campaigns for the prevention of illicit drug use are very common worldwide but only few campaigns have been formally evaluated (Wammes 2007). Furthermore, most of those evaluations (Rossi 2003) assessed only the process (in terms of understanding, retention and appeal of the messages) and the very few that assessed outcomes (in terms of behaviours of use) often found weak or counterproductive effects.
Description of the condition
Initiation of use of all substances typically occurs during the teens or early years of adulthood (ESPAD 2011; UNODC 2012). Since the neurological or psychological factors that may influence how and whether addiction develops are unknown, "even occasional drug use can inadvertently lead to addiction" (Leshner 1997; Leshner 1999). Indeed, research has found that drug use leading to dependence usually starts in adolescence (Camí 2003; McLelland 2000; Swendsen 2009).
Since the neurological and social mechanisms of dependence are similar for all addictive substances, a common view, therefore, is that prevention should focus on an age group (teenagers) rather than specific substances (Ashton 2003; Leshner 1997; Nestler 1997; Wise 1998).
Description of the intervention
The mass media (TV, Internet, radio, newspapers, billboards) have increasingly been used as a way of delivering preventive health messages. They have the potential to modify the knowledge or attitudes of a large proportion of the community (Redman 1990). They also have the potential to reach large populations of susceptible individuals and groups that may be difficult to access through more traditional approaches. In addition, in terms of the per capita cost of prevention messages, they are relatively inexpensive (Brinn 2010).
This review is limited to mass media campaigns that aim to prevent the uptake of illicit drug use (both in general or that of specific substances) or to reduce or stop the use of illicit drugs. It excludes mass media campaigns that aim to promote safer or less harmful use of drugs.
The following table summarises the main characteristics of most mass media campaign.
| Category | Objective | Target audience | Details |
| Information campaign | Warning | General or youth population | Information about the dangers and risks of a range of illicit substances |
| Empowerment | General population, especially parents | Information about how to contribute to drug prevention through your own behaviour | |
| Information about where and how to seek support, counselling and treatment regarding illicit drug use, especially for your children | |||
| Youth population | Information about where and how to seek support, counselling and treatment regarding illicit drug use | ||
| Support | General population | Information about existing prevention interventions or programmes in communities, in schools or for families in order to strengthen community involvement and support for them | |
| Social marketing campaign | Correct erroneous normative beliefs | General or youth population | Declared purpose is to correct erroneous normative beliefs about the extent and acceptance of drug use in peer populations ("you're not weird if you don't use because 80% of your peers don't either") |
| Setting or clarifying social and legal norms | General or youth population | Declared purpose is to deglamorise and demystify drug use and related behaviour (e.g. drug driving) and to explain the rationale of community norms and control measures | |
| Setting positive role models or social norms | General or youth population | Declared purpose is to promote non‐drug‐use‐related prototypes of lifestyles, behaviour and personality |
How the intervention might work
Most campaigns are based on a limited number of theoretical models, such as the health belief model (lack of knowledge about health harms may lead to drug use), the theory of planned behaviour (drug use is a rational decision due to attitude toward drugs, perceived social norms and perceived control over drugs) and the social norms theory (overrated perception of prevalence among peers may lead to drug use). In summary, the theories most frequently used as base for anti‐drugs mass media campaigns are:
Health belief model. This model (Glanz 2002) is based on the concept that the perceived susceptibility to and the severity of the disease and the perceived benefits of action to avoid disease are the key factors in motivating a positive health action. So, based on some elements of the model, the provision of factual information about the negative effects and dangers of drugs should deter use or prevent substance abuse by creating negative attitudes towards drug use.
Intervention based on this theory: information campaign
Theory of reasoned action/theory of planned behavior. The theory of reasoned action/theory of planned behaviour (Ajzen 1991) proposes that an individual's behavioural intentions have three constituent parts: the individual's attitude towards the behaviour, the social norms as perceived by the individual and the perceived control over the behaviour. Individuals may weight these differently in assessing their behavioural intentions. According to this model, drug use is a consequence of a rational decision (intention), which is based on the belief about drug use, the social norms towards drug use and the belief about control over the behaviour.
Intervention based on this theory: social marketing campaigns with the objective of setting or clarifying social and legal norms as well as information campaigns
Social norms theory. This theory (Perkins 1986) states that "our behaviour is influenced by incorrect perceptions of how other members of our social groups think and act" (Berkowitz 2004, p. 5). Campaigns based on this theory, which are also referred to as 'normative education', challenge the misconception that many adults and most adolescents use drugs. For example, students are provided with information on the prevalence ‐ from either national or local surveys ‐ of drug use among their peers so that they can compare their own estimates of drug use with the actual prevalence.
Related to this is the Super‐Peer Theory (Strasburger 2008). The Super‐Peer Theory postulates that media portrayal of drug use (or casual sex or violence) influences the susceptible teens.
Intervention based on this theory: social marketing campaigns that aim to correct erroneous normative beliefs
Social learning theory. The social learning theory (Bandura 1977) postulates that personality is an interaction between environment, behaviours and the psychological processes of an individual. Also referred to as observational learning, the theory of social learning places an emphasis on observing and modelling other people's behaviours, attitudes and emotional reaction.
Intervention based on this theory: social marketing campaigns setting positive role models or social norms
Why it is important to do this review
Bühler and Kröger (Bühler 2006) conclude their review of reviews with the recommendation to use media campaigns only as supporting measures and not as a single strategy alone, whereas Hawks 2002, in line with the review of reviews by the Health Development Agency (HDA) (McGrath 2006), concludes that "the use of the mass media on its own, particularly in the presence of other countervailing influences, has not been found to be an effective way of reducing different types of psychoactive substance use. It has however been found to raise information levels and to lend support to policy initiatives".
Despite concerns in reviews about poor effectiveness and possible harm of anti‐drug prevention activities (Faggiano 2008), media campaigns are still very popular worldwide and in European Union member states (EMCDDA 2009).
An assessment of both positive and negative (iatrogenic) effects is important for ethical reasons as well, because mass media campaigns ‐ unlike other social or health interventions ‐ are imposed on populations that have neither asked for nor explicitly consented to the intervention (Sumnall 2007). A systematic review of all the studies assessing media campaign interventions aimed at preventing illicit drug use in young people is therefore necessary in order to inform future strategies and to help design campaigns that avoid harm. Such a review will also contribute to the identification of further areas for research.
Objectives
To assess the effectiveness of mass media campaigns in preventing or reducing the use of or intention to use illicit drugs amongst young people.
Methods
Criteria for considering studies for this review
Types of studies
Any study that evaluates the effectiveness of mass media campaigns in influencing drug use, intention to use or the attitude of young people towards illicit drugs.
Randomised controlled trials in which the unit of randomisation is an individual or a cluster (the school, community or geographical region)
Controlled trials without randomisation allocating schools, communities or geographical regions
Prospective and retrospective cohort studies
Interrupted time series
Controlled before and after studies
Types of participants
Young people under the age of 26.
Types of interventions
Experimental intervention
The following definition was adopted by a similar Cochrane review (Brinn 2010): "Mass media is defined here as channels of communication such as television, radio, newspapers, billboards, posters, leaflets or booklets intended to reach large numbers of people and which are not dependent on person to person contact". To be included in the review, a study needs to assess a mass media campaign explicitly aimed at influencing people's drug use, intention to use or attitude towards illicit drugs use.
Control intervention
1) No intervention; 2) other types of communication interventions such as school‐based drug abuse prevention programmes (Faggiano 2008); 3) community‐based prevention programmes; 4) lower exposure to intervention; 5) time before exposure to intervention.
Types of outcome measures
Primary outcomes
Self reported or biomarker‐assessed illicit drug use
Secondary outcomes
Intentions not to use/to reduce use/to stop use
Attitudes towards illicit drug use
Knowledge about the effects of illicit drugs on health
Understanding of intended message and objectives
Perceptions (including perceptions of peer norms and perceptions about illicit drug use)
Adverse effects induced by the campaign (reactance, i.e. a reaction to contradict the prevailing norms of rules and positive descriptive norms, i.e. increased perception that drug use in peer population is common, normal or acceptable)
Search methods for identification of studies
Electronic searches
We obtained relevant trials from the following sources:
Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library 2013, Issue 1) which includes the Cochrane Drugs and Alcohol Group's Specialised Register;
MEDLINE through PubMed (freely accessible at http://www.ncbi.nlm.nih.gov/pubmed/) (from 1966 to 29 January 2013);
EMBASE (from 1974 to 30 January 2013);
ProQuest Dissertations & Theses A&I (from 1861 to 3 February 2013).
We compiled detailed search strategies for each database searched. These were based on the search strategy developed for PubMed but revised appropriately for each database to take account of differences in controlled vocabulary and syntax rules.
The search strategy for:
CENTRAL is shown in Appendix 1;
PubMed is shown in Appendix 2;
EMBASE is shown in Appendix 3;
ProQuest Dissertations & Theses A&I was: (media campaigns OR mass media) AND illicit drug* AND preventi*.
We searched for ongoing clinical trials and unpublished studies on the following Internet sites:
Searching other resources
We also searched other sources to identify relevant studies. We assessed conference proceedings that were likely to contain relevant material and contacted the authors. We contacted investigators or experts in the field to seek information on unpublished or incomplete trials. We also reviewed EMCDDA National Focal Points Annual National Reports for any description of relevant studies conducted in Europe.
We used the first studies identified as fulfilling the inclusion criteria to inspect the MeSH terms and to integrate the search strategies. Moreover, we used the "related articles" function of PubMed in a "capture‐recapture method" to validate the inclusiveness of the search strategy.
We did not apply any language restriction.
Data collection and analysis
Selection of studies
Two review authors (EA and MF) inspected the search hits by reading the titles and the abstracts. We obtained each potentially relevant study identified in the search in full text and at least two review authors assessed studies for inclusion independently. In case of doubts as to whether a study should have been included, this was resolved by discussion between the review authors. We collated and assessed multiple publications as one study.
Data extraction and management
Two review authors (EA and AB) independently extracted data and input relevant information into Review Manager (Review Manager 2012) for meta‐analysis. Two review authors (MF and FF) assessed the theoretical background of the campaigns. We discussed and solved every step by consensus. We produced a narrative synthesis of the key findings along with a meta‐analysis of studies which used appropriate measures.
Assessment of risk of bias in included studies
Four review authors (EA, AB, MF and FF) performed quality assessments independently. We discussed and solved any disagreement by consensus. We uploaded final assessments into Review Manager. In order to obtain more information on the criteria for reducing risk of bias, we contacted the authors of most of the studies.
To assess RCTs we followed the criteria recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). The recommended approach for assessing risk of bias in studies included in Cochrane Reviews is a two‐part tool, addressing seven specific domains, namely sequence generation and allocation concealment (selection bias), blinding of participants and providers (performance bias) blinding of outcome assessor (detection bias), incomplete outcome data (attrition bias) selective outcome reporting (reporting bias) and other source of bias. The first part of the tool involves describing what was reported to have happened in the study. The second part of the tool involves assigning a judgement relating to the risk of bias for that entry, in terms of low, high or unclear risk. The domains of sequence generation and allocation concealment (avoidance of selection bias) were addressed in the tool by a single entry for each study. Blinding of participants might not be applicable for this type of intervention, and we therefore considered blinding of personnel and outcome assessors (avoidance of performance bias and detection bias). We considered a study to have low risk of bias if the data were obtained with an anonymous questionnaire or administered by computer. We considered incomplete outcome data (avoidance of attrition bias) for all outcomes.
For ITS studies we used the tools developed by the Effective Practice and Organization of Care (EPOC) Group (Appendix 4). For cohort studies we used the SIGN Quality Criteria described in Appendix 5.
Measures of treatment effect
We intended to analyse dichotomous outcomes (such as intention to use or actual use of illicit substances) by calculating the risk ratio (RR) or odds ratio (OR) for each trial and express the uncertainty in each result with their 95% confidence intervals. We only found continuous outcome measures which we analysed by calculating the standardised mean difference (SMD) with its corresponding 95% confidence intervals.
Unit of analysis issues
In the case of cluster‐randomised trials the unit of analysis is either the school or the town. We stated at protocol level that in this case we would have taken into account the criteria for assessing bias in cluster‐randomised trials as described in the Cochrane Handbook. We inflated each arm's standard deviation for two studies (Slater 2006; Newton 2010) by multiplying it by the study design effect, a coefficient which takes into account the average cluster size and the study intra‐class correlation.
Dealing with missing data
Where needed, we contacted the authors of the studies for integration of any possible missing data.
Assessment of heterogeneity
The presence of heterogeneity between the trials was tested using the I2 statistic and the Chi2 test. A P value of the I2 statistic higher than 0.50 and a P value of the Chi2 test lower than 0.10 suggests that there is some evidence of heterogeneity.
Assessment of reporting biases
We intended to use funnel plots (plots of the effect estimate from each study against the standard error) to assess the potential for bias related to the size of the trials, which could indicate possible publication bias. In fact we did not reach the minimum number of (10) studies included in the meta‐analysis which is suggested as sufficient for conducting a funnel plot (Higgins 2011).
Data synthesis
We intended to carry out a meta‐analysis by combining RR/OR or the SMD where possible. We performed a meta‐analysis of the RCTs using a random‐effect model in order to take into consideration the heterogeneity among studies.
For the studies evaluating the Meth Project (Colorado Meth 2011; Georgia Meth 2011; Hawaii Meth 2011; Idaho Meth 2010; Wyoming Meth 2011) we performed a separate meta‐analysis. An interrupted time series (ITS) design was applied for estimating the differences in prevalence of methamphetamine use before and after the Meth Project intervention, adjusting for any underlying temporal trend. Statistical models were based on multilevel mixed effects logistic regression, with State as a random intercept modelling baseline log odds of methamphetamine use to vary randomly across states. The relatively few data points did not allow exploring of more complex models, e.g. the temporal trend could not be assumed to vary randomly across states. The fixed part of the final model assumes (i) a different baseline by age group, but similar among states; (ii) a linear temporal trend homogeneous across states; (iii) an effect of the intervention differing by age group but constant across time and occurring immediately after the intervention. The model may be written as logit(useij) = β0 + u0j + β1timei + β2intervi + β3agei + β4age×intervi + ϵij, with use as prevalence of methamphetamine use, time as a continuous variable, intervention and age as two‐level categorical variables and J indicating state. The exponentiated coefficient β2 is interpretable as the ratio between the odds of using methamphetamine after (numerator) and before (denominator) the intervention (Gilmour 2006).The model was fitted separately for past‐month and past‐year use of methamphetamine. Data points regarding lifetime use of methamphetamine were not analysed.
Subgroup analysis and investigation of heterogeneity
We intended to perform stratified meta‐analysis in order to assess the differential effect of the campaigns based on different theoretical approaches. However the impact of media campaigns may be mediated by the sub‐cultural environment and, in particular, by the attitude towards substance use in a given culture. Therefore, at protocol level it was anticipated that subsets of studies were to be analysed by characteristics of target participants (regional location, users versus non‐users etc.) whenever possible. Studies could also be compared by type of campaign, based on different theoretical approaches. We did not reach the number of studies sufficient to perform any type of sub‐set analysis.
Sensitivity analysis
To incorporate the assessment of risk of bias in the review process we first plotted the intervention effect estimates against the assessment of risk of bias. We subsequently inspected the results stratified for risk of bias and we did not find significant associations between measure of effect and risk of bias. We therefore decided to not include the 'Risk of bias' assessment in the meta‐analysis and to discuss it narratively in the results section. The items considered in the sensitivity analysis were the random sequence, blinding of personnel and outcome assessors, and selective reporting.
Results
Description of studies
See: Characteristics of included studies, Characteristics of excluded studies and Characteristics of studies awaiting classification.
Results of the search
The study flow chart is presented in Figure 1.
1.

Study flow diagram. Please note that some studies include more than one article. This explains why there are 23 included studies out of 28 included articles.
Search sources
On 29 January 2013 we performed a PubMed (MEDLINE) search as described in Appendix 2, which identified 5877 records. On 30 January 2013 we searched CENTRAL which returned 566 results and EMBASE which gave 4945 records. On 3 February 2013 we also performed a ProQuest 'Dissertations & Theses A&I' search which returned 6638 records.
We also obtained additional records (N = 317) from one single paper (Hornik 2006) using PubMed's 'Similar articles' feature, and from papers extracted from 10 reviews (Battjes 1985; Berberian 1976; Hailey 2008; Kumpfer 2008; Romer 1994; Romer 1995; Schilling 1990; Stephenson 2003b; Wakefield 2010; Werb 2011), three reports (EMCDDA 2010; Know the Score 2007; NCI 2008) and three book chapters (Crano 2001; Flay 1983; Moskowitz 1983).
Screening
We independently screened records from each source search, i.e. no automatic removal of duplicates was used because of the risk of false‐positive duplicates. Therefore, we screened 18,343 titles and abstracts. Of them, we excluded 18,253 records (99.5%) as obviously irrelevant.
Full‐text analysis
We examined the full‐text articles of the remaining 90 records. Of them, 62 records were either excluded (N = 53) due to ineligibility of intervention type, participant age and reported outcome, or set in a pending status (N = 9) due to missing information. We contacted authors whenever possible.
Twenty‐eight records corresponded to 23 unique studies which were included in this review. A subset of 13 studies (eight RCTs and five ITS) could also be included in meta‐analyses, mostly thanks to personal communication with some authors who provided us with unpublished data and additional reports.
Included studies
Study design
Out of 23 unique studies, 12 were randomised controlled trials (RCT) (Czyzewska 2007; Fang 2010; Fishbein 2002; Kelly 1992; Lee 2010; Newton 2010; Palmgreen 1991; Polansky 1999; Schwinn 2010; Slater 2011; Yzer 2003; Zhao 2006), two were prospective cohort studies (PCS) (Hornik 2006; Scheier 2010), one study was both a RCT and a PCS (Slater 2011), six were ITS (Carpenter 2011; Colorado Meth 2011; Hawaii Meth 2011; Idaho Meth 2010; Palmgreen 2001; Wyoming Meth 2011) and two were before and after (CBA) studies (Georgia Meth 2011; Miller 2000).
Population
No study enrolled subjects younger than 10 years old. Twenty‐one studies included subjects older than 10 and younger than 20 years old. Two studies included subjects older than 20 years old and younger than this review's limit of 26 years old; one of them included only people older than 20 (Miller 2000) and one people aged 18 to 22 (Palmgreen 1991).
Three studies included only girls (Fang 2010; Kelly 1992; Schwinn 2010). The others did not specify any sex‐related selection criteria.
Two studies focused on specific ethnic or racial groups: one on Mexican‐American boys and girls (Polansky 1999) and one on Asian‐American girls (Fang 2010). The remaining studies did not use ethnicity, racial or socioeconomic characteristics to define the selection criteria.
Intervention
Mass media components
Eight studies evaluated standalone TV/radio commercials (Czyzewska 2007; Fishbein 2002; Kelly 1992; Palmgreen 1991; Palmgreen 2001; Polansky 1999; Yzer 2003; Zhao 2006) and four studies evaluated standalone Internet‐based interventions (Fang 2010; Lee 2010; Newton 2010; Schwinn 2010). Eleven studies evaluated multi‐component interventions, three regarding TV/radio and printed advertising (Miller 2000; Slater 2006; Slater 2011) and eight regarding TV/radio commercials, printed advertisements and Internet advertising (Carpenter 2011; Hornik 2006; Scheier 2010 and the five Meth Projects). No study evaluated interventions using standalone printed advertising.
Three studies added a school‐based drug prevention curriculum (Slater 2006; Slater 2011) or a combination of peer education, computer resources, campus policy and campus‐wide events (Miller 2000) to the mass media component(s).
Setting
Eleven studies were conducted in only one setting: eight studies in a school/college setting (Czyzewska 2007; Fishbein 2002; Kelly 1992; Lee 2010; Miller 2000; Newton 2010; Polansky 1999; Yzer 2003), two in a community setting (Fang 2010; Schwinn 2010) and one in a national/statewide setting (Palmgreen 2001).
Twelve studies were conducted in multiple settings: three in school and community settings (Palmgreen 1991; Slater 2006; Zhao 2006), eight in community and national settings (Carpenter 2011; Hornik 2006; Scheier 2010 and the five Meth Projects), while one (Slater 2011) reported evaluations of two similar but distinct interventions ‐ one implemented in a school and community setting and one aired to the whole nation.
Comparison group
Fourteen studies compared one or more mass media interventions with no intervention (Fang 2010; Fishbein 2002; Lee 2010; Miller 2000; Palmgreen 2001; Schwinn 2010; Slater 2006; Yzer 2003; Zhao 2006 and the five Meth projects). Four studies compared higher to lower exposure to a mass media intervention (Carpenter 2011; Hornik 2006; Scheier 2010; Slater 2011). Five studies compared anti‐drug advertisements with another intervention (Czyzewska 2007; Kelly 1992; Newton 2010; Palmgreen 1991; Polansky 1999). Two studies (Palmgreen 1991; Yzer 2003) had different intervention arms comparing either another intervention or no intervention. For details of control interventions see the table Characteristics of included studies.
The following table summarises the interventions evaluated and the exposure of the comparison groups, as well as the theories underlying the interventions.
| Studies | Explicit underpinning theory | Intervention | Comparison group | ||||
| Internet‐based intervention |
PSA (public service ‐ TV/radio) advertisements |
Printed advertisement | No intervention | Lower exposure to intervention | Other intervention/different combination of same intervention | ||
| Palmgreen 1991 | Influence of sensation‐seeking on drug use | X | X | ||||
| Kelly 1992 | Role of discussion on attitudes and opinions | X | X | ||||
| Polansky 1999 | Decision theory | X | X | ||||
| Miller 2000 | Self regulation theory | X | X | X | |||
| Palmgreen 2001 | Influence of sensation‐seeking on drug use | X | X | ||||
| Fishbein 2002 | Beliefs, norms or self efficacy | X | X | ||||
| Yzer 2003 | Theories of behavioral change: persuasion effects | X | X | X | |||
| Slater 2006 | Social‐ecological framework (norms and expectations influence drug use) | X | X | X | |||
| Zhao 2006 | Normative beliefs | X | X | ||||
| Czyzewska 2007 | Reactance theory | X | X | ||||
| Hornik 2006 | Unclear | X | X | X | X | ||
| Scheier 2010 | Social marketing | X | X | X | X | ||
| Schwinn 2010 | Social learning theory | X | X | ||||
| Lee 2010 | Readiness to change | X | X | ||||
| Fang 2010 | Family‐oriented | X | X | ||||
| Newton 2010 | Social influence approach | X | X | ||||
| Idaho Meth 2010 | Perception of risk and perception of social disapproval are correlated with drug consumption | X | X | X | X | ||
| Colorado Meth 2011 | |||||||
| Georgia Meth 2011 | |||||||
| Hawaii Meth 2011 | |||||||
| Wyoming Meth 2011 | |||||||
| Slater 2011 | Autonomy and aspiration perceptions as mediators marijuana use | X | X | X | |||
| Carpenter 2011 | Unclear; evaluated many heterogeneous mass media campaigns | X | X | X | X | ||
Outcome
The sum of studies described in this paragraph exceeds the number of included studies because many studies measured more than one outcome.
Sixteen studies measured the effect of mass media campaigns on illicit drugs use. Thirty‐six studies reported the following secondary outcomes (seven were without primary outcomes):
seven studies: intentions not to use/to reduce use/to stop use;
15 studies: attitudes towards illicit drug use;
two studies: knowledge about the effects of illicit drugs on health;
one study: understanding of intended message and objectives;
11 studies: perceptions (including perceptions of peer norms and perceptions about illicit drug use).
Country
Twenty‐one studies were conducted in the USA, one in the USA and Canada (Schwinn 2010), and one in Australia (Newton 2010).
Duration
No follow‐up was described, or was applicable, for seven studies (Carpenter 2011; Czyzewska 2007; Fishbein 2002; Palmgreen 1991; Polansky 1999; Yzer 2003; Zhao 2006). Follow‐up was shorter than 12 months for four studies (Fang 2010; Kelly 1992; Lee 2010; Schwinn 2010), and longer than or equal to 12 months for the remaining 12 studies.
Excluded studies
Several thousand studies were excluded after screening their title and abstract because they did not meet the inclusion criteria. Fifty‐three studies required closer scrutiny and are listed in the Characteristics of excluded studies table.
Four were excluded because the population studied did not meet the inclusion criteria; nine studies included interventions different from our inclusion criteria The remainder were excluded because the study design did not met the inclusion criteria.
Risk of bias in included studies
Randomised controlled trials (RCTs)
Approximately half of the included studies are randomised and quasi‐randomised controlled trials. One of them is a mixed RCT‐cohort study (Slater 2011). The results of their 'Risk of bias' assessments are presented in Figure 2 and Figure 3 and described in detail in Table 1.
2.

Randomised controlled trial 'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Randomised controlled trial 'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
1. 'Risk of bias' assessment of interrupted time series studies.
| Miller 2000 | ||
| Criterion | Score | Notes |
| a) Protection against secular changes | ||
| The intervention is independent of other changes | Done | "The usual environmental influences such as prices, taxes, state regulations, campus policies, and enforcement did not change substantially during the study period. Neither was there any reason to expect that students on the two campuses would respond differentially to anonymous surveys. The only obvious difference between the two campuses that might be expected to affect substance use differentially was the implementation of the prevention program at UNM", page 756 |
| There are sufficient data points to enable reliable statistical inference | Not done | 2 data points (before and after) |
| Formal test for trend. Complete this section if authors have used ANOVA modelling | Done | |
| b) Protection against detection bias | ||
| Intervention unlikely to affect data collection | Done | "All questionnaires were completed anonymously. To encourage participation, those who returned the survey (by mail) were entered into a lottery for cash prizes by separating a numbered ticket, returning one part with the completed survey and retaining the other half. Winning numbers were announced through the campus newspaper, the Daily Lobo. As an additional incentive for the follow‐up survey, respondents were invited to participate in a contest to guess the actual levels of alcohol/drug use on campus, as revealed by the first survey", page 750 |
| Blinded assessment of primary outcome(s) | Done | Anonymous surveys, page 750 |
| c) Completeness of data set | Done | "At baseline (fall) assessment, 1,400 surveys were distributed to enrolled UNM students, a sample of approximately 6% selected randomly by the university s computerized mailing list program. Of these, 567 surveys were returned and usable (41%). At the control campus, 1,080 surveys were distributed to a random sample of students, 457 of whom returned them (42.3%). [..] The return rates were 431 (31%) at UNM and 434 (34%) at NMSU", page 751 |
| d) Reliable primary outcome measure(s) | Done | "Use measures (14 items) included a frequency (number of drinking days per 30) and quantity index of drinking (number of standard drinks consumed per drinking occasion; range: 0‐15) that were multiplied to form a single quantity frequency measure (number of drinks per month) [..]", page 750 "Problem measures included 14 indicators of alcohol dependence and adverse consequences of heavy drinking or illicit drug use in the prior year. [..]", page 750 "Risk assessment included 13 items regarding the extent to which students perceived risk or consequences related to alcohol or other drug use [..]", page 750 |
| Palmgreen 2001 (includes Stephenson 1999) | ||
| Criterion | Score | Notes |
| a) Protection against secular changes | ||
| The intervention is independent of other changes | Unclear | |
| There are sufficient data points to enable reliable statistical inference | Done | 32 data points |
| Formal test for trend. Complete this section if authors have used ANOVA modelling | Done | ANOVA modelling was used. See from page 186 on |
| b) Protection against detection bias | ||
| Intervention unlikely to affect data collection | Done | Methodology of data collection is not reported to have changed across data points |
| Blinded assessment of primary outcome(s) | Done | Anonymous computer‐administered questionnaire (p. 293) |
| c) Completeness of data set | Unclear | |
| d) Reliable primary outcome measure(s) | Done | 30‐day use of marijuana, attitudes, beliefs, intentions |
| Idaho Meth 2010, Colorado Meth 2011, Georgia Meth 2011, Hawaii Meth 2011 and Wyoming Meth 2011 | ||
| Criterion | Score | Notes |
| a) Protection against secular changes | ||
| The intervention is independent of other changes | Unclear | |
| There are sufficient data points to enable reliable statistical inference | Done | Data points for each study ranged from 2 to 4 including only one baseline survey. However, overall, there are a sufficient number of observations |
| Formal test for trend. Complete this section if authors have used ANOVA modelling | Not done | |
| b) Protection against detection bias | ||
| Intervention unlikely to affect data collection | Done | Despite some slight changes, methodology of data collection is consistent across studies and across data points |
| Blinded assessment of primary outcome(s) | Done | Anonymous questionnaires |
| c) Completeness of data set | Unclear | Not applicable |
| d) Reliable primary outcome measure(s) | Done | Past‐month use of marijuana, attitudes, perceptions |
| Carpenter 2011 | ||
| Criterion | Score | Notes |
| a) Protection against secular changes | ||
| The intervention is independent of other changes | Done | Adjustment by many individual and market variables (page 949) |
| There are sufficient data points to enable reliable statistical inference | Not done | 3 data points (page 949) |
| Formal test for trend. Complete this section if authors have used ANOVA modelling | Done | "multivariate logistic regression" (page 949) |
| b) Protection against detection bias | ||
| Intervention unlikely to affect data collection | Done | Ads were broadcasted independently on the surveys |
| Blinded assessment of primary outcome(s) | Done | Monitoring the Future (MTF) surveys used anonymous questionnaires |
| c) Completeness of data set | Unclear | |
| d) Reliable primary outcome measure(s) | Done | Past‐month and lifetime marijuana use (page 951) |
Overall the quality of the included RCTs is acceptable: the stronger dimension is the consideration of risk of attrition bias (incomplete data addressed in the discussion) and the weaker dimension the risk of selection bias (unclear description of method for randomisation). More than half of the studies were clearly free of selective outcome reporting. In one case (Schwinn 2010) there was a clear indication of potential high risk of reporting bias.
Other potential sources of bias
Ecological factors are likely to interfere with the effect of a media campaign. These factors can include exposures to other media campaigns (advertisements), films or mass media debates directly addressing illicit drugs or other factors acting indirectly (for example, a popular singer who dies from an overdose).
Interrupted time series (ITS) and before and after studies (CBA)
Six studies are ITS and two studies are CBA. The results of their 'Risk of bias' assessments are presented in Figure 4 and Figure 5.
4.

Interrupted time series 'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
5.
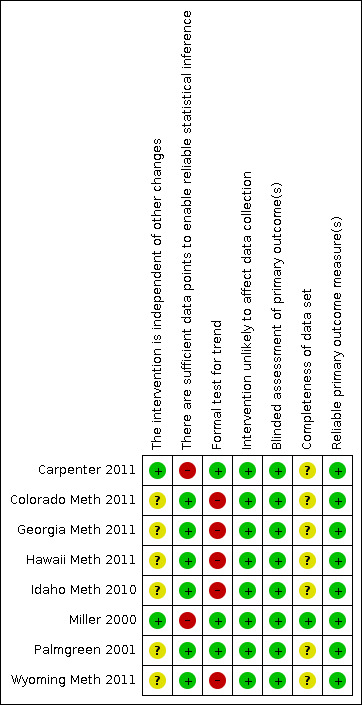
Interrupted time series 'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Overall the studies reported sufficient data points to enable reliable statistical inferences; they also had good strategies to ensure anonymous or computer‐administered questionnaires and to ensure that interventions did not affect data collection. The reliability of primary outcome measures was also satisfactory for all the studies. The weaker points were the lack of a formal test for trends and the unclear completeness of the data sets for many studies.
Prospective cohort studies (PCS)
Three studies are cohort studies and one of them is a mixed RCT‐cohort study (Slater 2011). The results of their 'Risk of bias' assessments are presented in Table 2, Figure 6 and Figure 7.
2. 'Risk of bias' assessment of cohort studies (Hornik 2006, Scheier 2010, Slater 2011).
| Hornik 2006 | ||
| Criterion | Score/Info | Notes |
| In a well‐conducted cohort study: | ||
| The study addresses an appropriate and clearly focused question | Well covered | "We examined the cognitive and behavioral effects of the National Youth Anti‐Drug Media Campaign on youths aged 12.5 to 18 years and report core evaluation results", abstract |
| Selection of subjects | ||
| The 2 groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation | Well covered | "The sample was selected to provide an efficient and nearly unbiased cross‐section of US youths and their parents. Respondents were selected through a stratified 4‐stage probability sample design: 90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2229‐30 |
| The study indicates how many of the people asked to take part did so, in each of the groups being studied | Well covered | Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, Appendix A, page A‐6, table A‐1 and page A‐11 tables A‐8 to A‐10 |
| The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis | Well covered | "Analyses were restricted to youths who were nonusers of marijuana at the current round (for cross‐sectional analyses) or at the previous round (for lagged analyses).", page 2232 |
| What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed | 35% | "The overall response rate among youths for the first round was 65%, with 86% to 93% of still eligible youths interviewed in subsequent rounds.", page 2230 Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, page 2‐12, table 2‐A "Completed interviews by wave" |
| Comparison is made between full participants and those lost to follow‐up, by exposure status | Not reported | |
| Assessment | ||
| The outcomes are clearly defined | Well covered | "For 3 reasons, all drug‐related measures reported here relate to marijuana use. [..] Four measures or indices represented the following constructs: (1) marijuana intentions, (2) marijuana beliefs and attitudes, (3) social norms, and (4) self‐efficacy to resist use.", page 2230 |
| The assessment of outcome is made blind to exposure status | Not applicable | Blinding to exposure status was not applicable for this study |
| Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome | Well covered | "A measure of general exposure to antidrug advertising was derived from responses to questions about advertising recall for each medium or media grouping: television and radio, print, movie theatres or videos, and outdoor advertising.", page 2230 |
| The measure of assessment of exposure is reliable | Well covered | "For 3 reasons, all drug‐related measures reported here relate to marijuana use.", page 2230 |
| Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable | Well covered | "For 3 reasons, all drug‐related measures reported here relate to marijuana use. First, marijuana is by far the illicit drug most heavily used by youths. Second, for other drugs, the low levels of use meant that the NSPY sample sizes were not large enough to detect meaningful changes in use with adequate power. Third, to the extent that the campaign did target a specific drug, it was almost always marijuana. [..] The cognitive measures were developed on the basis of 2 health behavior theories, the theory of reasoned action and social cognitive theory", page 2230 |
| Exposure level or prognostic factor is assessed more than once | Well covered | "3 nationally representative cohorts of US youths aged 9 to 18 years were surveyed at home 4 times.", abstract |
| Confounding | ||
| The main potential confounders are identified and taken into account in the design and analysis | Well covered | "Potential confounder measures. The analyses employed propensity scoring for confounder control by weighting adjustments,9–14 incorporating a wide range of standard demographic variables and variables known to be related to youths' drug use or thought likely to be related to exposure to antidrug messages. Propensity scores were developed for the general and specific exposure measures. More than 150 variables were considered possible confounders.", page 2231 |
| Statistical analysis | ||
| Have confidence intervals been provided? | Well covered | Tables 1‐4, pages 2233‐4 |
| Overall assessment of the study | ||
| How well was the study done to minimise the risk of bias or confounding, and to establish a causal relationship between exposure and effect? Code ++,+, or − |
++ | Propensity scoring from 150 confounders, page 2231 |
| Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the exposure being investigated? | Yes | This study includes very good control for possible confounders |
| Are the results of this study directly applicable to the patient group targeted in this guideline? | Unclear | Results are applicable to US youth; it is unclear whether they are generalisable outside the US |
| Description of the study | ||
| Do we know who the study was funded by? | Public Funds (NIDA), Government (Congress) | "Research for and preparation of this article were supported by the National Institute on Drug Abuse (grants 3‐N01‐DA085063‐002 and 1‐R03‐DA‐020893‐01). The evaluation of the National Youth Anti‐Drug Media Campaign was funded by Congress as part of the original appropriation for the campaign. The White House Office of National Drug Control Policy directly supervised the campaign. The National Institute on Drug Abuse supervised the evaluation; Westat, with the Annenberg School for Communication at the University of Pennsylvania as a subcontractor, received the contract. All authors were funded for this evaluation and other projects by the National Institute on Drug Abuse.", page 2235 |
| How many centres are patients recruited from? | USA as a whole | "90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2230 |
| From which countries are patients selected? (Select all those involved. Note additional countries after 'Other') | USA | |
| What is the social setting (i.e. type of environment in which they live) of patients in the study? | Mixed | "More than 150 variables were considered possible confounders. [..] They include [..] urban–rural residency; [..]", page 2231 |
| What criteria are used to decide who should be INCLUDED in the study? | 4‐stage selection | "Respondents were selected through a stratified 4‐stage probability sample design: 90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2229‐30 |
| What criteria are used to decide who should be EXCLUDED from the study? | Youth living in boarding schools and college dormitories | "As mentioned previously, youth residing in group quarters were not eligible for selection in any of the three recruitment waves. Thus, youth living in boarding schools and college dormitories were excluded from the scope of the survey. This exclusion was made because it was felt that dormitory residents could not be easily interviewed at their parents' homes and that their experiences were so", Report, A‐10 |
| What intervention or risk factor is investigated in the study? (Include dosage where appropriate) | The National Youth Anti‐Drug Media Campaign | |
| What comparisons are made in the study (i.e. what alternative treatments are used to compare the intervention/exposure with). Include dosage where appropriate | Lower exposure versus higher exposure to anti‐drug campaign | "The analyses reported here were based on 3 types of measures: recalled exposure to antidrug messages aired by the campaign and other sources; cognitions and behavior related to marijuana, as outcomes; and individual and household characteristics, including a wide range of variables known to be related to drug cognitions and use and to exposure to antidrug messages.", page 2230 |
| What methods were used to randomise patients, blind patients or investigators, and to conceal the randomisation process from investigators? | Randomisation: not applicable, but propensity scoring was employed Blinding of patients: not applicable Blinding of investigators: not reported Randomisation concealment: not applicable |
|
| How long did the active phase of the study last? | September 1999 to June 2004 (58 months) | |
| How long were patients followed up for, during and after the study? | November 1999 to June 2004 (56 months). | |
| List the key characteristics of the patient population. Note if there are any significant differences between different arms of the trial | Representative of US youths aged 9 to 18 | "The sample was selected to provide an efficient and nearly unbiased cross‐section of US youths and their parents", page 2229 |
| Record the basic data for each arm of the study. If there are more than 4 arms, note data for subsequent arms at the bottom of the page | Tables 1‐4, pages 2233‐4 | |
| Record the basic data for each IMPORTANT outcome in the study. If there are more than 4, note data for additional outcomes at the bottom of the page | Tables 1‐4, pages 2233‐4 | |
| Notes. Summarise the authors' conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question | Through June 2004, the campaign is unlikely to have had favourable effects on youths and may have had delayed unfavourable effects The evaluation challenges the usefulness of the campaign |
|
| Scheier 2010 | ||
| Criterion | Score/Info | Notes |
| In a well‐conducted cohort study: | ||
| The study addresses an appropriate and clearly focused question | Well covered | "In this study, we examined whether awareness (recall) of the National Youth Anti‐Drug Media Campaign (NYADMC) benefited youth by attenuating their drug use.", abstract |
| Selection of subjects | ||
| The 2 groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation | Well covered | Same as Hornik 2008 ("The sample was selected to provide an efficient and nearly unbiased cross‐section of US youths and their parents. Respondents were selected through a stratified 4‐stage probability sample design: 90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2229‐30) |
| The study indicates how many of the people asked to take part did so, in each of the groups being studied | Well covered | Same as Hornik 2008 (Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, Appendix A, page A‐6, table A‐1 and page A‐11 tables A‐8 to A‐10) |
| The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis | Well covered | Same questionnaire was administered at baseline and at follow‐up. "National Survey of Parents and Youth (NSPY) [..] could be used to assess youths' awareness of the campaign messages and monitor any corresponding changes in drug use trends.", page 241‐2 |
| What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed | 35% | Same as Hornik 2008 ("The overall response rate among youths for the first round was 65%, with 86% to 93% of still eligible youths interviewed in subsequent rounds. ", page 2230 Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, page 2‐12, table 2‐A "Completed interviews by wave") |
| Comparison is made between full participants and those lost to follow‐up, by exposure status | Well covered | "Attrition analyses were structured to determine whether certain factors operate systematically to cause dropout from the study. Proportional analyses using the v2 test were used for cross tabulation of binary measures and logistic regression modelling to examine the optimal predictors of retention (coded '1' stay and '0' dropout). We used the WesVar software program to estimate logistic regression models of panel attrition. This statistical modelling program enables us to adjust (through poststratification) the sample variance estimators for the undersampling of primary sampling units and correct any bias in parameter estimates related directly to the complex sampling design (using replicate variance estimators to adjust standard errors for design effects). Proportional tests indicated that panel youth were significantly more likely to be female, smoke more cigarettes, drink alcohol, and smoke marijuana (all v2 proportional tests significant at the p .0001) compared with dropout youth. Given the large number of variables possibly related to retention status, logistic models were run separately for five individual domains (demographics, campaign awareness, drug use, school‐related factors, and psychosocial risk).7 Following tests of the individual domains, we culled only significant predictors and tested these in a combined model predicting retention. The final model indicated that retained youth were less at risk for marijuana use (unstandardized b =‐3.51, p<= .0001, OR =.03), engaged in more antisocial behavior (evidencing suppression: [b = .23, p <=.0001, OR = 1.26]), spent fewer hours listening to the radio on a daily basis (b =‐.09, p <=.01, OR = .91), and were more likely to have attended school in the past year (b = 1.05, p<= .01, OR = 2.87) compared with their dropout counterparts. Using the Cox‐Snell likelihood pseudo‐R2 statistic, the model accounted for 12% of the variance in retention status, F(14,87) = 12.127, p <=.0001.", page 250 |
| Assessment | ||
| The outcomes are clearly defined | Well covered | "Assessment of alcohol and drug use relied on an Anonymous Computer Assisted Self‐report Interview (ACASI). Two alcohol use items6 assessed being drunk or high ("How many times were you drunk or very high from alcohol in the last 12 months?") with response categories ranging from "I don't use alcohol" (0) through "40 or more occasions" (7); and heavy alcohol use based on a measure of binge drinking ("How many days have you had five or more drinks in the last 30 days?") with response categories ranging from "I don't drink" (0) through "10 or more times" (6). Cigarette use was assessed with a single item ("How many cigarettes smoked a day during the last 30 days?") with response categories ranging from "None" (0) through "More than 35 per day, about 2 packs or more" (7). A single frequency item assessed marijuana involvement ("How many times have you used marijuana in the last 12 months?") with response categories ranging from "I have never used marijuana" (0) through "40 or more occasions" (6).", page 248 |
| The assessment of outcome is made blind to exposure status | Not applicable | Blinding to exposure status was not applicable for this study |
| Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome | Not reported | |
| The measure of assessment of exposure is reliable | Well covered | "Turning to the campaign awareness parameters, we see two findings worth noting. First, growth in campaign awareness is positive for the earlier years (12 to 14), except for television viewing behavior, which had a slope not significantly different from zero. As these youth became older (14 to 18), their awareness declined for every media venue except specific recall (videos shown on laptops) and radio listening behavior. Also, the magnitude of the slope terms were considerably larger at the younger age for recall of stories about drugs and youth, brand awareness, specific recall, and radio listening but larger in magnitude for television (declining) as these youth transitioned to high school.", page 253 "Figure 2 graphically presents a generic template for testing the bivariate cohort growth models. Again, two slope trends are posited to capture the different rates of growth for youth when they were younger versus when they were older, and this is repeated for both drug use (D) and awareness (A) measures.", page 253 |
| Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable | Well covered | "Assessment of alcohol and drug use relied on an Anonymous Computer Assisted Self‐report Interview (ACASI). Two alcohol use items6 assessed being drunk or high ("How many times were you drunk or very high from alcohol in the last 12 months?") with response categories ranging from "I don't use alcohol" (0) through "40 or more occasions" (7); and heavy alcohol use based on a measure of binge drinking ("How many days have you had five or more drinks in the last 30 days?") with response categories ranging from "I don't drink" (0) through "10 or more times" (6). Cigarette use was assessed with a single item ("How many cigarettes smoked a day during the last 30 days?") with response categories ranging from "None" (0) through "More than 35 per day, about 2 packs or more" (7). A single frequency item assessed marijuana involvement ("How many times have you used marijuana in the last 12 months?") with response categories ranging from "I have never used marijuana" (0) through "40 or more occasions" (6).", page 248 |
| Exposure level or prognostic factor is assessed more than once | Well covered | Yes: 4 rounds of data collection. Table 1, page 249 |
| Confounding | ||
| The main potential confounders are identified and taken into account in the design and analysis | Not reported | |
| Statistical analysis | ||
| Have confidence intervals been provided? | No | Page 264 |
| Overall assessment of the study | ||
| How well was the study done to minimise the risk of bias or confounding, and to establish a causal relationship between exposure and effect? Code ++, +, or − |
‐ | "...there was no "intervention" to speak of, but rather the campaign took shape as a naturalistic observational study conducted at a particular point in time with no clear demarcation from various historical influences that could affect patterns of reported drug use", page 264 |
| Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the exposure being investigated? | No, because no adjustment for confounders was reported | |
| Are the results of this study directly applicable to the patient group targeted in this guideline? | Unclear | Results are applicable to US youth; it is unclear whether they are generalisable outside the US |
| Description of the study | ||
| Do we know who the study was funded by? | No | |
| How many centres are patients recruited from? | USA as a whole | Same as Hornik 2008 ("90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2230) |
| From which countries are patients selected? (Select all those involved. Note additional countries after 'Other') | USA | |
| What is the social setting (i.e. type of environment in which they live) of patients in the study? | Mixed | Same as Hornik 2008 ("More than 150 variables were considered possible confounders. [..] They include [..] urban–rural residency; [..]", page 2231) |
| What criteria are used to decide who should be INCLUDED in the study? | 4‐stage selection | Same as Hornik 2008 ("Respondents were selected through a stratified 4‐stage probability sample design: 90 primary sampling units—typically county size—were selected at the first stage, geographical segments were selected within the sampled primary sampling units at the second stage, households were selected within the sampled segments at the third stage, and then, at the final stage, 1 or 2 youths were selected within each sampled household, as well as 1 parent in that household.", page 2229‐30) |
| What criteria are used to decide who should be EXCLUDED from the study? | Youth living in boarding schools and college dormitories | Same as Hornik 2008 ("As mentioned previously, youth residing in group quarters were not eligible for selection in any of the three recruitment waves. Thus, youth living in boarding schools and college dormitories were excluded from the scope of the survey. This exclusion was made because it was felt that dormitory residents could not be easily interviewed at their parents' homes and that their experiences were so", Report, Appendix A, A‐10) |
| What intervention or risk factor is investigated in the study? (Include dosage where appropriate) | The National Youth Anti‐Drug Media Campaign | "...there was no "intervention" to speak of, but rather the campaign took shape as a naturalistic observational study conducted at a particular point in time with no clear demarcation from various historical influences that could affect patterns of reported drug use", page 264 |
| What comparisons are made in the study (i.e. what alternative treatments are used to compare the intervention/exposure with). Include dosage where appropriate | Exposure versus drug use | Varius models, e.g. see page 256 |
| What methods were used to randomise patients, blind patients or investigators, and to conceal the randomisation process from investigators? | Randomisation: not applicable Blinding of patients: not applicable Blinding of investigators: not reported Randomisation concealment: not applicable | |
| How long did the active phase of the study last? | September 1999 to June 2004 (58 months) | |
| How long were patients followed up for, during and after the study? | November 1999 to June 2004 (56 months) | |
| List the key characteristics of the patient population. Note if there are any significant differences between different arms of the trial | Representative of US youths aged 9 to 18 | Same as Hornik 2008 ("The sample was selected to provide an efficient and nearly unbiased cross‐section of US youths and their parents", page 2229) |
| Record the basic data for each arm of the study. If there are more than 4 arms, note data for subsequent arms at the bottom of the page | Table 2, page 251 | |
| Record the basic data for each IMPORTANT outcome in the study. If there are more than 4, note data for additional outcomes at the bottom of the page | Tables 3‐4‐5, pages 252‐7 | |
| Notes. Summarise the authors' conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question | When they were younger, these youth accelerated their drug use and reported increasing amounts of campaign awareness. When they were older, [..] no effects for marijuana were significant but trended in the direction of increased awareness associated with declining drug use |
"Behavior change is guided by the Theory of Reasoned Action (TRA: Ajzen & Fishbein, 1973, 1977) and draws also from social persuasion (McGuire, 1961, 1966, 1968) and communication theories (Hovland, Janis, & Kelley, 1953). According to the TRA, the influence of attitudes (i.e., subjective evaluations of behavior consequences) and beliefs (subjective norms and behavioral outcomes or expectancies) on behavior is mediated through intentions (i.e., future intent to engage the behavior). In other words, youth form impressions of whether drugs are good or bad, and they combine this information with normative beliefs (whether their close friends approve of drug use) and behavioral expectations (perceived benefits and negative consequences of drug use) toward drug use. These steps are necessary but not sufficient conditions, as the final decision to use drugs is guided by their behavioral willingness or intentions.", page 242 "To date, analyses of the media campaign efficacy have used traditional linear regression or correlation techniques to examine campaign effects. While this tactic has been useful to delineate the basic statistical associations between campaign awareness and drug use, a major weakness of this approach is that it fails to provide a developmental perspective and incorporate systematic features of change in either awareness or drug use.[..] Growth modelling is clearly a more definitive way to address the question of change and increasingly has been advocated as a means to assess prevention effects that unfold over time (Brown, Catalano, Fleming, Haggerty, & Abbott, 2005; Mason, Kosterman, Hawkins, Haggerty, & Spoth, 2003; Park et al., 2000; Taylor, Graham, Cumsille, & Hansen, 2000). [..] The age mixture within each round makes it imperative to estimate growth using age‐ cohort models", page 242‐3 |
| Slater 2011 | ||
| Criterion | Score/Info | Notes |
| In a well‐conducted cohort study: | ||
| The study addresses an appropriate and clearly focused question | Well covered | "...(a) provide two simultaneous tests of autonomy and aspiration perceptions as mediators of impact on marijuana use as a consequence of exposure to each of these campaigns, b) conduct the first independent assessment of the ONDCP media campaign, which did not have a formal independent evaluation in place during the years of this study, and c) assess the simultaneous impact of a national campaign and a similar community/in‐school effort.", page 12‐13 |
| Selection of subjects | ||
| The 2 groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation | Not reported | "3,236 students participated in at least one survey, with 48% males, 52% females and a mean age at baseline of 12.4 years (SD = 0.6); 75% were European‐American, 11.5% African‐American, and 13.5% of other racial backgrounds. One‐quarter of the youth were of Hispanic ethnicity.", page 15 |
| The study indicates how many of the people asked to take part did so, in each of the groups being studied | Poorly addressed | Only average: "The average rate of student participation in each school was 32% of total student enrolment, lower than the prior study because of stricter IRB requirements being imposed on recruitment procedures. 57.1% of respondents provided data at all four measurement occasions; 27.2% provided data on three, 9.4% provided data on two and 5.3% provided data on just one of the measurement occasions. Missed surveys appear to be a matter more of absenteeism or slips in getting students to survey sessions, than of panel mortality; 84.5% of participants filled out the wave 1 survey, 86.2% wave 2, 86.1% wave 3, and 81.3% wave 4.", page 15 |
| The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis | Well covered | "Lifetime use of marijuana was measured at each measurement wave [..]", page 15 |
| What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed | 42.9% | "The average rate of student participation in each school was 32% of total student enrolment, lower than the prior study because of stricter IRB requirements being imposed on recruitment procedures. 57.1% of respondents provided data at all four measurement occasions; 27.2% provided data on three, 9.4% provided data on two and 5.3% provided data on just one of the measurement occasions. Missed surveys appear to be a matter more of absenteeism or slips in getting students to survey sessions, than of panel mortality; 84.5% of participants filled out the wave 1 survey, 86.2% wave 2, 86.1% wave 3, and 81.3% wave 4.", page 15 |
| Comparison is made between full participants and those lost to follow‐up, by exposure status | Not reported | |
| Assessment | ||
| The outcomes are clearly defined | Well covered | "Autonomy and Aspirations Inconsistent With Marijuana Use Autonomy inconsistent with marijuana use was measured using responses to four items following the phrase "Not using marijuana": 1) is a way to be true to myself; 2) is an important part of who I am; 3) is a way of being in control of my life; and 4) is a way of showing my own independence, where responses ranged from 1 = definitely disagree to 4 = definitely agree. Similarly, aspirations inconsistent with marijuana use were measured using the responses to three items following the phrase "Using marijuana would: 1) keep me from doing the things I want to; 2) mess up my plans for when I am older; and 3) get in the way of what is important to me." Because responses to each scale's items were heavily skewed, with 82% of respondents selecting "definitely agree" for all aspiration items and 84% of respondents selecting "definitely agree" for all autonomy items, each scale was dichotomized such that a "1" was assigned if all responses to the scale items were "definitely agree" and a "0" otherwise. The Cronbach's alpha values (Cronbach 1951) for each dichotomized measure were .9 or greater at each of the four waves. Marijuana Use Lifetime use of marijuana was measured at each measurement wave using four questions: "How old were you the first time you used marijuana?", "How often in the last month have you used marijuana?", "How often in the last 3 months have you used marijuana?", and "Have you ever tried marijuana? (pot, grass, hash, etc.)?" If a subject responded affirmatively to any one question (or indicated an age when they first used marijuana), lifetime marijuana use was scored a "1", while an indication of never using marijuana resulted in a score of "0". The reliability for the scale was above 0.7 for the first two measurement occasions, .64 on the third occasion, and .69 at the fourth occasion.", page 15 |
| The assessment of outcome is made blind to exposure status | Not applicable | Blinding to exposure status was not applicable for this study |
| Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome | Not reported | |
| The measure of assessment of exposure is reliable | Well covered | p. 15 |
| Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable | Well covered | = 1.7 |
| Exposure level or prognostic factor is assessed more than once | Well covered | 4 waves, page 17 |
| Confounding | ||
| The main potential confounders are identified and taken into account in the design and analysis | Adequately addresses | p. 16 |
| Statistical analysis | ||
| Have confidence intervals been provided? | Well covered | Standard errors, e.g. Table 1 and 2, p. 18 |
| Overall assessment of the study | ||
| How well was the study done to minimise the risk of bias or confounding, and to establish a causal relationship between exposure and effect? Code ++, +, or − |
+ | |
| Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the exposure being investigated? | Fairly: selectivity (do no know if representative); no propensity scoring for national media campaign | |
| Are the results of this study directly applicable to the patient group targeted in this guideline? | Unclear | Results are applicable to US youth; it is unclear whether they are generalisable outside the US |
| Description of the study | ||
| Do we know who the study was funded by? | Public Funds (NIDA) | "This research was supported by grant DA12360 from the National Institute on Drug Abuse (NIDA) to the first author.", page 12 |
| How many centres are patients recruited from? | 20 communities | |
| From which countries are patients selected? (Select all those involved. Note additional countries after 'Other') | USA | |
| What is the social setting (i.e. type of environment in which they live) of patients in the study? | Mixed | p. 14 |
| What criteria are used to decide who should be INCLUDED in the study? | IRB requirements | "The average rate of student participation in each school was 32% of total student enrolment, lower than the prior study because of stricter IRB requirements being imposed on recruitment procedures", page 15 |
| What criteria are used to decide who should be EXCLUDED from the study? | Exaggerators | "Students who responded that they had tried all drugs listed including one that had been invented were considered exaggerators and were excluded from analyses; there were no more than 0.4% of such exaggerators in any given wave of data collection.", page 15 |
| What intervention or risk factor is investigated in the study? (Include dosage where appropriate) | (a) school‐ and community‐based media intervention 'Be Under Your Influence' and (b) national anti‐drug media campaign 'Above the Influence' | p. 12 |
| What comparisons are made in the study (i.e. what alternative treatments are used to compare the intervention/exposure with). Include dosage where appropriate | Exposure versus drug use/aspirations/autonomy; exposure x time versus drug use/aspirations/autonomy | |
| What methods were used to randomise patients, blind patients or investigators, and to conceal the randomisation process from investigators? | Randomisation: not applicable for mass media campaign, but done for 'Be Under Your Own Influence' school‐ and community‐based media intervention | |
| How long did the active phase of the study last? | Autumn 2005 to Spring 2009 (˜42 months) | |
| How long were patients followed up for, during and after the study? | 24 months | |
| List the key characteristics of the patient population. Note if there are any significant differences between different arms of the trial | 48% males, 52% females and a mean age at baseline of 12.4 years (SD = 0.6); 75% were European‐American, 11.5% African‐American, and 13.5% of other racial backgrounds One‐quarter of the youth were of Hispanic ethnicity | p. 15 |
| Record the basic data for each arm of the study. If there are more than 4 arms, note data for subsequent arms at the bottom of the page | Table 1 and 2, page 18 | |
| Record the basic data for each IMPORTANT outcome in the study. If there are more than 4, note data for additional outcomes at the bottom of the page | Table 1 and 2, page 18 | |
| Notes. Summarise the authors' conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question | Results indicate that earlier effects of the 'Be Under Your Own Influence' intervention replicated only in part and that the most plausible explanation of the weaker effects is high exposure to the similar but more extensive ONDCP 'Above the Influence' national campaign. Self reported exposure to the ONDCP campaign predicted reduced marijuana use, and analyses partially support indirect effects of the 2 campaigns via aspirations and autonomy | |
SD: standard deviation
IRB= Institutional Review Board, is a committee that has been formally designated to approve, monitor, and review biomedical and behavioralresearch involving humans
6.

Prospective cohort studies 'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
7.

Prospective cohort studies 'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Overall, all PCS addressed an appropriate and clearly focused question. In two studies subjects were selected with proper procedures in order to make them comparable in all respects. The same two studies indicated how many of the people asked to take part actually participated in the study. One study (Slater 2011) failed to address these issues. Attrition was 35% in two studies and 42.9% in Slater 2011. Comparison between participants and those lost to follow‐up was made only in Scheier 2010.
Assessment
The outcomes were clearly defined in all studies. Blinding to exposure status was not applicable for any of the studies. In one study (Hornik 2006) there was some recognition that knowledge of exposure status could have influenced the assessment of the outcomes. In all studies the measure of assessment of exposure was reliable: evidence from other sources was used to demonstrate that the method of outcome assessment was valid and reliable, and exposure level or prognostic factor was assessed more than once.
Confounding
The main potential confounders were adequately identified and taken into account in two studies (Hornik 2006; Slater 2011).
Statistical analysis
Confidence intervals were provided in two studies. One study reported only P values (Scheier 2010).
Overall assessment of the study
One study did very well in addressing the risk of bias or confounding (Hornik 2006), one did quite well (Slater 2011) and one did not adjust for potential confounders (Scheier 2010).
Effects of interventions
Primary outcomes
Self reported or biomarker‐assessed illicit drug use
This primary outcome is measured in 15 studies: five randomised controlled trials (RCT) + one RCT and prospective cohort study; two prospective cohort studies; six interrupted time series (ITS) and one controlled before and after (CBA) study.
The five RCTs (Fang 2010; Lee 2010; Newton 2010; Schwinn 2010; Slater 2006) enrolled 5470 young people and were included in a meta‐analysis (see Figure 8). Their pooled results show no effect of media campaign intervention (standardised mean difference (SMD) ‐ 0.02; 95% confidence interval (CI) ‐0.15 to 0.12, heterogeneity P = 0.02) (Analysis 1.1). Youngsters exposed to a media campaign tend to use, on average, fewer illicit substances measured through an array of published and unpublished scales including the American Drug and Alcohol Survey (Centers for Disease Control and Prevention), Youth Risk Behavior Survey, Australian National Drug Strategy Household Survey and Global Appraisal of Individual Needs‐I (see Table 3).
8.

Forest plot of comparison: 1 Mass media versus no mass media intervention (RCT), outcome: 1.1 Drug use.
1.1. Analysis.

Comparison 1 Mass media versus no mass media intervention (RCT), Outcome 1 Drug use.
3. Measurement scales used in included studies.
| Study | Was a specific scale developed? (Yes/no/unclear) | Measurement scale(s) used | Reference | Was the scale adapted? (Yes/no/unclear) |
| Palmgreen 1991 | No | Sensation seeking Scale, Form V | Zuckerman, M (1979). Sensation seeking: beyond the optimal level of arousal. Hillsdale, NJ:Lawrence Erlbaum Associates, Inc. | No |
| No | Instruments used in a continuing survey of young people by the Institute for Social Research at the University of Michigan (NB to measure levels of use of illicit drugs) | Johnston LD, Bachman JG, O'Malley PM (1982). Monitoring the future: questionnaire responses from the nations' high school seniors, 1981. Ann Arbor: University of Michigan, Survey Response Centre, Institute for Social Research | Yes | |
| Yes | Behavioural Intention Index p. 221 "immediately after the second viewing of the PSA, subjects were asked "If you wanted information about alternatives to drug use, how likely it is, on a scale of 1 to 5, that you would call na 800 hotline?" | n/a | n/a | |
| Yes | Attitude towards drug use p. 222 "After behavioural intention was measured, subjects were asked to indicate on a scale of 1 to 5 how they felt about their personal use of drugs in relation to each of six adjectives word pairs." | n/a | n/a | |
| Kelly 1992 | Unclear | Not mentioned | n/a | n/a |
| Polansky 1999 | No | Drug Attitude Scale (12 items on a Likert scale) | Swisher JD, Horan JJ (1973). The Pennsylvania State University Evaluation Scales. In LA Abrams, E Garfield & JD Swisher (eds). Accountability in drug education: a model for evaluation (pp 87‐99). Washington, DC: Drug Abuse Council | Unclear (: in the text is mentioned "updated version" but no further clarification) |
| No | Tentative Drug Use Scale (10 items scale) | Horan JJ, Williams JM (1975). The tentative drug use scale: a quick and relatively problem free outcome measure for drug abuse prevention projects. Journal of Drug education; 5: 381‐4 | No | |
| Yes | Help‐Seeking Questionnaire and Knowledge Questionnaire p. 190 "two 10‐items achievement rests were developed for this study" | n/a | n/a | |
| No | Drug Conformity Scale (16 questions reflecting varying levels of assertive competency) | Horan JJ, Williams JM (1982). Longitudinal study of assertion training as a drug abuse prevention strategy. American Educational Research Journal; 19: 341‐51 | No | |
| Palmgreen 2001 (Stephenson 1999) | Yes | Beliefs 12 marijuana‐related beliefs about occasional use of marijuana and 12 belief items about regular marijuana use were assessed on a 4‐point scale with the response options of disagree strongly, disagree somewhat, agree somewhat and agree strongly | n/a | n/a |
| Yes | Attitudes Seven marijuana‐related attitudes about occasional use and 7 items about regular use were assessed on a 4‐point scale, with the response options of disagree strongly, disagree somewhat, agree somewhat and agree strongly | n/a | n/a | |
| Yes | Intentions Participants were asked their intent to engage in experimental or regular marijuana use in the future. With 2 items on a 3‐point scale with the response options probably will not, probably will and definitely will | n/a | n/a | |
| Miller 2000 | Yes | Use Recent drug use was measured by asking respondents about the frequency and recency with which they used 10 types of drugs (using commonly recognised names): cannabis, cocaine, other stimulants, tranquillisers, sedative‐hypnotics, hallucinogens, opioids, phencyclidine, amyl and butyl nitrates and inhalants such as glue, paint or gasoline (4‐ point scale ranging from 1 = never to 4 = at least once in the past month) | n/a | n/a |
| Yes | Risks perception Risk assessment included 13 items regarding the extent to which students perceived risk or consequences related to alcohol or other drug use. Personal risk for alcohol and other drug problems was judged relative to students' perceptions of "most people" (ranging from 1 = higher than most people to 3 = lower than most people) | n/a | n/a | |
| Palmgreen 2001 | No | Brief Sensation Seeking Scale | Hoyle RH, Stephenson MT. The sensation seeking scale for adolescents. In: Lennox RD, Scott‐Lennox JA, Cutler BL, eds. Applied Psychometrics for Health Outcomes Research. Chapel Hill, NC: Health Statistics Lab. | No |
| Fishbein 2002 | Yes | Specifically developed instrument p. 241 "the instrument for the study consisted of questionnaire with 3 parts." First: demographic questions Second: series of questions on realism/content/recall of intervention Third: assessment of the respondent perceptions of the danger and harmful effects of engaging in 8 risky behaviours ‐ perceived danger = 1 item per behaviour on yes/no basis ‐ perceived harmfulness = 1 item per behaviour on a 5‐point scale ‐ perceived norms = 1 item per behaviour on a 5‐point scale | n/a | n/a |
| Yzer 2003 | Yes | A specific questionnaire was developed for the study. Available upon request by the authors (p. 135) Intention to use marijuana: 1 to 2 (depending on the first answer) items using a 4‐point scale Attitude: 4 items using a 7‐point scale Outcome beliefs: 36 items using a 5‐point scale | n/a | n/a |
| Slater 2006 | No | Selected items from the American Drug and Alcohol Survey Alcohol lifetime score: 3 items Smoking lifetime score: 3 items Marijuana lifetime score: 5 items | American Drug and Alcohol Survey, with permission by the Rocky Mountain Behavioural Science Institute | No |
| Zhao 2006 | Yes | Intentions not to use/to reduce use/to stop use | n/a | No |
| Unclear | Attitudes towards illicit drug use: 7‐point scale from ‐3 (bad/foolish/...) to +3 (good/wise/...) | n/a | n/a | |
| Yes | Perceptions (including perceptions of peer norms and perceptions about illicit drug use): 5‐point scales from ‐2 to +2. "Although we did some analyses at the level of individual beliefs, we generally used two types of belief clusters in our analyses" | n/a | No | |
| Czyzewska 2007 | Unclear | Declared intention to use marijuana | n/a | |
| Unclear | Attitudes towards illicit drug use (pre‐test explicit attitudes): 10‐point Likert scales | n/a | ||
| Yes | Attitudes towards illicit drug use (post‐test implicit attitudes): IAT test. "Two computerized Implicit Association Tests (IAT) were designed to assess implicit attitudes to tobacco and marijuana. [..] The only difference to the standard IAT procedure was the extended number of practice trials to 40 in order to reduce the typical effect of order in which the combined categorization tasks are performed" | See Table 1 for IAT test content Scale was adapted from: Greenwald AG, McGhee DE, Schwartz JLK (1998). Measuring individual differences in social cognition: The Implicit Association Test. Journal of Personality and Social Psychology; 74: 1464‐80 With updates from: Greenwald AG, Nosek BA, Banaij MR (2003). Understanding and using the Implicit Association Test: An improved scoring algorithm. Journal of Personality and Social Psychology; 85(2):197‐216 |
Yes | |
| Unclear | Attitudes towards illicit drug use (post‐test explicit attitudes): 3 sets of 7 5‐point scales (= 21 5‐point scales) | n/a | ||
| Hornik 2006 | No | National Survey of Parents and Youth (NSPY). 3 types of measures: recalled exposure to anti‐drug messages aired by the campaign and other sources; cognitions and behavior related to marijuana, as outcomes; and individual and household characteristics, including a wide range of variables known to be related to drug cognitions and use and to exposure to anti‐drug messages | http://archives.drugabuse.gov/initiatives/westat/ | No |
| Scheier 2010 | Yes | Alcohol and Drug Use Assessment of alcohol and drug use relied on an Anonymous Computer Assisted Self‐report Interview (ACASI) | n/a | n/a |
| Fang 2010 | No | Occasions of use in the past 30 days ± standard error, SE | None, but it is a standard question in this field | No |
| Unclear | Intentions not to use/to reduce use/to stop use: 5‐point scales; higher scores are better. No additional information | Unclear | ||
| Lee 2010 | No | 90‐day marijuana use: "items were adapted from the Global Appraisal of Individual Needs‐I" | Dennis ML, Titus JC, Diamond G, Donaldson J, Godley SH, Tims FM. The CYT Steering Committee (2002). The cannabis youth treatment (CYT) experiment: Rationale, study design and analysis plans. Addiction; 97(Suppl 1): 16–34 | Yes |
| No | Intentions not to use/to reduce use/to stop use: 4‐point score (higher = more "contemplation"). "Contemplation to change marijuana use was assessed with four items (alpha = 0.79) adapted from the Readiness to Change Questionnaire (RTCQ)" | Heather N, Gold R, Rollnick S (1991). Readiness to change questionnaire: User's manual. (Tech. Rep. 15). Kensington, Australia: National Drug and Alcohol Research Center, University of New South Wales | Yes | |
| No | Knowledge about the effects of illicit drugs on health: negative consequences due to marijuana use. 5‐point score (from 0 = never to 4 = more than 10 times). "Consequences of marijuana use were assessed using the Rutgers Merijuana Problem Index (RMPI)" | White HR, Labouvie EW, Papadaratsakis V (2005). Changes in substance use during the transition to adulthood: A comparison of college students and their non‐college age peers. Journal of Drug Issues; 35: 281–306 | Unclear | |
| Newton 2010 | No | Frequency of cannabis use: times per week ± SE in the past 12 months "Cannabis use was assessed from a questionnaire in the 2007 National Drug Strategy Household Survey (NDSHS) that identified the frequency of use of cannabis [1]." | Australian Institute of Health and Welfare. 2007 National Drug Strategy Household Survey: First Results. Canberra: AIHW; 2008 | Yes |
| No | Attitudes towards illicit drug use: score ± SE "Attitudes towards cannabis were measured by four items from the Life Skills Training Questionnaire [37], which has acceptable internal consistency (a = 0.86)." | National Health Promotion Associates (NHPA) Incorporated. Life Skills Training Questionnaire—Middle School. New York: NHPA; 2004 | Unclear | |
| No | Knowledge about the effects of illicit drugs on health: score ± SE "The cannabis knowledge questionnaire was adapted from the Cannabis Quiz and included 16 items [33]." | Bleeker A, Malcolm A. The Cannabis Quiz. Sydney: Manly Drug Education and Counselling Centre; 2001 | Yes | |
| No | Knowledge about the effects of illicit drugs on health: score ± SE "Cannabis harms were assessed with six questions derived from the Adolescent Cannabis Problems Questionnaire (test–retest reliability, r = 0.91) [35]." | Martin G, Copeland J, Gilmour S, Gates P, Swift W. The adolescent cannabis problems questionnaire (CPQ‐A): psychometric properties. Addictive Behaviors 2006; 31: 2238–48 | No | |
| Schwinn 2010 | No | Past 30‐day drug use (marijuana): occasions of use (0 to 40) "...adapted from the CDC's Youth Risk Behavior Survey (YRBS; Centers for Disease Control and Prevention 2005), asked girls to report how many times in the past month and week they used alcohol, cigarettes, marijuana, cocaine, inhalants, methamphetamines, and ecstasy. Response options ranged from "0 times" to "40 or more times." Test–retest reliability for YRBS items is 0.82 to 0.95 (Centers for Disease Control and Prevention 2004)" | Centers for Disease Control and Prevention. (2005). Youth Risk Behavior Survey. Retrieved February 20, 2009, from http://www.cdc.gov/healthyyouth/yrbs/ | Yes |
| No | Past 30‐day drug use, poly drug use (cigarettes, marijuana cocaine, inhalants, met., ectasy): 7‐point score (0 to 6). Same as above | Same as above | Yes | |
| No | Past 30‐day drug use, total substance (= poly drug use + alcohol): 8‐point score (0 to 7). Same as above | Same as above | Yes | |
|
Idaho Meth 2010; Colorado Meth 2011; Georgia Meth 2011; Hawaii Meth 2011; Wyoming Meth 2011 |
No | Past‐year and past‐month use of methamphetamine: "Have used meth in past year"; "Have used meth in past month" | n/a | Unclear |
| Unclear | Attitudes towards illicit drug use: "Please indicate how much you approve or disapprove of the following activities." (Strongly disapprove, strongly/somewhat approve) | n/a | Unclear | |
| Unclear | Perceptions (including perceptions of peer norms and perceptions about illicit drug use: binary and categorical questions, such as "How difficult, or easy, do you think it would be for you to get each of the following types of drugs?" (easy, difficult) and "Please indicate how much risk, if any, you think there is involved in each of the following activities." (Great risk, great/moderate risk, little/no risk) | n/a | Unclear | |
| Slater 2011 | Yes | Description of study measures and survey components (p. 15) Autonomy inconsistent with marijuana use: 4 items on a 4‐point scale Aspirations inconsistent with marijuana use: 3 items on a 4‐point scale Lifetime marijuana use: 4 items Exposure to ONDCP's campaign: 1 item on a 3‐point scale | n/a | n/a |
| Carpenter 2011 | No | Lifetime marijuana use | n/a | Unclear |
| No | Past‐month marijuana use | n/a | Unclear | |
| No | Alcohol use | n/a | Unclear |
IAT: Implicit Association Test n/a: not applicable ONDCP: Office of National Drug Control Policy SE: standard error
Several time points of use were available in the different studies, but we chose the six‐month follow‐up as a standard comparable across studies. To do this we have used both published and unpublished data kindly provided by the authors. Among the six‐month assessments, Slater 2006 and Schwinn 2010 measured use in the past 30 days, Lee 2010 measured use in the past three months and Newton 2010 frequency of use in the past 12 months.
The pooled result shows no effect of the intervention, with overall significant heterogeneity among studies (P < 0.05); this can be partially explained by the results of Newton 2010 which showed a reduction of use in the control group.
The theoretical background for the five studies was varied, with two studies based on the social learning theory (Schwinn 2010) and the social ecological framework (Slater 2006) providing the better results, whereas the study based on the social influence approach (Newton 2010) favoured the control group.
Five ITS (Colorado Meth 2011; Georgia Meth 2011; Hawaii Meth 2011; Idaho Meth 2010; Wyoming Meth 2011, N = 26,405) evaluated the Meth Project intervention in five US states. In every study the first year reports pre‐campaign figures. Observed and predicted overall and state‐specific probabilities were plotted against time for both past‐month (Figure 9) and past‐year (Figure 10) use of methamphetamine. Among study participants aged 12 to 17 years old there was no evidence of an effect on past‐month prevalence of methamphetamine (odds ratio (OR) 1.16, 95% CI 0.63 to 2.13) and evidence of a reduction in past‐year prevalence (OR 0.59; 95% CI 0.42 to 0.84). Among participants aged between 18 and 24 years old there was no evidence of an effect for past‐month (OR 0.72; 95% CI 0.16 to 3.20) or past‐year (OR 0.91; 95% CI 0.43 to 1.94) prevalence of methamphetamine.
9.
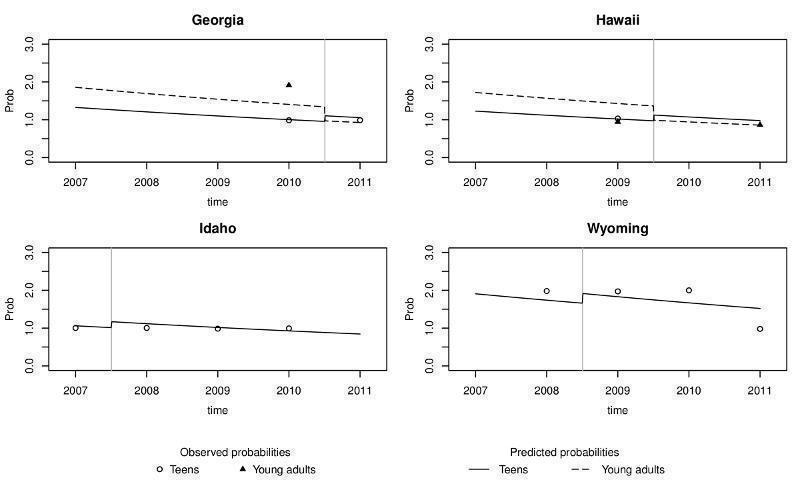
Observed and predicted probabilities of past‐month methamphetamine use in the Meth Project studies
10.

Observed and predicted probabilities of past‐year methamphetamine use in the Meth Project studies
Due to the intrinsic methodological limitations of ITS studies and the impossibility of conducting more sophisticated analyses (e.g. by adjusting for potential confounders), these findings should be considered with caution.
Slater 2011, the only RCT that included a prospective cohort study(the reason why it was not included in the meta‐analysis) found evidence that a community‐level campaign, adjusted for the effect of a school‐level campaign, reduced marijuana uptake compared to no intervention (estimate ‐0.511; P = 0.026).
Two prospective cohort studies (N = 10,632) found results ranging from non‐significantly effective to a significant iatrogenic effect. Namely, Scheier 2010 found that over time young participants in the experimental arms reported increasingly more awareness and recalled increasingly more campaign messages, and also a concomitant but not statistically significant decrease in their reported levels of marijuana use. Hornik 2006 measured past‐year marijuana use after exposure to a national media campaign as a function of exposure to a specific advertisement at a prior round and found an increase in use (odds ratio (OR) 1.21; 95% CI 1.19 to 1.65), controlled for considered confounders.
One ITS(Palmgreen 2001) was included in the meta‐analysis because the author we contacted for this review suggested presenting the data as in the original papers. In this 32‐month study, high sensation‐seekers exhibited a significant upward trend in 30‐day marijuana use before exposure to the campaign and a significant downward trend after exposure. This finding was reported in both the communities involved in the study (Knox County Time Series (P = 0.001) and the Fayette County Time Series (P = 0.003 and P = 0.001 after campaign 1 and 2, respectively)).
One ITS(Carpenter 2011) analysed the relationship between exposure to the 'Above the Influence' campaign in 210 US media markets and adolescent marijuana use from 2006 to 2008. The study showed lower rates of past‐month (adjusted odds ratio (AOR)0.67; 95% CI 0.52 to 0.87) and lifetime (AOR 0.76; 95% CI 0.62 to 0.93) marijuana use among girls in grade eight. For boys in grade eight and both girls and boys in grades 10 and 12 there was no evidence of an association between the campaign and a reduction in marijuana use.
The only controlled before and after (CBA) study (Miller 2000) found a modest increase in drug use in the control campus, paralleled by a modest decrease in drug use in the experimental campus, without statistical significance.
Secondary outcomes
Intentions not to use/to reduce use/to stop use
This outcome was measured by four RCTs, which found a non‐statistically significant effect in favour of media campaigns, and one prospective cohort study which, on the other hand, found a possible iatrogenic effect.
Four RCTs (Fang 2010; Polansky 1999; Yzer 2003; Zhao 2006) involving 1270 students were included in the meta‐analysis (see Figure 11) and the pooled analysis shows that there is no effect (SMD ‐0.07; 95% CI ‐0.19 to 0.04) (Analysis 1.2). Intentions to use drugs were measured with several unpublished scales and the Drug Attitude Scale (see Table 3 for a brief description of the scales used).
11.

Forest plot of comparison: 1 Mass media versus no mass media intervention (RCT), outcome: 1.2 Intention to use drugs.
1.2. Analysis.

Comparison 1 Mass media versus no mass media intervention (RCT), Outcome 2 Intention to use drugs.
Hornik 2008 was not included in the meta‐analysis because its study design (prospective cohort study) was not comparable with that adopted by the others (randomised controlled trial). The study found that at one round a higher level of exposition was associated with more intention to use marijuana (expressed as less intention to avoid marijuana use(y= –0.07; 95% CI –0.13 to –0.01).
Attitudes towards illicit drug use
Fourteen studies including 37,172 youngsters considered this outcome which was measured specifically by eight RCTs, one prospective cohort study and five ITS. No meta‐analysis was possible and results have been described narratively. Overall, no conclusions can be drawn on the basis of the available studies.
Eight RCTs showed mixed results with four studies giving positive results and four uncertain results. For example, Palmgreen 1991 found that media campaign messages specifically targeting high sensation‐seekers were more effective than controls in increasing negative attitude towards drug use. In Kelly 1992 the exposed group showed a change in attitude towards drugs. In Polansky 1999 ninth‐grade students exposed to media advertisement showed more ability to resist peer pressure to use drugs than the control group. In Czyzewska 2007 the anti‐marijuana advertisements group showed a tendency to more negative implicit attitudes to marijuana than the control whereas Newton 2010 showed that at the 12‐month follow‐up no differences between groups persisted for alcohol expectancies, cannabis attitudes or alcohol‐ and cannabis‐related harms. The advertisements studied by Yzer 2003 targeted the belief that marijuana is a gateway to use of stronger drugs. Nevertheless results did not support this as no clear persuasion was found for any of the ad sequences. In comparison to the control condition, adolescents in the explicit gateway condition tended to agree less with the gateway message and displayed weaker correlations between anti‐marijuana beliefs and their attitude towards marijuana use. Schwinn 2010 measured drug resistance/refusal skills; however they did not report results. Zhao 2006 did not find any significant effect on individual measures of attitude change.
Hornik 2006 found a small but significant increase in anti‐marijuana beliefs and attitudes in students exposed to media campaigns even though this was not accompanied by significant parallel gains in intentions not to use, social norms or self efficacy.
Heterogeneous results were reported in the five included Meth Project studies. In Wyoming Meth 2011 more teens disapproved of experimental meth use (i.e. trying meth once or twice) in 2008 than 2011, and both experimental and regular use of heroin, marijuana and cocaine. In Colorado Meth 2011 disapproval of experimental use of marijuana decreased but disapproval of regular use increased from 2009 to 2011. In Georgia Meth 2011 most 12 to 17‐year‐olds disapproved of experimental use of meth, heroin and cocaine in 2011 than in 2010. In Hawaii Meth 2011 more 12 to 17‐year‐olds disapproved experimental use of meth in 2009 than in 2011. Most 18 to 24‐year‐olds disapproved of experimental and regular use of meth and experimental use of heroin and cocaine. In Idaho Meth 2010 more teens disapproved of experimental and regular use of meth, heroin and cocaine in 2007 than in 2010.
Knowledge about the effects of illicit drugs on health
One RCT measured this outcome, finding a possible association between the effectiveness of the campaign and message on individual characteristics. One study shows significant improvement in knowledge about the target substance in the experimental group.
Lee 2010 found an association between contemplation for change and marijuana use at three‐month follow‐up. Intervention participants who were higher in contemplation for change showed a significant decrease in marijuana use. Nevertheless, this result was not confirmed at six months follow‐up. Newton 2010 showed that at the 12‐month follow‐up, significant improvements in alcohol and cannabis knowledge in students in the intervention group compared to the control group were present.
Understanding of intended message and objectives
Only one RCT addressed this outcome:Fishbein 2002 which adopted a measure of perceived effectiveness of a media campaign.
Perceptions (including perception of peer norms and perception of risks of use of illicit drugs)
This outcome was measured by 11 studies (N = 40,243): four RCTs, one prospective cohort study, one CBA and five ITS.
Only one of the four included RCTs found a significant effect in favour of media campaigns in changing towards a negative perception of marijuana use (Zhao 2006). The remainder found weaker results apparently in favour of interventions.
Fishbein 2002 adopted a measure of perceived effectiveness of media campaign based on realism, learning and emotional responses, all considered highly correlated with effective messages. Zhao 2006 found that students exposed to media campaign messages showed changes towards a negative perception about the consequences of marijuana use. Schwinn 2010 measured the normative belief among participants and found a change in the experimental group which was not maintained at six months follow‐up. As already mentioned Yzer 2003 targeted the belief that marijuana is a gateway to stronger drugs. Results did not support this and no clear persuasion was found for any of the ad sequences. In comparison to the control condition, adolescents in the explicit gateway condition tended to agree less with the gateway message and displayed weaker correlations between anti‐marijuana beliefs and their attitude toward marijuana use.
Hornik 2006, the only prospective cohort study investigating this outcome, found a small but significant increase in anti‐marijuana beliefs and attitudes in students exposed to media campaigns yet this was not accompanied by significant parallel gains in intentions not to use, social norms or self efficacy
The only CBA(Miller 2000) found that the students enrolled in the experimental arm showed significantly higher perceived risks from substance use
Results differed considerably across the five included Meth Project studies. In Wyoming Meth 2011 perception of ease to acquire any of the examined drugs (meth, heroin, marijuana and cocaine) decreased from 2008 to 2011. More teens agreed with all of the 14 perceived risks attributed to meth and more teens disagreed with six out of the nine perceived benefits attributed to meth. In Colorado Meth 2011 more teens in 2011 than in 2009 agreed with nine of the 14 items concerning risks attributed to meth. In Georgia Meth 2011 perception of ease to acquire cocaine and heroin decreased from 2010 to 2011 among 12 to 17‐year‐olds. More teens agreed with all of the 14 perceived risks attributed to meth, and fewer teens agreed with five of the nine perceived benefits attributed to meth. Among 18 to 24‐year olds, more young adults agreed with seven of the 14 perceived risks attributed to meth, and fewer young adults agreed with six of the nine perceived benefits attributed to meth. In Hawaii Meth 2011 perception of ease to acquire heroin decreased from 2009 to 2011 among 12 to 17‐year‐olds. The percentage of those who see a "great risk" in taking meth, heroin and cocaine decreased by around 10 points. More teens agree with 13 of the 14 perceived risks attributed to meth. Among 18 to 24‐year‐olds a reduction of perceived ease to acquire marijuana and cocaine was also described. In such an age group the percentage of those who see a "great risk" in taking meth, heroin and cocaine decreased by around 15 points. More young adults agreed with all of the 14 perceived risks attributed to meth and fewer young adults agreed with five of nine perceived benefits of meth. In Idaho Meth 2010 perception of risk in trying meth, heroin and cocaine once or twice increased from 2007 to 2010. More teens agreed with all of the 14 perceived risks attributed to meth and fewer teens agreed with all of the nine perceived benefits attributed to meth.
Adverse effects
Reactance (i.e. a reaction to contradict the prevailing norms of rules)
Fishbein 2002 found that six out of 16 studied Public Service Advertisements (PSA) were judged by the young participants as not effective. In other words, adolescents viewing these six PSAs reported that they and their friends would be more likely to try or to use drugs, and would feel less confident about how to deal with situations involving drugs. Specifically negative correlations were found for the advertisement tackling marijuana (r = –0.52), those not specifying a drug or talking about drugs in general, also tended to be judged as ineffective, although this relationship was not significant (r = –0.23). PSAs describing the "just say no" message tended to be judged as less effective (r = –0.29). Yzer 2003 found that adolescents exposed to the "Gateway" message (explicitly saying that marijuana use led to use of hard drugs) considered this message less effective and were (although not statistically significantly) more positive towards marijuana use, while Hornik 2006 found a possible presence of pro‐marijuana effects in at least two analyses out of 10 in terms of intention to use and initiation.
Positive descriptive norms (i.e. increased perception that drug use in peer population is common, normal or acceptable)
Palmgreen 2001 found a reinforcing effect of the media campaign on pro‐marijuana beliefs (particularly for occasional use).
Discussion
Summary of main results
The studies included in this review tested an array of different interventions including national campaigns, public service advertisements, television messages, video tapes and Internet‐based campaigns and the effects were measured by means of unpublished and published scales administered to the participating adolescents. Hence the first issue is the comparability of results.
Overall 15 studies measured the effects on the use of drugs of nine campaigns of which four used the Internet, one was performed in school setting and four were TV broadcasting campaigns (the Meth Project was assessed by five studies and the National Youth Anti‐Drug Media Campaign (NYADMC) was assessed at different stages by five studies).
The outcomes on the use of drugs of five randomised controlled trials (RCTs) (four on Internet‐based interventions and one on TV/radio broadcasting) have been pooled, resulting in no effect of mass media campaigns (standardised mean difference (SMD) ‐0.02; 95% confidence interval (CI) ‐0.15 to 0.12), with statistically significant heterogeneity (P = 0.02). The four studies including Internet‐based interventions gave contrasting results about drug use (some showed that the intervention reduced the use of drugs and some showed that the intervention could favour use), whereas the study on the national campaigns found a reduction in use in the experimental group.
The study evaluating the school media campaign found a non‐significant reduction in drug use in the experimental group.
The studies evaluating the Meth Project on methamphetamine were included in a separate meta‐analysis, the pooled results of which showed a significant reduction in the past‐year use of methamphetamine.
Five studies evaluated different phases of the NYADMC. The preliminary study showed positive results in favour of the campaign, the two studies evaluating the 1st phase showed an opposite effect, with a significant increase in drug use in the more robust study, and the two studies evaluating the 2nd phase showed positive results in favour of the campaign.
There are a series of observational studies, generally cohort studies or interrupted time series (ITS), which can be classified as field trials and evaluate the effectiveness of the multimedia‐TV campaigns intervention in its context. They show contrasting results, from weakly effective, as for the Meth Project campaign, to clearly harmful, as one form (Hornik 2006) reported statistically significant results in favour of the control group, showing an increase in marijuana use of 20% in those more exposed to the campaign compared to those less exposed. The multistage evaluation of the NYADMC campaign conducted to positive results.
Looking at the secondary outcomes, the RCTs included in the meta‐analysis showed non‐significant results in favour of the groups exposed to the campaign for intention to use, an outcome considered a proxy for future behavior (Litchfield 2006; Olds 2005). One observational study (Hornik 2006) found a possible reinforcing effect of media campaign exposure on intention to use, especially cannabis.
Summing up the available evidence from RCTs shows that media campaigns based on the Internet are not effective in reducing the use of drugs, whereas the evidence from observational studies shows that there are some positive effects in reducing last‐year prevalence in younger people. A study based on independent data collection gave overall positive results for girls and showed no effectiveness in boys in terms of marijuana use.
Overall completeness and applicability of evidence
The objective of this review was to measure the effect of media campaigns on influencing drug use among young people. The studies we included only partially answer the question and they are hardly comparable. In fact the studies focused on a variety of interventions and used several different scales to measure the outcomes. It was therefore not possible to have results on all the typologies of campaign listed in the introduction section, and any attempt to compare effects is limited.
A second threat to the applicability of results is the nature of the studies: the RCTs are always carried out in an experimental context such as, for example, schools in which the students randomised to the intervention arm are exposed to the media message, or the trials enrolling volunteers on the Internet, a very selected population. This appears to measure efficacy and not effectiveness of the intervention, given that subjects are out of the context in which they would be exposed in the real world. The other studies, called field studies, measure the effect in a real context, but are limited in numbers, overall methodological quality and are actually focused on two campaigns.
Furthermore, all the studies were conducted in the USA, apart from two in Canada and Australia, and as a consequence the generalisability to other geographical and social contexts, such as Europe, remains unclear.
Quality of the evidence
We included 23 studies on very different interventions, the effects of which were measured with several scales. The methodological quality of the included studies was hard to assess as many dimensions were unclear in the relevant publications. Nevertheless, when the dimensions were reported the quality of the studies was acceptable. In many cases further information was obtained by contacting the study authors. The main limitation of the evidence available is the lack of comparability of some measures of outcomes and, more importantly, the unclear causal relationship between the campaign size and its effect. This lack of clarity reduces the generalisability of results, i.e. it is still unclear which part of a campaign should be reproduced to achieve which results.
Potential biases in the review process
The inclusion of studies which are different from randomised controlled trials complicates the identification and retrieval of the studies, due to a less structured indexing of studies in different databases, and lack of devoted registries and unique identification of studies. We therefore acknowledge that we might have missed some studies. Nevertheless, an accurate cross‐check of all the reference lists and contacts with the principal investigators in the field may have reduced this risk.
The assessment of study quality relied on study design‐specific checklists, yet for many publications the majority of the information we used assess and score the quality criteria was unclear. We therefore contacted many authors to ask for clarification, but in the case of the older studies it was not possible to retrieve additional information.
Agreements and disagreements with other studies or reviews
Werb and colleagues (Werb 2011) performed a systematic review of all the studies assessing public service announcements (eight studies) including meta‐analyses for two outcomes: intention to use and and mean use of illicit drugs. In spite of different inclusion criteria (as we also included non‐PSA interventions) and criteria for analysis, we reached similar conclusions. Furthermore, Wakefield 2010, in their broader analysis of media campaigns aiming to change health behaviour, address the media campaign effect on illicit drugs use with five studies, concluding that the relevant evidence is inconclusive.
Authors' conclusions
Implications for practice.
The effectiveness of media campaigns to prevent illicit drug use among young people is not clearly supported, with some evidence of iatrogenic effects. Therefore it is recommended that such campaigns should only be provided in the context of rigorous, well‐designed and well‐powered evaluation studies.
Implications for research.
The great majority of the studies are conducted in the United States, thus more worldwide studies should be carried out. Moreover, validated and standardised tools to measure the outcome are recommended to allow comparability and generalisability of results. As the actual evidence suggests some effectiveness in specific populations (younger and female, for example) we need to focus better on investigation of the components of media campaigns which are effective in specific populations.
For this reason, beyond the general methodological recommendations, we suggest a strategy to make the best use of available resources and study designs. Our suggestions initially consider general improvement of methods:
field evaluation studies should adopt, whenever possible, a cohort design;
studies should be conducted in different countries and contexts;
validated, comparable and standard tools should be used for the measurement of effects;
the separate testing of specific media campaign components for their efficacy should be carried out by pilot randomised controlled trials in specific populations;
future studies should ensure consistency among hypothesis testing, study design and measures of outcomes.
In general, whenever possible, interrupted time series studies, using independent and current data collection (such as the one by Carpenter 2011), should be conducted to assess the overall effects of any anti‐drug media campaign.
Until the development of this research is ensured, we should not exclude the possibility of a campaign having iatrogenic effects.
Acknowledgements
We would like to thank Gregor Burkhart and V. Anna Gyamathy for collaborating in conceiving the protocol for this review. We are grateful to Jennifer Stagnaro, Joan Polansky, John Horan, Ling Fang, Marco Yzer, Michael Slater, Nicola Newton, Philip Palmgreen and Violeta Taneva for providing us with useful advice and, whenever possible, with their studies' unpublished data.
Appendices
Appendix 1. CENTRAL search strategy
| ID | Search | Hits |
| #1 | MeSH descriptor: [Substance‐Related Disorders] explode all trees | 10,355 |
| #2 | ((stimulant* or polydrug* or drug* or substance) near/3 (abuse* or abusing or consumption or addict* or disorder* or intoxicat* or misus* or use*)):ti,ab | 14,750 |
| #3 | (abuse* or abusing or consumption or addict* or disorder* or intoxicat* or misus* or use*):ti,ab | 198,966 |
| #4 | MeSH descriptor: [Narcotics] explode all trees | 681 |
| #5 | heroin:ti,ab | 762 |
| #6 | MeSH descriptor: [Street Drugs] explode all trees | 196 |
| #7 | MeSH descriptor: [Amphetamine] explode all trees | 632 |
| #8 | (amphetamine* or dextroamphetamine* or methamphetamine or Methylamphetamine*):ti,ab,kw (Word variations have been searched) | 1442 |
| #9 | (ecstasy or MDMA or hallucinogen*):ti,ab,kw (Word variations have been searched) | 234 |
| #10 | MeSH descriptor: [Cocaine] explode all trees | 576 |
| #11 | (crack or cocaine):ti,ab,kw (Word variations have been searched) | 1953 |
| #12 | MeSH descriptor: [Cannabis] explode all trees | 245 |
| #13 | (cannabis or marijuana or marihuana or Hashish):ti,ab,kw (Word variations have been searched) | 1158 |
| #14 | (Lysergic next Acid):ti,ab,kw | 76 |
| #15 | LSD:ti,ab,kw (Word variations have been searched) | 131 |
| #16 | (benzodiazepine* or barbiturate* or ketamine or solvent or inhalant):ti,ab,kw (Word variations have been searched) | 6370 |
| #17 | (benzodiazepine* or barbiturate* or ketamine or solvent or inhalant):ti,ab,kw (Word variations have been searched) | 6370 |
| #18 | #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 | 11,919 |
| #19 | #3 and #18 | 6547 |
| #20 | #1 or #2 or #19 | 26,077 |
| #21 | MeSH descriptor: [Mass Media] explode all trees | 1337 |
| #22 | MeSH descriptor: [Internet] explode all trees | 1248 |
| #23 | MeSH descriptor: [Videotape Recording] explode all trees | 790 |
| #24 | "Tv":ti,ab,kw (Word variations have been searched) | 386 |
| #25 | (media or communication* or audiovisual or telecommunication* or radio or television or internet or campaign* or advert* or twitter or facebook) (Word variations have been searched) | 27,766 |
| #26 | #21 or #22 or #23 or #24 or #25 | 28,828 |
| #27 | MeSH descriptor: [Adolescent] explode all trees | 68,885 |
| #28 | adolescen* or preadolescen* or child* or teen* or youth* or young or kid* or juvenile* or minors or boy* or girl*:ti,ab,kw (Word variations have been searched) | 157,753 |
| #29 | #27 or #28 | 157,753 |
| #30 | #20 and #26 and #29 | 566 |
Appendix 2. PubMed (MEDLINE) search strategy
| Search | Query | Items found |
| #16 | Search (((#3) AND #4) AND #11) AND #15 | 5877 |
| #15 | Search ((#12) OR #13) OR #14 | 3,041,802 |
| #14 | Search adolescen*[tiab] OR preadolescen*[tiab] OR child*[tiab] OR teen*[tiab] OR youth*[tiab] OR young[tiab] OR kid*[tiab] OR juvenile*[tiab] OR minors[tiab] OR boy*[tiab] OR girl*[tiab] | 1,662,519 |
| #13 | Search "Child"[Mesh] | 1,457,004 |
| #12 | Search "Adolescent"[Mesh] | 1,498,465 |
| #11 | Search ((((#5) OR #7) OR #8) OR #9) OR #10 | 797,788 |
| #10 | Search media[tiab] OR Communication*[tiab] OR audiovisual[tw] OR telecommunication*[tw] OR Educat*[tiab] OR radio[tw] OR television[tw] OR TV[tiab] OR internet[tw] OR campaign*[tw] OR advert*[tw] OR twitter[tw] OR facebook[tw] OR "instant messaging"[tw] | 751,996 |
| #9 | Search "Telecommunications"[Mesh] | 54,815 |
| #8 | Search Videotape Recording[Mesh] | 9970 |
| #7 | Search "Internet"[Mesh] | 43,359 |
| #5 | Search "Mass Media"[Mesh] | 37,325 |
| #4 | Search "heroin"[Mesh] OR heroin[tiab] OR "Street Drugs"[Mesh] OR "Designer Drugs"[Mesh] OR "Crack Cocaine"[Mesh] OR "Lysergic Acid Diethylamide"[Mesh] OR drug*[tiab] OR polydrug[tiab] OR substance[tiab] OR hallucinogen*[tw] OR cocaine[tw] OR amphetamine*[tw] OR "lysergic acid diethylamide"[tw] OR LSD [tiab] OR ketamine[tw] OR cannabis[tw] OR marihuana[tw] OR marijuana[tiab] OR hashish[tw] OR steroid*[tw] OR morphine[tiab] OR ecstasy[tw] OR MDMA[tw] OR benzodiazepine[tw] | 1,136,251 |
| #3 | Search (#1) OR #2 | 1,812,638 |
| #2 | Search abus*[tiab] OR consumption[tiab] OR misus*[tiab] OR use*[tiab] OR addict*[tiab] OR disorder*[tiab] | 1,570,344 |
| #1 | Search "Substance‐Related disorders"[Mesh] | 344,574 |
Appendix 3. EMBASE search strategy
| ID | Query |
| #1 | 'substance abuse'/exp |
| #2 | 'drug abuse'/exp |
| #3 | abus*:ab,ti OR consumption:ab,ti OR misus*:ab,ti OR use*:ab,ti OR addict*:ab,ti OR disorder*:ab,ti |
| #4 | #1 OR #2 OR #3 |
| #5 | heroin:ab,ti OR drug*:ab,ti OR polydrug:ab,ti OR substance:ab,ti OR hallucinogen*:ab,ti OR cocaine:ab,ti OR amphetamine*:ab,ti OR 'lysergic acid diethylamide':ab,ti OR lsd:ab,ti OR ketamine:ab,ti OR cannabis:ab,ti OR marihuana:ab,ti OR marijuana:ab,ti OR hashish:ab,ti OR steroid*:ab,ti OR morphine:ab,ti OR ecstasy:ab,ti OR mdma:ab,ti OR benzodiazepine:ab,ti |
| #6 | 'diamorphine'/exp |
| #7 | 'designer drug'/exp |
| #8 | 'street drug'/exp |
| #9 | 'cocaine'/exp |
| #10 | 'cannabis smoking'/exp |
| #11 | #5 OR #6 OR #7 OR #8 OR #9 OR #10 |
| #12 | 'mass medium'/exp |
| #13 | 'internet'/exp |
| #14 | 'videorecording'/exp |
| #15 | 'telecommunication'/exp |
| #16 | media:ab,ti OR communication*:ab,ti OR audiovisual:ab,ti OR telecommunication*:ab,ti OR educat*:ab,ti OR radio:ab,ti OR television:ab,ti OR tv:ab,ti OR internet:ab,ti OR campaign*:ab,ti OR advert*:ab,ti OR twitter:ab,ti OR facebook:ab,ti |
| #17 | #12 OR #13 OR #14 OR #15 OR #16 |
| #18 | 'adolescent'/exp |
| #19 | 'child'/exp |
| #20 | adolescen*:ab,ti OR preadolescen*:ab,ti OR child*:ab,ti OR teen*:ab,ti OR youth*:ab,ti OR young:ab,ti OR kid*:ab,ti OR juvenile*:ab,ti OR minors:ab,ti OR boy*:ab,ti OR girl*:ab,ti |
| #21 | #18 OR #19 OR #20 |
| #22 | #4 AND #11 AND #17 AND #21 AND [embase]/lim |
Appendix 4. EPOC criteria for quality assessment of interrupted time series
The following seven standard criteria should be used to assess the methodological quality of ITS designs included in EPOC reviews. Each criterion is scored DONE, NOT CLEAR or NOT DONE. The results of the quality assessment for each study are reported in the Characteristics of included studies table in RevMan. Examples can be obtained from the EPOC Group Co‐ordinator.
| Criterion | Score | ||
| DONE | NOT CLEAR | NOT DONE | |
| a) Protection against secular changes | |||
| The intervention is independent of other changes | If the intervention occurred independent of other changes over time | If not specified (will be treated as NOT DONE if information cannot be obtained from the authors) | If reported that intervention was not independent of other changes in time |
| There are sufficient data points to enable reliable statistical inference | (a) If at least 20 points are recorded before the intervention AND the authors have done a traditional time series analysis (ARIMA model) | If not specified in paper, e.g. number of discrete data points not mentioned in text or tables (will be treated as NOT DONE if information cannot be obtained from the authors) | If any of the above conditions are unmet |
| OR (b) If at least 3 points are recorded pre and post intervention AND the authors have done a repeated measures analysis | |||
| OR (c) If at least 3 points are recorded pre and post intervention AND the authors have used ANOVA or multiple t‐tests AND there are at least 30 observations per data point | |||
| Formal test for trend. Complete this section if authors have used ANOVA modelling | If formal test for change in trend using appropriate method is reported (e.g. see Cook & Campbell 1979) | If not specified in the paper (will be treated as NOT DONE if information cannot be obtained from the authors) | If formal test for change in trend has not been done |
| b) Protection against detection bias | |||
| Intervention unlikely to affect data collection | If the investigators report that the intervention itself was unlikely to affect data collection (for example, sources and methods of data collection were the same before and after the intervention) | If not reported (will be treated as NOT DONE if information cannot be obtained from the authors) | If the intervention itself was likely to affect data collection (for example, any change in source or method of data collection reported) |
| Blinded assessment of primary outcome(s)* | If the authors state explicitly that the primary outcome variables were assessed blindly OR the outcome variables are objective, e.g. length of hospital stay, drug levels as assessed by a standardised test | If not specified (will be treated as NOT DONE if information cannot be obtained from the authors) | If the outcomes were not assessed blindly |
| c) Completeness of data set | If data set covers 80% to 100% of the total number of participants or episodes of care in the study | If not specified (will be treated as NOT DONE if information cannot be obtained from the authors) | If data set covers less than 80% of the total number of participants or episodes of care in the study |
| d) Reliable primary outcome measure(s)** | If 2 or more raters with at least 90% agreement or kappa greater than or equal to 0.8 OR the outcome is obtained from some automated system, e.g. length of hospital stay, drug levels as assessed by a standardised test | If reliability is not reported for outcome measures that are obtained by chart extraction or collected by an individual (will be treated as NOT DONE if information cannot be obtained from the authors) | If agreement is less than 90% or kappa is less than 0.8 |
*Primary outcome(s) are those variables that correspond to the primary hypothesis or question as defined by the authors. In the event that some of the primary outcome variables were assessed in a blind fashion and others were not, score each separately.
**In the event that some outcome variables were assessed in a reliable fashion and others were not, score each separately.
Appendix 5. Quality Criteria for Cohort Controlled Studies (SIGN)
| SIGN | Methodology Checklist 3: Cohort studies | |||||
| Study identification (include author, title, year of publication, journal title, pages) | ||||||
| Guideline topic: | Key Question No: | Reviewer: | ||||
|
Before completing this checklist, consider: 1.Is the paper really a cohort study? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. 2.Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist. | ||||||
| Reason for rejection: 1. Paper not relevant to key question □ 2. Other reason □ (please specify): Please note that a retrospective study (i.e. a database or chart study) cannot be rated higher than + | ||||||
| Section 1: Internal validity | ||||||
| In a well‐conducted cohort study: | Does this study do it? | |||||
| 1.1 | The study addresses an appropriate and clearly focused question.[i] | Yes □ Can't say □ |
No □ |
|||
| Selection of subjects | ||||||
| 1.2 | The 2 groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation.[ii] | Yes □ Can't say □ |
No □ Does not apply □ |
|||
| 1.3 | The study indicates how many of the people asked to take part did so, in each of the groups being studied.[iii] |
Yes □ |
No □ Does not apply □ |
|||
| 1.4 | The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis.[iv] | Yes □ Can't say □ |
No □ Does not apply □ |
|||
| 1.5 | What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed.[v] | |||||
| 1.6 | Comparison is made between full participants and those lost to follow‐up, by exposure status.[vi] | Yes □ Can't say □ |
No □ Does not apply □ |
|||
| ASSESSMENT | ||||
| 1.7 | The outcomes are clearly defined.[i] | Yes □ Can't say □ |
No □ |
|
| 1.8 | The assessment of outcome is made blind to exposure status. If the study is retrospective this may not be applicable.[ii] | Yes □ Can't say □ |
No □ Does not apply □ |
|
| 1.9 | Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome.[iii] | Yes □ Can't say □ |
No □ □ |
|
| 1.10 | The method of assessment of exposure is reliable.[iv] | Yes □ Can't say □ |
No □ |
|
| 1.11 | Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable.[v] | Yes □ Can't say □ |
No □ Does not apply□ |
|
| 1.12 | Exposure level or prognostic factor is assessed more than once.[vi] | Yes □ Can't say □ |
No □ Does not apply □ |
|
| CONFOUNDING | ||||
| 1.13 | The main potential confounders are identified and taken into account in the design and analysis.[vii] | Yes □ Can't say □ |
No □ |
|
| STATISTICAL ANALYSIS | ||||
| 1.14 | Have confidence intervals been provided?[viii] | Yes □ | No □ | |
| Section 2: OVERALL ASSESSMENT OF THE STUDY | ||||
| 2.1 | How well was the study done to minimise the risk of bias or confounding?[ix] |
High quality (++) □ Acceptable (+) □ Unacceptable – reject 0 |
||
| 2.2 | Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, how strong do you think the association between exposure and outcome is? | |||
| 2.3 | Are the results of this study directly applicable to the patient group targeted in this guideline? | Yes □ | No □ | |
| 2.4 | Notes. Summarise the authors' conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above. | |||
[i] This relates to the risk of detection bias.* Once enrolled in the study, participants should be followed until specified end points or outcomes are reached. In a study of the effect of exercise on the death rates from heart disease in middle aged men, for example, participants might be followed up until death, or until reaching a predefined age. If outcomes and the criteria used for measuring them are not clearly defined, the study should be rejected.
[ii] This relates to the risk of detection bias.* If the assessor is blinded to which participants received the exposure, and which did not, the prospects of unbiased results are significantly increased. Studies in which this is done should be rated more highly than those where it is not done, or not done adequately.
[iii] This relates to the risk of detection bias.* Blinding is not possible in many cohort studies. In order to asses the extent of any bias that may be present, it may be helpful to compare process measures used on the participant groups ‐ e.g. frequency of observations, who carried out the observations, the degree of detail and completeness of observations. If these process measures are comparable between the groups, the results may be regarded with more confidence.
[iv] This relates to the risk of detection bias.* A well‐conducted study should indicate how the degree of exposure or presence of prognostic factors or markers was assessed. Whatever measures are used must be sufficient to establish clearly that participants have or have not received the exposure under investigation and the extent of such exposure, or that they do or do not possess a particular prognostic marker or factor. Clearly described, reliable measures should increase the confidence in the quality of the study
[v] This relates to the risk of detection bias.* The primary outcome measures used should be clearly stated in the study. If the outcome measures are not stated, or the study bases its main conclusions on secondary outcomes, the study should be rejected. Where outcome measures require any degree of subjectivity, some evidence should be provided that the measures used are reliable and have been validated prior to their use in the study.
[vi] This relates to the risk of detection bias.* Confidence in data quality should be increased if exposure level is measured more than once in the course of the study. Independent assessment by more than one investigator is preferable.
[vii] Confounding is the distortion of a link between exposure and outcome by another factor that is associated with both exposure and outcome. The possible presence of confounding factors is one of the principal reasons why observational studies are not more highly rated as a source of evidence. The report of the study should indicate which potential confounders have been considered, and how they have been assessed or allowed for in the analysis. Clinical judgement should be applied to consider whether all likely confounders have been considered. If the measures used to address confounding are considered inadequate, the study should be downgraded or rejected, depending on how serious the risk of confounding is considered to be. A study that does not address the possibility of confounding should be rejected.
[viii] Confidence limits are the preferred method for indicating the precision of statistical results, and can be used to differentiate between an inconclusive study and a study that shows no effect. Studies that report a single value with no assessment of precision should be treated with extreme caution.
[ix] Rate the overall methodological quality of the study, using the following as a guide: High quality (++): Majority of criteria met. Little or no risk of bias. Results unlikely to be changed by further research. Acceptable (+): Most criteria met. Some flaws in the study with an associated risk of bias. Conclusions may change in the light of further studies. Low quality (0): Either most criteria not met, or significant flaws relating to key aspects of study design. Conclusions likely to change in the light of further studies.
Data and analyses
Comparison 1. Mass media versus no mass media intervention (RCT).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Drug use | 5 | 5470 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.15, 0.12] |
| 2 Intention to use drugs | 4 | 1270 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.07 [‐0.19, 0.04] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Carpenter 2011.
| Methods | Study design: interrupted time series study Sampling: systematic sampling (schools are selected within geographic areas that are determined by the sampling section of the University of Michigan Survey Research Center, page 949) Comparison group(s): pre‐intervention surveys Follow‐up duration: n/a Study time span: 2006 to 2008 (approximately 36 months) |
|
| Participants | 130,245 youths from 8th to 12th grade (13‐ to 18‐year‐old) | |
| Interventions | All media for 210 media markets for 2006 to 2008, after the introduction of the Above the Influence campaign | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Colorado Meth 2011.
| Methods | Study design: interrupted time series study Sampling: n/a Comparison group(s): pre‐intervention survey Follow‐up duration: n/a Study time span: March 2009 to April 2011 (26 months) |
|
| Participants | 1803 youths (600 + 601 + 602) | |
| Interventions | Meth Project (USA), a "messaging campaign, supported by community outreach, and public policy initiatives". The campaign comprises "television, radio, print, billboard, and Internet advertising" | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaires |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Czyzewska 2007.
| Methods | Study design: randomised controlled trial Sampling: not specified Comparison group(s): 4 = 2 anti‐tobacco advertisements x 2 orders of advertisements (i.e. explicit attitudes towards tobacco or marijuana) Follow‐up duration: not applicable Study time span: not specified |
|
| Participants | 229 college students aged 18 to 19 years | |
| Interventions | 15 advertisement embedded in a 15‐minute science programme (USA). 10 advertisements were youth directed, 5 were non‐youth directed. Each programme comprised of 90‐second science film segments, 30‐second youth‐directed ad, 30‐second non‐youth‐directed ad, then again another 30‐second youth‐directed ad. There were 4 versions of recorded programme corresponding to 4 experimental conditions: 2 types of advertisements (i.e. anti‐tobacco or anti‐marijuana) x 2 orders of advertisements (i.e. explicit attitudes towards tobacco or marijuana) | |
| Outcomes |
|
|
| Notes | Implicit attitudes were assessed through the Implicit Association Test (IAT) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | p. 117 "They were randomly assigned to experimental conditions", but randomisation details are not reported |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 117: "Two groups of 18‐ to 19‐year‐old college students were exposed to either anti‐tobacco or anti‐marijuana advertisements followed by implicit and explicit tests of attitudes to both, marijuana and tobacco" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 119 "Next to a computer, each person had a survey with a pre‐recorded ID number on it" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the test (being a post‐only design); p. 117 "Two groups of 18‐ to 19‐year‐old college students were exposed to either anti‐tobacco or anti‐marijuana advertisements followed by implicit and explicit tests of attitudes to both, marijuana and tobacco" |
| Selective reporting (reporting bias) | Unclear risk | No study protocol was mentioned |
Fang 2010.
| Methods | Study design: randomised controlled trial Sampling: random sampling (through online advertisement and community service agencies) Comparison group(s): no intervention Follow‐up duration: 6.25 months Study time span: September 2007 to ˜December 2008 (˜16 months) |
|
| Participants | 108 Asian‐American girls aged 10 to 14 with private access to a computer, and their mothers | |
| Interventions | Internet‐based prevention programme (USA) guided by family interaction theory and aiming to prevent girls' substance use through enhancing mother‐daughter interactions. 9 sessions: mother‐daughter relationship, conflict management, substance use opportunities, body image, mood management, stress management, problem solving, social influences, self efficacy. The programme was not designed expressly for Asian‐Americans | |
| Outcomes |
|
|
| Notes | Only 1 post‐test survey. Unclear whether the intervention focused on a single substance or many | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | p. 530 "Mother–daughter dyads were randomly assigned to intervention (n = 56) and control arms (n = 52)", but randomisation details are not reported |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 530: "Delivered by voice‐over narration, animated graphics, and games, session content involved skill demonstrations and interactive exercises that required the joint participation of mothers and daughters." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Online questionnaire p. 530 "Girls and mothers had separate and unique log‐in names and passwords, and each completed a pretest and posttest survey online" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low number of missing outcome data; missing data balanced in numbers across study groups p. 530 "Mother–daughter dyads were randomly assigned to intervention (n = 56) and control arms (n = 52)" "Two mother–daughter dyads attrited from each arm, and 104 dyads (54 intervention and 50 control) successfully completed both pretest and posttest measures" |
| Selective reporting (reporting bias) | Unclear risk | p. 530 "The study protocol was approved by Columbia University's Institutional Review Board" |
Fishbein 2002.
| Methods | Study design: randomised controlled trial Sampling: systematic random sampling (letters from each included middle/high school) Comparison group(s): 5 experimental (6 advertisements each, embedded in a 24‐minute documentary) + versus no intervention (documentary only) condition Follow‐up duration: not applicable Study time span: not specified |
|
| Participants | 3608 youths aged 11 to 18 years (grades 4 to 12), median age 15 years | |
| Interventions | 30 public service announcements produced by the Partnership for a Drug Free America (USA) | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No mention of the sequence generation in the article (methods section p. 239) |
| Allocation concealment (selection bias) | Unclear risk | No mention of the sequence generation in the article (methods section p. 239) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 240 "Confidentiality and anonymity were emphasized in the instructions, both in written and audio‐video form" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Apparently almost all the sample exposed to interventions were included in the final analysis (and filled out the questionnaires). But no mention of the number originally enrolled, mention of some drop‐outs apparently unlinked to outcomes but no absolute numbers reported |
| Selective reporting (reporting bias) | Low risk | Protocol not available but we do not suspect selective reporting |
Georgia Meth 2011.
| Methods | Study design: before and after study Sampling: 4‐stage probability sampling Comparison group(s): pre‐intervention survey Follow‐up duration: n/a Study time span: November 2009 to April 2011 (18 months) |
|
| Participants | 4454 youths (2432 + 2022) | |
| Interventions | Meth Project (USA), a "messaging campaign, supported by community outreach, and public policy initiatives". The campaign comprises "television, radio, print, billboard, and Internet advertising" | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaires |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Hawaii Meth 2011.
| Methods | Study design: interrupted time series study Sampling: 4‐stage probability sampling Comparison group(s): pre‐intervention survey Follow‐up duration: n/a Study time span: March 2009 to March 2011 (25 months) |
|
| Participants | 3305 youths (1065 + 1035 + 1205) | |
| Interventions | Meth Project (USA), a "messaging campaign, supported by community outreach, and public policy initiatives". The campaign comprises "television, radio, print, billboard, and Internet advertising" | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaires |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Hornik 2006.
| Methods | Study design: prospective cohort study Sampling: systematic sampling (4‐stage, geographic) Comparison group(s): lower exposure to intervention Follow‐up duration: November 1999 to June 2004 (56 months) Study time span: September 1999 to June 2004 (58 months). Up to 4 observations per each of the 3 cohorts. Interviews were carried out at home |
|
| Participants | 8117 youths aged 12.5 to 18 years in the first round | |
| Interventions | The National Youth Anti‐Drug Media Campaign (USA) was a comprehensive social marketing campaign aimed at youths aged 9 to 18 years and disseminated though television, radio, websites, magazines, movie theatres and others. The campaign established partnership with civic, professional and community groups and outreach programs with the media, entertainment and sport industries | |
| Outcomes |
|
|
| Notes | NIDA report 'Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings. June 2006', on which this article is based, was also used to retrieve information for this meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous and administered via computer p. 2230 (Hornik 2008) "NSPY questionnaires were administered on laptop computers brought into the respondents' homes. The interviewer recorded answers for the opening sections, but for most of the interview, to protect privacy, respondents heard pre‐recorded categories of questions and answer through headphones and responded via touch screen selection on the computer. Interviews could be conducted in English or Spanish" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "The overall response rate among youths for the first round was 65%, with 86% to 93% of still eligible youths interviewed in subsequent rounds", page 2230 in Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, page 2‐12, table 2‐A "Completed interviews by wave" |
| Selective reporting (reporting bias) | Low risk | No protocol available but the we do not suspect selective reporting bias |
Idaho Meth 2010.
| Methods | Study design: interrupted time series study Sampling: 4‐stage probability sampling Comparison group(s): pre‐intervention survey Follow‐up duration: n/a Study time span: September 2007 to December 2010 (40 months) |
|
| Participants | 11,143 youths (3091 + 2590 + 2641 + 2821) | |
| Interventions | Meth Project (USA), a "messaging campaign, supported by community outreach, and public policy initiatives". The campaign comprises "television, radio, print, billboard, and Internet advertising" | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaires |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Kelly 1992.
| Methods | Study design: randomised controlled trial. Sampling: not specified. Comparison group(s):
Follow‐up duration: 1.5 months (6 weeks). Study time span: not specified, at least 1.5 months. |
|
| Participants | 79 female college students, primarily 18 to 19 years old | |
| Interventions | Anti‐drug messages (USA) selected from the library of the Media Advertising Partnership for a Drug‐Free America and centred on drugs and alcohol | |
| Outcomes |
|
|
| Notes | Pre‐test, post‐test and 6‐week follow‐up means are provided. Standard deviations are not provided | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported p.80 "Subjects were randomly divided into a total of 9 discussion groups." |
| Allocation concealment (selection bias) | Unclear risk | Not reported Baseline comparisons reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessors not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data and clear reporting of sample size both of the intervention and control group |
| Selective reporting (reporting bias) | Low risk | No study protocol available but clear reporting of main study hypothesis and direct correlation between main topics investigated in the experiment and reported outcomes TOPICAL EXPERIMENTAL AREAS: p. 79 "two topical areas chosen for the study were (1) the age at which parents should talk to their children about dangers of drugs, (2) how much responsibility one has, if any, for another's drug use" OUTCOMES: p. 80 "three questions asking at what age children should be spoken to about marijuana, cocaine and crack" p. 81 "one question asked subjects to rate their agreement on a 5 point Likert scale with the statement "whether or not I get drunk is nobody's business". Similar question were asked regarding use of marijuana, cocaine and crack" |
Lee 2010.
| Methods | Study design: randomised controlled trial Sampling: random sampling (letters and email sent to ˜4000 college students at a "large public university in the Northwest United States") Comparison group(s): no intervention (no feedback or information, students were asked to complete web‐based assessments) Follow‐up duration: 6 months Study time span: June 2005 to not specified (at least 6 months because a 6‐month follow‐up was performed) |
|
| Participants | 341 college students aged 17 to 19 with any use of marijuana in the 3 months before study | |
| Interventions | Internet‐based personalised feedback intervention (USA). Participants were presented with feedback about their marijuana use, perceived and actual descriptive norms about marijuana use, and perceived pros and cons of using marijuana. Skills and training tips for avoiding marijuana and making changes in use were provided, as well as limited alcohol feedback. Perceived high‐risk contexts and alternative activities around campus and in the communities were provided | |
| Outcomes |
|
|
| Notes | Baseline survey, then 3‐ and 6‐month follow‐ups | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐based p. 267, "Students were randomly assigned to a personalized feedback intervention (PFI) or control condition based on their screening responses (prior to baseline), using a stratified randomization procedure to produce groups with equivalent use rates at randomization" |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 268: "Students in the intervention group received individual personalized feedback based on baseline information. On completion of the baseline survey, PFI participants could immediately view feedback online and could choose to print feedback to their own printer. Participants could return to view feedback on the web for 3 months" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Computer‐administered questionnaire (p. 266‐7) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | p. 268 "All analyses are based on intent‐to‐treat, regardless of whether participants viewed their feedback" |
| Selective reporting (reporting bias) | Unclear risk | p. 267 "All study procedures were approved by the university IRB and a federal Certificate of Confidentiality was obtained from the National Institutes of Health" |
Miller 2000.
| Methods | Study design: before and after study Sampling: random sampling Comparison group(s): no intervention (other campus with no intervention) Follow‐up duration: 1 year Study time span: 1988‐9, for 1.5 years |
|
| Participants | 1024 college students at baseline (median age 25 in the intervention group, 22 in the control group), 865 at 1‐year follow‐up | |
| Interventions | The Campuswide Alcohol and Drug Abuse Prevention Program (CADAPP; USA), based on self regulation theory. The campaign made use of printed materials, videotapes, speakers, peer‐education, computer resources, campus policy, campus wide events. Other components of CADAPP targeted particular at‐risk segments: free and confidential psychological 'drinker's checkup', list of drug/alcohol referral services available in the community, free psychological help for concerned family members and friends, alcohol self control training for on‐campus fraternities | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 746 "Impact of CADAPP was measured through anonymous surveys of students on each campus [..]" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | p. 751 "At baseline (fall) assessment, 1,400 surveys were distributed to enrolled UNM students, a sample of approximately 6% selected randomly by the university's computerized mailing list program. Of these, 567 surveys were returned and usable (41%). At the control campus, 1,080 surveys were distributed to a random sample of students, 457 of whom returned them (42.3%). [..] The return rates were 431 (31%) at UNM and 434 (34%) at NMSU" |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Newton 2010.
| Methods | Study design: randomised controlled trial Sampling: cluster sampling Comparison group(s): other type of communication interventions (usual health classes) Follow‐up duration: 12 months Study time span: March 2007 to November 2008 (21 months) |
|
| Participants | 764 13‐year‐old students from 10 Australian independent secondary schools (intervention branch: N = 397, 5 schools; control branch: N = 367, 5 schools). Students who enrol in independent schools come predominantly from high socioeconomic backgrounds | |
| Interventions | Climate Schools course (Australia) is an Internet‐based intervention founded on the social influence approach, derived from Bandura's social learning theory. The course delivered 2 sets of 6 40‐minute lessons, each including 15 to 20‐minute Internet‐based lesson completed individually and 20 to 25‐minute teacher‐delivered activities. During the Internet‐based part, students followed a cartoon storyline of teenagers experiencing real‐life situations and problems with alcohol and cannabis | |
| Outcomes |
|
|
| Notes | Assessment: baseline, immediately post, and 6 and 12 months following completion of the intervention Hybrid intervention: both school‐ and Internet‐based |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | p. 750 "The 10 participating schools were assigned randomly using an online randomization system (www.randomizer.org) to either the control condition (usual drug education) or the intervention condition (the Climate Schools: Alcohol and Cannabis course)" |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 750 "The Climate Schools: Alcohol and Cannabis course comprised the delivery of two sets of six 40‐minute lessons. The Climate Schools: Alcohol module was delivered immediately after the baseline assessment, and the Climate Schools: Alcohol and Cannabis module was delivered 6 months later in the same school year. Each lesson included a 15–20‐minute Internet‐based lesson completed individually, where students followed a cartoon storyline of teenagers experiencing real‐life situations and problems with alcohol and cannabis. The second part of each lesson was a predetermined activity delivered by the teacher to reinforce the information taught in the cartoons. Intervention group teachers were provided with a programme manual but no additional training." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | p. 751 "A self‐report questionnaire was completed online by all students in a classroom setting, where anonymity and confidentiality were assured" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar attrition % over the 2 study groups (figure 1, page 754) p. 754 "Compared to students who were present at baseline and any follow‐up occasion, students present only at baseline had significantly higher alcohol‐related knowledge [7.66 versus 7.48 (of 16); F(1, 758) = 4.88, P < 0.05]. There were no significant differences on any other alcohol or cannabis outcome measures, nor was there evidence of differential attrition" |
| Selective reporting (reporting bias) | Unclear risk | No study protocol was mentioned |
Palmgreen 1991.
| Methods | Study design: randomised controlled trial. Sampling: random sampling (students were recruited from a variety of sources, including driver's licence listings, recruitment advertisements in local newspapers and shopper weekly, etc) Comparison group(s): 2 experimental viewing conditions
Follow‐up duration: not applicable Study time span: not specified, at least 1 day |
|
| Participants | 207 18‐ to 22‐year‐old youths | |
| Interventions | 2 national‐quality 30‐second embedded PSAs, one aimed at HSS and the other at LSS (USA) | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not clearly reported p. 221 "LSSs ad HSSs were randomly assigned to one of the experimental conditions or the control group" |
| Allocation concealment (selection bias) | Unclear risk | Not reported No baseline comparisons reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessors not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data and clear reporting of sample size both of the intervention and control group |
| Selective reporting (reporting bias) | Low risk | No study protocol available but clear reporting of main study hypothesis (p. 219) and outcomes measures |
Palmgreen 2001.
| Methods | Study design: interrupted time series study Sampling: systematic sampling (geographical and grade stratification from enrolment lists of 7th to 10th graders in spring 1996) Comparison group(s): pre‐intervention surveys Follow‐up duration: n/a Study time span: March 1996 to December 1998 (34 months) |
|
| Participants | 6371 youths from 7th to 10th grade (12‐ to 17‐year‐olds), 3174 from Fayette County and 3197 youths from Knox County | |
| Interventions | 3 anti‐marijuana public service announcements televised from January through April 1997 and from January through April 1998 in Fayette and Knox Counties (USA). These advertisements were based on the SENTAR (sensation‐seeking targeting) prevention approach | |
| Outcomes |
|
|
| Notes | The 2 samples differed significantly on some independent (e.g. perceived peer and family drug use, delinquency) and dependent (use of marijuana) variables, although demographic and sensation‐seeking variables were consistent between the 2 samples | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 293 "Interviews were private and anonymous, with self‐administration of drug and alcohol items via laptop computer" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Polansky 1999.
| Methods | Study design: randomised controlled trial Sampling: systematic sampling (gender, classroom) Comparison group(s): 2 × 2 × 4 design (replication × gender × treatment) Follow‐up duration: not specified Study time span: not specified |
|
| Participants | 312 7th through to 9th graders from a rural south‐western Mexican‐American community | |
| Interventions | 3 substance abuse prevention videotapes (USA) derived from different theoretical frameworks: information‐based programming, social skills approach and assertiveness training (a subset of social skills approach) | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation procedure not clearly reported p. 189 "…and then randomly assigned to one of the four treatment and control conditions" |
| Allocation concealment (selection bias) | Unclear risk | Not reported No baseline comparisons reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 191 "to permit collating pre‐post protocols while preserving respondent anonymity, the students devised an identification code that they placed on all materials" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Unclear reporting of the size of both the intervention and control group Moreover unclear whether the final number of students (312) is the initial sample or is the final number of just those who answered (i.e. after drop‐out) Abstract "participants were 312 students" p. 189 "153 seventh and eighth grade student responses and 159 ninth‐grader responses were analysed" |
| Selective reporting (reporting bias) | Low risk | No study protocol available but all outcome measures expected (per hypothesis p. 188) have been reported, including those not statistically significant (p. 192/194) |
Scheier 2010.
| Methods | Study design: prospective cohort study Sampling: systematic sampling (representative of major racial groups) Comparison group(s): lower exposure to intervention Follow‐up duration: 48 months Study time span: April 1999 to March 2003 (48 months) |
|
| Participants | 2515 youth aged 12 to 18 interviewed by the National Survey of Parents and Youth (NSPY) | |
| Interventions | The National Youth Anti‐Drug Media Campaign (USA), already described in Hornik 2006 | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous and computer‐administered questionnaire p. 248 "Assessment of alcohol and drug use relied on an Anonymous Computer Assisted Self‐report Interview (ACASI)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Same as Hornik 2008 ("The overall response rate among youths for the first round was 65%, with 86% to 93% of still eligible youths interviewed in subsequent rounds", page 2230 Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings, page 2‐12, table 2‐A "Completed interviews by wave") |
| Selective reporting (reporting bias) | Unclear risk | Not applicable |
Schwinn 2010.
| Methods | Study design: randomised controlled trial Sampling: random sampling Comparison group(s): no intervention Follow‐up duration: 6 months Study time span: at least 8 months (not directly specified, but pretest was administered 6 weeks before intervention and last follow‐up was assessed after 6 months) |
|
| Participants | 236 girls aged 13 to 14 from 42 US states and 4 Canadian provinces, recruited through the youth‐oriented website Kiwibox.com™ | |
| Interventions | Internet‐based gender‐specific intervention (USA, Canada) composed by 12 sessions. This intervention is a pilot test of a gender‐specific intervention based on the social learning theory and employs a social competence and skill building strategy. High interaction | |
| Outcomes |
|
|
| Notes | Baseline and 6‐month follow‐up | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | p. 26 "After study enrolment, girls were randomly assigned to the intervention or control arm" |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 26 "After completing online pretest measures, intervention girls were immediately directed to the first program session. Control girls were thanked for their time and reminded that they would be notified when the next survey was available." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Computer‐administered questionnaire p. 26 "After completing online pretest measures, intervention girls were immediately directed to the first program session. [..] Immediately following completion of the last program module, girls in the intervention group completed the post‐test" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | p. 28 "Differential attrition was assessed across the three measurement occasions using the same variables analysed in baseline equivalency. Pretest to posttest attrition was 6.8%; the attrition rates for girls in intervention and control groups did not differ, X2 (1) = 1.74, p>0.05. At final follow‐up, attrition was 9%; again, rates did not differ by study group, X2 (1) = 0.84, p>0.05" |
| Selective reporting (reporting bias) | High risk | Protocol not mentioned. Subjective outcomes were not described in full but only as predictors of objective outcomes (substance use) |
Slater 2006.
| Methods | Study design: quasi‐randomised controlled trial (assignment to media condition was random; assignment to school condition was not fully random because of problem of staff scheduling in 7 of the 16 communities) Sampling: randomised cluster sampling (treatment and control communities were extracted from 4 major regions of the US) Comparison group(s): no intervention (8 intervention versus 8 non‐intervention communities) Follow‐up duration: 24 months Study time span: Autumn 1999 to Spring 2003 (˜42 months; but intervention lasted 24 months for each community, entry to the in project was different in different communities) |
|
| Participants | 4216 6th‐ and 7th‐grade students; mean age at baseline was 12.2 years | |
| Interventions | The 'Be Under Your Own Influence' programme (USA) is a school‐ and community‐based media effort on marijuana, alcohol and tobacco uptake. The programme emphasised "non‐use as an expression of personal identity and the consistency of non‐use with youth aspiration". The school‐based intervention was research‐based All Stars™ (13 sessions in the first year + 7 booster sessions in the second year); the community intervention was composed of workshops held by trained project staff | |
| Outcomes |
|
|
| Notes | This intervention ran concurrently with the Office of National Drug Policy's national anti‐drug campaign (Hornik 2006; Scheier 2010), but their simultaneous effect was not assessed in this study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Matching procedure described but no specification of random sequence generation |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessors not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Missing data have been imputed using appropriate methods (p. 161) |
| Selective reporting (reporting bias) | Low risk | No protocol available but the we do not suspect selective reporting bias |
Slater 2011.
| Methods | Study design: randomised controlled trial with a nested prospective cohort study Sampling: systematic sampling (schools were recruited based on National Center for Educational Statistics district listings) Comparison group(s): 4 groups, each including 10 schools and each comprising low to high exposure to the ONDCP campaign
Follow‐up duration: 24 months Study time span: Autumn 2005 to Spring 2009 (˜42 months) |
|
| Participants | 3236 students, mean age 12.4 ± 0.6 years | |
| Interventions | The Office of National Drug Control Policy's (ONDCP) 'Above the Influence' media campaign (USA) and a school‐ and community‐based mass media intervention, 'Be Under Your Own Influence' (BUYOI; USA). They both started in 2005 and ran concurrently
Although the ONDCP's campaign used far more creative executions given its funding levels, both campaigns were similar in concept, i.e. both linked substance use with autonomy and aspiration threats |
|
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Page 15 "Random assignment used a group‐matching procedure: NCES data on community demographics and location were used to generate possible randomization schemes in which major demographics and location were balanced to the degree possible across experimental conditions and one of the acceptable schemes was randomly selected." |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is unclear who administered the questionnaires and whether they were anonymous |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Reasons for missing outcome data unlikely to be related to true outcome |
| Selective reporting (reporting bias) | Low risk | No protocol available but the we do not suspect selective reporting |
Wyoming Meth 2011.
| Methods | Study design: interrupted time series study Sampling: 4‐stage probability sampling Comparison group(s): pre‐intervention survey Follow‐up duration: n/a Study time span: April 2008 to May 2011 (34 months) |
|
| Participants | 5700 youths (909 + 913 + 2652 + 1226) | |
| Interventions | Meth Project (USA), a "messaging campaign, supported by community outreach, and public policy initiatives". The campaign comprises "television, radio, print, billboard, and Internet advertising" | |
| Outcomes |
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not applicable |
| Allocation concealment (selection bias) | Unclear risk | Not applicable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaires |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported |
| Selective reporting (reporting bias) | Unclear risk | No information regarding potential reporting bias |
Yzer 2003.
| Methods | Study design: randomised controlled trial Sampling: random sampling (from middle and high schools) Comparison group(s):
Follow‐up duration: not applicable (post‐only design) Study time span: March 2000 to not specified |
|
| Participants | 418 students of middle/high schools in urban Philadelphia, mean age 14 ± 1.89 years | |
| Interventions | Anti‐marijuana and anti‐hard drugs advertisements embedded in a documentary video (USA) | |
| Outcomes |
|
|
| Notes | Similar to Zhao 2006, many of the authors wrote both papers | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomly assigned to 1 of the 4 experimental conditions, and the stimuli were randomly presented using a randomisation feature in MediaLab software. (Personal communication with the author) |
| Allocation concealment (selection bias) | Low risk | Participants did not know which condition they were assigned to, and thus did not know which stimuli they and participants in other conditions were exposed to. (Personal communication with the author) |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Anonymous questionnaire p. 135 "All videos and the questionnaire were programmed onto a laptop computer using an interactive program that allows random ordering of questions and videos within blocks" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There were no missing data. (Personal communication with the author) |
| Selective reporting (reporting bias) | Low risk | No protocol available but the we do not suspect selective reporting bias |
Zhao 2006.
| Methods | Study design: randomised controlled trial Sampling: not specified (informational letters to parents in the 2 school‐based studies, mall‐intercept of lists held by market researchers for the mall‐based study) Comparison group(s): no intervention (documentary about television production, without the embedded anti‐marijuana advertisements) Follow‐up duration: not applicable (post‐only design) Study time span: not specified |
|
| Participants | 435 youths whose mean age was 15.2 ± 1.88 years | |
| Interventions | 3 anti‐marijuana advertisements (USA) addressing normative beliefs. The advertisements were embedded and randomly included in a video documentary about television production | |
| Outcomes |
|
|
| Notes | Results were based on combined data from 3 studies done at different points in time, but "identical in terms of methodology, procedures, experimental conditions, ad the structure of the outcome questionnaire". However, whereas study 1 and 2 were collected at middle and high schools, study 3 was conducted at various malls around the country | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | p. 190 "Participants were randomly assigned to condition", but randomisation details are not reported |
| Allocation concealment (selection bias) | Low risk | Although full allocation concealment is not possible for this kind of study, there is low risk of selection bias because researchers administering the intervention were unlikely to know the children. See p. 190: "The experimental group saw the three advertisements that challenged undesirable normative beliefs about marijuana use (see Table 1 for a description of the messages). The advertisements were embedded and randomly rotated in a video documentary about television production. The control group was not exposed to any anti‐marijuana messages but saw the same documentary as the experimental group" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Computer‐administered questionnaire p. 191 "The instrument (including the video clips) was programmed onto laptop computers using an interactive program called MediaLab (Jarvis, 1998), which allows random ordering of blocks of questions and videos within the questionnaire" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed the test (being a post‐only design); p. 190 "All three studies used the same between‐subjects, post‐only design, with one experimental condition and one control condition" |
| Selective reporting (reporting bias) | Unclear risk | No study protocol was mentioned |
n/a: not applicable PSA: public service announcement
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Alemi 1996 | Target population is pregnant women who already use or used cocaine |
| An 2007 | This intervention aims to promote inquiry of prescription medicines/treatments, not to hinder use of illicit drugs |
| Andrews 1995 | The purpose of the campaign was to promote public awareness of the link between addiction and child maltreatment, not to prevent addiction |
| Barber 1990 | Target population mean age is 40 |
| Beaudoin 2007 | Presented outcomes are not included among those of this review |
| Beck 2008 | Overview of drugs prevalence and school‐based prevention interventions in France. Some information about therapeutic interventions, but no information about mass media prevention interventions |
| Belenko 2009 | This study analyses data from the National Survey of Parents and Youth, which was not designed to provide quality information about exposure to anti‐ or pro‐drug websites. This study aims to find factors (e.g. gender, parent‐reported income, prior exposure to drugs) associated with viewing of drug websites, not to assess whether viewing of anti‐drug websites can influence outcomes included in the protocol of this review |
| Black 1994 | This study aims to assess consistency of data collected with 2 different sampling methods |
| Brannon 1989 | None of the evaluated outcomes (i.e. participation, satisfaction and perceived efficacy of programme) met the inclusion criteria for this review |
| Chambers 2005 | Not a mass media intervention |
| Chiauzzi 2008 | This study assesses the effectiveness of an online stress management tool. Outcomes do not include substance use, intention to use or any other outcome relevant to this review |
| Collins 1991 | This paper aims to prevent alcohol abuse |
| Cook 1999 | Review of books and media, not of studies |
| David 2006 | Evaluated intervention is adolescent discussion about anti‐drug advertisements, not advertisements themselves |
| DeJong 1999 | This paper raises concern about the Office of National Drug Control Policy (ONDCP)'s National Youth Anti‐Drug Media Campaign without reporting results of its effectiveness assessment |
| Di Noia 2003 | The majority of recruited professionals were older than 26 and the assessed outcomes are not among those needed for inclusion |
| Donohew 2000 | The aim of the study is to understand the relationship between mediators (sensation‐seeking and decision‐making processes) and alcohol and risky sexual behaviours in adolescents |
| Epstein 1999 | Survey with control group but without pre‐intervention questionnaire |
| Erceg‐Hurn 2008 | It is not possible to compare different years due to the different methodology used in surveys (see also commentary paper Erceg‐Hurn 2008) |
| Everett 1995 | This study does not evaluate intervention effectiveness but matching between HSV/LSV interventions and HSV/LSV subjects |
| Flay 2000 | Reviews of mainly anti‐tobacco media‐, school‐ and community‐based interventions |
| Hannon 2000 | Narrative review of key African American community values and provides recommendations as to how this information might be incorporated into the development of anti‐drug messages and materials targeted at African Americans |
| Harrington 2003 | This study does not evaluate intervention effectiveness but matching between HSV/LSV interventions and HSV/LSV subjects |
| Helme 2007 | Intervention was an anti‐smoking campaign |
| Johnson 1990 | The mass media intervention was administered to both study groups |
| Jordan 2005 | This study design (survey) does not allow us to evaluate intervention effectiveness |
| Kang 2009 | This study is an evaluation of the perceived effectiveness of specific elements of the interventions, not the effectiveness of whole interventions on outcome variables included in the protocol for this review |
| Know the Score 2007 | For the 2 cocaine reports: the 4 study waves differed slightly but in many respects (age and working status of respondents, survey locations and, more importantly, survey questions) For the 2 heroin reports: respondent age is not fully comparable across study waves. Additionally, participants in waves 1 and 3 were older than 25 |
| Lorch 1994 | No pretest drug‐related measure was taken. This study aims to predict responses to PSA and drug use by different sensation‐seeking profiles |
| Lubman 2007 | Narrative review on substance addiction prevention. Data were not presented here |
| Marsiglia 2009 | This study evaluates a school‐based intervention which has no media‐related component |
| Myers 2006 | Not a prevention intervention. It does not include illicit drug‐related outcomes |
| Palmgreen 2007 | This study does not evaluate intervention effectiveness but matching between the intervention and HSV/LSV subjects |
| Pentz 1990 | The fffect of the mass media component could not be disentangled from other components |
| Ramirez 1999 | Description of theoretical basis, development and implementation of 'Mirame!/Look at Me!' media‐ and school‐based programme for substance abuse among Hispanic youth. However, the programme's effectiveness was not assessed |
| Reis 1994 | Survey. This study design does not allow us to evaluate intervention effectiveness |
| Ruggiero 2006 | Participants are older than 26 |
| Schmeling 1980 | Intervention targets prescription drug abusers |
| Siegel 2008 | No blank control, one group focusing on physical harms of inhalant use, the other focusing on social harms |
| Skinner 1995a | The outcome (perceived persuasiveness) is not among the outcome measures included in our protocol |
| Sloboda 2006 | This book does not include data on studies evaluating mass media programmes |
| Spitzer 2010 | Outcomes concern 'values' and therefore do not meet the inclusion criteria |
| Stephenson 2002 | The aim of this study was to find predictors of exposure from an anti‐marijuana media campaign, not to evaluate the effectiveness of the campaign |
| Stephenson 2002a | CBA study aiming to link perceived message sensation value and viewer's reaction to an anti‐heroin PSA |
| Stephenson 2003 | Survey with control group aiming to evaluate sensation‐seeking as a moderating variable |
| Stephenson 2005 | This study analyses the content of ads but does not assess their effectiveness |
| Stevens 1996 | School‐based intervention with added community activities |
| Stryker 2003 | Ecological study about the impact of media coverage of the negative consequences of marijuana use. This study does not assess the effectiveness of a single prevention intervention |
| Sussman 1987 | Survey with a control group but without a pre‐intervention questionnaire |
| Tait 2010 | Systematic review on Internet‐based interventions for the treatment of alcohol misuse |
| Taylor 1984 | Outcomes in the pilot study (the statewide intervention was not evaluated) were knowledge, attitudes and behaviours about friendships and human relationships, not substance use/misuse |
| Varshavsky 2003 | Qualitative content analysis of a national campaign |
| Werch 2010 | Not a mass media intervention |
CBA: controlled before and after (study) PSA: public service announcement
HSV: high sensation value
LSV: low sensation value
Characteristics of studies awaiting assessment [ordered by study ID]
Block 2002.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We contacted authors for results and are waiting for a response |
Duncan 2000.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We contacted authors for results and are waiting for a response |
Flay 1986.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to retrieve the paper's full text |
Longshore 2006.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We contacted authors for results and are waiting for a response |
Marsch 2007.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to retrieve the paper's full text |
Moore 2011.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to retrieve the paper's full text |
Moreno 2009.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We contacted authors for results and are waiting for a response |
Skinner 1995.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to retrieve the paper's full text |
Williams 2005.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We contacted authors for results and are waiting for a response |
Contributions of authors
Marica Ferri and Fabrizio Faggiano conceived the systematic review and overviewed study inclusion and exclusion, methodological assessment of studies, and wrote the review. Marica Ferri and Elias Allara selected the studies for inclusion. Alessandra Bo and Elias Allara extracted the data from the studies and contributed to writing the review; Elias Allara contacted the trial authors for further information. Along with Alessandra Bo, Elias Allara input data for meta‐analysis into Review Manager. Antonio Gasparrini and Elias Allara did the meta‐analysis of interrupted time series studies.
Marica Ferri, Fabrizio Faggiano, Elias Allara and Alessandra Bo regularly discussed each step of review process and equally participated in each decision regarding the studies and the analysis.
Marica Ferri, Gregor Burkhart and Fabrizio Faggiano conceived the protocol, Elias Allara and Alessandra Bo performed the preliminary search strategy and participated in writing the protocol. Anna V Gyarmathy provided input to the protocol for the theories description and editing of the text.
Sources of support
Internal sources
-
European Monitoring Centre for Drugs and Drug Addiction, Portugal.
The authors were allowed to use their working time, the offices and the working resources (computers, printers, internet access) to conduct the systematic review.
External sources
No sources of support supplied
Declarations of interest
None of the authors report conflict of interest.
New
References
References to studies included in this review
Carpenter 2011 {published data only}
- Carpenter CS, Pechmann C. Exposure to the Above the Influence antidrug advertisements and adolescent marijuana use in the United States, 2006‐2008. American Journal of Public Health 2011;101(5):948‐54. [PUBMED: 21421952] [DOI] [PMC free article] [PubMed] [Google Scholar]
Colorado Meth 2011 {published and unpublished data}
- Colorado Meth: Use & Attitudes Survey 2011. The Meth Project 2011.
Czyzewska 2007 {published data only}
- Czyzewska M, Ginsburg HJ. Explicit and implicit effects of anti‐marijuana and anti‐tobacco TV advertisements. Addictive Behaviors 2007;32(1):114‐27. [PUBMED: 16675148] [DOI] [PubMed] [Google Scholar]
Fang 2010 {published data only}
- Fang L, Schinke SP, Cole KC. Preventing substance use among early Asian‐American adolescent girls: initial evaluation of a web‐based, mother‐daughter program. Journal of Adolescent Health 2010;47(5):529‐32. [PUBMED: 20970090] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fishbein 2002 {published data only}
- Fishbein M, Hall‐Jamieson K, Zimmer E, Haeften I, Nabi R. Avoiding the boomerang: testing the relative effectiveness of antidrug public service announcements before a national campaign. American Journal of Public Health 2002;92(2):238‐45. [PUBMED: 11818299] [DOI] [PMC free article] [PubMed] [Google Scholar]
Georgia Meth 2011 {published and unpublished data}
- Georgia Meth: Use & Attitudes Survey 2011. The Meth Project 2011.
Hawaii Meth 2011 {published and unpublished data}
- Hawaii Meth: Use & Attitudes Survey 2011. The Meth Project 2011.
Hornik 2006 {published data only}
- Hornik R. Personal influence and the effects of the National Youth Anti‐Drug Media Campaign. The ANNALS of the American Academy of Political and Social Science 2006;608(1):282‐300. [Google Scholar]
- Hornik R, Jacobsohn L. The best laid plans: disappointments of the National Youth Anti‐Drug Media Campaign. LDI Issue Brief 2008;14(2):1‐4. [PUBMED: 19288618] [PubMed] [Google Scholar]
- Hornik R, Jacobsohn L, Orwin R, Piesse A, Kalton G. Effects of the National Youth Anti‐Drug Media Campaign on youths. American Journal of Public Health 2008;98(12):2229‐36. [PUBMED: 18923126] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orwin R, Cadell D, Chu A, Kalton G, Maklan D, Morin C, et al. Evaluation of the National Youth Anti‐Drug Media Campaign: 2004 Report of Findings. Westat, 2006. [Google Scholar]
Idaho Meth 2010 {published and unpublished data}
- Idaho Meth: Use & Attitudes Survey 2010. The Meth Project 2010.
Kelly 1992 {published data only}
- Kelly K, Edwards R. Observations: Does discussion of advertising transform its effects? Yes...sometimes: A case among college students and their response to anti‐drug advertising. Journal of Advertising Research 1992;32(4):79‐83. [Google Scholar]
Lee 2010 {published data only}
- Lee CM, Neighbors C, Kilmer JR, Larimer ME. A brief, web‐based personalized feedback selective intervention for college student marijuana use: a randomized clinical trial. Psychology of Addictive Behaviors 2010;24(2):265‐73. [PUBMED: 20565152] [DOI] [PMC free article] [PubMed] [Google Scholar]
Miller 2000 {published data only}
- Miller WR, Toscova RT, Miller JH, Sanchez V. A theory‐based motivational approach for reducing alcohol/drug problems in college. Health Education and Behavior 2000;27(6):744‐59. [PUBMED: 11104373] [DOI] [PubMed] [Google Scholar]
Newton 2010 {published and unpublished data}
- Newton NC, Andrews G, Teesson M, Vogl LE. Delivering prevention for alcohol and cannabis using the Internet: a cluster randomised controlled trial. Preventive Medicine 2009;48(6):579‐84. [PUBMED: 19389420] [DOI] [PubMed] [Google Scholar]
- Newton NC, Teesson M, Vogl LE, Andrews G. Internet‐based prevention for alcohol and cannabis use: final results of the Climate Schools course. Addiction 2010;105(4):749‐59. [PUBMED: 20148791] [DOI] [PubMed] [Google Scholar]
Palmgreen 1991 {published data only}
- Palmgreen P, Donohew L, Lorch EP, Rogus M, Helm D, Grant N. Sensation seeking, message sensation value, and drug use as mediators of PSA effectiveness. Health Communication 1991;3(4):217‐27. [Google Scholar]
Palmgreen 2001 {published data only}
- Palmgreen P, Donohew L, Lorch EP, Hoyle RH, Stephenson MT. Television campaigns and adolescent marijuana use: tests of sensation seeking targeting. American Journal of Public Health 2001;91(2):292‐6. [PUBMED: 11211642] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephenson MT, Palmgreen P, Hoyle RH, Donohew L, Lorch EP, Colon SE. Short‐term effects of an anti‐marijuana media campaign targeting high sensation seeking adolescents. Journal of Applied Communication Research 1999;27(3):175‐95. [Google Scholar]
Polansky 1999 {unpublished data only}
- Polansky JM, Buki LP, Horan JJ, Ceperich SD, Burows DD. The effectiveness of substance abuse prevention videotapes with Mexican American adolescents. Hispanic Journal of Behavioral Sciences 1999;21(2):186‐98. [Google Scholar]
Scheier 2010 {published data only}
- Scheier LM, Grenard JL. Influence of a nationwide social marketing campaign on adolescent drug use. Journal of Health Communication 2010;15(3):240‐71. [PUBMED: 20432107] [DOI] [PubMed] [Google Scholar]
Schwinn 2010 {published data only}
- Schwinn TM, Schinke SP, Noia J. Preventing drug abuse among adolescent girls: outcome data from an internet‐based intervention. Prevention Science 2010;11(1):24‐32. [PUBMED: 19728091] [DOI] [PMC free article] [PubMed] [Google Scholar]
Slater 2006 {unpublished data only}
- Slater MD, Kelly KJ, Edwards RW, Thurman PJ, Plested BA, Keefe TJ, et al. Combining in‐school and community‐based media efforts: reducing marijuana and alcohol uptake among younger adolescents. Health Education Research 2006;21(1):157‐67. [PUBMED: 16199491] [DOI] [PubMed] [Google Scholar]
Slater 2011 {published data only}
- Slater MD, Kelly KJ, Lawrence FR, Stanley LR, Comello ML. Assessing media campaigns linking marijuana non‐use with autonomy and aspirations: "Be Under Your Own Influence" and ONDCP's "Above the Influence". Prevention Science 2011;12(1):12‐22. [PUBMED: 21271357] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wyoming Meth 2011 {published and unpublished data}
- Wyoming Meth: Use & Attitudes Survey 2011. The Meth Project 2011.
Yzer 2003 {unpublished data only}
- Yzer MC, Cappella JN, Fishbein M, Hornik R, Ahern RK. The effectiveness of gateway communications in anti‐marijuana campaigns. Journal of Health Communication 2003;8(2):129‐43. [PUBMED: 12746037] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhao 2006 {published data only}
- Zhao X, Sayeed S, Cappella J, Hornik R, Fishbein M, Ahern RK. Targeting norm‐related beliefs about marijuana use in an adolescent population. Health Communication 2006;19(3):187‐96. [PUBMED: 16719722] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Alemi 1996 {published data only}
- Alemi F, Stephens RC, Javalghi RG, Dyches H, Butts J, Ghadiri A. A randomized trial of a telecommunications network for pregnant women who use cocaine. Medical Care 1996;34(10 Suppl):OS10‐20. [PUBMED: 8843933] [DOI] [PubMed] [Google Scholar]
An 2007 {published data only}
- An S. Attitude toward direct‐to‐consumer advertising and drug inquiry intention: the moderating role of perceived knowledge. Journal of Health Communication 2007;12(6):567‐80. [PUBMED: 17763053] [DOI] [PubMed] [Google Scholar]
Andrews 1995 {published data only}
- Andrews AB, McLeese DG, Curran S. The impact of a media campaign on public action to help maltreated children in addictive families. Child Abuse and Neglect 1995;19(8):921‐32. [PUBMED: 7583751] [DOI] [PubMed] [Google Scholar]
Barber 1990 {published data only}
- Barber JJ, Grichting WL. Australia's media campaign against drug abuse. International Journal of the Addictions 1990;25(6):693‐708. [DOI] [PubMed] [Google Scholar]
Beaudoin 2007 {published data only}
- Beaudoin CE, Thorson E. Evaluating the effects of a youth health media campaign. Journal of Health Communication 2007;12(5):439‐54. [PUBMED: 17710595] [DOI] [PubMed] [Google Scholar]
Beck 2008 {published data only}
- Beck F, Legleye S, Obradovic I, Mutatayi C, Cohen B, Karila L. Drug use among youths [Les plus jeunes adolescents face aux drogues: reperage des usages problematiques et elements de reponse institutionnelle en France.]. Medecine Sciences: M/S 2008;24(8‐9):758‐67. [PUBMED: 18789225] [DOI] [PubMed] [Google Scholar]
Belenko 2009 {published data only}
- Belenko S, Dugosh KL, Lynch K, Mericle AA, Pich M, Forman RF. Online illegal drug use information: an exploratory analysis of drug‐related website viewing by adolescents. Journal of Health Communication 2009;14(7):612‐30. [PUBMED: 19851914] [DOI] [PubMed] [Google Scholar]
Black 1994 {published data only}
- Black GS, Zastowny TR, Green PJ, Adams EH, Lawton KB. The consistency of estimates obtained through central‐location sampling: analysis of the Partnership for a Drug‐Free America Attitude Tracking Study. American Journal of Drug and Alcohol Abuse 1994;20(2):199‐222. [DOI] [PubMed] [Google Scholar]
Brannon 1989 {published data only}
- Brannon BR, Dent CW, Flay BR, Smith G, Sussman S, Pentz MA, et al. The television, school, and family project. V. The impact of curriculum delivery format on program acceptance. Preventive Medicine 1989;18(4):492‐502. [PUBMED: 2798371] [DOI] [PubMed] [Google Scholar]
Chambers 2005 {published data only}
- Chambers M, Connor SL, McElhinney S. Substance use and young people: the potential of technology. Journal of Psychiatric and Mental Health Nursing 2005;12(2):179‐86. [PUBMED: 15788035] [DOI] [PubMed] [Google Scholar]
Chiauzzi 2008 {published data only}
- Chiauzzi E, Brevard J, Thum C, Decembrele S, Lord S. MyStudentBody‐Stress: an online stress management intervention for college students. Journal of Health Communication 2008;13(6):555‐72. [PUBMED: 18726812] [DOI] [PubMed] [Google Scholar]
Collins 1991 {published data only}
- Collins D, Cellucci T. Effects of a school‐based alcohol education program with a media prevention component. Psychological Reports 1991;69(1):191‐7. [PUBMED: 1961790] [DOI] [PubMed] [Google Scholar]
Cook 1999 {published data only}
- Cook C. Book and media reviews. Addiction Biology 1999;4(2):245‐51. [PUBMED: 20575792] [Google Scholar]
David 2006 {published data only}
- David C, Cappella Joseph N, Fishbein M. The social diffusion of influence among adolescents: group interaction in a chat room environment about antidrug advertisements. Communication Theory 2006;16(1):118‐40. [Google Scholar]
DeJong 1999 {published data only}
- DeJong W, Wallack L. A critical perspective on the drug czar's antidrug media campaign. Journal of Health Communication 1999;4(2):155‐60. [PUBMED: 10977283] [DOI] [PubMed] [Google Scholar]
Di Noia 2003 {published data only}
- Noia J, Schwinn TM, Dastur ZA, Schinke SP. The relative efficacy of pamphlets, CD‐ROM, and the Internet for disseminating adolescent drug abuse prevention programs: an exploratory study. Preventive Medicine 2003;37(6 Pt 1):646‐53. [PUBMED: 14636798] [DOI] [PMC free article] [PubMed] [Google Scholar]
Donohew 2000 {published data only}
- Donohew L, Zimmerman R, Cupp PS, Novak S, Colon S, Abell R. Sensation seeking, impulsive decision‐making, and risky sex: implications for risk‐taking and design of interventions. Personality and Individual Differences 2000;28(6):1079‐91. [Google Scholar]
Epstein 1999 {published data only}
- Epstein J, McGaha AC. ATOD‐TV: evaluation of a multimedia program designed to educate the public about substance abuse. Computers in Human Behavior 1999;15(1):73‐83. [Google Scholar]
Erceg‐Hurn 2008 {published and unpublished data}
- Montana Meth: Use & Attitudes Survey 2008. The Meth Project 2008.
- Erceg‐Hurn DM. Drugs, money, and graphic ads: a critical review of the Montana Meth Project. Prevention Science 2008;9(4):256‐63. [PUBMED: 18686033] [DOI] [PubMed] [Google Scholar]
Everett 1995 {published data only}
- Everett MW, Palmgreen P. Influences of sensation seeking, message sensation value, and program context on effectiveness of anticocaine public service announcements. Health Communication 1995;7(3):225‐48. [Google Scholar]
Flay 2000 {published data only}
- Flay BR. Approaches to substance use prevention utilizing school curriculum plus social environment change. Addictive Behaviors 2000;25(6):861‐85. [DOI] [PubMed] [Google Scholar]
Hannon 2000 {published data only}
- Hannon SW. Background and principles of an African American targeted national anti‐drug campaign. Journal of Public Health Management and Practice 2000;6(3):65‐71. [PUBMED: 10848485] [DOI] [PubMed] [Google Scholar]
Harrington 2003 {published data only}
- Harrington NG, Lane DR, Donohew L, Zimmerman RS, Norling GR, An JH, et al. Persuasive strategies for effective anti‐drug messages. Communication Monographs 2003;70(1):1‐1. [Google Scholar]
Helme 2007 {published data only}
- Helme DW, Donohew RL, Baier M, Zittleman L. A classroom‐administered simulation of a television campaign on adolescent smoking: testing an activation model of information exposure. Journal of Health Communication 2007;12(4):399‐415. [PUBMED: 17558790] [DOI] [PubMed] [Google Scholar]
Johnson 1990 {published data only}
- Johnson CA, Pentz MA, Weber MD, Dwyer JH, Baer N, MacKinnon DP, et al. Relative effectiveness of comprehensive community programming for drug abuse prevention with high‐risk and low‐risk adolescents. Journal of Consulting and Clinical Psychology 1990;58(4):447‐56. [PUBMED: 2212182] [DOI] [PubMed] [Google Scholar]
Jordan 2005 {published data only}
- Jordan S. www.drugcom.de‐‐an Internet based information and counselling project for the prevention of addiction [www.drugcom.de‐‐ein Informations‐ und Beratungsangebot zur Suchtpravention im Internet.]. Praxis der Kinderpsychologie und Kinderpsychiatrie 2005;54(9):742‐54. [PUBMED: 16305021] [PubMed] [Google Scholar]
Kang 2009 {published data only}
- Kang Y, Cappella JN, Fishbein M. The effect of marijuana scenes in anti‐marijuana public service announcements on adolescents' evaluation of ad effectiveness. Health Communication 2009;24(6):483‐93. [PUBMED: 19735026] [DOI] [PMC free article] [PubMed] [Google Scholar]
Know the Score 2007 {published data only}
- Binnie I, Kinver A, Lam P. Know the Score: Cocaine Wave 3 – 2005/06 Post‐Campaign Evaluation. Scottish Executive Social Research, June 2006. [Google Scholar]
- Phillips R, Kinver A. Know the Score: Cocaine Wave 4 – 2006/07 Post‐campaign Evaluation. Scottish Executive Social Research, February 2007. [Google Scholar]
- TNS System Three. Know the Score – Heroin 2005 Pre‐ and Post‐Campaign Evaluation. Scottish Executive Social Research, 2006. [Google Scholar]
- TNS System Three. Know the Score: Anti‐Heroin 2006/07 Campaign Evaluation. Scottish Executive Social Research, 2006. [Google Scholar]
Lorch 1994 {published data only}
- Lorch EP, Palmgreen P, Donohew L, Helm D, Baer SA, Dsilva MU. Program context, sensation seeking, and attention to televised anti‐drug public service announcements. Human Communication Research 1994;20(3):390‐412. [Google Scholar]
Lubman 2007 {published data only}
- Lubman DI, Hides L, Yucel M, Toumbourou JW. Intervening early to reduce developmentally harmful substance use among youth populations. Medical Journal of Australia 2007;187(7 Suppl):S22‐5. [PUBMED: 17908020] [DOI] [PubMed] [Google Scholar]
Marsiglia 2009 {published data only}
- Marsiglia FF, Kulis S, Rodriguez GM, Becerra D, Castillo J. Culturally specific youth substance abuse resistance skills: applicability across the U.S.‐Mexico border. Research on Social Work Practice 2009;19(2):152‐64. [PUBMED: 19924268] [DOI] [PMC free article] [PubMed] [Google Scholar]
Myers 2006 {published data only}
- Myers K, Valentine J, Morganthaler R, Melzer S. Telepsychiatry with incarcerated youth. Journal of Adolescent Health 2006;38(6):643‐8. [PUBMED: 16730590] [DOI] [PubMed] [Google Scholar]
Palmgreen 2007 {published data only}
- Palmgreen P, Lorch EP, Stephenson MT, Hoyle RH, Donohew L. Effects of the Office of National Drug Control Policy's Marijuana Initiative Campaign on high‐sensation‐seeking adolescents. American Journal of Public Health 2007;97(9):1644‐9. [PUBMED: 17395843] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pentz 1990 {published data only}
- Pentz MA, Trebow EA, Hansen WB, MacKinnon DP, Dwyer JH, Johnson CA, et al. Effects of program implementation on adolescent drug use behavior: the Midwestern Prevention Project (MPP). Evaluation Review 1990;14(3):264‐89. [Google Scholar]
Ramirez 1999 {published data only}
- Ramirez AG, Gallion KJ, Espinoza R, Chalela P. Developing a media‐ and school‐based program for substance abuse prevention among Hispanic youth: a case study of Mirame!/Look at Me!. Nicotine and Tobacco Research 1999;1 Suppl 1:S99‐104. [PUBMED: 11072412] [DOI] [PubMed] [Google Scholar]
Reis 1994 {published data only}
- Reis EC, Duggan AK, Adger HJ, DeAngelis C. The impact of anti‐drug advertising. Perceptions of middle and high school students. Archives of Pediatrics & Adolescent Medicine 1994;148(12):1262‐8. [PUBMED: 7951804] [DOI] [PubMed] [Google Scholar]
Ruggiero 2006 {published data only}
- Ruggiero KJ, Resnick HS, Acierno R, Coffey SF, Carpenter MJ, Ruscio AM, et al. Internet‐based intervention for mental health and substance use problems in disaster‐affected populations: a pilot feasibility study. Behavior Therapy 2006;37(2):190‐205. [PUBMED: 16942971] [DOI] [PubMed] [Google Scholar]
Schmeling 1980 {published data only}
- Schmeling DG, Wotring CE. Making anti‐drug‐abuse advertising work. Journal of Advertising Research 1980; Vol. 20, issue 3:33‐7.
Siegel 2008 {published data only}
- Siegel JT, Alvaro EM, Crano WD, Skenderian J, Lac A, Patel N. Influencing inhalant intentions by changing socio‐personal expectations. Prevention Science 2008;9(3):153‐65. [PUBMED: 18543103] [DOI] [PMC free article] [PubMed] [Google Scholar]
Skinner 1995a {published data only}
- Skinner ER, Slater MD. Family communication patterns, rebelliousness, and adolescent reactions to anti‐drug PSAs. Journal of Drug Education 1995;25(4):343‐55. [DOI] [PubMed] [Google Scholar]
Sloboda 2006 {published data only}
- Sloboda Z, Bukoski WJ (editors). Handbook of Drug Abuse Prevention. Boston, MA: Springer US, 2006. [9780387354088] [Google Scholar]
Spitzer 2010 {published data only}
- Spitzer JE. Above the Influence: a Value Analysis of Anti‐drug Public Service Announcements. ProQuest Dissertation, 2010. [750165158; 9781124200040] [Google Scholar]
Stephenson 2002 {published data only}
- Stephenson MT, Morgan SE, Lorch EP, Palmgreen P, Donohew L, Hoyle RH. Predictors of exposure from an antimarijuana media campaign: outcome research assessing sensation seeking targeting. Health Communication 2002;14(1):23‐43. [PUBMED: 11853208] [DOI] [PubMed] [Google Scholar]
Stephenson 2002a {published data only}
- Stephenson MT. Sensation seeking as a moderator of the processing of anti‐heroin PSAs. Communication Studies 2002;53(4):358‐80. [Google Scholar]
Stephenson 2003 {published data only}
- Stephenson MT. Examining adolescents' responses to antimarijuana PSAs. Human Communication Research 2003;29(3):343‐69. [Google Scholar]
Stephenson 2005 {published data only}
- Stephenson MT, Quick BL. Parent ads in the National Youth Anti‐Drug Media Campaign. Journal of Health Communication 2005;10(8):701‐10. [PUBMED: 16316934] [DOI] [PubMed] [Google Scholar]
Stevens 1996 {published data only}
- Stevens MM, Freeman DHJ, Mott L, Youells F. Three‐year results of prevention programs on marijuana use: the New Hampshire study. Journal of Drug Education 1996;26(3):257‐73. [PUBMED: 8952210] [DOI] [PubMed] [Google Scholar]
Stryker 2003 {published data only}
- Stryker JE. Media and marijuana: A longitudinal analysis of news media effects on adolescents' marijuana use and related outcomes, 1977‐1999. Journal of Health Communication 2003;8(4):305‐28. [PUBMED: 12907398] [DOI] [PubMed] [Google Scholar]
Sussman 1987 {published data only}
- Sussman S, Flay BR, Sobel JL, Rauch JM, Hansen WB, Johnson CA. Viewing and evaluation of a televised drug education program by students previously or concurrently exposed to school‐based substance abuse prevention programming. Health Education Research 1987;2(4):373‐83. [Google Scholar]
Tait 2010 {published data only}
- Tait RJ, Christensen H. Internet‐based interventions for young people with problematic substance use: a systematic review. Medical Journal of Australia 2010;192(11 Suppl):S15‐21. [PUBMED: 20528701] [DOI] [PubMed] [Google Scholar]
Taylor 1984 {published data only}
- Taylor RL, Lam DJ, Roppel CE, Barter JT. Friends can be good medicine: an excursion into mental health promotion. Community Mental Health Journal 1984;20(4):294‐303. [PUBMED: 6518742] [DOI] [PubMed] [Google Scholar]
Varshavsky 2003 {published data only}
- Varshavsky T. Media drug prevention and public service advertising: evaluating The National Youth Anti‐Drug Media Campaign. Communication and Media Studies Senior Thesis 2003.
Werch 2010 {published data only}
- Werch CE, Bian H, Diclemente CC, Moore MJ, Thombs D, Ames SC, et al. A brief image‐based prevention intervention for adolescents. Psychology of Addictive Behaviors 2010;24(1):170‐5. [PUBMED: 20307126] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Block 2002 {unpublished data only}
- Block LG, Morwitz VG, Putsis WPJ, Sen SK. Assessing the impact of antidrug advertising on adolescent drug consumption: results from a behavioral economic model. American Journal of Public Health 2002;92(8):1346‐51. [PUBMED: 12144995] [DOI] [PMC free article] [PubMed] [Google Scholar]
Duncan 2000 {published and unpublished data}
- Duncan TE, Duncan SC, Beauchamp N, Wells J, Ary DV. Development and evaluation of an interactive CD‐ROM refusal skills program to prevent youth substance use: "refuse to use". Journal of Behavioral Medicine 2000;23(1):59‐72. [PUBMED: 10749011] [DOI] [PubMed] [Google Scholar]
Flay 1986 {published data only}
- Flay BR. Mass media linkages with school‐based programs for drug abuse prevention. Journal of School Health 1986;56(9):402‐6. [PUBMED: 3537525] [DOI] [PubMed] [Google Scholar]
Longshore 2006 {published and unpublished data}
- Longshore D, Ghosh‐Dastidar B, Ellickson PL. National Youth Anti‐Drug Media Campaign and school‐based drug prevention: Evidence for a synergistic effect in ALERT Plus. Addictive Behaviors 2006;31(3):496‐508. [PUBMED: 15979245] [DOI] [PubMed] [Google Scholar]
Marsch 2007 {published data only}
- Marsch LA, Bickel WK, Grabinski MJ. Application of interactive, computer technology to adolescent substance abuse prevention and treatment. Adolescent Medicine: State of the Art Reviews 2007;18(2):342‐56, xii. [PUBMED: 18605650] [PubMed] [Google Scholar]
Moore 2011 {published data only}
- Moore LS. After Six Years...: an Examination of the Effectiveness of the Above The Influence Campaign on Its Initial Target Audience (Master's thesis). Retrieved from ProQuest Dissertations & Theses A&I, 2011. [UMI 1505413] [Google Scholar]
Moreno 2009 {published and unpublished data}
- Moreno MA, Vanderstoep A, Parks MR, Zimmerman FJ, Kurth A, Christakis DA. Reducing at‐risk adolescents' display of risk behavior on a social networking web site: a randomized controlled pilot intervention trial. Archives of Pediatrics and Adolescent Medicine 2009;163(1):35‐41. [PUBMED: 19124701] [DOI] [PubMed] [Google Scholar]
Skinner 1995 {published data only}
- Skinner ER, Slater MD. Family communication patterns, rebelliousness, and adolescent reactions to anti‐drug PSAs. Journal of Drug Education 1995;25(4):343‐55. [PUBMED: 8907405] [DOI] [PubMed] [Google Scholar]
Williams 2005 {published and unpublished data}
- Williams C, Griffin KW, Macaulay AP, West TL, Gronewold E. Efficacy of a drug prevention CD‐ROM intervention for adolescents. Substance Use and Misuse 2005;40(6):869‐78. [PUBMED: 15974146] [DOI] [PubMed] [Google Scholar]
Additional references
Ajzen 1991
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes 1991;50:179‐211. [Google Scholar]
Ashton 2003
- Ashton B. The American Star comes to England. Drug and Alcohol Findings 2003;8:21‐6. [Google Scholar]
Bandura 1977
- Bandura A. Social Learning Theory. New York: General Learning Press , 1977. [Google Scholar]
Battjes 1985
- Battjes RJ. Prevention of adolescent drug abuse. International Journal of the Addictions 1985;20(6‐7):1113‐34. [PUBMED: 2416701] [DOI] [PubMed] [Google Scholar]
Berberian 1976
- Berberian RM, Gross C, Lovejoy J, Paparella S. The effectiveness of drug education programs: a critical review. Health Education Monographs 1976;4(4):377‐98. [PUBMED: 1010754] [DOI] [PubMed] [Google Scholar]
Berkowitz 2004
- Berkowitz A. The Social Norms Approach: Theory, Research, and Annotated Bibliography. http://www.alanberkowitz.com/articles/social_norms.pdf 2004.
Brinn 2010
- Brinn MP, Carson KV, Esterman AJ, Chang AB, Smith BJ, Sowden AJ. Mass media interventions for preventing smoking in young people. Cochrane Database of Systematic Reviews 2010, Issue 11. [DOI: 10.1002/14651858.CD001006.pub2] [DOI] [PubMed] [Google Scholar]
Bühler 2006
- Bühler A, Kröger C. Expertise zur Prävention des Substanzmissbrauchs (Forschung und Praxis der Gesundheitsförderung Band 29). Köln: Bundeszentralefür gesundheitliche Aufklärung BZgA, 2006. [Google Scholar]
Camí 2003
- Camí J, Farré M. Drug addiction. New England Journal of Medicine 2003;348(10):975‐86. [DOI: 10.1056/NEJMra023160] [DOI] [PubMed] [Google Scholar]
Crano 2001
- Crano WD, Burgoon M, Oskamp S. Mass Media and Drug Prevention: Classic and Contemporary Theories and Research. Mahwah, New Jersey: Lawrence Erlbaum Associates, 2001. [Google Scholar]
EMCDDA 2009
- European Monitoring Centre for Drugs and Drug Addiction. 2009 Annual Report on the State of the Drugs Problem in Europe. Publications Office of the European Union, November 2009. [Google Scholar]
EMCDDA 2010
- European Monitoring Centre for Drugs and Drug Addiction. The State of the Drugs Problem in Europe. Luxembourg: Publications Office of the European Union, 2010. [DOI: 10.2810/33349; 978‐92‐9168‐432‐8] [DOI] [Google Scholar]
ESPAD 2011
- Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi A, et al. The 2011 ESPAD Report ‐ Substance Use Among Students in 36 European Countries. Stockholm: Swedish Council for Information on Alcohol and other Drugs, European Monitoring Centre for Drugs and Drug Addiction, 2012. [Google Scholar]
Faggiano 2008
- Faggiano F, Vigna‐Taglianti FD, Versino E, Zambon A, Borraccino A, Lemma P. School‐based prevention for illicit drugs use: a systematic review. Preventive Medicine 2008;46(5):385‐96. [PUBMED: 18258289] [DOI] [PubMed] [Google Scholar]
Flay 1983
- Flay BR, Sobel JL. The role of mass media in preventing adolescent substance abuse. Preventing Adolescent Drug Abuse Intervention Strategies. NIDA Research Monograph 47, 1983. [PubMed] [Google Scholar]
Gilmour 2006
- Gilmour S, Degenhardt L, Hall W, Day C. Using intervention time series analyses to assess the effects of imperfectly identifiable natural events: a general method and example. BMC Medical Research Methodology 2006;6:16. [PUBMED: 16579864] [DOI] [PMC free article] [PubMed] [Google Scholar]
Glanz 2002
- Glanz K, Rimer BK, Lewis FM. Health Behavior and Health Education. Theory, Research and Practice. San Francisco: Wiley & Sons, 2002. [Google Scholar]
Hailey 2008
- Hailey D, Roine R, Ohinmaa A. The effectiveness of telemental health applications: a review. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie 2008;53(11):769‐78. [PUBMED: 19087471] [DOI] [PubMed] [Google Scholar]
Hawks 2002
- Hawks D. A Selected Review of What Works in the Area of Prevention. World Health Organization, 2002. [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org 2011.
Hornik 2008
- Hornik R, Jacobsohn L. The best laid plans: disappointments of the National Youth Anti‐Drug Media Campaign. Leonard Davis Institute Issue Brief 2008;14(2):1‐4. [PubMed] [Google Scholar]
Kumpfer 2008
- Kumpfer KL, Smith P, Summerhays JF. A wakeup call to the prevention field: are prevention programs for substance use effective for girls?. Substance Use and Misuse 2008;43(8‐9):978‐1001. [PUBMED: 18649225] [DOI] [PubMed] [Google Scholar]
Leshner 1997
- Leshner AI. Drug abuse and addiction treatment research: the next generation. Archives of General Psychiatry 1997;54:691‐4. [DOI: 10.1001/archpsyc.1997.01830200015002] [DOI] [PubMed] [Google Scholar]
Leshner 1999
- Leshner AI. Science‐based views of drug addiction and its treatment. JAMA 1999;282(14):1314‐6. [DOI: 10.1001/jama.282.14.1314] [DOI] [PubMed] [Google Scholar]
Litchfield 2006
- Litchfield RA, White KM. Young adults' willingness and intentions to use amphetamines: An application of the theory of reasoned action. E‐Journal of Applied Psychology 2006;2(1):1‐9. [Google Scholar]
McGrath 2006
- McGrath Y, Sumnall H, McVeigh J, Bellis M. Drug Use Prevention Among Young People: A Review Of Reviews. Evidence Briefing Update. Health Development Agency (HDA), 2006. [Google Scholar]
McLelland 2000
- McLelland T, Lewis DC, O'Brien CP, Kleber HD. Drug dependence, a chronic medical disease: Implications for treatment, insurance and outcome evaluation. JAMA 2000;284:1689‐95. [PUBMED: 11015800] [DOI] [PubMed] [Google Scholar]
Moskowitz 1983
- Moskowitz JM. Preventing adolescent substance abuse through drug education. Preventing Adolescent Drug Abuse Intervention Strategies. NIDA Research Monograph 47, 1983. [PubMed] [Google Scholar]
NCI 2008
- National Cancer Institute. The Role of the Media in Promoting and Reducing Tobacco Use. Vol. 19, Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute, 2008. [NIH Pub. No. 07‐6242] [Google Scholar]
Nestler 1997
- Nestler EJ, Aghajanian GK. Molecular and cellular basis of addiction. Science 1997;278:58‐63. [DOI: 10.1126/science.278.5335.58] [DOI] [PubMed] [Google Scholar]
Olds 2005
- Olds RS, Thombs DL, Tomasek JR. Relations between normative beliefs and initiation intentions toward cigarette, alcohol and marijuana. Journal of Adolescent Health 2005;37(1):75. [PUBMED: 15963910] [DOI] [PubMed] [Google Scholar]
Perkins 1986
- Perkins HW, Berkowitz AD. Perceiving the community norms of alcohol use among students: some research implications for campus alcohol education programming. International Journal of the Addictions 1986;21(9‐10):961‐76. [DOI] [PubMed] [Google Scholar]
Redman 1990
- Redman S, Spencer EA, Sanson‐Fisher RW. The role of mass media in changing health‐related behaviour: a critical appraisal of two models. Health Promotion International 1990;5:85‐101. [DOI: 10.1093/heapro/5.1.85] [DOI] [Google Scholar]
Review Manager 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Romer 1994
- Romer D. Using mass media to reduce adolescent involvement in drug trafficking. Pediatrics 1994;93(6 Pt 2):1073‐7. [PUBMED: 8197010] [PubMed] [Google Scholar]
Romer 1995
- Romer D, Kim S. Health interventions for African American and Latino youth: the potential role of mass media. Health Education Quarterly 1995;22(2):172‐89. [PUBMED: 7622386] [DOI] [PubMed] [Google Scholar]
Rossi 2003
- Rossi PH, Freeman HE. Evaluation: A Systematic Approach. 7th Edition. Newbury Park: Sage Publications, Inc, 2003. [Google Scholar]
Schilling 1990
- Schilling RF, McAlister AL. Preventing drug use in adolescents through media interventions. Journal of Consulting and Clinical Psychology 1990;58(4):416‐24. [PUBMED: 2212178] [DOI] [PubMed] [Google Scholar]
Stephenson 2003b
- Stephenson MT. Mass media strategies targeting high sensation seekers: what works and why. American Journal of Health Behavior 2003;27 Suppl 3:S233‐8. [PUBMED: 14672384] [DOI] [PubMed] [Google Scholar]
Strasburger 2008
- Strasburger VC, Wilson BJ, Jordan AB. Children, Adolescents, and the Media. 2nd Edition. Sage Publications, 2008. [Google Scholar]
Sumnall 2007
- Sumnall HR, Bellis MA. Can health campaigns make people ill? The iatrogenic potential of population‐based cannabis prevention. Journal of Epidemiology and Community Health 2007;61(11):930‐1. [DOI: 10.1136/jech.2007.060277] [DOI] [PMC free article] [PubMed] [Google Scholar]
Swendsen 2009
- Swendsen J, Conway KP, Degenhardt L, Dierker L, Glantz M, Jin R, et al. Socio‐demographic risk factors for alcohol and drug dependence: the 10‐year follow‐up of the national comorbidity survey. Addiction 2009;104(8):1346‐55. [DOI: 10.1111/j.1360-0443.2009.02622.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
UNODC 2012
- UNODC. World Drug Report 2012. E.12.XI.1. Vienna: United Nations, 2012. [Google Scholar]
Wakefield 2010
- Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet 2010;376:1261‐71. [DOI: 10.1016/S0140-6736(10)60809-4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wammes 2007
- Wammes A, Van Leeuwen, Lokman S. Evaluatierapport DVP‐Campagne 2006 'Je bent niet gek als jeniet blowt'. Utrecht: Trimbos Institute, 2007. [Google Scholar]
Werb 2011
- Werb D, Mills EJ, Debeck K, Kerr T, Montaner JS, Wood E. The effectiveness of anti‐illicit‐drug public‐service announcements: a systematic review and meta‐analysis. Journal of Epidemiology and Community Health 2011;65(10):834‐40. [PUBMED: 21558482] [DOI] [PubMed] [Google Scholar]
Wise 1998
- Wise RA. Drug‐activation of brain reward pathways. Drug and Alcohol Dependence 1998;51:13‐22. [DOI] [PubMed] [Google Scholar]