

Abstract
Abstract
Objectives
We aimed to examine the characteristics, features and content of suicide prevention mobile apps available in app stores in Canada and the UK.
Design
Suicide prevention apps were identified from Apple and Android app stores between March and April 2023. Apps were screened against predefined inclusion criteria, and duplicate apps were removed. Data were then extracted based on descriptive (eg, genre, app developer), security (eg, password protection) and design features (eg, personalisation options). Content of apps was assessed using the Essential Features Framework. Extracted data were analysed using a content analysis approach including narrative frequencies and descriptive statistics.
Data sources
Apple and Android app stores between March and April 2023.
Eligibility criteria
Identified apps were eligible for inclusion if they were: (a) free, (b) developed in the English language, (c) could be downloaded on an Apple or Android device in England or Canada, (d) the focus of the app was suicide prevention and (e) the target users of the app were individuals experiencing suicide-related thoughts and/or behaviours.
Data extraction and synthesis
Apps were assessed on basic descriptive data (eg, name, genre, developer of the app), alongside security (eg, whether password protection was available) and design features (eg, whether the app could be personalised). App content was examined using the Essential Features Framework.
Results
52 suicide prevention apps were included within the review. Most were tailored for the general population and were in English language only. One app had the option to increase app accessibility by offering content presented using sign language. Many apps allowed some form of personalisation by adding text content, however most did not facilitate further customisation such as the ability to upload photo and audio content. All identified apps included content from at least one of the domains of the Essential Features Framework. The most commonly included domains were sources of suicide prevention support, and information about suicide. The domain least frequently included was screening tools followed by wellness content. No identified apps had the ability to be linked to patient medical records.
Conclusions
The findings of this research present implications for the development of future suicide prevention apps. Development of a co-produced suicide prevention app which is accessible, allows for personalisation and can be integrated into clinical care may present an opportunity to enhance suicide prevention support for individuals experiencing suicidal thoughts and behaviours.
Keywords: MENTAL HEALTH, Suicide & self-harm, Digital Technology, PSYCHIATRY, Health informatics
STRENGTHS AND LIMITATIONS OF THIS STUDY.
This app review used an established method for systematically identifying and examining suicide prevention apps, which has been successfully used previously.
Only free apps available in the UK and Canada in the English language were identified using limited search terms. Current provision and content of suicide prevention apps may differ across countries (including those available in lower- and middle-income countries) alongside apps which require payment.
Due to resource and time constraints, the quality of apps and underpinning theoretical frameworks were not assessed.
The study also excludes apps that were designed solely for use by healthcare providers as such this may limit the conclusions such as integration with mental health services.
The authors encountered a high variability in app availability, this may lead to difficulties in reproducibility but does highlight a continually changing app market.
Introduction
Suicide is a global public health problem, where over 700 000 people die by suicide each year.1 Suicide and self-harm are disproportionately prevalent among certain groups of individuals, including but not limited to individuals experiencing mental health conditions,2 middle-aged men,3 adolescents4 and LGBTQIA+ populations.5 6
Despite the high demand for suicide prevention resources, many individuals with suicidal thoughts or behaviours face barriers to receiving care. Individuals attempting to access primary or secondary mental health services may experience long waiting lists for treatment, inconsistent intervention provision across regions, and perceived or actual stigma associated with accessing care.7 Additionally, individuals presenting to emergency departments following self-harm or a suicide attempt may face further barriers to appropriate care including a lack of time and space for a full psychosocial assessment, and inadequate staff training in mental healthcare.8 Finally, worldwide, healthcare providers are experiencing staffing shortages, with projections of a potential 18 million person shortfall of health workers by 2030, with low- and middle-income countries most affected.9 As a result of these issues, there is a need to consider modes to supplement suicide prevention care.
Mobile apps may offer a novel adjunct to suicide prevention interventions delivered by health, social care or voluntary service practitioners. Mobile device use is common in the general population. As of 2022, estimates suggest 86% of people in the UK, and 84% of people in Canada own a smartphone, with levels expected to increase in the coming years.10 App based resources may assist in mitigating the detrimental impacts of staffing shortages, waitlists for treatment and social distancing measures.11 12 Furthermore, benefits for users may include anonymity, cost-effectiveness and the ability to use interventions at the user’s own pace.13 Several reviews have examined the potential efficacy of digital interventions for self-harm and suicide prevention. Several reviews have shown that digital interventions targeted for suicide prevention may reduce suicide ideation, however, it is currently unclear as to whether this effect translates into reductions in self-harm or suicide.713,15 Furthermore, reviews have highlighted the need for further research specifically evaluating the efficacy of mobile interventions such as apps, especially given the ready availability of these to the general public.14 16 Alongside efficacy, one review also examined acceptability and feasibility, finding interventions were largely viewed as acceptable by users, however usage appears to drop over time.7
Despite several advantages in the introduction of digital technology such as apps to supplement care, such solutions also introduce multiple challenges. These may include varied adherence to clinical guidelines, technical issues, privacy and security concerns, lower engagement levels, lack of personalisation, implementation challenges and the absence of a therapeutic relationship.17 Furthermore, digital solutions may contribute to pre-existing health inequalities as a result of the ‘digital divide’,18 with groups such as older adults, individuals with disabilities, rural and indigenous populations, individuals with low income, or lower levels of education disproportionately affected.19 20
In addition to broader challenges of digital care, problems with suicide prevention apps currently available have been identified. Reviews of apps available in the USA and Australia have found a lack of adherence to clinical guidelines regarding provision of evidence-based support. For example, apps have been found to lack content such as psychoeducation, safety plans and access to support networks or emergency/crisis support.21,23 Furthermore, app availability has been shown to be unpredictable, with apps regularly becoming unavailable and search results for relevant apps being highly variable on date of searching.24 In order to develop a novel suicide prevention app, there is a need to understand what is currently available to users, in this case for an app tailored for a UK and Canadian audience.
In recent years efforts have been made to design tools to allow systematic assessment of suicide prevention apps. One such tool is the Essential Features Framework25 which aims to facilitate analysis of apps based on content, features and design. Importantly the framework was not developed to allow users to assess the quality of an app, rather the aim is to systematically categorise app content. The framework was developed using a systematic review of articles examining development, implementation, feasibility or effectiveness of suicide prevention apps, where features of apps included were synthesised using thematic analysis. The framework is comprised of eight domains (a) general information regarding suicide; (b) wellness; (c) positivity and inspiration; (d) distraction and alternate activities; (e) safety planning; (f) screening tools; (g) helpful resources; and (h) immediate help-seeking. Definitions of each framework domain and examples of eligible features are presented in table 1. No published studies have yet used this framework to assess the content of suicide prevention apps.
Table 1. Essential Features Framework25.
| Definition and example features | |
| General information about suicide | |
| Information about suicide including risk factors and warning signs, dispelling myths about suicide and information regarding how to support someone who is suicidal | |
| Wellness | |
| Tools to promote well-being such as mindfulness and relaxation exercises | |
| Positivity and inspiration | |
| Content such as inspirational messages, quotes from individuals with lived experience and suggested reasons for living | |
| Distraction and alternate activities | |
| Tools and suggestions to support users such as coping strategies and distraction activities | |
| Safety planning | |
| A tool to help someone cope with suicidal thoughts, or to support someone who experiences suicidal thoughts. Includes ways to recognise when someone may be nearing a crisis, coping strategies to use, and useful sources of support to contact (eg, family, friends, clinicians, helplines)37 | |
| Screening tools | |
| Tools used for identifying and monitoring mood, screening for psychological distress or ‘suicide risk’ | |
| Helpful resources (for help-seeking) | |
| Information and contact details for suicide prevention helplines, mental health services and emergency departments | |
| Immediate help-seeking | |
| Fast access to immediate help such as links to suicide helplines and emergency services on the app homepage | |
Objectives
We aimed to use the Essential Features Framework to review the characteristics and content of suicide prevention apps available within the UK and Canada to inform the development of an evidence-based suicide prevention app to be made available in these countries.
Methods
App store search
Development of search terms followed previous research.21 26 The search terms used were “Suicide Prevention”, “Suicide” and “Safety Plan” and no restrictions were imposed related to store subcategories. Searches of the ‘Apple App Store’ and ‘Google Play’ in the UK and Canada were conducted from 3 March to 12 April 2023. The UK app search was conducted by SG (using a Google Pixel 6a) and LB-P (using an iPhone 12 mini, iOS V.16.1.1). HDS (using an iPhone 11 Pro, iOS V.15.6.1) and JK (using an iPhone 11, iOS V.16.4.1) conducted the Canadian app search.
Selection criteria
Identified apps were eligible for inclusion if they were: (a) free, (b) developed in the English language, (c) could be downloaded on an Apple or Android device in England or Canada, (d) the focus of the app was suicide prevention and (e) the target users of the app were individuals experiencing suicide-related thoughts and/or behaviours. Apps tailored for individuals supporting someone with suicidal thoughts were also included, but only if they had suicide prevention resources such as the ability to call for emergency support for someone experiencing suicidal thoughts themselves. Similarly, general mental health apps or apps developed for a specific mental health condition were included if the app contained a suicide prevention resource such as a suicide safety plan. We excluded apps solely designed for healthcare providers.
Apps were initially screened independently for eligibility based on the app title and description visible on the app store page (LB-P, SG, JK, HDS). Potentially eligible apps were then downloaded and the full content of apps screened against the eligibility criteria (LB-P, SG, JK). Duplicate apps (eg, if an app was identified by both UK and Canadian searches) were manually removed.
Data extraction
SG, LB-P and JK extracted data. A template data extraction form is shown in online supplemental file 1. Briefly, basic descriptive data were extracted (eg, name, genre, developer of the app), alongside security (eg, whether password protection available) and design (eg, whether the app could be personalised) features. App content was examined using the Essential Features Framework.25 The framework was developed as method to categorise the content of suicide prevention apps rather than assess quality of apps. Data extraction was performed by one researcher (this was a specific person dependent on app location and Apple or Android availability) and was then independently checked by a second reviewer. Any conflicts during this process were discussed, including consultation with other members of the research team until consensus was reached. Quality of apps was not assessed.
Analysis
Content analysis was used as this method has been previously used to analyse suicide prevention apps.23 A coding framework was developed using the Essential Features Framework, alongside content of preliminary discussions held during co-production workshops regarding perceived important features of suicide prevention apps. These workshops gained the perspectives of service users, informal carers and clinicians. Extracted data were synthesised using narrative descriptions of app features, alongside frequencies and percentages of app characteristics (data analysis performed by LB-P and SG).
Results
Search results
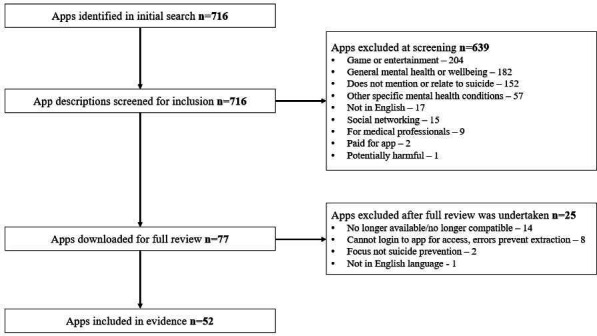
Following de-duplication 716 apps were identified by searches. After title and description screening, 77 apps remained, and following full app assessment, 52 apps were included within the review (see figure 1 for the Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for screening process and online supplemental file 2 for a list of included and excluded apps alongside reasons for exclusion). Search results were highly variable on day of searching, with a further number of apps (n=14) becoming unavailable during data extraction. During extraction, the authors encountered malfunctions and errors in multiple apps (20, 38.5%), ranging from apps freezing during use, to erroneous links to outside resources and helplines.
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram of app screening, review and inclusion in evidence.
Basic app characteristics
Included apps were mostly developed in the USA (32/52, 61.5%), with apps also developed in Australia (7/52, 13.5%), Canada (6/52, 11.5%), the UK (6/52, 11.5%) and Zimbabwe (1/52, 1.9%). Most were available in English only (45/52, 86.5%), and only one app had an accessibility feature (1/52, 1.9%), in this case by including content presented in British Sign Language. User ratings were available for some apps (15/52, 28.8%) with an average rating of 4.3 out of 5.0, among apps showing ratings. Data were available on Android apps regarding the number of downloads (N=41/52, 78.8%). The two most popular apps had been downloaded over 100 000 times. Android apps also stated the date of the most recent app update. Some apps (16/41, 39.0%) had not been updated in over 3 years. See table 2 for basic characteristics of included apps.
Table 2. Basic characteristics of included apps.
| Characteristic category | Number (%) of apps meeting criteria | |
| Country of development | ||
| USA | 32 (61.5%) | |
| Australia | 7 (13.5%) | |
| Canada | 6 (11.5%) | |
| UK | 6 (11.5%) | |
| Zimbabwe | 1 (1.9%) | |
| Target audience of app | ||
| General population | 31 (59.6%) | |
| Military staff | 12 (23.1%) | |
| University students | 6 (11.5%) | |
| Individuals supporting suicidal person | 3 (5.8%) | |
| App store category* | ||
| Health and fitness | 26 (50.0%) | |
| Education | 15 (28.8%) | |
| Medical | 5 (9.6%) | |
| Books and references | 3 (5.8%) | |
| Lifestyle | 3 (5.8%) | |
| Most recent app update†‡ | ||
| Less than 1 year | 18 (43.9%) | |
| 1–2 years | 3 (7.3%) | |
| 2 years and 1 day to 3 years | 4 (9.8%) | |
| Over 3 years | 16 (39.0%) | |
| Content available in multiple languages | ||
| Yes | 7 (13.5%) | |
| No | 45 (86.5%) | |
| Accessibility options within app | ||
| Yes | 1 (1.9%) | |
| No | 51 (98.1%) | |
| User guide within app | ||
| Yes | 9 (17.3%) | |
| No | 43 (82.7%) | |
Some apps were categorizedcategorised differently in Android and Apple app stores.
Data available only for apps Android apps (denominator N=41).
As of review date of August 2023.
The majority of apps were tailored for the general population (31/52, 59.6%), with some of these specifically designed for young people (4/31, 12.9%). Additional apps were tailored to staff at military bases or veterans (12/52, 23.1%), students at specific universities (6/52, 11.5%) and individuals who are supporting, or are concerned about someone who may be suicidal (3/52, 5.8%). Despite the majority of apps being tailored specifically for users experiencing suicidal thoughts (by necessity of inclusion criteria), almost three-quarters of apps also contained content for those concerned about a person who may be suicidal (38/52, 73.1%). For example, some apps provided advice on what to say or avoid saying if someone shares that they are thinking about suicide, potential warning signs that a person may be suicidal, and suggestions of potential methods of support. Although some apps gave the user space to enter the contact details of clinicians for future reference, no apps had the ability to share content entered into an app with a clinician. For example, sharing safety plans with clinical teams or medical records.
Privacy
When searching the app store, over half of included apps displayed their privacy policy on the app’s product page (34/52, 65.4%). However, far fewer had their privacy policy integrated into the app itself (19/52, 36.5%), and in some of these, the policy did not load. Nearly a third of apps had no policy available on either the app or product page (15/52, 28.8%). A small number of apps asked users to agree to a set of terms and conditions before using the app, including information about privacy, and limits of the app (9/52, 17.3%). Only two apps allowed users to create a password protected account, however one of these apps required users to pay for an upgrade to use this feature (2/52, 3.8%).
Design
Many apps included some form of personalisation options, with over half prompting users to add text which could be saved and referred back to at later times (30/52, 57.7%). For example, allowing users to enter and save the contact details of support sources. Fewer had the ability for users to upload their own media content, such as photos, music or voice notes (6/52, 11.5%). Only two (2/52, 3.8%) apps allowed the user to personalise app appearance, for example, choosing background colours. However, one of these required the user to pay for an upgrade, and the other malfunctioned when reviewers attempted to use the feature. While most apps contained only text content, around a quarter contained multimedia content such as videos and audio-recordings (14/52, 26.9%). A few apps offered notifications to the user (11/52, 21.2%), for example, reminders to complete mood monitoring or update safety plans.
App content
When assessed against the Essential Features Framework, only two (2/52, 3.8%) apps included content from all domains. Almost three-quarters of apps contained four or more domains (37/52, 71.2%). The domain covered by most apps was helpful resources for help-seeking where every app included at least one suggestion of a source of support (52/52, 100.0%), followed by both immediate sources of help-seeking (47/52, 90.4%) and general information about suicide (47/52, 90.4%), positivity and inspiration (33/52, 63.5%), distraction and alternate activities (22/52, 42.3%), safety planning resources (20/52, 38.5%) and wellness content (11/52, 21.2%). The domain covered by the least apps was screening tools (9/52, 17.3%). In the following section app content related to each domain of the Essential Features Framework is discussed in detail. The denominators used within these sections reflect the number of apps covering the domain.
General information about suicide (covered by 47/52, 90.4% of apps)
Most apps included information related to suicide for the user (47/52, 90.4%). Almost all of these apps included information on warning signs that a suicidal crisis may occur (43/47, 91.5%). Nearly half also covered risk factors related to suicide (23/47, 48.9%), with fewer providing information about mental health generally (10/47, 21.3%) or health behaviours such as information about diet, sleep and exercise (14/47, 29.8%). Over a third of apps contained information related to suicide among marginalised groups (16/47, 34.0%), for example, statistics regarding the risk of attempting suicide among LGBTQIA+ groups. Over three-quarters contained information tailored for individuals concerned or supporting someone who may be suicidal (37/47, 78.7%), with a few of these providing information about bereavement through suicide (6/47, 12.8%).
Wellness (covered by 11/52, 21.2% of apps)
Few apps contained content related to wellness (11/52, 21.2%). Of those, most related to relaxation techniques such as breathing and grounding exercises (10/11, 90.9%), and almost half had mindfulness and meditation resources (5/11, 45.5%). Some of these apps also had space for users to keep a journal or diary (4/11, 36.4%).
Positivity and inspiration (covered by 33/52, 63.5% of apps)
Over half of apps included content related to positivity and inspiration (33/52, 63.5%). Most of these included inspirational messaging (30/33, 90.9%) such as encouraging individuals to seek help, reminding users they are not alone and messages surrounding hope for the future. Some encouraged users to save their reasons for living, usually within a safety plan (13/33, 39.4%). A minority included inspirational quotes from individuals with lived experience (4/33, 12.1%), including individuals who had experienced suicidal thoughts or attempts, or individuals who had supported a person with these experiences.
Distraction and alternate activities (covered by 22/52, 42.3% of apps)
Almost half of apps contained content aimed to distract users from suicidal thoughts, or provide alternate activities for users (22/52, 42.3%). All of these included suggestions of coping strategies, including suggestions for places or activities aimed at distraction (14/22, 63.6%). Most of this information was presented within safety planning tools.
Safety planning (covered by 20/52, 38.5% of apps)
Multiple apps allowed users to construct a customisable safety plan (20/52, 38.5%). There was variation in the content of safety plans between apps, however all but one app prompted users to enter the details of trusted contacts in case of crisis (19/20, 95.0%). Some plans requested users to reflect on potential means of suicide method, and how to protect themselves from these when in crisis. However, concerningly some of these apps listed potential means of suicide in this section demonstrating potentially harmful content. Few of the apps containing safety plans allowed the safety plan to be directly shared from the app to another person (6/20, 30.0%).
Monitoring and screening tools (covered by 9/52, 17.3% of apps)
Screening tools were the least common feature among included apps (9/52, 17.3%). Among those containing such tools, most involved screening for suicide risk or mental distress (8/9, 88.9%). Examples of screening tools included the Patient Health Questionnaire (PHQ-9),27 Kessler Psychological Distress Scale (K10)28 and the Columbia-Suicide Severity Rating Scale (C-SSRS).29 Only five tools allowed users to monitor their mood, for example, using a tracker (5/9, 55.6%).
Helpful resources (for help-seeking) (covered by 52/52, 100% of apps)
All apps included helpful resources of help-seeking. This included the contact details of suicide prevention phone lines (49/52, 94.2%) and emergency or mental health services (48/52, 92.3%). Many also allowed users to save the contact details of trusted support sources (30/52, 57.7%). This was usually but not always presented within a safety plan. Almost three-quarters of apps contained support sources tailored for marginalised groups, or groups who may be at increased risk of suicidal behaviours such as LGBTQIA+ individuals and veterans (38/52, 73.1%). Some apps allowed sources of support to be personalised by user location (11/52, 21.2%), for example, displaying a map with local hospitals and crisis centres.
Immediate resources (covered by 47/52, 90.4% of apps)
Most apps gave users access to immediate resources (47/52, 90.4%). Some of these apps had links to emergency support embedded within the app homepage (25/47, 53.2%), most commonly the link to emergency medical support (eg, 999 in UK, 911 in Canada) or a suicide prevention phone line.
Discussion
We analysed the characteristics and content of 52 suicide prevention apps available in the UK and Canada. All apps included at least one type of suicide prevention content as categorised by the Essential Features Framework, most commonly sources of support and information about suicide. The content of apps varied greatly, with the least common content including mood monitoring tools. During the review, the authors experienced multiple issues identifying apps.
Availability of suicide prevention apps was highly transient throughout, with many becoming unavailable during the study process. The instability of healthcare apps has been frequently demonstrated.24 30 31 Specific to suicide prevention apps, in one study, 50% of available suicide prevention apps had changed within 115 days of conducting initial searches.32 Also, when conducting searches, many apps were far down the app store search results, therefore lacking visibility to potential users. Difficulty finding relevant apps is a longstanding problem for app users.33 App developers should consider how individuals may search for their app and ensure that an app’s name, description or category includes explicit mention of terms such as mental health, suicide, safety planning and other commonly used search terms. This will ensure intended users are able to easily find relevant apps most suitable to their current needs. Without consideration for how users search for and select mobile apps for suicide prevention, app developers risk poor uptake and retention of digital interventions.34
Similar to previous reviews of suicide prevention apps,22 a significant proportion of apps had not been recently updated or had malfunctioning content. In the context of suicide prevention this may have dangerous implications, for example, if a signposted support organisation has since closed. Apps targeted at mental health and suicide prevention may benefit from a review by an independent regulator to ensure safe content,22 alongside app developers having a standardised process to ensure app content is regularly updated. A significant number of apps lacked a clear privacy statement. Lack of data privacy, and ‘clunky’ apps have been identified as barriers to use of mental health apps by mental health professionals integrating mobile technology into mental health services35 and users of such apps.36
All of the included apps contained at least one type of suicide prevention tool. However, there was a distinct lack in some types of content, some of which have growing evidence base related to effective and acceptable support surrounding suicide prevention. For example, safety plans.37,39 Additionally, similar to previous reviews of mental health apps, many lacked accessibility40 or personalisation options, which previous research suggests are important facilitators of app use alongside promoting inclusivity in access.41 42 Few apps used notifications, which may contribute to poor user retention and engagement. Indeed, a previous systematic review noted a decline in app engagement over time.7 Notifications have been shown to increase user engagement in apps,43 44 but users of mental health apps have been shown to have mixed opinions as to their appropriateness. For example, notifications may appear as intrusive, reduce the level of privacy due to visibility on a user’s screen, or remind users of the difficulties they are facing.45 The considerations mentioned above provide evidence for the importance of prioritising co-production with the intended user group during app development to ensure content meets the preferences and values of users. Important considerations are included in the app evaluation model developed by the American Psychiatric Association. This model reiterates the importance of the accessibility, privacy and security, clinical foundation, usability, and data integration towards therapeutic goals for all mental health apps.46
No apps identified for this study were designed for integration with mental health services, nor were they connected to any electronic health record system. Embedding apps into clinical practice may present several benefits for service users and staff. This may include the ability for clinicians to collect daily mood monitoring data, patients being able to complete ‘between-session’ activities, and the potential for integration of wearable devices to gather clinical data such as sleep and activity tracking.47 A scoping review has examined the literature on information and communication technology-based suicide prevention interventions (including apps) that have been implemented in clinical settings.48 The reviewers excluded apps available in app stores if they were not implemented in clinical settings and identified 10 suicide prevention apps which were implemented in multiple clinical settings (eg, inpatient, outpatient and community), and groups of patients (eg, adults, children and young adults). Several barriers were identified as hindering integration such as lack of skills to use technology, unstable internet connection and lack of buy-in. These challenges are not unique to technologies for suicide prevention or mental health; many other mobile health interventions face challenges with adoption and can be abandoned soon after initiating use.7 49 As such, the significance of implementation efforts cannot be underestimated. These efforts involve analysing the barriers and facilitators for the successful integration of suicide prevention app-based interventions into routine clinical practice and developing targeted approaches to address these barriers while leveraging facilitators.48
Strengths and limitations
This research benefitted from the use of a novel framework to assist categorisation of suicide prevention app content25 During this study, we have been able to identify considerations for further development of the framework. For example, assessment of whether content is evidence-based, and whether app content has a theoretical underpinning (eg, CBT). This may be particularly important given a recent trial showed that a digital brief Dialectical Behaviour Therapy Skills Training programme significantly increased risk of self-harm among adult outpatients compared with usual care.50 Considerations should also be acknowledged related to the limited search terms, eligibility criteria and timeframe of the present study. Paid-for apps, apps not available in Canada and the UK, and apps for only healthcare providers were not included, therefore limiting search results. It is well documented that on the date of searching application availability can greatly vary. Therefore, the present results are solely representative of the apps identified within the study period.
Conclusions
This article has analysed the content and features of suicide prevention apps available in UK and Canada. Although all apps contained some form of suicide prevention tools, specific content included varied greatly, and many lacked personalisation and accessibility options. The findings suggest implications for future evidence-based suicide prevention app development. There is the potential for apps to be used as an adjunct to clinical care, however a cautious approach must be taken if apps link to clinical notes and/or electronic health records, and apps should not be considered as an alternative to provision of therapeutic interventions with appropriately trained staff. The development of future suicide preventions apps provides an opportunity for authentic co-production with both service users and staff, and a novel way to evaluate data in real time.
supplementary material
Footnotes
Funding: This research received support from the Centre for Addiction and Mental Health (CAMH) and Oxford Health NHS Foundation Trust (OHFT).
Prepublication history and additional supplemental material for this paper are available online. To view these files, please visit the journal online (https://doi.org/10.1136/bmjopen-2024-087468).
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Not applicable.
Ethics approval: Ethical approval was not required for this study as it did not involve human participants or their data.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Data availability statement
Data are available upon reasonable request.
References
- 1.World Health Organization Suicide. 2021. https://www.who.int/news- room/fact-sheets/detail/suicide Available.
- 2.Yeh HH, Westphal J, Hu Y, et al. Diagnosed Mental Health Conditions and Risk of Suicide Mortality. Psychiatr Serv. 2019;70:750–7. doi: 10.1176/appi.ps.201800346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.The University of Manchester The National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH). Suicide by middle-aged men. 2021. https://documents.manchester.ac.uk/display.aspx?DocID=55305 Available.
- 4.Glenn CR, Kleiman EM, Kellerman J, et al. Annual Research Review: A meta-analytic review of worldwide suicide rates in adolescents. J Child Psychol Psychiatry. 2020;61:294–308. doi: 10.1111/jcpp.13106. [DOI] [PubMed] [Google Scholar]
- 5.Miranda-Mendizábal A, Castellví P, Parés-Badell O, et al. Sexual orientation and suicidal behaviour in adolescents and young adults: systematic review and meta-analysis. Br J Psychiatry. 2017;211:77–87. doi: 10.1192/bjp.bp.116.196345. [DOI] [PubMed] [Google Scholar]
- 6.Kidd G, Marston L, Nazareth I, et al. Suicidal thoughts, suicide attempt and non-suicidal self-harm amongst lesbian, gay and bisexual adults compared with heterosexual adults: analysis of data from two nationally representative English household surveys. Soc Psychiatry Psychiatr Epidemiol. 2024;59:273–83. doi: 10.1007/s00127-023-02490-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Arshad U, Farhat-Ul-Ain. Gauntlett J, et al. A Systematic Review of the Evidence Supporting Mobile- and Internet-Based Psychological Interventions For Self-Harm. Suicide Life Threat Behav. 2020;50:151–79. doi: 10.1111/sltb.12583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Richards H, Rajaram G, Lamblin M, et al. Staff perceptions of barriers to self-harm care in the emergency department: A cross-sectional survey study. Aust Emerg Care. 2024;27:15–20. doi: 10.1016/j.auec.2023.07.002. [DOI] [PubMed] [Google Scholar]
- 9.WHO Working for health and growth: investing in the health workforce - High-Level Commission on Health Employment and Economic Growth. 2016. https://www.who.int/publications/i/item/9789241511308 Available.
- 10.Wike R, Silver L, Fetterolf J, et al. Internet, smartphone and social media use. 2022. https://www.pewresearch.org/global/2022/12/06/internet-smartphone-and-social-media-use-in-advanced-economies-2022/ Available.
- 11.Leigh S, Flatt S. App-based psychological interventions: friend or foe?: Table 1. Evid Based Mental Health . 2015;18:97–9. doi: 10.1136/eb-2015-102203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rauschenberg C, Schick A, Hirjak D, et al. Evidence Synthesis of Digital Interventions to Mitigate the Negative Impact of the COVID-19 Pandemic on Public Mental Health: Rapid Meta-review. J Med Internet Res. 2021;23:e23365. doi: 10.2196/23365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Torok M, Han J, Baker S, et al. Suicide prevention using self-guided digital interventions: a systematic review and meta-analysis of randomised controlled trials. Lancet Dig Health. 2020;2:e25–36. doi: 10.1016/S2589-7500(19)30199-2. [DOI] [PubMed] [Google Scholar]
- 14.Witt K, Spittal MJ, Carter G, et al. Effectiveness of online and mobile telephone applications ('apps’) for the self-management of suicidal ideation and self-harm: a systematic review and meta-analysis. BMC Psychiatry. 2017;17:297. doi: 10.1186/s12888-017-1458-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sutori S, Hadlaczky G, Eliasson E, et al. Systematic Review and Meta-Analysis: Effectiveness of Stand-Alone Digital Suicide Preventive Interventions for the Self-Management of Suicidality. J technol behav sci. 2024;9:440–51. doi: 10.1007/s41347-023-00374-7. [DOI] [Google Scholar]
- 16.Melia R, Francis K, Hickey E, et al. Mobile Health Technology Interventions for Suicide Prevention: Systematic Review. JMIR Mhealth Uhealth. 2020;8:e12516. doi: 10.2196/12516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Giebel GD, Speckemeier C, Abels C, et al. Problems and Barriers Related to the Use of Digital Health Applications: Scoping Review. J Med Internet Res . 2023;25:e43808. doi: 10.2196/43808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.van Dijk JAGM. Digital divide research, achievements and shortcomings. Poetics (Amst) 2006;34:221–35. doi: 10.1016/j.poetic.2006.05.004. [DOI] [Google Scholar]
- 19.Office for National Statistics Exploring the UK’s digital divide, Exploring the UK’s digital divide. 2019. https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/articles/exploringtheuksdigitaldivide/2019-03-04 Available.
- 20.Haight M, Quan-Haase A, Corbett BA. Revisiting the digital divide in Canada: the impact of demographic factors on access to the internet, level of online activity, and social networking site usage. Inf Comm Soc. 2014;17:503–19. doi: 10.1080/1369118X.2014.891633. [DOI] [Google Scholar]
- 21.Larsen ME, Nicholas J, Christensen H. A Systematic Assessment of Smartphone Tools for Suicide Prevention. PLoS One. 2016;11:e0152285. doi: 10.1371/journal.pone.0152285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Martinengo L, Van Galen L, Lum E, et al. Suicide prevention and depression apps’ suicide risk assessment and management: a systematic assessment of adherence to clinical guidelines. BMC Med. 2019;17:231. doi: 10.1186/s12916-019-1461-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wilks CR, Chu C, Sim D, et al. User Engagement and Usability of Suicide Prevention Apps: Systematic Search in App Stores and Content Analysis. JMIR Form Res. 2021;5:e27018. doi: 10.2196/27018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mercurio M, Larsen M, Wisniewski H, et al. Longitudinal trends in the quality, effectiveness and attributes of highly rated smartphone health apps. Evid Based Mental Health . 2020;23:107–11. doi: 10.1136/ebmental-2019-300137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sequeira L, Kassam I, Kemp J, et al. Mobile Apps for Suicide Prevention: Developing an Evidence-Based Framework for Essential Features [Poster Presentation] AMIA. 2022 [Google Scholar]
- 26.Aguirre RTP, McCoy MK, Roan M. Development Guidelines from a Study of Suicide Prevention Mobile Applications (Apps) J Technol Hum Serv. 2013;31:269–93. doi: 10.1080/15228835.2013.814750. [DOI] [Google Scholar]
- 27.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32:959–76. doi: 10.1017/s0033291702006074. [DOI] [PubMed] [Google Scholar]
- 29.Posner K, Brent D, Lucas C, et al. Columbia-Suicide Severity Rating Scale (C-SSRS) New York, NY: Columbia University Medical Center; 2008. [Google Scholar]
- 30.Grau-Corral I, Gascon P, Grajales III FJ, et al. Availability of Spanish-Language Medical Apps in Google Play and the App Store: Retrospective Descriptive Analysis Using Google Tools. JMIR Mhealth Uhealth. 2020;8:e17139. doi: 10.2196/17139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lau N, O’Daffer A, Colt S, et al. Android and iPhone Mobile Apps for Psychosocial Wellness and Stress Management: Systematic Search in App Stores and Literature Review. JMIR Mhealth Uhealth. 2020;8:e17798. doi: 10.2196/17798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Larsen ME, Nicholas J, Christensen H. Quantifying App Store Dynamics: Longitudinal Tracking of Mental Health Apps. JMIR Mhealth Uhealth. 2016;4:e96. doi: 10.2196/mhealth.6020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Park DH, Liu M, Zhai C, et al. Leveraging user reviews to improve accuracy for mobile app retrieval. SIGIR ’15; Santiago Chile. Aug 9, 2015. pp. 33–542. Available. [DOI] [Google Scholar]
- 34.Kaveladze BT, Wasil AR, Bunyi JB, et al. User Experience, Engagement, and Popularity in Mental Health Apps: Secondary Analysis of App Analytics and Expert App Reviews. JMIR Hum Factors . 2022;9:e30766. doi: 10.2196/30766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Melia R, Monahan L, Duggan J, et al. Exploring the experiences of mental health professionals engaged in the adoption of mobile health technology in Irish mental health services. BMC Psychiatry. 2021;21:412. doi: 10.1186/s12888-021-03426-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Borghouts J, Eikey EV, Mark G, et al. Understanding Mental Health App Use Among Community College Students: Web-Based Survey Study. J Med Internet Res. 2021;23:e27745. doi: 10.2196/27745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stanley B, Brown GK. Safety Planning Intervention: A Brief Intervention to Mitigate Suicide Risk. Cogn Behav Pract. 2012;19:256–64. doi: 10.1016/j.cbpra.2011.01.001. [DOI] [Google Scholar]
- 38.Nuij C, van Ballegooijen W, de Beurs D, et al. Safety planning-type interventions for suicide prevention: meta-analysis. Br J Psychiatry. 2021;219:419–26. doi: 10.1192/bjp.2021.50. [DOI] [PubMed] [Google Scholar]
- 39.Ferguson M, Rhodes K, Loughhead M, et al. The Effectiveness of the Safety Planning Intervention for Adults Experiencing Suicide-Related Distress: A Systematic Review. Arch Suicide Res. 2022;26:1022–45. doi: 10.1080/13811118.2021.1915217. [DOI] [PubMed] [Google Scholar]
- 40.Camacho E, Cohen A, Torous J. Assessment of Mental Health Services Available Through Smartphone Apps. JAMA Netw Open. 2022;5:e2248784. doi: 10.1001/jamanetworkopen.2022.48784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Grist R, Porter J, Stallard P. Acceptability, Use, and Safety of a Mobile Phone App (BlueIce) for Young People Who Self-Harm: Qualitative Study of Service Users’ Experience. JMIR Ment Health. 2018;5:e16. doi: 10.2196/mental.8779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Ballantyne M, Jha A, Jacobsen A, et al. Study of accessibility guidelines of mobile applications. MUM 2018; Cairo Egypt. Nov 25, 2018. Available. [DOI] [Google Scholar]
- 43.Bidargaddi N, Almirall D, Murphy S, et al. To Prompt or Not to Prompt? A Microrandomized Trial of Time-Varying Push Notifications to Increase Proximal Engagement With a Mobile Health App. JMIR Mhealth Uhealth. 2018;6:e10123. doi: 10.2196/10123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Freyne J, Yin J, Brindal E, et al. Push Notifications in Diet Apps: Influencing Engagement Times and Tasks. Int J Hum-Comput Interact. 2017;33:833–45. doi: 10.1080/10447318.2017.1289725. [DOI] [Google Scholar]
- 45.Garrido S, Oliver E, Chmiel A, et al. Encouraging help-seeking and engagement in a mental health app: What young people want. Front Digit Health. 2022;4:1045765. doi: 10.3389/fdgth.2022.1045765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.American Psychiatric Association App advisor an American Psychiatric Association initiative. https://www.psychiatry.org/psychiatrists/practice/mental-health-apps/the-app-evaluation-model Available.
- 47.Bruen AJ, Wall A, Haines-Delmont A, et al. Exploring Suicidal Ideation Using an Innovative Mobile App-Strength Within Me: The Usability and Acceptability of Setting up a Trial Involving Mobile Technology and Mental Health Service Users. JMIR Ment Health. 2020;7:e18407. doi: 10.2196/18407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Shin HD, Durocher K, Sequeira L, et al. Information and communication technology-based interventions for suicide prevention implemented in clinical settings: a scoping review. BMC Health Serv Res. 2023;23:281. doi: 10.1186/s12913-023-09254-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Greenhalgh T, Wherton J, Papoutsi C, et al. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. J Med Internet Res. 2017;19:e367. doi: 10.2196/jmir.8775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Simon GE, Shortreed SM, Rossom RC, et al. Effect of Offering Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adult Outpatients With Suicidal Ideation: A Randomized Clinical Trial. JAMA. 2022;327:630–8. doi: 10.1001/jama.2022.0423. [DOI] [PMC free article] [PubMed] [Google Scholar]