

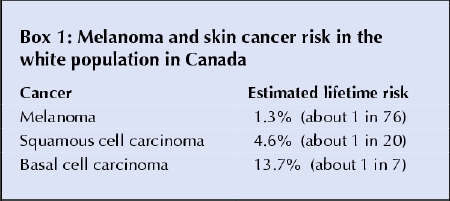
Skin cancers are the most common form of malignant disease in white populations worldwide. Although the incidence of cutaneous malignant melanoma is relatively low (Box 1), almost 15% of cases are fatal. Squamous cell carcinoma and basal cell carcinoma, the 2 most common forms of nonmelanoma skin cancer, are usually treated surgically. They rarely cause death, but because they occur predominantly on sun-exposed sites such as the face, they can be disfiguring.
Box 1.
It is well established that sunlight can initiate and promote carcinogenesis and that excessive exposure is the main cause of both melanoma and nonmelanoma skin cancer. The proportion of melanoma in Canada caused by sunlight exposure is estimated to be more than 90%,1 and this figure likely also applies to nonmelanoma skin cancers.
Because such a high proportion of malignant skin disease is attributable to sunlight exposure, skin cancer prevention messages and programs have become common in countries where the majority of the population has a lighter skin colour. In many of these programs, chemical sunscreens are suggested as a “last resort” in sun protection, to be used only if reductions in sunlight exposure cannot be achieved by the use of shade and protective clothing (long-sleeved shirts and long pants) and by limiting the time spent outdoors. Although the “cover-up” strategy may work well in countries like Australia, where sunlight abounds throughout the year, it is less effective in Canada, where sunshine is reliably available only 3 months each year. The question, then, for Canadian physicians making recommendations to their patients, is “What can sunscreens do and what can't they do?”
We know that all modern sunscreens with a high (15+) “sun protection factor” (SPF) give good protection against sunburn when properly applied. Sunburn is caused largely by ultraviolet B radiation (300–320 nm), and older sunscreens also gave good protection from these wavelengths. There is some evidence that melanoma may also be related to ultraviolet A exposure, but this is controversial since the studies showing such results use an animal model (fish of the Xiphophorus genus) with little resemblance to humans.2 Sunscreen manufacturers have responded with broad-spectrum sunscreens that provide substantial protection from ultraviolet A and B radiation.
The use of these new agents is not without concern, however. The results of a European trial of the use of unlabelled sunscreens of SPF 10 and 30 by people aged 18–24 demonstrated that those wearing the SPF 30 preparation spent more time in the sun per day (3.1 v. 2.6 hours) when on holiday than those using the SPF 10 compound.3 The amount of sunscreen used by each group was similar, as was the holiday duration. The degree of sunburn reported by each group was similar, so the higher SPF compound clearly provides better sunburn protection. However, if people spend more time in the sun to acquire the same degree of tan obtained when a lower SPF preparation is used, then this raises concerns about the long-term effects of increased exposure, largely because DNA damage can occur long before sunburn appears. Is there evidence that high-SPF, broad-spectrum sunscreens provide protection against skin cancer? The answer appears to both “yes” and “no.”
Squamous cell carcinoma and basal cell carcinoma
First, the good news. A number of trials have provided good evidence that, when applied consistently, sunscreens can realistically play a role in reducing the risk of squamous cell carcinoma (Box 2).
Box 2.
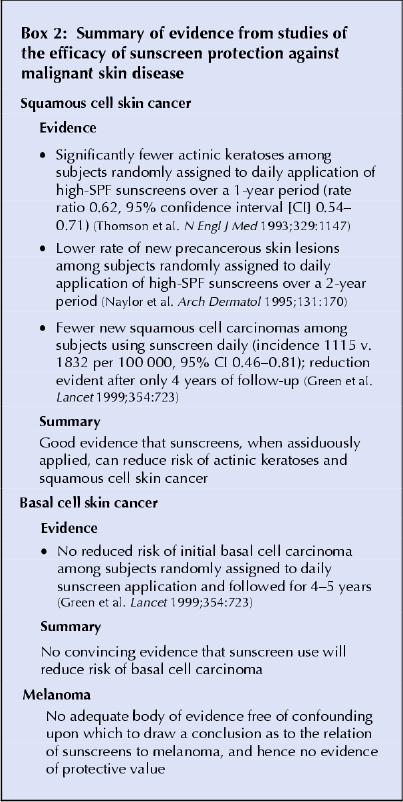
The story with basal cell carcinoma is less hopeful. Although studies are continuing, there is as yet no convincing evidence that sunscreen use reduces the risk of this type of carcinoma (Box 2).
Melanoma
Melanoma is a story unto itself. Because it is so much less common than either of the nonmelanoma skin cancers, it has not been feasible to conduct randomized trials aimed at sunscreen evaluation. Results from a randomized trial indicate that sunscreens attenuate the development of nevi in children over the short term (3 years),4 but it is not clear that this effect will persist, or that it predicts a reduced risk for melanoma later in life.
All other studies of the relation between sunscreen use and melanoma have been retrospective in nature (Box 3). Most showed no protective effects from sunscreen use, and some even indicated an increased risk for users. The results of these studies must be treated with caution. Most research conducted before the 1990s was designed to investigate the association between sun exposure, pigmentation characteristics and melanoma. As a consequence the data collected on sunscreen use was usually relatively cursory. To fairly evaluate the association, additional information is required, including whether a high-SPF sunscreen was used, whether it was applied in adequate amounts to attain the advertised SPF value, the frequency of sunscreen use, and the body sites it was applied to. Without accurate information on these variables, there is likely to be substantial misclassification in usage data with consequent dilution of the probability of finding a protective effect.
Box 3.
In addition to the information quality problems that affected earlier studies, serious potential problems with uncontrolled confounding are likely to have affected the results of even the more recent studies. Sunscreens are most commonly used by those with a strong propensity to burn in the sun because of fair skin. These same people are also at elevated risk of melanoma because of that same sun sensitivity, and techniques to measure sun sensitivity in population-based studies are unfortunately relatively crude. Thus it is highly likely that there is some degree of uncontrolled confounding from this factor in virtually all retrospective studies, and this may well be the reason why a number of the investigations show a direct rather than an inverse relation between use and melanoma risk (Box 3). Finally, there is evidence from previous etiologic studies that the degree of sun exposure in childhood and adolescence may be of particular importance in the later genesis of melanoma. If this is true, and effective sunscreens were not available to study subjects in this period, subsequent use will suggest a positive relation with risk.
Clearly these limitations present major problems in determining whether sunscreens have a role in melanoma prevention, and it is unlikely that they can be addressed through more retrospective investigations. A randomized trial beginning with the induction of healthy subjects would be the optimum method for moving forward, but such trials may not be practical for reasons of cost and study duration.
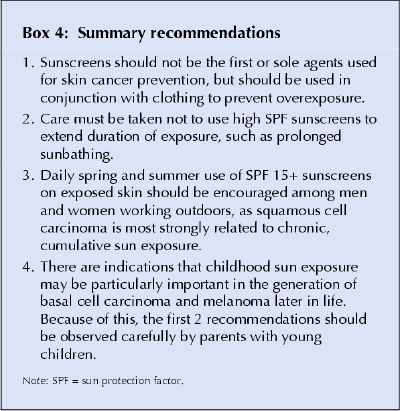
It is clear from this data that sunscreens cannot protect against all forms of skin cancer, and thus a rational strategy for skin cancer prevention must also include use of protective clothing. In addition, because all skin cancers are related to sun exposure, avoiding the sun is also likely to be beneficial. A practical approach is shown in Box 4.
Box 4.
It is important that these recommendations are accompanied by encouragement to participate in vigorous outdoor activity, with moderate sun exposure. With obesity on the rise, particularly among children, it would be counterproductive to encourage avoidance of outdoor activity. In addition, recent evidence suggests that vitamin D (largely generated through sun exposure) may be more important in health maintenance than we have traditionally believed.
Richard P. Gallagher Cancer Control Research Program B.C. Cancer Agency Department of Health Care and Epidemiology Division of Dermatology University of British Columbia Vancouver, BC
References
- 1.Armstrong BK, Kricker A. How much melanoma is caused by sun exposure? Melanoma Res 1993;3:395-401. [DOI] [PubMed]
- 2.Setlow RB, Grist E, Thompson K, Woodhead AD. Wavelengths effective in induction of malignant melanoma. Proc Natl Acad Sci USA 1993;90:6666-70. [DOI] [PMC free article] [PubMed]
- 3.Autier P, Dore JF, Negrier S, Lienard D, Panizzon R, Lejeune FJ, et al. Sunscreen use and duration of sun exposure: a double-blind randomized trial. J Natl Cancer Inst 1999;91:1304-9. [DOI] [PubMed]
- 4.Gallagher RP, Rivers JK, Lee TK, Bajdik CD, McLean DI, Coldman AJ. Broad-spectrum sunscreen use and the development of new nevi in white children. A randomized controlled trial. JAMA 2000;283:2955-60. [DOI] [PubMed]