

Abstract
Objective
To describe the results from the Global Burden Disease (GBD) study 2019 on the burden of other musculoskeletal (MSK) disorders in Latin America and the Caribbean (LAC).
Methods
In this cross-sectional study, we analyzed data from all LAC region in the GBD study from 1990 to 2019. Other MSK (other than rheumatoid arthritis, osteoarthritis, gout, low back pain, and neck pain) burden was measured as prevalence, mortality, years lived with disability (YLD), and disability-adjusted life (DALY), by year, sex, and country. We show the counts, rates, and 95% uncertainty intervals (95% UI). Joinpoint regression analysis was used to estimate the average annual percentage change (AAPC) from 1990 to 2019. A correlational analysis between the burden parameters and sociodemographic index (SDI) was performed.
Results
In 2019, there were 52.0 million (95% UI, 44.8–60.1 million) individuals with other MSK disorders in LAC. The age-standardized mortality rate in 2019 was 1.2 (95% UI, 0.8–1.6) per 100,000 inhabitants. The AAPC was estimated as 0.1% (95% confidence interval [CI], 0.1–0.2) and 0.2% (95% CI, 0.1–0.3) for prevalence and mortality rates, respectively. The age-standardized DALY rate was 685.4 (95% UI, 483.6–483.6) per 100,000 inhabitants, representing an AAPC of 0.2% (95% CI, 0.1–0.3). The burden was larger in women and the elderly. The SDI was positively correlated with the prevalence of YLD in 2019.
Conclusions
LAC region has experienced a significant burden of other MSK disorders over the last three decades. To challenge this growing burden, population-based strategies designed to reduce the burden of other MSK and strengthen health systems to contribute effective and cost-efficient care are necessary.
Key Words: burden, epidemiology, musculoskeletal disorders, systemic lupus erythematosus
Disease burden is the impact of a health condition on a given population and can be measured using a variety of indicators such as mortality, morbidity, and financial cost. Disease burden is often measured using accepted indicators that facilitate comparison of the burden of different diseases and take into account both mortality and morbidity.1 The Global Burden Disease Study (GBD) is a systematic, scientific effort to quantify the magnitude of all major diseases, risk factors, and intermediate clinical outcomes in a highly standardized way to allow for comparison over time, across populations, and between health problems. In previous publications, the burden of musculoskeletal (MSK) disorders was described mainly through rheumatoid arthritis (RA), osteoarthritis (OA), low back pain (LBP), neck pain (NP), and gout using the GBD studies conducted in 20102 and 2017.3 In the GBD 2019 study, it was demonstrated that the burden of MSK conditions tends to be lower in countries with higher sociodemographic index (SDI) than in lower SDI regions.4 Several other MSK disorders were not captured initially in an individual fashion, but they are considered in the group of “other MSK disorders.” This category, which is one of the world's highest sources of global disability burden, includes diverse conditions, such as systemic lupus erythematosus (SLE), systemic connective disorders, inflammatory polyarthropathies, and infectious arthropathies, among others.5 Some diseases in the group of other MSK disproportionately affect Latin American and Caribbean (LAC) populations, with worse outcomes compared with nonminority populations.6 The burden of these conditions has been reported globally, regionally, and nationally.3 At the global level, the age-standardized prevalence rate (ASPR) of other MSK diseases in 2017 was 4151.1 (+3.4% from the previous GBD study) and the mortality rate 1.0 (+7.2%).7 Point prevalence estimates were higher in women and increased with age. Moreover, the age-standardized disability-adjusted life years (DALY) in 2017 increased by 3.4%. At national level, the largest increases in ASPR in 2017 were observed in Bangladesh, India, and Nepal, and the greatest increases in ASPR were observed in Romania, Croatia, and Armenia.7 Other studies have also reported the burden of MSK disorders, reporting either more regionally or nationally. In Latin America and the Caribbean (LAC), a Mexican study analyzed the burden of all MSK disorder categories (1990–2016),8 these are significant causes of premature death and disability. In 2019, the GBD was updated, providing an opportunity to incorporate newly available datasets, thus enhancing the method performance and standardization.9 Between 1990 and 2019, the global age-standardized DALY rate in MSK remained nearly constant by sex and age group, but mainly decreased among young females, while it increased in about 80% of countries and territories for both women and men aged 50 to 74 years and 75 years or older.10 This circumstance creates a substantial burden on social and economic values related to medical care and productivity decline.11 In addition, the intricate interaction of health factors in LAC emphasizes the need to evaluate other MSK disorders to guarantee sufficient financial, clinical, and scientific resource distribution in the area. Furthermore, there are socioeconomic inequalities concerning access barriers to health services in LAC,12 predominantly in women,13 a group frequently affected by other MSK disorders. The previous analysis of the burden from the GBD 2019 study did not consider the other MSK group separately. This, combined with the fact that in the LAC region, has several disadvantages such as poverty, limited access to rheumatologists and restricted rheumatology training programs,14 an evaluation of the burden of other MSK in LAC is needed. Therefore, we aimed to investigate the burden of other MSK disorders in LAC utilizing the estimates presented by the GBD study from 1990 to 2019, by age, sex, and SDI.
METHODS
We analyzed the burden of other MSK disorders in adults and children in 17 countries and five subregions (Supplementary Table S1, http://links.lww.com/RHU/A630). The GBD 2019 study covered estimates generated annually from 1990 to 2019, and the data incorporated 369 diseases and injuries by age and sex. The explanation of the approaches employed by the GBD and the distinct process used for the mortality evaluation of other MSK disorders has already been already described.9 The GBD 2019 study applied the same covariates utilized in the GBD 2017 study, and significant modifications from the GBD 2017 modeling approach were identified.5
Data Sources
The information employed by the GBD for each disorder or injury included censuses, population surveys, civil registrations, vital statistics, and systematic reviews with meta-analysis, among other sources.15 The systematic review focused on detecting health surveys evaluating the complete number of MSK conditions and complaints.9 According to the GBD ranking process, most LAC countries showed acceptable estimates, taking into account some relevant characteristics, such as the details of data and completeness, among others.16
Other MSK diseases are a miscellaneous group combining general conditions of muscles, bones, and ligaments, which were not covered in the GBD-defined MSK conditions (RA, OA, LBP, NP, and gout) and that are not considered long-term injury sequelae. The dataset created for the GBD 2019 data involved 20,372 site-years of vital registration estimates for other MSK disorders.9
The GBD 2019 study utilized the International Classification of Disease (ICD) codes (ICD-9 and ICD-10) definitions of other MSK disorders, such as SLE (ICD-9: 710.0, ICD-10: M32), inflammatory polyarthropathies (ICD-9: 712–713, ICD-10: M20-M25), spondylopathies (ICD-9: 720–721, ICD-10: M46-M46), disorders of muscles (ICD-9: 725, ICD-10: M60-M63), among others. Supplementary Table S2, http://links.lww.com/RHU/A630 shows the complete list of codes listed as “other MSK disorders”.
Definition of GBD Study Metrics
The data extracted from the GBD 2019 study included estimates of prevalence, mortality, disability, and DALY for sex and all accessible age groups. In order to evaluate the burden of disease, the GBD assesses the DALY, years of life lost (YLL), and years lived with disability (YLD). YLL are used to assess premature mortality, which is calculated as the product of the total counts of other MSK disorders in every age group and the referenced life expectancy at the mean age of death of those who passed away in the age group.9 YLD estimate the impact of disability by multiplying the prevalence of each other MSK disorder by the GBD disability weight. DALYs is a measure that combines YLD and YLL. One DALY is equivalent to losing 1 year of good health due to premature mortality, disease, or disability. One DALY describes one lost year of healthy life. Moreover, the GBD provided the SDI, an outline indicator of social and economic development that permits the analysis of disease burden patterns across various resource conditions.17,18 SDI was calculated from the geometric mean of three components: total fertility rate under 25 years, lag-distributed income per capita, and average educational attainment for all areas in the GBD study.17
The SDI scales from 0 to 1, with 1 denoting the region with the highest per capita income, number of years of schooling, and the lowest fertility rate.
Data Extraction
Two authors independently extracted data from the GBD 2019 database from the years 1990–2019. We extracted the following metrics per country or sub-region: prevalence, mortality, DALY, YLL, YLD and SDI. These indicators were reported as absolute numbers and as standardized rates (ASRs for 100,000 individuals). The databases were transferred from the GBD study website (open access) http://ghdx.healthdata.org/gbd-results-tool. The data were tabulated on a Microsoft Excel spreadsheet.
Statistical Analysis
Descriptive analyses were performed to describe the burden of other MSK diseases based on age, year, sex, and location. GBD estimates of the disease burden were reported using the 95% uncertainty intervals (95% UI). The 95% UI explain the variability in the estimations and includes the uncertainty presented during the estimation calculations.9 We contemplated the rates to be significantly different if their 95% UI did not overlap. Age-standardized rates (ASRs) were calculated using the GBD study's world standard population in the corresponding age group. Through the direct method using age-standardized rates, the GBD age framework facilitates analogies among countries irrespective of the size and age framework of the inhabitants. The percentages of change from 1990 to 2019 were also reported to compare the overall trends across the sub-regions and countries that were not originally provided in the platform. In addition, the average annual percent change (AAPC) and the corresponding 95% confidence intervals (CI) between 1990 and 2019 for overall prevalence, mortality, DALY, YLL, and YLD rates were calculated by the Joinpoint regression program, version 5.0.1 (National Cancer Institute, Rockville, MD).
Finally, a correlation analysis was performed to identify a possible relationship between the burden parameters and SDI using the Spearman correlation test. Statistical significance was set at p < 0.05 was considered statistically significant. SPSS Statistics for Mac version 23 software (IBM Corp., Armonk, NY) was used for the data analysis.
RESULTS
Prevalence, Prevalence Rates, and Trajectories
Our findings showed that in 2019, there were 52.0 million (95% UI 44.8–60.1 million) individuals with other MSK disorders in LAC, while the prevalence rate of other MSK disorders in 2019 was 7541.9 (95% UI, 6510.1–8709.8) per 100,000 inhabitants. The prevalence rate increased significantly from 1990 to 2019 with AAPC of 0.1% (95% CI, 0.1–0.2; p = 0.001). Table 1 shows the estimates in LAC region.
TABLE 1.
Burden of Other Musculoskeletal Disorders in Latin America and Caribbean in Absolute Number and in Age-Standardized Rates (1990–2019) in Both Sexes and by Sex
| 1990 | 2019 | Changes | |||
|---|---|---|---|---|---|
| Number (in Thousands) (95% UI) | Age Standardized Rate (by 100,000 Population) (95% UI) | Number (in Thousands) (95% UI) | Age Standardized Rate (by 100,000 Population) (95% UI) | AAPC of Age Standardized Rates, 1990–2019 (95% CI) | |
| Overall Latin America | |||||
| Prevalence | 24,583.2 (21,024.7–28,513.3) | 7193.3 (6126.1–8306.2) | 52,044.5 (44,805.4–60,086.8) | 7541.9 (6510.1–8709.8) | 0.1% (0.1–0.2) |
| Deaths | 3545.3 (2635.1–5175.7) | 1.2 (0.8–1.6) | 8243.7 (5781.9–10,947.7) | 1.2 (0.9–1.6) | 0.2% (0.1–0.3) |
| DALYs | 2255.9 (1573.5–3083.7) | 649.6 (457.5–888.9) | 4728.9 (3330.5–6460.7) | 685.4 (483.6–935.7) | 0.2% (0.1–0.3) |
| YLLs | 154.3 (116.4–207.9) | 39.4 (29.8–59.2) | 301.8 (207.9–398.9) | 44.4 (30.7–58.7) | 0.4% (0.3–0.6) |
| YLDs | 2101.6 (1427.5–2935.8) | 610.3 (418.1–849.6) | 4427.1 (3016.3–6184.2) | 641.0 (437.7–892.6) | 0.1 (0.1–0.2) |
Values p < 0.05 are given in bold.
Prevalence in Subgroups
The prevalence rate in 2019 was higher in females, 8729.2 (95% UI, 7639.5–9997.8) per 100,000 inhabitants than in males, 6230.7 (95% UI, 5259.5–7317.4) per 100,000 inhabitants. The highest prevalence rate was identified in patients in the category aged 50 to 69 years (16,576.3; 95% UI, 13,129.4–20,681.5) per 100,000 inhabitants, followed by the group 70 years and older (15,596.3; 95% UI, 11,283.9–20,556.0) per 100,000 inhabitants, and the group aged 15 to 49 years (10,782.6; 95% UI, 8734.5–13,093.5) per 100,000 inhabitants. The subregion with the largest ASPR for overall LAC in 2019 was South Latin America (Argentina, Chile, and Uruguay) with 9935.6 (95% UI, 8598.7–11,449.2) per 100,000 inhabitants, and the subregion with the lowest ASPR was the Caribbean with 4333.1 (95% UI, 3614.4–5105.9) per 100,000 inhabitants. However, the subregion with the highest increase from 1990 to 2019 was the Caribbean (+22.2%), and the subregion of Tropical Latin America exhibited a decrease from 1990 to 2019 (−7.9).
Bolivia was the country with the lowest ASPR in 2019, with 5836.3 (95% UI, 4968.0–6810.9) per 100,000 inhabitants, followed by Peru with 6121.7 (95% UI, 5245.7–7149.9) per 100,000 inhabitants, whereas the country with the highest ASPR was Chile with 10,107.8 (95% UI, 8132.5–11,603.0) per 100,000 inhabitants. Variations by sex, age, and geographical areas were considered statistically significant because of the lack of overlapping 95% UIs. Supplementary Table S3, http://links.lww.com/RHU/A630 shows the burden of other MSK disorders by country in both sexes and Table S4, http://links.lww.com/RHU/A630 shows the burden by country and by sex.
Mortality Rates and Trajectories
The age-standardized mortality rate (ASMR) attributable to other MSK disorders in LAC in 2019 was 1.2 (95% UI, 0.9–1.6) per 100,000 inhabitants. This was also confirmed when the AAPC was considered (AAPC, 0.2%; 95% CI, 0.1–0.3; p < 0.001).
Mortality in Subgroups
In 2019, it was higher in women 1.6 (95% UI, 1.0–2.5) per 100,000 inhabitants than in males, 0.7 (95% UI, 0.4–0.8) per 100,000 inhabitants. The ASMR by age groups is shown in Figure 1.
FIGURE 1.
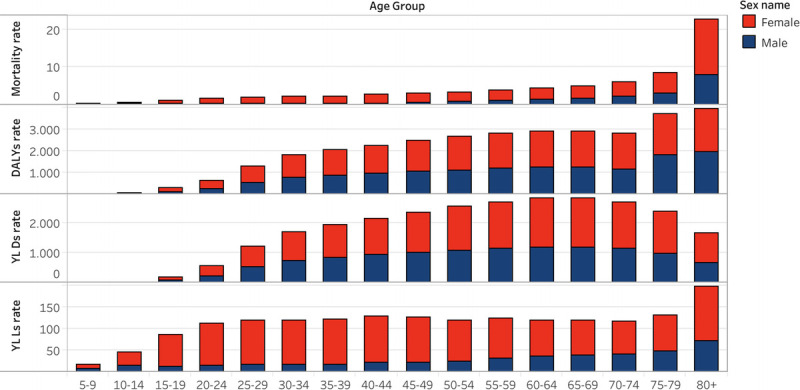
DALYs, YLLs, YLDs and deaths rates (per 100,000 inhabitants) for other MSK disorders by age subgroup (in females and males) in LAC in 2019.
The highest ASMR was observed in patients in the category aged 70 years and older (6.3; 95% UI, 4.6–8.8) per 100,000 inhabitants, followed by the group aged 50–69 years (1.9; 95% UI, 1.3–2.6) per 100,000 inhabitants.
Central Latin America had the largest ASMR in 2019 (1.43; 95% UI, 0.9–1.9 per 100,000 inhabitants), and Andean Latin America had the lowest (0.7; 95% UI, 0.5–0.9 per 100,000 inhabitants). The country with the largest ASMR was Honduras (1.6; 95% UI, 1.1–2.3 per 100,000 inhabitants), followed by Costa Rica (1.6; 95% UI, 1.1–2.4 per 100,000 inhabitants). The country with the lowest ASMR was Peru (0.5; 95% UI, 0.3–0.6 per 100,000 inhabitants), followed by Uruguay (0.6; 95% UI, 0.4–1.0 per 100,000 inhabitants). Since the 95% UIs did not overlap, the national-level variations were statistically significant.
Burden of Other MSK Disorders
DALY. The total DALY count for other MSK disorders in LAC in 2019 was 4.7 million (95% UI, 3.3–6.5 million). The ASR of DALY in LAC was 685.4 (95% UI, 483.6–935.7) per 100,000 inhabitants, driven by the YLD (93.5%). The AAPC also showed an increment over the entire period of study (0.2%, 95% CI 0.1–0.3; p = 0.005)
The ASR of DALY was higher in women (807.5; 95% UI, 577.4–1088.6 per 100,000 inhabitants) than in men (552.1; 95% UI, 381.2–764.9 per 100,000 inhabitants), as was the case in 1990. Patients aged 50–69 years had the highest ASR of DALY (1446.9; 95% UI, 970.8–2052.8).
The sub-region with the largest ASR was South Latin America (878.7; 95% UI, 613.5–1215.2 per 100,000 inhabitants), whereas the sub-region with the lowest ASR was the Caribbean (417.7; 95% UI, 299.5–565.7 per 100,000 inhabitants). Chile was the country with the highest ASR of DALY (895.1 95% UI, 623.0–1231.5 per 100,000 inhabitants), followed by Argentina (874.6; 95% UI, 608.8–1202.9 per 100,000 inhabitants). The countries with the lowest ASR of DALY were Bolivia (523.2; 95% UI 361.6–716.6 per 100,000 inhabitants) and Peru (536.9; 95% UI, 362.6–745.3 per 100,000 inhabitants). These geographical differences did not have overlapping confidence intervals; therefore, they were considered significant.
YLD. The total count of YLD in 2019 was 4.4 million (95% UI, 3.0–6.2 million). The ASR of YLD was 641.0 (95% UI, 437.7–892.6) per 100,000 inhabitants, which was 5.0% higher than the 1990 rate. The ASR of YLD was higher in women (737.6; 95% UI, 512.9–1021.7 per 100,000 inhabitants) than in men (534.5; 95% UI, 362.4–748.2 per 100,000 inhabitants). The highest rate was observed in patients aged 50–69 years (1386.5; 95% UI, 908.5–1993.3).
The sub-region with the largest rate was South Latin America (848.8.0; 95% UI, 584.6–1184.1 per 100,000 inhabitants), while the sub-region with the lowest rate was the Caribbean (370.0; 95% UI, 246.2–515.5). Chile and Argentina were the countries with the highest ASR of YLD (862.5; 95% UI, 590.8–1197.2; and 844.9; 95% UI, 576.8–1174.6 per 100,000 inhabitants, respectively), while Bolivia and Ecuador had the lowest rates of YLD (496.9; 95% UI, 337.4–690.8 and 425.5; 95% UI, 355.4–728.3 per 100,000 inhabitants, respectively). However, these regional and by-country differences were not statistically significant.
YLL. In 2019, total data for other MSK disorders in LAC were 4.4 million (95% UI, 3.0–6.2 million). The ASR of YLL was 44.4 (95% UI, 30.7–58.7) per 100,000 inhabitants, that is, an increase of 12.58% from the 1990 rate. The ASR of YLL was greater in women (69.7; 95% UI, 43.6–96.4 per 100,000 inhabitants) than in men (17.7; 95% UI, 12.4–21.1 per 100,000 inhabitants). Patients aged 70 years and older had the largest ASR of YLL (74.5; 95% UI, 53.4–102.4). Central Latin America had the highest rate (54.4; 95% UI, 36.3–74.1 per 100,000 inhabitants), while Andean Latin America had the lowest rate (22.7; 95% UI, 15.3–28.7 per 100,000 inhabitants). The country with the highest the ASR of YLL was Venezuela (67.9; 95% UI, 40.5–100.3 per 100,000 inhabitants), followed by Colombia (63.2; 95% UI, 31.1–89.9 per 100,000 inhabitants). The nations with the lowest rates of YLL were Peru (12.3 (95% UI, 7.3–17.1 per 100,000 inhabitants) and Uruguay (16.4; 95% UI, 12.9–31.2 per 100,000 inhabitants).
CORRELATION ANALYSIS
We identified a positive correlation between ASPR (rho = 0.64; p = 0.004), ASMR (rho = 0.47; p = 0.04), DALY (rho = 0.61; p = 0.007), ASR of YLD (rho = 0.64; p = 0.004), and SDI in 1990. Similarly, a correlation was reported between ASPR (rho = 0.67; p = 0.002), ASR of DALY (rho = 0.66; p = 0.011), and ASR of YLD (rho = 0.67; p = 0.002), and SDI in 2019, but not for ASMR (rho = −0.38; p = 0.12). However, we did not identify a significant correlations between YLL and SDI in either 1990 or 2019 (rho = 0.05; p = 0.85 and rho = −0.20; p = 0.43, respectively).
DISCUSSION
The burden of other MSK disorders, measured by the ASR of DALY, increased from 649.6 in 1990 to 685.4 per 100,000 inhabitants in 2019 (approximately 6%) in the LAC, mainly driven by the YLD. In addition, the prevalence rate increased significantly in the majority of LAC countries. We identified that 52.0 million persons lived with other MSK disorders in LAC in 2019, representing 8.0% of all persons with this diagnosis globally. Although the number of deaths from other MSK disorders was notably augmented in most LAC countries, ASMR exhibited diverse performances. The increase in burden was higher in both adults and older adults. Although there was a decrease in ASMR in children, YLD increased in this age group. Furthermore, LAC countries accumulated 2.6% of the worldwide DALY for other MSK disorders, ranking third among GBD regions (after South Asia and North America). Chile and Argentina were the nations with the most considerable burdens, and those with the smallest estimates were Bolivia and Peru. Interestingly, SDI was positively correlated with the frequency of other MSK disorders and disability burden, but not with mortality.
At the country-level data, we identified interesting findings. The countries with the highest ASPR were Chile and Argentina, which also had the highest burden (DALY), with the predominance of YLD. Thus, Chile and Argentina have the greatest burden of disability due to other MSK disorders. Interestingly, countries such as Chile and Argentina scored high on the Human Development Index in the region,19 have the highest income in the region, and also have universal insurance coverage.20 The reasons for these findings remain unclear. Although epidemiological-data registration is good functioning, mainly in death certificates, with quality and high completeness reported,21 in data on prevalence, DALY rates are subject to restrictions, such as data sources quality. Some researchers remarked on fragmentation and decentralization in providing good healthcare services in Argentina's health system. In addition, the economic and social disparities challenge the achievement of adequate universal health coverage, which may have an impact on MSK health outcomes.22
Furthermore, Argentina, as compared with other LAC countries, was described as a potential predictor of damage in patients with SLE (the disease that contributed the most in terms of mortality within the group of other MSK) in the overall GLADEL (Grupo Latino Americano De Estudio del Lupus) cohort.6 In the case of Chile, there are some possible explanations for the results found in the present study. Difficulties complicating women's access to healthcare have been found, and among female users of the health system and problems of access have been observed.23 Disparities in health services for elderly individuals have been reported in the Chilean health system.24 This is important in terms of the mean age of the population with other MSK disorders.25
Although some countries in the LAC region do not present the lowest Human Development Index scores,19 had high burden indicator rates, possibly due to limited access to adequate and opportune diagnosis and management. In addition, the introduction of novel beneficial therapies, such as biologics for some of the diseases included in the group of other MSK disorders, like SLE or autoimmune diseases, which have higher mortality rates, could impact burden indicators in the future.26 In contrast, Bolivia and Peru had the lowest rates of point prevalence and burden of other MSK disorders in terms of DALY and YLD, whereas Peru had the lowest ASMR in LAC. This result from Peru is striking; thus, dissecting the causes of this low mortality rate is very important. Some studies have found that the global prevalence of some autoimmune diseases like SLE in Peru could be lower than that in other LAC countries.27 It is noteworthy that despite the positive results shown here, there remain specific needs regarding Peru's health system.
Although other MSK disorders are a diverse remaining MSK group comprising a broad category of disorders, the majority of deaths due to this group of conditions are derived from autoimmune disorders such as SLE and systemic sclerosis, which comprise more than half of the deaths in ICD-10 coded vital registrations of data globally.28 Previous research has found that the ASMR by SLE in LAC between 2001 and 201429 was five times greater than that observed in Europe, a trend that was not observed in the other autoimmune diseases studied. These results were consistent with those reported by other authors.30 Given that patients with SLE in LAC countries face unique problems for diagnosis, prognosis, and treatment, specific SLE therapeutic guidelines have been developed for this population, with the hope that these would be followed by an engaging health system and implemented by specialists, the latter being significant advances toward an improvement in SLE management in LAC and low/middle-income countries.31,32 Improving access to high-cost therapies for many MSK disorders in low/middle-income countries is a great challenge; however, potential strategies have been recently described, and some examples are increasing and restructuring resources, stimulating research evaluating cost-effectiveness and health technology assessment (described as the systematic evaluation of medical technologies concerning effectiveness, appropriateness, and efficiency), flexible patent laws for the use of generics and biosimilar drugs.32–34
Based on our findings, we believe that public health efforts are required for LAC. First, there is a limited number of rheumatologists, particularly in rural areas; therefore, the majority of MSK care depends on primary care physicians, who often lack essential skills. This aspect can be partially solved by structured, validated training in MSK disorder diagnosis and treatment for primary care physicians, of which few have been launched, except in high-income economies.35 In addition, increasing education for nurse practitioners and ancillary care personnel, principally in primary care, should be relevant. Examples of this strategy are those proposed by the Pan-American League of Associations for Rheumatology (PANLAR).36 Although the number of rheumatologists has increased, this appears to be limited. In LAC, four countries currently do not provide rheumatology programs.37 Second, we propose the creation of National Programs of Musculoskeletal Health promoted by either national Rheumatology societies and/or through PANLAR recommendations, which will aid in growing awareness and provide guidance for the prevention and management of all care levels, including primary care, in rural regions (first level). In hospitals with well-trained rheumatologists and internists (second level), and third level, not only general rheumatologists but also rheumatology experts in different rheumatic diseases, such as lupus (“lupologists”). Finally, these programs should be incorporated at all attention levels by using telemedicine strategies.38 With the COVID-19-pandemic, these tools appear feasible in the LAC region.39
In terms of potential impact, prevention of MSK diseases has a great potential for public health benefits, given the burden of these conditions regarding disability and lost productivity. Besides implementing new pharmacological therapies, like biological agents, tertiary prevention, includes interventions focusing on self-management and physical activity requires active patient involvement. The body of evidence supporting the beneficial effects of physical activity is large on cardiorespiratory fitness, muscle strength, and reduced mortality rates.40
Interestingly, the SDI, which increased in all LAC countries from 1990 to 2019, was positively correlated with prevalence and YLD, but not with mortality rates, possibly indicating that the increased burden of these disorders in developed countries was related to the aging of the population. Economic development may only improve other MSK disorders associated with mortality, but more strategies are needed to improve disabilities related to other MSK disorders. Therefore, other determinants such a well-organized healthcare system, strong primary care, effective self-management, and employment, might be limited as a consequence of political, social, and cultural conditions, which are not related to purely economic development.41
All burden metrics evaluated in this study were higher in women than in men, which is consistent with the results of previous GBD studies.7,42 The variations observed by sex could be due to incidence varying with gender, biological differences in the disease course, or access to care. In addition, in some MSK diseases, such as spondyloarthritis, which is part of the group of other MSK disorders, women are reported to have greater disease activity and worse functional decline than with men.43,44 This represents a significant consideration for the therapeutic management of women with these disorders.
Furthermore, the ASPR increased with age. The age group of 70 years or older had the highest ASMR in 2019. Therefore, more prevention strategies should be implemented in these age groups to minimize future disease burden.
Our study has several limitations. First, our analysis is a secondary to the general GBD study, which depends on the exhaustiveness and validity of previous investigations. The GBD study estimates the disease burden from different data sources and population-based epidemiological analysis, subject to measurement error, systematic biases, and modeling and extrapolation to compensate for incomplete data. Second, some assumed estimates for countries with inadequate information might impact the precision of national estimates; that is, underreporting, which might underestimate some mortality and DALY rates. Therefore, analysis of the local or regional burden of other MSK disorders in LAC should be performed with caution. Third, some differences among the estimates identified in our findings are only exploratory because this study was descriptive, showing overlapping 95% UI. Finally, the prevalence and YLD were not estimated in persons prior to the age of 10 years.
In conclusion, GBD approaches generate standardized, complete, and comparable to other MSK disorders estimates, which lead to the recognition of critical concerns about public health, trend changes over time and the burden differences among countries. Over the past three decades, the burden of other MSK disorders in LAC has increased and has contributed substantially to the worldwide burden. According to our findings, this burden is derived from YLD, mainly in adults and older adults. The increased death and YLL rates per 100,000 inhabitants in LAC may indicate limited access to efficient therapies for rheumatology care. For that reason, there is an urgent need that cannot be postponed to improve access to therapies in LAC. Finally, estimating the burden of specific-diseases in the group of other MSK disorders would be valuable for future GBD generations.
Supplementary Material
ACKNOWLEDGMENTS
The GBD 2019 study was supported by the Bill and Melinda Gates Foundation.
Footnotes
ORCID iD: 0000-0002-5101-7705
ORCID iD: 0000-0002-5857-4299
ORCID iD: 0000-0002-6967-7939
ORCID iD: 0000-0003-3145-2440
ORCID iD: 0000-0002-0613-2819.
ORCID iD: 0000-0001-7463-0580
ORCID iD: 0000-0003-1696-9871.
C.M.-P. and I.E.-M. are co-first authors.
Author contributions statement: C.M.-P. and I.E.-M. were responsible for conceptualization, study design, literature search, formal analysis, supervision, data collection, analysis, and interpretation, writing the original draft, reviewing, and editing. P.M.-R. contributed with conceptualization, formal analysis, data interpretation, writing, review, and editing. A.R.-V. and A.D.O.-P. performed data curation, writing, review, and editing. S.M.-M. contributed to the analysis, data interpretation, visualization, writing, review, and editing. M.G.-C. collaborated in writing, reviewing, and editing. All authors had full access to all the data in the study and the final responsibility for the decision to submit for publication.
Funding statement: The authors have not declare a specific grant for this research.
Competing interests: None declared.
Ethical approval: This study was based on data from the GBD 2019 study, which did not require specific institutional ethics approval.
Data availability: Data are available from the Global Health Data Exchange GBD 2019 website (http://ghdx.healthdata.org/gbd-results-tool).
Supplemental digital content is available for this article. Direct URL citation appears in the printed text and is provided in the HTML and PDF versions of this article on the journal’s Web site (www.jclinrheum.com).
Contributor Information
Claudia Mendoza-Pinto, Email: cmendozap.26@gmail.com.
Ivet Etchegaray-Morales, Email: ivetcheg@gmail.com.
Adriana Rojas-Villarraga, Email: sarojas@fucsalud.edu.co.
Ángel David Osorio-Peña, Email: angeldav37@gmail.com.
Socorro Méndez-Martínez, Email: socorro.mendez@imss.gob.mx.
Mario García-Carrasco, Email: mgc30591@yahoo.com.
REFERENCES
- 1.Murray CJL. The Global Burden of Disease Study at 30 years. Nat Med. 2022;28:2019–2026. [DOI] [PubMed] [Google Scholar]
- 2.Hoy DG Smith E Cross M, et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann Rheum Dis. 2014;73:982–989. [DOI] [PubMed] [Google Scholar]
- 3.Safiri S Kolahi AA Cross M, et al. Prevalence, deaths, and disability-adjusted life years due to musculoskeletal disorders for 195 countries and territories 1990-2017. Arthritis Rheum. 2021;73:702–714. [DOI] [PubMed] [Google Scholar]
- 4.Liu S Wang B Fan S, et al. Global burden of musculoskeletal disorders and attributable factors in 204 countries and territories: a secondary analysis of the Global Burden of Disease 2019 study. BMJ Open. 2022;12:e062183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pons-Estel BA Catoggio LJ Cardiel MH, et al. The GLADEL multinational Latin American prospective inception cohort of 1,214 patients with systemic lupus erythematosus: ethnic and disease heterogeneity among ‘Hispanics’. Medicine (Baltimore). 2004;83:1–17. [DOI] [PubMed] [Google Scholar]
- 7.Safiri S Kolahi AA Cross M, et al. Global, regional, and national burden of other musculoskeletal disorders 1990-2017: results from the Global Burden of Disease Study 2017. Rheumatology. 2021;60:855–865. [DOI] [PubMed] [Google Scholar]
- 8.Clark P Denova-Gutiérrez E Razo C, et al. The burden of musculoskeletal disorders in Mexico at national and state level, 1990–2016: estimates from the global burden of disease study 2016. Osteoporos Int. 2018;29:2745–2760. [DOI] [PubMed] [Google Scholar]
- 9.GBD 2019 Diseases and Injuries Collaborators . Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–1222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ziolkowski S Liu S Montez-Rath ME, et al. Association between cause of kidney failure and fracture incidence in a national US dialysis population cohort study. Clin Kidney J. 2022;15:2245–2257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lewis R Gómez Álvarez CB Rayman M, et al. Strategies for optimising musculoskeletal health in the 21(st) century. BMC Musculoskelet Disord. 2019;20:164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Houghton N, Bascolo E, Del Riego A. Socioeconomic inequalities in access barriers to seeking health services in four Latin American countries. Rev Panam Salud Publica. 2020;44:e11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Houghton N Báscolo E Jara L, et al. Barriers to access to health services for women and children in Latin AmericaBarreiras de acesso aos serviços de saúde para mulheres e crianças na América Latina. Rev Panam Salud Publica. 2022;46:e94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dey D Sciascia S Pons-Estel GJ, et al. Health disparities in rheumatic diseases: understanding global challenges in Africa, Europe, Latin America, and Asia and proposing strategies for improvement. Rheum Dis Clin N Am. 2021;47:119–132. [DOI] [PubMed] [Google Scholar]
- 15.Murray CJL, Lopez AD. Measuring global health: motivation and evolution of the global burden of disease study. Lancet. 2017;390:1460–1464. [DOI] [PubMed] [Google Scholar]
- 16.Naghavi M. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the global burden of disease study 2016. BMJ. 2019;364:l94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Global Burden of Disease Study 2019 (GBD 2019) Socio-Demographic Index (SDI) 1950–2019, https://ghdx.healthdata.org/record/ihme-data/gbd-2019-socio-demographic-index-sdi-1950-2019 (accessed 10 September 2022).
- 18.Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1859–1922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Human development in Latin America, https://www.theglobaleconomy.com/rankings/human_development/Latin-Am/ (accessed 14 September 2022).
- 20.Bernales-Baksai P. Tackling segmentation to advance universal health coverage: analysis of policy architectures of health care in Chile and Uruguay. Int J Equity Health. 2020;19:106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Seitz K Deliens L Cohen J, et al. Feasibility of using death certificates for studying place of death in Latin America. Rev Panam Salud Publica. 2021;45:e149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Palacios A, Espinola N, Rojas-Roque C. Need and inequality in the use of health care services in a fragmented and decentralized health system: evidence for Argentina. Int J Equity Health. 2020;19:67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Paredes-Fernández D Lenz-Alcayaga R Rojas-Cáceres C, et al. Womens access to health care: gaps that the future health care reform in Chile must solve. Fortschr Med. 2021;21:e8490. [DOI] [PubMed] [Google Scholar]
- 24.Villalobos Dintrans P. Health systems, aging, and inequity: an example from Chile. Int J Environ Res Public Health. 2020;17:6546. Epub ahead of print September 2020. doi: 10.3390/ijerph17186546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rada I, Oyarte M, Cabieses B. A comparative analysis of health status of international migrants and local population in Chile: a population-based, cross-sectional analysis from a social determinants of health perspective. BMC Public Health. 2022;22:1329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yen EY Shaheen M Woo JMP, et al. 46-year trends in systemic lupus erythematosus mortality in the United States, 1968 to 2013: a nationwide population-based study. Ann Intern Med. 2017;167:777–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pons-Estel GJ, Ugarte-Gil MF, Alarcón GS. Epidemiology of systemic lupus erythematosus. Expert Rev Clin Immunol. 13. Epub ahead of print 2017. doi: 10.1080/1744666X.2017.1327352. [DOI] [PubMed] [Google Scholar]
- 28.Other musculoskeletal disorders — Level 3 cause, https://www.healthdata.org/results/gbd_summaries/2019/other-musculoskeletal-disorders-level-3-cause (accessed 12 September 2022).
- 29.Scherlinger M Mertz P Sagez F, et al. Worldwide trends in all-cause mortality of auto-immune systemic diseases between 2001 and 2014. Autoimmun Rev. 2020;19:102531. [DOI] [PubMed] [Google Scholar]
- 30.Mendoza-Pinto C Etchegaray-Morales I Garcia-Carrasco M, et al. Twenty-year trends in all-cause mortality of patients with systemic lupus erythematosus in Mexico: results from a nationwide health registry. Lupus. 2022;31:382–391. [DOI] [PubMed] [Google Scholar]
- 31.Pons-Estel BA Bonfa E Soriano ER, et al. First Latin American clinical practice guidelines for the treatment of systemic lupus erythematosus: Latin American Group for the Study of Lupus (GLADEL, Grupo Latino Americano de Estudio del Lupus)-Pan-American League of Associations of Rheumatology (PANLAR). Ann Rheum Dis. 2018;77:1549–1557. Epub ahead of print 2018. doi: 10.1136/annrheumdis-2018-213512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mendoza-Pinto C, Etchegaray-Morales I, Ugarte-Gil MF. Improving access to SLE therapies in low and middle-income countries. Rheumatology (Oxford). 2023;62:i30–i35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.WHO . Health technology assessment., https://www.who.int/health-topics/health-technology-assessment#tab=tab_1 (accessed 12 September 2022).
- 34.Garcia R, Araujo DV. The regulation of Biosimilars in Latin America. Curr Rheumatol Rep. 2016;18:16. [DOI] [PubMed] [Google Scholar]
- 35.Dziedzic KS French S Davis AM, et al. Implementation of musculoskeletal models of care in primary care settings: theory, practice, evaluation and outcomes for musculoskeletal health in high-income economies. Best Pract Res Clin Rheumatol. 2016;30:375–397. [DOI] [PubMed] [Google Scholar]
- 36.Drenkard C Fuentes-Silva Y Parente Costa Seguro L, et al. Let's talk about lupus. Overview of an innovative, high-reach, online program to fill the education gaps of Latin Americans living with lupus. J Clin Rheumatol. 2022;28:e368–e374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fernández-Ávila DG Patino-Hernandez D Kowalskii S, et al. Rheumatology training in Latin America: a collaborative study by the Pan American League of Associations for Rheumatology. J Clin Rheumatol. 2022;28:e440–e443. [DOI] [PubMed] [Google Scholar]
- 38.Piga M Floris A Congia M, et al. Telemedicine in rheumatology: high specificity and sensitivity of follow-up virtual video consultations during COVID-19 pandemic. Rheumatology. 2022;61:1795–1801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tang W Inzerillo S Weiner J, et al. The impact of telemedicine on rheumatology care. Front Med (Lausanne). 2022;9:876835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Esbensen BA, Kennedy N, Brodin N. Prevention and adherence in rheumatic and musculoskeletal disease. Best Pract Res Clin Rheumatol. 2020;34:101525. [DOI] [PubMed] [Google Scholar]
- 41.Nicolson PJA Williamson E Morris A, et al. Musculoskeletal pain and loneliness, social support and social engagement among older adults: analysis of the Oxford pain, activity and lifestyle cohort. Musculoskeletal Care. 2021;19:269–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Smith E Hoy DG Cross M, et al. The global burden of other musculoskeletal disorders: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1462–1469. [DOI] [PubMed] [Google Scholar]
- 43.Tournadre A Pereira B Lhoste A, et al. Differences between women and men with recent-onset axial spondyloarthritis: results from a prospective multicenter French cohort. Arthritis Care Res. 2013;65:1482–1489. [DOI] [PubMed] [Google Scholar]
- 44.Gossec L Walsh JA Michaud K, et al. Women with psoriatic arthritis experience higher disease burden than men: findings from a real-world survey in the United States and Europe. J Rheumatol. 2023;50:192–196. [DOI] [PubMed] [Google Scholar]