

ABSTRACT
Objective
The present trial evaluated the first‐time application of autogenous demineralized dentin graft with injectable platelet‐rich fibrin (ADDG + i‐PRF) versus autogenous demineralized dentin graft (ADDG), in alveolar ridge preservation (ARP) in the maxillary aesthetic zone.
Material and Methods
Twenty‐two maxillary (n = 22) non‐molar teeth indicated for extraction were randomized into two groups (n = 11/group). Extracted teeth were prepared into ADDG, implanted into extraction sockets with or without i‐PRF amalgamation and covered by collagen sponge. Cone‐beam computed tomography scans at baseline and 6 months were compared to assess ridge‐dimensional changes. Keratinized tissue width, patient satisfaction, pain score and chair time were recorded. In the course of dental implant placements at 6 months, bone core biopsies of engrafted sites were obtained and analysed histomorphometrically.
Results
Reduction in ridge width was 1.71 ± 1.08 and 1.8 ± 1.35 mm, while reduction in ridge height was 1.11 ± 0.76 and 1.8 ± 0.96 mm for ADDG + i‐PRF and ADDG, respectively (p > 0.05). Significant differences in keratinized tissue width reduction were notable between ADDG + i‐PRF and ADDG (0.12 ± 0.34 and 0.58 ± 0.34 mm respectively; p = 0.008). Postoperative pain scores were significantly lower in ADDG + i‐PRF (p = 0.012). All patients in the two groups were satisfied with no differences in chair time (p > 0.05). No differences in total percentage area of newly formed bone, soft tissue or graft particles were observed between the groups (p > 0.05).
Conclusions
ADDG alone or in combination with i‐PRF yields similar results regarding ARP clinically, quality of the formed osseous tissues, as well as patients' satisfaction. Yet, the addition of i‐PRF to ADDG tends to preserve the keratinized tissue and lessen postoperative pain.
Keywords: alveolar, autogenous, dentin, extraction, platelets, preservation
1. Introduction
With the thickness of the facial bone being < 1 mm in 90% of cases and < 0.5 mm in about 50% of cases in the anterior maxilla (Braut et al. 2011), exodontia, accompanied by the loss of bundle bone and its functions, is usually followed by significant dimensional changes of the alveolar ridge (Heimes et al. 2021; Van der Weijden, Dell'Acqua, and Slot 2009). Alveolar ridge preservation (ARP) techniques typically involve socket osseous grafting, possibly combined with a barrier membrane or soft tissue graft to seal the socket orifice (Horváth et al. 2013; Stumbras et al. 2019). The primary aim remains to lessen dimensional changes following exodontia along with optimizing the contour of the alveolar ridge, possibly for subsequent prosthetic rehabilitation (Mardas et al. 2023, 2015; Sanz et al. 2015).
Dentin and alveolar bone show comparable biochemical compositions, both consisting of organic and inorganic components (Kim et al. 2013), with related embryonic origins (Melek and Marwan 2016). Similar to alveolar bone, dentin harbours type I and III collagen as well as a variety of growth factors, including bone morphogenic protein (BMP), insulin‐like growth factor‐II (IGF‐II) and transforming growth factor‐β (TGF‐β) (Schmidt‐Schultz and Schultz 2005), and was thus suggested as an alternative grafting material with osteoconductive and osteoinductive properties (Park et al. 2015; Um, Kim, and Mitsugi 2017).
Platelets in turn encompass a variety of growth factors such as b‐fibroblast growth factor (b‐FGF), IGF, vascular endothelial growth factor (VEGF), platelet‐derived growth factor (PDGF) and TGF‐β (Boyapati and Wang 2006). Various platelet concentrates were studied in the field of periodontology, including platelet‐rich plasma (PRP) (Harnack et al. 2009), platelet‐rich fibrin (PRF) (Dohan et al. 2006; Elbehwashy et al. 2021), advanced platelet‐rich fibrin (A‐PRF) (Abdulrahman et al. 2022) and injectable platelet‐rich fibrin (i‐PRF) (Alshoiby et al. 2023; Miron and Zhang 2018; Yusri et al. 2024). A‐PRF and i‐PRF were developed through employment of the low‐speed centrifugation (LSCC) concepts (Choukroun and Ghanaati 2018), to retain increased levels of immune cells, growth factors and cytokines (Wend et al. 2017). When combined with bone grafts, they could provide various advantages, including graft stability and ease of handling for the resulting fibrin bone amalgamate “sticky graft” (Miron, Fujioka‐Kobayashi, Bishara, et al. 2017; Miron, Fujioka‐Kobayashi, Hernandez, et al. 2017; Miron et al. 2023).
The combination of i‐PRF and autogenous dentin graft in ARP was described in a case report (van Orten, Goetz, and Bilhan 2022), suggesting that this combination could be valuable in dimensional ridge preservation as well as obtaining vital and good quality bone structure. To the best of the authors' knowledge, no randomized clinical trials, evaluating the combination of i‐PRF to autogenous demineralized dentin graft (ADDG), are currently present in the literature. Hence, the aim of the present randomized controlled trial was to assess the buccolingual ridge width (primary outcome), as well as the height of buccal and lingual ridges of the socket, pain scores, patient satisfaction, chair time, keratinized tissue width and the quality of the newly formed osseous tissue histologically (secondary outcomes), following the application of i‐PRF with ADDG, in comparison to ADDG alone in ARP. The null hypothesis defined was that no differences would be observed between the two groups in term of buccolingual ridge width.
2. Materials and Methods
2.1. Study Design and Registration
The current study was designed as a double‐blind, randomized, parallel arms‐controlled clinical trial, with a 1:1 allocation ratio to compare i‐PRF and ADDG (test group) to ADDG alone (control group) in ARP of post‐extraction alveolar sockets of the aesthetic zone of the maxilla. The research protocol was registered on www.clinicaltrials.gov in June 2022 (ID:NCT05437172). Research protocol, informed consent templates and biological sample collection requests were approved by the Research Ethics Committee, Faculty of Dentistry, Cairo University, in April 2022 (IRB number: 6|04|22). The trial was conducted in compliance with the ethical principles of the Helsinki Declaration for medical research involving human subjects as revised in Seoul, 2008.
2.2. Recruitment of Participants
The study was conducted at the Faculty of Dentistry, Cairo University, Egypt. Participants were recruited from the outpatient clinic of the Department of Oral Medicine and Periodontology at Cairo University's Faculty of Dentistry, between September 2022 and July 2023. Recruitment of participants was conducted by screening patients who were admitted to the outpatient clinic, requiring tooth extractions for subsequent dental implants placement in the maxillary aesthetic zone, until the desired sample size was achieved.
Potential candidates requiring at least one single‐rooted tooth extraction, with periodontally healthy adjacent teeth in the maxillary aesthetic zone between the two the maxillary 2nd premolars (Stumbras et al. 2020), were screened for eligibility and voluntarily recruited. Teeth were extracted if they were non‐restorable due to tooth fracture, unfavourable crown‐to‐root ratio, and extensive caries (Avila et al. 2009; Elfana et al. 2021). Patients had to be systemically healthy, older than 18 years of age, with good oral hygiene and plaque index < 15%. Following extraction, sockets were checked to assure that they were inside the bony housing and having type 1 subdivision B sockets, with intact four walls and thin labial bone thickness (≤ 1 mm; Kim et al. 2021; Steigmann et al. 2022). Smokers, patients reporting any known allergies or systemic conditions that may compromise healing or bone metabolism (e.g., uncontrolled diabetes or hyperthyroidism), having a history of radiotherapy, chemotherapy or bisphosphonate therapy, females who were pregnant or lactating and patients with poor oral hygiene were excluded.
2.3. Sample Size
Sample size was determined based on a difference in buccopalatal alveolar ridge width (primary outcome) equivalent to 0.6 mm as the minimum clinically acceptable value and a standard deviation of 0.45 mm (Elfana et al. 2021). With a power β = 0.8 and α = 0.05, and based on independent samples t test, 10 sites per group were required to reject the null hypothesis, which was increased to 12 sites to account for a possible 20% dropout rate. Calculations were conducted using PS Power and Sample Size Calculations version 3.1.2.
2.4. Randomization
Participants were randomly assigned to receive either i‐PRF + ADDG (test group) or ADDG only (control group), following atraumatic teeth extraction with a 1:1 allocation ratio. A computer‐generated randomization list (www.randomizer.org) was performed by an investigator (MD) who was not involved in the recruitment for the purpose of concealment. Allocation was concealed in serially numbered, identical and opaque sealed envelopes. The investigator (MD), disclosed the allocation only after the atraumatic extraction step had been completed.
2.5. Blinding
Blinding was feasible for the outcome assessor (NS) and biostatistician (KK). However, it was not possible for the principal investigator to be blinded, given that the surgical procedures of the two groups were fundamentally distinct. Blinding of participants was not possible, as the test group participants were administered a distinct intervention, requiring venous blood withdrawal for the i‐PRF preparation.
2.6. Preoperative Phase
Following patients' inclusion, medical history was obtained, teeth of interest were clinically examined and a periapical radiograph was performed. Participants read and signed informed consents after detailed explanation of the aim of the study, benefits to participants, surgical procedures, harms and timeline. Professional mechanical plaque removal (PMPR) was performed and oral hygiene techniques were explained and emphasized.
2.7. Surgical Procedures
Patients were instructed to rinse with 0.12% chlorhexidine mouthwash (Hexitol, Adco Pharma Co., Egypt). Local anaesthesia was administered using 2% mepivacaine HCL, combined with 1:1000 levonordefrin (Alexandria Company for Pharmaceuticals). The removal of the non‐restorable tooth, using a minimally traumatic flapless extraction technique, was initiated by performing a supracrestal fiberotomy. Following tooth loosening via periotomes (Nordent Manufacturing Inc., IL, USA) and straight thin elevators (Nordent Manufacturing Inc., IL, USA), forceps (Nordent Manufacturing Inc., IL, USA) were used to extract it from its socket, followed by inspection of the integrity of the extraction socket using a periodontal probe.
For the ADDG group: The extracted tooth was thoroughly cleaned of any residual periodontal ligaments, cementum, soft tissue attachments, caries or restorations using a high‐speed fine finishing stone and irrigation by saline. Using sterile endodontic files, the pulp chamber was thoroughly cleaned. Subsequently, the tooth was ground using a bone rongeur and a hand bone mill (Gold Bone Mill, MCT Bio, Korea) to obtain chips powder (Kim 2015). To prepare ADDG particles, tooth graft particles were first demineralized by immersing them in 0.6 N hydrochloric acid for 30 min, followed by twice rinsing with saline and drying, using a sterile gauze (Elfana et al. 2021). Subsequently, the graft was placed into the socket and covered by a collagen sponge and a single crisscross 5‐0 polypropylene suture (Figure 1).
FIGURE 1.

Clinical steps of graft harvesting, demineralization, placement, suturing and 6 months of follow‐up for the test and control groups. i‐PRF withdrawal, mixture of ADDG with i‐PRF in the test group. Biopsy harvesting steps using trephine bure and implant placement.
For the i‐PRF + ADDG group: Following the atraumatic extraction technique and the preparation of the dentin graft as previously described, 10 mm of venous blood was collected in a sterile vacutainer plastic tube. The blood was centrifuged at 700 rpm (60 g‐force) for 3 min (Miron, Fujioka‐Kobayashi, Bishara, et al. 2017; Miron, Fujioka‐Kobayashi, Hernandez, et al. 2017). The i‐PRF liquid layer was collected from the top of the tube and mixed with ADDG. The mixture was then allowed to set for 10 min to produce the sticky ADDG. Subsequently, the sticky ADDG was placed in the socket and covered with a collagen sponge and a crisscross 5‐0 polypropylene suture (Eldawlia Tibbi Atik Medical, Istanbul, Turkey; Figure 1).
2.8. Post‐Operative Care and Follow Up
Participants were instructed to avoid any trauma at the operative site, prevent any interference with the suture and abstain from consuming hot food or rinsing for a period of 24 h (Mani et al. 2021). It was recommended to avoid brushing of the surgical area and resume gentle brushing at the area of the operation after a period of 2 weeks (Alazzawi, Ghazi, and Jikia 2018; Bertoldi et al. 2021; Elfana et al. 2021). Participants were prescribed amoxicillin 500 mg (Misr Co. for Pharmaceutical Industries, Egypt) three times daily for a period of 10 days (Ben Amara et al. 2021; Corning and Mealey 2019) or doxycycline 100 mg (Doxymycin, Nile Co. for Pharmaceutical and Chemical Industries, Egypt) twice daily as an alternative to penicillin sensitivity (Corning and Mealey 2019), along with ibuprofen 600 mg (Brufen, Kahira Pharmaceuticals, Egypt) when necessary to alleviate severe pain (Santos et al. 2021). Additionally, a 0.12% chlorhexidine mouthwash was recommended for gentle rinsing, to be used twice daily for a period of 2 weeks (Demetter, Calahan, and Mealey 2017). On the second day postoperatively, baseline cone‐beam computed tomography (CBCT) was performed. The sutures were removed 2 weeks after surgery. Final follow‐up visits and CBCT scans were carried out 6 months postoperatively.
2.9. Outcomes
2.9.1. Radiographic Outcomes
At parameters of 0.2 mm voxel size, 90 KV and 8 mA, CBCT scans (Planmeca ProMax 3D Classic, Helsinki, Finland) were obtained at baseline and 6 months post‐operatively. Following exposure and image acquisition, these images were called “basis images” and transferred through a network for “Image reconstruction.” Scans were exported in DICOM format to the 3D viewer software (Ondemand 3D, Cybermed, 1.0.9, Seoul, South Korea). Preoperative images were fused to postoperative images using manual registration, followed by automatic registration through landmarks on the jaw (Fettouh et al. 2023). All measurements were first recorded on the primary image. Then the measurement on the primary image was left and the primary image itself was cancelled leaving the secondary image. New measurements were subsequently recorded on the secondary image on the same plane direction and cut of the primary image, ensuring standardization. Buccopalatal ridge width was measured from the outermost surface of the buccal and palatal ridges of the extraction socket at three levels (1, 3, and 5 mm below the most coronal aspect of the bone crest; Al Qabbani et al. 2017; dos Santos Canellas et al. 2020; Jung et al. 2013; Yang et al. 2023). For each image (baseline and six months of follow‐up) a colour code was assigned for identification. After the superimposition, measurements were recorded. The loss in alveolar ridge dimensions was reported by subtracting final values from baseline values and expressed in millimetres and percentages (Figure 2). For the buccal and palatal ridge heights, a tangential line was drawn at the most apical point of the socket depth, parallel to the horizontal plane (line A). This was followed by points marked at the most crestal parts of the buccal and lingual/palatal ridges (Point B). The line was then dropped from point B to line A to measure buccal and lingual/palatal ridge heights. The loss in alveolar ridge dimensions was reported by subtracting final values from baseline values and expressed in millimetres and percentages (Pohl, Binderman, and Tomac 2020; Figure 2).
FIGURE 2.

CBCT images illustrating ridge width measurements (a–c) and ridge height measurements (d–f), (a) initial CBCT scan with ridge width measurements at 1, 3 and 5 mm below the most coronal aspect of the crest, (b) fusion superimposition of the initial and 6 months post‐operative scans, (c) 6 months postoperative scan, (d) initial CBCT scan showing a tangential line drawn at the most apical point of the socket depth parallel to the horizontal plane (*), points marked at the most crestal parts of the buccal and palatal ridges (+) and line dropped from (*) to (+) to measure buccal and palatal ridge heights, (e) fusion superimposition of the initial and 6 months post‐operative scans, (f) 6 months postoperative scan.
2.9.2. Clinical Outcomes
2.9.2.1. Post‐Operative Patient Satisfaction
Patient satisfaction was assessed on the same day of extraction after the completion of the surgical procedures by asking the patients whether they were satisfied about the treatment provided, if they would do it again and whether they would recommend the treatment to others (Shirley and Sanders 2013).
2.9.2.2. Chair Time
Chair time was measured using a timer starting from injection of the local anaesthesia and ending at the completion of sutures in both groups (Ribeiro et al. 2011).
2.9.2.3. Keratinized Tissue (KT) Width
The measurement of KT width was carried out at baseline and 6 months post‐operatively (Hong et al. 2019). Measurements were taken at the vertical distance from a line connecting the two adjacent teeth at the CEJs to the free gingival margin (FGM) using an UNC 15 probe (Nordent Manufacturing Inc., IL, USA).
2.9.2.4. Pain Score
Pain was assessed at the suture removal appointment (Machtei et al. 2019), where the patients reported any pain along the previous 2 weeks after the completion of surgical procedures using a 0–10 visual analogue scale (VAS) in which 0 means no pain while 10 represents the worst pain possible (Santos et al. 2021).
2.9.3. Histological Analysis
Microscopic examination and histomorphometric analysis were conducted on four core biopsies obtained from four patients during implant placement (two from the ADDG + i‐PRF group and two from the ADDG group). A trephine bur with an outer diameter of 3.3 mm and an inner diameter of 2.8 mm (Helmut, Zepf Medizintechnik, Seitingen‐Oberflacht, Germany) was used to obtain bone biopsies prior to implant placement (Figure 2). The collected samples were preserved in 10% formalin solution, decalcified in 10% formic acid for a period of 10–15 days to be prepared for embedding in paraffin blocks, which were then sliced longitudinally into thin histological 5 μm sections. This was followed by staining the prepared histological sections with haematoxylin and eosin (H&E) stain to detect area of newly formed bone and also to inspect any inflammatory changes. Also, Masson's trichromatic (MT) stain was used in other sections for histological inspection and histomorphometric analysis of the quality of the newly formed bone (Figure 3). A Leica Digital Microscope (Leica Digital Microscope, Leica Microsystems, Wetzlar, Germany) was used for the microscopic examination of all histologically stained sections and photomicrographs of some prepared slides were captured. Photomicrographs were taken by Leica Application Suite program (Leica Microsystems, Heerbrugg, Switzerland) for capturing the histological sections examined under the microscope (Leica Microsystems, Heerbrugg, Switzerland). Histomorphometric analysis for all the prepared MT‐stained sections was performed using image analyser software (Leica QWin 500 image analysis software, Leica Microsystems, Heerbrugg, Switzerland). Areas of newly formed bone (as unmineralized (osteoid) bone or mineralized (osseous) bone), along with the remaining graft particles and soft fibrous tissue in marrow spaces were measured using a measuring frame with a surface area of 24,790 μm2. Five fields were carefully selected for each sample in each group (Ersanli, Olgac, and Leblebicioglu 2004) and examined at magnification of ×100. The mean percentages for each group were measured, calculated and recorded (Elfana et al. 2021).
FIGURE 3.
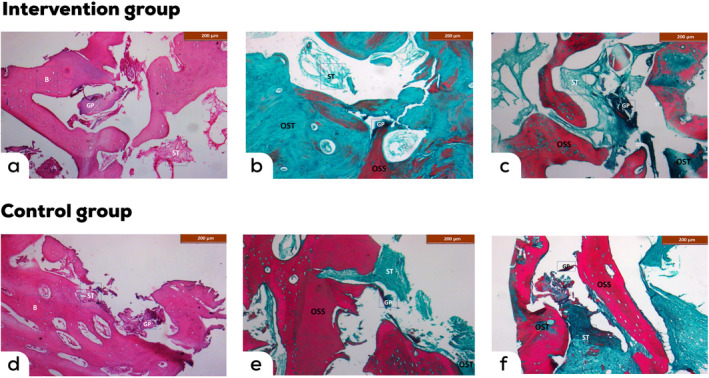
Qualitative histological examination. Representative microscopic images (100× magnification) with haematoxylin and eosin staining of histological sections of ADDG + i‐PRF (a) and ADDG (d) biopsies. Masson trichrome staining of histological sections of ADDG + i‐PRF (b, c) and ADDG (e, f) biopsies. B, newly formed bone; GP, graft particles; OSS, osseous tissue; OST, unmineralized osteoid tissue; ST, soft tissue.
2.10. Statistical Analysis
Data were explored for normality by checking the distribution of data and using tests of normality (Kolmogorov–Smirnov and Shapiro–Wilk tests). Age, buccolingual ridge width, ridge height and chair‐side time data showed normal (parametric) distribution while KTW, reduction in all parameters and pain scores data showed non‐normal (non‐parametric) distribution. Data were presented as mean, standard deviation (SD), median and range values. For parametric data, Student's t‐test was used to compare between mean age and chair‐side time values in the two groups. Two‐way repeated measures ANOVA test was used to compare between the two groups as well as to study the changes by time within each group. Bonferroni's post hoc test was used for pair‐wise comparisons when ANOVA test is significant. For non‐parametric data, Mann–Whitney U test was used to compare between the two groups. Wilcoxon‐signed rank test was used to study the changes by time within each group. Qualitative data were presented as frequencies and percentages. The significance level was set at p ≤ 0.05. Statistical analysis was performed with IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.
After performing the histomorphometric analysis and recording the mean and standard deviation values for the area percentage for each histological structure in each study group, statistical analysis was done using an independent t‐test.
The trial was conducted and reported in compliance with the CONSORT guidelines/checklist.
3. Results
3.1. Baseline Characteristics
The present study included a total of 24 participants who were recruited and treated between September 2022 and July 2023, among them, 22 completed their follow‐up (Figure S1). No adverse effects were observed and all participants exhibited complete soft tissue healing at follow‐up. The ADDG + i‐PRF group included six males and five females with mean age of 36.5 ± 10.8 years, while the ADDG group included four males and seven females with mean age of 34.5 ± 4.9 years. The ADDG + i‐PRF group included five incisors, one canine and five premolars, while in the ADDG group, two incisors, two canines and seven premolars were included (Table 1).
TABLE 1.
Descriptive statistics and results of chi‐square, Fisher's exact test and Student's t‐test for comparisons between baseline characteristics in the two groups.
| Baseline characteristics | ADDG + i‐PRF (n = 11) | ADDG (n = 11) |
|---|---|---|
| Gender (n, [%]) | ||
| Male | 6 (54.5%) | 4 (36.4%) |
| Female | 5 (45.5%) | 7 (63.6%) |
| Age [Mean, SD] | 36.5 (10.8) | 34.5 (4.9) |
| Tooth (n, [%]) | ||
| Incisors | 5 (45.5%) | 2 (18.2%) |
| Canine | 1 (9.1%) | 2 (18.2%) |
| Premolar | 5 (45.5%) | 7 (63.6%) |
Abbreviations: ADDG, autogenous demineralized dentin graft; i‐PRF, injectable platelet‐rich fibrin.
3.2. Radiographic Analysis
3.2.1. Bucco‐Palatal Ridge Width
A significant reduction in buccolingual ridge width and height between baseline and six months of follow‐up was notable up in both groups independently (p < 0.001). The mean buccolingual ridge width reduction at 1, 3 and 5 mm was 2.85 ± 2.12, 1.48 ± 0.92 and 0.81 ± 0.92 mm for the ADDG + i‐PRF group, respectively, while the ADDG group showed 2.88 ± 2.16, 1.76 ± 1.36 and 0.77 ± 0.81 mm respectively, with no differences between both groups (p > 0.05, Table 1). The overall width reduction was 1.71 ± 1.08 mm for the ADDG + i‐PRF group and 1.8 ± 1.35 mm for the ADDG group with no difference between the two groups (p > 0.05, Tables 2 and S1).
TABLE 2.
Descriptive statistics and results of Mann–Whitney U test for comparison between reductions in buccolingual ridge width and ridge height measurements (mm) in the two groups.
| Level | ADDG + i‐PRF (n = 11) | ADDG (n = 11) | p | Effect size (d) | ||
|---|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | |||
| 1 mm | 1.89 (1.07, 4.3) | 2.85 (2.12) | 2.79 (0.83, 4.26) | 2.88 (2.16) | 0.948 | 0.028 |
| 3 mm | 1.29 (1.09, 1.58) | 1.48 (0.92) | 1.87 (0.29, 2.73) | 1.76 (1.36) | 0.532 | 0.268 |
| 5 mm | 0.65 (0, 1.45) | 0.81 (0.92) | 0.93 (0, 1.27) | 0.77 (0.81) | 0.893 | 0.056 |
| Overall | 1.33 (0.84, 2.58) | 1.71 (1.08) | 2.03 (0.37, 3.06) | 1.8 (1.35) | 0.974 | 0.014 |
| Side | ADDG + i‐PRF (n = 11) | ADDG (n = 11) | p | Effect size (d) | ||
|---|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | |||
| Buccal | 1.32 (0.81, 1.97) | 1.33 (0.82) | 2.17 (1.37, 2.43) | 1.89 (0.89) | 0.101 | 0.747 |
| Lingual | 0.71 (0, 1.41) | 0.89 (0.98) | 1.6 (0.53, 2.81) | 1.7 (1.47) | 0.137 | 0.664 |
| Overall | 1.14 (0.41, 1.37) | 1.11 (0.67) | 1.69 (1.08, 2.86) | 1.8 (0.96) | 0.140 | 0.664 |
Abbreviations: ADDG, autogenous demineralized dentin graft; i‐PRF, injectable platelet‐rich fibrin.
3.2.2. Buccal and Palatal Ridge Height
Mean reduction in buccal and palatal ridge heights were 1.33 ± 0.82 and 0.89 ± 0.98 mm for in ADDG + i‐PRF group, and 1.89 ± 0.89 and 1.7 ± 0.47 mm in the ADDG group respectively, with no difference between both groups (p > 0.05, Table 2). The overall height reduction was 1.11 ± 0.76 mm for the ADDG + i‐PRF group and 1.8 ± 0.96 mm for the ADDG group with no difference between the two groups (p > 0.05, Tables 2 and S2).
3.3. Clinical Outcomes
3.3.1. KT Width
No significant reduction was notable in KT width between baseline and 6 months of follow‐up in the ADDG + i‐PRF group (p > 0.05), while for the ADDG group a significant reduction was evident (p = 0.005). A significant difference in the mean overall KT width after 6 months was further notable between ADDG + i‐PRF and ADDG groups (3.52 ± 1 and 2.33 ± 1.22 mm respectively, p = 0.017, Table 3). The mean overall reduction was significant between the two groups, with 0.12 ± 0.34 mm for the ADDG + i‐PRF and 0.58 ± 0.34 mm for the ADDG group (p = 0.008, Tables 3 and S3).
TABLE 3.
Descriptive statistics and results of Mann–Whitney U test for comparison between reductions in KTW measurements (mm) in the two groups.
| Site | ADDG + i‐PRF (n = 11) | ADDG (n = 11) | p | Effect size (d) | ||
|---|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | |||
| Mesial | 0 (0, 0) | 0.18 (0.4) | 0 (0, 1) | 0.45 (0.52) | 0.180 | 0.475 |
| Mid‐buccal | 0 (0, 0) | 0 (0.63) | 1 (0, 1) | 0.82 (0.6) | 0.008* | 1.211 |
| Distal | 0 (0, 0) | 0.18 (0.4) | 0 (0, 1) | 0.45 (0.52) | 0.180 | 0.475 |
| Overall | 0 (0, 0.33) | 0.12 (0.34) | 0.67 (0.33, 1) | 0.58 (0.34) | 0.008* | 1.303 |
Abbreviations: ADDG, autogenous demineralized dentin graft; i‐PRF, injectable platelet‐rich fibrin.
Significant at p ≤ 0.05.
3.3.2. Pain (VAS) Scores, Patient Satisfaction and Chair Time
Significantly lower pain scores were evident in the ADDG + i‐PRF compared to the ADDG group (p = 0.012, Table 4). All patients in the two groups were satisfied; thus, no statistical comparison was performed. Furthermore, no significant difference between chair times in the two groups was notable, with a mean of 68.6 ± 10.5 min and 66.4 ± 10.8 min for ADDG + i‐PRF and ADDG groups respectively (p > 0.05).
TABLE 4.
Descriptive statistics and results of Mann–Whitney U test for comparison between pain (VAS scores) in the two groups.
| ADDG + i‐PRF (n = 11) | ADDG (n = 11) | p | Effect size (d) | ||
|---|---|---|---|---|---|
| Median (IQR) | Mean (SD) | Median (IQR) | Mean (SD) | ||
| 2 (1, 3) | 2.18 (1.17) | 4 (3, 5) | 3.82 (1.33) | 0.012* | 1.234 |
Abbreviations: ADDG, autogenous demineralized dentin graft; i‐PRF, injectable platelet‐rich fibrin.
Significant at p ≤ 0.05.
3.4. Histological Evaluation and Histomorphometric Analysis
Regarding the H&E‐stained sections, areas of new bone formation without any inflammatory changes were observed surrounding the graft particles in both groups. On MT‐stained sections, soft unmineralized (osteoid) bone stained blue to green, while hard mineralized (osseous) bone was coloured pink to red. In the ADDG + i‐PRF group, the mean percentage area of mineralized osteoid tissue was 15.5%, mineralized osseous tissue was 33.8%, soft tissue part was 6.5%, and the remaining graft particles were 1.15%. While, for the ADDG group, the mean percentage area of unmineralized osteoid tissue was 10.7%, mineralized osseous tissue was 40.1%, soft tissue part was 14.4% and the remaining graft particles was 0.6%, with no significant differences between both groups (p > 0.05, Table 5).
TABLE 5.
Histomorphometric analysis of percentages of histological tissue for each group.
| Newly formed bone | Soft tissue part | Remaining graft particles | ||
|---|---|---|---|---|
| Unmineralized osteoid tissue | Mineralized osseous tissue | |||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| ADDG + i‐PRF | 15.5 (7.2) | 33.8 (5.9) | 6.5 (2.3) | 1.15 (1.2) |
| ADDG | 10.7 (9.2) | 40.1 (3.9) | 14.4 (7.6) | 0.6 (0.04) |
| p‐value | 0.5 | 0.2 | 0.2 | 0.5 |
Abbreviations: ADDG, autogenous demineralized dentin graft; i‐PRF, injectable platelet‐rich fibrin.
4. Discussion
ARP aims at reducing post‐extraction alveolar bone resorption (Bassir et al. 2018; Stumbras et al. 2019; Tan et al. 2012), thus preserving the dimensions of the alveolar ridge (Mardas et al. 2015; Willenbacher et al. 2016). The maxillary aesthetic region is commonly linked to a greater degree of horizontal and vertical post‐extraction bone resorption, since it possesses mostly a thin labial plate of bone (Chappuis et al. 2013; Couso‐Queiruga et al. 2021). In a recent case report (van Orten, Goetz, and Bilhan 2022), the combination of i‐PRF with autogenous dentin graft was suggested as a valuable alternative for obtaining vital and good quality bone structure in post‐extraction ARP. The aim of the present randomized controlled trial was to compare for the first time the combination of ADDG with i‐PRF versus ADDG alone in ARP of extraction sockets in the maxillary aesthetic region.
Atraumatic tooth extraction was carefully conducted for maximal hard and soft tissue preservation (Singla and Sharma 2020). A collagen sponge sealed all extraction sockets to prevent possible graft displacement or soft tissue downgrowth (Kim et al. 2011). In the current investigation, ADDG was used as it is a non‐antigenic and chair‐side autologous grafting material (Hazballa et al. 2021) for ARP, with studies demonstrating equivalence in its radiologic and histologic outcomes to bone grafts (Cenicante et al. 2021). Earlier findings demonstrated that the ADDG compared to the mineralized dentin form showed better graft remodelling, integration and osteoinductive properties histologically (Elfana et al. 2021). The demineralization process could expose a variety of growth factors contained in the dentin matrix, including IGF‐II, BMP‐2 and TGF‐β (Strauss et al. 2019). Additionally, the combination of i‐PRF with osseous grafting materials (Kyyak et al. 2020, 2021; Nagrani et al. 2023) enhances their handling characteristics forming a “sticky graft” (Miron, Fujioka‐Kobayashi, Bishara, et al. 2017; Miron, Fujioka‐Kobayashi, Hernandez, et al. 2017), in the current trial the “sticky ADDG.”
In line with the current findings, earlier investigations demonstrated the potential of ADDG in ARP (Elfana et al. 2021; Jung et al. 2018). Similar to studies evaluating the effects of autogenous demineralized tooth matrix with PRF membrane (Ouyyamwongs, Leepong, and Suttapreyasri 2019), freeze‐dried bone allograft (FDBA) with PRF (Azangookhiavi et al. 2020), or mineralized dentin graft with chopped PRF (Pohl, Binderman, and Tomac 2020), the current amalgamation of ADDG with i‐PRF yielded comparable results regarding ARP. It is noteworthy to report that all implants subsequently placed, whether in the control or intervention groups, did not need any additional augmentation, similar to previous findings (van Orten, Goetz, and Bilhan 2022).
No significant differences were observed between the ADDG + i‐PRF and the ADDG group regarding alveolar ridge dimensions, with similar patient satisfaction between groups. Furthermore, the i‐PRF preparation process, consisting of venous blood withdrawal followed by a 3‐min centrifugation protocol did not result in a significant difference regarding chair time of both treatments. Yet, in accordance with earlier studies demonstrating the potential of PRF to improve soft tissue healing (Ali and Selim 2018; De Angelis et al. 2019; Kızıltoprak and Uslu 2020), significantly higher KT conservation potential was observed in the ADDG + i‐PRF compared to the ADDG group 6 months following ARP. This could be attributed to the ability of PRF to stimulate the proliferation of dermal gingival fibroblasts and keratinocytes, and its involvement in the production of extracellular matrix components and collagen 1 (Miron, Fujioka‐Kobayashi, Bishara, et al. 2017; Miron, Fujioka‐Kobayashi, Hernandez, et al. 2017). Furthermore, The use of i‐PRF produces higher and sustained release TGF‐β, platelet‐derived growth factors (PDGF), and collagen‐1 molecules and a protection against proteolytic degradation of endogenous fibrogenic factors that are important in wound healing (Choukroun, Aalam, and Miron 2017).
Similarly, in agreement with earlier investigations, demonstrating the ability of PRF to reduce postoperative pain (De Angelis et al. 2019; Marenzi et al. 2015; Pan et al. 2019), in the present study significantly lower pain scores were evident in the ADDG + i‐PRF. These effects could be attributed to the ability of i‐PRF to create a three‐dimensional fibrin scaffold, which in addition to forming a haemostatic plug, enriches the healing site with a variety of cytokines and growth/differentiation factors, endorsing cellular migration, proliferation, angiogenesis, laying down of fibronectin and collagen‐I, tissue formation and epithelization (Bahar, Karakan, and Vurmaz 2024; Choukroun, Aalam, and Miron 2017; Davis et al. 2014; Locatelli et al. 2021; Schär et al. 2015; van Orten, Goetz, and Bilhan 2022). Compared to higher speed centrifugation protocols as employed in L‐PRF, the LSSC of i‐PRF further heightens the levels of these cytokines and growth/differentiation factors (Wend et al. 2017), augmenting its soft and hard tissues healing potentials (Pall et al. 2023; Reda et al. 2021). Additionally, i‐PRF harbours leukocytes and exerts anti‐microbial properties (Kour et al. 2018; Moojen et al. 2008).
Histological evaluations provide an advantage for detecting the quality of newly formed bone (either unmineralized or mineralized) as well as early immune responses surrounding graft particles prior to the appearance of clinical or radiographic evidence. Two weeks following grafting, osteoid tissues are formed and could persist for up to 6 months prior to complete mineralization (Aludden et al. 2020; Wortmann et al. 2020). Qualitatively, similar to earlier findings histological sections of the ADDG + i‐PRF (Alrmali et al. 2023; Andrade et al. 2020) and the ADDG (Elfana et al. 2021) groups demonstrated new bone formation with no inflammatory infiltrates, with a tendency for thicker bone trabeculae in the ADDG + i‐PRF group. In both groups, the ADDG particles seemed to be resorbed and encircled by osteoid tissues with vascularized bone marrow spaces, suggesting the active stage of new bone formation (Forni et al. 2013).
Yet, the present findings should be carefully interpreted within the current trial's limitations. First, as the study involved blood withdrawal for i‐PRF preparation, some patients refused to participate. Furthermore, the blood withdrawal procedure might have influenced the patient's perception and reporting of any postoperative pain in the test group. Secondly, although particles were ground to the clinically most possible size via bone rongeurs and mills, no standardization of the ADDG particle size was possible. Yet due to the subsequent demineralization process differences in mineralized ADDG particle sizes may have been relativized. Thirdly, although the study involved one single‐rooted teeth extraction sites per patient, the use of ADDG in ARP of multiple extraction sockets would have been restricted by its limited availability, relying on the presence of teeth indicated for extraction to provide the allogenic grafting material. Fourthly, generalizability of the findings is not ensured as the current investigation was conducted on single‐rooted teeth and excluded multirooted ones. Fifth, histological sections of higher quality could have provided a more profound base for drawing conclusions of the biological healing events. Finally, chairside preparation of ADDG required considerable time and effort.
5. Conclusions
Both ADDG + i‐PRF or ADDG alone provide effective grafting materials for ARP, with ADDG + i‐PRF possibly associated with easier graft handling, lower patient‐reported pain and enhanced keratinized tissue preservation upon healing. Further randomized clinical trials are needed, standardizing and testing various dentin graft particle sizes as well as ARP effects in molar extraction sockets.
Author Contributions
Odai Amer: conceptualization, methodology, writing – review and editing, investigation. Nesma Shemais: supervision, formal analysis, writing – review and editing, data curation, investigation. Karim Fawzy El‐Sayed: formal analysis, writing – original draft, writing – review and editing, validation. Heba Ahmed Saleh: formal analysis, data curation, writing – review and editing. Mona Darhous: supervision, project administration, writing – review and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Appendix S1.
Appendix S2.
Acknowledgements
The authors would like to thank the members of Periodontology Department Cairo University for their cooperation and help along the research.
Funding: The authors received no specific funding for this work.
Odai Amer, Nesma Shemais, and Karim Fawzy El‐Sayed contributed equally to the manuscript.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
- Abdulrahman, Y. A. , Hosny M. M., Elfana A., and Fawzy El‐Sayed K. M.. 2022. “Clinical and Radiographic Evaluation of Low‐Speed Platelet‐Rich Fibrin (PRF) for the Treatment of Intra‐Osseous Defects of Stage‐III Periodontitis Patients: A Randomized Controlled Clinical Trial.” Clinical Oral Investigations 26, no. 11: 6671–6680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al Qabbani, A. , Razak N. H. A., Al Kawas S., Hamid S. S. A., Wahbi S., and Samsudin A.. 2017. “The Efficacy of Immediate Implant Placement in Extraction Sockets for Alveolar Bone Preservation: A Clinical Evaluation Using Three‐Dimensional Cone Beam Computerized Tomography and Resonance Frequency Analysis Value.” Journal of Craniofacial Surgery 28, no. 4: e318–e325. [DOI] [PubMed] [Google Scholar]
- Alazzawi, A. , Ghazi M., and Jikia M.. 2018. “Complications During and After Extraction of Third Molar.” Caucasus Journal of Health Sciences and Public Health 2, no. 2: 28–31. [Google Scholar]
- Ali, S. , and Selim K.. 2018. “Bone and Soft Tissue Changes After Alveolar Ridge Preservation Using PRF Socket Plug Technique Versus Socket Plug Technique.” Egyptian Dental Journal 64: 3195–3208. [Google Scholar]
- Alrmali, A. , Saleh M. H., Mazzocco J., Zimmer J. M., Testori T., and Wang H. L.. 2023. “Auto‐Dentin Platelet‐Rich Fibrin Matrix Is an Alternative Biomaterial for Different Augmentation Procedures: A Retrospective Case Series Report.” Clinical and Experimental Dental Research 9, no. 6: 993–1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alshoiby, M. M. , Fawzy El‐Sayed K. M., Elbattawy W., and Hosny M. M.. 2023. “Injectable Platelet‐Rich Fibrin With Demineralized Freeze‐Dried Bone Allograft Compared to Demineralized Freeze‐Dried Bone Allograft in Intrabony Defects of Patients With Stage‐III Periodontitis: A Randomized Controlled Clinical Trial.” Clinical Oral Investigations 27, no. 7: 3457–3467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aludden, H. , Mordenfeld A., Dahlin C., Hallman M., and Starch‐Jensen T.. 2020. “Histological and Histomorphometrical Outcome After Lateral Guided Bone Regeneration Augmentation of the Mandible With Different Ratios of Deproteinized Bovine Bone Mineral and Autogenous Bone. A Preclinical In Vivo Study.” Clinical Oral Implants Research 31, no. 10: 1025–1036. [DOI] [PubMed] [Google Scholar]
- Andrade, C. , Camino J., Nally M., Quirynen M., Martínez B., and Pinto N.. 2020. “Combining Autologous Particulate Dentin, L‐PRF, and Fibrinogen to Create a Matrix for Predictable Ridge Preservation: A Pilot Clinical Study.” Clinical Oral Investigations 24: 1151–1160. [DOI] [PubMed] [Google Scholar]
- Avila, G. , Galindo‐Moreno P., Soehren S., Misch C. E., Morelli T., and Wang H. L.. 2009. “A Novel Decision‐Making Process for Tooth Retention or Extraction.” Journal of Periodontology 80, no. 3: 476–491. 10.1902/jop.2009.080454. [DOI] [PubMed] [Google Scholar]
- Azangookhiavi, H. , Ghodsi S., Jalil F., and Dadpour Y.. 2020. “Comparison of the Efficacy of Platelet‐Rich Fibrin and Bone Allograft for Alveolar Ridge Preservation After Tooth Extraction: A Clinical Trial.” Frontiers in Dentistry 17, no. 1: 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bahar, Ş. Ç. , Karakan N. C., and Vurmaz A.. 2024. “The Effects of Injectable Platelet‐Rich Fibrin Application on Wound Healing Following Gingivectomy and Gingivoplasty Operations: Single‐Blind, Randomized Controlled, Prospective Clinical Study.” Clinical Oral Investigations 28, no. 1: 85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bassir, S. H. , Alhareky M., Wangsrimongkol B., Jia Y., and Karimbux N.. 2018. “Systematic Review and Meta‐Analysis of Hard Tissue Outcomes of Alveolar Ridge Preservation.” International Journal of Oral and Maxillofacial Implants 33, no. 5: 979–994. [DOI] [PubMed] [Google Scholar]
- Ben Amara, H. , Kim J. J., Kim H. Y., Lee J., Song H. Y., and Koo K. T.. 2021. “Is Ridge Preservation Effective in the Extraction Sockets of Periodontally Compromised Teeth? A Randomized Controlled Trial.” Journal of Clinical Periodontology 48, no. 3: 464–477. [DOI] [PubMed] [Google Scholar]
- Bertoldi, C. , Generali L., Cortellini P., et al. 2021. “Influence of Tooth‐Brushing on Early Healing After Access Flap Surgery: A Randomized Controlled Preliminary Study.” Materials 14, no. 11: 2933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyapati, L. , and Wang H.‐L.. 2006. “The Role of Platelet‐Rich Plasma in Sinus Augmentation: A Critical Review.” Implant Dentistry 15, no. 2: 160–170. [DOI] [PubMed] [Google Scholar]
- Braut, V. , Bornstein M. M., Belser U., and Buser D.. 2011. “Thickness of the Anterior Maxillary Facial Bone Wall‐A Retrospective Radiographic Study Using Cone Beam Computed Tomography.” International Journal of Periodontics and Restorative Dentistry 31, no. 2: 125–131. [PubMed] [Google Scholar]
- Cenicante, J. , Botelho J., Machado V., et al. 2021. “The Use of Autogenous Teeth for Alveolar Ridge Preservation: A Literature Review.” Applied Sciences 11, no. 4: 1853. [Google Scholar]
- Chappuis, V. , Engel O., Reyes M., Shahim K., Nolte L. P., and Buser D.. 2013. “Ridge Alterations Post‐Extraction in the Esthetic Zone: A 3D Analysis With CBCT.” Journal of Dental Research 92, no. 12 Suppl: 195S–201S. 10.1177/0022034513506713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choukroun, J. , Aalam A. A., and Miron R. J.. 2017. “Platelet Rich Fibrin “PRF” and Regenerative Medicine:‘The Low‐Speed Concept’.” In MSCs and Innovative Biomaterials in Dentistry, 21–42. Cham: Springer. [Google Scholar]
- Choukroun, J. , and Ghanaati S.. 2018. “Reduction of Relative Centrifugation Force Within Injectable Platelet‐Rich‐Fibrin (PRF) Concentrates Advances patients' Own Inflammatory Cells, Platelets and Growth Factors: The First Introduction to the Low Speed Centrifugation Concept.” European Journal of Trauma and Emergency Surgery 44: 87–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corning, P. J. , and Mealey B. L.. 2019. “Ridge Preservation Following Tooth Extraction Using Mineralized Freeze‐Dried Bone Allograft Compared to Mineralized Solvent‐Dehydrated Bone Allograft: A Randomized Controlled Clinical Trial.” Journal of Periodontology 90, no. 2: 126–133. [DOI] [PubMed] [Google Scholar]
- Couso‐Queiruga, E. , Stuhr S., Tattan M., Chambrone L., and Avila‐Ortiz G.. 2021. “Post‐Extraction Dimensional Changes: A Systematic Review and Meta‐Analysis.” Journal of Clinical Periodontology 48, no. 1: 127–145. [DOI] [PubMed] [Google Scholar]
- Davis, V. L. , Abukabda A. B., Radio N. M., et al. 2014. “Platelet‐Rich Preparations to Improve Healing. Part II: Platelet Activation and Enrichment, Leukocyte Inclusion, and Other Selection Criteria.” Journal of Oral Implantology 40, no. 4: 511–521. 10.1563/aaid-joi-d-12-00106. [DOI] [PubMed] [Google Scholar]
- De Angelis, P. , De Angelis S., Passarelli P. C., Liguori M. G., Manicone P. F., and D'Addona A.. 2019. “Hard and Soft Tissue Evaluation of Different Socket Preservation Procedures Using Leukocyte and Platelet‐Rich Fibrin: A Retrospective Clinical and Volumetric Analysis.” Journal of Oral and Maxillofacial Surgery 77, no. 9: 1807–1815. [DOI] [PubMed] [Google Scholar]
- Demetter, R. S. , Calahan B. G., and Mealey B. L.. 2017. “Histologic Evaluation of Wound Healing After Ridge Preservation With Cortical, Cancellous, and Combined Cortico‐Cancellous Freeze‐Dried Bone Allograft: A Randomized Controlled Clinical Trial.” Journal of Periodontology 88, no. 9: 860–868. [DOI] [PubMed] [Google Scholar]
- Dohan, D. M. , Choukroun J., Diss A., et al. 2006. “Platelet‐Rich Fibrin (PRF): A Second‐Generation Platelet Concentrate. Part II: Platelet‐Related Biologic Features.” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 101, no. 3: e45–e50. [DOI] [PubMed] [Google Scholar]
- dos Santos Canellas, J. V. , da Costa R. C., Breves R. C., et al. 2020. “Tomographic and Histomorphometric Evaluation of Socket Healing After Tooth Extraction Using Leukocyte‐and Platelet‐Rich Fibrin: A Randomized, Single‐Blind, Controlled Clinical Trial.” Journal of Cranio‐Maxillofacial Surgery 48, no. 1: 24–32. [DOI] [PubMed] [Google Scholar]
- Elbehwashy, M. T. , Hosny M. M., Elfana A., Nawar A., and Fawzy El‐Sayed K.. 2021. “Clinical and Radiographic Effects of Ascorbic Acid‐Augmented Platelet‐Rich Fibrin Versus Platelet‐Rich Fibrin Alone in Intra‐Osseous Defects of Stage‐III Periodontitis Patients: A Randomized Controlled Clinical Trial.” Clinical Oral Investigations 25: 6309–6319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elfana, A. , El‐Kholy S., Saleh H. A., and Fawzy El‐Sayed K.. 2021. “Alveolar Ridge Preservation Using Autogenous Whole‐Tooth Versus Demineralized Dentin Grafts: A Randomized Controlled Clinical Trial.” Clinical Oral Implants Research 32, no. 5: 539–548. [DOI] [PubMed] [Google Scholar]
- Ersanli, S. , Olgac V., and Leblebicioglu B.. 2004. “Histologic Analysis of Alveolar Bone Following Guided Bone Regeneration.” Journal of Periodontology 75, no. 5: 750–756. [DOI] [PubMed] [Google Scholar]
- Fettouh, A. I. A. , Ghallab N. A., Ghaffar K. A., et al. 2023. “Bone Dimensional Changes After Flapless Immediate Implant Placement With and Without Bone Grafting: Randomized Clinical Trial.” Clinical Implant Dentistry and Related Research 25, no. 2: 271–283. [DOI] [PubMed] [Google Scholar]
- Forni, F. , Marzagalli M., Tesei P., and Grassi A.. 2013. “Platelet Gel: Applications in Dental Regenerative Surgery.” Blood Transfusion 11, no. 1: 102–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harnack, L. , Boedeker R., Kurtulus I., Boehm S., Gonzales J., and Meyle J.. 2009. “Use of Platelet‐Rich Plasma in Periodontal Surgery—A Prospective Randomised Double Blind Clinical Trial.” Clinical Oral Investigations 13: 179–187. [DOI] [PubMed] [Google Scholar]
- Hazballa, D. , Inchingolo A., Inchingolo A., et al. 2021. “The Effectiveness of Autologous Demineralized Tooth Graft for the Bone Ridge Preservation: A Systematic Review of the Literature.” Journal of Biological Regulators and Homeostatic Agents 35, no. Suppl. S1: 283–294. [DOI] [PubMed] [Google Scholar]
- Heimes, D. , Schiegnitz E., Kuchen R., Kämmerer P. W., and Al‐Nawas B.. 2021. “Buccal Bone Thickness in Anterior and Posterior Teeth—A Systematic Review.” Healthcare 9: 1663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hong, H. R. , Chen C. Y., Kim D. M., and Machtei E. E.. 2019. “Ridge Preservation Procedures Revisited: A Randomized Controlled Trial to Evaluate Dimensional Changes With Two Different Surgical Protocols.” Journal of Periodontology 90, no. 4: 331–338. [DOI] [PubMed] [Google Scholar]
- Horváth, A. , Mardas N., Mezzomo L. A., Needleman I. G., and Donos N.. 2013. “Alveolar Ridge Preservation. A Systematic Review.” Clinical Oral Investigations 17, no. 2: 341–363. 10.1007/s00784-012-0758-5. [DOI] [PubMed] [Google Scholar]
- Jung, G.‐U. , Jeon T.‐H., Kang M.‐H., et al. 2018. “Volumetric, Radiographic, and Histologic Analyses of Demineralized Dentin Matrix Combined With Recombinant Human Bone Morphogenetic Protein‐2 for Ridge Preservation: A Prospective Randomized Controlled Trial in Comparison With Xenograft.” Applied Sciences 8, no. 8: 1288. [Google Scholar]
- Jung, R. E. , Philipp A., Annen B. M., et al. 2013. “Radiographic Evaluation of Different Techniques for Ridge Preservation After Tooth Extraction: A Randomized Controlled Clinical Trial.” Journal of Clinical Periodontology 40, no. 1: 90–98. 10.1111/jcpe.12027. [DOI] [PubMed] [Google Scholar]
- Kim, E. S. 2015. “Autogenous Fresh Demineralized Tooth Graft Prepared at Chairside for Dental Implant.” Maxillofacial Plastic and Reconstructive Surgery 37, no. 1: 8. 10.1186/s40902-015-0009-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, J.‐J. , Amara H. B., Chung I., and Koo K.‐T.. 2021. “Compromised Extraction Sockets: A New Classification and Prevalence Involving Both Soft and Hard Tissue Loss.” Journal of Periodontal & Implant Science 51, no. 2: 100–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, Y. K. , Lee J., Um I. W., et al. 2013. “Tooth‐Derived Bone Graft Material.” Journal of the Korean Association of Oral and Maxillofacial Surgeons 39, no. 3: 103–111. 10.5125/jkaoms.2013.39.3.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, Y.‐K. , Yun P.‐Y., Lee H.‐J., Ahn J.‐Y., and Kim S.‐G.. 2011. “Ridge Preservation of the Molar Extraction Socket Using Collagen Sponge and Xenogeneic Bone Grafts.” Implant Dentistry 20, no. 4: 267–272. 10.1097/ID.0b013e3182166afc. [DOI] [PubMed] [Google Scholar]
- Kızıltoprak, M. , and Uslu M. Ö.. 2020. “Comparison of the Effects of Injectable Platelet‐Rich Fibrin and Autologous Fibrin Glue Applications on Palatal Wound Healing: A Randomized Controlled Clinical Trial.” Clinical Oral Investigations 24: 4549–4561. [DOI] [PubMed] [Google Scholar]
- Kour, P. , Pudakalkatti P. S., Vas A. M., Das S., and Padmanabhan S.. 2018. “Comparative Evaluation of Antimicrobial Efficacy of Platelet‐Rich Plasma, Platelet‐Rich Fibrin, and Injectable Platelet‐Rich Fibrin on the Standard Strains of Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans .” Contemporary Clinical Dentistry 9, no. Suppl 2: S325–S330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kyyak, S. , Blatt S., Pabst A., Thiem D., Al‐Nawas B., and Kämmerer P. W.. 2020. “Combination of an Allogenic and a Xenogenic Bone Substitute Material With Injectable Platelet‐Rich Fibrin–A Comparative In Vitro Study.” Journal of Biomaterials Applications 35, no. 1: 83–96. [DOI] [PubMed] [Google Scholar]
- Kyyak, S. , Blatt S., Schiegnitz E., et al. 2021. “Activation of Human Osteoblasts via Different Bovine Bone Substitute Materials With and Without Injectable Platelet Rich Fibrin In Vitro.” Frontiers in Bioengineering and Biotechnology 9: 599224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Locatelli, L. , Colciago A., Castiglioni S., and Maier J. A.. 2021. “Platelets in Wound Healing: What Happens in Space?” Frontiers in Bioengineering and Biotechnology 9: 716184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Machtei, E. E. , Mayer Y., Horwitz J., and Zigdon‐Giladi H.. 2019. “Prospective Randomized Controlled Clinical Trial to Compare Hard Tissue Changes Following Socket Preservation Using Alloplasts, Xenografts vs no Grafting: Clinical and Histological Findings.” Clinical Implant Dentistry and Related Research 21, no. 1: 14–20. [DOI] [PubMed] [Google Scholar]
- Mani, A. , Mani S., Sachdeva S., Sodhi J. K., Vora H. R., and Gholap S.. 2021. “Post‐Surgical Care in Surgical Periodontics.” International Journal of Periodontology and Implantology 6: 74–78. [Google Scholar]
- Mardas, N. , Macbeth N., Donos N., Jung R. E., and Zuercher A. N.. 2023. “Is Alveolar Ridge Preservation an Overtreatment?” Periodontology 2000 93: 289–308. [DOI] [PubMed] [Google Scholar]
- Mardas, N. , Trullenque‐Eriksson A., MacBeth N., Petrie A., and Donos N.. 2015. “Does Ridge Preservation Following Tooth Extraction Improve Implant Treatment Outcomes: A Systematic Review: Group 4: Therapeutic Concepts & Methods.” Clinical Oral Implants Research 26: 180–201. [DOI] [PubMed] [Google Scholar]
- Marenzi, G. , Riccitiello F., Tia M., di Lauro A., and Sammartino G.. 2015. “Influence of Leukocyte‐and Platelet‐Rich Fibrin (L‐PRF) in the Healing of Simple Postextraction Sockets: A Split‐Mouth Study.” BioMed Research International 2015: 369273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Melek, L. , and Marwan E. S.. 2016. “Evaluation of “Autogenous Bioengineered Injectable PRF – Tooth graft” Combination (ABIT) in Reconstruction of Maxillary Alveolar Ridge Defects: CBCT Volumetric Analysis.” Saudi Journal for Dental Research 8: 86–96. [Google Scholar]
- Miron, R. J. , Fujioka‐Kobayashi M., Bishara M., Zhang Y., Hernandez M., and Choukroun J.. 2017. “Platelet‐Rich Fibrin and Soft Tissue Wound Healing: A Systematic Review.” Tissue Engineering Part B: Reviews 23, no. 1: 83–99. [DOI] [PubMed] [Google Scholar]
- Miron, R. J. , Fujioka‐Kobayashi M., Hernandez M., et al. 2017. “Injectable Platelet Rich Fibrin (i‐PRF): Opportunities in Regenerative Dentistry?” Clinical Oral Investigations 21, no. 8: 2619–2627. 10.1007/s00784-017-2063-9. [DOI] [PubMed] [Google Scholar]
- Miron, R. J. , Gruber R., Farshidfar N., Sculean A., and Zhang Y.. 2023. “Ten Years of Injectable Platelet‐Rich Fibrin.” Periodontology 2000 94, no. 1: 92–113. [DOI] [PubMed] [Google Scholar]
- Miron, R. J. , and Zhang Y.. 2018. “Autologous Liquid Platelet Rich Fibrin: A Novel Drug Delivery System.” Acta Biomaterialia 75: 35–51. [DOI] [PubMed] [Google Scholar]
- Moojen, D. J. F. , Everts P. A., Schure R. M., et al. 2008. “Antimicrobial Activity of Platelet‐Leukocyte Gel Against Staphylococcus aureus .” Journal of Orthopaedic Research 26, no. 3: 404–410. [DOI] [PubMed] [Google Scholar]
- Nagrani, T. , Kumar S., Haq M. A., et al. 2023. “Use of Injectable Platelet‐Rich Fibrin Accompanied by Bone Graft in Socket Endurance: A Radiographic and Histological Study.” Cureus 15, no. 10: e46909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ouyyamwongs, W. , Leepong N., and Suttapreyasri S.. 2019. “Alveolar Ridge Preservation Using Autologous Demineralized Tooth Matrix and Platelet‐Rich Fibrin Versus Platelet‐Rich Fibrin Alone: A Split‐Mouth Randomized Controlled Clinical Trial.” Implant Dentistry 28, no. 5: 455–462. [DOI] [PubMed] [Google Scholar]
- Pall, E. , Roman A., Olah D., Beteg F. I., Cenariu M., and Spînu M.. 2023. “Enhanced Bioactive Potential of Functionalized Injectable Platelet‐Rich Plasma.” Molecules 28, no. 4: 1943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pan, J. , Xu Q., Hou J., et al. 2019. “Effect of Platelet‐Rich Fibrin on Alveolar Ridge Preservation: A Systematic Review.” Journal of the American Dental Association 150, no. 9: 766–778. [DOI] [PubMed] [Google Scholar]
- Park, M. , Mah Y.‐J., Kim D.‐H., Kim E.‐S., and Park E.‐J.. 2015. “Demineralized Deciduous Tooth as a Source of Bone Graft Material: Its Biological and Physicochemical Characteristics.” Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 120, no. 3: 307–314. [DOI] [PubMed] [Google Scholar]
- Pohl, S. , Binderman I., and Tomac J.. 2020. “Maintenance of Alveolar Ridge Dimensions Utilizing an Extracted Tooth Dentin Particulate Autograft and Platelet‐Rich Fibrin: A Retrospective Radiographic Cone‐Beam Computed Tomography Study.” Materials 13, no. 5: 1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reda, R. M. , Gawish A., Shafik M., and Ghoniem M.. 2021. “Evaluation of Injectable Platelet Rich Fibrin (I‐PRF) With Bone Graft Around Immediate Dental Implant in Esthetic Zone.” Al‐Azhar Dental Journal for Girls 8, no. 3‐B: 471–482. [Google Scholar]
- Ribeiro, F. V. , Casarin R. C., Palma M. A., Júnior F. H., Sallum E. A., and Casati M. Z.. 2011. “Clinical and Patient‐Centered Outcomes After Minimally Invasive Non‐surgical or Surgical Approaches for the Treatment of Intrabony Defects: A Randomized Clinical Trial.” Journal of Periodontology 82, no. 9: 1256–1266. [DOI] [PubMed] [Google Scholar]
- Santos, A. , Botelho J., Machado V., et al. 2021. “Autogenous Mineralized Dentin Versus Xenograft Granules in Ridge Preservation for Delayed Implantation in Post‐Extraction Sites: A Randomized Controlled Clinical Trial With an 18 Months Follow‐Up.” Clinical Oral Implants Research 32, no. 8: 905–915. [DOI] [PubMed] [Google Scholar]
- Sanz, M. , Donos N., Alcoforado G., et al. 2015. “Therapeutic Concepts and Methods for Improving Dental Implant Outcomes. Summary and Consensus Statements. The 4th EAO Consensus Conference 2015.” Clinical Oral Implants Research 26: 202–206. [DOI] [PubMed] [Google Scholar]
- Schär, M. O. , Diaz‐Romero J., Kohl S., Zumstein M. A., and Nesic D.. 2015. “Platelet‐Rich Concentrates Differentially Release Growth Factors and Induce Cell Migration In Vitro.” Clinical Orthopaedics and Related Research 473, no. 5: 1635–1643. 10.1007/s11999-015-4192-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt‐Schultz, T. H. , and Schultz M.. 2005. “Intact Growth Factors Are Conserved in the Extracellular Matrix of Ancient Human Bone and Teeth: A Storehouse for the Study of Human Evolution in Health and Disease.” Biological Chemistry 386, no. 8: 767–776. 10.1515/bc.2005.090. [DOI] [PubMed] [Google Scholar]
- Shirley, E. D. , and Sanders J. O.. 2013. “Patient Satisfaction: Implications and Predictors of Success.” Journal of Bone and Joint Surgery 95, no. 10: e69. [DOI] [PubMed] [Google Scholar]
- Singla, D. , and Sharma D.. 2020. “Latest Trends in Atraumatic Extraction of Teeth.” International Journal of Applied Dental Sciences 6: 361–366. 10.22271/oral.2020.v6.i4f.1088. [DOI] [Google Scholar]
- Steigmann, L. , Di Gianfilippo R., Steigmann M., and Wang H.‐L.. 2022. “Classification Based on Extraction Socket Buccal Bone Morphology and Related Treatment Decision Tree.” Materials 15, no. 3: 733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauss, F. J. , Di Summa F., Stähli A., et al. 2019. “TGF‐β Activity in Acid Bone Lysate Adsorbs to Titanium Surface.” Clinical Implant Dentistry and Related Research 21, no. 2: 336–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stumbras, A. , Januzis G., Gervickas A., Kubilius R., and Juodzbalys G.. 2020. “Randomized and Controlled Clinical Trial of Bone Healing After Alveolar Ridge Preservation Using Xenografts and Allografts Versus Plasma Rich in Growth Factors.” Journal of Oral Implantology 46, no. 5: 515–525. [DOI] [PubMed] [Google Scholar]
- Stumbras, A. , Kuliesius P., Januzis G., and Juodzbalys G.. 2019. “Alveolar Ridge Preservation After Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet Concentrates: A Systematic Review.” Journal of Oral and Maxillofacial Research 10, no. 1: e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tan, W. L. , Wong T. L., Wong M. C., and Lang N. P.. 2012. “A Systematic Review of Post‐Extractional Alveolar Hard and Soft Tissue Dimensional Changes in Humans.” Clinical Oral Implants Research 23, no. Suppl 5: 1–21. 10.1111/j.1600-0501.2011.02375.x. [DOI] [PubMed] [Google Scholar]
- Um, I. W. , Kim Y. K., and Mitsugi M.. 2017. “Demineralized Dentin Matrix Scaffolds for Alveolar Bone Engineering.” Journal of Indian Prosthodontic Society 17, no. 2: 120–127. 10.4103/jips.jips_62_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van der Weijden, F. , Dell'Acqua F., and Slot D. E.. 2009. “Alveolar Bone Dimensional Changes of Post‐Extraction Sockets in Humans: A Systematic Review.” Journal of Clinical Periodontology 36, no. 12: 1048–1058. 10.1111/j.1600-051X.2009.01482.x. [DOI] [PubMed] [Google Scholar]
- van Orten, A. , Goetz W., and Bilhan H.. 2022. “Tooth‐Derived Granules in Combination With Platelet‐Rich Fibrin (“Sticky Tooth”) in Socket Preservation: A Histological Evaluation.” Dentistry Journal 10, no. 2: 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wend, S. , Kubesch A., Orlowska A., et al. 2017. “Reduction of the Relative Centrifugal Force Influences Cell Number and Growth Factor Release Within Injectable PRF‐Based Matrices.” Journal of Materials Science. Materials in Medicine 28, no. 12: 188. 10.1007/s10856-017-5992-6. [DOI] [PubMed] [Google Scholar]
- Willenbacher, M. , Al‐Nawas B., Berres M., Kämmerer P. W., and Schiegnitz E.. 2016. “The Effects of Alveolar Ridge Preservation: A Meta‐Analysis.” Clinical Implant Dentistry and Related Research 18, no. 6: 1248–1268. [DOI] [PubMed] [Google Scholar]
- Wortmann, D. E. , Klein‐Nulend J., van Ruijven L. J., Vissink A., Raghoebar G. M., and Schortinghuis J.. 2020. “Histomorphometric and Micro‐CT Analyses of Calvarial Bone Grafts Used to Reconstruct the Extremely Atrophied Maxilla.” Clinical Implant Dentistry and Related Research 22, no. 5: 593–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang, F. , Ruan Y., Bai X., et al. 2023. “Alveolar Ridge Preservation in Sockets With Severe Periodontal Destruction Using Autogenous Partially Demineralized Dentin Matrix: A Randomized Controlled Clinical Trial.” Clinical Implant Dentistry and Related Research 25, no. 6: 1019–1032. [DOI] [PubMed] [Google Scholar]
- Yusri, S. , Elbattawy W., Zaaya S., Mokhtar M., Ramzy A., and Fawzy El‐Sayed K. M.. 2024. “Modified Minimally Invasive Surgical Technique With Clindamycin‐Augmented or Non‐Augmented Platelet‐Rich Fibrin in Periodontal Regeneration: A Randomized Clinical Trial.” Journal of Periodontal Research. Published ahead of print, September 3, 2024. 10.1111/jre.13344. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1.
Appendix S2.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.