

Abstract
Background
Virtual reality (VR) has promise as an innovative nonpharmacologic treatment for improving a patient’s quality of life. VR can be used as an adjunct or treatment for many acute and chronic conditions, including serious illnesses.
Objective
This systematic review aims to assess the current state of the literature of randomized controlled trials that use VR in patients with serious illnesses. Two secondary aims include assessing intervention components associated with improved quality of life and functional outcomes among older adults, as well as evaluating how well the randomized controlled trials adhere to consensus standards for VR research.
Methods
We searched PubMed, Embase, and CINAHL for randomized controlled studies published at any time. We screened and accepted studies that reported outcomes related to patients’ quality of life, provided an immersive VR intervention, and included patients with serious illness. We narratively summarized key attributes of publications that shed light on study efficacy, generalizability, replicability, and clinical utility. All studies were assessed for study quality with the Cochrane Risk of Bias tool and for concordance with 8 recent consensus standards for VR research.
Results
From the 12,621 articles searched in May 2024, a total of 24 (0.19%) studies met the inclusion criteria, and of these, 88% (21/24) reported an improvement in at least 1 patient quality of life outcome and 67% (16/24) had a high risk of bias. In 7 (n=24, 29%) studies, VR was used to provide distraction therapy to reduce pain. In total, 5 (n=24, 21%) studies included training, supervision, and assistance in VR use, which demonstrated improvements in patient quality of life–related outcomes. Of 24 studies, 9 (38%) included patients with stroke, 9 (38%) included patients with cancer, 4 (17%) included patients with cardiovascular disease, 1 (4%) included patients with chronic obstructive pulmonary disease, and 1 (4%) included patients who reported pain in hospital. In all 9 studies that included patients with stroke, the main purpose of VR was to improve mobility and strength; these studies had higher frequency and longer durations of VR use, ranging from 2 to 9 weeks, as compared to a VR use duration of <2 weeks for studies aiming to reduce pain or anxiety. Regarding consensus standards for VR research, 29% (7/24) of the studies adhered to all 8 criteria, and all studies (24/24, 100%) adhered to ≥5 criteria.
Conclusions
Nascent evidence suggests VR’s potential in mitigating pain, anxiety, and depression and improving mobility among persons with serious illnesses. Most studies did not provide detailed information about unassisted or assisted use, suggesting that VR for older adults is currently most appropriate for observed settings with assistance available.
Trial Registration
PROSPERO CRD42022346178; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=346178
Keywords: virtual reality, serious illness, pain, anxiety, older adults, patient outcomes, systematic review, palliative care, hospice
Introduction
Background
More than 60% of Americans will face a period of significant disability before death, incurring a diminished quality of life from the impact of serious illness, including multimorbidity [1-3]. Serious illness is defined as a health condition with a high risk of mortality that either negatively impacts daily function or quality of life or strains a person’s caregivers [4]. Serious illnesses include those of indeterminate but limited prognosis and those that have a detrimental effect on the quality of life of patients and their caregivers. They encompass malignancy, organ failure, or frailty, a complex state of vulnerability that is often associated with dementia [4,5]. Serious illnesses are associated with burdensome symptoms and functional decline and include many leading causes of death, such as stroke, as well as multimorbidity [6]. Patients also face a significant financial burden because of medical treatment [7]. These conditions interfere with a person’s ability to engage in activities they once enjoyed and impose emotional and physical burdens on family members and other caregivers; these conditions are of growing importance with the population aging [4].
Functional outcomes are a useful adjunct to other quality of life–relevant measures to understand the impact of serious illness on a person’s life [8]. Activities of daily living (ADLs) include basic functions such as dressing, maintaining personal cleanliness, toileting, transferring, and eating. The impairment of 1 to 2 ADLs occurs in most Americans during the years before death, and ≥3 ADL impairments are associated with institutionalization. Important goals for patients include dying at home and maintaining cleanliness, both of which are abetted by functional status or require dedicated caregiving if adequate support is unavailable [9]. Evaluating functional outcomes in patients with serious illness is especially important because it directly reflects their quality of life and their ability to perform ADLs [10].
Virtual reality (VR) is one among emerging interventions (eg, smart technologies) with the potential to improve a patient’s quality of life, patient-reported outcomes, psychological outcomes, and functional outcomes for persons living with serious illness [11-14]. VR offers a computer-generated, stereoscopically rendered, 3D visual environment, often with complementary sound, which responds continuously to a patient’s movement. Immersive VR creates a psychological experience of treating the virtual simulation as a real experience. The sensory experience is thus distinct from nonimmersive reality, such as augmented reality that allows the participant to see computer-generated images superimposed on the real-world visual field [15,16]. Immersion and distraction therapies have been shown to be helpful in improving quality of life and functional outcomes. The use of VR in health care for serious illness care has been expanding to address pain, anxiety, and other needs in palliative care and hospice settings [17,18]. There is a need to understand the quality of research and VR’s efficacy, especially in randomized controlled trials (RCTs), as it applies to older, seriously ill adults.
Objectives
Several recent reviews have explored content salient to our interest, although not in the specific context of applying VR to palliative care and serious illness [19-21]. We aim to determine the extent to which rigorous studies have focused on the rapidly growing population of older adults, the quality of that research, the extent to which it adheres to recently accepted VR research standards, and the characteristics of that research (eg, common outcomes) [22-24]. Two secondary aims include assessing the components of interventions in RCTs associated with improved quality of life and functional outcomes, as well as assessing the extent to which the current RCTs related to VR adhere to recommended consensus standards for high-quality VR research.
Methods
Protocol and Registration
Our review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) protocols statement and Enhancing the Quality and Transparency of Health Research guidelines [25,26]. We registered our protocol to the PROSPERO (CRD42022346178) [27].
Eligibility Criteria
Included in this systematic review are studies published in peer-reviewed journals up through May 2024 that meet the following criteria organized by population, intervention, comparator, outcomes, timing, and setting framework (Textbox 1) [28]. Functional outcomes include patient-reported outcomes relating to the quality of life and patient-demonstrated outcomes (eg, arm curl, chair stand, back scratch, chair sit, reach, walk test, overall cognition, and memory) [29,30]. Biological intermediaries (eg, functional magnetic resonance imaging scans, cortisol levels, blood test values, and balance) that do not directly demonstrate patient function are not included as patient functional outcomes [31]. Eligibility criteria are described using the population, intervention, comparator, outcomes, timing, and setting framework (Textbox 1).
Eligibility criteria using the population, intervention, comparator, outcomes, timing, and setting framework.
Population
Inclusion criteria: studies that include adult patients (aged ≥18 years) with serious illness, such as stroke, defined by a variable but limited prognosis and an important illness impact quality of life
Exclusion criteria: studies that include pediatric or adolescent patients (aged ≤18 years) or patients without serious illness
Intervention
Inclusion criteria: study participants must use some form of immersive virtual reality in the intervention arm.
-
Exclusion criteria
Intervention description insufficient to describe immersiveness
Augmented or extended reality (ie, nonimmersive reality)
2D screens (eg, Wii and Wii Fit [Nintendo], Xbox [Microsoft Gaming], and YouGrabber)
Comparator
Usual care
Outcomes
Inclusion criteria: patient quality of life–related outcomes, including patient-reported (eg, pain and anxiety) or patient-demonstrated (eg, arm curl, chair stand, back scratch, chair sit, reach, walk test, overall cognition, and memory) outcomes
Exclusion criteria: only biological intermediaries reported as results (eg, functional magnetic resonance imaging scans, cortisol levels, blood test values, and balance)
Timing: interventions with any follow-up period
Setting: any care setting (including in-patient clinics or outpatient and ambulatory care)
Selection of Sources for Evidence
Concepts included in the literature search were RCTs, VR, and serious illness as shown in Multimedia Appendix 1. We searched PubMed, Embase, and CINAHL for studies published at any time and identified 12,814 articles (n=10,799, 84.28% articles after duplicates were removed). During the title and abstract screening and full-text screening phases, 3 coauthor reviewers screened each study and were blinded to each other’s decisions (BM, AK, and SF). During the title and abstract screening, we resolved conflicts predominantly by a “gold standard” reviewer (KL or KG), occasionally by majority consensus. During the full-text screening, reasons for exclusion were identified. Only the gold standard reviewer (KL or KG) resolved conflicts during full-text screening. During full-text screening, if any systematic reviews met inclusion criteria, we added their included articles to the title and abstract screening phase. We used the Covidence (Veritas Health Innovation) software to generate a PRISMA diagram to track studies at each stage of the review (Multimedia Appendix 2 [25]) [32].
Data Extraction
We built an abstraction form through an iterative process (Multimedia Appendix 3). All aspects of the included article interventions were recorded, including what the intervention entailed; the type of VR and media (eg, type of scenery or activity) used; any training, supervision, or assistance provided during VR use; the duration of sessions; frequency of sessions; and duration of intervention. The main outcomes collected were related to patient quality of life–related outcomes. Data abstraction for the included studies was done through Covidence with 2 reviewers per article. Two reviewers (BM, AK, or NI) abstracted each article independently and resolved all abstraction conflicts through a consensus discussion.
Risk of Bias and Quality Assessment
Risk assessment for bias was done using the Cochrane Risk of Bias tool for RCTs [33]. Two reviewers (SF, AK, or BM) independently assessed the risk of bias in the domains of randomization, allocation concealment, blinding, accounting of patients and outcome events, and selective outcome reporting bias. Any disagreements were discussed by each of the 2 reviewers, and a consensus was reached.
Synthesis of Results
We performed a narrative synthesis of the data abstracted due to the high degree of heterogeneity of the results, as each included article reported different forms of patient functional outcomes. We synthesized each VR-based intervention and extracted the purpose of VR within the intervention and whether there was any training, supervision, or assistance provided in the use of VR. To better understand the individual differences that may affect the efficacy of VR-based interventions, we looked at the average patient age, SD and range, type of serious illness, patient gender, patient ethnicity, and study location for each of the studies. We characterized each study’s adherence to recent consensus standards for high-quality VR research using the definitions below [22].
Patient population: clear description of the study population (including inclusion and exclusion criteria)
Clinical setting: appropriate setting for the VR treatment
Control and randomization: justification for control and appropriate randomization
Blinding and concealment of allocation: description of the method of allocation concealment
End points: determination and justification of end points before the initiation of the study
Study duration: determination and justification of the study duration before the initiation of the study; the study should be an a priori decision or hypothesis
Presentation and analysis of results: clear presentation of results with appropriate statistical analysis
Reporting the trial: reporting of the trial with a national or international registry (World Health Organization International Clinical Trials or ClinicalTrials.gov)
Results
Literature Selection
A total of 12,621 unique titles and abstracts were dual screened by coauthors as per the inclusion and exclusion criteria. A total of 152 full-text articles were retrieved and further assessed for eligibility. Of the 152 full-text articles reviewed, 128 (84.2%) studies were excluded for reasons noted in the PRISMA flow diagram (Figure 1 [34]). Finally, we included 24 total studies in our review [35-58], of which 21 (88%) reported an improvement in at least 1 patient functional outcome [35-43,45-48,51-58]. The included articles are summarized in Table 1.
Figure 1.
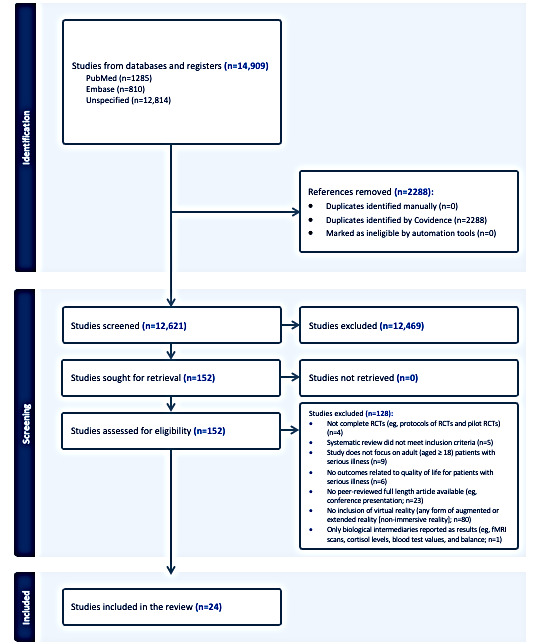
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart. fMRI: functional magnetic resonance imaging; RCT: randomized controlled trial.
Table 1.
Summary of the included studies (n=24).
| Study | Description of the intervention and media content | Control arm | Purpose of VRa in the intervention | Training, supervision, or assistance provided in the use of VR | Patient-reported outcomes or patient-demonstrated outcomes |
| Bani Mohammad and Ahmad [35], 2018 | The patients wore a head-mounted display with headphones and chose either deep sea diving or sitting on the beach. The VR exposure session ended at the peak time of morphine efficacy. |
|
Distraction therapy to improve pain and anxiety in patients | The primary investigator remained near the participants during the VR session. |
|
| Burrai et al [36], 2023 | Participants used the Oculus Quest 2 HMDd to observe specific virtual environments in a contemplative mode. The scenarios included 310 videos classified into 9 categories (eg, Africa, hills, rivers, lakes, and waterfalls). The audio content of scenarios had a background of nature sounds and soothing musical stimuli in high definition with panning stereo, and was listened to via earphones to ensure an immersive audiovisual experience with high-intensity multisensory immersion. |
|
Distraction from the stress of antiblastic therapy to reduce anxiety, fatigue, and pain | A nurse helped each participant position the VR headset and the joysticks. After immersion, the nurse removed the VR headset visor from the participant. |
|
| Chatterjee et al [37], 2022 | The main requirement was to allow the patients to practice ADLe completely or in part when placed within a suitable environment. The materials needed such as food items, kitchen gadgets, and coins were within reach of the patient when they were immersed in the environment. All the tasks were designed to be completed from a sitting position using a single handheld controller. The intervention was delivered 5 days a week for up to 2 weeks before the patient’s hospital discharge. The dose of the virtue treatment varied depending on the benefit and tolerability. |
|
Improve recovery and reduce the time that a patient spends in the hospital | Supervised by a therapy assistant while taking part in the VR session. Assisted in wearing the headset and ensured a comfortable and correct seating position. The virtue program was started by the therapy assistant, and the difficulty of each scenario was graded depending on their needs. |
|
| Chirico et al [38], 2020 | Each chemotherapy treatment lasted for 45 to 90 minutes. Patients used the VR system for 5 to 10 minutes to become accustomed to it, and then the nurse administered the chemotherapy. In particular, participants explored an island by walking through a forest, observing different animals, climbing a mountain, and swimming in the sea. |
|
Reduce the anxiety, depression, and fatigue related to chemotherapy through distraction | A research nurse, together with a trained psychologist, explained how to use the VR equipment and helped patients with putting on the headset. |
|
| Groninger et al [39], 2021 | The study used the Forest of Serenity (Holosphere VR), which features a 10-minute guide through a forest and waterfall with voice narration. Each assigned experience (VR or guided imagery) was administered at the bedside by the study coordinator. When the participant was ready, the coordinator left the bedside to stand immediately outside the room, started to time the experience per the protocol, and waited either for the end of the assigned experience time or for a verbal signal from the participant requesting assistance with the equipment. |
|
VR aimed to provide distraction therapy | The study coordinator explained the equipment and positioned it, then left the room until the end or if assistance was asked for. |
|
| Hsu et al [40], 2022 | In addition to 20 minutes of therapist-facilitated task-specific training as a usual care session, patients each received 30 minutes of VR time. The sequences of the hand exercises of VR consisted of the movements of the forearm, supination or pronation, wrist extension or flexion, finger extension or flexion, thumb opposition with the little finger, thumb extension or flexion, and tendon-gliding exercises, which involve a series of hand movements (straight hand, hook fist, straight fist, and full fist). Each movement was repeated 50 times. The participant sat in a comfortable chair in front of a desk with the VR system. |
|
Improve upper extremity movement, quality of motor movement in the affected arm, and manual dexterity | Participants received 20 minutes of therapist-facilitated task-specific training. They were supervised and assisted by the physical therapist. |
|
| Huang et al [41], 2022 | A total of 20 VR scenes from commercial games were selected for the participants. Selected scenes were chosen based on the original upper limb activities. Participants could accomplish the first-contact task with the help of their unaffected hand, and then, they were encouraged to use the affected hand or both hands at the same time. Upper limb movements in most scenes involved aiming, shooting, hitting, waving arms, punching, and throwing objects. Participants’ activity performance and information were recorded, including training intensity, duration, game scores, level completed, and invalid activities. This information allowed the therapist to assign the tasks, adjust the difficulty in the VR game settings, and even design a new way to play the game for each participant according to their needs and capacities. |
|
VR aimed to improve upper extremity movement and range of motion | After the participant confirmed that the sight and sound were clear and comfortable, the controllers were handed to the participant, and the therapist could even design a new way to play the game for each participant according to their needs and capacities. |
|
| Huang et al [42], 2024 | Participants in the imVRk system received the first 30 minutes of conventional rehabilitation, and in the second 30 minutes, the rehabilitation was performed in imVR systems. Participants in the imVR group were required to complete 6 programs: frying dumplings and noodles by controlling a wok handle in a virtual kitchen; popping balloons by controlling a sword in a virtual fencing hall; punching dolls by controlling a big fist in a virtual boxing arena; playing basketball in a virtual court, in which the ball is shot by a controller and the height and distance is varied over time; collecting eggs into a virtual basket by a controller; and tidying up a desk and moving objects to a designated position in a virtual office. All participants received rehabilitation training for 5 days per week for 3 weeks. |
|
Improve motor impairment and ADL | No training, supervision, or assistance was provided; however, in the early stages of rehabilitation, due to poor functioning of the hemiplegic side upper limb, participants used the help of their unaffected side limb. |
|
| Jo et al [43], 2024 | Each participant of the 360° MTGl performed treatment tasks using their unaffected extremities, which were recorded with a 360° camera (Insta 360° X3; Insta 360). The patients received treatment in the same place where the videos were recorded. The therapist instructed and guided patients to use the affected side following the immersive video during all tasks. The MTm tasks were the same as those of TMTGn (finger flexion and extension, wrist flexion and extension, pronation and supination, and elbow flexion and extension for 10 repetitions; the tasks instructed participants to use the affected limb while following the mirror images of the unaffected limb to induce movement re-education; and playable tasks using ring toys were also provided for 5 repetitions). The 360° MT was provided for 30 minutes per session, 3 sessions a week for 4 weeks. The 360° MTG also received additional conventional physical therapy. |
|
Upper extremity rehabilitation in patients with stroke | A therapist adjusted the device to fit the eye level of each patient. The therapist instructed and guided patients to use the affected side following the immersive video during all tasks. |
|
| Laghlam et al [44], 2021 | The VR session started during the preparative phase, at least 5 minutes before the removal of the drains, and was continued for 10 minutes after. We used a VRx helmet with a 90° field of view with head tracking. Patients had a choice between 5 different immersive environments (360° videos): a snowy mountain, a landscape in India or Camargue (France), a balloon ride, or a canoe descent. |
|
Reduce pain during cardiac surgery, specifically during the removal of drains | The nurse supervised and assisted patients while using VR. |
|
| Lee and Kang [45], 2020 | The “Relaxing Music for Meditation” program was designed to induce meditation and consists of 8 meditation videos of 30 minutes. Scenes of mountains, seas, or lakes appear on the VR screen, and background sounds and calm music allow participants to immerse themselves in the experience. The study began on the day of admission to the ICUr. |
|
Induce meditation and improve sleep quality | No training, supervision, or assistance was mentioned; however, it took about 20 minutes for the experimental group to learn how to use the HMD. |
|
| Mekbib et al [46], 2021 | The VR rehabilitation training included reaching, grasping, and releasing tasks. Following the training schema, all patients in the VR group received 1-hour VR and 1-hour OT per day, 4 days per week for 2 weeks. In each VR session, the therapy modes were set by a therapist based on the patient’s interest and actual motor capability. After choosing the therapy mode, the therapist randomly set 20 colored balls from the aerial view map. Then, the patient was instructed to reach, grasp, and release each ball into the basket. After completing the first VR session (20 balls), the therapist could set the next VR session and adjust the task complexity to be slightly higher or lower or keep it as it was in the previous session based on the patient’s activity performance. |
|
Upper extremities to aid in the recovery of motor function after stroke and improve upper extremity function and the ability to perform ADL | The therapist helped train the patient. If the patient was not able to move their upper extremity toward the target ball, the therapist could help move the affected extremity to assist in the intended task. |
|
| Menekli et al [47], 2022 | Patients in the intervention group were educated on the use of VR glasses by the researcher. A smartphone and the various number of parks, nature, and seaside walks; submarine; and museum tours with the Matic Music were provided to patients in the intervention group. Each of these videos took approximately 3 to 10 minutes, and patients could choose the video that they wanted to watch. Patients started to use the VR after the baseline assessment (about 1 minute before the implantation) and continued to use it until the end of the implantation. Patients were instructed to use VR after implantation when they felt pain from the implantation. |
|
Pain management after implantation | Supervision and assistance were provided by a nurse, who was giving directions to patients on how to use the videos. |
|
| Ögün et al [48], 2019 | Patients used the VR device to play task-oriented games that focused on gripping and handling objects with arm and forearm motion and stability. A different game was used for each function, with 4 games: a cube handling game used for grip function integrated with the leap motion device to make the patients feel like they were handling a real object using their own fingers without the use of any external device to track hand motion; another leap motion–integrated game involving decorating a tree with leaves and fruits or picking up vegetables from a bowl and putting them back, which was chosen to facilitate all hand motions combined with complex motions in a task-oriented job; a kitchen experience game used for stimulating forearm supination and pronation and for combining complex arm movements; and a drumming game, selected to randomly assign each separate movement of upper extremity flexion and abduction. |
|
Improve upper extremity functionality and make daily activities more accessible | None mentioned |
|
| Park et al [49], 2013 | The VR-based postural control program consisted of a program for the improvement of gait ability by visual feedback compared to reference motion scenes and reality motion. The program consisted of 3 stages: trunk stability and pelvic tilting in a supine position (stage 1); trunk upright control and pelvic tilting exercise in a sitting position, and a selective movement between trunk and pelvis (stage 2); and lower extremity muscle strengthening exercise and weight bearing under maintenance of trunk stability in a standing position (stage 3). The participants were provided with specific scenes on HMD showing the simultaneous output. |
|
Improve postural control, spatiotemporal gait ability, and functional gait ability and to increase walking ability | The participant saw the prerecorded reference motion and practiced it again 3 times. No other provision of training, supervision, or assistance was mentioned. |
|
| Rousseaux et al [50], 2022 | A 20-minute VR session was conducted, where participants watched a 3D graphical landscape consisting of a mountain cabin near a lake at sunrise, followed by a relaxing moment in the clouds. The display was visual and audio, with sounds of ambient nature but no voice. |
|
Lower anxiety and decrease pain | None mentioned |
|
| Rutkowski et al [51], 2021 | The primary aim of the software was to calm the patient down and improve his or her mood. The software features a virtual therapeutic garden and is based on the Ericksonian psychotherapy approach. The garden is a metaphor for the patient’s health: at the beginning, it appears untidy and gray; however, with each session, it becomes more colorful and alive, thus symbolizing the process of recovery of energy and vigor. The 2 groups participated in the traditional pulmonary rehabilitation program. Components were performed once a day each, for 15 to 30 minutes (depending on the task), 5 times a week for 2 weeks. Exercises were performed as follows: fitness exercises while standing on the knees and lying on the side, abdomen, and back; strengthening exercises of the diaphragm with resistance; prolonged exhalation exercise; chest percussion; inhalation with a 3% sodium chloride isotonic solution administered via an ultrasonic device; and stationary cycle ergometer exercise to obtain a training heart rate according to GOLDw spirometric stages. The difference between the groups is in the type of relaxation training: the VR group performed 10 VR therapy sessions of 20 minutes, and the CG performed 10 Schultz autogenic training sessions of 20 minutes. |
|
Reduce depression, anxiety, and stress levels and improve functional capacity | None mentioned |
|
| Shin et al [52], 2023 | In the virtual world, patients were greeted by their respective attending physicians and guided through the visual and audio unfolding of the RTaa process. Patients were guided virtually with 360° viewing of the different treatment environments and RT machines that they would encounter when undergoing RT. Throughout the physician’s explanation, patients were able to witness a real example of a patient with breast cancer undergoing the RT, offering patients a concrete example of what to expect on treatment days. |
|
Alleviate anxiety related to undergoing RT | Patients were assisted with the proper positioning of the VR headset and noise-cancelation earphones provided by the hospital. |
|
| Song and Lee [53], 2021 | The VRBATae group underwent immersive VRBAT. The VR content consisted of rehabilitation tasks to improve upper limb function, the ability to perform ADL, and visual perception. The VR tasks performed included everyday activities, such as turning on lights, organizing a chest of drawers, organizing a kitchen, watering plants, and purchasing items at a convenience store. The virtual living room, kitchen, veranda, and convenience store were designed to simulate real environments. Interventions were performed for 30 minutes a day, 5 times a week, for 4 weeks, for a total of 20 sessions. All participants in the VRBAT group also underwent an hour of conventional rehabilitation per day. |
|
Improve the range of motion, bilateral upper extremity movement, and upper limb function | There was some training, supervision, or assistance provided; however, this was not written, although figures in the study show someone guiding the participant. |
|
| Spiegel et al [54], 2019 | Participants selected one of the 21 VR experiences from an app. Patients were asked to use the headset for 10 minutes in the presence of study staff to practice with the equipment and then advised to use the headsets thrice daily, for 10 minutes per session, and later, as needed for breakthrough pain, for the subsequent 48 hours. Following these initial instructions, patients decided for themselves and in partnership with their care team whether, how frequently, and how long to use the VR equipment without direct input from study staff. |
|
Reduce pain in hospitalized patients | Participants were instructed on procedures for wearing the headset, how to select among the 21 VR experiences, and how to adjust volume and brightness. Regarding supervision, patients were initially asked to use the headset for 10 minutes with the presence and assistance of the study staff and care team. |
|
| Torres García et al [55], 2023 | The sessions recreated a chemotherapy procedure. Using VR, patients managed their anxiety and fear through relaxation, attentional focus, and mindfulness strategies. The complete intervention included 3 modules, which each patient repeated during 4 individual sessions, aiming to improve their preparation and adaptation to the cancer treatment they had to start. |
|
Improve patients’ anticipatory anxiety and adherence to chemotherapy and facilitate better and faster adaptation to treatment coping mechanisms | The therapist was present throughout the procedure. |
|
| Turrado et al [56], 2021 | A realistic environment was generated in which the patient could experience the various steps of their admission to surgery, from the first interview with the surgeon to admission into the surgical ward, the operating room, and the postoperative recovery room. Patients completed both questionnaires to assess their basal anxiety levels. The patients in the intervention group had unlimited access to VR glasses and to the VR app. This group completed both questionnaires again on the day before the surgical procedure. |
|
Reduce presurgical anxiety and depression | None mentioned |
|
| Uslu and Arslan [57], 2023 | The patients watched and listened to beach and nature content with VR glasses for 30 minutes. The VR glasses used were Zore G04BS VR Shinecon VR glasses, compatible with smartphones (eg, Android and IOS). The contents were determined in the YouTube library and included 360° relaxing beach and nature images. |
|
Reduce anxiety and fatigue levels | Patients were informed about using VR and viewing the content. From the content opened by the researcher, it was ensured that the patient watched and listened to the content of their choice. |
|
| Zhang et al [58], 2023 | The patients watched and listened to beach and nature content with VR glasses for 30 minutes. The VR glasses used were Zore G04BS VR Shinecon VR glasses, compatible with smartphones (eg, Android and IOS). The contents were determined in the YouTube library and included 360° relaxing beach and nature images. |
|
Reducing anxiety and fatigue levels | Patients were informed about using VR and viewing the content. From the content opened by the researcher, it was ensured that the patient watched and listened to the content of their choice. |
|
aVR: virtual reality.
bVAS: visual analog scale.
cSAI: State Anxiety Inventory.
dHMD: head-mounted display.
eADL: activities of daily living.
fMoCA: Montreal Cognitive Assessment.
gFACIT-Pal: Functional Assessment of Chronic Illness Therapy–Palliative Care.
hOT: occupational therapy.
iFMA-UE: Fugl-Meyer assessment for upper extremity.
jMAL-AOU: motor activity log-amount of use.
kimVR: immersive virtual reality.
lMTG: mirror therapy group.
mMT: mirror therapy.
nTMTG: traditional mirror therapy group.
oMFT: manual function test.
pBBT: box and block test.
qCG: control group.
rICU: intensive care unit.
sBI: Barthel Index.
tARAT: action research arm test.
uFIM: functional independence measure.
vPASS: performance assessment of self-care skills.
wGOLD: Global Initiative for Chronic Obstructive Lung Disease.
xHADS-A: Hospital Anxiety and Depression Scale-Anxiety.
yHADS-D: Hospital Anxiety and Depression Scale-Depression.
zHADS: Hospital Anxiety and Depression Scale.
aaRT: radiation therapy.
abAPAIS: Amsterdam Preoperative Anxiety and Information Scale.
acSTAI: State-Trait Anxiety Inventory.
adLASA: linear analog scale assessment.
aeVRBAT: VR-based bilateral arm training.
afMini-MAC: mini-mental adjustment to cancer.
Participant Characteristics
In total, the studies included 1225 participants. Of the 24 included studies, 3 (12%) included patients with an average age of <50 years [43,49,58]; 8 (33%) included patients with an average age of 51 to 60 years [35,36,38-41,46,52,55,57]; 5 (21%) included patients with an average age of 61 to 65 years [42,45,48,51,52]; 3 (12%) included patients with an average age of 66 to 70 years [44,50,56]; and 1 (4%) included patients with an average age of >75 years [37]. Two studies did not report the average age of the patients, as listed in Table 2 [47,54]. No studies reported how many patients in the sample were aged >65 years. A total of 16 (67%) of the 24 included studies had a high risk of bias (Multimedia Appendix 4 [35-58]).
Table 2.
Patient characteristics.
| Study | Patients, n | Patient age (y), average (SD); range | Serious illness, n (%) | Sex, n (%) | Study location | Ethnicity |
| Bani Mohammad and Ahmad [35], 2018 | 80 |
|
Breast cancer stage:
|
|
Jordan |
|
| Burrai et al [36], 2023 | 74 |
|
|
|
Italy |
|
| Chatterjee et al [37], 2022 | 40 |
|
|
|
United Kingdom |
|
| Chirico et al [38], 2020 | 92 |
|
Breast cancer stages:
|
|
Italy |
|
| Groninger et al [39], 2021 | 88 |
|
|
|
United States |
|
| Hsu et al [40], 2022 | 52 |
|
Stroke type:
|
|
Taiwan |
|
| Huang et al [41], 2022 | 30 |
|
|
|
Taiwan |
|
| Huang et al [42], 2024 | 40 |
|
Stroke type:
|
|
China |
|
| Jo et al [43], 2024 | 45 |
|
Stroke paretic side:
|
|
South Korea |
|
| Laghlam et al [44], 2021 | 180 |
|
|
|
France |
|
| Lee and Kang [45], 2020 | 48 |
|
|
|
South Korea |
|
| Mekbib et al [46], 2021 | 23 |
|
Stroke type:
|
|
China |
|
| Menekli et al [47], 2022 | 139 |
|
|
|
Turkey |
|
| Ögün et al [48], 2019 | 65 |
|
|
|
Turkey |
|
| Park et al [49], 2013 | 16 |
|
Stroke type:
|
|
Korea |
|
| Rousseaux et al [50], 2022 | 100 |
|
|
|
Belgium |
|
| Rutkowski et al [51], 2021 | 50 |
|
|
|
Poland |
|
| Shin et al [52], 2023 | 196 |
|
Breast cancer stages:
|
|
South Korea |
|
| Song and Lee [53], 2021 | 10 |
|
|
|
Korea |
|
| Spiegel et al [54], 2019 | 120 |
|
Intervention:
|
|
United States |
|
| Torres García et al, 2023 [55] | 133 |
|
|
|
Spain |
|
| Turrado et al [56], 2021 | 126 |
|
|
|
Spain |
|
| Uslu and Arslan [57], 2023 | 66 |
|
|
|
Turkey |
|
| Zhang et al [58], 2023 | 60 |
|
|
|
China |
|
aCHF: congestive heart failure.
bMI: myocardial infarction.
cCOPD: chronic obstructive pulmonary disease.
dLAR: low anterior resection.
eTaTME: transanal total mesorectal resection.
Serious Illness
Stroke, cancer, and cardiovascular disease were the most common types of serious illnesses for which VR interventions were used to impact the outcomes related to patients’ quality of life. Out of 24 included studies, 9 (38%) focused on patients who experienced stroke, which included both ischemic stroke and hemorrhagic stroke [37,40-43,46,48,49,53], and 9 (38%) included patients who were diagnosed with some type of cancer, varying in the stages of cancer in each patient [35,36,38,42,43,47,52,55-58]. In 5 (21%) of the 24 studies, only patients who were diagnosed with breast cancer were included; 1 study (4%) included patients with colorectal cancer, and 1 (4%) included patients with heterogeneous types of cancer. Four (17%) out of 24 studies included patients who had some form of cardiovascular disease, including heart failure and other conditions that required cardiac surgery [39,44,45,50]. One study included patients with chronic obstructive pulmonary disease (COPD), and another included patients who reported pain during their hospitalization [51,54].
Purpose and Content of VR
In 9 (38%) out of 24 included studies, the main purpose of VR was to improve mobility and strength in the patient, ranging from upper extremity, lower extremity, and pelvic or abdominal region to a combination of these regions [37,40-43,46,48,49,53]. All of these mobility studies also included patients who experienced strokes. The VR media used in these studies encouraged active participation from the patients in various tasks and games. Some examples of VR media used to help improve mobility and strength in patients’ poststroke treatment were daily exercises that encouraged increased range of motion, strength for specific movements, and reach and grasp through the use of balls. A total of 8 (89%) of the 9 studies that used VR for the purpose of improving mobility and strength improved patient quality of life–related outcomes [37,40-43,46,48,53].
There was some overlap in the protocols and diseases of the additional studies. Out of 24 studies, 12 (50%) used VR distraction therapy to reduce pain in patients with cancer or, cardiovascular disease or hospitalized patients [35,36,38,39,42-44,47,50,52,54-58]. A total of 9 (38%) out of 24 studies used VR to reduce anxiety in patients with cancer, cardiovascular disease, or COPD [36,38,42,43,50-52,55-58]. In studies aiming to reduce pain and anxiety, patients experienced immersive natural scenery and comforting music while comfortably sitting or lying down. In another study, to reduce anxiety, patients experienced the hospital environment and could visualize and review all the steps of an upcoming procedure [56]. In another study, patients with cardiovascular disease went through a visual guided meditation track with the VR media for patients with cardiovascular disease [45].
Training, Supervision, and Assistance
In 18 (75%) out of 24 studies, staff or physical therapists either trained patients on VR use before the intervention or supervised or assisted them through the experiment. Supervision was defined as the research team watching over the participants, ensuring their use and adherence to study guidelines. However, assistance was defined as the research team supporting patients during the intervention without constant watching throughout the experiment. A total of 5 (20.8%) out of 24 studies included VR training, supervision, and assistance, all of which reported improvements in patient quality of life–related outcomes [38,40,43,46,54]. Of 24 studies, 7 (29.2%) included VR supervision and assistance only [36,37,41,44,47,53,57], and 2 (8.3%) included VR training and assistance only [39,49]. Two (8.3%) out of 24 studies included only VR supervision while patients were using VR [35,55]. In studies that included a variation of personnel working with the patient, only 1 staff member physically accompanied the patient in the room, where they freely communicated with the patient to fulfill their role. During a typical training, the staff member would walk the patient through the VR activity and teach them how to adjust the headset. Out of 24 studies, 6 (25%) did not describe training, supervision, or assistance with the use of VR [42,45,48,50,51,56].
Frequency and Duration of Intervention on Quality of Life Outcomes
The frequency and duration of VR experience varied based on the intervention purpose; interventions aiming to improve pain or anxiety were shorter. while those aiming to improve mobility and strength were longer. Out of the 24 included studies, 9 (38%) studies with pain or anxiety reduction as a goal, involved only 1 VR session, ranging from 8 minutes to 4 hours (ie, patients could use VR at any time within a 4-hour window) [35,38,39,44,47,50,52,56]. A total of 7 (78%) of these 9 studies had improvements in pain and anxiety metrics, such as the Hospital Anxiety and Depression Scale (HADS), State Anxiety Index, or the Numeric Pain Scale (NPS). One study, which conducted a single 30-minute meditation session, showed improvement in sleep scores of patients with cardiovascular disease [45]. In 1 case where VR was used for 10 minutes per session, for 3 sessions per day for 2 days, patients experienced statistically significant improvement in the NPS (P<.04) [54]. Patients in another study who used VR for 20 minutes per session for 5 sessions per week for 2 weeks had statistically significant improvement in the HADS (P<.001) [51].
In the 9 studies aimed at improving mobility and strength in patients who had a stroke, VR was used for a longer duration than in pain and anxiety studies. Out of 9 studies, 6 (67%) lasted between 2 and 4 weeks [37,42,43,46,49,53], while 3 (33%) lasted between 5 and 9 weeks [40,41,48]. A total of 8 (89%) of these 9 studies showed an improvement in the patient’s functional capacity measured via the Fugl-Meyer upper extremity assessment, proprioception, or orientation metrics.
Gold Standard Adherence
As shown in Table 3, 7 studies adhered to all the 8 gold standard VR consensus standards criteria (100%) [41,43,44,48,51,52,54], 10 adhered to 7 criteria (88%) [36,37,39,40,42,46,55-58], 6 adhered to 6 criteria (75%) [35,38,47,49,50,53], and 1 adhered to 5 criteria (62%). The reasons for not adhering to the criteria were inadequate blinding, concealment of allocation, reporting of the trial, and a priori failure to justify study duration. The studies that did not report the trial via World Health Organization International Clinical Trials or Clinicaltrials.gov originated from countries where it may not be standard practice to report the clinical trial before the study initiation. All 24 assessed studies received the institutional review board or ethics committee approval. A total of 4 (17%) of the 24 included articles were published before the 2019 study by Birckhead et al [22] that defined the gold standard VR consensus standards criteria.
Table 3.
Study adherence to the “gold standard.”
| Study | Patient population | Clinical setting | Control and randomization | Blinding and concealment of allocation | End points | Study duration | Presentation and analysis of results | Reporting the trial | |
| Bani Mohammad and Ahmad [35], 2019 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
Medical and surgical wards of a specialized cancer center in Jordan | Random assignment was done based on flipping a coin; if heads appeared, then the first participant was placed in the intervention group. The rest of the participants were placed in the study groups by the order of meeting the eligibility criteria. | N/Aa | The VASb was used to measure pain, and the SAIc was used to measure anxiety. | One session occurred for 20 to 30 minutes; VRd was timed with peak morphine efficacy and the goal was acute pain relief. |
|
None mentioned outside of ethics or IRBf approvals from individual hospitals |
|
| |||||||||
| Burrai et al [36], 2023 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Regional hospital in Italy | An independent researcher used a random number generation software with simple randomization. A total of 3 numerical codes for the 3 allocation groups were used: 1 for the VR group, 2 for the narrative medicine group, and 3 for the standard care group. To implement the random allocation sequence, sequentially numbered, opaque, sealed envelopes were used. | Owing to the nature of VR and narrative medicine interventions, it was impossible to obtain a blinding between the participants and knowledge of the group, so this study is open-label type. | Anxiety was measured with the STAI-Y1g; fatigue was measured with the revised Piper Fatigue Scale; and pain was measured with the VAS scored from 0 to 10, where 0 indicates no pain and 10 indicates the worst possible pain. | VR was administered just after ATh began and the immersion duration was 30 minutes. |
|
The study was registered in the US National Institutes of Health (NCT05629507). |
| Chatterjee et al [37], 2022 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Stroke unit at the Countess of Chester Hospital NHSi Foundation Trust. | Participants were randomized on a 3:1 allocation basis. | This study was not effective to implement as a double-blind trial, as most patients were able to deduce whether they were a part of the treatment group. | The MoCAjwas the primary measure used and the NEADLk, HADSl, and quality of life (EuroQoLm) were the secondary measures used. | A total of 5 days a week for up to 2 weeks before their hospital discharge time that each patient spent in a VR session was very specific to the individual. Time spent in a session would depend on their level of wellness on the day and how tired they were feeling. |
|
The trial was registered in the ISRCTNn registry (ISRCTN16608742). |
| Chirico et al [38], 2020 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
National Cancer Institute, IRCCS “Fonda-zione G. Pascale,” Naples, Italy | Patients were randomly assigned to the VR or music therapy group and were compared with a nonconcurrently recruited CGo. | Participants and personnel knew which groups were control and intervention groups. | SAI for adults and SV‐POMSp | Each chemotherapy treatment lasted for 45 to 90 minutes, but the patient used VR for 20 minutes. |
|
None mentioned outside of ethics or IRB approvals from individual hospitals. |
| Groninger et al [39], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
A 912-bed academic hospital located within MWHCr in Washington, DC. | Participants were randomized by the study coordinator on a 1:1 basis using a computerized randomized scheme. | The nature of the study prevented participants and the study coordinator from being blinded to assigned interventions. | Self-reported pain scores and the FACIT-Pal 14s item scale were used. | There was 1 session for 10 minutes. In distraction therapy research, there is currently no predetermined time threshold for the effect on pain experience; 10 minutes falls within the range of time frames (2 to 15 minutes) that have demonstrated the benefit of using VR for pain management. |
|
The trial was registered on ClinicalTrials.gov (identifier: NCT04572425). |
| Hsu et al [40], 2022 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
Department of physical medicine and rehabilitation at a medical center in South Taiwan | Following eligibility screening, patients meeting the inclusion criteria were randomly allocated to conditions using opaque envelopes with computer-generated random numbers that the investigator opened upon receiving a consenting participant. | Eligible patients were randomly allocated until all the available envelopes had been exhausted, resulting in a 1:1:1 ratio in the MTt, COTu, or VR-MT group. | The FMA-UEv motor coordination score and the MALw were used. | The study duration was 30 minutes twice a week for 9 weeks. VR timing was time-matched to the control group. |
|
None mentioned outside of ethics or IRB approvals from individual hospitals |
| Huang et al [41], 2022 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
The VR equipment was installed in a room without external disturbances, and the virtual environment was set in a 6 m2 physical space in a hospital in southern Taiwan. | A total of 30 patients with chronic stroke were randomized to the VR or COT groups | Clinical assessments were performed within 1 week before and after the interventions by another therapist not involved in training and blinded to the purpose and group allocation. | The FMA-UE and AROMx were used. | All participants received 16 sessions of intervention for 60 min per day, 2 to 3 days per week. |
|
The trial was registered in the WHOy International Clinical Trials registry (ChiCTR2100047853). |
|
| |||||||||
| Huang et al [42], 2024 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, China | Each participant was randomly assigned a code based on computer-generated, permuted block randomization with a block size of 4. | Because of the nature of the intervention, participants and therapists could not be blinded to the allocated treatment. These therapists did not participate in assessments of the outcomes. | The FMA-UE [20] and the BIz were used. | All participants received rehabilitation training for 5 days per week for 3 weeks. The first 30 minutes was conventional rehabilitation, followed by 30 minutes of rehabilitation performed in imVRaa systems |
|
The trial was registered on ClinicalTrials.gov (identifier: NCT03086889). |
| Jo et al [43], 2024 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Hospital in Seoul, Republic of Korea | Randomized controlled trial with the participants randomly allocated into 3 groups using a computer-generated list of numbers at a 1:1:1 ratio: imVR-based 360° MTGab, TMTGac, and a CG | The study was conducted as an assessor-blinded and randomized controlled trial. | FMA-UE was used, and secondary outcome measurements were MFTad and BBTae. | In addition to conventional physical therapy, traditional MT was provided for 30 minutes per session, 3 sessions a week, for 4 weeks |
|
The trial was registered on ClinicalTrials.gov (NCT05796843) and received approval from the Sahmyook University IRB (SYU 2023-01-009-001) |
|
| |||||||||
| Laghlam et al [44], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
ICUaf of the Centre Médico-Chirurgical Ambroise Paré in Neuilly-sur-Seine, France. | Randomization was performed using an external interactive web response system. | Patients were randomly assigned (1:1) in permuted blocks. | The NRSsag for pain and anxiety were used. | One session started at least 5 minutes before the removal of the drains and continued for 10 minutes after the removal of the drains. VR was timed with morphine administration (and the goal was for acute pain relief). |
|
The trial was registered on ClinicalTrials.gov (NCT03956264). |
| Lee and Kang [45], 2020 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Did not completely meet | Completely met | Not completely met |
|
|
Description |
|
Cardiac ICU, Dong-A University Medical Center, Busan, South Korea. | Patients were randomly allocated with a 1:1 random list order using the random allocation software program (version 2.0.0). ICU nurses did not know which group the next participant would be assigned to. | Double blindness was not possible due to the interventional characteristics of the study using VR equipment. | The PSQIah was used. | The study duration was 30 minutes before bedtime (9 PM to 11 PM) on the day of ICU admission. The difference in sleep quality and the effects of intervention during the ICU stay could not be investigated |
|
Nothing was mentioned other than the IRB approval. |
| Mekbib et al [46], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
Department of Rehabilitation Medicine at Zhejiang Province People’s Hospital (Hangzhou, China). | This clinical trial used a single-blind, randomized, parallel group design. Patients were randomly assigned to either the VR or OTai group using random numbers generated by a computer program. | The group allocation procedure was managed by a physician who was unaware of the study protocol. | The FMA-UE and BI scores were used. | Study duration was 1 hour VR and 1 hour OT per day, 4 days per week for 2 weeks. VR timing was time-matched to the CG. |
|
None mentioned outside of ethics or IRB approvals from individual hospitals and the Helsinki Declaration of Ethical Principles for Medical Research Involving Human Subjects |
|
| |||||||||
| Menekli et al [47], 2022 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Not completely met | Completely met | Completely met |
|
|
Description |
|
Malatya Turgut Özal University Oncology Hospital | Computer-assisted simple randomization was used to determine the groups. | There was no blinding for the patients or the researchers throughout the study. | The SAI and VAS scores were used. | The study was conducted at the liberty of the patient throughout the procedure, lasting 4 hours. |
|
The trial was registered on ClinicalTrials.gov (NCT05140707). |
|
| |||||||||
| Ögün et al [48], 2019 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Bolu Abant Izzet Baysal University, Physical Therapy and Rehabilitation Hospital | Patients were randomly divided into 2 groups, VR or control, with stratified randomization according to age, sex, and stroke onset, using an online randomization website. | Both patients and outcome assessors were masked, achieved using sham VR therapy with the CG, with the outcome assessor blinded to the groups. | FMA-UE, ARATaj, FIMak, PASS-IADLal, and PASS-BADLam were used as secondary outcome measurements. | The VR group received VR rehabilitation 3 days a week, on Monday, Wednesday, and Friday, at the same time each day for 6 weeks. Each session lasted approximately 60 minutes and comprised 4 games that lasted 15 minutes each. |
|
The trial was registered on ClinicalTrials.gov (NCT03135418). |
|
| |||||||||
| Park et al [49], 2013 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
Stroke units of a hospital in Seoul, Korea. | The 16 participants were randomly assigned to either the experimental group (n=8) or the CG (n=8) by selection of white or black go stones 1 hour before the start of the pretest. | N/A | The patient’s spatiotemporal gait ability, functional gait ability, and increased functional walking ability were measured. | The study duration was 60 minutes per day, 5 days per week for 4 weeks. VR timing was time-matched to the CG. |
|
None mentioned outside of ethics or IRB approvals from individual hospitals |
|
| |||||||||
| Rousseaux et al [50], 2022 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Not completely met | Completely met | Completely met |
|
|
Description |
|
Liege University Hospitals, Domaine Universitaire du Sart Tilman | Randomization was undertaken in blocks of 5 patients. | Given the nature of the techniques, neither the patients nor the investigators were blinded to the treatment assignment. | The VAS was used. | The study comprised a 20-minute session on the preoperative day (T0 and T1) and a 20-minute session after surgery (T2 and T3). No justification was written in the manuscript for the study duration. |
|
The trial was registered retrospectively on ClinicalTrials.gov (NCT03820700). |
| Rutkowski et al [51], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
A specialist Hospital in Głuchołazy, Poland | Randomization was performed using the Research Randomizer (ratio of 1:1), a web-based service that offers instant random assignment. Sealed envelopes were used for group assignments. | An assessor-blinded parallel group | The HADS, PSQao, 6MWTap, and lung function test with FEV1aq were used. | The study was conducted once a day, each session for 15 to 30 minutes (depending on the task), 5 times a week for 2 weeks. VR group performed 10 VR therapy sessions of 20 minutes. |
|
The trial was registered on ClinicalTrials.gov (NCT0460154). |
| Shin et al [52], 2023 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Academic hospital in Seoul, South Korea. | Randomization was done using an online randomizing tool (www.randomizer. org) by an independent research coordinator. | Physicians were blinded to the study arms and did not interact with the coordinator. | Anxiety levels were measured using the APAISat as the primary end point and the STAI and LASAau as secondary end points | The study was for a single time; on the same day of randomization, patients watched the 7- to 8-minute-long VR video. |
|
The protocol was registered on ClinicalTrials.gov (NCT04141943) and approved by the Severance Hospital IRB (4-2019-0795). |
| Song and Lee [53], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Not completely met |
|
|
Description |
|
C Rehabilitation Hospital or G Rehabilitation Hospital in Gwangju city | Randomization was achieved using the opaque sealed envelope method. | N/A | Manual function test and proprioception test | Interventions were performed for 30 minutes a day, 5 times a week, for 4 weeks, for 20 sessions. |
|
None mentioned outside of ethics or IRB approvals from individual hospitals |
|
| |||||||||
| Spiegel et al [54], 2019 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Cedars-Sinai Medical Center, a large, urban, tertiary care hospital | Patients were randomized on a 1:1 basis between groups using the Microsoft Excel random number generator. | A script that used neutral language regarding both interventions was used. Investigator interactions with the study participant were minimized, relying on nonstudy nursing staff to collect pain scores. | An NRS of patient-reported pain was used. | The study duration was 10 minutes per session, 3 times a day, for 48 hours; 10 minutes was selected to reduce the risk of developing cybersickness. Longer exposure times are associated with a higher risk of cybersickness. |
|
The trial was registered on ClincialTrials.gov (NCT02887989). |
|
| |||||||||
| Torres García et al [55], 2023 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
OCCUav of the CIMAaw Campus, Milenium Iradier Medical Center, Barcelona, Spain | Randomization was carried out using a random number list obtained with the Random.org app. The order in which it was generated was unknown to the oncologist. | The oncologist was unaware of the information provided other than the order in which randomization was generated. | HADS, DDEax scale, and the Mini-MACay coping scale were used. | The study comprised 4 sessions lasting approximately 30 to 45 minutes. The first 3 sessions coincided with the chemotherapy treatment prescribed by the oncologist. The fourth session was conducted 3 months after the third session to check whether the benefits of the previous interventions were maintained. |
|
The study was approved by the Clinical Research Ethics Committee (CEIC) of Hospital CIMA (Barcelona, Spain), a center authorized by the Department of Health (H08621946). |
|
| |||||||||
| Turrado et al [56], 2021 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Third-level Academic Center in the Gastrointestinal Surgery Department in Barcelona, Spain | Patients were randomized using en bloc randomization with random block sizes. | Patients and health care professionals could not be blinded regarding group assignment. | HAD-D, HAD-A, STAI_A/S, and STAI_A/T scores were used. | The patients in the intervention group had unlimited access to VR glasses and to the VR app. |
|
The trial was registered on ClinicalTrials.gov (NCT04058600). |
| Uslu and Arslan [57], 2023 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
Oncology outpatient department of a university hospital in Turkey | This study was conducted using the randomization block method (6:5). Combinations with randomization were enumerated using a web-based random queue generator with permuted random block allocation (block size: 33). The intervention group and CG were determined by lots. | Blinding was not possible due to the nature of the study. With VR, the patients could not be blinded during the intervention because they knew that they were in the intervention group. Randomization was prepared by a statistician, but this was hidden from the researcher performing the study. | The STAI scale and the CFSbb were used. | The study was conducted once every 21 days for 4 sessions (1 session per chemotherapy cycle for 4 cycles) for 30 minutes. |
|
The trial was registered with the US National Institutes of Health Clinical Trials Registry on September 12, 2021 (NCT05168696) |
| Zhang et al [58], 2023 | |||||||||
|
|
Met criteria | Completely met | Completely met | Completely met | Not completely met | Completely met | Completely met | Completely met | Completely met |
|
|
Description |
|
A public hospital in Guangzhou, China | Participants were randomly assigned to the intervention group and CG in a 1:1 ratio by generating 70 codes written on identically sized pieces of paper, which were placed in opaque, sealed, and sequentially numbered envelopes. | Owing to the nature of VR intervention, blinding the participants and the interventionist was impossible. | The SAI scale, CES-Dbc scale, and FACT-leubd questionnaire were used. | From days 1 to 14, participants experienced 14 different immersive videos. To avoid interruption from common treatment activities, every intervention occurred from 3 PM to 6 PM. | Those in the intervention group demonstrated a significantly greater reduction in anxiety (P<.05) and improvement in quality of life (P=.04). There was no significant difference in depression levels between groups (P=.09), although a decreasing trend was observed in the intervention group. |
The protocol was registered retrospectively in the ISRCTN registry (ISRCTN 84842464; June 6, 2022). |
aN/A: not applicable.
bVAS: Visual Analog Scale.
cSAI: State Anxiety Inventory.
dVR: virtual reality.
eMCID: minimal clinically important difference.
fIRB: institutional review board.
gSTAI-Y1: State-Trait Anxiety Inventory-Y1.
hAT: antiblastic therapy.
iNHS: National Health Service.
jMoCA: Montreal Cognitive Assessment.
kNEADL: Nottingham extended activities of daily living.
lHADS: Hospital Anxiety and Depression Scale.
mEuroQOL: European Quality of Life.
nISRCTN: International Standard Randomized Controlled Trial Number.
oCG: control group.
pSV-POMS: short version of profile of mood states.
qAHA or ACC: American Heart Association or American College of Cardiology.
rMWHC: MedStar Washington Hospital Center.
sFACIT-Pal 14: Functional Assessment in Chronic Illness Therapy–Palliative Care 14-item scale.
tMT: mirror therapy.
uCOT: conventional occupational therapy.
vFMA-UE: Fugl-Meyer assessment for upper extremity.
wMAL: motor activity log.
xAROM: active range of motion.
yWHO: World Health Organization.
zBI: Barthel Index.
aaimVR: immersive virtual reality.
ab360° MTG: 360° mirror therapy group.
acTMTG: traditional mirror therapy group.
adMFT: manual function test.
aeBBT: box and block test.
afICU: intensive care unit.
agNRS: numeric rating scale.
ahPSQI: Pittsburg Sleep Quality Index.
aiOT: occupational therapy.
ajARAT: action research arm test.
akFIM: functional independence measure.
alPASS-IADL: performance assessment of self-care skills—instrumental activities of daily living.
amPASS-BADL: performance assessment of self-care skills—basic activities of daily living.
anCOPD: chronic obstructive pulmonary disease.
aoPSQ: Perception of Stress Questionnaire.
ap6MWT: 6-minute walk test.
aqFEV1: forced expiratory volume for 1 second.
arHADS-A: Hospital Anxiety and Depression Scale-Anxiety.
asHADS-D: Hospital Anxiety and Depression Scale-Depression.
atAPAIS: Amsterdam Preoperative Anxiety and Information Scale.
auLASA: Linear Analog Scale Assessment.
avOCCU: Oncology Counseling and Care unit.
awCIMA: Chartered Institute of Management Accountants.
axDDE: emotional discomfort detection.
ayMini-MAC: mini-mental adjustment to cancer.
azLAR: low anterior resection.
baTaTME: transanal total mesorectal resection.
bbCFS: Cancer Fatigue Scale.
bcCES-D: Center for Epidemiological Studies-Depression Scale.
bdFACT-leu: functional assessment of cancer therapy-leukemia.
Discussion
Principal Findings
We found 24 RCTs of VR for older adults with serious illness that encompassed diverse conditions, such as stroke, cancer, cardiovascular disease, and COPD. Among these studies, VR has been applied to improve anxiety and pain, as measured by the HADS, State Anxiety Inventory, or NPS, or mobility and strength, as measured by the Fugl-Meyer upper extremity assessment, proprioception, or orientation metrics. In this review, short VR experiences were typically used to improve outcomes related to anxiety and pain, while longer ones were used to improve mobility and strength after stroke. Training, supervision, and assistance provided were described in 5 studies [38,40,43,46,54]. Of the included RCTs, all 24 studies addressed older adults; however, only a few focused entirely on the older adult population: 3 studies (12%) included adults with an average age of 66 to 70 years [44,50,56], and only 1 study (4%) included older adults with an average age of >75 years [37]. From the 24 RCTs included in this systematic review, 7 (29%) studies adhered to all 8 gold standard VR consensus standards criteria, and all studies (100%) adhered to at least 5 criteria.
Although there are emerging bodies of evidence on VR use for acute pain, physical therapy, and mental health, we found relatively few studies that met our criteria, focused on symptomatic and functional aspects of serious illness or their use for older adults [59-61]. Acute pain and pain associated with serious illness are distinct, as suggested by the total pain model for serious illness by Saunders; are multifactorial; and explicitly consider physical, emotional, social, and existential factors in worsening symptoms [62,63]. Function is also impaired to a greater degree in older adults, and the average American lives with 1 to 2 ADL disabilities during the last 2 years of life [64]. Comorbidity is common among older adults, and underlying conditions and treatments can interact to exacerbate symptoms [65]. Owing to this, the same interventions used to manage acute pain may not be efficacious for managing pain associated with serious illness, especially among older adults with serious illnesses.
The practicality and efficacy of VR for older patients may be limited by difficulty using the technology, cost, and limited accessibility in medical settings [66]. For example, an approximately 1- to 2-pound VR headset may be relatively heavy, which is challenging for patients with frailty, as well as those with a serious illness [67]. In many cases, older patients may tend to be unfamiliar with new technologies and, therefore, may require supervision and assistance. This role can be fulfilled with caregivers, friends, or clinicians. In addition, immersive VR can cause motion sickness, which is a concern for older adults with serious illnesses, and are costlier than nonimmersive therapies [68]. Unfortunately, 5 (21%) of the 24 assessed studies lacked descriptions of supervision, training, or assistance provided, which may limit the ability of other researchers or providers to translate the results to their settings [45,48,50,51,56]. Therefore, VR assessments in older adults should include whether and how users were trained and supported, how their clinical condition impacted their ability to use the system, and how their ability to independently use VR was verified.
The extent to which VR treatment efficacy is reliant on media content remains unclear. This is particularly important because VR audio and visual media content varies generally within and between different VR systems. Furthermore, different clinical conditions and intervention goals may lead to the use of specific VR resources, interactive functionality, interactivity, and content. As a result, there are fundamental limitations for researchers and clinicians in understanding the mechanisms and efficacy of VR due to the opaqueness or lack of content descriptions in many publications [69]. In addition, subtleties in achieving high presence or in how perceived reality is portrayed may significantly impact the clinical impact and patient satisfaction. Therefore, better-published specifications of VR media, such as soundscapes, public accessibility, and other features, are required to better evaluate and clinically apply VR to patients [11].
This evaluation is limited by the sparse availability of specific VR content that was used in the previous studies. In addition, the outcomes related to patients’ quality of life in the different studies were heterogeneous, and therefore, a quantitative synthesis was not possible. These factors, combined, limited the ability to characterize the effects of specific VR features on patient outcomes. However, this may be a representation of an evolving field with limited reporting guidelines. In addition, this study focused specifically on immersive VR, and future research can further examine the effectiveness of different types of VR. One of the original aims of this study was to compare individual differences in VR effectiveness (eg, by gender, race, and ethnicity); however, this was not possible due to a lack of sufficient detail in included studies. Nonetheless, this systematic review provides researchers and clinicians with a detailed overview of the current state of the literature for older adults with serious illness, as well as an awareness and emphasis on the need to follow standard best practices to enhance VR research rigor. Future directions to build upon this systematic review include evaluating different types of VR media and frequency and duration to target improvements in specific outcomes in patients with serious illness. Future studies may also consider more structured supervision and training for VR use for older adults and determine whether this leads to increased compliance and efficacy of VR to improve outcomes in serious illness. Finally, future research can focus on making VR more accessible to everyone, including older adults [70].
Conclusions
Our systematic review identified a growing body of research evaluating VR apps for older adults with serious illness through RCTs. The literature review illustrates the potential of VR in this population and finds promising but limited extant evidence. These limitations also highlight an important gap in the development and understanding of using VR to improve health and wellness, which are crucial to address for rapidly aging populations.
Acknowledgments
This study would not have been possible without the support of Stanford University School of Medicine and the VA Center for Innovation to Implementation.
Abbreviations
- ADL
activity of daily living
- COPD
chronic obstructive pulmonary disease
- HADS
Hospital Anxiety and Depression Scale
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
randomized controlled trial
- VR
virtual reality
Search strategy.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Abstraction form.
Risk of bias of included studies.
Data Availability
The datasets analyzed during this study are publicly available, as detailed in the Methods section.
Footnotes
Authors' Contributions: BM contributed to the project ideation, data collection, data analysis, manuscript writing, and manuscript editing. AK contributed to the project ideation, data collection, data analysis, and manuscript editing. NI contributed to the data collection, data analysis, and manuscript writing. SF, JB, BB, and KG contributed to the project ideation, data analysis, and manuscript editing. CK and TO contributed to manuscript editing. KL contributed to the project ideation, data collection, data analysis, manuscript editing, and overall project oversight. All authors read and approved the final version of this manuscript.
Conflicts of Interest: Author TO contributed to the project while working at the VA, however, is now employed at Microsoft. After his participation in the project, he also recently became an advisor for the VR enabled company RadiusXR.
References
- 1.Sanders JJ, Curtis JR, Tulsky JA. Achieving goal-concordant care: a conceptual model and approach to measuring serious illness communication and its impact. J Palliat Med. 2018 Mar;21(S2):S17–27. doi: 10.1089/jpm.2017.0459. https://europepmc.org/abstract/MED/29091522 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, Elkind MS, Evenson KR, Eze-Nliam C, Ferguson JF, Generoso G, Ho JE, Kalani R, Khan SS, Kissela BM, Knutson KL, Levine DA, Lewis TT, Liu J, Loop MS, Ma J, Mussolino ME, Navaneethan SD, Perak AM, Poudel R, Rezk-Hanna M, Roth GA, Schroeder EB, Shah SH, Thacker EL, VanWagner LB, Virani SS, Voecks JH, Wang NY, Yaffe K, Martin SS. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022 Feb 22;145(8):e153–639. doi: 10.1161/CIR.0000000000001052. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000001052?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PubMed] [Google Scholar]
- 3.Kelley AS. Epidemiology of care for patients with serious illness. J Palliat Med. 2013 Jul;16(7):730–3. doi: 10.1089/jpm.2013.9498. https://europepmc.org/abstract/MED/23718871 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kelley AS, Bollens-Lund E. Identifying the population with serious illness: the "denominator" challenge. J Palliat Med. 2018 Mar;21(S2):S7–16. doi: 10.1089/jpm.2017.0548. https://europepmc.org/abstract/MED/29125784 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Murray SA, Kendall M, Boyd K, Sheikh A. Illness trajectories and palliative care. BMJ. 2005 Apr 30;330(7498):1007–11. doi: 10.1136/bmj.330.7498.1007. https://europepmc.org/abstract/MED/15860828 .330/7498/1007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ahmad FB, Anderson RN. The leading causes of death in the US for 2020. JAMA. 2021 May 11;325(18):1829–30. doi: 10.1001/jama.2021.5469. https://europepmc.org/abstract/MED/33787821 .2778234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.May P, Normand C, Cassel JB, Del Fabbro E, Fine RL, Menz R, Morrison CA, Penrod JD, Robinson C, Morrison RS. Economics of palliative care for hospitalized adults with serious illness: a meta-analysis. JAMA Intern Med. 2018 Jun 01;178(6):820–9. doi: 10.1001/jamainternmed.2018.0750. https://europepmc.org/abstract/MED/29710177 .2678833 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–67. doi: 10.2147/PROM.S156279. https://europepmc.org/abstract/MED/30464666 .prom-9-353 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Stone MJ. Goals of care at the end of life. Proc (Bayl Univ Med Cent) 2001 Apr 11;14(2):134–7. doi: 10.1080/08998280.2001.11927748. https://europepmc.org/abstract/MED/16369602 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hayes RD, Chang CK, Fernandes AC, Begum A, To D, Broadbent M, Hotopf M, Stewart R. Functional status and all-cause mortality in serious mental illness. PLoS One. 2012 Sep 6;7(9):e44613. doi: 10.1371/journal.pone.0044613. https://dx.plos.org/10.1371/journal.pone.0044613 .PONE-D-12-15838 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Javaid M, Haleem A. Virtual reality applications toward medical field. Clin Epidemiol Global Health. 2020 Jun;8(2):600–5. doi: 10.1016/j.cegh.2019.12.010. [DOI] [Google Scholar]
- 12.Park B, Kim Y, Park J, Choi H, Kim SE, Ryu H, Seo K. Integrating biomarkers from virtual reality and magnetic resonance imaging for the early detection of mild cognitive impairment using a multimodal learning approach: validation study. J Med Internet Res. 2024 Apr 17;26:e54538. doi: 10.2196/54538. https://www.jmir.org/2024//e54538/ v26i1e54538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Elavsky S, Knapova L, Janiš K, Cimler R, Kuhnova J, Cernicky T. Multiple perspectives on the adoption of SMART technologies for improving care of older people: mixed methods study. J Med Internet Res. 2024 Feb 07;26:e45492. doi: 10.2196/45492. https://www.jmir.org/2024//e45492/ v26i1e45492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sheng Y, Bond R, Jaiswal R, Dinsmore J, Doyle J. Augmenting k-means clustering with qualitative data to discover the engagement patterns of older adults with multimorbidity when using digital health technologies: proof-of-concept trial. J Med Internet Res. 2024 Mar 28;26:e46287. doi: 10.2196/46287. https://www.jmir.org/2024//e46287/ v26i1e46287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kardong-Edgren S, Farra SL, Alinier G, Young HM. A call to unify definitions of virtual reality. Clin Simul Nurs. 2019 Jun;31:28–34. doi: 10.1016/j.ecns.2019.02.006. [DOI] [Google Scholar]
- 16.Osborne TF, Arreola DM, Veigulis ZP, Morley C, Choudhry O, Lan W, Teague KR, Vega R, Mahajan SM. Augmented reality demonstration survey results from a veteran affairs medical center. Fed Pract. 2023 Mar;40(3):90–7. doi: 10.12788/fp.0364. https://europepmc.org/abstract/MED/37228426 .fp-40-03-90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rawlins CR, Veigulis Z, Hebert C, Curtin C, Osborne TF. Effect of immersive virtual reality on pain and anxiety at a veterans affairs health care facility. Front Virtual Real. 2021 Oct 5;2:719681. doi: 10.3389/frvir.2021.719681. [DOI] [Google Scholar]
- 18.McCullough M, Osborne TF, Rawlins C, Reitz RJ 3rd, Fox PM, Curtin C. The impact of virtual reality on the patients and providers experience in wide-awake, local-only hand surgery. J Hand Surg Glob Online. 2023 May;5(3):290–3. doi: 10.1016/j.jhsg.2023.01.014. https://linkinghub.elsevier.com/retrieve/pii/S2589-5141(23)00018-X .S2589-5141(23)00018-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Corregidor-Sánchez AI, Segura-Fragoso A, Rodríguez-Hernández M, Jiménez-Rojas C, Polonio-López B, Criado-Álvarez JJ. Effectiveness of virtual reality technology on functional mobility of older adults: systematic review and meta-analysis. Age Ageing. 2021 Feb 26;50(2):370–9. doi: 10.1093/ageing/afaa197.5926560 [DOI] [PubMed] [Google Scholar]
- 20.Mo J, Vickerstaff V, Minton O, Tavabie S, Taubert M, Stone P, White N. How effective is virtual reality technology in palliative care? A systematic review and meta-analysis. Palliat Med. 2022 Jul 30;36(7):1047–58. doi: 10.1177/02692163221099584. https://journals.sagepub.com/doi/abs/10.1177/02692163221099584?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dermody G, Whitehead L, Wilson G, Glass C. The role of virtual reality in improving health outcomes for community-dwelling older adults: systematic review. J Med Internet Res. 2020 Jun 01;22(6):e17331. doi: 10.2196/17331. https://www.jmir.org/2020/6/e17331/ v22i6e17331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Birckhead B, Khalil C, Liu X, Conovitz S, Rizzo A, Danovitch I, Bullock K, Spiegel B. Recommendations for methodology of virtual reality clinical trials in health care by an international working group: iterative study. JMIR Ment Health. 2019 Jan 31;6(1):e11973. doi: 10.2196/11973. https://mental.jmir.org/2019/1/e11973/ v6i1e11973 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Välimäki M, Hätönen HM, Lahti ME, Kurki M, Hottinen A, Metsäranta K, Riihimäki T, Adams CE. Virtual reality for treatment compliance for people with serious mental illness. Cochrane Database Syst Rev. 2014 Oct 08;2014(10):CD009928. doi: 10.1002/14651858.CD009928.pub2. https://europepmc.org/abstract/MED/25300174 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ose SO, Færevik H, Kaasbøll J, Lindgren M, Thaulow K, Antonsen S, Burkeland O. Exploring the potential for use of virtual reality technology in the treatment of severe mental illness among adults in mid-Norway: collaborative research between clinicians and researchers. JMIR Form Res. 2019 Jun 10;3(2):e13633. doi: 10.2196/13633. https://formative.jmir.org/2019/2/e13633/ v3i2e13633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. https://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015 Jan 02;350:g7647. doi: 10.1136/bmj.g7647. https://www.bmj.com/lookup/pmidlookup?view=long&pmid=25555855 . [DOI] [PubMed] [Google Scholar]
- 27.Bailenson J, Fereydooni S, Giannitrapani K, Kraft A, Lorenz K, Maheta B, Schapira L, Wong HN. Using virtual reality to improve quality of life among seriously ill adults: a systematic review of randomized control trials. PROSPERO 2022 CRD42022346178. 2022. [2025-01-05]. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022346178 .
- 28.Hartmann KE, Matchar DB, Chang SM. Chapter 6: Assessing applicability of medical test studies in systematic reviews. In: Chang SM, Matchar DB, Smetana GW, Umscheid CA, editors. Methods Guide for Medical Test Reviews [Internet] Rockville, MD: Agency for Healthcare Research and Quality (US); 2012. Jun, [PubMed] [Google Scholar]
- 29.Deyo RA. Measuring functional outcomes in therapeutic trials for chronic disease. Control Clin Trials. 1984 Sep;5(3):223–40. doi: 10.1016/0197-2456(84)90026-6.0197-2456(84)90026-6 [DOI] [PubMed] [Google Scholar]
- 30.Deshpande PR, Rajan S, Sudeepthi BL, Abdul Nazir CP. Patient-reported outcomes: a new era in clinical research. Perspect Clin Res. 2011 Oct;2(4):137–44. doi: 10.4103/2229-3485.86879. http://www.picronline.org/article.asp?issn=2229-3485;year=2011;volume=2;issue=4;spage=137;epage=144;aulast=Deshpande .PCR-2-137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fung CH, Hays RD. Prospects and challenges in using patient-reported outcomes in clinical practice. Qual Life Res. 2008 Dec 18;17(10):1297–302. doi: 10.1007/s11136-008-9379-5. https://europepmc.org/abstract/MED/18709564 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Van der Mierden S, Tsaioun K, Bleich A, Leenaars CH. Software tools for literature screening in systematic reviews in biomedical research. ALTEX. 2019;36(3):508–17. doi: 10.14573/altex.1902131. https://doi.org/10.14573/altex.1902131 . [DOI] [PubMed] [Google Scholar]
- 33.Lundh A, Gøtzsche PC. Recommendations by Cochrane Review Groups for assessment of the risk of bias in studies. BMC Med Res Methodol. 2008 Apr 21;8:22. doi: 10.1186/1471-2288-8-22. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-8-22 .1471-2288-8-22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Henderson LK, Craig JC, Willis NS, Tovey D, Webster AC. How to write a Cochrane systematic review. Nephrology (Carlton) 2010 Sep;15(6):617–24. doi: 10.1111/j.1440-1797.2010.01380.x. [DOI] [PubMed] [Google Scholar]
- 35.Bani Mohammad E, Ahmad M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: a randomized control trial. Palliat Support Care. 2018 Sep 10;17(1):29–34. doi: 10.1017/s1478951518000639. [DOI] [PubMed] [Google Scholar]
- 36.Burrai F, Ortu S, Marinucci M, De Marinis MG, Piredda M. Effectiveness of immersive virtual reality in people with cancer undergoing antiblastic therapy: a randomized controlled trial. Semin Oncol Nurs. 2023 Aug;39(4):151470. doi: 10.1016/j.soncn.2023.151470. https://linkinghub.elsevier.com/retrieve/pii/S0749-2081(23)00114-6 .S0749-2081(23)00114-6 [DOI] [PubMed] [Google Scholar]
- 37.Chatterjee K, Buchanan A, Cottrell K, Hughes S, Day TW, John NW. Immersive virtual reality for the cognitive rehabilitation of stroke survivors. IEEE Trans Neural Syst Rehabil Eng. 2022;30:719–28. doi: 10.1109/tnsre.2022.3158731. [DOI] [PubMed] [Google Scholar]
- 38.Chirico A, Maiorano P, Indovina P, Milanese C, Giordano GG, Alivernini F, Iodice G, Gallo L, De Pietro G, Lucidi F, Botti G, De Laurentiis M, Giordano A. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J Cell Physiol. 2020 Jun 20;235(6):5353–62. doi: 10.1002/jcp.29422. [DOI] [PubMed] [Google Scholar]
- 39.Groninger H, Stewart D, Fisher JM, Tefera E, Cowgill J, Mete M. Virtual reality for pain management in advanced heart failure: a randomized controlled study. Palliat Med. 2021 Dec 25;35(10):2008–16. doi: 10.1177/02692163211041273. [DOI] [PubMed] [Google Scholar]
- 40.Hsu HY, Kuo LC, Lin YC, Su FC, Yang TH, Lin CW. Effects of a virtual reality-based mirror therapy program on improving sensorimotor function of hands in chronic stroke patients: a randomized controlled trial. Neurorehabil Neural Repair. 2022 Jun 28;36(6):335–45. doi: 10.1177/15459683221081430. [DOI] [PubMed] [Google Scholar]
- 41.Huang CY, Chiang WC, Yeh YC, Fan SC, Yang WH, Kuo HC, Li PC. Effects of virtual reality-based motor control training on inflammation, oxidative stress, neuroplasticity and upper limb motor function in patients with chronic stroke: a randomized controlled trial. BMC Neurol. 2022 Jan 11;22(1):21. doi: 10.1186/s12883-021-02547-4. https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-021-02547-4 .10.1186/s12883-021-02547-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Huang Q, Jiang X, Jin Y, Wu B, Vigotsky AD, Fan L, Gu P, Tu W, Huang L, Jiang S. Immersive virtual reality-based rehabilitation for subacute stroke: a randomized controlled trial. J Neurol. 2024 Mar 10;271(3):1256–66. doi: 10.1007/s00415-023-12060-y. https://europepmc.org/abstract/MED/37947856 .10.1007/s00415-023-12060-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jo S, Jang H, Kim H, Song C. 360° immersive virtual reality-based mirror therapy for upper extremity function and satisfaction among stroke patients: a randomized controlled trial. Eur J Phys Rehabil Med. 2024 Apr;60(2):207–15. doi: 10.23736/s1973-9087.24.08275-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Laghlam D, Naudin C, Coroyer L, Aidan V, Malvy J, Rahoual G, Estagnasié P, Squara P. Virtual reality vs. Kalinox® for management of pain in intensive care unit after cardiac surgery: a randomized study. Ann Intensive Care. 2021 May 13;11(1):74. doi: 10.1186/s13613-021-00866-w. https://europepmc.org/abstract/MED/33983498 .10.1186/s13613-021-00866-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lee SY, Kang J. Effect of virtual reality meditation on sleep quality of intensive care unit patients: a randomised controlled trial. Intensive Crit Care Nurs. 2020 Aug;59:102849. doi: 10.1016/j.iccn.2020.102849.S0964-3397(20)30052-5 [DOI] [PubMed] [Google Scholar]
- 46.Mekbib DB, Debeli DK, Zhang L, Fang S, Shao Y, Yang W, Han J, Jiang H, Zhu J, Zhao Z, Cheng R, Ye X, Zhang J, Xu D. A novel fully immersive virtual reality environment for upper extremity rehabilitation in patients with stroke. Ann N Y Acad Sci. 2021 Jun 14;1493(1):75–89. doi: 10.1111/nyas.14554. [DOI] [PubMed] [Google Scholar]
- 47.Menekli T, Yaprak B, Doğan R. The effect of virtual reality distraction intervention on pain, anxiety, and vital signs of oncology patients undergoing port catheter implantation: a randomized controlled study. Pain Manag Nurs. 2022 Oct;23(5):585–90. doi: 10.1016/j.pmn.2022.03.004.S1524-9042(22)00095-9 [DOI] [PubMed] [Google Scholar]
- 48.Ögün MN, Kurul R, Yaşar MF, Turkoglu SA, Avci S, Yildiz N. Effect of leap motion-based 3D immersive virtual reality usage on upper extremity function in ischemic stroke patients. Arq Neuro Psiquiatr. 2019 Oct;77(10):681–8. doi: 10.1590/0004-282x20190129. [DOI] [PubMed] [Google Scholar]
- 49.Park YH, Lee CH, Lee BH. Clinical usefulness of the virtual reality-based postural control training on the gait ability in patients with stroke. J Exerc Rehabil. 2013 Oct 31;9(5):489–94. doi: 10.12965/jer.130066. https://europepmc.org/abstract/MED/24282810 .jer-9-5-489-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Rousseaux F, Dardenne N, Massion PB, Ledoux D, Bicego A, Donneau AF, Faymonville ME, Nyssen AS, Vanhaudenhuyse A. Virtual reality and hypnosis for anxiety and pain management in intensive care units: a prospective randomised trial among cardiac surgery patients. Eur J Anaesthesiol. 2022 Jan 01;39(1):58–66. doi: 10.1097/EJA.0000000000001633. https://hdl.handle.net/2268/265123 .00003643-202201000-00007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Rutkowski S, Szczegielniak J, Szczepańska-Gieracha J. Evaluation of the efficacy of immersive virtual reality therapy as a method supporting pulmonary rehabilitation: a randomized controlled trial. J Clin Med. 2021 Jan 18;10(2):352. doi: 10.3390/jcm10020352. https://www.mdpi.com/resolver?pii=jcm10020352 .jcm10020352 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Shin J, Chang JS, Kim JS, An JY, Chung SY, Yoon SY, Kim YB. An investigation of the effect of virtual reality on alleviating anxiety in patients with breast cancer undergoing radiation therapy: a randomized controlled trial. Int J Radiat Oncol Biol Phys. 2023 Dec 01;117(5):1191–9. doi: 10.1016/j.ijrobp.2023.06.275.S0360-3016(23)04706-5 [DOI] [PubMed] [Google Scholar]
- 53.Song YH, Lee HM. Effect of immersive virtual reality-based bilateral arm training in patients with chronic stroke. Brain Sci. 2021 Aug 03;11(8):1032. doi: 10.3390/brainsci11081032. https://www.mdpi.com/resolver?pii=brainsci11081032 .brainsci11081032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Spiegel B, Fuller G, Lopez M, Dupuy T, Noah B, Howard A, Albert M, Tashjian V, Lam R, Ahn J, Dailey F, Rosen BT, Vrahas M, Little M, Garlich J, Dzubur E, IsHak W, Danovitch I. Virtual reality for management of pain in hospitalized patients: a randomized comparative effectiveness trial. PLoS One. 2019 Aug 14;14(8):e0219115. doi: 10.1371/journal.pone.0219115. https://dx.plos.org/10.1371/journal.pone.0219115 .PONE-D-18-32917 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Torres García A, Morcillo Serra C, Argilés Huguet M, González Gardó L, Abad Esteve A, Ramos Quiroga JA. Efficacy of a virtual reality intervention for reducing anxiety, depression, and increasing disease coping in patients with breast cancer before their first chemotherapy dose. Cogn Ther Res. 2023 Oct 27;48(3):451–65. doi: 10.1007/s10608-023-10440-2. [DOI] [Google Scholar]
- 56.Turrado V, Guzmán Y, Jiménez-Lillo J, Villegas E, de Lacy FB, Blanch J, Balibrea JM, Lacy A. Exposure to virtual reality as a tool to reduce peri-operative anxiety in patients undergoing colorectal cancer surgery: a single-center prospective randomized clinical trial. Surg Endosc. 2021 Jul;35(7):4042–7. doi: 10.1007/s00464-021-08407-z.10.1007/s00464-021-08407-z [DOI] [PubMed] [Google Scholar]
- 57.Uslu A, Arslan S. The effect of using virtual reality glasses on anxiety and fatigue in women with breast cancer receiving adjuvant chemotherapy: a pretest-posttest randomized controlled study. Semin Oncol Nurs. 2023 Oct;39(5):151503. doi: 10.1016/j.soncn.2023.151503.S0749-2081(23)00152-3 [DOI] [PubMed] [Google Scholar]
- 58.Zhang B, Jin X, Kuang X, Shen B, Qiu D, Peng J, Chen E, Dai X, Chen X, Wong CL. Effects of a virtual reality-based meditation intervention on anxiety and depression among patients with acute leukemia during induction chemotherapy: a randomized controlled trial. Cancer Nurs. 2023 Jan 23;47(3):E159–67. doi: 10.1097/NCC.0000000000001206.00002820-990000000-00104 [DOI] [PubMed] [Google Scholar]
- 59.Feng H, Li C, Liu J, Wang L, Ma J, Li G, Gan L, Shang X, Wu Z. Virtual reality rehabilitation versus conventional physical therapy for improving balance and gait in Parkinson’s disease patients: a randomized controlled trial. Med Sci Monit. 2019 Jun 05;25:4186–92. doi: 10.12659/msm.916455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Smith V, Warty RR, Sursas JA, Payne O, Nair A, Krishnan S, da Silva Costa F, Wallace EM, Vollenhoven B. The effectiveness of virtual reality in managing acute pain and anxiety for medical inpatients: systematic review. J Med Internet Res. 2020 Nov 02;22(11):e17980. doi: 10.2196/17980. https://www.jmir.org/2020/11/e17980/ v22i11e17980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Baghaei N, Chitale V, Hlasnik A, Stemmet L, Liang HN, Porter R. Virtual reality for supporting the treatment of depression and anxiety: scoping review. JMIR Ment Health. 2021 Sep 23;8(9):e29681. doi: 10.2196/29681. https://mental.jmir.org/2021/9/e29681/ v8i9e29681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ong CK, Forbes D. Embracing Cicely Saunders's concept of total pain. BMJ. 2005 Sep 10;331(7516):576–7. doi: 10.1136/bmj.331.7516.576-d. https://europepmc.org/abstract/MED/16150775 .331/7516/576-d [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Clark D. 'Total pain', disciplinary power and the body in the work of Cicely Saunders, 1958-1967. Soc Sci Med. 1999 Sep;49(6):727–36. doi: 10.1016/s0277-9536(99)00098-2.S0277953699000982 [DOI] [PubMed] [Google Scholar]
- 64.Smith AK, Walter LC, Miao Y, Boscardin WJ, Covinsky KE. Disability during the last two years of life. JAMA Intern Med. 2013 Sep 09;173(16):1506–13. doi: 10.1001/jamainternmed.2013.8738. https://europepmc.org/abstract/MED/23836120 .1710125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Desbiens NA, Wu AW, Broste SK, Wenger NS, Connors AF Jr, Lynn J, Yasui Y, Phillips RS, Fulkerson W. Pain and satisfaction with pain control in seriously ill hospitalized adults: findings from the SUPPORT research investigations. For the SUPPORT investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. Crit Care Med. 1996 Dec;24(12):1953–61. doi: 10.1097/00003246-199612000-00005. [DOI] [PubMed] [Google Scholar]
- 66.Baker S, Waycott J, Robertson E, Carrasco R, Neves BB, Hampson R, Vetere F. Evaluating the use of interactive virtual reality technology with older adults living in residential aged care. Inf Process Manag. 2020 May;57(3):102105. doi: 10.1016/j.ipm.2019.102105. [DOI] [Google Scholar]
- 67.Lee LN, Kim MJ, Hwang WJ. Potential of augmented reality and virtual reality technologies to promote wellbeing in older adults. Appl Sci. 2019 Aug 30;9(17):3556–847. doi: 10.3390/app9173556. https://journals.physiology.org/doi/10.1152/jn.00931.2017?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [Google Scholar]
- 68.Lee J, Kim M, Kim J. A study on immersion and VR sickness in walking interaction for immersive virtual reality applications. Symmetry. 2017 May 22;9(5):78. doi: 10.3390/sym9050078. [DOI] [Google Scholar]
- 69.Mazurek J, Kiper P, Cieślik B, Rutkowski S, Mehlich K, Turolla A, Szczepańska-Gieracha J. Virtual reality in medicine: a brief overview and future research directions. Hum Mov. 2019 May 27;20(3):16–22. doi: 10.5114/hm.2019.83529. [DOI] [Google Scholar]
- 70.Peck TC, McMullen KA, Quarles J. DiVRsify: break the cycle and develop VR for everyone. IEEE Comput Graph Appl. 2021 Nov 1;41(6):133–42. doi: 10.1109/mcg.2021.3113455. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy.
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Abstraction form.
Risk of bias of included studies.
Data Availability Statement
The datasets analyzed during this study are publicly available, as detailed in the Methods section.