

Abstract
Background
Respectful Maternal Care (RMC) is a crucial strategy for improving the quality of maternity care and reducing mortality and morbidity among mothers. This study aimed to evaluate the effect of an RMC educational intervention on reducing mistreatment during maternal care.
Methods
A quasi-experimental study was conducted in two intervention hospitals and two control hospitals affiliated with Tehran University of Medical Sciences. Initially, the provision of RMC in all four hospitals was assessed through an RMC questionnaire completed by newly delivered mothers (n = 357) in a cross-sectional study. Subsequently, an educational intervention was designed and implemented from September to November 2020 exclusively in the two intervention hospitals, targeting midwives working in the delivery department. Approximately four months post-intervention, in June 2021, the status of RMC was evaluated in all hospitals through a cross-sectional survey of 383 newly delivered women. The differences in RMC scores between pre- and post-intervention between the two groups of hospitals were assessed. The Generalized Estimating Equations (GEE) model was used to analyze the effectiveness of the educational intervention in practicing RMC while controlling for background variables.
Results
Mothers who received delivery services at certain hospitals, had lower levels of education, or were younger were more likely to experience disrespectful maternal care during labor and delivery. During the baseline phase, the intervention and control hospitals exhibited similar rates of mistreatment, with scores of 11.3 and 11.4, respectively. However, four months after implementing the intervention, the incidence of mistreatment in the control hospitals increased by approximately 7 points, while the score in the intervention hospitals decreased by around 10 points. Consequently, the difference between the intervention and control hospitals exceeded 17 points (p < 0.001), which was statistically significant.
Conclusions
The RMC educational intervention significantly reduced mistreatment during childbirth. To fully realize its potential, this intervention should be implemented alongside other strategies by all stakeholders, including providing specialized personnel, motivating staff, and educating mothers about their rights.
Keywords: Respectful maternity care, Childbirth, Educational intervention, Hospital, Iran
Background
Respectful Maternity Care (RMC) has been identified as a crucial strategy for reducing preventable maternal mortality and morbidity, thereby accelerating progress towards achieving the Sustainable Development Goals (SDGs) for improving maternal health [1]. These targets emphasize the importance of not only providing effective clinical interventions but also promoting respectful care for mothers. Additionally, RMC introduces standards for enhancing the quality of maternal and newborn care in health facilities. The World Health Organization (WHO) has highlighted the vital role of RMC as one of the eight key dimensions of care quality [1, 2]. According to the WHO definition, RMC involves providing care to women in a manner that respects their privacy, dignity, and autonomy, protects them from harm or mistreatment, and enables them to make informed decisions and receive continuous support before, during, and after childbirth [3]. Studies have shown that RMC can lead to positive experiences during natural childbirth, reduce cesarean delivery rates, improve access to care during pregnancy and childbirth, promote equitable care based on women’s needs and preferences, reduce health disparities, and ultimately decrease maternal mortality [4]. However, a growing body of evidence suggests that many women worldwide face disrespectful, abusive, and neglectful behavior during this vulnerable period [5].
There is no internationally agreed-upon definition of mistreatment or disrespect, as cultural norms and expectations of acceptable behavior vary widely across communities [6]. Nevertheless, the Charter of Reproductive Rights identifies a range of behaviors that constitute violence and abuse against women during childbirth, including physical violence, non-consensual care, breaches of confidentiality, verbal abuse, discrimination based on specific conditions and individual characteristics, abandonment or refusal of care, and detention in health centers due to non-payment of fees [7, 8]. These behaviors can cause significant psychological distress and physical harm, ultimately discouraging women from seeking skilled care during childbirth and putting their lives and health at risk [5, 9].
Iran has made notable progress in maternal health, achieving the fifth Millennium Development Goal (MDG) to improve maternal health [10]. Each year, approximately one million women give birth in Iran, with 96% of births taking place in health facilities with skilled birth attendance [11]. However, there is a lack of clearly defined strategies and operational indicators for providing RMC [12]. Furthermore, research on this topic in Iran is limited and primarily focused on mothers’ and caregivers’ perceptions and related factors [13–15]. Limited evidence suggests that the quality of childbirth care, including support, timely attention, accurate diagnosis and prevention, continuity of services, respect, security, and access to basic facilities, is not satisfactory [15, 16]. In a study by Hajizadeh et al., most women (75.7%) reported one or more types of perceived disrespectful maternity care. The most prevalent cases included restrictions on women’s choice of labor positions (44.3%) and restrictions on movement during labor (42.5%) [14]. A study by Shakibazadeh et al. found that all mothers surveyed experienced at least one instance of inappropriate behavior during childbirth care, including being confined to bed without a companion (99.7%), irrational demands, receiving cash or non-cash gifts (95.8%), inadequate care (73.4%), inappropriate behavior during vaginal examination (51.8%), verbal abuse (50.4%), physical abuse (12.9%), and stigma and discrimination (4.5%) [16]. Another study by Tajvar et al. revealed that while some midwives had good theoretical knowledge, they lacked practical professional skills, highlighting the need for improved human resource training as a barrier to providing RMC [17].
Given the significance of RMC and the relatively high prevalence of disrespectful maternity care reported in Iran [14, 16–18], as well as in other countries, particularly in Africa [6, 19–24], it is essential to provide evidence on ways to improve RMC for Iranian mothers. Numerous interventions globally include multi-component approaches, focusing on addressing healthcare providers’ attitudes, engaging local communities, and improving health systems, such as open maternity days, RMC training for providers, and user feedback, which collectively improve care experiences during childbirth [25]. Although previous studies have reported that provider education about RMC is essential and the impact of education on the knowledge and performance of midwives has been documented from their own perspective, the impact of this training on the performance of midwives from the recipient’s perspective has not yet been investigated in Iran [14–16]. Moridi et al. highlight that Iranian midwives prioritize maternal and infant well-being over preventing mistreatment, suggesting the importance of such interventions [14]. As no study has been conducted on the effectiveness of training-based interventions for midwives in Iran, this study aims to conduct a quasi-experimental study to examine the effectiveness of an educational intervention on midwives working in hospitals in improving RMC and reducing mistreatment in maternal care.
Methods
Study design
This study was conducted in four teaching hospitals affiliated with Tehran University of Medical Sciences (TUMS), all of which had delivery blocks. The study employed a quasi-experimental design, with two hospitals (Baharlu and Ziaian) randomly selected to implement an educational intervention program, and the other two hospitals (Arash and Valiasr) serving as controls. The study population, who were exposed to educational intervention, consisted of midwives working in labor and delivery units, as well as mothers who gave birth in these hospitals. The educational intervention focused on RMC and was implemented among midwives, but the effect of the intervention examined among mothers. The main study hypothesis was that our developed educational intervention program can significantly improve the behavior of midwives with mothers to provide higher RMC; thereby the satisfaction of mothers will be improved by receiving higher more respectful care. The study commenced in September 2020 and evaluation of intervention was completed in June 2021.
Inclusion and exclusion criteria for study participants
Forty midwives working in the two intervention hospitals were recruited to participate in the educational intervention. Inclusion criteria for midwives included: (1) holding at least a bachelor’s degree in midwifery, (2) having at least one year of experience working in labor and delivery units, and (3) at the time of the study, had direct responsibility and active participation in labor and childbirth care. Mothers who received care from participating midwives were also included in the study if they were undergoing a low-risk singleton natural birth and were medically cleared for discharge from the hospital. Both groups provided informed and voluntary consent to participate in the research. Exclusion criteria included unwillingness to participate, births resulting from non-natural methods, pre-term or post-term births, and multiple births.
Sample size calculation
The sample size for both the intervention and control groups, in post intervention phase, was determined based on a previous phase, with the results published earlier [16], using a proportion (P) of 0.3, a significance level (α) of 0.05, and a confidence coefficient of 90%, the estimated sample size was 383.
A stratified random sampling method was employed to select participants, with the proportionate share of each hospital determined based on their birth numbers and rates. Therefore, from the total of 383 mothers, 41 (10.7%) were from Valiasr Hospital, 150 (39.2%) from Arash Hospital, 150 (39.2%) from Baharlu Hospital, and 42 (11.0%) from Ziaian Hospital.
Study process and phases
The study consisted of four stages:
Assessment of RMC in all four hospitals pre intervention: This stage involved administering a structured questionnaire to 357 mothers who gave birth at hospitals affiliated to TUMS to access the status of provision of RMC in the hospitals. The results of this stage have been published elsewhere [16].
Designing an educational intervention on RMC: The educational intervention program was designed based on the results of stage 1, which identified gaps in RMC and related educational needs. A review of international experiences in designing and implementing training programs in RMC was conducted, and the WHO program and the White Ribbon Statement [26, 27] were utilized in compiling the content of the educational program. Expert opinions were sought to validate the content and ensure its cultural relevance and comprehensiveness. Content of this educational intervention is provided in Table 1.
Training of midwives in RMC: Forty midwives working in the two intervention hospitals were recruited to participate in the educational intervention. The educational intervention was conducted through two 8-hour workshops, which employed various educational methods, including lectures, scenario creation, film screening, brainstorming, and focused group discussion. The workshops were designed to address the challenges and solutions of providing RMC based on midwives’ experiences.
Measuring and comparing intervention and control group hospitals in terms of RMC: The state of RMC in the intervention group hospitals was compared to the control group hospitals approximately four months after the intervention in June 2021. Eligible women were 383 mothers who presented at the participating hospitals to give birth naturally were invited to complete the study questionnaire after delivery and on the day of discharge.
Table 1.
Content of the educational program designed for RMC intervention
| Session | General dimensions of education | Details of educational content | Teaching methods |
|---|---|---|---|
| 1 | Introduction | Presentation of the workshop program, the importance and generality of the topic | Lectures, questions and answers. Interactive |
| Dimensions of disrespect and violence | physical violence; care without consent; non-confidential care; Disrespectful care included verbal abuse; Discrimination based on the existence of special conditions and individual characteristics; abandonment or refusal of care; Detention at the service center | Lecture, question and answer Interactive and group discussion to along with the related educational video | |
| Approved reproductive rights | freedom from any abuse and improper treatment; Right to information, consent or refusal freely, respect to choices and preferences, including participation in maternal care; respecting the principle of confidentiality and privacy; dignity and respect; equality, freedom from discrimination, fair care; Benefit from timely care and the highest level of health accessible; Freedom, independence, autonomy and freedom from coercion | Lecture, question and answer Interactive and group discussion to Along with the related educational video | |
| The dimensions of RMC according to the White Ribbon Alliance and the statement of the WHO |
carefree from any harm (physical and verbal); Informed consent; independence; Privacy protection and confidential care; Nondiscrimination; respect when receiving care; enough attention |
Lecture, question and answer Interactive and group discussion to along with the related educational video | |
| Dimensions of RMC according to secondary studies |
freedom from harm and abuse; providing privacy and confidentiality; preserving the dignity of women; preparation Information perspective and informed consent request; Ensuring continued access to family support and society; improving the quality of the environment and resources; providing equitable maternity care; interaction with effective communication; respect for women’s choices that enhance their ability to give birth; Access to manpower Competent and motivated; providing efficient and effective care; Continuity of care |
Lecture, question and answer Interactive and group discussion to along with the related educational video | |
| 2 | Summarizing the contents of Session 1 | Summarizing the contents of the seven dimensions of RMC (verbal abuse, Physical abuse, stigmatization and discrimination, vaginal examinations, mobility, fluids and companionship, other demands reasonable and improper care of the mother) | Lecture, question and answer Interactive and group discussion to along with the related educational video |
| Summarizing the contents of Session 2 | Presenting scenarios related to the seven dimensions of RMC | Scenario creation, questions and answers, Interactive group discussion | |
| Focus group discussion session | Challenges and obstacles in the implementation of RMC from the participants’ point of view and providing solutions. | Brainstorming and group discussion |
Measurement tool and data collection
The standard questionnaire of RMC, validated by Bohren et al. in 2018 [23], was used as the measurement tool in the first and last stages of the study. The questionnaire consisted of two parts with a total of 97 questions, including 21 questions related to individual and background information of mothers and 76 questions related to seven dimensions of RMC. Higher scores indicated experiencing a higher level of disrespect in the hospital. The validity and reliability of this tool has been tested and confirmed in Iran by Shakibazadeh et al. Its content validity index (CVI) and content validity ratio (CVR) in this study are reported as 0.89 and 0.75 respectively. Also, the reliability level has been reported as 72% using Cohen’s Kappa coefficient [16].
Data was collected through a three-month period after intervention, during which the researcher obtained permission to enter the studied hospitals and visited the maternity department. Informed consent was obtained from eligible mothers who agreed to participate, and participants completed the questionnaire.
Data analysis
Data analysis was conducted using SPSS 24 software. Descriptive statistics, including mean, standard deviation, median, and range, were used to present the data. The Pearson Chi-Square test was used to compare the scores of misbehavior dimensions before and after the intervention. Multilevel regression analysis was employed to compare the trend of score changes between the intervention and control groups. Given the complex design of this study, finally Generalized Estimating Equations (GEE) model was used to analyze the effectiveness of the educational intervention in practicing RMC, controlling for background variables. The Bonferroni test was employed for multiple comparisons.
Ethical considerations
This study received ethical approval from the ethics committee of TUMS with the code of IR.TUMS.SRE.1397.015. Throughout all stages of the research, the researchers prioritized the convenience of the participants, maintaining confidentiality of information, and ensuring their voluntary and informed participation.
Results
As stated, 357 mothers who had recently given birth participated in the first phase (pre intervention) and 383 mothers participated in the next phase (post intervention). The results of the first phase have been published before [16]. In the second phase, the average age of mothers was 28 years. The number of pregnancies ranged from one to seven during their reproductive life. The majority of participants (43.3%) had a secondary education, were housewives (98.2%), and resided in Tehran (83.3%). Additionally, most participants (73.4%) reported an average economic status.
Incidence of disrespect in hospitals before and after the intervention
As shown in Table 2, the minimum, maximum, and mean (standard deviation) scores for reported incidents of disrespect were 4, 22, and 11.4 (3.3), respectively, before the intervention, and 1, 34, and 9.6 (10.4), respectively, after the intervention. Although the overall number of incidents decreased after the intervention, the variance in mothers’ experiences of disrespect increased. Before the intervention, each mother experienced at least four incidents of disrespect, whereas after the intervention, this number decreased. However, the maximum number of incidents observed before the intervention was 22 out of 66, which increased to 34 cases after the intervention.
Table 2.
Descriptive comparison of general misbehavior scores before and after the intervention
| Before the intervention (time 1) | After the intervention (time 2) | |
|---|---|---|
| Number of available data | 357 | 383 |
| Mean | 11.40 | 9.65 |
| Mode | 11.00 | 2.00 |
| Standard deviation | 3.03 | 10.40 |
| Range | 18.00 | 33.00 |
| Minimum | 4.00 | 1.00 |
| Maximum | 22.00 | 34.00 |
As shown in Table 3, based on the Pearson Chi-Square test, a significant decrease in disrespectful maternity care was observed in all dimensions (P < 0.005), except for “restrictions on mobility, fluids, and companionship” (P = 1), in the hospitals of the intervention group after the intervention. In contrast, the hospitals in the control group showed a significant increase in misbehavior in 4 out of 7 dimensions, but a significant reduction in “unreasonable demand, receiving money” dimension (P = 0.009). The other two dimensions had approximately the same status. Regarding all hospitals (n = 4), a significant decrease in disrespectful maternity care was observed in 4 out of 7 dimensions, and no significant difference between two periods in “physical” abuse, “stigma and discrimination” and “restrictions on mobility, fluids, and companionship”. Overall, a significant decrease was observed in the total score of misbehavior across all hospitals studied (P < 0.05).
Table 3.
Comparison of the frequency and prevalence of different dimensions of disrespectful maternity care in both groups of hospitals before and after the intervention
| Dimensions of disrespect | Interventional hospitals (n = 2) | Pearson Chi-Square | |||
|---|---|---|---|---|---|
| Before intervention | After intervention | ||||
| N = 181 | Percent | N = 192 | Percent | ||
| Verbal | 87 | 48.0 | 0 | 0 | P < 0.001 |
| Physical | 83 | 45.8 | 9 | 4.6 | P < 0.001 |
| Sigma and discrimination | 8 | 4.4 | 0 | 0 | P = 0.003 |
| Vaginal examination | 169 | 93.3 | 15 | 7.8 | P < 0.001 |
| Restriction in mobility, liquids, companions | 181 | 100 | 192 | 100 | P = 1 |
| Unreasonable demand, receiving money | 179 | 98.8 | 0 | 0 | P < 0.001 |
| Improper care of the mother | 128 | 70.7 | 0 | 0 | P < 0.001 |
| Control Hospitals (n = 2) | Pearson Chi-Square | ||||
|---|---|---|---|---|---|
| Before intervention | After intervention | ||||
| N = 176 | Percent | N = 191 | Percent | ||
| Verbal | 93 | 52.8 | 148 | 77.5 | P < 0.001 |
| Physical | 53 | 30.1 | 155 | 81.2 | P < 0.001 |
| Sigma and discrimination | 8 | 4.5 | 21 | 11.0 | P = 0.022 |
| Vaginal examination | 172 | 97.7 | 181 | 94.8 | P = 0.139 |
| Restriction in mobility, liquids, companions | 176 | 100 | 191 | 100 | P = 1 |
| Unreasonable demand, receiving money | 163 | 92.6 | 160 | 83.8 | P = 0.009 |
| Improper care of the mother | 117 | 66.5 | 162 | 84.8 | P < 0.001 |
| All hospitals (n = 4) | |||||
| Before intervention | After intervention | Pearson Chi-Square | |||
|---|---|---|---|---|---|
| N = 357 | Percent | N = 383 | Percent | ||
| Verbal | 180 | 50.4 | 148 | 38.6 | P < 0.001 |
| Physical | 136 | 38.1 | 164 | 42.8 | P = 0.055 |
| Sigma and discrimination | 16 | 4.5 | 21 | 50.5 | P = 0.466 |
| Vaginal examination | 340 | 95.5 | 196 | 51.2 | P < 0.001 |
| Restriction in mobility, liquids, companions | 357 | 100 | 383 | 100 | P = 1 |
| Unreasonable demand, receiving money | 340 | 95.8 | 160 | 41.8 | P = 0.002 |
| Improper care of the mother | 245 | 68.6 | 162 | 42.3 | P < 0.001 |
Relationship between investigated characteristics and the incidence of disrespectful maternal care during labor and delivery
An examination of the relationship between misbehavior and the characteristics investigated revealed that three factors were significantly associated with the reported incidence of misbehavior. These factors were the hospital where delivery services were received (Coefficient = 0.82, P < 0.001), the mother’s level of education (Coefficient = -0.078, P = 0.015), and the mother’s age (Coefficient = 0.079, P = 0.014). In other words, mothers who received delivery services at certain hospitals, had lower levels of education, or were younger, were more likely to experience disrespectful maternal care during labor and delivery.
Changes in the incidence of misbehavior due to educational intervention
The results of generalized estimating equations test presented in Table 4 indicate that the overall score for misbehavior decreased by 17.4 and 17.3 points in the first and second models, respectively. Both reductions were statistically significant (P < 0.001). This suggests that after the intervention, there was a significant difference of more than 17 points between the intervention and control hospitals in terms of the occurrence of misbehavior.
Table 4.
Results of the simple and controlled models of the Generalized Estimating Equations (GEE) test to determine the EFFECT of the educational intervention on general misbehavior.
| Parameter | Model 1-Crude analysis | *Model 2-adjusted analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| B | 95% Wald CI | P. value | B | 95% Wald CI | P. value | |||
| Lower | Upper | Lower | Upper | |||||
| Before intervention | Ref | – | – | Ref | – | – | ||
| After intervention | 7.00 | 6.58 | 7.42 | < 0.001 | 7.14 | 6.79 | 7.49 | < 0.001 |
| Control group | Ref | – | – | Ref | – | – | ||
| Intervention group | 0.000 | − 0.41 | 0.42 | 0.99 | -0.13 | -0.58 | 0.31 | 0.56 |
| Interaction between time and group | − 17.42 | − 17.95 | − 16.88 | < 0.001 | − 17.32 | − 17.97 | − 16.68 | < 0.001 |
| Dependent variable: Total Model 2 adjusted for contextual variables | ||||||||
As Fig. 1 shows, during the baseline phase, the intervention and control group hospitals exhibited similar incidence rates of misbehavior, with scores of 11.3 and 11.4, respectively. However, four months after the intervention was implemented, the incidence of misbehavior in the control hospitals increased by approximately 7 points, reaching a score of 18.2. In contrast, the score in the intervention hospitals decreased by around 10 points, reaching a score of 1.3. Consequently, with a difference of more than 17 points (p < 0.001), the difference between the intervention and control hospitals was statistically significant.
Fig. 1.
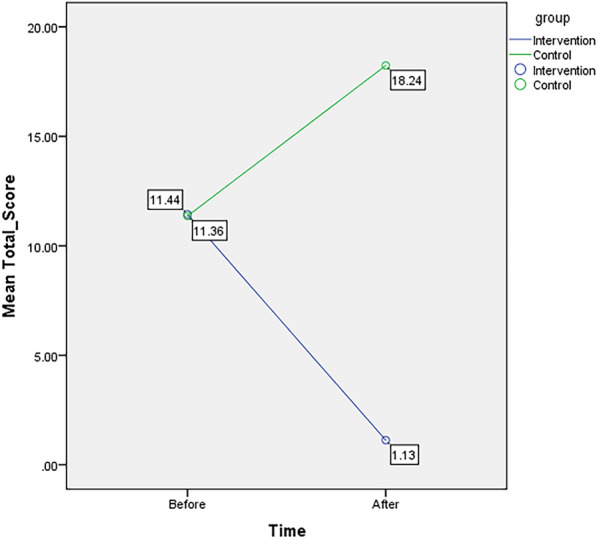
The effect of the educational intervention on the reduction of misbehavior before and after the intervention in intervention and control group hospitals
Discussion
This study is the first to investigate the effectiveness of an educational intervention promoting RMC in Iran. The study’s framework was based on the WHO’s and the White Ribbon Union’s [26, 27].published dimensions and frameworks for RMC during childbirth. The analysis of the findings revealed a significant reduction in the prevalence of abuse and disrespect following the implementation of the educational intervention in hospitals within the intervention group. Notably, the number of reported cases of disrespect decreased from 11 to 1 in intervention hospitals, whereas control hospitals experienced a worsening situation, with reported cases of disrespect increasing from 11 to 17 during the same period.
It is worth noting that the data collection before the intervention took place from June to September 2019, before the COVID-19 outbreak in Iran, and the data collection after the intervention occurred from March to June 2020. The increase in misbehavior in the control group may be attributed to the stressful conditions during the pandemic, which put immense psychological pressure on healthcare personnel. However, despite these challenging conditions, the intervention group showed a significant improvement in RMC, suggesting that the educational intervention had a positive impact on their behavior.
The results of this study demonstrate a significant improvement in the provision of RMC in hospitals within the intervention group. These findings are consistent with previous studies [6, 18–23, 28]. Almost all studies were from low- and middle-income African countries including Ghana, Kenya, Tanzania and Ethiopia and one study were from Spain as a high-income country. These educational interventions were different based on content, duration and teaching and evaluation methods. However, evidence supported the effectiveness of these interventions to improve knowledge/attitude of midwives and/or nurses regarding respectful maternity care, and woman-provider communication, and reduce women’s experience of disrespect and abuse. The adoption of RMC requires both scientific and interpersonal skills from healthcare providers, and thus, it is essential to identify obstacles and apply effective solutions to promote RMC [29].
Numerous training-based interventions have been conducted worldwide to address the increasing prevalence of misbehavior during childbirth. These interventions aim to reduce and eliminate disrespect and have demonstrated a positive impact on the incidence of misbehavior [6, 19, 22]. For instance, a study in Kenya by Abuya et al. used multifaceted interventions, including childbirth tours and training workshops for service recipients and providers, and reported a 7% reduction in the incidence of misbehavior during childbirth [22]. Similarly, a study in Ethiopia by Asefa et al. implemented interventions, including training for service providers, wall posters in delivery rooms, and support visits, and reported an 18% decrease in the prevalence of misbehavior during childbirth care [6].
In the present study, the most significant reduction in misbehavior occurred in the area of inattentive care, with a reduction of over 50% after the intervention. Other areas, such as vaginal examinations, improper care of the mother, and verbal abuse, also showed significant reductions after the intervention. These improvements in respectful behavior among providers during delivery care demonstrate the positive effect of the educational intervention on reducing misbehavior.
The findings of this study suggest that educational intervention had a positive impact on the knowledge, attitude, and behavior of providers, as well as an increase in their awareness of mothers’ rights during delivery care and improved communication between midwives and mothers. These results are consistent with the findings of Ratcliffe’s study [21], which demonstrated the positive impact of educational interventions on improving patient-provider communication and reducing misbehavior.
The study’s results also suggest that the educational intervention led to improved understanding, friendly support, and empathy among midwives, which is consistent with the findings of Oosthuizen and Kujawski’s studies [29, 30]. However, the intervention did not show significant improvements in other areas, such as the physical environment, the presence of a companion, and stigmatization and discrimination. Therefore, promoting RMC and reducing misbehavior cannot be fully achieved through educational interventions alone, but rather requires a multifaceted approach that includes changes to the health system, organization, and society as a whole [29, 31, 32].
Conclusions
The findings of this study demonstrate that an educational intervention focused on RMC can have a significant impact on reducing misbehavior during childbirth. However, to fully realize the provision of RMC and eliminate existing misbehavior, a comprehensive and collaborative approach is necessary. This requires the involvement of all stakeholders across various levels of the health system, including policymakers, planners, hospital managers, maternity ward supervisors, healthcare providers, and the community.
To institutionalize a culture of RMC throughout the healthcare system, it is essential to prioritize ongoing and periodic training for healthcare providers. Additionally, other interventions are recommended, such as: Ensuring the availability of specialist personnel in maternity departments; Motivating employees to provide high-quality care; Providing necessary infrastructure and resources to support RMC; Educating mothers about their rights and empowering them to advocate for themselves. By taking a multi-faceted approach, we can work towards eliminating misbehavior and promoting a culture of respect and dignity in maternity care.
This study had several limitations, including the timing of data collection after intervention, which coincided with the COVID-19 pandemic and the higher number of mistreatment in the control group compared to before intervention may be due to this, and the fact that the impact of the intervention on RMC was only evaluated once after the intervention. Additionally, the inability to conduct field observations and assess the actual delivery of care during childbirth meant that only the experiences reported by mothers were used.
Based on the results of this study, here are some important suggestions for both clinicians and policymakers to improve the RMC. By implementing these suggestions, clinicians and policymakers can work together to improve RMC and promote a culture of respect and dignity in maternity care.
Foster a culture of respect: Promote a culture of respect and dignity within the healthcare system and prioritize the well-being and autonomy of mothers.
Address power imbalances: Recognize and address power imbalances between healthcare providers and mothers, and work to create a more equitable and inclusive healthcare system.
Support research and evaluation: Support research and evaluation on RMC to better understand the barriers and facilitators of RMC and to identify effective interventions.
Collaborate with stakeholders: Collaborate with stakeholders, including mothers, families, healthcare providers, and community leaders, to promote RMC and improve healthcare outcomes.
Acknowledgments
This article originated from an MS thesis on health care management at the School of Public Health, Tehran University of Medical Sciences. The researchers would like to express their sincere gratitude to all those who have assisted and took part in the study.
Abbreviations
- RMC
Respectful maternity care
- GEE
Generalized estimating equations
- WHO
World Health Organization
- SDGs
Sustainable development goals
- MDGs
Millennium development goals
- TUMS
Tehran University of Medical Sciences
- OBD
Open birth days
Author contributions
M.T., SH.A., E.SH., Z.K.: assisted in conceptualization and design of the study and performed statistical analysis and interpretation of results. O.A., Z.K., AS. S and E.K.: drafted the manuscript. M.T., Z.K., and O.A. reviewed the manuscript. All authors read and approved the final manuscript.
Funding
The author received no specific funding for this work.
Availability of data and materials
The data used and analyzed in the present study will be made available upon reasonable request through the corresponding author.
Declarations
Ethics approval and consent to participate
The present study has obtained ethical approval from the Ethics Committee of Tehran University of Medical Science (TUMS) with the reference number IR.TUMS.SPH.REC.1397.015. In all stages of the research, the necessary information about the study and its objectives was provided to the participants, and informed consent was obtained from them before their participation in the study. Furthermore, their data was analyzed confidentially. The authors affirm that all procedures were conducted in compliance with the relevant guidelines and regulations (Declaration of Helsinki).
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Maryam Tajvar, Email: mtajvar@tums.ac.ir.
Zeinab Khaledian, Email: z-khaledian@razi.tums.ac.ir.
References
- 1.World Health Organization. Strategies toward ending preventable maternal mortality (EPMM). Geneva: World Health Organization; 2015. [Google Scholar]
- 2.World Health Organization. Standards for improving quality of maternal and newborn care in health facilities. Geneva: World Health Organization; 2016. [Google Scholar]
- 3.World Health Organization. WHO recommendations: Intrapartum care for a positive childbirth experience. Geneva: World Health Organization; 2018. [PubMed] [Google Scholar]
- 4.Shakibazadeh E, Namadian M, Bohren MA, Vogel JP, Rashidian R, NogueiraPileggi V. Respectful care during childbirth in health facilities globally: a qualitative evidence synthesis. BJOG. 2017. 10.1111/1471-0528.15015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Silveira MA, Mesenburg MA, Bertoldi AD, DeMola CL, Bassani DC, Domingues MR. The association between disrespect and abuse of women during childbirth and postpartum depression: findings from the 2015 Pelotas birth cohort study. J Affect Disord. 2019;256:441–7. 10.1016/j.jad.2019.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Asefa A, Morgan A, Gebremedhin S, et al. Mitigating the mistreatment of childbearing women: evaluation of respectful maternity care intervention in Ethiopian hospitals. BMJ Open. 2020;10: e038871. 10.1136/bmjopen-2020-38871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kassa ZY, Tsegaye B, Abeje A. Disrespect and abuse of women during the process of childbirth at health facilities in sub-Saharan Africa: a systematic review and meta-analysis. BMC Int Health Hum Rights. 2020; 20(23). [DOI] [PMC free article] [PubMed]
- 8.Asadi N, Salmani F, Salmani M. The relationship between aggressive behaviors of preschool children and the violence against Iranian women in the COVID-19 pandemic. BMC Women’s Health. 2022. 10.1186/s12905-022-01954-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Reed R, Sharman R, Inglis C. Women’s descriptions of childbirth trauma relating to care provider actions and interactions. BMC Pregnancy Childbirth. 2017. 10.1186/s12884-016-1197-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.The United Nations Population Fund. Maternal deaths halved in 20 years, but faster progress needed. United Nations, New York: The United Nations Population Fund; 2012. https://www.unfpa.org/press/maternal-deaths-halved-20-years-faster-progress-needed. Accessed September 25, 2019.
- 11.Pazandeh F, Huss R, Hirst J, House A, Baghban AA. An evaluation of the quality of care for women with low risk pregnancy: the use of evidence-based practice during labor and childbirth in four public hospitals in Tehran. Midwifery. 2015;31(11):1045–53. 10.1016/j.midw.2015.07.003. [DOI] [PubMed] [Google Scholar]
- 12.Ministry of Health and Medical Education. Instructions for promoting natural childbirth. Office of Hospital Management and Clinical Services Excellence. Tehran. Iran. 2018. [Origin Persian].
- 13.Ayoubi S, Pazandeh F, Simbar M, Moridi M, Zare E, Potrata B. A questionnaire to assess women’s perception of respectful maternity care. (WP-RMC): development and psychometric properties. Midwifery. 2020;80:102573. [DOI] [PubMed] [Google Scholar]
- 14.Hajizadeh K, Vaezi M, Meedya S, Mohammad AlizadehCharandabi S, Mirghafourvand M. Respectful maternity care and its related factors in maternal units of public and private hospitals in Tabriz: a sequential explanatory mixed method study protocol. Reprod Health. 2020;17(1):9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Moridi M, Pazandeh F, Hajian S, Potrata B. Midwives’ perspectives of respectful maternity care during childbirth: a qualitative study. PLoS ONE. 2020;15(3): e0229941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shakibazadeh A, Taherkhani F, Shojaeizadeh D, Yakani Nejad M, Tajvar M. Prevalence of abuse with mothers in the maternity ward of Tehran University of Medical Sciences hospitals and related factors. J School Nurs Midwifery Tehran Univ Medical Sci (Hayat). 2020;27(3):262–77. [Google Scholar]
- 17.Tajvar M, Shakibazadeh E, Alipour S, Khaledian Z. Challenges and barriers in moving toward respectful maternity care (RMC) in labor and childbirth: a phenomenology study. Payesh. 2022; 21(2):151–161. (persion). http://payeshjournal.ir/article-1-1711-en.html.
- 18.Mirghafourvand M, et al. Iranian mothers’ perspectives about aspects and determining factors of respectful maternity care during labor and delivery: a qualitative study. Tasvir-i Salamat. 2024;15(3):255-69. Available from: https://typeset.io/journals/tasvir-i-salamat-13vjuwn9/2024.
- 19.Asefa A, Morgan A, Bohren MA, Kermode M. Lessons learned through respectful maternity care training and its implementation in Ethiopia: an interventional mixed methods study. Reprod Health. 2020;17:103. 10.1186/s12978-020-00953-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wilson-Mitchell K, Eustace L, Robinson J, Shemdoe A, Simba S. Overview of literature on RMC and applications to Tanzania. Reprod Health. 2018;15(1):167. 10.1186/s12978-018-0599-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Webber. G, Chirangi B. Magatti N. Promoting respectful maternity care in rural Tanzania nurses’ experiences of the “health workers for change “program. BMC Health Serv Res. 2018; 18 (658). [DOI] [PMC free article] [PubMed]
- 22.Ratcliffe HL, Sando D, Lyatuu GW, Emil F, Mwanyika-sando M, Chalamilla G, LanGer A, McDonald KP. Mitigation disrespect and abuse during childbirth in Tanzania: an exploratory study of the effects of two facility-based interventions in a large public hospital. Report Health. 2016;13(1):79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Abuya T, Ndwiga C, Ritter J, et al. The effect of a multi-component intervention on disrespect and abuse during childbirth in Kenya. BMC Pregnancy Childbirth. 2015. 10.1186/s12884-015-0645-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dzomeku VM, Boamah Mensah AB, Nakua EK, Agbadi P, Lori JR, Donkor P. Midwives’ experiences of implementing respectful maternity care knowledge in daily maternity care practices after participating in a four-day RMC training. BMC Nurs. 2021;20(1):39. 10.1186/s12912-021-00559-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vivekanandan K, Sharma U, Sharma B, Subbiah N, Raina D. Respectful maternal care—need for educational interventions among maternal health care providers. ECS Trans. 2022;107(1):5899. 10.1149/10701.5899ecst. [Google Scholar]
- 26.The White Ribbon Alliance for Safe Motherhood. Respectful maternity care: The universal rights of childbearing women. White Ribb Alliance Safe Mother [Internet], 2011: 1–6. Available from: http://whiteribbonalliance.org/wpcontent/uploads/2013/10/final_rmc_charter.pdf.
- 27.WHO Reproductive Health Library. WHO recommendation on respectful maternity care. (February 2018). The WHO Reproductive Health Library; Geneva: World Health Organization, 2018.
- 28.Mena-Tudela D, González-Chordá VM, Soriano-Vidal FJ, Bonanad-Carrasco T, Centeno-Rico L, Vila-Candel R, Castro-Sánchez E, Gasch ÁC. Changes in health sciences students’ perception of obstetric violence after an educational intervention. Nurse Educ Today. 2020. 10.1016/j.nedt.2020.104364. [DOI] [PubMed] [Google Scholar]
- 29.Kujawski SA, Freedman LP, Ramsey K, Mbaruku G, Mbuyita S, Moyo W, Kruk M. Community and health system intervention to reduce disrespect and abuse during childbirth in Tanga Region, Tanzania: a comparative before-and-after study. PLoS Med. 2017;14(7):e1002341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Oosthuizen SJ, Bergh AM, Grimbeek J, Pattinson RC. CLEVER maternity care: a before-and-after study of women’s experience of childbirth in Tshwane, South Africa. Afr J Prim Health Care Fam Med. 2020;12(1):a2560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kasaye H, Sheehy A, Scarf V, Baird K. The roles of multi-component interventions in reducing mistreatment of women and enhancing respectful maternity care: a systematic review. BMC Pregnancy Childbirth. 2023;23(1):305. 10.1186/s12884-023-05640-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dhakal P, Creedy DK, Gamble J, Newnham E, McInnes R. Educational interventions to promote respectful maternity care: a mixed-methods systematic review. Nurse Educ Pract. 2022;60: 103317. 10.1016/j.nepr.2022.103317. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used and analyzed in the present study will be made available upon reasonable request through the corresponding author.