

Abstract
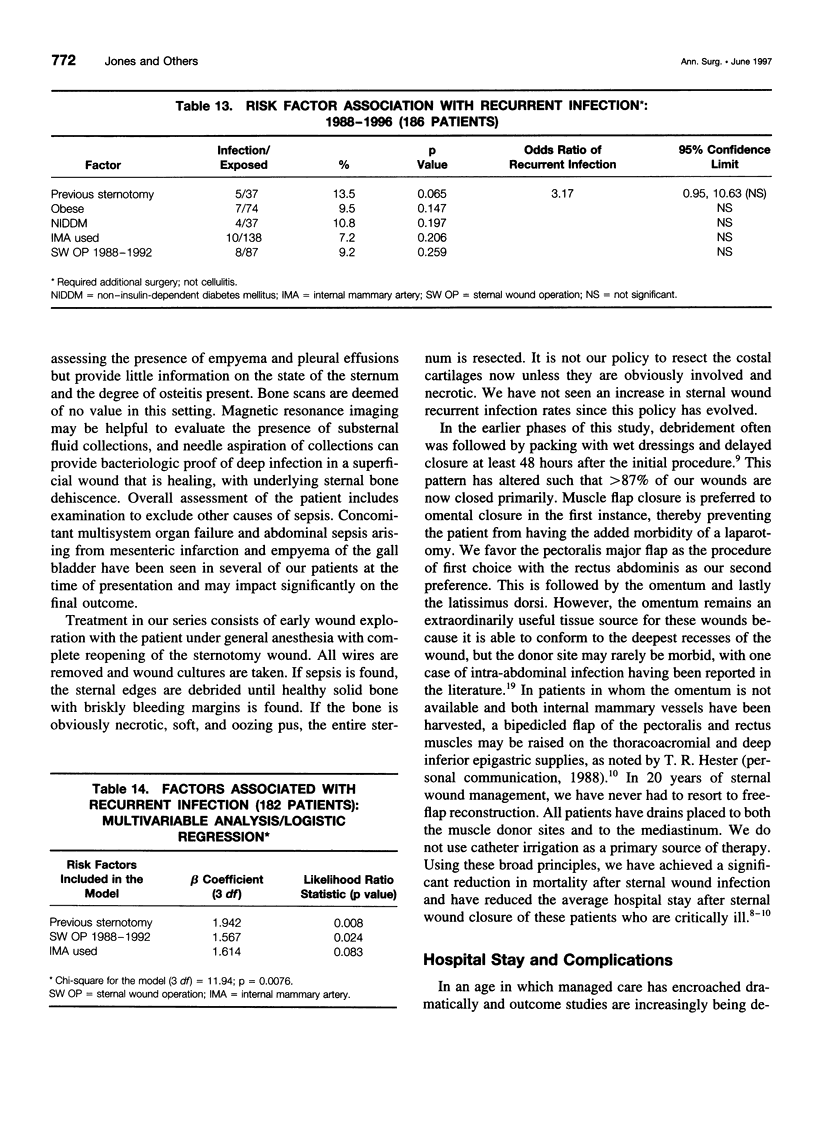
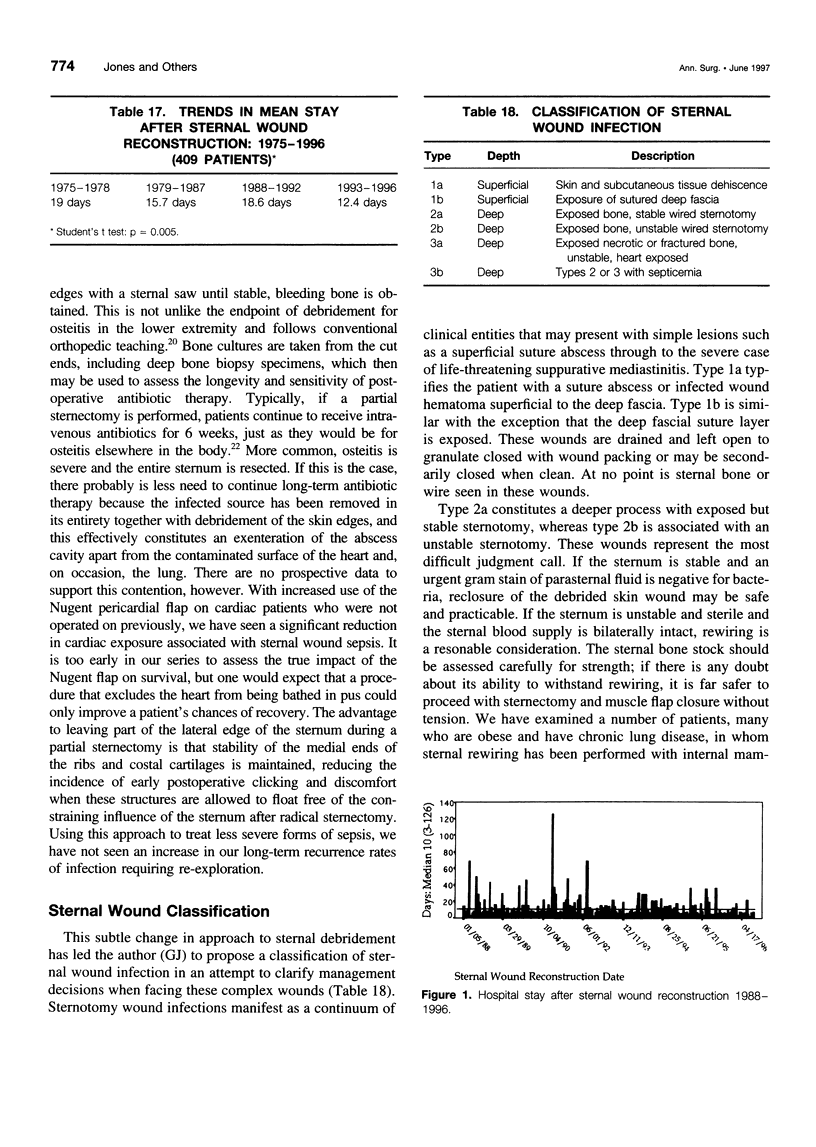
OBJECTIVE: The purpose of the study is to define those patient variables that contribute to morbidity and mortality of median sternotomy wound infection and the results of treatment by debridement and closure by muscle flaps. BACKGROUND: Infection of the median sternotomy wound after open heart surgery is a devastating complication associated with significant mortality. Twenty years ago, these wounds were treated with either open packing or antibiotic irrigation, with a mortality approaching 50% in some series. In 1975, the authors began treating these wounds with radical sternal debridement followed by closure using muscle or omental flaps. The mortality of sternal wound infection has dropped to < 10%. METHODS: The authors' total experience with 409 patients treated over 20 years is described in relation to flap choices, hospital days after sternal wound closure, and incidence rates of morbidity and mortality. One hundred eighty-six patients treated since January 1988 were studied to determine which patient variables had impact on rates of flap closure complications, recurrent sternal wound infection, or death. Variables included obesity, history of smoking, hypertension, diabetes, poststernotomy septicemia, internal mammary artery harvest, use of intra-aortic balloon pump, and perioperative myocardial infarction and were analyzed using chi square tests. Fisher's exact tests, and multivariable logistic regression analysis. RESULTS: The mortality rate over 20 years was 8.1% (33/49). Additional procedures for recurrent sternal wound infection were necessary in 5.1% of patients. Thirty-one patients (7.6%) required treatment for hematoma, and 11 patients (2.7%) required hernia repair. Among patients treated since 1988, variables strongly associated with mortality were septicemia (p < 0.00001), perioperative myocardial infarction (p = 0.006), and intra-aortic balloon pump (p = 0.0168). Factors associated with wound closure complications were intra-aortic balloon pump (p = 0.0287), hypertension (p = 0.0335), and history of smoking (p = 0.0741). Factors associated with recurrent infection were history of sternotomy (p = 0.008) and patients treated for sternal wound infection from 1988 to 1992 (p = 0.024). Mean hospital stay after sternal wound reconstruction declined from 18.6 days (1988-1992) to 12.4 days (1993-1996) (p = 0.005). To clarify management decisions of these difficult cases, a classification of sternal wound infection is presented. CONCLUSIONS: Using the principles of sternal wound debridement and early flap coverage, the authors have achieved a significant reduction in mortality after sternal wound infection and have reduced the mean hospital stay after sternal wound closure of these critically ill patients. Further reductions in mortality will depend on earlier detection of mediastinitis, before onset of septicemia, and ongoing improvements in the critical care of patients with multisystem organ failure.
Full text
PDF





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Acinapura A. J., Godfrey N., Romita M., Cunningham J., Jr, Adams P. X., Jacobowitz I. J., Rose D. M., Nealon T., Jr Surgical management of infected median sternotomy: closed irrigation vs. muscle flaps. J Cardiovasc Surg (Torino) 1985 Sep-Oct;26(5):443–446. [PubMed] [Google Scholar]
- Backer C. L., Pensler J. M., Tobin G. R., Mavroudis C. Vascularized muscle flaps for life-threatening mediastinal wounds in children. Ann Thorac Surg. 1994 Apr;57(4):797–802. doi: 10.1016/0003-4975(94)90179-1. [DOI] [PubMed] [Google Scholar]
- Bjerno T., Arendrup H. C., Alstrup P. Mediastinalinfektion efter åben hjertekirurgi. Ugeskr Laeger. 1990 Dec 3;152(49):3699–3702. [PubMed] [Google Scholar]
- Bryant L. R., Spencer F. C., Trinkle J. K. Treatment of median sternotomy infection by mediastinal irrigation with an antibiotic solution. Ann Surg. 1969 Jun;169(6):914–920. doi: 10.1097/00000658-196906000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frimpong-Boateng K., Warnecke H., Schüler S., Haverich A., Borst H. G. Transposition of the greater omentum for management of mediastinal infection following orthotopic heart transplantation: a case report. J Heart Transplant. 1986 Jul-Aug;5(4):330–331. [PubMed] [Google Scholar]
- Guedon C., Gandjbakhch I., Piwnica A., Bors V., Romano M., Pavie A., Lessana A., Mesnildray P., Touati G., Laborde F. Place actuelle de la chirurgie reconstructrice dans le traitement des médiastinites aiguës après chirurgie cardiaque. Chirurgie. 1992;118(1-2):36–41. [PubMed] [Google Scholar]
- JULIAN O. C., LOPEZ-BELIO M., DYE W. S., JAVID H., GROVE W. J. The median sternal incision in intracardiac surgery with extracorporeal circulation; a general evaluation of its use in heart surgery. Surgery. 1957 Oct;42(4):753–761. [PubMed] [Google Scholar]
- Jurkiewicz M. J., Arnold P. G. The omentum: an account of its use in the reconstruction of the chest wall. Ann Surg. 1977 May;185(5):548–554. doi: 10.1097/00000658-197705000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jurkiewicz M. J., Bostwick J., 3rd, Hester T. R., Bishop J. B., Craver J. Infected median sternotomy wound. Successful treatment by muscle flaps. Ann Surg. 1980 Jun;191(6):738–744. doi: 10.1097/00000658-198006000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karwande S. V., Renlund D. G., Olsen S. L., Gay W. A., Jr, Richenbacher W. E., Hawkins J. A., Millar R. C., Marks J. D. Mediastinitis in heart transplantation. Ann Thorac Surg. 1992 Dec;54(6):1039–1045. doi: 10.1016/0003-4975(92)90067-e. [DOI] [PubMed] [Google Scholar]
- Lee A. B., Jr, Schimert G., Shaktin S., Seigel J. H. Total excision of the sternum and thoracic pedicle transposition of the greater omentum; useful strategems in managing severe mediastinal infection following open heart surgery. Surgery. 1976 Oct;80(4):433–436. [PubMed] [Google Scholar]
- Nahai F., Rand R. P., Hester T. R., Bostwick J., 3rd, Jurkiewicz M. J. Primary treatment of the infected sternotomy wound with muscle flaps: a review of 211 consecutive cases. Plast Reconstr Surg. 1989 Sep;84(3):434–441. doi: 10.1097/00006534-198909000-00009. [DOI] [PubMed] [Google Scholar]
- Pairolero P. C., Arnold P. G. Management of recalcitrant median sternotomy wounds. J Thorac Cardiovasc Surg. 1984 Sep;88(3):357–364. [PubMed] [Google Scholar]
- SHUMACKER H. B., Jr, MANDELBAUM I. Continuous antibiotic irrigation in the treatment of infection. Arch Surg. 1963 Mar;86:384–387. doi: 10.1001/archsurg.1963.01310090034006. [DOI] [PubMed] [Google Scholar]
- Sarr M. G., Gott V. L., Townsend T. R. Mediastinal infection after cardiac surgery. Ann Thorac Surg. 1984 Oct;38(4):415–423. doi: 10.1016/s0003-4975(10)62300-4. [DOI] [PubMed] [Google Scholar]
- Scully H. E., Leclerc Y., Martin R. D., Tong C. P., Goldman B. S., Weisel R. D., Mickleborough L. L., Baird R. J. Comparison between antibiotic irrigation and mobilization of pectoral muscle flaps in treatment of deep sternal infections. J Thorac Cardiovasc Surg. 1985 Oct;90(4):523–531. [PubMed] [Google Scholar]
- Toporoff B., Rosado L. J., Appleton C. P., Sethi G. K., Copeland J. G. Successful treatment of early infective endocarditis and mediastinitis in a heart transplant recipient. J Heart Lung Transplant. 1994 May-Jun;13(3):546–548. [PubMed] [Google Scholar]