

Abstract
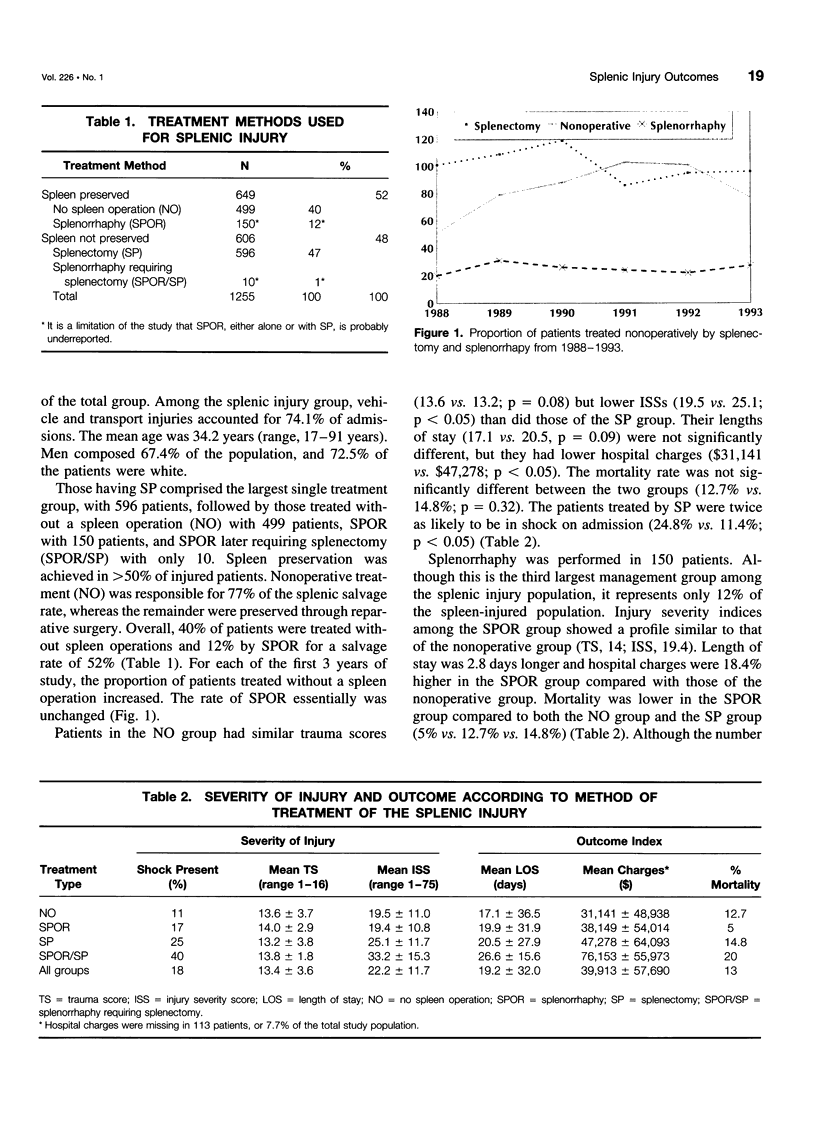
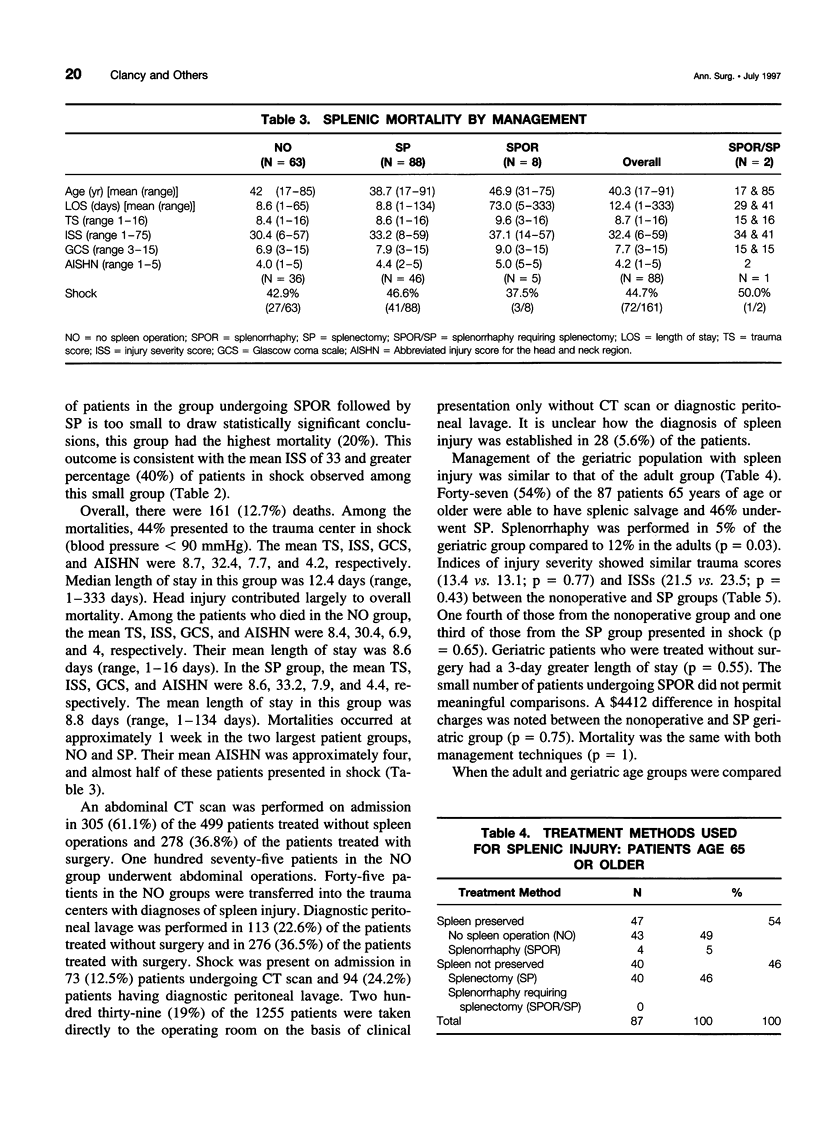
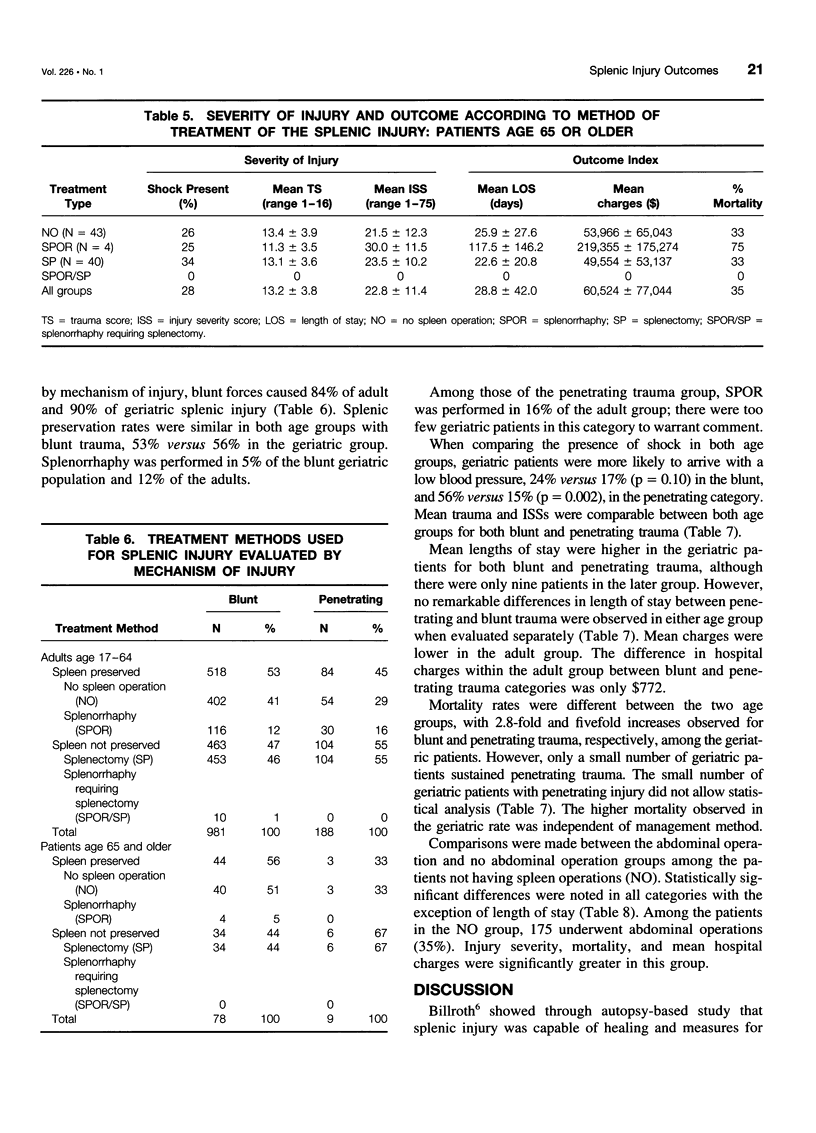
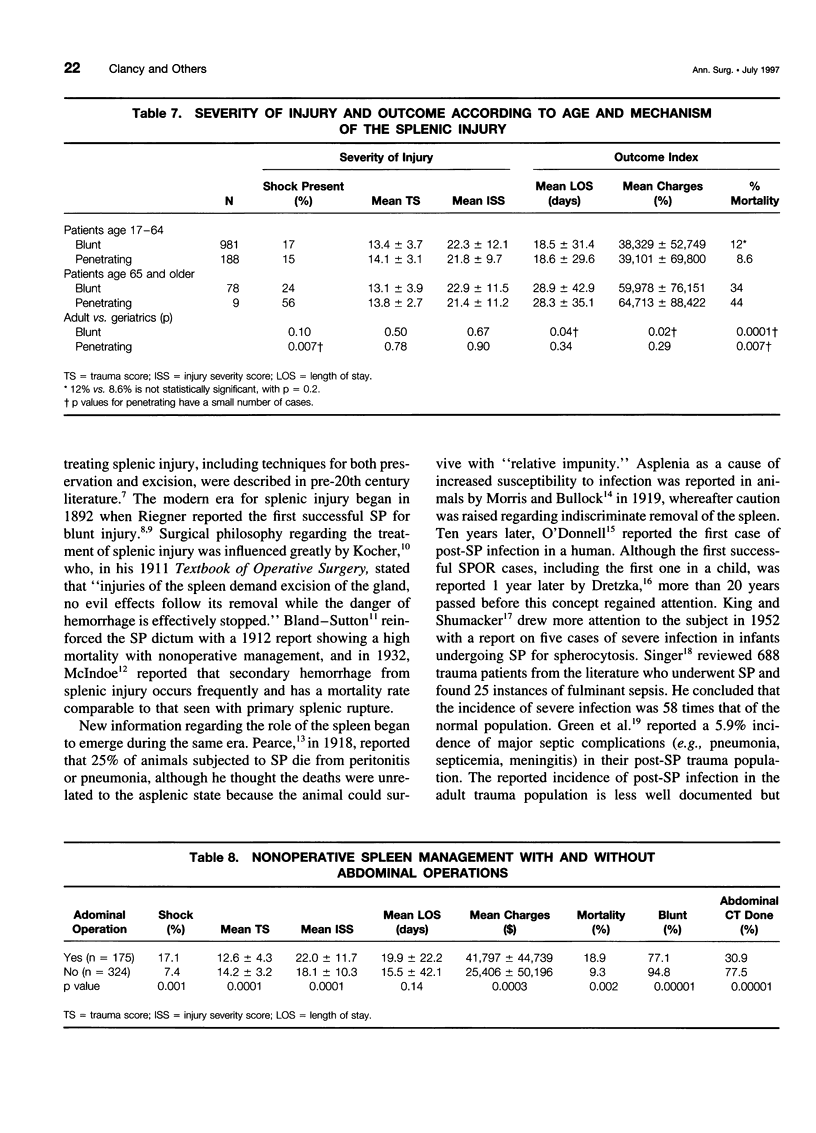
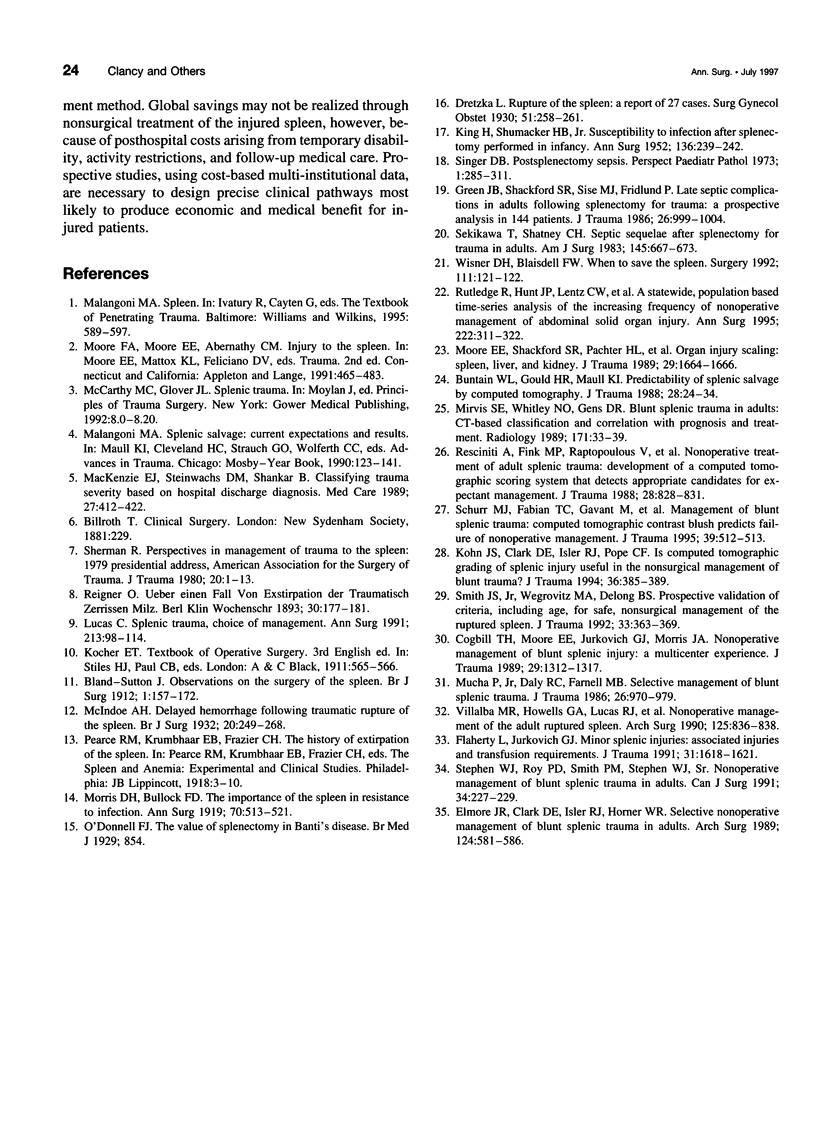
OBJECTIVE: Clinical pathways now highlight both observation and operation as acceptable initial therapeutic options for the management of patients with splenic injury. The purpose of this study was to evaluate treatment trends for splenic injury in all North Carolina trauma centers over a 6-year period. METHODS: Splenic injuries in adults over a 6-year period (January 1988-December 1993) were identified in the North Carolina Trauma Registry using ICD-9-CM codes. Patients were divided into four groups by method of management: 1) no spleen operation, 2) splenectomy, 3) definitive splenorrhaphy, and 4) splenorrhaphy failure followed by splenectomy. The authors examined age, mechanism of injury, admitting blood pressure, and severity of injury by trauma score and injury severity score. SUMMARY BACKGROUND DATA: Comparisons were made between adult (17-64 years of age) and geriatric (older than 65 years of age) patients and between patients with blunt and penetrating injury. Resource utilization (length of stay, hospital charges) and outcome (mortality) were compared. RESULTS: One thousand two hundred fifty-five patients were identified with splenic injury. Rate of splenic preservation increased over time and was achieved in more than 50% of patients through nonoperative management (40%) and splenorrhaphy (12%). Splenorrhaphy was not used commonly in either blunt or penetrating injury. Overall mortality was 13%. Geriatric patients had a higher mortality and resource utilization regardless of their mechanism of injury or method of management.CONCLUSIONS: Nonoperative management represents the prevailing method of splenic preservation in both the adult and geriatric population in North Carolina trauma center hospitals. Satisfactory outcomes and economic advantages accompany nonoperative management in this adult population.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Buntain W. L., Gould H. R., Maull K. I. Predictability of splenic salvage by computed tomography. J Trauma. 1988 Jan;28(1):24–34. doi: 10.1097/00005373-198801000-00004. [DOI] [PubMed] [Google Scholar]
- Cogbill T. H., Moore E. E., Jurkovich G. J., Morris J. A., Mucha P., Jr, Shackford S. R., Stolee R. T., Moore F. A., Pilcher S., LoCicero R. Nonoperative management of blunt splenic trauma: a multicenter experience. J Trauma. 1989 Oct;29(10):1312–1317. doi: 10.1097/00005373-198910000-00002. [DOI] [PubMed] [Google Scholar]
- Elmore J. R., Clark D. E., Isler R. J., Horner W. R. Selective nonoperative management of blunt splenic trauma in adults. Arch Surg. 1989 May;124(5):581–586. doi: 10.1001/archsurg.1989.01410050071015. [DOI] [PubMed] [Google Scholar]
- Flaherty L., Jurkovich G. J. Minor splenic injuries: associated injuries and transfusion requirements. J Trauma. 1991 Dec;31(12):1618–1621. doi: 10.1097/00005373-199112000-00009. [DOI] [PubMed] [Google Scholar]
- Green J. B., Shackford S. R., Sise M. J., Fridlund P. Late septic complications in adults following splenectomy for trauma: a prospective analysis in 144 patients. J Trauma. 1986 Nov;26(11):999–1004. doi: 10.1097/00005373-198611000-00007. [DOI] [PubMed] [Google Scholar]
- KING H., SHUMACKER H. B., Jr Splenic studies. I. Susceptibility to infection after splenectomy performed in infancy. Ann Surg. 1952 Aug;136(2):239–242. doi: 10.1097/00000658-195208000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohn J. S., Clark D. E., Isler R. J., Pope C. F. Is computed tomographic grading of splenic injury useful in the nonsurgical management of blunt trauma? J Trauma. 1994 Mar;36(3):385–390. doi: 10.1097/00005373-199403000-00018. [DOI] [PubMed] [Google Scholar]
- Lucas C. E. Splenic trauma. Choice of management. Ann Surg. 1991 Feb;213(2):98–112. doi: 10.1097/00000658-199102000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKenzie E. J., Steinwachs D. M., Shankar B. Classifying trauma severity based on hospital discharge diagnoses. Validation of an ICD-9CM to AIS-85 conversion table. Med Care. 1989 Apr;27(4):412–422. doi: 10.1097/00005650-198904000-00008. [DOI] [PubMed] [Google Scholar]
- Mirvis S. E., Whitley N. O., Gens D. R. Blunt splenic trauma in adults: CT-based classification and correlation with prognosis and treatment. Radiology. 1989 Apr;171(1):33–39. doi: 10.1148/radiology.171.1.2928544. [DOI] [PubMed] [Google Scholar]
- Moore E. E., Shackford S. R., Pachter H. L., McAninch J. W., Browner B. D., Champion H. R., Flint L. M., Gennarelli T. A., Malangoni M. A., Ramenofsky M. L. Organ injury scaling: spleen, liver, and kidney. J Trauma. 1989 Dec;29(12):1664–1666. [PubMed] [Google Scholar]
- Morris D. H., Bullock F. D. THE IMPORTANCE OF THE SPLEEN IN RESISTANCE TO INFECTION. Ann Surg. 1919 Nov;70(5):513–521. doi: 10.1097/00000658-191911000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mucha P., Jr, Daly R. C., Farnell M. B. Selective management of blunt splenic trauma. J Trauma. 1986 Nov;26(11):970–979. doi: 10.1097/00005373-198611000-00003. [DOI] [PubMed] [Google Scholar]
- Resciniti A., Fink M. P., Raptopoulos V., Davidoff A., Silva W. E. Nonoperative treatment of adult splenic trauma: development of a computed tomographic scoring system that detects appropriate candidates for expectant management. J Trauma. 1988 Jun;28(6):828–831. [PubMed] [Google Scholar]
- Rutledge R., Hunt J. P., Lentz C. W., Fakhry S. M., Meyer A. A., Baker C. C., Sheldon G. F. A statewide, population-based time-series analysis of the increasing frequency of nonoperative management of abdominal solid organ injury. Ann Surg. 1995 Sep;222(3):311–326. doi: 10.1097/00000658-199509000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schurr M. J., Fabian T. C., Gavant M., Croce M. A., Kudsk K. A., Minard G., Woodman G., Pritchard F. E. Management of blunt splenic trauma: computed tomographic contrast blush predicts failure of nonoperative management. J Trauma. 1995 Sep;39(3):507–513. doi: 10.1097/00005373-199509000-00018. [DOI] [PubMed] [Google Scholar]
- Sekikawa T., Shatney C. H. Septic sequelae after splenectomy for trauma in adults. Am J Surg. 1983 May;145(5):667–673. doi: 10.1016/0002-9610(83)90118-6. [DOI] [PubMed] [Google Scholar]
- Sherman R. Perspectives in management of trauma to the spleen: 1979 presidential address, American Association for the Surgery of Trauma. J Trauma. 1980 Jan;20(1):1–13. [PubMed] [Google Scholar]
- Singer D. B. Postsplenectomy sepsis. Perspect Pediatr Pathol. 1973;1:285–311. [PubMed] [Google Scholar]
- Smith J. S., Jr, Wengrovitz M. A., DeLong B. S. Prospective validation of criteria, including age, for safe, nonsurgical management of the ruptured spleen. J Trauma. 1992 Sep;33(3):363–369. doi: 10.1097/00005373-199209000-00005. [DOI] [PubMed] [Google Scholar]
- Villalba M. R., Howells G. A., Lucas R. J., Glover J. L., Bendick P. J., Tran O., Jafri S. Z. Nonoperative management of the adult ruptured spleen. Arch Surg. 1990 Jul;125(7):836–839. doi: 10.1001/archsurg.1990.01410190028004. [DOI] [PubMed] [Google Scholar]
- Wisner D. H., Blaisdell F. W. When to save the ruptured spleen. Surgery. 1992 Feb;111(2):121–122. [PubMed] [Google Scholar]