

Abstract
Background
The rapid implementation of telemedicine during the early stages of the COVID-19 pandemic raises questions about the sustainability of this intervention at the global level.
Objective
This research examines the patient experience, health inequalities, and clinician-patient relationship in telemedicine during the COVID-19 pandemic’s first 2 years, aiming to identify sustainability factors.
Methods
This study was based on a prepublished protocol using the Joanna Briggs Institute (JBI) methodology for scoping reviews. We included academic and gray literature published between March 2020 and March 2022 according to these criteria: (1) population (any group); (2) concepts (patient experience, clinician-patient relationship, health inequalities); (3) context (telemedicine in primary and outpatient care); (4) excluding studies pertaining to surgery, oncology, and (inpatient) psychiatry. We searched Ovid Medline/PubMed (January 1, 2022), Web of Science (March 19, 2022), Google/Google Scholar (February and March 2022), and others. The risk of bias was not assessed as per guidance. We used an analysis table for the studies and color-coded tabular mapping against a health care technology adoption framework to identify sustainability (using double-blind extraction).
Results
Of the 134 studies that met our criteria, 49.3% (66/134) reported no specific population group. Regarding the concepts, 41.8% (56/134) combined 2 of the concepts studied. The context analysis identified that 56.0% (75/134) of the studies referred to, according to the definition in the United Kingdom, an outpatient (ambulatory care) setting, and 34.3% (46/134) referred to primary care. The patient experience analysis reflected positive satisfaction and sustained access during lockdowns. The clinician-patient relationship impacts were nuanced, affecting interaction and encounter quality. When mapping to the nonadoption, abandonment, scale-up, spread, and sustainability (NASSS) framework, 81.3% (109/134) of the studies referenced the innovation’s sustainability. Although positive overall, there were some concerns about sustainability based on quality, eHealth literacy, and access to health care for vulnerable migrants and the uninsured.
Conclusions
We identified confusion between the concepts of patient experience and patient satisfaction; therefore, future research could focus on established frameworks to qualify the patient experience across the whole pathway and not just the remote encounter. As expected, our research found mainly descriptive analyses, so there is a need for more robust evidence methods identifying impacts of changes in treatment pathways. This study illustrates modern methods to decolonize academic research by using gray literature extracts in other languages. We acknowledge that the use of Google to identify gray literature at the global level and in other languages has implications on reproducibility. We did not consider synchronous text-based communication.
Trial Registration
Open Science Framework 4z5ut; https://osf.io/4z5ut/
Keywords: pandemic, primary care, outpatients, telemedicine, ambulatory care, global health, patient experience, NASSS, clinician-patient relationship, health inequalities, gray literature, PRISMA
Introduction
Following the World Health Organization (WHO) announcement declaring COVID-19 a pandemic on March 11, 2020, the organization recommended telemedicine as one of the first critical interventions to minimize demands on stretched supplies of personal protective equipment [1,2]. Although telehealth was not new as a delivery mode, there were great expectations particularly around the use of video consultations in this context. In Africa, telemedicine held promise, as it rationalized human resources allowing national or international experts to relay advice to other clinicians [3]; in the United Kingdom, the pandemic was deemed a “burning platform” to propel the UK National Health Service (NHS) toward widespread adoption of video consultations [4]. Most medical specialties responded to the WHO recommendation with rapid changes in service delivery toward telemedicine (both telephone and a new medium—video consultations) in primary and secondary care across the globe.
In the United Kingdom, 15 months into the pandemic, the academic community and political groups raised questions around the sustainability and impacts of the move toward telemedicine, building upon the learning of the past year toward a “new normal,” particularly as social distancing and lockdown measures were removed [5]. A 2021 report by the UK Health and Social Care Committee defined telemedicine as a “welcomed and positive innovation” overall while highlighting concerns by various national organizations on its impact on health inequalities in terms of exclusion (lack of access), quality, and patient safety. The committee reported important consensus from recognized local institutions such as the Health Foundation and the Kings Fund and patient organizations such as National Voices and Healthwatch on the need for additional research to assess the future of telemedicine in a patient-centered way [6].
In previous protocols [7,8], we relayed how prepandemic evidence synthesis identified several barriers and objections that hindered telemedicine uptake, including technology, workload, and confidentiality [9], as well as concerns regarding appropriateness [10]. However, at the outset of the pandemic, these objections were rapidly overcome, supported by major regulatory and financial enablers [11,12]. Given the considerable incentives and support toward the implementation of telemedicine, there are concerns about the risks of losing some of the advantages of this mode of delivery in a postpandemic future [13], particularly once incentives are no longer in place [14,15]. These concerns apply to not only the United Kingdom, Canada, or the United States but also sub-Saharan Africa [16] and Latin America [17] where considerable barriers persist and there has been more limited evidence of uptake.
The purpose of this scoping review was to explore the global evidence (both academic and nonacademic) surrounding the rapid adoption of telemedicine in outpatient and primary care settings during the first 2 years of the COVID-19 pandemic to identify how elements related to patient experience, clinician-patient relationship, and health inequalities support (or take away from) the sustainability of this delivery model.
Methods
Protocol
This review was conducted according to an a priori published protocol [8] following the Joanna Briggs Institute (JBI) methodology for scoping reviews, updated guidance, and data extraction guidance [18-20]. This last guidance clarifies that a review can focus on the most relevant section of a document for analysis, without having to review whole studies in scoping reviews [20]. We outlined deviations from the original protocol and the methodology in Multimedia Appendix 1. A key contribution of this study hinges on the methods used to search and extract gray literature across a wider set of countries as to achieve truly global representation.
Inclusion Criteria
Population, Concept, Context Principle
The inclusion criteria used the Population, Concept, Context (PCC) principle. We classified each article against the PCC framework. Namely, for each document, we sought to identify (1) the population group (if any) to which the document referred, (2) the concept to which it referred (patient experience, clinician-patient relationship, health inequalities, or a combination of these), and (3) in which (clinical) context telemedicine was being used (outpatient, primary care, or particular specialties).
Population
The review focused on primary care services offered to the general population. Studies focusing on specific population groups or those with particular conditions within a particular country or geographical area were included.
Concept
Although the key concept under consideration was the adoption of “telemedicine,” as defined in the Introduction, we narrowed our inclusion criteria to the sustainability of the interventions, focusing on patient experience, health inequalities, and clinician-patient relationship. Telemedicine has been defined as per our protocol [8] using academic literature [21] and the WHO [22], which defines it as “The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies [...].” Although we focused on telephone and video as communication technologies, we thank an anonymous peer reviewer who identified that text messaging also falls in this category (albeit not included in our review).
Context
The context was primary care services provided during the COVID-19 pandemic in any setting or country during the first 2 years of the pandemic (March 2020-March 2022).
Types of Sources
This scoping review considered quantitative, qualitative, and mixed methods study designs for inclusion. In addition, systematic reviews, protocols, other documents, and commentaries or opinions were considered for inclusion in the proposed scoping review. These commentaries or other documents might have appeared in peer-reviewed journals or other gray literature such as industry magazines or reports [23,24].
Search Strategy
This section summarizes our prepublished protocol [8]. We structured this section by first explaining the selection and identification of search terms (both in English and other languages), then how we used those terms to search for academic and gray literature. To note, the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) [25] was used to structure our review protocol [8].
Identifying Search Terms
Our search terms, which were in English, centered around telemedicine, primary care, and COVID-19 and were expanded through a limited search on Ovid Medline and Web of Science. We also sought guidance from University of Warwick librarians, who identified COVID-19 search terms from the National Institute for Health and Care Excellence (NICE) [26]. Additionally, we examined previous telemedicine protocols in general practice [27] and Primary Care Cochrane Library Protocols. For search terms in other languages, we used a 2-step process to identify relevant terms for the included non-English search results. We used Google Translate and engaged in discussions with native speakers to ensure these were accurate translations.
Search Approaches
We had 2 distinct approaches depending on whether we were searching for academic or gray literature. With the aforementioned terms, we searched the following academic databases: Ovid Medline (equivalent to PubMed [28]), Web of Science, and Google Scholar. PROSPERO and Cochrane Library were used to inform our design. PROSPERO in particular was used to check whether there was any ongoing review on the topic. All identified search terms and examples of the searches (for academic and gray literature) can be found in Multimedia Appendix 2, as per our previously published protocol [8].
We searched Ovid Medline/PubMed (January 13, 2022), Web of Science (March 19, 2022), Livivo (March 15, 2022), Scopus (March 19, 2022), PROSPERO (January 12, 2022), Cochrane Library (January 12, 2022), and Google/Google Scholar (February 2022 and March 2022).
As shown in Multimedia Appendix 2, to identify relevant gray literature published at the time of the pandemic, we used advanced Google search criteria with simplified search terms. We combined the terms telemedicine, “Primary Care,” and COVID-19 with (1) “patient experience,” (2) “health inequalities,” or (3) “patient-clinician interaction” and asked the search engine to provide pdf-only results within the years 2020 through 2022. Although we recognize it is not fully possible to reproduce Google searches, the selection of pdf documents was aimed at identifying the most retrievable and credible gray literature [8] while, at the same time, supporting reproducibility of the analysis [23,24].
We undertook these searches in English, Chinese, Spanish, Arabic, Portuguese, Hindi, and Indonesian. To improve representation of African countries due to difficulties searching in Urdu, we undertook additional Google searches in English including country-specific results for the 5 largest African countries by population (Nigeria, Ethiopia, Democratic Republic of Congo, Egypt, and South Africa [29]). For Google searches, we selected the first 30 results by relevance, and for English-based results, we selected the top 10 results by country. We selected the first 30 results based on the literature [30-33], timeline, and budget. Further, as can be seen in the example for a failed search for Pakistan in Multimedia Appendix 2, Google searches only provided less than a handful of results when restricting by country of publication.
We followed established guidelines for analyzing non-English text [34]. We used machine translation via Google Translate to translate at least 3 paragraphs containing the key search terms (telemedicine, primary care, and any of the combinations of patient experience, clinician-patient relationship, and health inequalities). We selected 3 paragraphs that were roughly equivalent in the number of words to that of an abstract.
Screening
The authors used a single-phase, double-blind screening of abstracts and extracts based on the eligibility criteria. Screening instructions were tested by 4 authors across a sample of 50 abstracts to verify the instructions had been properly understood. The remaining articles were allocated across several combinations of pairs of authors using double-blind screening and Rayyan [35] as an aid. Any discrepancies were resolved by the pair of authors themselves and verified by the lead author before data extraction. Given the extended scope of our review, and in agreement with the prepublished protocol and the latest JBI guidance [20], there was no full-text screening as the abstracts and extracts were our main data source. Abstracts and extracts have been made available in Multimedia Appendix 3.
Data Extraction
The authors used double-blind extraction of data using an Excel table template as outlined in Multimedia Appendix 4. Following the latest JBI guidance for scoping reviews [20], we chose to focus data extraction on abstracts and extracts only, reflecting the wide research design that allowed us to accommodate the breadth of the review in terms of (1) themes; (2) a worldwide, multilanguage approach; and (3) sources. Using a data extraction tool shared in Multimedia Appendix 4, we mapped the text in tabular form against the NASSS framework [36] domains, noting some of the document sections might touch upon 1 or more domains.
Data Analysis and Presentation
In agreement with the latest JBI methodological guidance [18-20], no critical appraisal was undertaken, and the final presentation of results consisted of the following. In the first section, the results of the search were presented in a PRISMA-ScR flow diagram [25], including a flowchart and a checklist, and we conducted a table analysis of more detailed characteristics of the included documents (Table S1 in Multimedia Appendix 5). We captured the number of articles that included certain data against the PCC framework. Understandably, in the “population” label, the numbers do not add up to the total as some categories are not mutually exclusive. A color-coded (heat map) mapping was created in tabular form against the NASSS framework’s [36] domains: (1) the condition, (2) the technology, (3) the value proposition, (4) adopters, (5) organizations, (6) wider system, and (7) embedding and adaptation over time. The heat map shows graphically the maximum and minimum numbers of references for each domain (using the average counts for double-blind data extraction and mapping). We performed a narrative analysis (including sentiment analysis) of references to the sustainability of video consultations outside of social distancing restrictions brought about by the pandemic. The results are discussed from the point of view of sociotechnical grounded theory, providing strengths and limitations of the sources and the review method itself. We included a statement of positionality in our conclusions, as well as recommendations for research and practice. We believe that reflexivity through researcher positionality is fundamental to decolonizing global health research that seeks to include voices and perspectives usually marginalized from the academic discourse [37-39].
Results
PRISMA Study Inclusion
Academic database searches identified 983 records, and 171 additional records were identified through Google searches for various languages and countries. For Google Arabic and Google Pakistan, there were no results that matched the search criteria. Of the total 1154 articles, 181 were identified as duplicates and were removed: 160 duplicates were academic articles, and 21 duplicates were identified among the nonacademic articles. After the removal of duplicates, there were 973 articles to be screened. Of these 973 articles, 823 articles were from academic databases, and 150 were from nonacademic databases. After the abstract screening and before data extraction, 703 academic and 136 nonacademic articles were excluded, leaving a total of 134 documents [29,40-171] for data extraction including 120 academic articles and 14 extracts from gray literature searches. See the PRISMA-ScR [25] flowchart (Figure 1).
Figure 1.
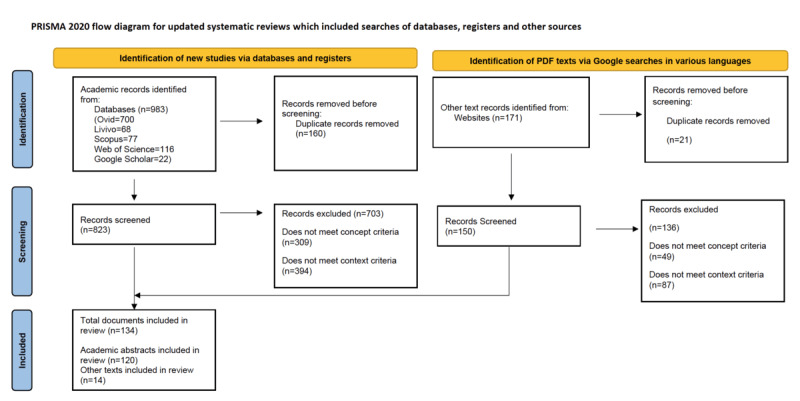
PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) flowchart outlining the process of identification, screening, and final inclusion across various types of data sources.
Summary of Document Types
We separated the academic studies (which we identified as those having a clearly labelled abstract with introduction, aims, methods, results, and discussion sections) from the other documents (or gray literature) and found that these other documents represented 27.6% (37/134) of the selected documents. Searches in academic databases and journals provided a small group of gray literature in the form of commentaries or guidelines. Conversely, general internet searches also identified a minority of academic documents.
The document pool achieved global representation, with documents from all continents, including South America [46,110,166] and Africa [116,121]. There was, however, overrepresentation from North America (58/134, 43%), with a large proportion of documents from the United States.
In terms of the methodology in the selected documents, over 72% (96/134) of the documents used surveys, questionnaires, or interviews. The use of surveys and questionnaires was closely related to the type of design observed, with most studies being cross-sectional (96/134, 72%). Finally, regarding the telemedicine medium, the documents did not specify the medium by generally referring to “telemedicine” in 57% (77/134) of documents. More details are provided in Table S2 in Multimedia Appendix 5.
Quantitative Classification Against the PCC Framework
Table S3 in Multimedia Appendix 5 includes the characteristics of the 134 documents against the protocol’s PCC. We follow with a short commentary highlighting any documents that exemplify these findings. Table 1 shows how the documents related to the various key concepts explored (clinician-patient relationship, health inequalities, and patient experience), and the following paragraphs summarize the key findings. In addition, Figure 2 shows the results of the bibliographic keyword analysis.
Table 1.
Classification of the documents against the key concepts.
| Concept | Documents, n | |
| 1 concept | ||
| Clinician-patient relationship | 28 | |
|
|
Health inequalities | 11 |
| Patient experience | 26 | |
| 2 concepts | ||
|
|
Clinician-patient relationship, health inequalities | 11 |
|
|
Clinician-patient relationship, patient experience | 29 |
| Health inequalities, patient experience | 16 | |
| All 3 concepts | ||
| Clinician-patient relationship, patient experience, health inequalities | 13 | |
Figure 2.

Bibliographic keyword analysis.
In terms of population groups, a large subset of abstracts and extracts (66/134, 49.3%) reported no specific demographics nor patient characteristics (see, for example, the extract from the board report from the East Kent Hospitals NHS Foundation Trust [64] or Karacabeyli et al [95]). The main demographic characteristics reported in abstracts and extracts were age (39/134, 29.1%) and sex (20/134, 14.9%), with studies also considering sociodemographic factors. It is important to note that a particular document might have tracked more than one characteristic; see, for example, Manski-Nankervis et al [113], which tracked education status, gender, age, and whether patients spoke English at home.
In terms of the concepts studied, the most popular concept was the clinician-patient relationship, reported in 28 abstracts. The majority of documents (69/134, 51.5%) combined 2 or 3 concepts. In the following paragraphs, we provide a brief summary of results across the various concepts.
Regarding patient experience, we found 26 studies solely focused on this concept. Patient experience was mostly equated with patient satisfaction and access. There were positive levels of satisfaction overall [99,121,149] and sustained access at the time of lockdowns [48,53].
Regarding health inequalities, there were only 11 studies solely focused on this concept. We found gaps in evidence that made it difficult to pinpoint the impacts on health inequalities of specific groups, with some evidence of health inequality exacerbation for those considered to be at the fringe of the economic and health system (such as vulnerable migrants, families with high levels of economic deprivation or health care insurance exclusion, or rural communities with limited access to technology) [74,116,140].
Regarding the clinician-patient relationship, there were 28 documents solely focused on this concept, mainly on the clinician-patient interaction and quality of the encounter. There was no consensus regarding whether the impact of telemedicine on the interaction had been positive, neutral, or negative [43,56,70], while there was consensus on the added value of the quality of the remote encounter for triage, follow-up consultations, or chronic condition management [128,133,155].
Finally, concerning the context, we identified 46 documents focused solely on primary care, general outpatient care featured in 19 documents, and various outpatient specialties were featured in 56 extracts.
Mapping Against the NASSS Framework
As shown in Figure 3, there was considerable variability in evidence across the NASSS [36] domains and subdomains. Domains 6 (wider system), 7 (time domain), and 3 (value proposition) had the most information. For domain 6, documents referenced the pandemic or pandemic-related lockdowns and infection control measures coupled with regulatory enablers or recommendations (such as mandatory online triage in primary care, parity in payments between face-to-face and telemedicine appointments). There was lower density of information about specific conditions that were being managed with telemedicine (subdomain 1a), knowledge needed to use telemedicine (subdomain 2c), and organizational or implementation aspects (domain 5).
Figure 3.
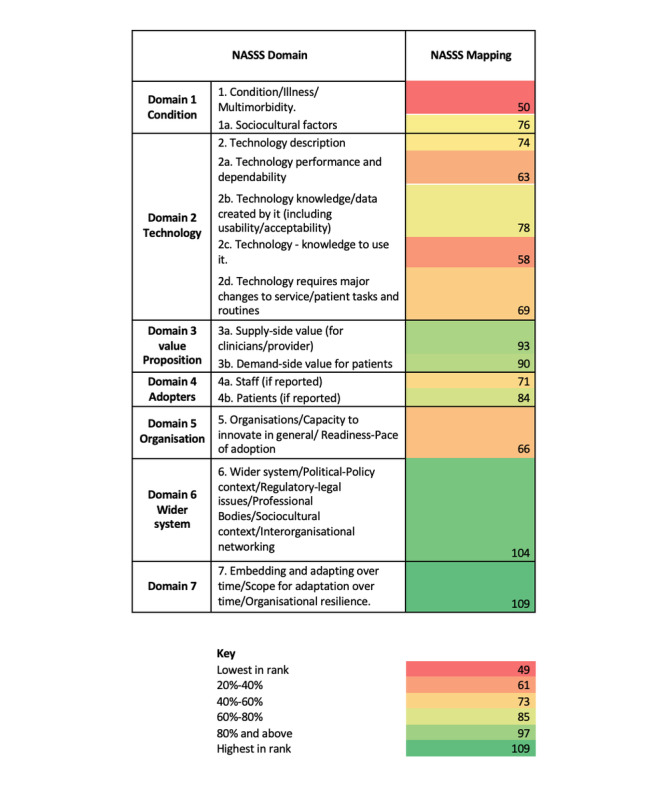
Heat map against each of the nonadoption, abandonment, scale-up, spread, and sustainability (NASSS) domains.
Narrative Analysis of Sustainability
Roughly over one-half of the documents (75/134, 56%) identified challenges in terms of sustainability or made recommendations on how to address them. Among these, sentiment was mixed or neutral in 40 documents and positive in 31 documents, with only a small subgroup [68,89,141,148] viewing such challenges negatively as barriers to further planning and progress. Challenges and areas of consideration included general planning such as workforce training, digital resources, patient experience, and ethical issues [92] or a more focused look at the technology itself such as more effective digital platforms and increased use of home medical equipment [43]. Other issues such as patient selection were also noted with consideration to disease progression, language and cognitive ability, health literacy, and technology access [40]. The systematic review by Mbunge et al [116] of the digital technologies deployed in South Africa during the pandemic identified a “digital divide” barrier in rural areas and advocated for better networks.
Almost one-third (38/134, 28%) of the documents set out plans for sustainable growth and further embedding, with generally positive sentiment. The report by the East Kent Hospitals NHS Foundation Trust in 2021 [64] mentioned an enhanced engagement plan to meet ambitious targets set by health care authorities for the delivery of telemedicine appointments. Tulupova et al [162] referred to plans for the creation of telemedicine guidelines and an educational program on communications in health care using digital technologies for patients to improve digital health literacy. The remaining documents either did not address the area of sustainability [42,44,49,66,95,101,106,110,111,122,132,143,153,167] or had a generally negative view on the sustainability of the intervention [63,74,80,112,169]. The negative commentary was based on concerns about quality (ie, treating musculoskeletal conditions), eHealth literacy, and access to health care for those at the fringe of the health care system coverage (such as vulnerable migrants and the uninsured).
Discussion
This section includes 4 main areas: (1) a summary of our findings, (2) a sociotechnical grounded theory research interpretation of the findings (based on Hoda [172]), (3) positioning against the wider and recent literature, and (4) strengths and limitations of our study. The section finalizes with a short conclusion.
Summary of Findings
Concerning the protocol’s PCC, 49% (66/134) of the documents reported no specific population group targeted by the study (population); according to the UK definition, 55% (74/134) of the studies referred to an outpatient (ambulatory care) setting, and 34% (46/134) referred to primary care (context); and 49% (66/134) of the studies referred to only 1 of the concepts studied (concept).
Mapping to the NASSS framework [36] identified that 93% (125/134) of the studies referenced the sustainability of telemedicine with moderately positive comments.
Global Representation
We found 134 studies meeting our criteria and achieved global representation. We highlight some of the global results from limited-resource countries here.
Despite the limited evidence for African countries (2 studies [116,121]), our findings were aligned with other African reviews around insufficient evidence of use due to considerable barriers in this region [16] and a lack of “meaningful investment” in this area [173]. We concurred with Nittari et al [174] that several barriers are still present that risk the sustainability of this delivery mode beyond the pandemic.
Studies in South America [46,110,166] provide examples of effective use in outpatient settings (specifically speech and language therapy [46]), as well as reflections on how this new delivery mode in the context of the wider pandemic might have generated an element of mistrust and fear in the clinician-patient relationship [166].
Results from Middle Eastern and Asian countries [41,97,104,105] provide perspectives on the use of telemedicine in orthopedics and hematology while indicating the equivalence of audio and video consultations, an important point to inform telemedicine programs in low-income countries as a way of increasing access to health services.
Positioning Against the Wider and Recent Literature
This review can be positioned in the emerging literature of reviews around telemedicine during the pandemic period [175-183].
A key finding of our study is how patient experience was generally equated with patient satisfaction. Other studies have found these are often used interchangeably [184-186]. However, accepted definitions of patient experience go beyond satisfaction and “focus on individualized care and tailoring of services to meet patients’ needs” [187]. This is related to another finding, as the studies are mainly observational with no reference to patient experience frameworks, let alone to some emerging frameworks specific to the digital patient experience [173,188]. Our findings on patient experience are aligned with another recently published review focused on the COVID-19 pandemic, with similar categories and findings [178]. In terms of the clinician-patient relationship, our findings were mixed, but recent reviews found that the relationship was “troubled” telemedicine given both patient and clinician reluctance to use [177]. However, others found the tool useful [106].
de Oliveira Andrade et al [175] focused on the role of legislation in the widespread utilization of telemedicine during the pandemic, finding that regulatory frameworks enabled telemedicine spread in areas related to ethics, reimbursement, data safety, and pandemic-related regulatory relaxation (in the United States, for instance, relaxation of interstate practice was particularly relevant [183]). We found a lack of consensus in terms of sustainability as these financial and regulatory incentives dissipated; however, supportive regulation would be a defining factor in its sustainability. Our evidence seems more nuanced than other recent reviews [177,189]. We are aware specialties like family medicine and general practice seem to have a preference for a particular medium, such as telephone instead of video [190], with more work being undertaken regarding the impacts on quality [191] or equivalence between face-to-face and remote consultations [183].
Regarding the impact on health inequalities, another review identified emerging literature on the opinions of vulnerable populations regarding telemedicine [180]. We saw references [192-195] to an emerging framework for digital health equity [196], which we expect will help address the gaps we identified in the design and evaluation of inclusive digital health care services to address the “self-reinforcing effect of digital and social exclusion” [197] and its impact on health care inequalities in access and experience. Our concerns about implications on health inequality resonate with other similar reviews for telemedicine [179].
Strengths and Limitations
Strengths
We mapped the emerging literature (gray and academic) on telemedicine during the pandemic to a well-established framework using 3 lenses (patient experience, health inequalities, and clinician-patient relationship). We identified this as the only systematic review of its kind. Only 1 other review mapped academic literature on video consultations to the NASSS framework [36] but outside the context of the pandemic [37]. Notably, we effectively reflected the experiences of non–English-speaking countries with literature across the 5 continents, so it is truly global health–oriented, with the added values and perspectives of a diverse, multidisciplinary research team.
When identifying the limited literature at the intersection of health inequalities and telemedicine, we provided a brief taxonomy of potential groups impacted differently. Recognizing the multidimensionality and intersectionality of social exclusion, we show that demographic characteristics such as age, sex, and socioeconomic factors have received some attention, but there is still very limited information and not enough to draw solid conclusions on impacts.
From a methodological standpoint, we provided additional insight on how to integrate effectively other documents and nontraditional voices and experiences into academic research with a reproducible approach.
Limitations of the Sources
The authors sought gray literature directly via Google to ensure a unified source and methodology to identify and capture experiences from non–English-speaking countries. This is a method with limited reproducibility. Researchers interested in gray literature information in English can consult the UK National Grey Literature Collection Funded by Health Education England. We are aware of additional databases with non-English literature that could be used [198]. Emerging literature has covered mostly single-center survey studies with limited sample sizes, reflective of the immediate experiences arising in the context of the pandemic.
Limitations of the Review
We have limited the depth of analysis to accommodate for the extensive scope, in accordance with the JBI guidelines for data extraction [199]. The use of document extracts using the “surrounding keyword” approach needs further development and testing, as we recognize slightly longer extracts are better at conveying enough information to support screening and analysis. We did not consider synchronous text-based communication. The methodology of scoping reviews is still skewed toward evidence from academic publications, which are biased toward researchers from North America and Europe. Although not specified in the current guidance, capping the number of results from traditional academic databases provides a more balanced representation and could reduce duplication while having limited effects on how comprehensive the findings are.
In conclusion, our discussion section has highlighted considerable variation in the emerging literature during the pandemic regarding changes in pathways toward telemedicine. We highlighted the different focus of studies focused on health inequality or outpatient care and the global representation of the studies included (which is a key strength). Of note is the finding equating patient experience with satisfaction, which reflects a potentially limited understanding of sociotechnical views of human-computer interaction and human factors in traditional health service research.
Conclusions
This section is divided into 3 parts comprising a reflection of our positionality as researchers in analyzing these themes as well as further recommendations for research and practice.
Statement of Positionality
Following the method by Pant et al [37], we frame some of our conclusions in the context of our positionality and our aims. We are a diverse group of researchers (with roots in Latin America, the Middle East, Asia, and Africa and with supervisors from the United Kingdom), but our gaze is colonially influenced by our education and current positionality in this country.
By opening our search criteria to non-English documents and gray literature, we succeeded in capturing immediate, emerging experiences at the global level, with 27.6% (37/134) of our documents having no structured abstract and classified as gray literature, with 5 documents from South America and Africa and 13 documents from Asia. The balance, however, is still very skewed toward the United States and English-speaking countries.
Our positionality and knowledge of the UK health system and legislation meant it was difficult to translate these categories to other systems, and we had to modify our parameters and analysis. For instance, although our choice of the UK diversity legislation (“protected characteristics”) as a framework for categorizing health inequalities was helpful, the UK definition of “primary care” was not helpful due to its contrast with the definition set out by the WHO (for example in the work by Dimer et al [46] in Brazil, classifying speech and language therapy services as a “primary health care service,” which are not available in the United Kingdom in this setting).
Recommendations for Research
From a methodological standpoint, we urge researchers looking to decolonize academic research to test and evaluate further our approach to using gray literature extracts in other languages, particularly in scoping reviews, as it provides that additional level of immediacy with the phenomenon of study. We noticed confusion on the use of patient satisfaction and patient experience, so research should focus on more robust frameworks reviewing the overall patient pathway (away from the evaluation of a remote encounter [184-186]). As expected, our research found mainly descriptive documents, so future research should focus on robust evaluation of clinical outcomes arising from changes in diagnostic and treatment pathways away from face-to-face settings. We recommend future research with a narrower approach to specific population groups and more focused on access and outcomes (Table S1 in Multimedia Appendix 5). From a sociotechnical research perspective, we recommend future research using modern techniques (natural language processing, data mining, and sentiment analysis) focusing on categories with closer links to human-computer interaction. Following publication, we will publish our data on Open Science Framework [200].
Recommendations for Practice
The impact of telemedicine on patient safety is critical to determine the sustainability of this intervention when contrasting it with the under- or overutilization of resources [201]. If not ruling out the continued use of telemedicine, the authors outlined the importance of further research and refinements to the intervention itself. We found that models such as the Dynamic Sustainability Framework [75] might be useful to support learning and adaptation with care toward the potential disenfranchisement of some patient groups.
Acknowledgments
ChatGPT and Grammarly were used to edit the final draft. Many thanks to Cee MacDonald at Paperaid for the assistance with extract retrieval and text formatting.
This research did not receive any external funding and was undertaken as part of DV’s self-funded PhD studies.
Abbreviations
- JBI
Joanna Briggs Institute
- NASSS
nonadoption, abandonment, scale-up, spread, and sustainability
- NHS
National Health Service
- NICE
National Institute for Health and Care Excellence
- PCC
Population, Concept, Context
- PRISMA-ScR
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
- WHO
World Health Organization
Deviations from the protocol.
Example searches.
Abstracts-extracts used in the study.
Data collection template.
Summary characteristics of the included studies.
PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) Checklist.
Footnotes
Authors' Contributions: These contributions use Contributor Roles Taxonomy (CRediT) guidelines. As this article is also a pedagogic exercise related to various individuals’ studies, it was agreed that all voluntary contributors would be set as co-authors regardless of the degree of contribution.
This article contributes to DV’s PhD studies at the University of Warwick, and DV contributed to the study conceptualization, data curation (lead), formal analysis (lead), investigation (lead), methodology (lead), project administration (lead), software, validation, visualization, writing of the original manuscript draft (lead), and manuscript review and editing. AS contributed to the data curation (lead), formal analysis (support), investigation (support), methodology (equal), project administration (support), software (support), visualization (support), writing of the original manuscript draft (support), and copyediting (lead). DOM and IL contributed to the data curation (support), investigation (support), and methodology (equal). GH and HZ contributed to the formal analysis (support), visualization (support), and writing of the original manuscript draft (support). TB contributed to the data curation (support), investigation (support), methodology (equal), and manuscript review and editing (support). SAI contributed to the data curation (support), formal analysis (support), and methodology (support). RP contributed to study supervision (lead), validation (lead), and manuscript review and editing (support). RS contributed to study supervision (support), manuscript review and editing (lead), and validation (lead). JD contributed to study supervision (support). AP contributed to validation of data extraction (support) and preparation of the final draft. LJM and KTK contributed to the data curation (support).
Conflicts of Interest: At the time of publication, DV, TB, and HZ worked in the UK National Health Service in the United Kingdom. The research was undertaken independently of DV’s, TB’s, and HZ’s occupations and does not represent the views of their employers. The remaining authors declare no conflict of interest.
References
- 1.WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. World Health Organization. 2020. Mar 11, [2021-02-20]. https://tinyurl.com/tn4rtbse .
- 2.Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19) World Health Organization. 2020. Mar 19, [2021-06-08]. https://apps.who.int/iris/bitstream/handle/10665/331498/WHO-2019-nCoV-IPCPPE_use-2020.2-eng.pdf .
- 3.Chersich MF, Gray G, Fairlie L, Eichbaum Q, Mayhew S, Allwood B, English R, Scorgie F, Luchters S, Simpson G, Haghighi MM, Pham MD, Rees H. COVID-19 in Africa: care and protection for frontline healthcare workers. Global Health. 2020 May 15;16(1):46. doi: 10.1186/s12992-020-00574-3. https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-020-00574-3 .10.1186/s12992-020-00574-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Greenhalgh T, Wherton J, Shaw S, Morrison C. Video consultations for covid-19. BMJ. 2020 Mar 12;368:m998. doi: 10.1136/bmj.m998. [DOI] [PubMed] [Google Scholar]
- 5.Wherton J, Greenhalgh T. Evaluation of the Near Me video consulting service in Scotland during COVID-19, 2020: Summary Report. Scottish Government. 2021. Mar, [2024-11-06]. https://tinyurl.com/3nmavy8m .
- 6.The NHS: lessons learnt and building for the future. UK Parliament. [2021-06-12]. https://publications.parliament.uk/pa/cm5801/cmselect/cmhealth/320/32009.htm .
- 7.Valdes D, Alqazlan L, Procter R, Dale J. Global evidence on the rapid adoption of telemedicine in primary care during the first year of the COVID-19 pandemic: a scoping review protocol. Research Square. 2021. Mar 16, [2024-11-27]. https://assets-eu.researchsquare.com/files/rs-302879/v1/5668b4f9-5d65-4353-93db-32249840ca3d.pdf . [DOI] [PMC free article] [PubMed]
- 8.Valdes D, Alqazlan L, Procter R, Dale J. Global evidence on the rapid adoption of telemedicine in primary care during the first 2 years of the COVID-19 pandemic: a scoping review protocol. Syst Rev. 2022 Jun 19;11(1):124. doi: 10.1186/s13643-022-01934-3. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-022-01934-3 .10.1186/s13643-022-01934-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rodgers M, Raine G, Thomas S, Harden M, Eastwood A. Informing NHS policy in ‘digital-first primary care’: a rapid evidence synthesis. Health Serv Deliv Res. 2019 Dec;7(41):1–124. doi: 10.3310/hsdr07410. [DOI] [PubMed] [Google Scholar]
- 10.Thiyagarajan A, Grant C, Griffiths F, Atherton H. Exploring patients' and clinicians' experiences of video consultations in primary care: a systematic scoping review. BJGP Open. 2020 Mar 17;4(1):bjgpopen20X101020. doi: 10.3399/bjgpopen20x101020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Guidance and standard operating procedures: general practice in the context of coronavirus (COVID-19) Version 3.4. Sheffield Local Medical Committee. 2020. Aug 10, [2024-11-06]. https://tinyurl.com/2s362d9z .
- 12.Gausvik C, Jabbarpour Y. COVID-19 Timeline: Centers for Medicare and Medicaid Services (CMS) changes and primary care support were not enough to prevent practice losses. J Am Board Fam Med. 2021 Feb;34(Suppl):S7–S9. doi: 10.3122/jabfm.2021.S1.200305. http://www.jabfm.org/cgi/pmidlookup?view=long&pmid=33622808 .34/Supplement/S7 [DOI] [PubMed] [Google Scholar]
- 13.Southgate G, Yassaee AA, Harmer MJ, Livesey H, Pryde K, Roland D. Use of telemedicine in pediatric services for 4 representative clinical conditions: scoping review. J Med Internet Res. 2022 Oct 26;24(10):e38267. doi: 10.2196/38267. https://www.jmir.org/2022/10/e38267/ v24i10e38267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Weiner S. What happens to telemedicine after COVID-19? Association of American Medical Colleges. 2021. Oct 21, [2022-11-26]. https://www.aamc.org/news-insights/what-happens-telemedicine-after-covid-19 .
- 15.Doarn CR. The receding tide: is telemedicine in retreat? Telemed J E Health. 2022 Nov 01;28(11):1553–1554. doi: 10.1089/tmj.2022.29082.editorial. [DOI] [PubMed] [Google Scholar]
- 16.Dodoo JE, Al-Samarraie H, Alzahrani AI. Telemedicine use in Sub-Saharan Africa: Barriers and policy recommendations for Covid-19 and beyond. Int J Med Inform. 2021 Jul;151:104467. doi: 10.1016/j.ijmedinf.2021.104467. https://europepmc.org/abstract/MED/33915421 .S1386-5056(21)00093-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pierce W, Schroeder D, Suchecki R. Telehealth in Latin America: progress, challenges, and opportunities in the face of COVID-19. Telehealth Med Today. 2021 Jan 28;6(1):1. doi: 10.30953/tmt.v6.238. https://telehealthandmedicinetoday.com/index.php/journal/article/view/238 . [DOI] [Google Scholar]
- 18.Aromataris E, Munn Z. JBI manual for evidence synthesis. JBI. 2020:1. doi: 10.46658/JBIMES-20-01. https://jbi-global-wiki.refined.site/space/MANUAL . [DOI] [Google Scholar]
- 19.Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, McInerney P, Godfrey CM, Khalil H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020 Oct;18(10):2119–2126. doi: 10.11124/JBIES-20-00167.02174543-202010000-00004 [DOI] [PubMed] [Google Scholar]
- 20.Pollock D, Peters M, Khalil H, McInerney P, Alexander L, Tricco A, Evans C, de Moraes ÉB, Godfrey CM, Pieper D, Saran A, Stern C, Munn Z. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evid Synth. 2023 Mar 01;21(3):520–532. doi: 10.11124/JBIES-22-00123.02174543-990000000-00076 [DOI] [PubMed] [Google Scholar]
- 21.Olszewski C, Thomson S, Strauss L, Graham R, Ezzeddine M, Dodenhoff K, Ambrosini A, Smith LD, Silla L, Schreiber A, Caraci C, Guzik A, Strowd RE. Patient experiences with ambulatory telehealth in neurology: results of a mixed-methods study. Neurol Clin Pract. 2021 Dec;11(6):484–496. doi: 10.1212/CPJ.0000000000001072. https://europepmc.org/abstract/MED/34992956 .NEURCLINPRACT2020069121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.WHO Global Observatory for eHealth Telemedicine: opportunities and developments in Member States: report on the second global survey on eHealth. World Health Organization. 2010. [2024-11-06]. https://iris.who.int/handle/10665/44497 .
- 23.Adams RJ, Smart P, Huff AS. Shades of grey: guidelines for working with the grey literature in systematic reviews for management and organizational studies. Int J Management Reviews. 2016 Apr 19;19(4):432–454. doi: 10.1111/ijmr.12102. [DOI] [Google Scholar]
- 24.Tyndall J. How low can you go? Toward a hierarchy of Grey Literature. Dreaming 08 – Australian Library and Information Association Biennial Conference; September 2-5, 2008; Alice Springs, NT, Australia. 2008. https://core.ac.uk/download/pdf/14931482.pdf . [DOI] [Google Scholar]
- 25.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson Asbjørn, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. https://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Interim process and methods for developing rapid guidelines on COVID-19. NICE. 2020. Mar 20, [2024-11-06]. https://www.nice.org.uk/process/pmg35 .
- 27.Downes MJ, Mervin MC, Byrnes JM, Scuffham PA. Telemedicine for general practice: a systematic review protocol. Syst Rev. 2015 Oct 05;4(1):134. doi: 10.1186/s13643-015-0115-2. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-015-0115-2 .10.1186/s13643-015-0115-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.How to compare Ovid MEDLINE and PubMed. Wolters Kluwer Health. 2019. Nov, [2024-11-06]. https://tinyurl.com/442zne52 .
- 29.Assenza G, Lanzone J, Brigo F, Coppola A, Di Gennaro G, Di Lazzaro V, Ricci L, Romigi A, Tombini M, Mecarelli O. Epilepsy care in the time of COVID-19 pandemic in Italy: risk factors for seizure worsening. Front Neurol. 2020;11:737. doi: 10.3389/fneur.2020.00737. https://europepmc.org/abstract/MED/32719655 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Garousi V, Felderer M, Mäntylä MV. Guidelines for including grey literature and conducting multivocal literature reviews in software engineering. Information and Software Technology. 2019 Feb;106:101–121. doi: 10.1016/j.infsof.2018.09.006. [DOI] [Google Scholar]
- 31.Altingovde IS, Demir E, Can F, Ulusoy Ö. Site-based dynamic pruning for query processing in search engines. SIGIR '08: 31st annual international ACM SIGIR conference on Research and development in information retrieval; July 20-24, 2008; Singapore, Singapore. 2008. [DOI] [Google Scholar]
- 32.Szmuda T, Özdemir C, Ali S, Singh A, Syed M, Słoniewski P. Readability of online patient education material for the novel coronavirus disease (COVID-19): a cross-sectional health literacy study. Public Health. 2020 Aug;185:21–25. doi: 10.1016/j.puhe.2020.05.041. https://europepmc.org/abstract/MED/32516624 .S0033-3506(20)30203-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Beel J, Gipp B. Google Scholar's Ranking Algorithm: The Impact of Articles' Age (An Empirical Study). Sixth International Conference on Information Technology: New Generations; April 27-29, 2009; Las Vegas, NV. 2009. [DOI] [Google Scholar]
- 34.Petticrew M, Roberts H. Systematic Reviews in the Social Sciences: A Practical Guide. Hoboken, NJ: John Wiley & Sons; 2008. [Google Scholar]
- 35.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016 Dec 05;5(1):210. doi: 10.1186/s13643-016-0384-4. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0384-4 .10.1186/s13643-016-0384-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Greenhalgh T, Wherton J, Papoutsi C, Lynch J, Hughes G, A'Court C, Hinder S, Fahy N, Procter R, Shaw S. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017 Nov 01;19(11):e367. doi: 10.2196/jmir.8775. https://www.jmir.org/2017/11/e367/ v19i11e367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pant I, Khosla S, Lama JT, Shanker V, AlKhaldi M, El-Basuoni A, Michel B, Bitar K, Nsofor IM. Decolonising global health evaluation: Synthesis from a scoping review. PLOS Glob Public Health. 2022 Nov 16;2(11):e0000306. doi: 10.1371/journal.pgph.0000306. https://europepmc.org/abstract/MED/36962490 .PGPH-D-21-00518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kumar M, Atwoli L, Burgess RA, Gaddour N, Huang KY, Kola L, Mendenhall E, Mugo C, Mutamba BB, Nakasujja N, Njuguna I, Obasi A, Petersen I, Shidhaye R. What should equity in global health research look like? The Lancet. 2022 Jul;400(10347):145–147. doi: 10.1016/s0140-6736(22)00888-1. [DOI] [PubMed] [Google Scholar]
- 39.van Wyk A. Decolonising research methods and knowledge: implications for stepping into a post-doctoral role. Health & Social Care Workforce. 2022. Aug 02, [2024-11-06]. https://tinyurl.com/34xcnf7c .
- 40.Adams L, Lester S, Hoon E, van der Haak H, Proudman C, Hall C, Whittle S, Proudman S, Hill CL. Patient satisfaction and acceptability with telehealth at specialist medical outpatient clinics during the COVID-19 pandemic in Australia. Intern Med J. 2021 Jul;51(7):1028–1037. doi: 10.1111/imj.15205. https://europepmc.org/abstract/MED/34213046 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Alhajri N, Simsekler MCE, Alfalasi B, Alhashmi M, AlGhatrif M, Balalaa N, Al Ali M, Almaashari R, Al Memari S, Al Hosani F, Al Zaabi Y, Almazroui S, Alhashemi H, Baltatu OC. Physicians' attitudes toward telemedicine consultations during the COVID-19 pandemic: cross-sectional study. JMIR Med Inform. 2021 Jun 01;9(6):e29251. doi: 10.2196/29251. https://medinform.jmir.org/2021/6/e29251/ v9i6e29251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alharbi KG, Aldosari MN, Alhassan AM, Alshallal KA, Altamimi AM, Altulaihi BA. Patient satisfaction with virtual clinic during Coronavirus disease (COVID-19) pandemic in primary healthcare, Riyadh, Saudi Arabia. J Family Community Med. 2021;28(1):48–54. doi: 10.4103/jfcm.JFCM_353_20. https://europepmc.org/abstract/MED/33679189 .JFCM-28-48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Aliberti GM, Bhatia R, Desrochers LB, Gilliam EA, Schonberg MA. Perspectives of primary care clinicians in Massachusetts on use of telemedicine with adults aged 65 and older during the COVID-19 pandemic. Prev Med Rep. 2022 Apr;26:101729. doi: 10.1016/j.pmedr.2022.101729. https://linkinghub.elsevier.com/retrieve/pii/S2211-3355(22)00036-5 .S2211-3355(22)00036-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Al-Iede M, Waters K, Aleidi S, Alqutawneh B, Alnawaiseh H, Alshraideh A, Almaaitah S, Mahmoud R, Abualsoud R, Kiswani A, Al-Zayadneh E, Yousef AM. Impact of COVID-19 lockdown on children with asthma in Jordan: a parental questionnaire. BMJ Paediatr Open. 2021;5(1):e001136. doi: 10.1136/bmjpo-2021-001136. https://europepmc.org/abstract/MED/34222681 .bmjpo-2021-001136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Altulaihi BA, Alharbi KG, Alhassan AM, Altamimi AM, Al Akeel MA. Physician's perception toward using telemedicine during COVID-19 pandemic in King Abdulaziz Medical City, Riyadh, Saudi Arabia. Cureus. 2021 Jul;13(7):e16107. doi: 10.7759/cureus.16107. https://europepmc.org/abstract/MED/34350074 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Dimer NA, do Canto-Soares N, Dos Santos-Teixeira L, de Goulart BNG. The COVID-19 pandemic and the implementation of telehealth in speech-language and hearing therapy for patients at home: an experience report. Codas. 2020;32(3):e20200144. doi: 10.1590/2317-1782/20192020144. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S2317-17822020000300401&lng=en&nrm=iso&tlng=en .S2317-17822020000300401 [DOI] [PubMed] [Google Scholar]
- 47.Ball E, Rivas C, Khan R. If virtual gynecology clinics are here to stay, we need to include everyone. AJOG Glob Rep. 2022 Feb;2(1):100043. doi: 10.1016/j.xagr.2021.100043. https://linkinghub.elsevier.com/retrieve/pii/S2666-5778(21)00041-1 .S2666-5778(21)00041-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Barkai G, Gadot M, Amir H, Menashe M, Shvimer-Rothschild L, Zimlichman E. Patient and clinician experience with a rapidly implemented large-scale video consultation program during COVID-19. Int J Qual Health Care. 2021 Feb 20;33(1):1. doi: 10.1093/intqhc/mzaa165. https://europepmc.org/abstract/MED/33313891 .6033552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Belenkiy IG. COVID-19 challenge: what has been done and what must be done? Traumatology and Orthopedics of Russia. 2020 Jul 06;26(2):15–19. doi: 10.21823/2311-2905-2020-26-2-15-19. [DOI] [Google Scholar]
- 50.Berg WT, Goldstein M, Melnick AP, Rosenwaks Z. Clinical implications of telemedicine for providers and patients. Fertil Steril. 2020 Dec;114(6):1129–1134. doi: 10.1016/j.fertnstert.2020.10.048. https://linkinghub.elsevier.com/retrieve/pii/S0015-0282(20)32620-0 .S0015-0282(20)32620-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bergman D, Bethell C, Gombojav N, Hassink S, Stange KC. Physical distancing with social connectedness. Ann Fam Med. 2020 May 01;18(3):272–277. doi: 10.1370/afm.2538. http://www.annfammed.org/cgi/pmidlookup?view=long&pmid=32393566 .18/3/272 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Byrne E, Watkinson S. Patient and clinician satisfaction with video consultations during the COVID-19 pandemic: an opportunity for a new way of working. J Orthod. 2021 Mar;48(1):64–73. doi: 10.1177/1465312520973677. [DOI] [PubMed] [Google Scholar]
- 53.Chesnel C, Hentzen C, Le Breton F, Turmel N, Tan E, Haddad R, Amarenco G. Efficiency and satisfaction with telephone consultation of follow-up patients in neuro-urology: Experience of the COVID-19 pandemic. Neurourol Urodyn. 2021 Mar;40(3):929–937. doi: 10.1002/nau.24651. https://europepmc.org/abstract/MED/33675263 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Chiang C, Halker Singh R, Lalvani N, Shubin Stein K, Henscheid Lorenz D, Lay C, Dodick DW, Newman LC. Patient experience of telemedicine for headache care during the COVID-19 pandemic: An American Migraine Foundation survey study. Headache. 2021 May;61(5):734–739. doi: 10.1111/head.14110. https://europepmc.org/abstract/MED/34021595 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.La Telemedicina Cara a Cara. Comité de ética asistencial de Atención Primaria de Bizkaia. 2020. Dec, [2022-10-26]. https://osalde.org/wp-content/uploads/2021/01/Telemedicina-aspectos-%C3%A9ticos-CEAAPB.pdf .
- 56.Conway J, Krieger P, Hasanaj L, Sun L, Scharf JM, Odel JG, Dinkin MJ, Oliveira C, Mackay DD, Rasool N, Ko M, Rucker JC, Galetta SL, Balcer LJ. Telemedicine evaluations in neuro-ophthalmology during the COVID-19 pandemic: patient and physician surveys. J Neuroophthalmol. 2021 Sep 01;41(3):356–361. doi: 10.1097/WNO.0000000000001370.00041327-202109000-00012 [DOI] [PubMed] [Google Scholar]
- 57.Curtis M, Duncan R, Jing M, Kim A, Lu VT, Redshaw J, Stevens RRY, Truppman-Lattie D, Young S, Zhou D, Fairchild-Brunt T, Hancox RJ, Atmore C. "Not a perfect situation, but..." A single-practice survey of patient experience of phone consultations during COVID-19 Alert Level 4 in New Zealand. N Z Med J. 2021 Oct 22;134(1544):35–48. [PubMed] [Google Scholar]
- 58.Day K, Hunter I, Rao V, Russell G, Roskvist R, Moir F, Gill E, van der Werf B. Survey protocol for exploring video and phone use in Aotearoa New Zealand general practice: considerations for future telehealth. BMJ Health Care Inform. 2021 Mar;28(1):1. doi: 10.1136/bmjhci-2020-100309. https://informatics.bmj.com/lookup/pmidlookup?view=long&pmid=33753326 .bmjhci-2020-100309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Dempsey CM, Serino-Cipoletta JM, Marinaccio BD, O'Malley KA, Goldberg NE, Dolan CM, Parker-Hartigan L, Williams LS, Vessey JA. Determining factors that influence parents' perceptions of telehealth provided in a pediatric gastroenterological practice: A quality improvement project. J Pediatr Nurs. 2022;62:36–42. doi: 10.1016/j.pedn.2021.11.023.S0882-5963(21)00354-7 [DOI] [PubMed] [Google Scholar]
- 60.Dhahri AA, Iqbal MR, Pardoe H. Agile application of video telemedicine during the COVID-19 pandemic. Cureus. 2020 Nov 04;12(11):e11320. doi: 10.7759/cureus.11320. https://europepmc.org/abstract/MED/33262918 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dietzen A, Ide W, Pavone L. Telehealth in pediatric rehabilitation medicine: A survey of clinician reported utilization and experience. J Pediatr Rehabil Med. 2020;13(3):281–288. doi: 10.3233/PRM-200762.PRM200762 [DOI] [PubMed] [Google Scholar]
- 62.Dooley AB, Houssaye NDL, Baum N. Use of telemedicine for sexual medicine patients. Sex Med Rev. 2020 Oct;8(4):507–517. doi: 10.1016/j.sxmr.2020.06.001. https://europepmc.org/abstract/MED/32739238 .S2050-0521(20)30061-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Dopelt K, Avni N, Haimov-Sadikov Y, Golan I, Davidovitch N. Telemedicine and eHealth literacy in the era of COVID-19: a cross-sectional study in a peripheral clinic in Israel. Int J Environ Res Public Health. 2021 Sep 10;18(18):9556. doi: 10.3390/ijerph18189556. https://www.mdpi.com/resolver?pii=ijerph18189556 .ijerph18189556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Board of Directors Meeting - Open (Thursday 27 May 2021) East Kent Hospitals NHS Foundation Trust. 2021. [2024-12-05]. https://www.ekhuft.nhs.uk/about-us/board-of-directors/
- 65.Ennis M, Wahl K, Jeong D, Knight K, Renner R, Munro S, Dunn S, Guilbert E, Norman WV. The perspective of Canadian health care professionals on abortion service during the COVID-19 pandemic. Fam Pract. 2021 Aug 27;38(Suppl 1):i30–i36. doi: 10.1093/fampra/cmab083. https://europepmc.org/abstract/MED/34448482 .6358430 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Estudio sobre la consulta de salud virtual y sus beneficios para el sistema sanitario. EsadeGov. 2020. Jul 16, [2022-10-26]. https://tinyurl.com/463ek5dw .
- 67.Esper GJ, Sweeney RL, Winchell E, Duffell JM, Kier SC, Lukens HW, Krupinski EA. Rapid systemwide implementation of outpatient telehealth in response to the COVID-19 pandemic. J Healthc Manag. 2020;65(6):443–452. doi: 10.1097/JHM-D-20-00131. https://europepmc.org/abstract/MED/33074968 .00115514-202012000-00013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.The organisation of resilient health and social care following the COVID-19 pandemic. European Commission. 2020. [2022-10-26]. https://health.ec.europa.eu/system/files/2020-12/026_health_socialcare_covid19_en_0.pdf .
- 69.Florea M, Lazea C, Gaga R, Sur G, Lotrean L, Puia A, Stanescu AMA, Lupsor-Platon M, Florea H, Sur ML. Lights and shadows of the perception of the use of telemedicine by Romanian family doctors during the COVID-19 pandemic. Int J Gen Med. 2021;14:1575–1587. doi: 10.2147/IJGM.S309519. https://europepmc.org/abstract/MED/33953605 .309519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Fluhr JW, Gueguen A, Legoupil D, Brenaut E, Abasq C, Araújo H, Misery L. Teledermatology in times of COVID-19 confinement: comparing patients' and physicians' satisfaction by the Standardized Brest Teledermatology Questionnaire. Dermatology. 2021 Feb 10;237(2):1–6. doi: 10.1159/000514029. https://doi.org/10.1159/000514029 .000514029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Frank HE, Grumbach NM, Conrad SM, Wheeler J, Wolff J. Mental health services in primary care: Evidence for the feasibility of telehealth during the COVID-19 pandemic. J Affect Disord Rep. 2021 Jul;5:100146. doi: 10.1016/j.jadr.2021.100146. https://linkinghub.elsevier.com/retrieve/pii/S2666-9153(21)00073-1 .S2666-9153(21)00073-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Franzosa E, Gorbenko K, Brody AA, Leff B, Ritchie CS, Kinosian B, Sheehan OC, Federman AD, Ornstein KA. "There is something very personal about seeing someone's face": provider perceptions of video visits in home-based primary care during COVID-19. J Appl Gerontol. 2021 Nov;40(11):1417–1424. doi: 10.1177/07334648211028393. https://europepmc.org/abstract/MED/34210200 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Franzosa E, Gorbenko K, Brody AA, Leff B, Ritchie CS, Kinosian B, Ornstein KA, Federman AD. "At Home, with Care": lessons from New York City home-based primary care practices managing COVID-19. J Am Geriatr Soc. 2021 Feb;69(2):300–306. doi: 10.1111/jgs.16952. https://europepmc.org/abstract/MED/33179761 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Fu L, Lindenmeyer A, Phillimore J, Lessard-Phillips L. Vulnerable migrants' access to healthcare in the early stages of the COVID-19 pandemic in the UK. Public Health. 2022 Feb;203:36–42. doi: 10.1016/j.puhe.2021.12.008. https://europepmc.org/abstract/MED/35026578 .S0033-3506(21)00469-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Gold KJ, Laurie AR, Kinney DR, Harmes KM, Serlin DC. Video visits: family physician experiences with uptake during the COVID-19 pandemic. Fam Med. 2021 Mar 4;53(3):207–210. doi: 10.22454/fammed.2021.613099. [DOI] [PubMed] [Google Scholar]
- 76.Gray DP, Sidaway-Lee K, Harding A, Evans P. Reduction in face-to-face GP consultations. Br J Gen Pract. 2020 Jul;70(696):328. doi: 10.3399/bjgp20X710849. https://bjgp.org/lookup/pmidlookup?view=long&pmid=32586804 .70/696/328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Grens H, de Bruin JP, Huppelschoten A, Kremer JAM. Fertility workup with video consultation during the COVID-19 pandemic: pilot quantitative and qualitative study. JMIR Form Res. 2022 Feb 07;6(2):e32000. doi: 10.2196/32000.v6i2e32000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Grosman-Dziewiszek P, Wiatrak B, Jęśkowiak I, Szeląg A. Patients' habits and the role of pharmacists and telemedicine as elements of a modern health care system during the COVID-19 pandemic. J Clin Med. 2021 Sep 17;10(18):4211. doi: 10.3390/jcm10184211. https://www.mdpi.com/resolver?pii=jcm10184211 .jcm10184211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Gupta T, Gkiousias V, Bhutta MF. A systematic review of outcomes of remote consultation in ENT. Clin Otolaryngol. 2021 Jul;46(4):699–719. doi: 10.1111/coa.13768. [DOI] [PubMed] [Google Scholar]
- 80.Hardcastle L, Ogbogu U. Virtual care: Enhancing access or harming care? Healthc Manage Forum. 2020 Nov 20;33(6):288–292. doi: 10.1177/0840470420938818. https://journals.sagepub.com/doi/abs/10.1177/0840470420938818?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Hays RD, Skootsky SA. Patient experience with in-person and telehealth visits before and during the COVID-19 pandemic at a large integrated health system in the United States. J Gen Intern Med. 2022 Mar;37(4):847–852. doi: 10.1007/s11606-021-07196-4. https://europepmc.org/abstract/MED/34982370 .10.1007/s11606-021-07196-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Heyck Lee S, Ramondino S, Gallo K, Moist LM. A quantitative and qualitative study on patient and physician perceptions of nephrology telephone consultation during COVID-19. Can J Kidney Health Dis. 2022;9:20543581211066720. doi: 10.1177/20543581211066720. https://journals.sagepub.com/doi/abs/10.1177/20543581211066720?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_20543581211066720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Hofmann G, Hampanda K, Harrison MS, Fasano M, Nacht A, Yeoman M. Virtual prenatal and postpartum care acceptability among maternity care providers. Matern Child Health J. 2022 Jul 15;26(7):1401–1408. doi: 10.1007/s10995-022-03412-7. https://europepmc.org/abstract/MED/35292887 .10.1007/s10995-022-03412-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Holtz BE. Patients perceptions of telemedicine visits before and after the coronavirus disease 2019 pandemic. Telemed J E Health. 2021 Jan 01;27(1):107–112. doi: 10.1089/tmj.2020.0168. https://home.liebertpub.com/tmj . [DOI] [PubMed] [Google Scholar]
- 85.Imlach F, McKinlay E, Middleton L, Kennedy J, Pledger M, Russell L, Churchward M, Cumming J, McBride-Henry K. Telehealth consultations in general practice during a pandemic lockdown: survey and interviews on patient experiences and preferences. BMC Fam Pract. 2020 Dec 13;21(1):269. doi: 10.1186/s12875-020-01336-1. https://bmcfampract.biomedcentral.com/articles/10.1186/s12875-020-01336-1 .10.1186/s12875-020-01336-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Isautier JM, Copp T, Ayre J, Cvejic E, Meyerowitz-Katz G, Batcup C, Bonner C, Dodd R, Nickel B, Pickles K, Cornell S, Dakin T, McCaffery KJ. People's experiences and satisfaction with telehealth during the COVID-19 pandemic in Australia: cross-sectional survey study. J Med Internet Res. 2020 Dec 10;22(12):e24531. doi: 10.2196/24531. https://www.jmir.org/2020/12/e24531/ v22i12e24531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Itamura K, Tang DM, Higgins TS, Rimell FL, Illing EA, Ting JY, Lee MK, Wu A. Comparison of patient satisfaction between virtual visits during the COVID-19 pandemic and in-person visits pre-pandemic. Ann Otol Rhinol Laryngol. 2021 Jul;130(7):810–817. doi: 10.1177/0003489420977766. https://journals.sagepub.com/doi/abs/10.1177/0003489420977766?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Javanparast S, Roeger L, Kwok Y, Reed RL. The experience of Australian general practice patients at high risk of poor health outcomes with telehealth during the COVID-19 pandemic: a qualitative study. BMC Fam Pract. 2021 Apr 08;22(1):69. doi: 10.1186/s12875-021-01408-w. https://bmcfampract.biomedcentral.com/articles/10.1186/s12875-021-01408-w .10.1186/s12875-021-01408-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Jhaveri D, Emeto TI, Alele FO, Strom A, Benham H. Use of telemedicine for rheumatology practice in Queensland, Australia: experiences before and during the COVID-19 pandemic. Intern Med J. 2022 Oct;52(10):1685–1690. doi: 10.1111/imj.15706. [DOI] [PubMed] [Google Scholar]
- 90.Johnsen TM, Norberg BL, Kristiansen E, Zanaboni P, Austad B, Krogh FH, Getz L. Suitability of video consultations during the COVID-19 pandemic lockdown: cross-sectional survey among Norwegian general practitioners. J Med Internet Res. 2021 Feb 08;23(2):e26433. doi: 10.2196/26433. https://www.jmir.org/2021/2/e26433/ v23i2e26433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Johnson C, Dupuis JB, Goguen P, Grenier G. Changes to telehealth practices in primary care in New Brunswick (Canada): A comparative study pre and during the COVID-19 pandemic. PLoS One. 2021;16(11):e0258839. doi: 10.1371/journal.pone.0258839. https://dx.plos.org/10.1371/journal.pone.0258839 .PONE-D-21-16369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Jonnagaddala J, Godinho MA, Liaw S. From telehealth to virtual primary care in Australia? A Rapid scoping review. Int J Med Inform. 2021 Jul;151:104470. doi: 10.1016/j.ijmedinf.2021.104470. https://europepmc.org/abstract/MED/34000481 .S1386-5056(21)00096-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Kalwani NM, Wang KM, Johnson AN, Deb JD, Gold T, Maddukuri AK, Savage EG, Parameswaran V, Dash R, Scheinker D, Rodriguez F. Application of the Quadruple Aim to evaluate the operational impact of a telemedicine program. Healthc (Amst) 2021 Dec;9(4):100593. doi: 10.1016/j.hjdsi.2021.100593. https://europepmc.org/abstract/MED/34749227 .S2213-0764(21)00076-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Kamimura A, Panahi S, Meng H, Sundrud J, Lucero M. Patient satisfaction with telehealth and dxperiences during the COVID-19 pandemic among uninsured free clinic patients. J Patient Exp. 2021 Jul 26;8:23743735211033107. doi: 10.1177/23743735211033107. https://journals.sagepub.com/doi/abs/10.1177/23743735211033107?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_23743735211033107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Karacabeyli D, Shea S, Keidar S, Pinkney S, Bepple K, Edwards D, Hale I, Suleman S, Amed S. The Live 5-2-1-0 Toolkit for family physicians: Mixed methods evaluation of a resource to facilitate health promotion in a primary care setting. BC Medical Journal. 2020;62(6):1. https://bcmj.org/articles/live-5-2-1-0-toolkit-family-physicians-mixed-methods-evaluation-resource-facilitate-health . [Google Scholar]
- 96.Kato-Lin Y, Thelen ST. Telemedicine for acute conditions during COVID-19: a nationwide survey using crowdsourcing. Telemed J E Health. 2021 Jul;27(7):714–723. doi: 10.1089/tmj.2020.0351. [DOI] [PubMed] [Google Scholar]
- 97.Khan ZA, Zahoor A, Afzal I, Butt U, Siddiqui AM, Khan Z, Shah IA, Shah JA. Evaluation of patient perception and satisfaction toward the use of telemedicine during pandemic of novel coronavirus in Pakistan. Telemed J E Health. 2021 Oct;27(10):1174–1179. doi: 10.1089/tmj.2020.0343. [DOI] [PubMed] [Google Scholar]
- 98.Kirby DJ, Fried JW, Buchalter DB, Moses MJ, Hurly ET, Cardone DA, Yang SS, Virk MS, Rokito AS, Jazrawi LM, Campbell KA. Patient and physician satisfaction with telehealth during the COVID-19 pandemic: sports medicine perspective. Telemed J E Health. 2021 Oct;27(10):1151–1159. doi: 10.1089/tmj.2020.0387. [DOI] [PubMed] [Google Scholar]
- 99.Kletečka-Pulker M, Völkl-Kernstock S, Fassl A, Klager E, Willschke H, Klomfar S, Wochele-Thoma T, Schaden E, Atanasov AG. Telehealth in times of COVID-19: spotlight on Austria. Healthcare (Basel) 2021 Mar 04;9(3):1. doi: 10.3390/healthcare9030280. https://www.mdpi.com/resolver?pii=healthcare9030280 .healthcare9030280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Kling SMR, Falco-Walter JJ, Saliba-Gustafsson EA, Garvert DW, Brown-Johnson CG, Miller-Kuhlmann R, Shaw JG, Asch SM, Yang L, Gold CA, Winget M. Patient and clinician perspectives of new and return ambulatory teleneurology visits. Neurol Clin Pract. 2021 Dec;11(6):472–483. doi: 10.1212/CPJ.0000000000001065. https://europepmc.org/abstract/MED/34992955 .NEURCLINPRACT2020068197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Kludacz-Alessandri M, Walczak R, Hawrysz L, Korneta P. The quality of medical care in the conditions of the COVID-19 pandemic, with particular emphasis on the access to primary healthcare and the effectiveness of treatment in Poland. J Clin Med. 2021 Aug 09;10(16):3502. doi: 10.3390/jcm10163502. https://www.mdpi.com/resolver?pii=jcm10163502 .jcm10163502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Kludacz-Alessandri M, Hawrysz L, Korneta P, Gierszewska G, Pomaranik W, Walczak R. The impact of medical teleconsultations on general practitioner-patient communication during COVID- 19: A case study from Poland. PLoS One. 2021;16(7):e0254960. doi: 10.1371/journal.pone.0254960. https://dx.plos.org/10.1371/journal.pone.0254960 .PONE-D-21-15441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Krasovsky T, Silberg T, Barak S, Eisenstein E, Erez N, Feldman I, Guttman D, Liber P, Patael SZ, Sarna H, Sadeh Y, Steinberg P, Landa J. Transition to multidisciplinary pediatric telerehabilitation during the COVID-19 pandemic: strategy development and implementation. Int J Environ Res Public Health. 2021 Feb 04;18(4):1. doi: 10.3390/ijerph18041484. https://www.mdpi.com/resolver?pii=ijerph18041484 .ijerph18041484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Kumar S, Kumar A, Kumar M, Kumar A, Arora R, Sehrawat R. Feasibility of telemedicine in maintaining follow-up of orthopaedic patients and their satisfaction: A preliminary study. J Clin Orthop Trauma. 2020 Oct;11(Suppl 5):S704–S710. doi: 10.1016/j.jcot.2020.07.026. https://europepmc.org/abstract/MED/32837105 .S0976-5662(20)30353-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Kumar P, Aggarwal M, Dhawan R, Dass J, Kumar G, Sharma V, Mirza S, Senapati J, Ganju N, Vaid T, Vijayran M, Panda T, Pragna GS, Krishna SS, Khandelwal A, Verghese R, Tyagi S, Seth T, Mahapatra M. Tele-medicine services in hematological practice during Covid pandemic: its feasibility and difficulties. Indian J Hematol Blood Transfus. 2021 Oct;37(4):528–533. doi: 10.1007/s12288-020-01385-7. https://europepmc.org/abstract/MED/33250594 .1385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Kurotschka PK, Serafini A, Demontis M, Serafini A, Mereu A, Moro MF, Carta MG, Ghirotto L. General practitioners' experiences during the first phase of the COVID-19 pandemic in Italy: a critical incident technique study. Front Public Health. 2021;9:623904. doi: 10.3389/fpubh.2021.623904. https://europepmc.org/abstract/MED/33614587 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.LeBrun DG, Malfer C, Wilson M, Carroll KM, Wang Ms V, Mayman DJ, Cross MB, Alexiades MM, Jerabek SA, Cushner FD, Vigdorchik JM, Haas SB, Ast MP. Telemedicine in an outpatient arthroplasty setting during the COVID-19 pandemic: early lessons from New York City. HSS J. 2021 Feb;17(1):25–30. doi: 10.1177/1556331620972659. https://journals.sagepub.com/doi/abs/10.1177/1556331620972659?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_1556331620972659 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Lewis YD, Elran-Barak R, Grundman-Shem Tov R, Zubery E. The abrupt transition from face-to-face to online treatment for eating disorders: a pilot examination of patients' perspectives during the COVID-19 lockdown. J Eat Disord. 2021 Mar 05;9(1):31. doi: 10.1186/s40337-021-00383-y. https://jeatdisord.biomedcentral.com/articles/10.1186/s40337-021-00383-y .10.1186/s40337-021-00383-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Li E, Tsopra R, Jimenez G, Serafini A, Gusso G, Lingner H, Fernandez M, Irving G, Petek D, Hoffman R, Lazic V, Memarian Ensieh, Koskela T, Collins C, Espitia S, Clavería Ana, Nessler K, O'Neill Braden Gregory, Hoedebecke K, Ungan M, Laranjo L, Ghafur S, Fontana G, Majeed A, Car J, Darzi A, Neves A. General practitioners' perceptions of using virtual primary care during the COVID-19 pandemic: An international cross-sectional survey study. PLOS Digit Health. 2022 May;1(5):e0000029. doi: 10.1371/journal.pdig.0000029. https://europepmc.org/abstract/MED/36812543 .PDIG-D-21-00123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Lopez Guzman Y, Barros Castillo SM, Leal Betancourt MI. Condiciones de vulnerabilidad, sociodemográficas y clínicas de la población con COVID-19 incluida en la estrategia de atención primaria en salud. Mosquera, 2020. Universidad del Rosario. 2021. Oct, [2022-10-26]. https://tinyurl.com/2ckxdpnu .
- 111.Maher DP, Hess D, Edwards C, Allen L. Changes in patient satisfaction scores during the early COVID-19 pandemic. J Patient Exp. 2021;8:23743735211034610. doi: 10.1177/23743735211034610. https://journals.sagepub.com/doi/abs/10.1177/23743735211034610?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_23743735211034610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Malliaras P, Merolli M, Williams CM, Caneiro JP, Haines T, Barton C. 'It's not hands-on therapy, so it's very limited': Telehealth use and views among allied health clinicians during the coronavirus pandemic. Musculoskelet Sci Pract. 2021 Apr;52:102340. doi: 10.1016/j.msksp.2021.102340. https://europepmc.org/abstract/MED/33571900 .S2468-7812(21)00024-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Manski-Nankervis J, Davidson S, Hiscock H, Hallinan C, Ride J, Lingam V, Holman J, Baird A, McKeown E, Sanci L. Primary care consumers’ experiences and opinions of a telehealth consultation delivered via video during the COVID-19 pandemic. Aust J Prim Health. 2022 Jun;28(3):224–231. doi: 10.1071/PY21193.PY21193 [DOI] [PubMed] [Google Scholar]
- 114.Massaroni V, Delle Donne V, Ciccarelli N, Ciccullo A, Borghetti A, Faliero D, Visconti E, Tamburrini E, Di Giambenedetto S. Use of telehealth for HIV care in Italy: Are doctors and patients on the same page? A cross-sectional study. Int J Med Inform. 2021 Dec;156:104616. doi: 10.1016/j.ijmedinf.2021.104616.S1386-5056(21)00242-2 [DOI] [PubMed] [Google Scholar]
- 115.Mathew T, Lee PC, Ianno DJ, Benson J. Telehealth and Australian general practice in 2020: A survey exploring patients' perspectives in the Adelaide Hills. Aust J Gen Pract. 2021 Oct;50(10):754–759. doi: 10.31128/AJGP-11-20-5727. https://www.racgp.org.au/AJGP/2021/october/telehealth-and-australian-general-practice/ [DOI] [PubMed] [Google Scholar]
- 116.Mbunge E, Batani J, Gaobotse G, Muchemwa B. Virtual healthcare services and digital health technologies deployed during coronavirus disease 2019 (COVID-19) pandemic in South Africa: a systematic review. Glob Health J. 2022 Jun;6(2):102–113. doi: 10.1016/j.glohj.2022.03.001. https://linkinghub.elsevier.com/retrieve/pii/S2414-6447(22)00023-9 .S2414-6447(22)00023-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Menhadji P, Patel R, Asimakopoulou K, Quinn B, Khoshkhounejad G, Pasha P, Garcia Sanchez R, Ide M, Kalsi P, Nibali L. Patients' and dentists' perceptions of tele-dentistry at the time of COVID-19. A questionnaire-based study. J Dent. 2021 Oct;113:103782. doi: 10.1016/j.jdent.2021.103782. https://europepmc.org/abstract/MED/34400252 .S0300-5712(21)00203-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Miller MJ, Pak SS, Keller DR, Barnes DE. Evaluation of pragmatic telehealth physical therapy implementation during the COVID-19 pandemic. Phys Ther. 2021 Jan 04;101(1):1. doi: 10.1093/ptj/pzaa193. https://europepmc.org/abstract/MED/33284318 .5930367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Mills KT, Peacock E, Chen J, Zimmerman A, He H, Cyprian A, Davis G, Fuqua SR, Gilliam DS, Greer A, Gray-Winfrey L, Williams S, Wiltz GM, Winfrey KL, Whelton PK, Krousel-Wood M, He J. Experiences and beliefs of low-income patients with hypertension in Louisiana and Mississippi during the COVID-19 pandemic. J Am Heart Assoc. 2021 Feb 02;10(3):e018510. doi: 10.1161/JAHA.120.018510. https://www.ahajournals.org/doi/abs/10.1161/JAHA.120.018510?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Moore A, Chavez C, Fisher MP. Factors enhancing trust in electronic communication among patients from an internal medicine clinic: qualitative results of the RECEPT study. J Gen Intern Med. 2022 Sep 19;37(12):3121–3127. doi: 10.1007/s11606-021-07345-9. https://europepmc.org/abstract/MED/35048293 .10.1007/s11606-021-07345-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Mostafa PIN, Hegazy AA. Dermatological consultations in the COVID-19 era: is teledermatology the key to social distancing? An Egyptian experience. J Dermatolog Treat. 2022 Mar;33(2):910–915. doi: 10.1080/09546634.2020.1789046. [DOI] [PubMed] [Google Scholar]
- 122.Gorgojo Martínez JJ, Murillo AZ, Rubio Herrera MÁ, Lesmes IB. TELECONSULTA en Endocrinología y Nutrición en tiempos de la pandemia COVID-19 y más allá. Sociedad Española de Endocrinología y Nutrición. [2024-11-06]. https://tinyurl.com/2jhyx2es .
- 123.Murren-Boezem J, Solo-Josephson P, Zettler-Greeley CM. On-demand, virtual health care during COVID-19: clinician redeployment and telemedicine utilization in a children's health system. Telemed J E Health. 2021 Oct;27(10):1111–1116. doi: 10.1089/tmj.2020.0461. [DOI] [PubMed] [Google Scholar]
- 124.Mustafa SS, Vadamalai K, Ramsey A. Patient satisfaction with in-person, video, and telephone allergy/immunology evaluations during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2021 May;9(5):1858–1863. doi: 10.1016/j.jaip.2021.01.036. https://europepmc.org/abstract/MED/33548516 .S2213-2198(21)00164-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Taskforce on Telehealth Policy (TTP): Findings and Recommendations. National Committee for Quality Assurance (NCQA) [2022-10-26]. https://tinyurl.com/4j67w4ju .
- 126.Nguyen OT, Watson AK, Motwani K, Warpinski C, McDilda K, Leon C, Khanna N, Nall RW, Turner K. Patient-level factors associated with utilization of telemedicine services from a free clinic during COVID-19. Telemed J E Health. 2022 Apr;28(4):526–534. doi: 10.1089/tmj.2021.0102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Olayiwola JN, Magaña C, Harmon A, Nair S, Esposito E, Harsh C, Forrest LA, Wexler R. Telehealth as a bright spot of the COVID-19 pandemic: recommendations from the virtual frontlines ("Frontweb") JMIR Public Health Surveill. 2020 Jun 25;6(2):e19045. doi: 10.2196/19045. https://publichealth.jmir.org/2020/2/e19045/ v6i2e19045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.O'Neill C, Matias MV, Peixoto VR, O'Neill H, Aguiar P, Castela E. [Teleconsultation in the Portuguese National Health Service during the COVID-19 pandemic: a survey of physicians' views and future implications] Acta Med Port. 2022 Jun 01;35(6):455–467. doi: 10.20344/amp.16724. https://doi.org/10.20344/amp.16724 . [DOI] [PubMed] [Google Scholar]
- 129.La Atención Primaria Rural en España lanza un grito de socorro para su supervivencia. Médicos y Pacientes. [2022-11-05]. https://tinyurl.com/3jna2w96 .
- 130.Orrange S, Patel A, Mack WJ, Cassetta J. Patient satisfaction and trust in telemedicine during the COVID-19 pandemic: retrospective observational study. JMIR Hum Factors. 2021 Apr 22;8(2):e28589. doi: 10.2196/28589. https://humanfactors.jmir.org/2021/2/e28589/ v8i2e28589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Parker K, Chia M. Patient and clinician satisfaction with video consultations in dentistry - part one: patient satisfaction. Br Dent J. 2021 May 27;:1–6. doi: 10.1038/s41415-021-3007-y. https://europepmc.org/abstract/MED/34045675 .10.1038/s41415-021-3007-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Parsons MW, Gardner MM, Sherman JC, Pasquariello K, Grieco JA, Kay CD, Pollak LE, Morgan AK, Carlson-Emerton B, Seligsohn K, Davidsdottir S, Pulsifer MB, Zarrella GV, Burstein SM, Mancuso SM. Feasibility and acceptance of direct-to-home tele-neuropsychology services during the COVID-19 pandemic. J Int Neuropsychol Soc. 2022 Feb;28(2):210–215. doi: 10.1017/S1355617721000436.S1355617721000436 [DOI] [PubMed] [Google Scholar]
- 133.Patel S, Douglas-Moore J. A reflection on an adapted approach from face-to-face to telephone consultations in our Urology Outpatient Department during the COVID-19 pandemic - a pathway for change to future practice? BJU Int. 2020 Sep 04;126(3):339–341. doi: 10.1111/bju.15119. https://europepmc.org/abstract/MED/32469096 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Written evidence submitted by Philips UKI (HSC0978) UK Parliament. 2021. Mar, [2022-10-18]. https://committees.parliament.uk/writtenevidence/25169/pdf/
- 135.Rego N, Pereira HS, Crispim J. Perceptions of patients and physicians on teleconsultation at home for diabetes mellitus: survey study. JMIR Hum Factors. 2021 Nov 23;8(4):e27873. doi: 10.2196/27873. https://humanfactors.jmir.org/2021/4/e27873/ v8i4e27873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Reicher S, Sela T, Toren O. Using telemedicine during the COVID-19 pandemic: attitudes of adult health care consumers in Israel. Front Public Health. 2021;9:653553. doi: 10.3389/fpubh.2021.653553. https://europepmc.org/abstract/MED/34079784 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Reynolds-Wright JJ, Boydell N, Cameron S, Harden J. A qualitative study of abortion care providers' perspectives on telemedicine medical abortion provision in the context of COVID-19. BMJ Sex Reprod Health. 2022 Jul;48(3):199–204. doi: 10.1136/bmjsrh-2021-201309. https://jfprhc.bmj.com/lookup/pmidlookup?view=long&pmid=34848554 .bmjsrh-2021-201309 [DOI] [PubMed] [Google Scholar]
- 138.Riedel L, Uscher-Pines L, Mehrotra A, Busch AB, Barnett ML, Raja P, Huskamp HA. Use of telemedicine for opioid use disorder treatment - Perceptions and experiences of opioid use disorder clinicians. Drug Alcohol Depend. 2021 Nov 01;228:108999. doi: 10.1016/j.drugalcdep.2021.108999. https://europepmc.org/abstract/MED/34517225 .S0376-8716(21)00494-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Rosler G. Pediatric telehealth experiences: myths and truths about video visits from a parent. J Patient Exp. 2020 Dec;7(6):836–838. doi: 10.1177/2374373520932724. https://journals.sagepub.com/doi/abs/10.1177/2374373520932724?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2374373520932724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.General practice in the post Covid world: challenges and opportunities for general practice. Royal College of General Practitioners. [2024-11-06]. https://tinyurl.com/4kkaxtxy .
- 141.Focus: artificial intelligence and technology in family medicine. Family Doctor. 2021. [2024-11-06]. https://www.nysafp.org/wp-content/uploads/2024/05/Winter-2021.pdf .
- 142.Saiyed S, Nguyen A, Singh R. Physician perspective and key satisfaction indicators with rapid telehealth adoption during the coronavirus disease 2019 pandemic. Telemed J E Health. 2021 Nov;27(11):1225–1234. doi: 10.1089/tmj.2020.0492. [DOI] [PubMed] [Google Scholar]
- 143.Scherer J, Back DA, Thienemann F, Kaufmann E, Neuhaus V, Willy C, Hepp P, Pape H, Osterhoff G. The effect of Covid-19 on the willingness to use video consultations among orthopedic and trauma outpatients: a multi-center survey in 1400 outpatients. Eur J Trauma Emerg Surg. 2022 Jun;48(3):2199–2206. doi: 10.1007/s00068-021-01774-1. https://europepmc.org/abstract/MED/34427693 .10.1007/s00068-021-01774-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Schweiberger K, Hoberman A, Iagnemma J, Schoemer P, Squire J, Taormina J, Wolfson D, Ray KN. Practice-level variation in telemedicine use in a pediatric primary care network during the COVID-19 pandemic: retrospective analysis and survey study. J Med Internet Res. 2020 Dec 18;22(12):e24345. doi: 10.2196/24345. https://www.jmir.org/2020/12/e24345/ v22i12e24345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Shachak A, Alkureishi MA. Virtual care: a 'Zoombie' apocalypse? J Am Med Inform Assoc. 2020 Nov 01;27(11):1813–1815. doi: 10.1093/jamia/ocaa185. https://europepmc.org/abstract/MED/32940711 .5907054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Sharma AE, Khoong EC, Sierra M, Rivadeneira NA, Nijagal MA, Su G, Lyles CR, DeFries T, Tuot DS, Sarkar U. System-level factors associated with telephone and video visit use: survey of safety-net clinicians during the early phase of the COVID-19 pandemic. JMIR Form Res. 2022 Mar 10;6(3):e34088. doi: 10.2196/34088. https://formative.jmir.org/2022/3/e34088/ v6i3e34088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Skelly JR, O'Connor T. Guidelines for the use of the Attend Anywhere Platform for Telecommunications within the pain service. Ir Med J. 2021 Aug 19;114(7):403. [PubMed] [Google Scholar]
- 148.Srinivasan M, Asch S, Vilendrer S, Thomas SC, Bajra R, Barman L, Edwards LM, Filipowicz H, Giang L, Jee O, Mahoney M, Nelligan I, Phadke AJ, Torres E, Artandi M. Qualitative assessment of rapid system transformation to primary care video visits at an academic medical center. Annals of Internal Medicine. 2020 Oct 06;173(7):527–535. doi: 10.7326/m20-1814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Staffieri SE, Mathew AA, Sheth SJ, Ruddle JB, Elder JE. Parent satisfaction and acceptability of telehealth consultations in pediatric ophthalmology: initial experience during the COVID-19 pandemic. J AAPOS. 2021 Apr;25(2):104–107. doi: 10.1016/j.jaapos.2020.12.003.S1091-8531(21)00049-5 [DOI] [PubMed] [Google Scholar]
- 150.Sugarman DE, Horvitz LE, Greenfield SF, Busch AB. Clinicians' perceptions of rapid scale-up of telehealth services in outpatient mental health treatment. Telemed J E Health. 2021 Dec;27(12):1399–1408. doi: 10.1089/tmj.2020.0481. https://europepmc.org/abstract/MED/33600272 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Hamui-Sutton L, Halabe-Cherem J. Videoconsultas: alcances y limitaciones. Medicina Interna de México. 2021;37(2):261–266. https://www.medigraphic.com/pdfs/medintmex/mim-2021/mim212m.pdf . [Google Scholar]
- 152.Swaminathan R, Mughal Z, Phillips D. Telephone Consultation in Otorhinolaryngology During the Coronavirus Disease 2019 Pandemic: a Cross-sectional Analysis of Effectiveness and Satisfaction for Patients and Clinicians. SN Compr Clin Med. 2022;4(1):36. doi: 10.1007/s42399-022-01119-y. https://europepmc.org/abstract/MED/35036851 .1119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Tai-Seale M, Rosen R, Ruo B, Hogarth M, Longhurst CA, Lander L, Walker AL, Stults CD, Chan A, Mazor K, Garber L, Millen M. Implementation of patient engagement tools in electronic health records to enhance patient-centered communication: protocol for feasibility evaluation and preliminary results. JMIR Res Protoc. 2021 Aug 26;10(8):e30431. doi: 10.2196/30431. https://www.researchprotocols.org/2021/8/e30431/ v10i8e30431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Taylor P, Berg C, Thompson J, Dean K, Yuan T, Nallamshetty S, Tong I. Effective access to care in a crisis period: hypertension control during the COVID-19 pandemic by telemedicine. Mayo Clin Proc Innov Qual Outcomes. 2022 Feb;6(1):19–26. doi: 10.1016/j.mayocpiqo.2021.11.006. https://linkinghub.elsevier.com/retrieve/pii/S2542-4548(21)00163-6 .S2542-4548(21)00163-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Tenforde AS, Iaccarino MA, Borgstrom H, Hefner JE, Silver J, Ahmed M, Babu AN, Blauwet CA, Elson L, Eng C, Kotler D, Homer S, Makovitch S, McInnis KC, Vora A, Borg-Stein J. Telemedicine during COVID-19 for outpatient sports and musculoskeletal medicine physicians. PM R. 2020 Sep;12(9):926–932. doi: 10.1002/pmrj.12422. https://europepmc.org/abstract/MED/32424977 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Teng T, Sareidaki DE, Chemaly N, Bar C, Coste-Zeitoun D, Kuchenbuch M, Nabbout R. Physician and patient satisfaction with the switch to remote outpatient encounters in epilepsy clinics during the Covid-19 pandemic. Seizure. 2021 Oct;91:60–65. doi: 10.1016/j.seizure.2021.05.013. https://linkinghub.elsevier.com/retrieve/pii/S1059-1311(21)00166-7 .S1059-1311(21)00166-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Thiele T, Beider S, Kühl H, Mielke G, Holz A, Hirsch S, Witte T, Hoeper K, Cossmann A, Happle C, Jablonka A, Ernst D. [Care of rheumatology patients during the lockdown in early 2020 : Telemedicine, delegation, patient satisfaction and vaccination behavior] Z Rheumatol. 2022 Mar;81(2):157–163. doi: 10.1007/s00393-021-01005-3. https://europepmc.org/abstract/MED/33974131 .10.1007/s00393-021-01005-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Tornero-Molina J, Sánchez-Alonso F, Fernández-Prada M, Bris-Ochaita M, Sifuentes-Giraldo A, Vidal-Fuentes J. Tele-rheumatology during the COVID-19 pandemic. Reumatol Clin (Engl Ed) 2020 Oct 29;18(3):157–63. doi: 10.1016/j.reuma.2020.10.004. http://www.elsevier.es/en/linksolver/pdf/pii/S1699-258X(20)30240-0 .S1699-258X(20)30240-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Tozour JN, Bandremer S, Patberg E, Zavala J, Akerman M, Chavez M, Mann DM, Testa PA, Vintzileos AM, Heo HJ. Application of telemedicine video visits in a maternal-fetal medicine practice at the epicenter of the COVID-19 pandemic. Am J Obstet Gynecol MFM. 2021 Nov;3(6):100469. doi: 10.1016/j.ajogmf.2021.100469. https://europepmc.org/abstract/MED/34450341 .S2589-9333(21)00164-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Triantafillou V, Layfield E, Prasad A, Deng J, Shanti RM, Newman JG, Rajasekaran K. Patient perceptions of head and neck ambulatory telemedicine visits: a qualitative study. Otolaryngol Head Neck Surg. 2021 May 14;164(5):923–931. doi: 10.1177/0194599820943523. [DOI] [PubMed] [Google Scholar]
- 161.Troncone A, Cascella C, Chianese A, Zanfardino A, Casaburo F, Piscopo A, Rosanio FM, di Candia F, Franzese A, Iafusco D, Mozzillo E. Doctor-patient relationship in synchronous/real-time video-consultations and in-person visits: an investigation of the perceptions of young people with type 1 diabetes and their parents during the COVID-19 pandemic. Int J Behav Med. 2022 Oct;29(5):638–647. doi: 10.1007/s12529-021-10047-5. https://europepmc.org/abstract/MED/35076861 .10.1007/s12529-021-10047-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Tulupova E, Dobiášová K, Kopsa Těšinová J. Patient experience with telemedicine in primary care during the COVID pandemic: a qualitative study. European Journal of Public Health. 2021;31(Supplement_3):ckab165.162. doi: 10.1093/eurpub/ckab165.162. [DOI] [Google Scholar]
- 163.Utley LM, Manchala GS, Phillips MJ, Doshi CP, Szatalowicz VL, Boozer JR. Bridging the telemedicine gap among seniors during the COVID-19 pandemic. J Patient Exp. 2021;8:23743735211014036. doi: 10.1177/23743735211014036. https://journals.sagepub.com/doi/abs/10.1177/23743735211014036?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_23743735211014036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Verduzco-Gutierrez M, Bean AC, Tenforde AS, Tapia RN, Silver JK. How to conduct an outpatient telemedicine rehabilitation or prehabilitation visit. PM R. 2020 Jul 07;12(7):714–720. doi: 10.1002/pmrj.12380. [DOI] [PubMed] [Google Scholar]
- 165.Verma P, Kerrison R. Patients' and physicians' experiences with remote consultations in primary care during the COVID-19 pandemic: a multi-method rapid review of the literature. BJGP Open. 2022 Jun;6(2):1. doi: 10.3399/BJGPO.2021.0192. http://bjgpopen.org/lookup/pmidlookup?view=long&pmid=35031558 .BJGPO.2021.0192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Villalobos J, Calvanese N. [The impact of COVID-19 pandemic on doctor-patient relationship] Rev Med Chil. 2021 Jul;149(7):1070–1074. doi: 10.4067/s0034-98872021000701070. http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0034-98872021000701070&lng=en&nrm=iso&tlng=en .S0034-98872021000701070 [DOI] [PubMed] [Google Scholar]
- 167.Volandes AE, Zupanc SN, Paasche-Orlow MK, Lakin JR, Chang Y, Burns EA, LaVine NA, Carney MT, Martins-Welch D, Emmert K, Itty JE, Moseley ET, Davis AD, El-Jawahri A, Gundersen DA, Fix GM, Yacoub AM, Schwartz P, Gabry-Kalikow S, Garde C, Fischer J, Henault L, Burgess L, Goldman J, Kwok A, Singh N, Alvarez Suarez AL, Gromova V, Jacome S, Tulsky JA, Lindvall C. Association of an advance care planning video and communication intervention with documentation of advance care planning among older adults: a nonrandomized controlled trial. JAMA Netw Open. 2022 Feb 01;5(2):e220354. doi: 10.1001/jamanetworkopen.2022.0354. https://europepmc.org/abstract/MED/35201306 .2789397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 168.Vongsachang H, Lagstein O, Boland MV, Repka MX, Kraus CL, Collins ME. Telemedicine utilization by pediatric ophthalmologists during the COVID-19 pandemic. J AAPOS. 2021 Oct;25(5):293–295.e1. doi: 10.1016/j.jaapos.2021.05.018. https://europepmc.org/abstract/MED/34600105 .S1091-8531(21)00540-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Webber EC, McMillen BD, Willis DR. Health care disparities and access to video visits before and after the COVID-19 pandemic: findings from a patient survey in primary care. Telemed J E Health. 2022 May;28(5):712–719. doi: 10.1089/tmj.2021.0126. [DOI] [PubMed] [Google Scholar]
- 170.White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med. 2011 Feb 20;30(4):377–99. doi: 10.1002/sim.4067. [DOI] [PubMed] [Google Scholar]
- 171.Wilson G, Windner Z, Bidwell S, Currie O, Dowell A, Halim AA, Toop L, Savage R, Ranaweera U, Beadel H, Hudson B. ‘Here to stay’: changes to prescribing medication in general practice during the COVID-19 pandemic in New Zealand. J. Prim. Health Care. 2021 Aug 13;13(3):222–230. doi: 10.1071/hc21035. [DOI] [PubMed] [Google Scholar]
- 172.Hoda R. Socio-technical grounded theory for software engineering. IIEEE Trans. Software Eng. 2022 Oct 1;48(10):3808–3832. doi: 10.1109/tse.2021.3106280. [DOI] [Google Scholar]
- 173.Chitungo I, Mhango M, Dzobo M, Denhere K, Chimene M, Musuka G, Dzinamarira T. Towards virtual doctor consultations: A call for the scale-up of telemedicine in sub-Saharan Africa during COVID-19 lockdowns and beyond. Smart Health (Amst) 2021 Jul;21:100207. doi: 10.1016/j.smhl.2021.100207. https://europepmc.org/abstract/MED/36570120 .S2352-6483(21)00029-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 174.Nittari G, Khuman R, Baldoni S, Pallotta G, Battineni G, Sirignano A, Amenta F, Ricci G. Telemedicine practice: review of the current ethical and legal challenges. Telemed J E Health. 2020 Dec;26(12):1427–1437. doi: 10.1089/tmj.2019.0158. https://europepmc.org/abstract/MED/32049608 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.de Oliveira Andrade A, Soares AB, de Andrade Palis A, Cabral AM, Barreto CGL, de Souza DB, de Paula Silva F, Santos FP, Silva GL, Guimarães JFV, de Araújo LAS, Nóbrega LR, Mendes LC, Luiz LMD, Brandão MR, Milagre ST, de Lima Gonçalves V, de Freitas Morales VH, da Conceição Lima V, Pereira AA. On the use of telemedicine in the context of COVID-19: legal aspects and a systematic review of technology. Res. Biomed. Eng. 2021 Mar 13;38(1):209–227. doi: 10.1007/s42600-021-00133-8. [DOI] [Google Scholar]
- 176.Ftouni R, AlJardali B, Hamdanieh M, Ftouni L, Salem N. Challenges of telemedicine during the COVID-19 pandemic: a systematic review. BMC Med Inform Decis Mak. 2022 Aug 03;22(1):207. doi: 10.1186/s12911-022-01952-0. https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-022-01952-0 .10.1186/s12911-022-01952-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Pogorzelska K, Chlabicz S. Patient satisfaction with telemedicine during the COVID-19 pandemic-a systematic review. Int J Environ Res Public Health. 2022 May 17;19(10):6113. doi: 10.3390/ijerph19106113. https://www.mdpi.com/resolver?pii=ijerph19106113 .ijerph19106113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 178.Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020 Dec 01;22(12):e24087. doi: 10.2196/24087. https://www.jmir.org/2020/12/e24087/ v22i12e24087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Silva A, Sindico S, Carneiro A, Henrique S, Fernandes A, Gomes J, Marinho T, Fernandes V. COVID-19 remote consultation services and population in health inequity-concentrating territories: a scoping review. Telemed J E Health. 2021 Aug;27(8):881–897. doi: 10.1089/tmj.2021.0145. https://europepmc.org/abstract/MED/34232749 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Boland J, Banks S, Krabbe R, Lawrence S, Murray T, Henning T, Vandenberg M. A COVID-19-era rapid review: using Zoom and Skype for qualitative group research. Public Health Res Pract. 2022 Jun 15;32(2):1. doi: 10.17061/phrp31232112. https://doi.org/10.17061/phrp31232112 .31232112 [DOI] [PubMed] [Google Scholar]
- 181.Andrews E, Berghofer K, Long J, Prescott A, Caboral-Stevens M. Satisfaction with the use of telehealth during COVID-19: An integrative review. Int J Nurs Stud Adv. 2020 Nov;2:100008. doi: 10.1016/j.ijnsa.2020.100008. https://linkinghub.elsevier.com/retrieve/pii/S2666-142X(20)30007-2 .S2666-142X(20)30007-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Beattie M, Lauder W, Atherton I, Murphy DJ. Instruments to measure patient experience of health care quality in hospitals: a systematic review protocol. Syst Rev. 2014 Jan 04;3(1):4. doi: 10.1186/2046-4053-3-4. https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/2046-4053-3-4 .2046-4053-3-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Shaver J. The state of telehealth before and after the COVID-19 pandemic. Prim Care. 2022 Dec;49(4):517–530. doi: 10.1016/j.pop.2022.04.002. https://europepmc.org/abstract/MED/36357058 .S0095-4543(22)00023-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Williams B, Coyle J, Healy D. The meaning of patient satisfaction: an explanation of high reported levels. Soc Sci Med. 1998 Nov;47(9):1351–9. doi: 10.1016/s0277-9536(98)00213-5.S0277953698002135 [DOI] [PubMed] [Google Scholar]
- 185.Williams S, Weinman J, Dale J. Doctor-patient communication and patient satisfaction: a review. Fam Pract. 1998 Oct;15(5):480–92. doi: 10.1093/fampra/15.5.480. [DOI] [PubMed] [Google Scholar]
- 186.Wolf JA, Niederhauser V, Marshburn D, LaVela SL. Defining patient experience. Patient Experience Journal. 2014;1(1):7–19. doi: 10.35680/2372-0247.1004. [DOI] [Google Scholar]
- 187.Garcia R, Adelakun O. A conceptual framework and pilot study for examining telemedicine satisfaction research. J Med Syst. 2019 Jan 25;43(3):51. doi: 10.1007/s10916-019-1161-4.10.1007/s10916-019-1161-4 [DOI] [PubMed] [Google Scholar]
- 188.Wang T, Giunti G, Melles M, Goossens R. Digital patient experience: umbrella systematic review. J Med Internet Res. 2022 Aug 04;24(8):e37952. doi: 10.2196/37952. https://www.jmir.org/2022/8/e37952/ v24i8e37952 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 189.Greenhalgh T, Ladds E, Hughes G, Moore L, Wherton J, Shaw SE, Papoutsi C, Wieringa S, Rosen R, Rushforth A, Rybczynska-Bunt S. Why do GPs rarely do video consultations? qualitative study in UK general practice. Br J Gen Pract. 2022 Feb 16;72(718):e351–e360. doi: 10.3399/bjgp.2021.0658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 190.Mohtar LN, Badr NG. Digital Bridge or Tradeoff: Telehealth Adoption and Healthcare Service Quality. A Scoping Review. In: Za S, Winter R, Lazazzara A, editors. Sustainable Digital Transformation. Lecture Notes in Information Systems and Organisation, vol 59. Cham, Switzerland: Springer International Publishing; 2023. pp. 253–268. [Google Scholar]
- 191.Lauffenburger JC, Khatib R, Siddiqi A, Albert MA, Keller PA, Samal L, Glowacki N, Everett ME, Hanken K, Lee SG, Bhatkhande G, Haff N, Sears ES, Choudhry NK. Reducing ethnic and racial disparities by improving undertreatment, control, and engagement in blood pressure management with health information technology (REDUCE-BP) hybrid effectiveness-implementation pragmatic trial: Rationale and design. Am Heart J. 2023 Jan;255:12–21. doi: 10.1016/j.ahj.2022.10.003. https://europepmc.org/abstract/MED/36220355 .S0002-8703(22)00197-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Jaworski BK, Webb Hooper M, Aklin WM, Jean-Francois B, Elwood WN, Belis D, Riley WT, Hunter CM. Advancing digital health equity: Directions for behavioral and social science research. Transl Behav Med. 2023 Apr 03;13(3):132–139. doi: 10.1093/tbm/ibac088. https://europepmc.org/abstract/MED/36318232 .6786016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Kelly M, Fullen B, Martin D, Bradley C, O'Mahony B, McVeigh J. Design and development of an eHealth intervention to support self-management in people with musculoskeletal disorders - ‘eHealth: It’s TIME’: a study protocol. HRB Open Res. 2022 Nov 14;5:73. doi: 10.12688/hrbopenres.13611.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Caillaud C, Lazarevic N, Pizzuti C, Rosic G, Boehm C, Williams K. Digital Health as a silver lining: exploring pregnancy digital health usage amidst the COVID-19 pandemic. Digitial Health Week. 2023 Dec 19;2(1):1. doi: 10.21203/rs.3.rs-2115070/v1. https://openjournals.library.sydney.edu.au/DHW/article/view/17935 . [DOI] [Google Scholar]
- 195.Richardson S, Lawrence K, Schoenthaler AM, Mann D. A framework for digital health equity. NPJ Digit Med. 2022 Aug 18;5(1):119. doi: 10.1038/s41746-022-00663-0. https://doi.org/10.1038/s41746-022-00663-0 .10.1038/s41746-022-00663-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196.Ragnedda M, Ruiu ML, Addeo F. The self-reinforcing effect of digital and social exclusion: The inequality loop. Telematics and Informatics. 2022 Aug;72:101852. doi: 10.1016/j.tele.2022.101852. [DOI] [Google Scholar]
- 197.James HM, Papoutsi C, Wherton J, Greenhalgh T, Shaw SE. Spread, scale-up, and sustainability of video consulting in health care: systematic review and synthesis guided by the NASSS framework. J Med Internet Res. 2021 Jan 26;23(1):e23775. doi: 10.2196/23775. https://www.jmir.org/2021/1/e23775/ v23i1e23775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Walpole SC. Including papers in languages other than English in systematic reviews: important, feasible, yet often omitted. J Clin Epidemiol. 2019 Jul;111:127–134. doi: 10.1016/j.jclinepi.2019.03.004.S0895-4356(18)30960-0 [DOI] [PubMed] [Google Scholar]
- 199.Peters M, Marnie C, Tricco A, Pollock D, Munn Z, Alexander L. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020:18–26. doi: 10.11124/jbies-20-00167. [DOI] [PubMed] [Google Scholar]
- 200.Valdes D. Global evidence on the rapid adoption of telemedicine in primary care in the COVID-19 pandemic. OSF. 2023. Jan 02, [2024-11-06]. https://osf.io/4z5ut/ [DOI] [PMC free article] [PubMed]
- 201.Chambers DA, Glasgow RE, Stange KC. The dynamic sustainability framework: addressing the paradox of sustainment amid ongoing change. Implement Sci. 2013 Oct 02;8(1):117. doi: 10.1186/1748-5908-8-117. https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-8-117 .1748-5908-8-117 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Deviations from the protocol.
Example searches.
Abstracts-extracts used in the study.
Data collection template.
Summary characteristics of the included studies.
PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) Checklist.