

Abstract
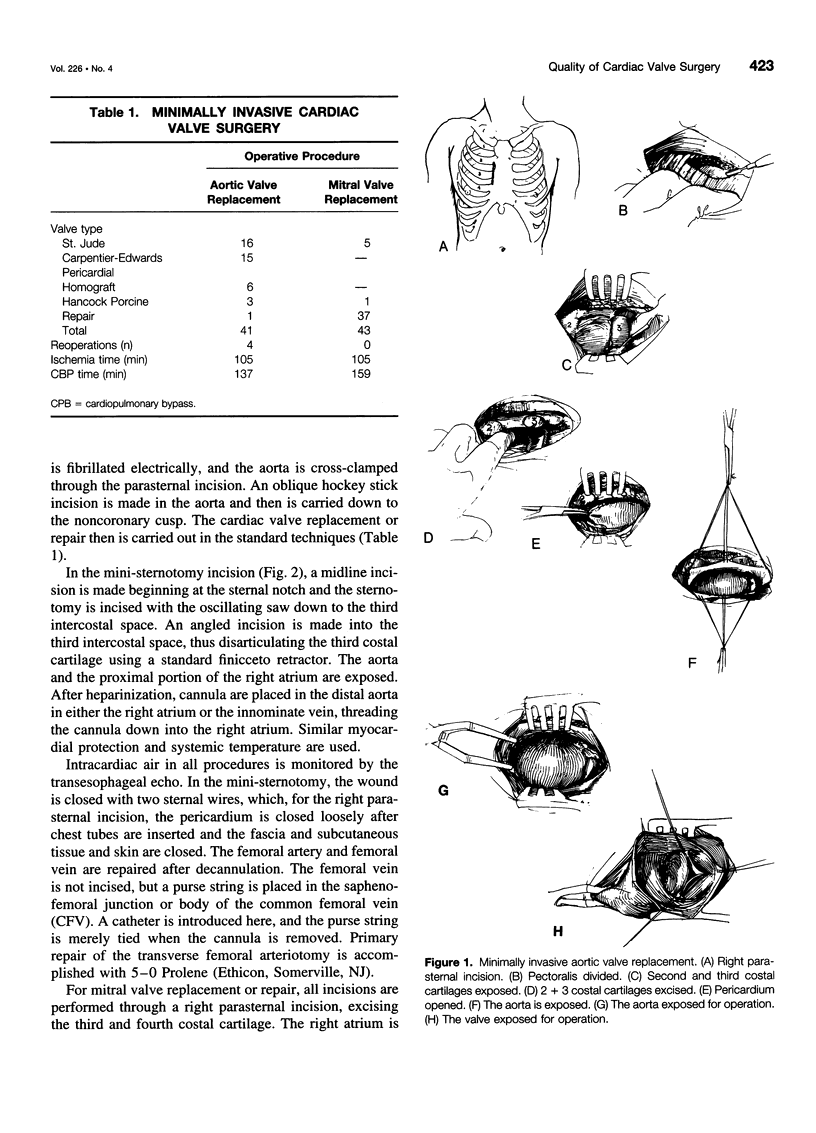
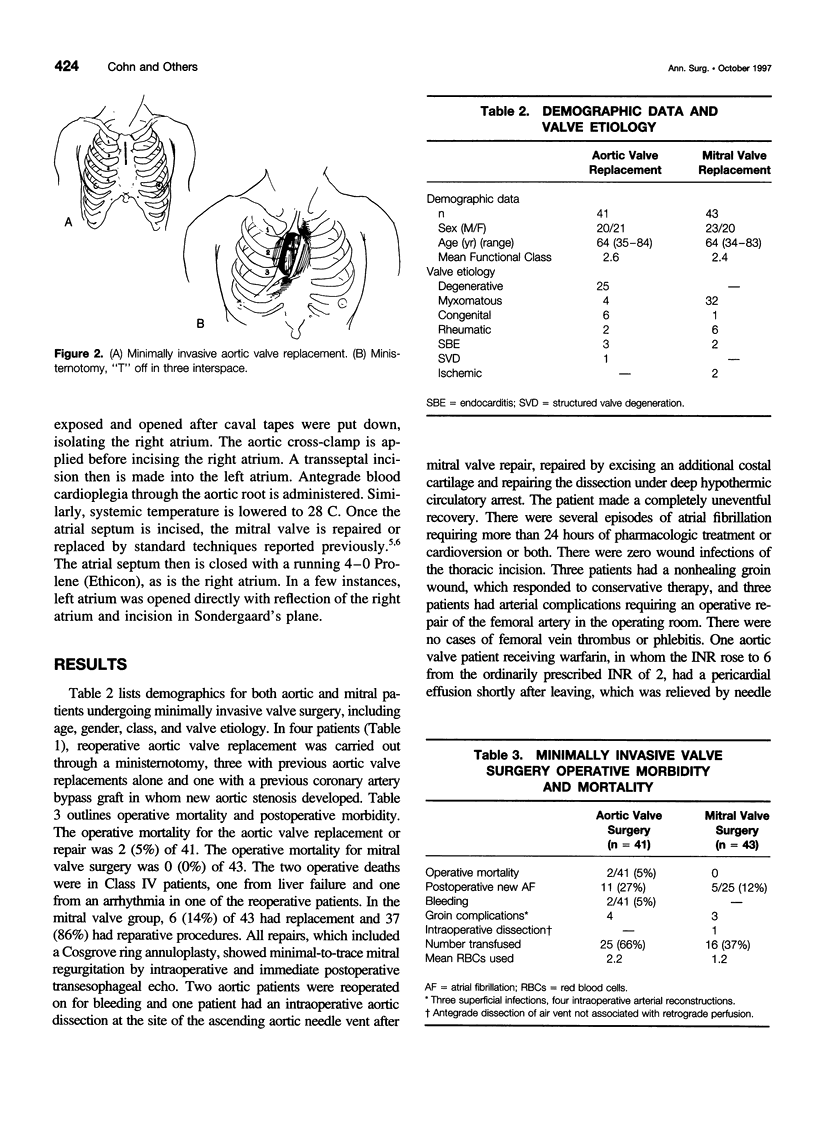
OBJECTIVE: This study compares the quality of valve replacement and repair performed through minimally invasive incisions as compared to the standard operation for aortic and mitral valve replacement. SUMMARY BACKGROUND DATA: With the advent of minimally invasive laparoscopic approaches to orthopedic surgery, urology, general surgery, and thoracic surgery, it now is apparent that standard cardiac valve operations can be performed through very small incisions with similar approaches. METHODS: Eighty-four patients underwent minimally invasive aortic (n = 41) and minimally invasive mitral valve repair and replacement (n = 43) between July 1996 and April 1997. Demographics, procedures, operative techniques, and postoperative morbidity and mortality were calculated, and a subset of the first 50 patients was compared to a 50-patient cohort who underwent the same operation through a conventional median sternotomy. Demographics, postoperative morbidity and mortality, patient satisfaction, and charges were compared. RESULTS: Of the 84 patients, there were 2 operative mortalities both in class IV aortic patients from multisystem organ failure. There was no operative mortality in the patients undergoing mitral valve replacement or repair. The operations were carried out with the same accuracy and attention to detail as with the conventional operation. There was minimal postoperative bleeding, cerebral vascular accidents, or other major morbidity. Groin cannulation complications primarily were related to atherosclerotic femoral arteries. A comparison of the minimally invasive to the conventional group, although operative time and ischemia time was higher in minimally invasive group, the requirement for erythrocytes was significantly less, patient satisfaction was significantly greater, and charges were approximately 20% less than those in the conventional group. CONCLUSIONS: Minimally invasive aortic and mitral valve surgery in patients without coronary disease can be done safely and accurately through small incisions. Patient satisfaction is up, return to normality is higher, and requirement for postrehabilitation services is less. In addition, the charges are approximately 20% less. These results serve as a paradigm for the future in terms of valve surgery in the managed care environment.
Full text
PDF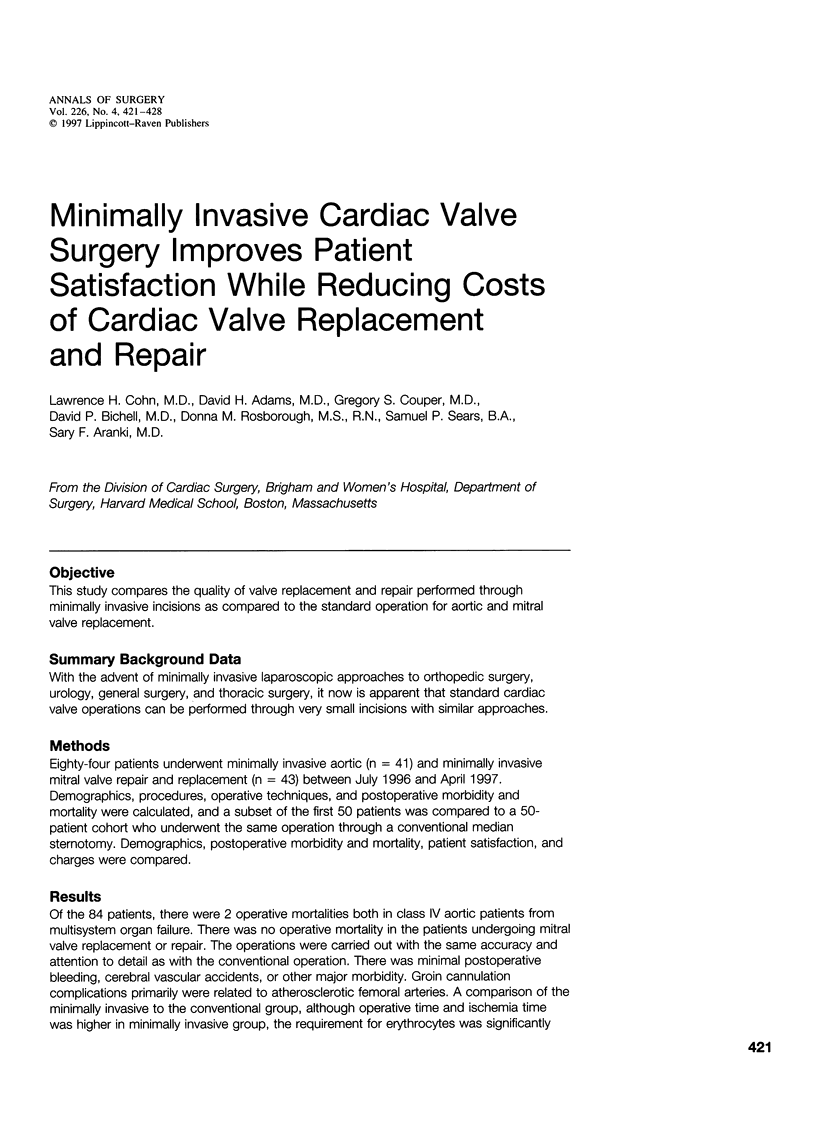

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bichell D. P., Adams D. H., Aranki S. F., Rizzo R. J., Cohn L. H. Repair of mitral regurgitation from myxomatous degeneration in the patient with a severely calcified posterior annulus. J Card Surg. 1995 Jul;10(4 Pt 1):281–284. doi: 10.1111/j.1540-8191.1995.tb00611.x. [DOI] [PubMed] [Google Scholar]
- Cohn L. H. Elliot Carr Cutler mitral valve surgery at Peter Bent Brigham Hospital 1923. J Card Surg. 1994 Mar;9(2 Suppl):137–138. doi: 10.1111/j.1540-8191.1994.tb00912.x. [DOI] [PubMed] [Google Scholar]
- Cohn L. H., Kowalker W., Bhatia S., DiSesa V. J., St John-Sutton M., Shemin R. J., Collins J. J. Comparative morbidity of mitral valve repair versus replacement for mitral regurgitation with and without coronary artery disease. 1988. Updated in 1995. Ann Thorac Surg. 1995 Nov;60(5):1452–1453. doi: 10.1016/0003-4975(95)00379-y. [DOI] [PubMed] [Google Scholar]
- Cohn L. H. The cost of treating heart valve related complications. J Heart Valve Dis. 1996 Mar;5(2):120–121. [PubMed] [Google Scholar]
- Cosgrove D. M., 3rd, Sabik J. F. Minimally invasive approach for aortic valve operations. Ann Thorac Surg. 1996 Aug;62(2):596–597. [PubMed] [Google Scholar]
- Falk V., Walther T., Diegeler A., Wendler R., Autschbach R., van Son J. A., Siegel L. C., Pompilli M. F., Mohr F. W. Echocardiographic monitoring of minimally invasive mitral valve surgery using an endoaortic clamp. J Heart Valve Dis. 1996 Nov;5(6):630–637. [PubMed] [Google Scholar]