

Abstract
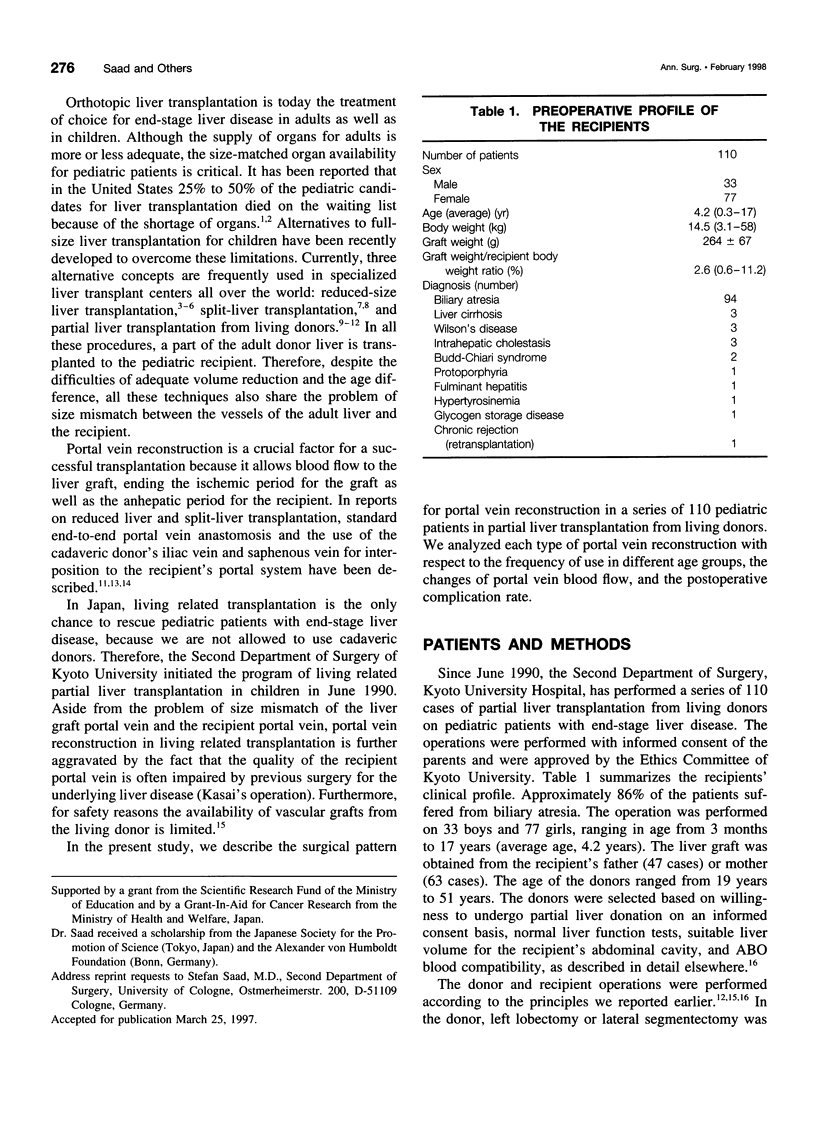
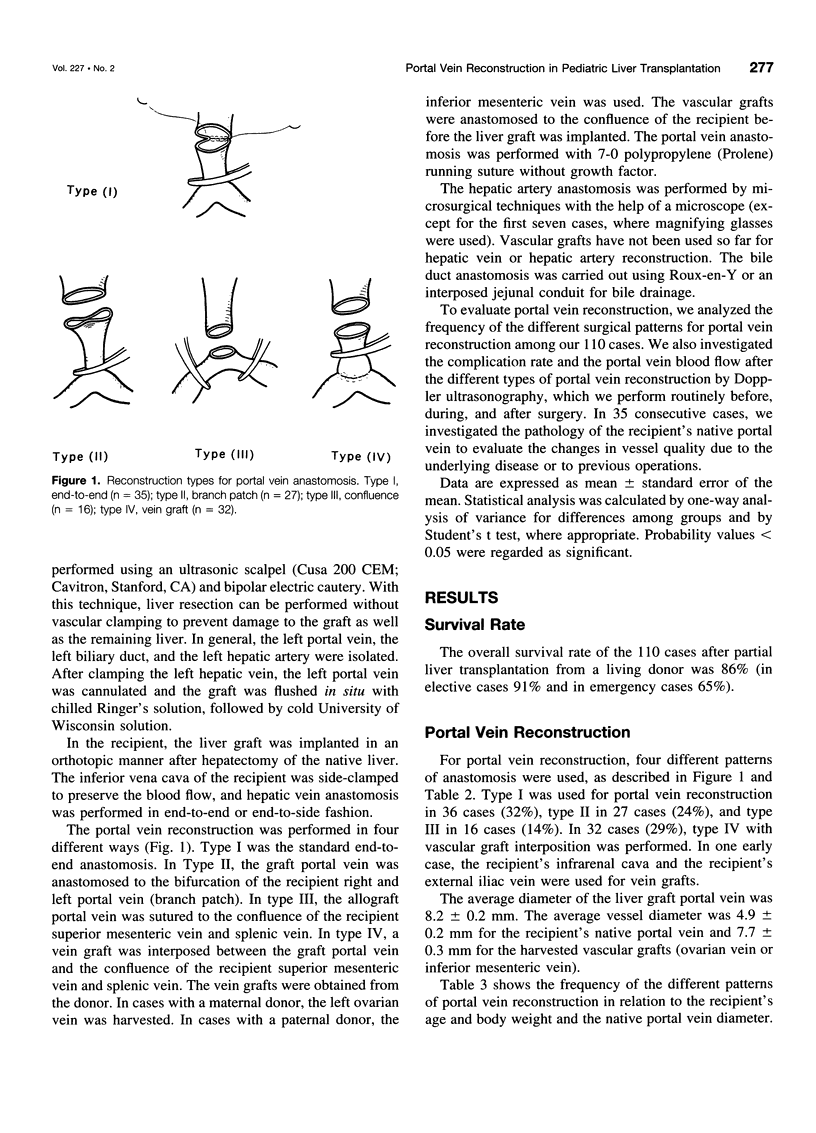
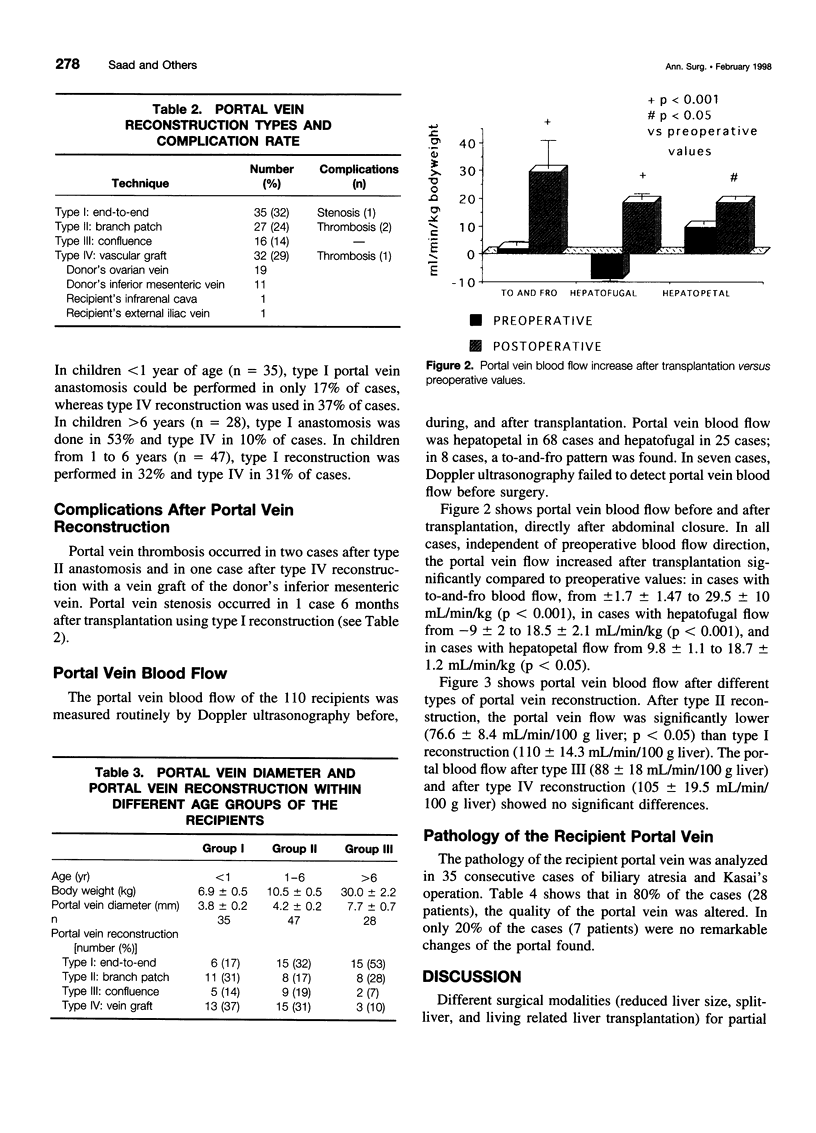
OBJECTIVE: The authors analyze the surgical pattern and the underlying rationale for the use of different types of portal vein reconstruction in 110 pediatric patients who underwent partial liver transplantation from living parental donors. SUMMARY BACKGROUND DATA: In partial liver transplantation, standard end-to-end portal vein anastomosis is often difficult because of either size mismatch between the graft and the recipient portal vein or impaired vein quality of the recipient. Alternative surgical anastomosis techniques are necessary. METHODS: In 110 patients age 3 months to 17 years, four different types of portal vein reconstruction were performed. The portal vein of the liver graft was anastomosed end to end (type I); to the branch patch of the left and right portal vein of the recipient (type II); to the confluence of the recipient superior mesenteric vein and the splenic vein (type III); and to a vein graft interposed between the confluence and the liver graft (type IV). Reconstruction patterns were evaluated by their frequency of use among different age groups of recipients, postoperative portal vein blood flow, and postoperative complication rate. RESULTS: The portal vein of the liver graft was anastomosed by reconstruction type I in 32%, II in 24%, III in 14%, and IV 29% of the cases. In children <1 year of age, type I could be performed in only 17% of the cases, whereas 37% received type IV reconstruction. Postoperative Doppler ultrasound (mL/min/100 g liver) showed significantly (p < 0.05) lower portal blood flow after type II (76.6 +/- 8.4) versus type I (110 +/- 14.3), type III (88 +/- 18), and type IV (105 +/- 19.5). Portal vein thrombosis occurred in two cases after type II and in one case after type IV anastomosis. Portal stenosis was encountered in one case after type I reconstruction. Pathologic changes of the recipient native portal vein were found in 27 of 35 investigated cases. CONCLUSION: In living related partial liver transplantation, portal vein anastomosis to the confluence with or without the use of vein grafts is the optimal alternative to end-to-end reconstruction, especially in small children.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bismuth H., Houssin D. Reduced-sized orthotopic liver graft in hepatic transplantation in children. Surgery. 1984 Mar;95(3):367–370. [PubMed] [Google Scholar]
- Broelsch C. E., Emond J. C., Thistlethwaite J. R., Rouch D. A., Whitington P. F., Lichtor J. L. Liver transplantation with reduced-size donor organs. Transplantation. 1988 Mar;45(3):519–524. doi: 10.1097/00007890-198803000-00003. [DOI] [PubMed] [Google Scholar]
- Broelsch C. E., Emond J. C., Whitington P. F., Thistlethwaite J. R., Baker A. L., Lichtor J. L. Application of reduced-size liver transplants as split grafts, auxiliary orthotopic grafts, and living related segmental transplants. Ann Surg. 1990 Sep;212(3):368–377. doi: 10.1097/00000658-199009000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broelsch C. E., Whitington P. F., Emond J. C., Heffron T. G., Thistlethwaite J. R., Stevens L., Piper J., Whitington S. H., Lichtor J. L. Liver transplantation in children from living related donors. Surgical techniques and results. Ann Surg. 1991 Oct;214(4):428–439. doi: 10.1097/00000658-199110000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emond J. C., Whitington P. F., Thistlethwaite J. R., Cherqui D., Alonso E. A., Woodle I. S., Vogelbach P., Busse-Henry S. M., Zucker A. R., Broelsch C. E. Transplantation of two patients with one liver. Analysis of a preliminary experience with 'split-liver' grafting. Ann Surg. 1990 Jul;212(1):14–22. doi: 10.1097/00000658-199007000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Esquivel C. O., Nakazato P., Cox K., Concepcion W., Berquist W., Russell T. R. The impact of liver reductions in pediatric liver transplantation. Arch Surg. 1991 Oct;126(10):1278–1286. doi: 10.1001/archsurg.1991.01410340120017. [DOI] [PubMed] [Google Scholar]
- Houssin D., Soubrane O., Boillot O., Dousset B., Ozier Y., Devictor D., Bernard O., Chapuis Y. Orthotopic liver transplantation with a reduced-size graft: an ideal compromise in pediatrics? Surgery. 1992 May;111(5):532–542. [PubMed] [Google Scholar]
- Kalayoglu M., D'Alessandro A. M., Sollinger H. W., Hoffman R. M., Pirsch J. D., Belzer F. O. Experience with reduced-size liver transplantation. Surg Gynecol Obstet. 1990 Aug;171(2):139–147. [PubMed] [Google Scholar]
- Lerut J., Tzakis A. G., Bron K., Gordon R. D., Iwatsuki S., Esquivel C. O., Makowka L., Todo S., Starzl T. E. Complications of venous reconstruction in human orthotopic liver transplantation. Ann Surg. 1987 Apr;205(4):404–414. doi: 10.1097/00000658-198704000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Otte J. B., de Ville de Goyet J., Sokal E., Alberti D., Moulin D., de Hemptinne B., Veyckemans F., van Obbergh L., Carlier M., Clapuyt P. Size reduction of the donor liver is a safe way to alleviate the shortage of size-matched organs in pediatric liver transplantation. Ann Surg. 1990 Feb;211(2):146–157. doi: 10.1097/00000658-199002000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pichlmayr R., Ringe B., Gubernatis G., Hauss J., Bunzendahl H. Transplantation einer Spenderleber auf zwei Empfänger (Splitting-Transplantation)--Eine neue Methode in der Weiterentwicklung der Lebersegmenttransplantation. Langenbecks Arch Chir. 1988;373(2):127–130. [PubMed] [Google Scholar]
- Raia S., Nery J. R., Mies S. Liver transplantation from live donors. Lancet. 1989 Aug 26;2(8661):497–497. doi: 10.1016/s0140-6736(89)92101-6. [DOI] [PubMed] [Google Scholar]
- Shaw B. W., Jr, Iwatsuki S., Bron K., Starzl T. E. Portal vein grafts in hepatic transplantation. Surg Gynecol Obstet. 1985 Jul;161(1):66–68. [PMC free article] [PubMed] [Google Scholar]
- Smith B. Segmental liver transplantation from a living donor. J Pediatr Surg. 1969 Feb;4(1):126–132. doi: 10.1016/0022-3468(69)90193-6. [DOI] [PubMed] [Google Scholar]
- Strong R., Ong T. H., Pillay P., Wall D., Balderson G., Lynch S. A new method of segmental orthotopic liver transplantation in children. Surgery. 1988 Jul;104(1):104–107. [PubMed] [Google Scholar]
- Tanaka K., Uemoto S., Tokunaga Y., Fujita S., Sano K., Nishizawa T., Sawada H., Shirahase I., Kim H. J., Yamaoka Y. Surgical techniques and innovations in living related liver transplantation. Ann Surg. 1993 Jan;217(1):82–91. doi: 10.1097/00000658-199301000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamaoka Y., Ozawa K., Tanaka A., Mori K., Morimoto T., Shimahara Y., Zaima M., Tanaka K., Kumada K. New devices for harvesting a hepatic graft from a living donor. Transplantation. 1991 Jul;52(1):157–160. doi: 10.1097/00007890-199107000-00035. [DOI] [PubMed] [Google Scholar]
- de Hemptinne B., Salizzoni M., Tan K. C., Otte J. B. The technique of liver size reduction in orthotopic liver transplantation. Transplant Proc. 1988 Feb;20(1 Suppl 1):508–511. [PubMed] [Google Scholar]