

Abstract
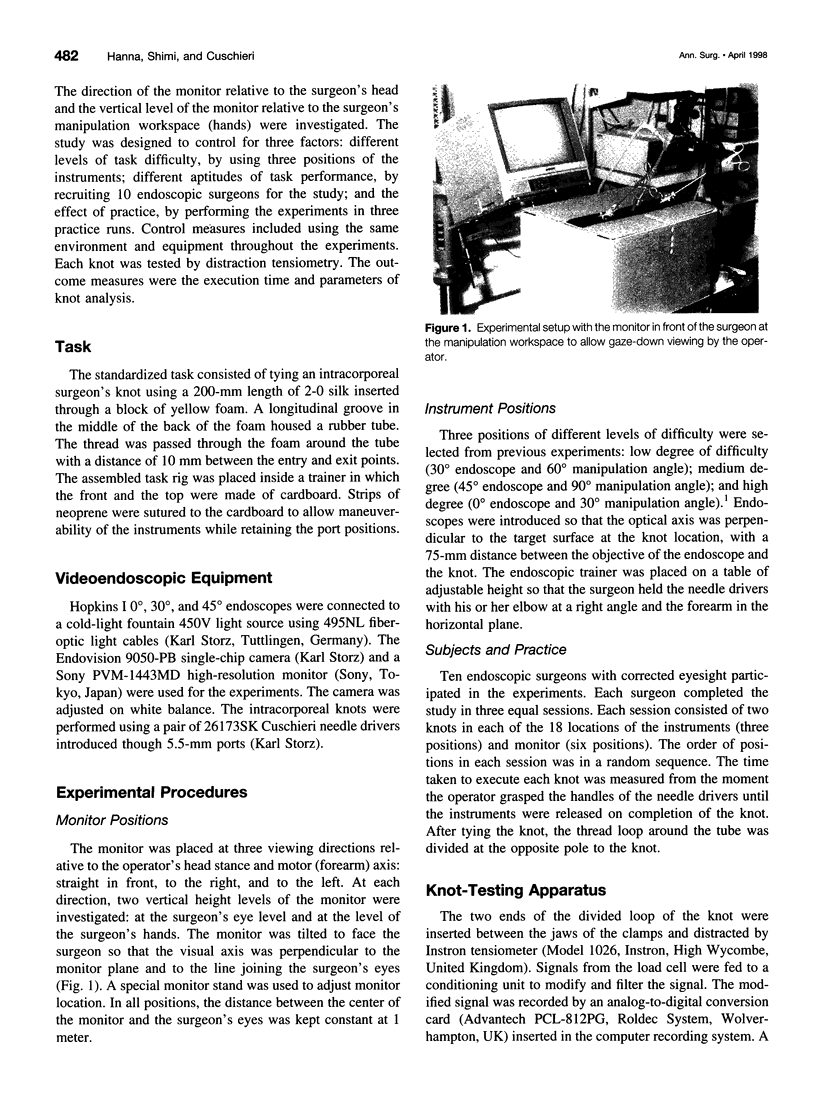
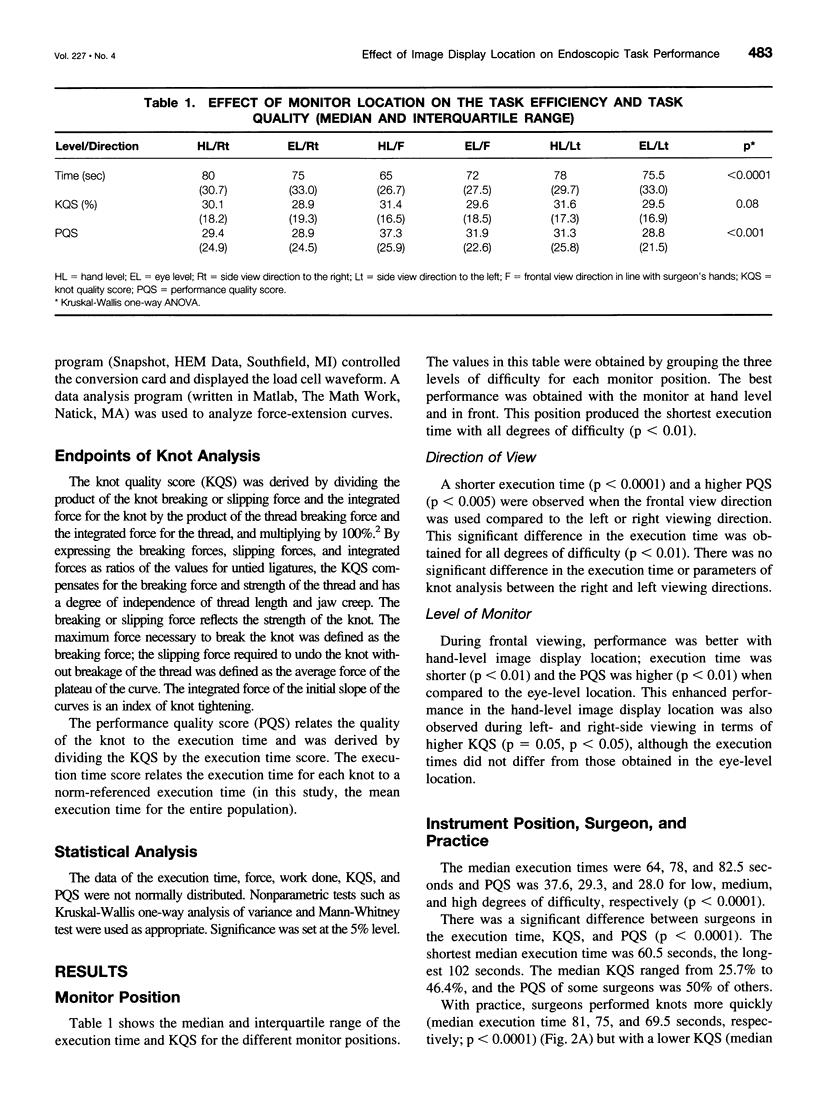
OBJECTIVE: To investigate the influence of image display location on endoscopic task performance in endoscopic surgery. SUMMARY BACKGROUND DATA: The image display system is the only visual interface between the surgeon or interventionist and the operative field. Several factors influence the correct perceptual processing and endoscopic manipulation from images. One of these is location of the image display with respect to the surgeon and to the operative site. The present study was conducted to investigate whether endoscopic task performance improves under two conditions: when the surgeon-to-monitor visual axis is aligned with the forearm-instrument motor axis and when the image display is close to the operator's manipulation workspace. METHODS: An endoscopic task (tying an intracorporeal surgeon's knot) was performed under standardized conditions except for varying monitor locations. These altered the direction of view--in front of, to the left, and to the right of the operator's head and hands. In each of these view directions, the monitor was placed at the surgeon's eye level and lower down, at the level of the operator's hands. The outcome measures were the execution time, knot quality score and performance quality score. RESULTS: Task performance was better with frontal view direction: execution time was shorter (p < 0.0001) and the performance score was higher (p < 0.005) than with side viewing, with no significant difference between right and left viewing directions. With frontal view direction, hand-level "gaze-down" viewing resulted in a shorter execution time (p < 0.01) and a higher performance score (p < 0.01) than eye-level viewing. CONCLUSIONS: Task performance improves when the image display is placed in front of the operator, at a level below the head and close to the hands.
Full text
PDF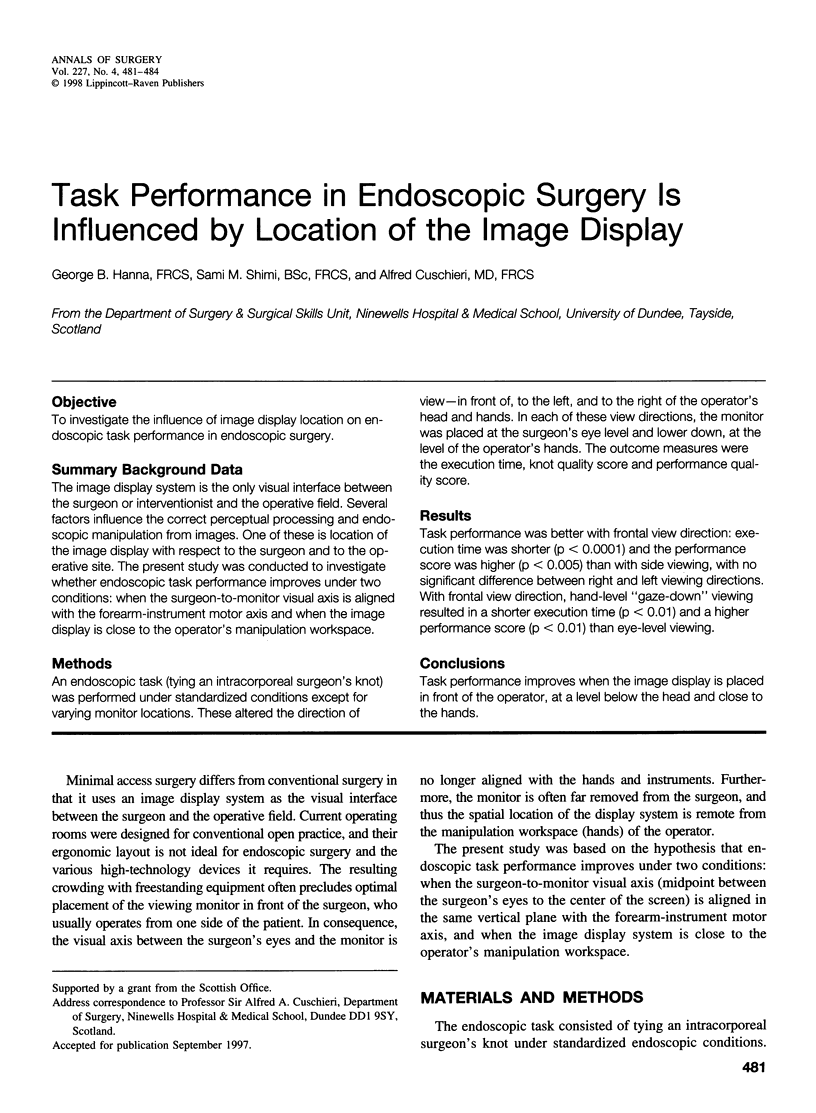
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cuschieri A. Visual Displays and Visual Perception in Minimal Access Surgery. Semin Laparosc Surg. 1995 Sep;2(3):209–214. doi: 10.1053/SLAS00200209. [DOI] [PubMed] [Google Scholar]
- Hanna G. B., Frank T. G., Cuschieri A. Objective assessment of endoscopic knot quality. Am J Surg. 1997 Oct;174(4):410–413. doi: 10.1016/s0002-9610(97)00129-3. [DOI] [PubMed] [Google Scholar]
- Hanna G. B., Shimi S., Cuschieri A. Influence of direction of view, target-to-endoscope distance and manipulation angle on endoscopic knot tying. Br J Surg. 1997 Oct;84(10):1460–1464. [PubMed] [Google Scholar]
- Quaranta Leoni F. M., Molle F., Scavino G., Dickmann A. Identification of the preferential gaze position through elevation of visual fatigue in a selected group of VDU operators. A preliminary study. Doc Ophthalmol. 1994;87(2):189–197. doi: 10.1007/BF01204797. [DOI] [PubMed] [Google Scholar]