

Abstract
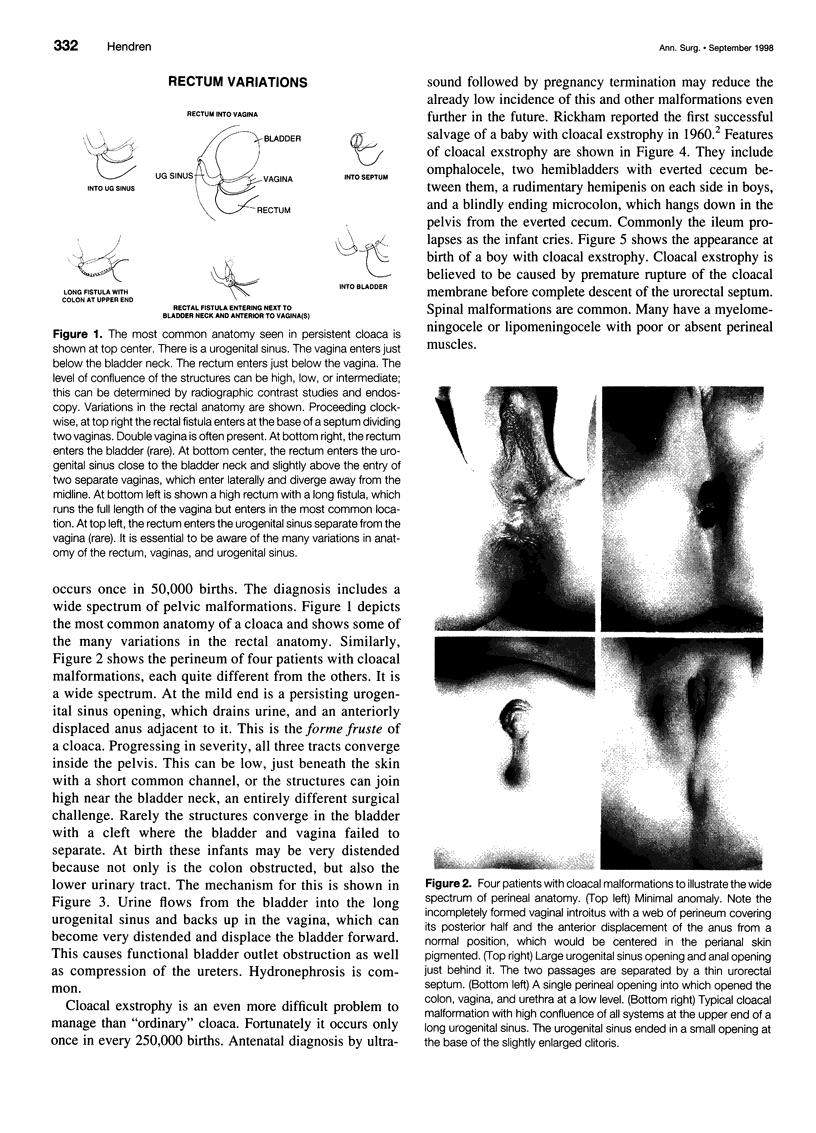
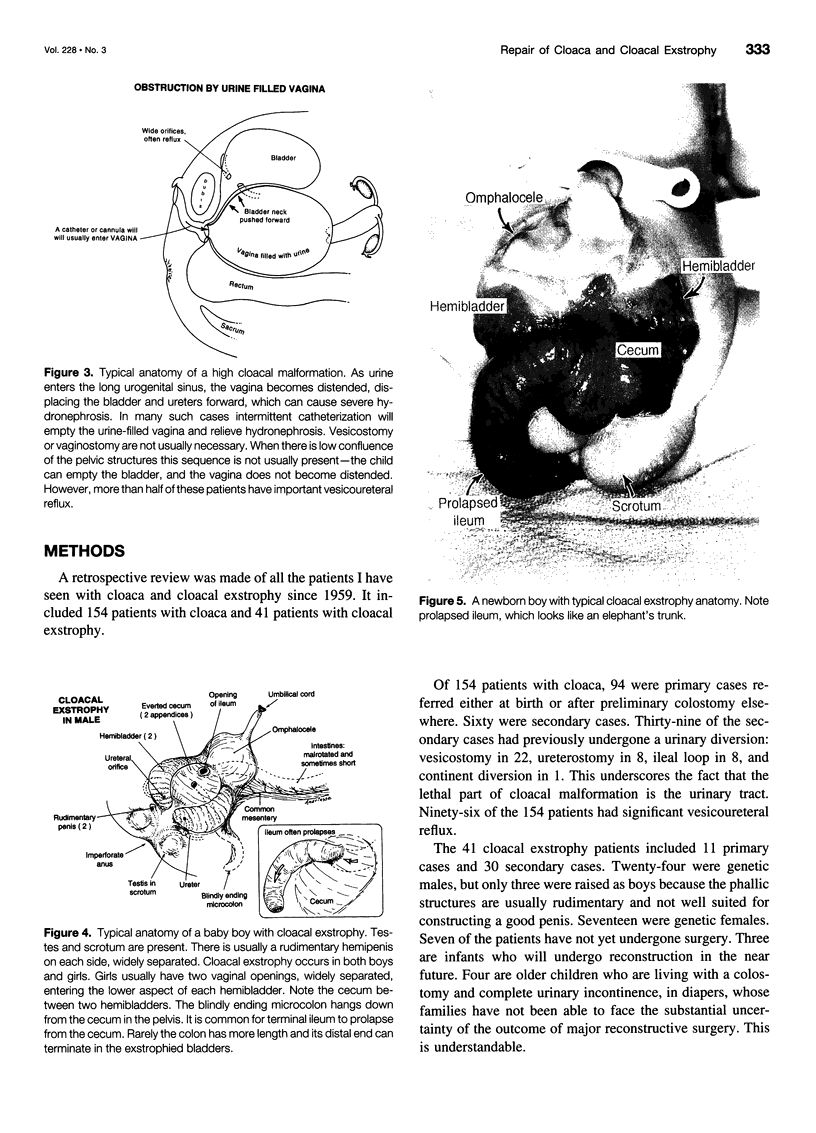
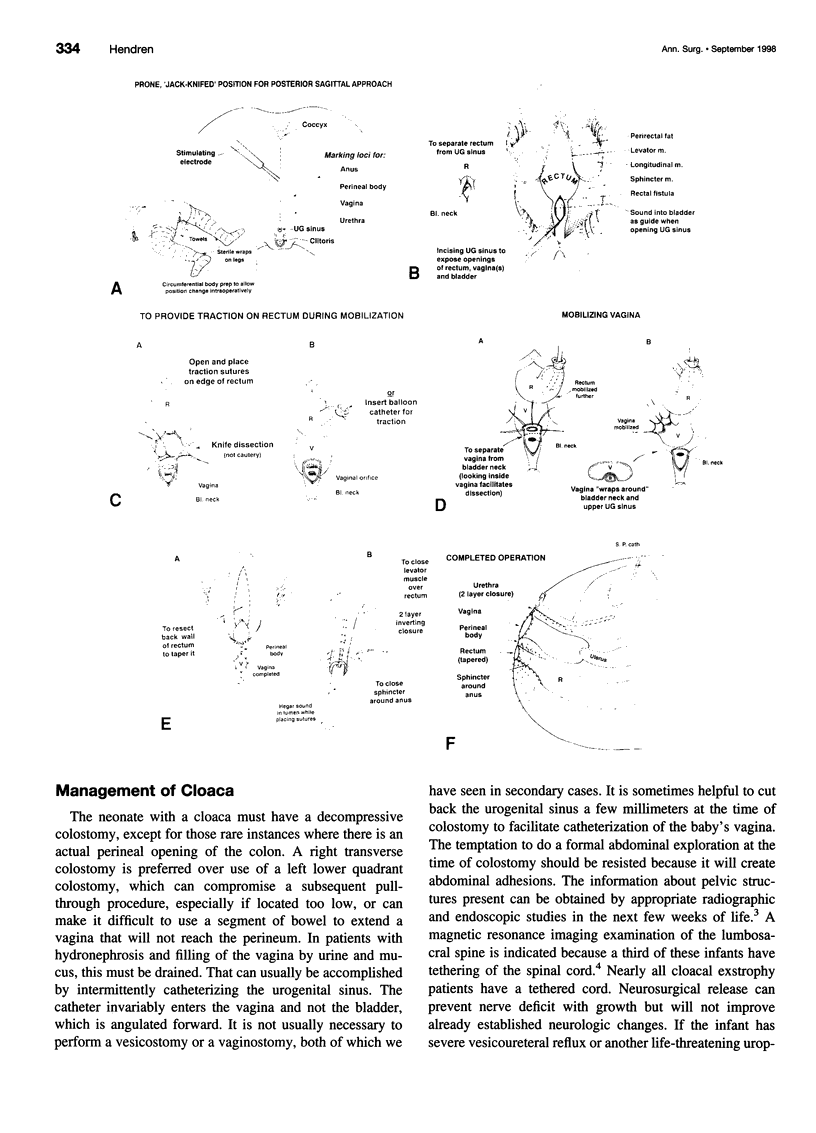
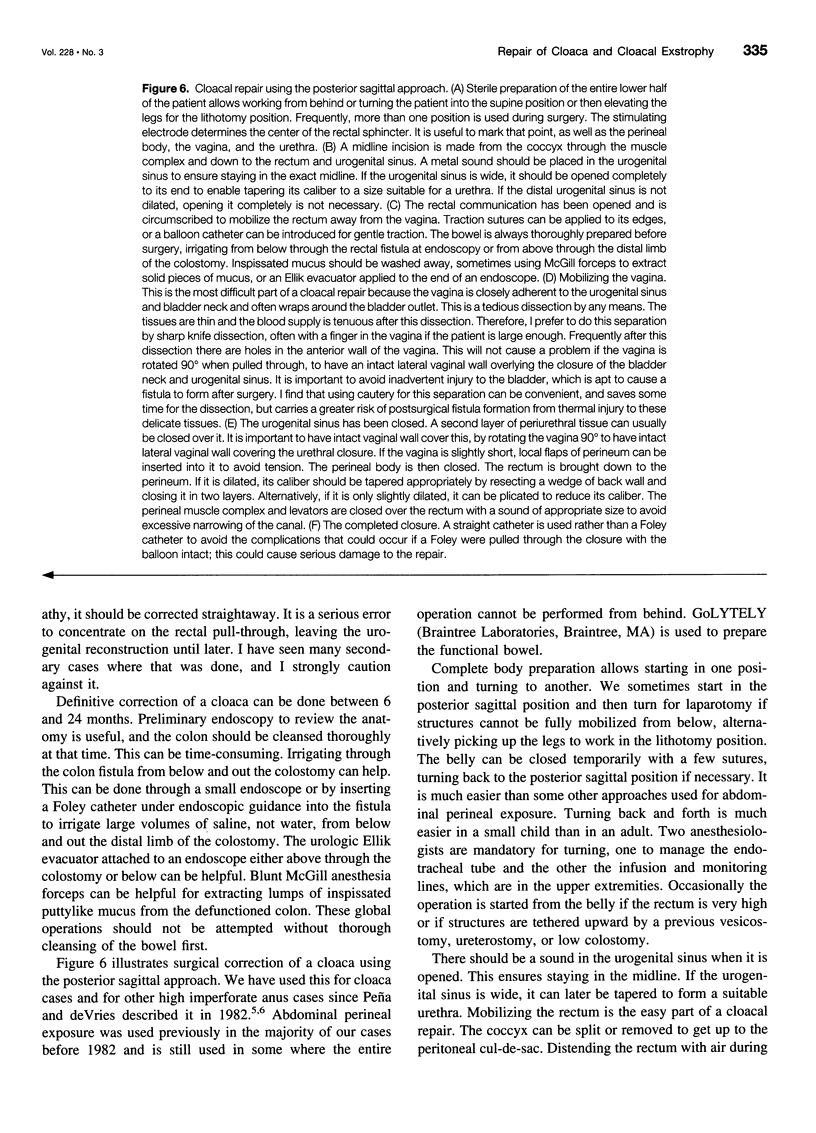
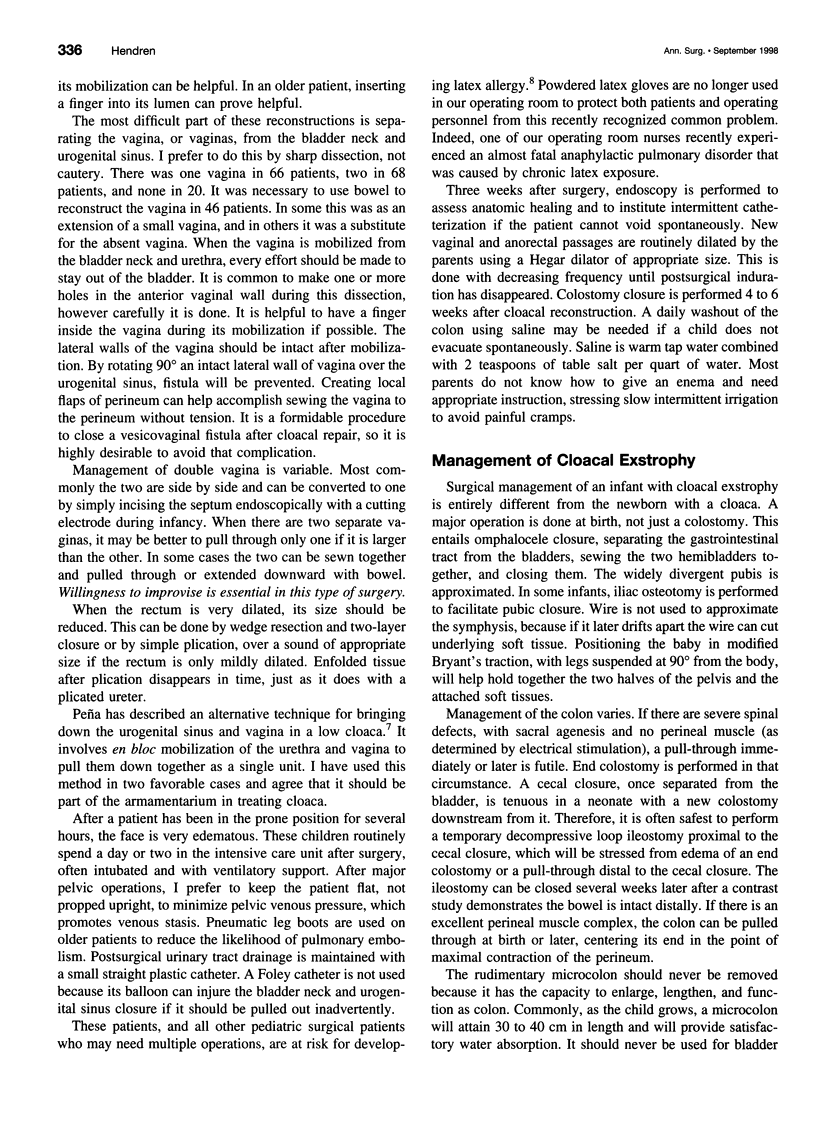
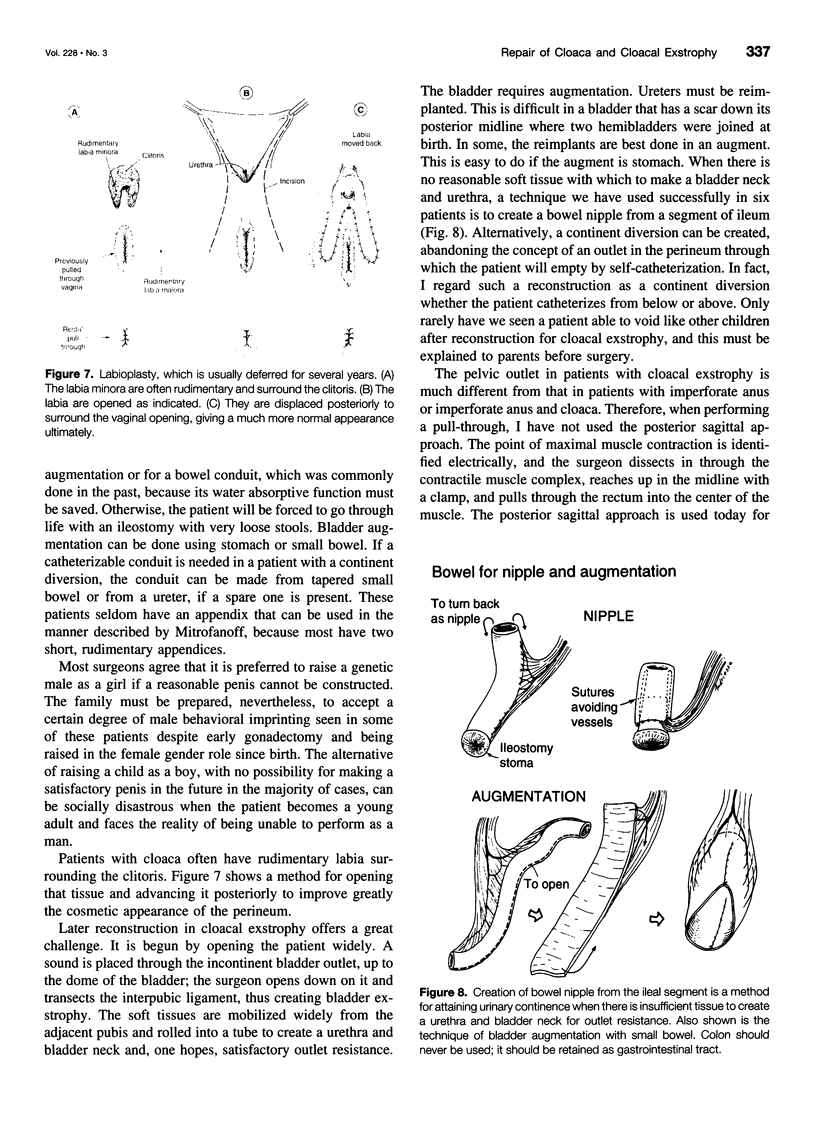
OBJECTIVE: To provide a follow-up of 195 patients with cloacal malformations seen by the author from 1959 to 1998. SUMMARY BACKGROUND DATA: Cloaca, which occurs in approximately 1 of 50,000 births, is the most complex type of imperforate anus with confluence of the rectum, vagina, and bladder in a urogenital sinus. Functional results for the bowel, the genital tract, and the urinary tract were formerly poor. Cloacal exstrophy, which is an even more complex spectrum of malformations, was uniformly fatal until 1960. In addition to imperforate anus, these babies have an omphalocele, two exstrophic bladders, between which there is an open cecum, and a blindly ending colon hanging down in the pelvis from the cecum. Although both of these diagnoses contain the word "cloaca," which is Latin for sewer, they are really two separate entities in terms of surgical management. Cloaca and cloacal exstrophy in most cases are very different anatomic problems. However, there are variants that are like a hybrid, which is the rationale for reporting together an experience with both entities. METHODS: Records were reviewed of 154 patients with cloaca and 41 patients with cloacal exstrophy to assess anorectal function, urinary continence, and sexual function where available. RESULTS: Follow-up was available in 141 cloaca patients: 82 have spontaneous bowel movements and satisfactory control, 38 use enemas to evacuate, 9 have a colostomy, 7 have fecal soiling, and 5 are too recently operated to evaluate. Regarding urinary control, 83 void spontaneously, 40 catheterize to empty, 4 have urinary diversion, 1 has a continent diversion, 5 patients are wet, and 8 are too recently operated to judge. Twenty-four patients are now adults, 17 of who have experienced coitus and 7 have not. Seven have had babies, all except one by cesarean section. Results of surgery for cloacal exstrophy are not as good, but are encouraging nonetheless for an anomaly that was uniformly fatal before 1960. Of the 41 cloacal exstrophy patients being followed, 7 have not undergone surgery. Fifteen have a colostomy; 19 had pull-through of the colon, but 3 were subsequently reversed for fecal incontinence. Most depend on enemas to evacuate. Urinary dryness was attained in 30 patients, usually by intermittent catheterization of the bladder, which was augmented with small bowel or stomach or both. Only three void voluntarily. Fifteen of the completed long-term patients wear no bag. Only three of the completed patients wear two bags. The rest have one bag. CONCLUSIONS: Imperforate anus and associated malformations in cloaca and cloacal exstrophy are not hopeless problems. A reasonable lifestyle can be achieved for most of these children with comprehensive surgical planning.
Full text
PDF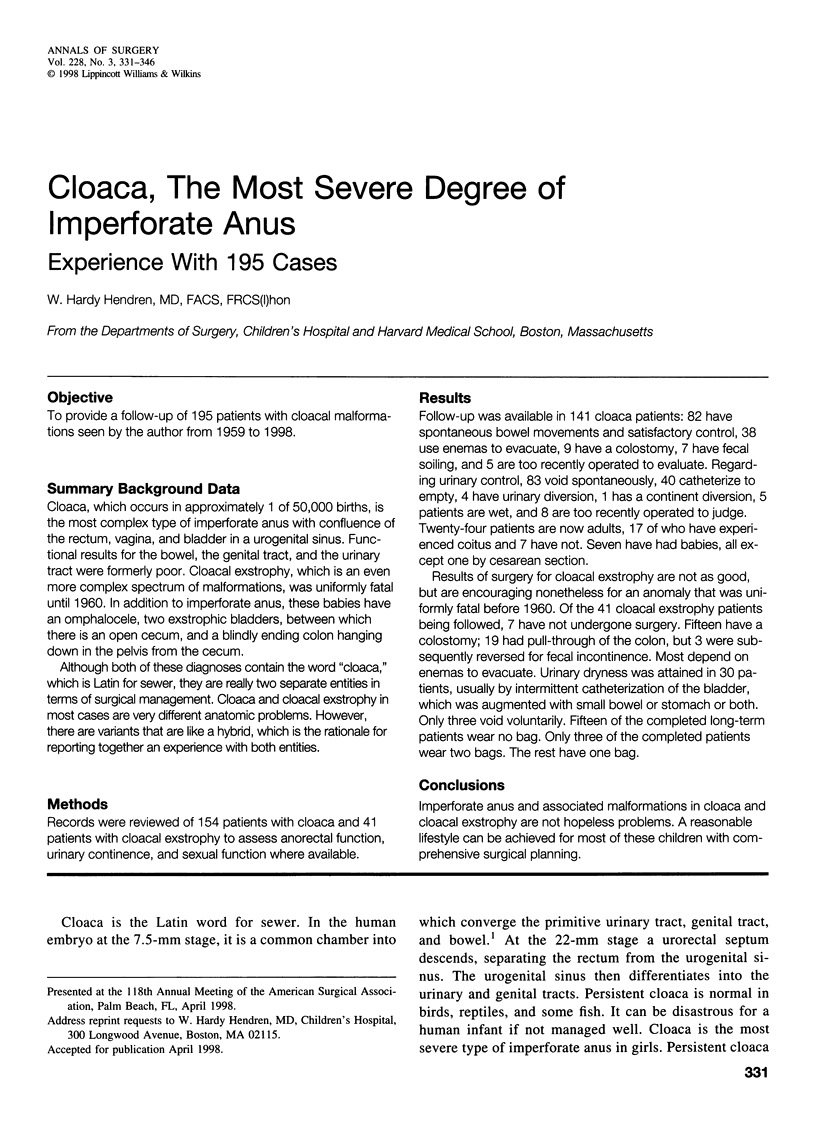

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Dykes E. H., Oesch I., Ransley P. G., Hendren W. H. Abnormal aorta and iliac arteries in children with urogenital abnormalities. J Pediatr Surg. 1993 May;28(5):696–700. doi: 10.1016/0022-3468(93)90035-j. [DOI] [PubMed] [Google Scholar]
- GOUGH M. H. Anorectal agenesis with persistence of cloaca. Proc R Soc Med. 1959 Oct;52:886–889. [PMC free article] [PubMed] [Google Scholar]
- Greenberg J. A., Hendren W. H. Vaginal delivery after cloacal malformation repair. Obstet Gynecol. 1997 Oct;90(4 Pt 2):666–667. doi: 10.1016/s0029-7844(97)00407-9. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Cloacal malformations: experience with 105 cases. J Pediatr Surg. 1992 Jul;27(7):890–901. doi: 10.1016/0022-3468(92)90393-l. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Further experience in reconstructive surgery for cloacal anomalies. J Pediatr Surg. 1982 Dec;17(6):695–717. doi: 10.1016/s0022-3468(82)80434-x. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Ileal nipple for continence in cloacal exstrophy. J Urol. 1992 Aug;148(2 Pt 1):372–379. doi: 10.1016/s0022-5347(17)36601-6. [DOI] [PubMed] [Google Scholar]
- Hendren W. H., Molenaar J. C. Simultaneous construction of vagina and rectum in a patient with absence of both. Z Kinderchir. 1987 Apr;42(2):112–114. doi: 10.1055/s-2008-1075564. [DOI] [PubMed] [Google Scholar]
- Hendren W. H., Oesch I. L., Tschaeppeler H., Bettex M. C. Repair of cloacal malformation using combined posterior sagittal and abdominal perineal approaches. Z Kinderchir. 1987 Apr;42(2):115–119. doi: 10.1055/s-2008-1075565. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Repair of cloacal anomalies: current techniques. J Pediatr Surg. 1986 Dec;21(12):1159–1176. doi: 10.1016/0022-3468(86)90032-1. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Surgical management of urogenital sinus abnormalities. J Pediatr Surg. 1977 Jun;12(3):339–357. doi: 10.1016/0022-3468(77)90010-0. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Urogenital sinus and anorectal malformation: experience with 22 cases. J Pediatr Surg. 1980 Oct;15(5):628–641. doi: 10.1016/s0022-3468(80)80514-8. [DOI] [PubMed] [Google Scholar]
- Hendren W. H. Urological aspects of cloacal malformations. J Urol. 1988 Nov;140(5 Pt 2):1207–1213. doi: 10.1016/s0022-5347(17)42004-0. [DOI] [PubMed] [Google Scholar]
- Holzman R. S. Latex allergy: an emerging operating room problem. Anesth Analg. 1993 Mar;76(3):635–641. doi: 10.1213/00000539-199303000-00034. [DOI] [PubMed] [Google Scholar]
- Hurwitz R. S., Manzoni G. A., Ransley P. G., Stephens F. D. Cloacal exstrophy: a report of 34 cases. J Urol. 1987 Oct;138(4 Pt 2):1060–1064. doi: 10.1016/s0022-5347(17)43502-6. [DOI] [PubMed] [Google Scholar]
- Jaramillo D., Lebowitz R. L., Hendren W. H. The cloacal malformation: radiologic findings and imaging recommendations. Radiology. 1990 Nov;177(2):441–448. doi: 10.1148/radiology.177.2.2217782. [DOI] [PubMed] [Google Scholar]
- Johnson R. J., Palken M., Derrick W., Bill A. H. The embryology of high anorectal and associated genitourinary anomalies in the female. Surg Gynecol Obstet. 1972 Nov;135(5):759–762. [PubMed] [Google Scholar]
- Lund D. P., Hendren W. H. Cloacal exstrophy: experience with 20 cases. J Pediatr Surg. 1993 Oct;28(10):1360–1369. doi: 10.1016/s0022-3468(05)80328-8. [DOI] [PubMed] [Google Scholar]
- Malone P. S., Ransley P. G., Kiely E. M. Preliminary report: the antegrade continence enema. Lancet. 1990 Nov 17;336(8725):1217–1218. doi: 10.1016/0140-6736(90)92834-5. [DOI] [PubMed] [Google Scholar]
- Mitchell M. E., Brito C. G., Rink R. C. Cloacal exstrophy reconstruction for urinary continence. J Urol. 1990 Aug;144(2 Pt 2):554–563. doi: 10.1016/s0022-5347(17)39521-6. [DOI] [PubMed] [Google Scholar]
- Palken M., Johnson R. J., Derrick W., Bill A. H. Clinical aspects of female patients with high anorectal agenesis. Surg Gynecol Obstet. 1972 Sep;135(3):411–416. [PubMed] [Google Scholar]
- Peña A. Anorectal malformations. Semin Pediatr Surg. 1995 Feb;4(1):35–47. [PubMed] [Google Scholar]
- Peña A., Devries P. A. Posterior sagittal anorectoplasty: important technical considerations and new applications. J Pediatr Surg. 1982 Dec;17(6):796–811. doi: 10.1016/s0022-3468(82)80448-x. [DOI] [PubMed] [Google Scholar]
- Peña A., Kessler O. Posterior cloaca: a unique defect. J Pediatr Surg. 1998 Mar;33(3):407–412. doi: 10.1016/s0022-3468(98)90079-3. [DOI] [PubMed] [Google Scholar]
- Peña A. The surgical management of persistent cloaca: results in 54 patients treated with a posterior sagittal approach. J Pediatr Surg. 1989 Jun;24(6):590–598. doi: 10.1016/s0022-3468(89)80514-7. [DOI] [PubMed] [Google Scholar]
- Peña A. Total urogenital mobilization--an easier way to repair cloacas. J Pediatr Surg. 1997 Feb;32(2):263–268. doi: 10.1016/s0022-3468(97)90191-3. [DOI] [PubMed] [Google Scholar]
- Raffensperger J. G., Ramenofsky M. L. The management of a cloaca. J Pediatr Surg. 1973 Oct;8(5):647–657. doi: 10.1016/0022-3468(73)90403-x. [DOI] [PubMed] [Google Scholar]
- Ricketts R. R., Woodard J. R., Zwiren G. T., Andrews H. G., Broecker B. H. Modern treatment of cloacal exstrophy. J Pediatr Surg. 1991 Apr;26(4):444–450. doi: 10.1016/0022-3468(91)90993-4. [DOI] [PubMed] [Google Scholar]
- Sato Y., Pringle K. C., Bergman R. A., Yuh W. T., Smith W. L., Soper R. T., Franken E. A., Jr Congenital anorectal anomalies: MR imaging. Radiology. 1988 Jul;168(1):157–162. doi: 10.1148/radiology.168.1.3380953. [DOI] [PubMed] [Google Scholar]
- Snyder W. H., Jr Some unusual forms of imperforate anus in female infants. Am J Surg. 1966 Mar;111(3):319–325. doi: 10.1016/s0002-9610(66)80006-5. [DOI] [PubMed] [Google Scholar]
- Warf B. C., Scott R. M., Barnes P. D., Hendren W. H., 3rd Tethered spinal cord in patients with anorectal and urogenital malformations. Pediatr Neurosurg. 1993;19(1):25–30. doi: 10.1159/000120696. [DOI] [PubMed] [Google Scholar]
- deVries P. A., Peña A. Posterior sagittal anorectoplasty. J Pediatr Surg. 1982 Oct;17(5):638–643. doi: 10.1016/s0022-3468(82)80126-7. [DOI] [PubMed] [Google Scholar]