

Abstract
Background:
Recent literature highlights the importance of treating hallux valgus (HV) as a 3-dimensional (3D) deformity. Although 3D printing may enhance visualization of the multiplanar aspects of HV, its influence on surgical planning remains unclear. This study assessed changes in surgical plans when surgeons sequentially reviewed 2D radiographs, 3D weightbearing computed tomography (WBCT), and 3D-printed models, hypothesizing that 3D printing would have the greatest impact.
Methods:
A single HV case (a 40-year-old woman, intermetatarsal angle [IMA] 21 degrees, HV angle [HVA] 47 degrees) was evaluated by 30 surgeons in a masked, stepwise manner. Surgical plans were recorded at each stage. Surgeons rated the influence of WBCT and 3D printing using a 5-point Likert scale. A follow-up survey examined the effect of these technologies on correction amplitudes.
Results:
The participants were mostly early career surgeons (median age 35.5 years, 2 years in practice). WBCT was accessible to 43.3% and used in 30% of HV cases, whereas 3D printing was accessible to 23.3% and used in 6.6%. Changes in the treatment algorithm occurred in 30% of cases after WBCT and in 43.3% after 3D printing. Significant differences (P < .05) were observed for the Lapicotton procedure between radiography and WBCT, and between WBCT and 3D printing. Surgeons performing <50 HV cases annually or with >70% Foot and Ankle specialization were more influenced by WBCT. Follow-up data (n = 23) indicated that WBCT and 3D printing influenced correction amplitudes, particularly for pronation and distal metatarsal articular angle (DMAA), more than for the IMA.
Discussion:
Both WBCT and 3D printing influenced surgical planning, mostly explained by changes in first ray tarsometatarsal procedures. The rotational components (pronation and DMAA) were perceived as the most significantly affected. Future studies should explore cost-effectiveness, patient outcomes, and the utility of combining WBCT and 3D printing in other deformities requiring multiplanar corrections.
Level of Evidence: Level IV, cross-sectional survey.
Keywords: weightbearing computed tomography, cone beam, 3D-printing, hallux valgus
Visual Abstract.

This is a visual representation of the abstract.
Introduction
The management of hallux valgus (HV) as a 3-dimensional (3D) deformity has been a recurring challenge in the literature.15,29,30 Recent advances, particularly through modern weightbearing computed tomography (WBCT), have enabled significant progress in understanding the deformity beyond the correction of the first intermetatarsal and metatarsophalangeal angles in the axial plane.7 -9,11,15,22 Consequently, the orientation of the metatarsal head or distal metatarsal articular angle (DMAA), the rotation and intrinsic torsion of the first metatarsal, and the dislocation of the sesamoid complex are now systematically addressed in the literature and in clinical practice, as colleagues are now well aware of these multidimensional components.9,17 -19,23 Conversely, translating this knowledge into clinically applicable solutions that may influence treatment plans remains underexplored. However, although 3D printing27,31,33 and ancillary-based surgical correction guides are increasingly referenced in orthopaedics, their application in HV literature remains limited.6,28,34 The multiplanar correction of HV remains for the most part bound to the surgeon’s own manual and visual assessment and corrective skills. Using 3D printing not only for personalized surgical guides but as a planning3,32 and an educational tool14,20,21 particularly to evaluate first metatarsophalangeal joint (MTP) congruity (Figure 1) offers potential and has not previously been reported in the literature in hallux valgus. The aim of the present study was to test the influence of introducing a 3D-printed model of an HV case in a Foot and Ankle training course, in order to evaluate the impact of 3D-printed models on surgical decision making. The theme of the course was not specifically related to WBCT or hallux valgus. A secondary objective was to investigate whether this influence was different in the population of surgeons who have access to WBCT and 3D printing. We hypothesized that being exposed to the 3D-printed model would result in measurable changes in the proposed treatment plan for most surgeons, with a heightened effect in those who have access to this technology.
Figure 1.

An example of first metatarsophalangeal joint congruity evaluation pre (left) and post (right) correction using a 3D-printed model.
Materials and Methods
Study Design
This study was conducted using a sample of convenience that included participants during the International Bone Research Association (IBRA) Foot and Ankle course in Austin, Texas, October 2024. A survey was administered to all course participants and faculty members who did not take part in preparing the study material. The case of a patient with an HV deformity requiring operative treatment was used for the current study, and 30 identical 3D-printed models were produced. The study adhered to the ethical standards of the institutional research committee. Ethical approval from the relevant institutional review board was obtained (Pro00113556). The CROSS (Consensus-based checklist for Reporting of Survey Studies) was used. 26 This study used a Level IV cross-sectional survey design.5,16
Case
The subject was a 40-year-old woman with a body mass index (BMI) of 36 who presented with an HV deformity that had progressively worsened over the past 2 years, primarily affecting her left side. The patient complained of pain on the medial aspect of the first metatarsal head and deformity but no joint pain. The arc of motion was pain-free. No metatarsalgia was noted. No hypermobility of the first TMT joint was noted by the physician. Conservative treatments, including shoe modifications and inserts, failed to alleviate her symptoms. Clinical examination also revealed a mild planus deformity. Full range of motion (ROM) was noted in all foot joints. Weightbearing radiographs indicated a first-second intermetatarsal angle (IMA) of 21 degrees and a hallux valgus angle (HVA) of 47 degrees (Figure 2). Automated measurements from WBCT scans showed an IMA of 17 degrees, an HVA of 33 degrees, and an HV interphalangeal angle of 8 degrees (measurements performed using Bonelogi Foot & Ankle Module (Disior Ltd, Helsinki, Finland). The sesamoid rotation and alpha angles were 36 and 18 degrees, respectively. Although these figures were measured a priori by investigators and given to participants, they were shown the whole WBCT data set and were able to assess themselves.
Figure 2.

Plain radiographic dorsal-plantar view of the case.
3D Printing Process
Conebeam WBCT scans were performed using a HiRise WBCT unit (CurveBeamAI, Hatfield, PA) with a voxel size of 0.37 mm; a 350-mm field-of-view diameter, a 200-mm field-of-view height, an exposure time of 9 seconds, and a total scan time of 54 seconds. The Digital Imaging and Communications in Medicine (DICOM) files were then downloaded via the WBCT manufacturer software (CubeView; CurvebeamAI). All foot bones, including both sesamoids but excluding the middle and distal phalanges of the second, third, fourth, and fifth toes, were semiautomatically segmented using Bonelogic Foot & Ankle Module (Disior Ltd). Subsequently, the stereolithography (*.STL) files of the segmented bones were imported into Geomagic Design X (Oqton Ghent, Belgium), where 2-mm-thick connecting bars of varying lengths were placed transversely at the center of all joints to ensure sufficient stability of the 3D-printed model. The segmented bones and connectors were fused and exported as a single STL file, which was then imported into Creality Print 5.1 software. The model was scaled to 75%, and support trees were generated automatically. Six models were printed simultaneously using a Creality K1 Max AI Fast 3D Printer (Shenzhen Creality 3D Technology Co, Ltd, Shenzhen, China) with a 0.4-mm nozzle size and a printing area of 300 × 300 × 300 mm. The filament used was 1.75-mm polylactic acid (PLA) in white, with a slice thickness of 0.2 mm. After printing, the support trees were carefully manually removed by sectioning the most distal tree branches with precision pliers.
Investigations and Measurements
Participants were introduced to the patient’s medical history and conventional weightbearing radiographs via a PowerPoint presentation, then asked to record their choice of treatment algorithm. Each subsequent step was masked to the next. Treatment algorithms were chosen and combined at will from a fixed list of options, including isolated first tarsometatarsal joint (TMT1) fusion, Lapidus procedure, Lapicotton 10 (TMT1 fusion with dorsal wedge bone block), scarf, chevron, minimally invasive chevron (MICA), Akin osteotomy, lateral release, first metatarsophalangeal joint (MTP1) fusion, distal and proximal double osteotomy, proximal rotational metatarsal osteotomy (PROMO). 29 Three-dimensional reconstructions were created from WBCT scans (Figure 3). Sagittal, coronal, and axial WBCT slices were shown in video format, as well as selected slices, then participants were asked again to record their treatment algorithm. Subsequently, each participant received a 3D-printed foot model for visual and tactile assessment (Figure 4, A and B). After 10 minutes of evaluation, participants were asked to record their choice of treatment algorithm for a third time, and then return a completed electronic questionnaire 1 with Likert scale questions (0 =not at all, 1 = slightly, 2 = significantly, 3 = a lot, 4 = 100%, couldn’t have done without it) to evaluate how WBCT and 3D printing models influenced decision making as compared with conventional radiographs, and how 3D printing compared to WBCT. Participants completed an electronic survey immediately following the presentation. 2 The last option was left open in case some participants did not find the proposed choices sufficient and could therefore express their potential biases. Subsequently, a follow-up electronic questionnaire was sent using Google forms to investigate how, even if the treatment plan did not change, the access to WBCT and 3D printing changed the amount of correction that would be planned in terms of intermetatarsal angle (IMA), the rotation and the distal metatarsal articular angle (DMAA). Participants were also asked whether they felt that 3D printing was an added value over radiographs and over WBCT.
Figure 3.
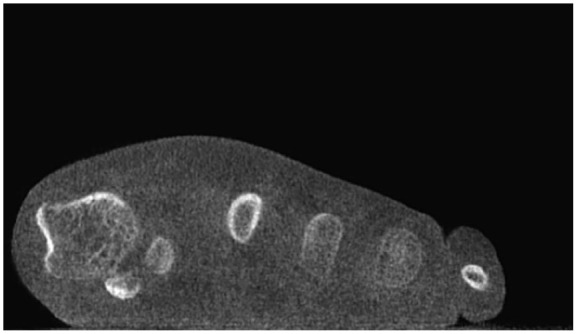
Weightbearing computed tomography coronal slice showing first metatarsal pronation and subluxation of the sesamoid complex.
Figure 4.

(A) Result of 3D printing showing a coronal view of the first column. (B) Result of 3D printing showing an anteroposterior view of the first column.
Statistical Analysis
Statistical analyses were performed using R (R Foundation for Statistical Computing, Vienna, Austria). Normality of continuous variables was assessed using the Shapiro-Wilk test. Non normally distributed variable results were reported as medians and interquartile ranges (IQRs). Participants were grouped based on their experience with hallux valgus: 1 = 0-50 cases per year, 2 = >50 cases. Binary and ordinal data were reported as frequencies and percentages. For each procedure, we analyzed changes in treatment algorithms for each procedure at 3 time points (after radiography, after WBCT, and after examining a 3D-printed model). Cochran Q test was used to assess overall differences across the 3 conditions. If Cochran Q was significant, we conducted pairwise McNemar tests to identify differences between specific time points. Discrete outcomes were compared with χ2 or Fisher exact test accordingly. The alpha risk was set to 5%.
Results
Surveyed Population Demographics
Participants demographics were non-normally distributed. The median age was 35.5 years (IQR 8.5), the median time in practice was 2 years (IQR 9.75). Foot and ankle surgery constituted 70% (IQR 88.75) of participants’ practice, with 53.3% being faculty, 33.3% fellows, and 13.3% residents. Eighteen participants (60%) came from the United States, whereas 12 were from other countries. A total of 73.3% of participants performed at least 10 cases of HV per year. Weightbearing CT was accessible for 43.3% of participants, who used it for planning HV surgery in 30% of cases. 3D-printing was accessible for 23.3%, who used it for planning in 6.6% of cases.
Changes in Treatment Algorithm
The initial treatment plan distribution is shown in Figure 6, with a majority of participants choosing Lapidus, fusion, Akin osteotomy, and lateral release (Figure 5). Changes in the treatment algorithm were observed in 30% of cases between radiography and WBCT assessment. After evaluating the 3D-printed model, an additional 33% of changes were observed. Overall, a total of 43.3% of changes occurred between the first radiographic step and the third 3D printing step. However, only the Lapicotton procedure showed statistically significant differences between time points. Specifically, the proportion of participants selecting Lapidus with plantarflexion osteotomy of the first ray differed significantly from the radiographic to the WBCT step (P < .05) and from the WBCT to 3D model step (P < .05). No other procedures demonstrated significant pairwise differences.
Figure 6.

(A) Pooled histogram of weightbearing computed tomography (WBCT) influence on algorithms based on experience with hallux valgus (HV). (B) Normalized pooled histogram of WBCT influence on algorithms based on surgeon specialization.
Figure 5.

Distribution of initial treatment algorithm after presentation of conventional radiographic material.
Group Comparison
Surgeons performing fewer than 50 cases per year judged that WBCT significantly changed their algorithm in 68.42% of cases compared with 27.27% for those who performed more than 50 cases per year (P < .05) (Figure 6, A and B). Conversely, surgeons whose practice comprised more than 70% foot and ankle surgery were influenced by WBCT findings in 80% of cases, compared with 73.3% for those with less specialized practices (P < .05). Whether participants had access to and used WBCT and/or 3D printing did not influence their choice and changes in treatment algorithms during this study.
Follow-Up Survey
Twenty-three participants (76.8%) answered the follow-up survey. Of these, 56.5% stated that WBCT would have influenced the amount of correction of the IMA, even if no change in the treatment plan was required. Although only 17.4% reported changes greater than 50%, those proportions increased respectively to 56.5% and 26% considering the DMAA and 82.6% and 21.17% considering the pronation of the first metatarsal. A majority of participants (86.9%) considered 3D printing as an added value over radiography, and 82.6% felt it added value over WBCT.
Discussion
We found significant overall changes in participants’ treatment algorithms after reviewing WBCT images and 3D printing models with only the Lapicotton procedure independently explaining those changes. Furthermore, we found that the less experienced and the more specialized participants were, the more their treatment algorithm was influenced by WBCT over radiographs. This was not the case for 3D printing over WBCT. Finally, we found that despite this point, most participants in the follow-up study declared that both 3D technologies would influence their approach to pronation of the first ray as opposed to the IMA or DMAA and considered these to be of added values compared with conventional radiography.
To our knowledge, this is the first study to evaluate 3D-printed models as educational tools for the specific purpose of planning HV surgery. As modern and game changing as it may be perceived intuitively in the Foot and Ankle community, it has seemingly remained a challenge to find and describe its role in education especially in such a common pathology as HV, and no study had until now investigated its use in the context of a specialized course. Previous literature on 3D-printed models around surgery has mostly investigated intraoperative variables along with results and outcomes when the models are available for inspection prior to surgery but did not investigate how they changed the actual surgical decision-making among a panel of surgeons. This literature has on the other hand reported noteworthy improvements with 3D models in regard to operative and fluoroscopy times, blood loss, quality of surgical reduction, and outcomes in fractures generally, 33 pelvic 31 and acetabular 20 fractures specifically, as well as in distal radius fracture. 35 In the foot and ankle, Shi et al 27 have reported similar benefits in calcaneal fractures treated by open reduction and internal fixation and Ozturk et al 24 in a randomized controlled setting reported the same in hallux valgus. The new and unique knowledge brought by the present work is that even before those demonstrated intraoperative and outcome benefits, 3D-printed models associated with WBCT may provide grounds for surgeons to make more informed and more confident surgical indication decisions. The finding that 43.3% of surgeons altered their treatment plans after reviewing 3D models underscores the broader clinical significance of these tools beyond technical precision. Particularly, regarding 3D components of the planned correction, we found that the Lapicotton procedure, which alters both rotation and elevation of the first ray, 10 explained most of our findings and was the only significant procedure change between the radiographic, WBCT, and 3D printing steps.
The use of 3D printing in orthopaedics in general and HV in particular has been better known for creating surgical navigation templates.12,13,34 Although guides are produced based on 3D anatomy using conventional (nonweightbearing) CT, the planning remains 2-dimensional as measurements are still mostly provided by conventional radiography. It is possible that in the future, these guides evolve to include 3D calculations of the metatarsal center of the rotational angle (CORA) to improve triplanar correction. The use of WBCT is better suited in HV to account for first ray rotation, 23 which was a key consideration in this study. We looked at the overall decision-making process (Cochrane Q), whereas the subsequent Mac Neymar test looked at intermediate modalities (between 2D and WBCT and WBCT and 3D models) thereby correlating the additional information provided by the 3D models and standard radiography, with significant changes in first ray procedures at each stage. Also, participants reported that the WBCT and the 3D-printed model influenced rotation more than the DMAA or the IMA. This tends to confirm that rotation is not well assessed through conventional imaging (either 2D and/or nonweightbearing). It also tends to confirm that a significant part of the apparent distal articular orientation of the first metatarsal head, mostly reported as the DMAA, may be a projection effect of first ray rotation, as previously reported. 18
Our results align with previous studies emphasizing the value of 3D printing in surgical planning and precision. Particularly, a previous study has highlighted the utility of 3D printing in addressing the 3D components of hallux valgus (HV), 6 demonstrating improvements in metrics such as the hallux valgus angle (HVA) and intermetatarsal angle (IMA), despite being a study based off nonweightbearing conventional CT scans, which may have altered their results. This concurs with our findings of significant changes in surgical plans after visualizing 3D WBCT data sets and physically examining a 3D model printed from these data. Similarly, Fernández-Ehrling et al 12 found that 3D-printed guides improved osteotomy accuracy, especially for less experienced surgeons, which mirrors our observation that 3D printing significantly influences surgical decision-making across various levels of experience. Future studies should aim at investigating how these technological improvements impact outcomes in HV surgery where they are available. Indeed, past literature and practice show that patients seem to be satisfied whatever the technique used, so it is important not to underestimate, but also not to overestimate, the clinical relevance of 3D technologies. Furthermore, the economics must be taken into account. WBCT has upfront costs reimbursement in the USA, generally ranging from $100 to $300 dependent on insurance coverage. These costs can be managed within the broader patient workflow, 4 while taking into account that these differ throughout the world. 25 The 3D printing process is not reimbursed, but a $1000 printer and a $20 spool of polylactic acid can produce 10 to 20 models, making it a manageable addition to surgical planning.
The authors acknowledge the following limitations in this study. First, as a survey-based study, it lacks the robustness of a clinical trial, which can quantify variables such as blood loss, fluoroscopy levels, surgical duration, and outcomes; however, that was not the focus here. However, this is mitigated by the live assessments of 30 orthopaedic surgeons with a follow-up survey and a 77% answering rate. The experience of surveyed participants was diverse, which could limit the applicability of our findings, but also provided interesting insights into the acceptability of 3D technology depending on the time in practice and the degree of specialization. Second, we performed the study using a severe case that may have overestimated the usefulness of 3D printing where WBCT is available and the generalizability of our findings is limited. Conversely, using a milder case could have underestimated it. It could be argued that we could have investigated both; however, the aim was to focus repeatably on changes in a unique surgical plan. Third, 3D printing does not yet allow the evaluation of soft tissue involvement in the deformity, which limits the applicability of our findings regarding soft tissue procedures. Finally, because we were in the setting of an educational course, the content or discussions could have influenced the decision process of participants. However, the opportunity of having access to a panel of surgeons and giving access to each to a 3D-printed model enabled to maximize data collection.
Conclusions
The clinical relevance of our findings is that 3D printing appears to enhance surgical planning, particularly considering the case of early career surgeons in HV and most significantly regarding the control of the 3D rotational aspect of the correction. Future research should focus on whether expanding the use of WBCT and 3D models in clinical trials will ultimately strengthen the evidence base and support their routine implementation in clinical workflows, similar to some recommendations from meta-analyses in the field of fracture management.32,33 Further studies should assess the cost-effectiveness of these advanced technologies applied to hallux valgus surgery.
Supplemental Material
Supplemental material, sj-pdf-1-fao-10.1177_24730114251325854 for A Hallux Valgus Surgical Planning Survey Using WBCT-based 3D Printing by François Lintz, Enrico Pozzessere, Wolfram Grün, Antoine Acker, Erik Jesús Huánuco Casas, Eric Ferkel and Cesar de Cesar Netto in Foot & Ankle Orthopaedics
Acknowledgments
The course attended by participants of the study was organized by the International Bone Research Association.
Footnotes
Ethical approval: Ethical approval for this study was obtained from Duke University Health Institutional Review Board (Pro00113556).
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: François Lintz, MD, PhD, reports disclosures from Paragon28 (consultant, shareholder), CurvebeamAI (consultant, shareholder), Newclip Technics (consultant, royalties), Podonov (consultant, royalties), LINNOV (founder, shareholder), Followinvest (shareholder), and International WBCT Society (cofounder, past president). Antoine Acker, MD, reports disclosures from CurvebeamAI (shareholder). Eric Ferkel, MD, reports disclosures from Ossio, Arthrex, Smith & Nephew, Medartis (consulting fees, royalties), International Bone Research Association (IBRA), American Academy of Orthopaedic Surgeons (AAOS) (support for attending meetings), and AAOS, American Orthopaedic Society for Sports Medicine (AOSSM), American Orthopaedic Foot & Ankle Society (AOFAS), Arthroscopy Association of North America (AANA) leadership roles. Cesar de Cesar Netto, MD, PhD, reports disclosures from Paragon28 (consultant, medical advisory board, royalties), CurvebeamAI (consultant, shareholder), Ossio (consultant), Zimmer (consultant), Stryker (consultant), International WBCT Society (cofounder, President), Exactech (consultant), Arthrex (consultant), Tayco Brace (shareholder), Extremity Medical (consultant), AOFAS committee member, and Foot Ankle Clinics (editor in chief). Disclosure forms for all authors are available online.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Article editorial processing fee for open access was paid for by first author. Support was provided by the Ramsay Healthcare Foundation to the first authors for this article editorial processing fee.
ORCID iDs: François Lintz, MD, PhD,  https://orcid.org/0000-0002-0163-6516
https://orcid.org/0000-0002-0163-6516
Cesar de Cesar Netto, MD, PhD,
https://orcid.org/0000-0001-6037-0685
References
- 1.3D-Printing Surgical Planning Study. https://forms.gle/1DpH9J6MFbpUprLU8
- 2.3D-Printing Surgical Planning Survey. https://forms.gle/Tk1KAvaQgpTpq1Hg6
- 3. Alemayehu DG, Zhang Z, Tahir E, Gateau D, Zhang DF, Ma X. Preoperative planning using 3D printing technology in orthopedic surgery. Biomed Res Int. 2021;2021:7940242. doi: 10.1155/2021/7940242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Alexander NB, Sarfani S, Strickland CD, et al. Cost analysis and reimbursement of weightbearing computed tomography. Foot Ankle Orthop. 2023;8(1):24730114231164143. doi: 10.1177/24730114231164143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bhandari M, Swiontkowski MF, Einhorn TA, et al. Interobserver agreement in the application of levels of evidence to scientific papers in the American volume of the Journal of Bone and Joint Surgery. J Bone Joint Surg Am. 2004;86(8):1717-1720. doi: 10.2106/00004623-200408000-00016 [DOI] [PubMed] [Google Scholar]
- 6. Cao J, Zhang Y, Wang X, et al. Comparative analysis of triplanar chevron osteotomy (TCO) and chevron osteotomy (CO) for treating mild to moderate hallux valgus via computer simulation and 3D printing: an observational study. Medicine (Baltimore). 2024;103(48):e40643. doi: 10.1097/MD.0000000000040643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Collan L, Kankare JA, Mattila K. The biomechanics of the first metatarsal bone in hallux valgus: a preliminary study utilizing a weight bearing extremity CT. Foot Ankle Surg. 2013;19(3):155-161. doi: 10.1016/j.fas.2013.01.003 [DOI] [PubMed] [Google Scholar]
- 8. Day J, de Cesar Netto C, Burssens A, Bernasconi A, Fernando C, Lintz F. A case-control study of 3D vs 2D weightbearing CT measurements of the M1-M2 intermetatarsal angle in hallux valgus. Foot Ankle Int. 2022;43(8):1049-1052. doi: 10.1177/10711007221091812 [DOI] [PubMed] [Google Scholar]
- 9. de Carvalho KAM, Walt JS, Ehret A, et al. Comparison between weightbearing-CT semiautomatic and manual measurements in hallux valgus. Foot Ankle Surg. 2022;28(4):518-525. doi: 10.1016/j.fas.2022.02.014 [DOI] [PubMed] [Google Scholar]
- 10. de Cesar Netto C, Ehret A, Walt J, et al. Early results and complication rate of the LapiCotton procedure in the treatment of medial longitudinal arch collapse: a prospective cohort study. Arch Orthop Trauma Surg. 2023;143(5):2283-2295. doi: 10.1007/s00402-022-04399-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. de Cesar Netto C, Richter M. Use of advanced weightbearing imaging in evaluation of hallux valgus. Foot Ankle Clin. 2020;25(1):31-45. doi: 10.1016/j.fcl.2019.10.001 [DOI] [PubMed] [Google Scholar]
- 12. Fernández-Ehrling N, Nieto-García E, Ramirez-Andrés L, et al. Surgical precision of MICA and Reverdin-Isham using 3D-printed guides: a cadaveric study. Medicina (Kaunas). 2024;60(10):1613. doi: 10.3390/medicina60101613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ferreira GF, Nunes GA, Banca VL, et al. Minimally invasive hallux valgus surgery using 3D printed patient specific instrumentation. Arch Orthop Trauma Surg. 2024;144(6):2553-2559. doi: 10.1007/s00402-024-05383-6 [DOI] [PubMed] [Google Scholar]
- 14. Hasenstein T, Patel KP, Moore JL, Meyr AJ. Printed 3-dimensional computed tomography scanned ankle fractures as an educational instrument. J Foot Ankle Surg. 2019;58(6):1081-1084. doi: 10.1053/j.jfas.2018.08.012 [DOI] [PubMed] [Google Scholar]
- 15. Kim Y, Kim JS, Young KW, Naraghi R, Cho HK, Lee SY. A new measure of tibial sesamoid position in hallux valgus in relation to the coronal rotation of the first metatarsal in CT scans. Foot Ankle Int. 2015;36(8):944-952. doi: 10.1177/1071100715576994 [DOI] [PubMed] [Google Scholar]
- 16. Kumar M, Gopalakrishna C, Swaminath PV, Mysore SS. Evidence-based surgery – evidence from survey and citation analysis in orthopaedic surgery. Ann R Coll Surg Engl. 2011;93(2):133-138. doi: 10.1308/003588411X1285163910787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Lalevée M, Barbachan Mansur NS, Dibbern K, et al. Coronal plane rotation of the medial column in hallux valgus: a retrospective case-control study. Foot Ankle Int. 2022;43(8):1041-1048. doi: 10.1177/10711007221091810 [DOI] [PubMed] [Google Scholar]
- 18. Lalevée M, Barbachan Mansur NS, Lee HY, et al. Distal metatarsal articular angle in hallux valgus deformity. Fact or fiction? A 3-dimensional weightbearing CT assessment. Foot Ankle Int. 2022;43(4):495-503. doi: 10.1177/10711007211051642 [DOI] [PubMed] [Google Scholar]
- 19. Lalevée M, de Carvalho KAM, Barbachan Mansur NS, et al. Distribution, prevalence, and impact on the metatarsosesamoid complex of first metatarsal pronation in hallux valgus. Foot Ankle Surg. 2023;29(6):488-496. doi: 10.1016/j.fas.2023.06.003 [DOI] [PubMed] [Google Scholar]
- 20. Lim PK, Stephenson GS, Keown TW, et al. Use of 3D printed models in resident education for the classification of acetabulum fractures. J Surg Educ. 2018;75(6):1679-1684. doi: 10.1016/j.jsurg.2018.04.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Maglara E, Angelis S, Solia E, et al. Three-dimensional (3D) printing in orthopedics education. J Long Term Eff Med Implants. 2020;30(4):255-258. doi: 10.1615/JLongTermEffMedImplants.2020036911 [DOI] [PubMed] [Google Scholar]
- 22. Mahmoud K, Metikala S, Mehta SD, Fryhofer GW, Farber DC, Prat D. The role of weightbearing computed tomography scan in hallux valgus. Foot Ankle Int. 2021;42(3):287-293. doi: 10.1177/1071100720962398 [DOI] [PubMed] [Google Scholar]
- 23. Mansur NSB, Lalevee M, Schmidt E, et al. Correlation between indirect radiographic parameters of first metatarsal rotation in hallux valgus and values on weight-bearing computed tomography. Int Orthop. 2021;45(12):3111-3118. doi: 10.1007/s00264-021-05136-9 [DOI] [PubMed] [Google Scholar]
- 24. Ozturk AM, Suer O, Coban I, Ozer MA, Govsa F. Three-dimensional printed anatomical models help in correcting foot alignment in hallux valgus deformities. Indian J Orthop. 2020;54(suppl 1):199-209. doi: 10.1007/s43465-020-00110-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Richter M, Lintz F, de Cesar Netto C, Barg A, Burssens A. Results of more than 11,000 scans with weightbearing CT – impact on costs, radiation exposure, and procedure time. Foot Ankle Surg. 2020;26(5):518-522. doi: 10.1016/j.fas.2019.05.019 [DOI] [PubMed] [Google Scholar]
- 26. Sharma A, Minh Duc NT, Luu Lam Thang T, et al. A consensus-based Checklist for Reporting of Survey Studies (CROSS). J Gen Intern Med. 2021;36(10):3179-3187. doi: 10.1007/s11606-021-06737-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Shi G, Liu W, Shen Y, Cai X. 3D printing-assisted extended lateral approach for displaced intra-articular calcaneal fractures: a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):682. doi: 10.1186/s13018-021-02832-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Smith KE, Dupont KM, Safranski DL, et al. Use of 3D printed bone plate in novel technique to surgically correct hallux valgus deformities. Tech Orthop. 2016;31(3):181-189. doi: 10.1097/BTO.0000000000000189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Wagner P, Ortiz C, Wagner E. Rotational osteotomy for hallux valgus. A new technique for primary and revision cases. Tech Foot Ankle Surg. 2017;16(1):3-10. doi: 10.1097/BTF.0000000000000142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Wagner P, Wagner E. Role of coronal plane malalignment in hallux valgus correction. Foot Ankle Clin. 2020;25(1):69-77. doi: 10.1016/j.fcl.2019.10.009 [DOI] [PubMed] [Google Scholar]
- 31. Wang J, Wang X, Wang B, et al. Comparison of the feasibility of 3D printing technology in the treatment of pelvic fractures: a systematic review and meta-analysis of randomized controlled trials and prospective comparative studies. Eur J Trauma Emerg Surg. 2021;47(6):1699-1712. doi: 10.1007/s00068-020-01532-9 [DOI] [PubMed] [Google Scholar]
- 32. Wood L, Ahmed Z. Does using 3D printed models for pre-operative planning improve surgical outcomes of foot and ankle fracture fixation? A systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2024;50(1):21-35. doi: 10.1007/s00068-022-02176-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Yammine K, Karbala J, Maalouf A, Daher J, Assi C. Clinical outcomes of the use of 3D printing models in fracture management: a meta-analysis of randomized studies. Eur J Trauma Emerg Surg. 2022;48(5):3479-3491. doi: 10.1007/s00068-021-01758-1 [DOI] [PubMed] [Google Scholar]
- 34. Zhao T, Chen H, Jia B, Zhang Y, Wang Y, Bai Y. Application of 3D printing navigation template technology in severe hallux valgus surgery. J Musculoskelet Neuronal Interact. 2023;23(4):448-455. [PMC free article] [PubMed] [Google Scholar]
- 35. Zhu D, Zhang Z, Zhang J, et al. The efficacy of 3D printing-assisted surgery in treating distal radius fractures: systematic review and meta-analysis. J Comp Eff Res. 2020;9(13):919-931. doi: 10.2217/cer-2020-0099 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-fao-10.1177_24730114251325854 for A Hallux Valgus Surgical Planning Survey Using WBCT-based 3D Printing by François Lintz, Enrico Pozzessere, Wolfram Grün, Antoine Acker, Erik Jesús Huánuco Casas, Eric Ferkel and Cesar de Cesar Netto in Foot & Ankle Orthopaedics