

Abstract
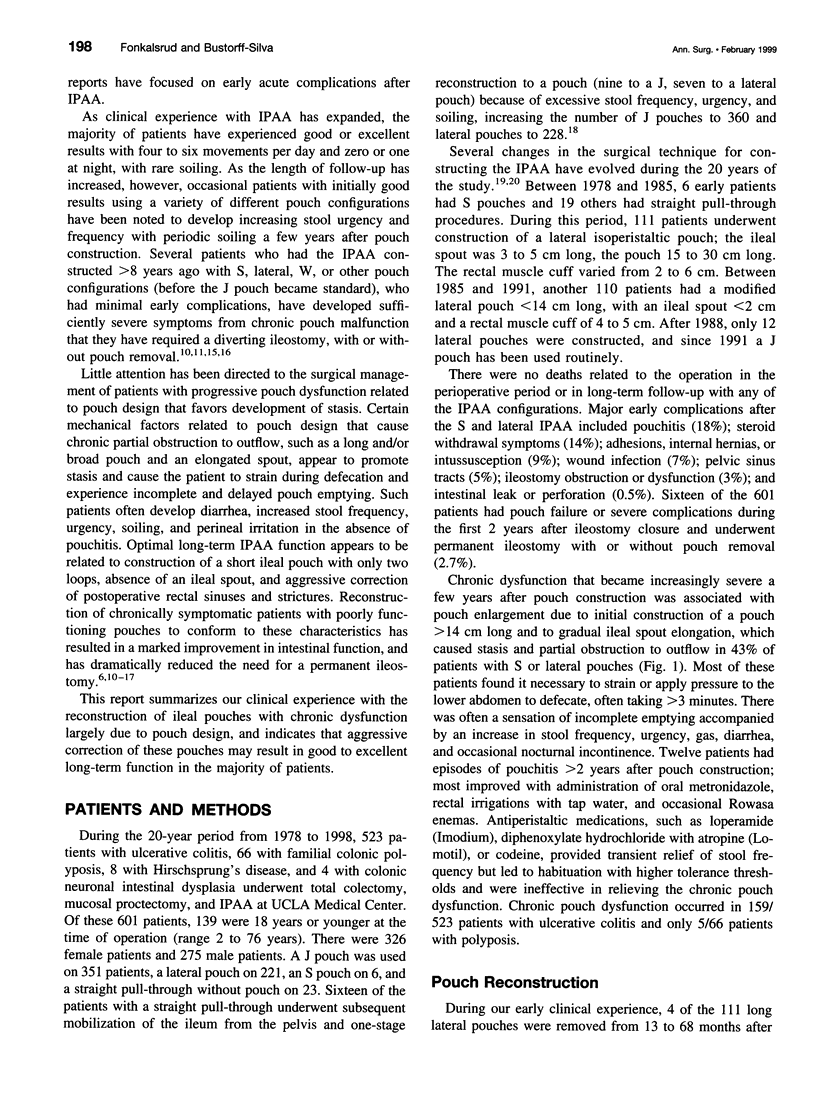
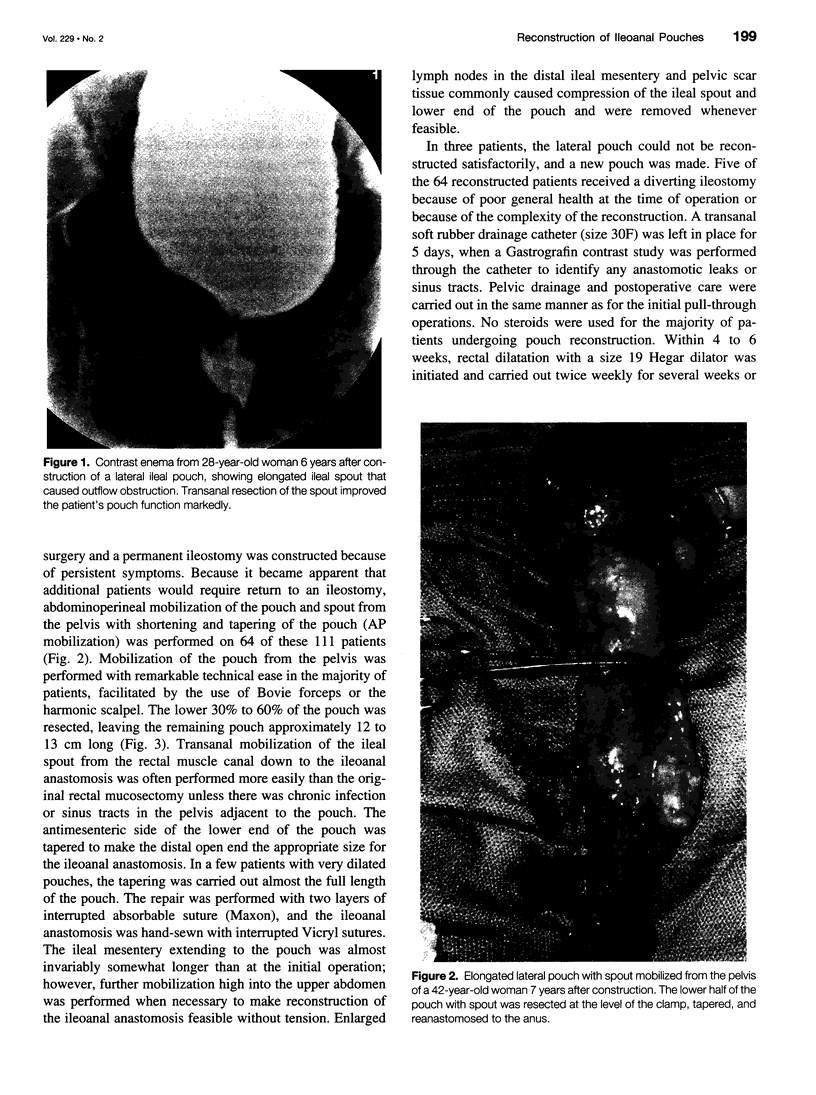
OBJECTIVE: A retrospective review was performed to determine the results after surgical reconstruction for chronic dysfunction of ileal pouch-anal procedures for ulcerative colitis and familial colonic polyposis at a university medical center. METHODS: During the 20-year period from 1978 to 1998, 601 patients underwent colectomy and ileal pouch-anal anastomosis (IPAA) for ulcerative colitis, familial colonic polyposis, or Hirschsprung's disease. A J pouch was used for 351 patients, a lateral pouch for 221, an S pouch for 6, and a straight pull-through for 23. Acute complications after pouch construction have been detailed in previous publications and are not included in this study. Chronic pouch stasis with diarrhea, frequency, urgency, and soiling gradually became more severe in 164 patients (27.3%), associated with pouch enlargement, an elongated efferent limb, and obstruction to pouch outflow, largely related to the pouch configuration used during the authors' early clinical experience. These patients were sufficiently symptomatic to be considered for reconstruction (mean 68 months after IPAA). Transanal resection of an elongated IPAA spout was performed on 58 patients; abdominoperineal mobilization of the pouch with resection and tapering of the lower end (AP reconstruction) and ileoanal anastomosis on 83; pouch removal and new pouch construction on 7; and conversion of a straight pull-through to a pouch on 16. RESULTS: Good long-term results (mean 7.7 years) with improvement in symptoms occurred in 98% of transanal resections, 91.5% of AP reconstructions, 86% of new pouch constructions, and 100% of conversions of a straight pull-through to a pouch. The average number of bowel movements per 24 hours at 6 months was 4.8. Complications occurred in 11.6% of reconstructed patients. Five of the 164 patients (3.1%) required eventual pouch removal and permanent ileostomy. The high rate of pouch revision in this series of patients undergoing IPAA is due to a policy of aggressive correction when patients do not experience an optimal functional result, or have a progressive worsening of their status. CONCLUSIONS: Although occasionally a major undertaking, reconstruction of ileoanal pouches with progressive dysfunction due to large size or a long efferent limb has resulted in marked improvement in intestinal function in >93% of patients and has reduced the need for late pouch removal.
Full text
PDF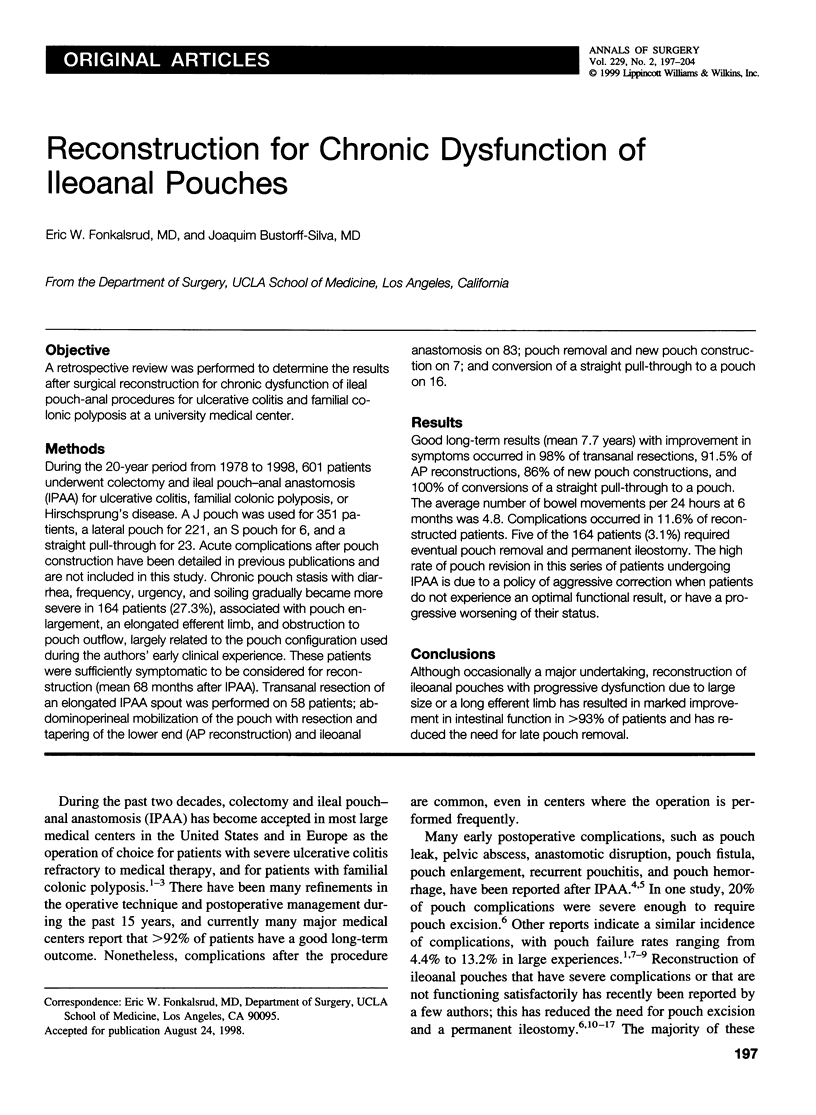

Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cohen Z., Smith D., McLeod R. Reconstructive surgery for pelvic pouches. World J Surg. 1998 Apr;22(4):342–346. [PubMed] [Google Scholar]
- Dayton M. T., Larsen K. P. Outcome of pouch-related complications after ileal pouch-anal anastomosis. Am J Surg. 1997 Dec;174(6):728–732. doi: 10.1016/s0002-9610(97)00188-8. [DOI] [PubMed] [Google Scholar]
- Fazio V. W., Ziv Y., Church J. M., Oakley J. R., Lavery I. C., Milsom J. W., Schroeder T. K. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. 1995 Aug;222(2):120–127. doi: 10.1097/00000658-199508000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foley E. F., Schoetz D. J., Jr, Roberts P. L., Marcello P. W., Murray J. J., Coller J. A., Veidenheimer M. C. Rediversion after ileal pouch-anal anastomosis. Causes of failures and predictors of subsequent pouch salvage. Dis Colon Rectum. 1995 Aug;38(8):793–798. doi: 10.1007/BF02049833. [DOI] [PubMed] [Google Scholar]
- Fonkalsrud E. W. Long-term results after colectomy and ileoanal pull-through procedure in children. Arch Surg. 1996 Aug;131(8):881–886. doi: 10.1001/archsurg.1996.01430200091016. [DOI] [PubMed] [Google Scholar]
- Fonkalsrud E. W., Phillips J. D. Reconstruction of malfunctioning ileoanal pouch procedures as an alternative to permanent ileostomy. Am J Surg. 1990 Sep;160(3):245–251. doi: 10.1016/s0002-9610(06)80016-4. [DOI] [PubMed] [Google Scholar]
- Fonkalsrud E. W., Stelzner M., McDonald N. Construction of an ileal reservoir in patients with a previous straight endorectal ileal pull-through. Ann Surg. 1988 Jul;208(1):50–55. doi: 10.1097/00000658-198807000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fonkalsrud E. W. Total colectomy and endorectal ileal pull-through with internal ileal reservoir for ulcerative colitis. Surg Gynecol Obstet. 1980 Jan;150(1):1–8. [PubMed] [Google Scholar]
- Galandiuk S., Scott N. A., Dozois R. R., Kelly K. A., Ilstrup D. M., Beart R. W., Jr, Wolff B. G., Pemberton J. H., Nivatvongs S., Devine R. M. Ileal pouch-anal anastomosis. Reoperation for pouch-related complications. Ann Surg. 1990 Oct;212(4):446–454. doi: 10.1097/00000658-199010000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herbst F., Sielezneff I., Nicholls R. J. Salvage surgery for ileal pouch outlet obstruction. Br J Surg. 1996 Mar;83(3):368–371. doi: 10.1002/bjs.1800830324. [DOI] [PubMed] [Google Scholar]
- Kelly K. A. Anal sphincter-saving operations for chronic ulcerative colitis. Am J Surg. 1992 Jan;163(1):5–11. doi: 10.1016/0002-9610(92)90244-l. [DOI] [PubMed] [Google Scholar]
- Korsgen S., Nikiteas N., Ogunbiyi O. A., Keighley M. R. Results from pouch salvage. Br J Surg. 1996 Mar;83(3):372–374. doi: 10.1002/bjs.1800830325. [DOI] [PubMed] [Google Scholar]
- Liljeqvist L., Lindquist K. A reconstructive operation on malfunctioning S-shaped pelvic reservoirs. Dis Colon Rectum. 1985 Jul;28(7):506–511. doi: 10.1007/BF02554098. [DOI] [PubMed] [Google Scholar]
- McIntyre P. B., Pemberton J. H., Wolff B. G., Beart R. W., Dozois R. R. Comparing functional results one year and ten years after ileal pouch-anal anastomosis for chronic ulcerative colitis. Dis Colon Rectum. 1994 Apr;37(4):303–307. doi: 10.1007/BF02053588. [DOI] [PubMed] [Google Scholar]
- Nicholls R. J., Gilbert J. M. Surgical correction of the efferent ileal limb for disordered defaecation following restorative proctocolectomy with the S ileal reservoir. Br J Surg. 1990 Feb;77(2):152–154. doi: 10.1002/bjs.1800770212. [DOI] [PubMed] [Google Scholar]
- Ogunbiyi O. A., Korsgen S., Keighley M. R. Pouch salvage. Long-term outcome. Dis Colon Rectum. 1997 May;40(5):548–552. doi: 10.1007/BF02055376. [DOI] [PubMed] [Google Scholar]
- Poggioli G., Marchetti F., Selleri S., Laureti S., Stocchi L., Gozzetti G. Redo pouches: salvaging of failed ileal pouch-anal anastomoses. Dis Colon Rectum. 1993 May;36(5):492–496. doi: 10.1007/BF02050016. [DOI] [PubMed] [Google Scholar]
- Sagar P. M., Dozois R. R., Wolff B. G., Kelly K. A. Disconnection, pouch revision and reconnection of the ileal pouch-anal anastomosis. Br J Surg. 1996 Oct;83(10):1401–1405. doi: 10.1002/bjs.1800831025. [DOI] [PubMed] [Google Scholar]
- Stelzner M., Fonkalsrud E. W., Lichtenstein G. Significance of reservoir length in the endorectal ileal pullthrough with ileal reservoir. Arch Surg. 1988 Oct;123(10):1265–1268. doi: 10.1001/archsurg.1988.01400340091015. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., Jensen L., Rothenberger D. A., Wong W. D., Goldberg S. M. Long-term functional analysis of the ileoanal reservoir. Dis Colon Rectum. 1989 Apr;32(4):275–281. doi: 10.1007/BF02553479. [DOI] [PubMed] [Google Scholar]