

Abstract
BACKGROUND AND AIMS:
Cerebral aneurysms are a potentially life-threatening condition for humans. Due to the anatomical variability of different aneurysm types in human patients, animal models are indispensable for endovascular research. The aim of our study was to evaluate an endovascular aneurysm model in chronical experiments using 12 female Aachen minipigs.
MATERIALS AND METHODS:
For aneurysm creation in external carotid and subclavian arteries, Amplatzer vascular plugs were used as occlusion devices, leaving simple stumps that serve as surrogate aneurysms. If necessary and anatomically possible, additional embolic materials, such as coils and liquid embolic agents were used.
RESULTS:
We created 42 aneurysms. Aneurysm creation was possible without complications in all cases. There was no spontaneous thrombosis of fabricated aneurysms. Complete perfusion arrest behind the fabricated aneurysm was challenging but achieved in 45% of cases. We were not able to identify significant factors that have an impact on the persisting perfusion of fabricated aneurysms on final imaging, particularly not the presence of side branches in the aneurysm lumen (P = 0.734) or volumes of the fabricated aneurysms (P = 0.620). Albeit not significant, the use of additional occlusive measures (coils, liquid embolic agents) and antithrombotic drugs (ASA, heparin and tirofiban) may be factors for persisting perfusion: Perfusion arrest behind the fabricated aneurysm was twice as high in animals treated with ASA and heparin compared to animals treated with ASA, heparin, and tirofiban (48% vs. 22%; P = 0.149).
CONCLUSION:
Despite its limitations, including persistent perfusion and impaired predictability for long-term experiments, the endovascular aneurysm model shows potential to replace certain surgical models and offers broad applications in biomedical research and aneurysm therapy.
Keywords: Aachen minipig, endovascular animal model, external carotic artery, intracranial in vivo model, neuroradiology, subclavian artery
Introduction
Intracranial aneurysms are a potentially life-threatening condition for humans.[1,2] Globally, the prevalence of unruptured intracranial aneurysms in adults is estimated to range from 2% to 8%, although these patients do not necessarily have symptoms.[3,4,5] Intracranial aneurysms are considered to have a relatively low risk of rupture at 0.25%. Nevertheless, around 500,000 people worldwide die every year from ruptured aneurysms.[4] The most common clinical manifestation of ruptured aneurysms is subarachnoid hemorrhage, which can lead to considerable morbidity and mortality.[4,6,7]
The risk factors of aneurysm rupture are well studied and include morphological characteristics such as large aneurysm size, irregular shape, and anatomical locations (e.g., posterior circulation).[6,8,9,10] In addition, hemodynamic factors such as shear stress and blood flow patterns have been identified to play a crucial role in the risk of aneurysm rupture.[11,12] Furthermore, patient characteristics such as advanced age, female gender, the presence of hypertension, and family history of aneurysms can increase the risk of aneurysm formation and rupture.[8,13,14,15] The prognosis also depends on whether the aneurysm had already bled before.[16]
The treatment of aneurysms primarily involves two major intervention strategies: Surgical clipping and endovascular techniques, including coiling, stent-assisted coiling, and the use of flow-diverting stents. The decision between open surgical intervention and endovascular approaches for both ruptured and unruptured aneurysms remains a case-by-case decision.[17,18,19,20] Due to the diversity of aneurysm morphology in human patients, various treatment techniques and different devices are still subject of ongoing research. Aneurysm research is highly translational and encompasses methods, such as theoretical models, in vitro models, and in vivo animal models.[21,22,23] Table 1 shows a comparison of the advantages and disadvantages of selected aspects of different aneurysm models that are suitable for similar research purposes.
Table 1.
Comparison of different aneurysm models with the presented aneurysm model
| Criterion | Species, aneurysm model | ||
|---|---|---|---|
|
| |||
| Endovascular aneurysm model in pigs | Elastase model, rabbit | Surgical models (canine lateral wall, canine bifurcation, swine lateral wall)[32,33,34,35] | |
| Aneurysms per animal | 3–4 aneurysms per animal | 1 aneurysm per animal[30,36] | 1–2 aneurysms per animal |
| Invasiveness of aneurysm creation | Minimally invasive, endovascular | More invasive: combination of surgical and endovascular methods[36] | More invasive: surgical methods |
| Morbidity and mortality | Low | Severe complications such as tracheal necrosis and high mortality (8.4%)[36] | Not reported |
| Waiting period | Aneurysm ready for treatment after creation | Waiting period of 2 weeks after initial creation[36] | Waiting period of at least 3 weeks after initial creation |
| Suitability for chronic studies/patency of aneurysms | Limited | Good long-term stability[36] | Good |
| Reproducibility | High | High[37,38] | High |
| Area of application | Device testing and development, long-term studies, acute applications (e.g., training) | Device testing and development[37] | Device testing and development |
| Morphology | Tubular | Saccular, neck size can be adjusted[36] | Lateral side wall or bifurcation depending on the model |
Pigs are a common animal in vivo model because of their body size, hemodynamic coagulation parameters, and vessel anatomy that is comparable to humans.[24,25,26,27,28,29] Mühlenbruch et al.[21] have developed an easy-to-establish endovascular in vivo aneurysm model in pigs destined for acute trials. Their minimally invasive aneurysm model is low traumatic and immediately available, whereas the elastase model in rabbits or surgical models in other species is more traumatic and/or time-consuming.[30,31] The disadvantage of the endovascular model, however, is the sole use in acute trials until today and the lack of data for chronic experiments.[21]
The aim of our study was to evaluate this endovascular model in chronic experiments using Aachen minipigs, highlighting its potential for applications such as device testing and neurointerventional training. We evaluated the aneurysm model with respect to aneurysm creation and stability of the model at 6 months.
Materials and Methods
Experimental design and animals
For this study, 12 female adult Aachen minipigs (Gerd Heinrichs, Heinsberg-Karken, Deutschland; 45.95 kg ± 5.07 kg [mean ± SD]; age of 17–21 months) were used. Female minipigs were chosen because their anatomy allows urinary catheters to be inserted in a noninvasive manner. Of the 12 minipigs, 3 minipigs were assigned to acute trials and 9 to chronic trials. The objective was to create 3 aneurysms per pig that were subsequently treated. The 36 treated aneurysms were part of the larger project that is not subject to this analysis in its entirety. Whenever the anatomical conditions permitted, a fourth aneurysm was created as an untreated control in chronic trials. These additional cases are the basis for our chronic analyses. Hence, the aim was to create at least 36 aneurysms and at best 45 aneurysms. Initial angiography was performed in all 12 animals. In the 9 chronic experiments, another angiographic control was performed at the end of the experiment at 6 months. All minipigs were part of a more complex endovascular experiment, during which imaging data were collected and which is not subject to this analysis in its entirety.
Animal preparation and procedures
Animal housing, feeding, and anesthetic management were conducted as previously described. Animals were fasted the day before experimental angiography without deprivation of water. Euthanasia at the termination of experiments was also carried out as previously described.[39]
During initial angiography, animals of acute experiments were administered a dose of 500 mg ASA (Aspirin®, Bayer, Leverkusen, Germany) during general anesthesia and continuous rate infusion of tirofiban (Aggrastat, correvio, Puteaux, F) 0.4 μg/kg/min for 30 min, and subsequently 0.1 μg/kg/min during the remaining time of the intervention. Animals in chronic experiments were administered a dose of 500 mg ASA during general anesthesia. Subsequently, for all animals (acute and chronic) activated clotting time of more than 200 s was targeted, and heparin boluses were administered for this purpose using a dose range of 2000–5000 I.U. of heparin (after administration of ASA).
The animals of chronic groups received perioperative antibiosis (750 mg Cefuroxim, Hikma, London, England) and postoperative analgesia (Carprofen 4 mg/kg i.m., Rimadyl ad. us. vet., Zoetis Schweiz GmbH, Zürich, Switzerland). A daily dose of 100 mg ASA (Aspirin®, Bayer, Leverkusen, Germany) was administered orally for 21 days. During final angiographies, animals were administered heparin as described above.
Postinterventional severity assessment was performed through a predefined score sheet including humane endpoints. During the chronic course of experiments, no animal had to be excluded due to signs of illness. One animal presented transient lameness and symptomatic treatment was successful. All animals of chronic groups remained within the study until the planned endpoints of the chronic course.
Aneurysm creation
Artificial aneurysms were created as described by Mühlenbruch et al.[21] Target vessels were chosen based on their anatomic features and based on whether the collateral situation allowed occlusion without harm. Hence, different target vessels (A. carotis externa and side branches of Aa. subclaviae) were chosen individually in each animal for aneurysm creation. Furthermore, the decision of whether a fourth aneurysm was created depended on the individual anatomical configuration and collateralization.
Target vessels were reached using a 6-French Envoy XB catheter with an angled tip (Codman, Boston, US) supported by a guide wire 0.035’’ Radiofocus GuidewireM with hydrophilic coating (Terumo, Somerset, NJ). For actual aneurysm creation, Amplatzer vascular plugs (AVPs) were used to occlude target vessels, leaving simple stumps that serve as surrogate aneurysms. AVPs of type 4 and II (AGA Medical, Plymouth, MN) were inserted into selected target vessels. AVPs with a size of 4–5 mm for subclavian and 6–7 mm for external carotid arteries were used. This is illustrated in Figure 1.
Figure 1.
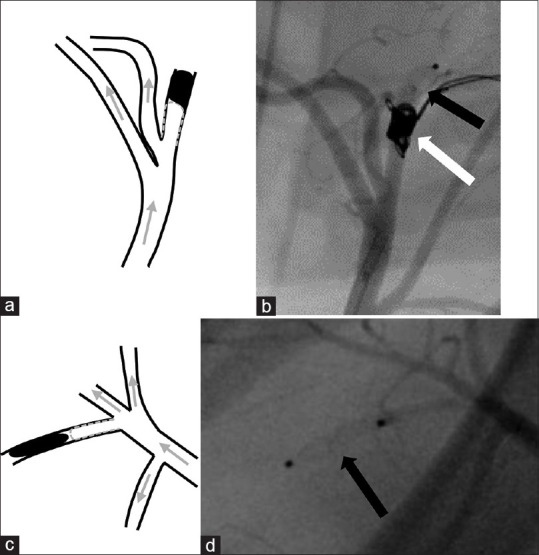
Endovascular creation of artificial aneurysms: Schematic drawings of the fabricated aneurysms on the left (a and c) and corresponding digital subtraction angiography images during initial experimental setup on the right (b and d). For aneurysm creation, Amplatzer vascular plugs (black arrow) were inserted into target vessels to create a vessel stump that serves as an artificial aneurysm. Porcine external carotid (a and b) and subclavian (c and d) arteries were used as target vessels. Additional coils were used in the first case (a and b) to ensure full target vessel occlusion (white arrow)
The patency of the parent vessel and the fabricated aneurysm was evaluated by angiography immediately after the aneurysm creation. If there was no perfusion arrest in the vessel behind the fabricated aneurysm, the aneurysm was controlled after 30–90 min. In case of persistent perfusion, additional measures for occlusion were taken: First, additional coils were used (Axiumnylon, Medtronic, Dublin, Ireland). If perfusion was still present, additional liquid embolic agents (Onyx 20 and Onyx 34, Medtronic, Minneapolis, USA) were used. If, due to anatomical configuration, the introduction of additional material would have filled the fabricated aneurysm, no escalation was performed. In selected cases, coiling was performed as a first step of aneurysm creation with subsequent placement of AVPs and possible escalation steps.
Our primary endpoint was successful aneurysm creation which was defined as a fabricated aneurysm without perfusion and without spontaneous thrombosis.
Image acquisition was performed using three different one-dimensional X-ray systems (Arcadis Avantic/Arcadis ORBIC, Siemens Healthcare GmbH, Erlangen, Germany; Ziehm Vision, Ziehm Imaging, Nürnberg, Germany). Iopamidol (Solutrast 300, 300 mg/mL; Bracco Imaging Deutschland GmbH, Konstanz, Germany) was administered as a contrast agent with a maximum dose of 5 mL/kg bodyweight through the femoral artery during digital subtraction angiography.
Statistical analysis
Data were tested for normal distribution using the Shapiro–Wilk test. Nonparametric data were presented as median and interquartile range (IQR). Fisher’s exact t-test was used for analyzing statistical differences in successful aneurysm creation rates in pigs with acute and chronic medical antithrombotic treatment, as well as aneurysms with and without side branches. Mann–Whitney U-test was performed to analyze the influence of aneurysm volumes on successful aneurysm creation. P values under the α-level of 0.05 were defined as significant. SPSS statistics 29 software (IBM, Armonk, NY, USA) was used for statistical analyses.
The sample size calculation of the superordinate study was based on effect size and expected complication rate and was considered less relevant for our current descriptive study, as we focused on aneurysm creation and long-term outcome. The other variables included in our analysis (e.g., medical treatment) were therefore not adjusted to the original sample size calculation. Although this limits the statistical power of these specific results, we believe that our study results can serve as an important basis for future studies.
Results
Aneurysm creation was possible without any complications (i.e., vessel perforation and dissection) and took a median time of 14 min (range: 7–36 min). We were able to create at least 3 aneurysms in all 12 animals and to create 6 additional chronic control aneurysms in 6 of these 12 animals. This resulted in an overall of 42 aneurysms to be included in our analysis. There was no spontaneous thrombosis of fabricated aneurysms.
On digital subtraction angiography, aneurysm sizes ranged in diameter from 2.1 mm to 5.9 mm (median, 3.3 mm; IQR: 2.7–3.9 mm) and in length from 3.8 mm to 25.2 mm (median, 10.0 mm; IQR: 9.8–10.0 mm). Aneurysm sizes in the subclavian arteries ranged in diameter from 2.1 mm to 3.9 mm (median: 2.9 mm; IQR: 2.7–3.4 mm) and in length from 3.8 mm to 13.5 mm (median: 10.0 mm; IQR: 10.0–10.0 mm). Aneurysm sizes in the carotid arteries ranged in diameter from 3.7 mm to 5.3 mm (median: 4.3 mm; IQR: 3.9–5.3 mm) and in length from 6.0 mm to 25.2 mm (median: 10.0 mm; IQR, 7.3–10.0 mm). The aneurysm volume was determined based on the length and diameter of the aneurysms with a median of 75.5 mm (IQR: 57.3–122.5 mm). The aneurysm volume had no statistically significant influence on the rate of successful aneurysm creation on final imaging (P = 0.620).
Of the 42 aneurysms, immediate perfusion arrest after AVP implantation was observed in 11/42 (26%) cases on initial angiography, whereas 31/42 (74%) fabricated aneurysms were still perfused. Escalation of aneurysm creation with additional coils and/or liquid embolic agents (Onyx) was possible in 12/31 (39%) cases. In 2 of these 12 cases, the methodological order of aneurysm creation was changed, with coils being implanted before the AVP and additional embolization with Onyx due to anatomical vessel configuration. In 8/12 cases (67%), additional coiling and/or liquid embolic agents allowed for aneurysm creation without persistent perfusion. In the remaining 4/12 (33%), there was persistent perfusion of the fabricated aneurysm. In the remaining 19 of 31 cases (61%) without initial perfusion arrest, further escalation was not possible, because this was expected to lead to complete occlusion of the aneurysm. Full results are listed in the supporting information file (Supplementary Table 1 Overview of all aneurysms on initial angiography).
Supplementary Table 1.
Overview of all aneurysms on initial and final angiography
| Animal number | Aneurysm number | Occlusion type | Additional coiling | Additional liquid embolic agents (onyx) | Location/artery | Length of aneurysm (mm) | Vessel size (mm) | Perfused side branch | Successful aneurysm creation | Perfusion arrest distal to AVP (initial) 1st angiography | Perfusion arrest distal to AVP (final) | Spon-taneous throm-bosis (initial angio-graphy) | Spon-taneous throm-bosis (final angio-graphy) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||||
| Aneurysms for treatment | |||||||||||||
| 1 | 1 | AVP II | No | No | A. subcl. dextra | 3.8 | 3.7 | Yes | Yes | Yes | NA | No | NA |
| 1 | 2 | AVP 4 | No | No | A. subcl. sinistra | 11.0 | 5.7 | Yes | Yes | No | NA | No | NA |
| 1 | 3 | AVP 4 | No | No | A. carotis dextra | 25.2 | 5.9 | No | Yes | No | NA | No | NA |
| 2 | 4 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 2.7 | No | Yes | No | NA | No | NA |
| 2 | 5 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 2.7 | No | Yes | No | NA | No | NA |
| 2 | 6 | AVP 4 | No | No | A. carotis dextra | 8.0 | 4.0 | Yes | Yes | No | NA | No | NA |
| 3 | 7 | AVP 4 | No | No | A subcl. dextra | 10.0 | 2.3 | No | Yes | No | NA | No | NA |
| 3 | 8 | AVP 4 | Yes | No | A subcl. sinistra | 8.0 | 3.2 | No | Yes | No | NA | No | NA |
| 3 | 9 | AVP 4 | Yes | No | A. carotis sinistra | 7.0 | 3.9 | Yes | Yes | Yes | NA | No | NA |
| 4 | 10 | AVP 4 | Yes | No | A. subcl. dextra | 10.0 | 3.5 | Yes | Yes | No | NA | No | NA |
| 4 | 11 | AVP4 | Yes | No | A. subcl. sinistra | 11.0 | 3.4 | No | Yes | Yes | NA | No | NA |
| 4 | 12 | AVP 4 | No | No | A. carotis sinistra | 10.0 | 5.4 | No | Yes | No | NA | No | NA |
| 5 | 13 | AVP 4 | No | No | A. subcl. dextra | 13.5 | 3.8 | No | Yes | Yes | NA | No | NA |
| 5 | 14 | AVP 4 | No | No | A. subcl. sinistra | 11.0 | 3.4 | No | Yes | No | NA | No | NA |
| 5 | 15 | AVP 4 | Yes | No | A. carotis sinistra | 6.5 | 5.6 | No | Yes | Yes | NA | No | NA |
| 6 | 16 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 3.2 | No | Yes | No | NA | No | NA |
| 6 | 17 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 3.5 | No | Yes | No | NA | No | NA |
| 6 | 18 | AVP 4 | Yes | No | A. carotis sinistra | 10.0 | 4.1 | Yes | Yes | Yes | NA | No | NA |
| 7 | 19 | AVP 4 | No | No | A. subcl. dextra | 7.0 | 2.8 | No | Yes | Yes | NA | No | NA |
| 7 | 20 | AVP 4 | No | No | A. subcl. sinistra | 6.6 | 2.7 | Yes | Yes | No | NA | No | NA |
| 7 | 21 | AVP 4 | Yes | No | A. carotis sinistra | 6.0 | 3.7 | No | Yes | Yes | NA | No | NA |
| 8 | 22 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 2.8 | No | Yes | No | NA | No | NA |
| 8 | 23 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 2.8 | No | Yes | No | NA | No | NA |
| 8 | 24 | AVP 4 | No | No | A. carotis sinistra | 10.0 | 4.0 | No | Yes | Yes | NA | No | NA |
| 9 | 25 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 3.1 | No | Yes | No | NA | No | NA |
| 9 | 26 | AVP 4 | No | No | A. subcl. sinistra | 9.0 | 2.9 | No | Yes | No | NA | No | NA |
| 9 | 27 | AVP 4 | Yes | No | A. carotis sinistra | 10.0 | 4.5 | No | Yes | Yes | NA | No | NA |
| 10 | 28 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 2,7 | No | Yes | No | NA | No | NA |
| 10 | 29 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 3.0 | No | Yes | No | NA | No | NA |
| 10 | 30 | AVP 4 | Yes | No | A. carotis sinistra | 10.7 | 3.8 | No | Yes | Yes | NA | No | NA |
| 11 | 31 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 3.1 | No | Yes | Yes | NA | No | NA |
| 11 | 32 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 3.0 | No | Yes | Yes | NA | No | NA |
| 11 | 33 | AVP 4 | Yes | Yes | A. carotis dextra | 10.0 | 5.0 | No | Yes | Yes | NA | No | NA |
| 12 | 34 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 3.4 | No | Yes | No | NA | No | NA |
| 12 | 35 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 3.3 | Yes | Yes | No | NA | No | NA |
| 12 | 36 | AVP 4 | No | No | A. carotis dextra | 10.0 | 4.8 | No | Yes | No | NA | No | NA |
|
| |||||||||||||
| Chronic aneurysms | |||||||||||||
|
| |||||||||||||
| 7 | 37 | AVP 4 | No | No | A. subcl. sinistra | 11.5 | 2.5 | No | Yes | Yes | No | No | No |
| 8 | 38 | AVP 4 | No | No | A. subcl. dextra | 7.2 | 2.5 | No | Yes | No | No | No | No |
| 9 | 39 | AVP 4 | No | No | A. subcl. sinistra | 11.9 | 2.6 | No | Yes | Yes | No | No | No |
| 10 | 40 | AVP 4 | No | No | A. subcl. dextra | 10.0 | 2.1 | No | Yes | Yes | No | No | No |
| 11 | 41 | AVP 4 | No | No | A. subcl. dextra | 7.0 | 2.2 | No | Yes | No | Yes | No | No |
| 12 | 42 | AVP 4 | No | No | A. subcl. sinistra | 10.0 | 2.5 | No | Yes | Yes | Yes | No | No |
AVP: Amplatzer vascular plug, NA: Spontaneous thrombosis was not applicable in treated aneurysms
Of the 6 chronic aneurysms, perfusion arrest behind the fabricated aneurysm was observed in 4/6 (67%) cases on initial angiography, whereas 2/6 (33%) aneurysms remained perfused with reduced blood flow. Final angiography after 6 months showed occlusion behind the fabricated aneurysm in 2/6 (33%), whereas there was persistent blood flow behind the fabricated aneurysm in 4/6 (67%) cases. These results are illustrated in Table 2 and Figure 2.
Table 2.
Overview of all untreated aneurysms on initial and final angiography
| Aneurysm number | Additional coiling/liquid embolic agents (onyx) | Location/artery | Length of aneurysm (mm) | Vessel size (mm) | Successful aneurysm creation | Perfusion arrest distal to AVP (initial) 1st angiography | Perfusion arrest distal to AVP (final) | Spontaneous thrombosis (initial angio-graphy) | Spontaneous thrombosis (final angio-graphy) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | No | A. subcl. sinistra | 11.5 | 2.5 | Yes | Yes | No | No | No |
| 2 | No | A. subcl. dextra | 7.2 | 2.5 | Yes | No | No | No | No |
| 3 | No | A. subcl. sinistra | 11.9 | 2.6 | Yes | Yes | No | No | No |
| 4 | No | A. subcl. dextra | 10.0 | 2.1 | Yes | Yes | No | No | No |
| 5 | No | A. subcl. dextra | 7.0 | 2.2 | Yes | No | Yes | No | No |
| 6 | No | A. subcl. sinistra | 10.0 | 2.5 | Yes | Yes | Yes | No | No |
AVP: Amplatzer vascular plug
Figure 2.
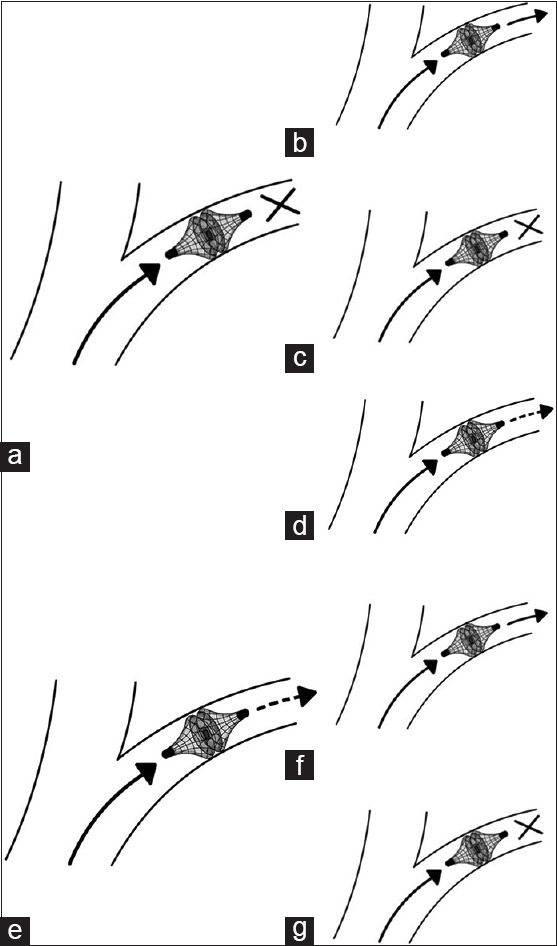
Schematic drawing of the evolution of aneurysms during the chronic course: The six chronic aneurysms showed different initial and final outcomes. (a) Depicts a full perfusion arrest behind the aneurysm on initial experimental imaging, which yielded three different outcomes at angiography after 6 months: (b) Re-perfusion, (c) complete perfusion arrest, and (d) incomplete perfusion arrest. (e) Depicts persisting perfusion after the aneurysm on initial experimental imaging, which yielded two different outcomes at angiography after 6 months: (f) Re-perfusion and (g) complete perfusion arrest
The long-term evolution of the 6 aneurysms in the chronic experiments is illustrated in Figure 3 and was as follows: In 1/6 (17%) cases, there was perfusion arrest of the vessel behind the fabricated aneurysm on initial and final angiography at 6 months. In 1/6 (17%) cases, there was perfusion arrest in the vessel behind the fabricated aneurysm on initial angiography and re-perfusion with slight blood flow behind the fabricated aneurysm on final angiography at 6 months. In 2/6 (33%) cases, there was perfusion arrest in the vessel behind the fabricated aneurysm on initial angiography and re-perfusion with normal blood flow behind the fabricated aneurysm on final angiography at 6 months. In 1/6 (17%) cases, there was reduced blood flow in the vessel behind the fabricated aneurysm on initial angiography and an increase of perfusion with normal blood flow on final angiography at 6 months. In 1/6 (17%) cases, there was reduced blood flow behind the fabricated aneurysm on initial angiography and complete perfusion arrest behind the fabricated aneurysm on final imaging at 6 months.
Figure 3.

Angiographic outcomes of chronic aneurysms during initial and final angiographies: a-d: Schematic drawing of a fabricated aneurysm in the left subclavian artery with complete perfusion arrest on initial imaging (a and b) and 6-month follow-up (c and d). (a and c) represent schematic drawings of the corresponding angiography images (b and d). e-h: Schematic drawing of a fabricated aneurysm in the left subclavian artery with perfusion on initial imaging (e and f) and 6-month follow-up (c and d). (e and g) represent schematic drawings of the corresponding angiography images (f and h)
Functional side branches were defined as vessels that originated from the lumen of the fabricated aneurysm and that had blood flow. Of the 42 created aneurysms, 8/42 (19%) had functional side branches. Of these 8 aneurysms with side branches, there was perfusion arrest in the vessel behind the fabricated aneurysm in 3/8 (38%) and there was persistent blood flow behind the fabricated aneurysm in the remaining 5/8 (62%) cases. There were 34/42 (81%) aneurysms without functional side branches. Of these 34 aneurysms without side branches, there was perfusion arrest in the vessel behind the fabricated aneurysm in 15/34 (44%) cases and there was persistent blood flow behind the fabricated aneurysm in the remaining 19/34 (56%) cases. These rates did not differ significantly on final imaging between aneurysms with and without functional side branches (P = 0.734).
There were no side branches in the 6 chronic aneurysms. Of these 6 aneurysms, there were 4 aneurysms with initially complete perfusion arrest of the vessel behind the fabricated aneurysm; 3 of these 4 aneurysms had re-perfusion on follow-up at 6 months.
The 3 animals undergoing acute experiments received antithrombotic medication consisting of ASA, tirofiban, and heparin. Of the 9 aneurysms in these 3 animals, there was perfusion arrest in the vessel behind the fabricated aneurysm in 2/9 (22%) cases and there was persistent blood flow behind the fabricated aneurysm in the remaining 7/9 (78%) cases. The 9 animals undergoing chronic experiments received antithrombotic medication consisting of ASA and heparin. Of the 33 aneurysms in these 9 animals, there was perfusion arrest in the vessel behind the fabricated aneurysm in 16/33 (48%) cases and there was persistent blood flow behind the fabricated aneurysm in the remaining 17/33 (52%) cases. These rates did not differ significantly between aneurysms in acute and chronic settings (P = 0.149).
Discussion
An endovascular aneurysm model should be easy to create, yield aneurysms without spontaneous thrombosis, especially in chronic trials, and be reproducible. In our study, aneurysm creation using the methodology described by Mühlenbruch et al. was generally possible and relatively simple for experienced neurointerventionalists.[21] There was no spontaneous thrombosis within the fabricated aneurysm, which we interpret as a positive result.
The aim of Mühlenbruch et al. was to occlude a vessel in an acute trial using an AVP, leaving a simple stump that serves as a surrogate aneurysm and is embolized during endovascular training or for research purposes. In our study, however, the creation of an aneurysm without blood flow in the subsequent vessel was challenging but could be achieved in 19/42 (45%) of the aneurysms. Perfusion arrest was possible with an AVP alone as proposed by Mühlenbruch et al. in 11/42 (26%) cases.[21] Escalation with additional procedures for perfusion arrest (coils, liquid embolic agents) was anatomically and physiologically possible in 12 of the remaining 31 (39%) cases and yielded perfusion arrest in 8 of these 12 cases (67%). Interestingly, there was no persistent perfusion behind the occlusive devices in 10/12 (83%) carotid arteries, in which we applied additional occlusive measures, underlining the importance of additional occlusive measures.
A major finding of our study is the high variability of long-term angiographic outcomes in such fabricated aneurysms. The natural history of our 6 chronic aneurysms was difficult to predict: Of the 4 aneurysms with initially complete perfusion arrest, 1 remained occluded after 6 months, whereas there was complete vessel re-perfusion in 2 cases and partial vessel re-perfusion in the remaining 1 case. Of the 2 aneurysms with initially incomplete perfusion arrest, one showed perfusion arrest after 6 months, whereas the other showed persistent perfusion. Persistent perfusion of the vessel behind the aneurysm was already observed by Mühlenbruch et al. and is not necessarily a disadvantage in acute trials and training.[21] However, persistent perfusion and reduced long-term predictability may pose a challenge for long-term experiments.
Mühlenbruch et al. suggested that side branches within the fabricated aneurysmal lumen contribute to incomplete perfusion arrest.[21] The authors reported on two aneurysms that had side branches, in which perfusion arrest behind the fabricated aneurysm could not be achieved. In our experiment, there was a slightly, statistically nonsignificantly, higher rate of perfusion arrest in the vessel behind the fabricated aneurysm of 44% (15/34) in aneurysms without side branches compared to 38% (3/8) in aneurysms with side branches. Hence, our results did not confirm that perfused side branches within the fabricated aneurysm lumen contribute to a significantly higher rate of perfusion. Notably, there was perfusion arrest behind fabricated aneurysm in 3 of 8 aneurysms with side branches, underlining the above-mentioned complex and to some degree difficult to predict the course of such fabricated aneurysms.
We hypothesized that successful aneurysm creation may depend on the size of the fabricated aneurysm, but it was found that aneurysm volume had no statistically significant impact. We do not have a sufficient explanation for this result. One possible explanation is that there are opposing effects: Larger aneurysms in larger vessels have a higher potential blood flow, but here the occlusion can also be escalated more easily. In smaller vessels, on the other hand, the blood flow is lower, but the occlusion cannot be escalated as easily. This underlines the difficulty of predicting the evolution of fabricated aneurysms.
Another important factor which may influence successful aneurysm creation is antithrombotic drugs, such as ASA, heparin, and tirofiban. In human patients, the use of ASA and heparin is known as a mild antithrombotic treatment in patients with endovascular implants.[40,41] The combination of ASA and heparin has been used in the study of Mühlenbruch et al. in the first three animals. Surprisingly, this resulted in a relatively high rate of 43% (3/7) of fabricated aneurysms with persistent perfusion behind the occlusion device.[21] We used a slightly different antithrombotic protocol in our acute trials with a standard medication consisting of ASA, heparin, and additionally tirofiban to reduce the risk of thrombosis. Under this protocol, 78% (7/9) of the aneurysms in acute trials showed persistent perfusion behind the occlusion device. Because of this high rate of perfused aneurysms, we limited antithrombotic medication for our chronic trials to ASA and heparin. This resulted in a lower rate of 52% (17/33) aneurysms with persistent perfusion behind the occlusion device. These results are comparable to those reported by Mühlenbruch et al. and underline the role of antithrombotic medication for this endovascular aneurysm model.[21] The high rate of arteries that were still perfused, partly despite the use of additional coils and endovascular embolic fluids, was surprising. In our study, the rate of persistent perfusion was lower with ASA and heparin therapy than with additional administration of tirofiban. Although the difference in our study did not reach statistical significance, our results suggest that further reduction of antithrombotic therapy, for example, to heparin monotherapy or no therapy at all, may contribute to an even lower rate of persistent perfusion behind the occlusion device.
In summary, the presented model is much easier to create than other surgical models. The endovascular methodology allows to create artificial aneurysms that can be used directly for experimental purposes, which is beneficial for endovascular training purposes and device testing studies. Another advantage of our method is that aneurysms can be created at many different anatomical locations. This represents a considerable benefit, particularly if aneurysm creation at a specific location is required to optimize its evaluation through additional diagnostic techniques. Finally, the high tolerability of the model compared to other models, such as the elastase model in the rabbit, is a substantial advantage, especially in long-term device testing studies.
Limitations
Persistent perfusion and impaired long-term predictability are challenges of the endovascular aneurysm model for long-term experiments. Furthermore, persistent perfusion limits the models’ suitability for studying fluid dynamics. If an experiment requires aneurysms that are not perfused and have a certain degree of stasis in their lumen, the model must be improved. From our experience, possible approaches are additional occlusion procedures such as the additional use of coils and liquid embolic agents. Another option would be to perform the aneurysm creation in a single intervention. After a waiting period of several weeks, the created aneurysms could then be angiographically examined for persistent perfusion and possibly further occluded or treated. An alternative starting point for optimizing the current aneurysm model is the choice of an appropriate antithrombotic treatment. The treatment regime with ASA and heparin resulted in lower persistent perfusion rates of created aneurysms than the treatment with ASA, heparin, and tirofiban. Further reduction of medication could be a possible strategy to lower the perfusion rate. In our opinion, studies with larger numbers of cases and more specific trial designs are required to investigate this issue. However, these measures are associated with an increased risk of unintentional vascular occlusion and potentially reduced perfusion. While this is not a problem in acute trials, in chronic trials the long-term effects of these measures on animal welfare must be given greater consideration. Therefore, in chronic experiments, the creation of such aneurysms always remains a case-by-case decision that must take anatomical and physiological circumstances into account.
Furthermore, the current model is limited to the creation of tubular aneurysms, lacking the capability to generate other morphologies, such as berry-shaped aneurysms. Furthermore, it does not simulate the natural pathogenesis of aneurysms, including the development of a fragile aneurysm wall. This is why we did not apply additional outcome parameters, such as computational fluid dynamics, as these techniques are particularly useful for investigating the risk of aneurysm rupture.[42,43] Finally, the aneurysm dome consists of endovascular material, so endothelial growth within the complete aneurysmal lumen is not achievable during the procedure of endovascular aneurysm creation. If complete endothelial growth is needed for specific research questions, it takes a couple of months.[44]
These limitations are all inherent to the endovascular approach, which in turn has the advantage that it is less invasive than surgical models and easy to perform. This results in an overall high tolerability for the animals, which is in accordance with the 3Rs (Replacement, Reducement, and Refinement) of Russell and Burch.[45]
Conclusion
When anticipating and respecting the limitations of the model, the proposed endovascular aneurysm model described in our study has the potential to replace certain surgical models and offers a wide range of applications in biomedical research and aneurysm therapy.
Author contributions
Conceptualization: LB, RM, MW, ON, CF; Data curation: LB, CD, RM, ON, CF; Formal analysis: LB, RM, MW, ON, CF; Funding aquisition: MW; Investigation: LB, TS, JM, CD, RM, CSW, DH, AS, HR, MW, ON, CF; Project administration: AS; Ressources: LB, TS, JM, CF; Supervision: RM, MW, AS, ON, CF; Visualisation: LB, TS, MW, ON, CF; Writing – original draft: LB; Writing – review & editing: LB, TS, JM, CD, RM, CSW, DH, AS, HR, MW, ON, CF.
Animal experimentation approval
The study was performed in accordance with the German Animal Welfare Act and EU Directive 2010/63/EU. The experimental protocol was granted by the Landesamt für Natur, Umwelt und Verbraucherschutz (LANUV) Nordrhein-Westfalen, Recklinghausen, Germany, under approval number AZ-81-02.04.2019A.412, dated on April 14th, 2020. Animal housing conditions complied with the requirements of Annex III of the EU Directive 2010/63/EU and the Annex of the European Agreement of March 18, 1986. Institutional guidelines regarding animal welfare and experimentation were followed.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of interest
Martin Wiesmann has the following disclosures: Consultancy: Stryker; Payment for lectures: Bracco, Medtronic, Siemens, Stryker; Educational Presentations: Bracco, Codman, Medtronic, Phenox, Siemens; has received grants for research projects or educational exhibits from Ab medica, Acandis, Bracco Imaging, Cerenovus, Kaneka Pharmaceuticals, Medtronic, Mentice AB, Microvention, Phenox, Siemens Healthcare and Stryker Neurovascular.
Omid Nikoubashman has the following disclosures: Grants: Stryker; Payment for lectures: Stryker, Phenox, and Werfen.
Hani Ridwan has the following disclosures: Consultancy: ThrombX Medical Inc.
Funding Statement
This work was funded by EFRE NRW 2014-2020 (Leitmarkt.Agentur NRW) through the project IANIS - Intraaneurysmales Implantat mit flussmodulierenden Eigenschaften (funding ID: EFRE-0801324, LS-2-01-012e).
References
- 1.Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms. Brain. 2000;123(( Pt 2)(2)):205–21. doi: 10.1093/brain/123.2.205. [DOI] [PubMed] [Google Scholar]
- 2.GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20:795–820. doi: 10.1016/S1474-4422(21)00252-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011;10:626–36. doi: 10.1016/S1474-4422(11)70109-0. [DOI] [PubMed] [Google Scholar]
- 4.Toth G, Cerejo R. Intracranial aneurysms: Review of current science and management. Vasc Med. 2018;23:276–88. doi: 10.1177/1358863X18754693. [DOI] [PubMed] [Google Scholar]
- 5.Brinjikji W, Zhu YQ, Lanzino G, Cloft HJ, Murad MH, Wang Z, et al. Risk factors for growth of intracranial aneurysms: A systematic review and meta-analysis. AJNR Am J Neuroradiol. 2016;37:615–20. doi: 10.3174/ajnr.A4575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Duan Z, Li Y, Guan S, Ma C, Han Y, Ren X, et al. Morphological parameters and anatomical locations associated with rupture status of small intracranial aneurysms. Sci Rep. 2018;8:6440. doi: 10.1038/s41598-018-24732-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007;369:306–18. doi: 10.1016/S0140-6736(07)60153-6. [DOI] [PubMed] [Google Scholar]
- 8.Kleinloog R, de Mul N, Verweij BH, Post JA, Rinkel GJ, Ruigrok YM. Risk factors for intracranial aneurysm rupture: A systematic review. Neurosurgery. 2018;82:431–40. doi: 10.1093/neuros/nyx238. [DOI] [PubMed] [Google Scholar]
- 9.Jirjees S, Htun ZM, Aldawudi I, Katwal PC, Khan S. Role of morphological and hemodynamic factors in predicting intracranial aneurysm rupture: A review. Cureus. 2020;12:e9178. doi: 10.7759/cureus.9178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zheng Y, Xu F, Ren J, Xu Q, Liu Y, Tian Y, et al. Assessment of intracranial aneurysm rupture based on morphology parameters and anatomical locations. J Neurointerv Surg. 2016;8:1240–6. doi: 10.1136/neurintsurg-2015-012112. [DOI] [PubMed] [Google Scholar]
- 11.Xiang J, Yu J, Choi H, Dolan Fox JM, Snyder KV, Levy EI, et al. Rupture Resemblance Score (RRS): Toward risk stratification of unruptured intracranial aneurysms using hemodynamic-morphological discriminants. J Neurointerv Surg. 2015;7:490–5. doi: 10.1136/neurintsurg-2014-011218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Leemans EL, Cornelissen BM, Slump CH, Majoie CB, Cebral JR, Marquering HA. Comparing morphology and hemodynamics of stable-versus-growing and grown intracranial aneurysms. AJNR Am J Neuroradiol. 2019;40:2102–10. doi: 10.3174/ajnr.A6307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jiranukool J, Thiarawat P, Galassi W. Prevalence of intracranial aneurysms among acute ischemic stroke patients. Surg Neurol Int. 2020;11:341. doi: 10.25259/SNI_506_2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Backes D, Rinkel GJ, Laban KG, Algra A, Vergouwen MD. Patient- and aneurysm-specific risk factors for intracranial aneurysm growth: A systematic review and meta-analysis. Stroke. 2016;47:951–7. doi: 10.1161/STROKEAHA.115.012162. [DOI] [PubMed] [Google Scholar]
- 15.Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors: A prospective Finnish cohort study. Stroke. 2014;45:1958–63. doi: 10.1161/STROKEAHA.114.005318. [DOI] [PubMed] [Google Scholar]
- 16.Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet. 2002;360:1267–74. doi: 10.1016/s0140-6736(02)11314-6. [DOI] [PubMed] [Google Scholar]
- 17.Sheth SA, Sanossian N, Hao Q, Starkman S, Ali LK, Kim D, et al. Collateral flow as causative of good outcomes in endovascular stroke therapy. J Neurointerv Surg. 2016;8:2–7. doi: 10.1136/neurintsurg-2014-011438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zijlstra IA, Verbaan D, Majoie CB, Vandertop P, van den Berg R. Coiling and clipping of middle cerebral artery aneurysms: A systematic review on clinical and imaging outcome. J Neurointerv Surg. 2016;8:24–9. doi: 10.1136/neurintsurg-2014-011478. [DOI] [PubMed] [Google Scholar]
- 19.Jindal G, Miller T, Beaty N, Puri A, Gandhi D. Ultra-small diameter coils for treatment of intracranial aneurysms. Interv Neuroradiol. 2015;21:50–4. doi: 10.15274/INR-2014-10105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Seibert B, Tummala RP, Chow R, Faridar A, Mousavi SA, Divani AA. Intracranial aneurysms: Review of current treatment options and outcomes. Front Neurol. 2011;2:45. doi: 10.3389/fneur.2011.00045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mühlenbruch G, Nikoubashman O, Steffen B, Dadak M, Palmowski M, Wiesmann M. Endovascular broad-neck aneurysm creation in a porcine model using a vascular plug. Cardiovasc Intervent Radiol. 2013;36:239–44. doi: 10.1007/s00270-012-0431-z. [DOI] [PubMed] [Google Scholar]
- 22.Sandmann J, Müschenich FS, Riabikin A, Kramer M, Wiesmann M, Nikoubashman O. Can silicone models replace animal models in hands-on training for endovascular stroke therapy? Interv Neuroradiol. 2019;25:397–402. doi: 10.1177/1591019919833843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kaiser EE, West FD. Large animal ischemic stroke models: Replicating human stroke pathophysiology. Neural Regen Res. 2020;15:1377–87. doi: 10.4103/1673-5374.274324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Schwartz RS, Edelman ER, Carter A, Chronos NA, Rogers C, Robinson KA, et al. Preclinical evaluation of drug-eluting stents for peripheral applications: Recommendations from an expert consensus group. Circulation. 2004;110:2498–505. doi: 10.1161/01.CIR.0000145164.85178.2E. [DOI] [PubMed] [Google Scholar]
- 25.Dondelinger RF, Ghysels MP, Brisbois D, Donkers E, Snaps FR, Saunders J, et al. Relevant radiological anatomy of the pig as a training model in interventional radiology. Eur Radiol. 1998;8:1254–73. doi: 10.1007/s003300050545. [DOI] [PubMed] [Google Scholar]
- 26.Mathern N, Yousefian E, Ridwan H, Nikoubashman O, Wiesmann M. Comparison of porcine and human vascular diameters for the optimization of interventional stroke training and research. PLoS One. 2022;17:e0268005. doi: 10.1371/journal.pone.0268005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dorn C, Bender L, Sichtermann T, Minkenberg J, Franko M, Yousefian E, et al. Comparison of artery diameters in the Aachen minipig serving as a human intracranial in vivo model. Lab Anim. 2024;58:65–72. doi: 10.1177/00236772231169809. [DOI] [PubMed] [Google Scholar]
- 28.Herrmann AM, Meckel S, Gounis MJ, Kringe L, Motschall E, Mülling C, et al. Large animals in neurointerventional research: A systematic review on models, techniques and their application in endovascular procedures for stroke, aneurysms and vascular malformations. J Cereb Blood Flow Metab. 2019;39:375–94. doi: 10.1177/0271678X19827446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.von Trotha KT, Butz N, Grommes J, Binnebösel M, Charalambakis N, Mühlenbruch G, et al. Vascular anatomy of the small intestine-a comparative anatomic study on humans and pigs. Int J Colorectal Dis. 2015;30:683–90. doi: 10.1007/s00384-015-2163-4. [DOI] [PubMed] [Google Scholar]
- 30.Thiex R, Hans FJ, Krings T, Möller-Hartmann W, Brunn A, Scherer K, et al. Haemorrhagic tracheal necrosis as a lethal complication of an aneurysm model in rabbits via endoluminal incubation with elastase. Acta Neurochir (Wien) 2004;146:285–9. doi: 10.1007/s00701-003-0198-8. [DOI] [PubMed] [Google Scholar]
- 31.Villano JS, Boehm CA, Carney EL, Cooper TK. Complications of elastase-induced arterial saccular aneurysm in rabbits: Case reports and literature review. Comp Med. 2012;62:480–6. [PMC free article] [PubMed] [Google Scholar]
- 32.Cruise GM, Shum JC, Plenk H. Hydrogel-coated and platinum coils for intracranial aneurysm embolization compared in three experimental models using computerized angiographic and histologic morphometry. J Mater Chem. 2007;17:3965–73. [Google Scholar]
- 33.Raymond J, Berthelet F, Desfaits AC, Salazkin I, Roy D. Cyanoacrylate embolization of experimental aneurysms. AJNR Am J Neuroradiol. 2002;23:129–38. [PMC free article] [PubMed] [Google Scholar]
- 34.Raymond J, Darsaut T, Salazkin I, Gevry G, Bouzeghrane F. Mechanisms of occlusion and recanalization in canine carotid bifurcation aneurysms embolized with platinum coils: An alternative concept. AJNR Am J Neuroradiol. 2008;29:745–52. doi: 10.3174/ajnr.A0902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Raymond J, Desfaits AC, Roy D. Fibrinogen and vascular smooth muscle cell grafts promote healing of experimental aneurysms treated by embolization. Stroke. 1999;30:1657–64. doi: 10.1161/01.str.30.8.1657. [DOI] [PubMed] [Google Scholar]
- 36.Brinjikji W, Ding YH, Kallmes DF, Kadirvel R. From bench to bedside: Utility of the rabbit elastase aneurysm model in preclinical studies of intracranial aneurysm treatment. J Neurointerv Surg. 2016;8:521–5. doi: 10.1136/neurintsurg-2015-011704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ding YH, Dai D, Lewis DA, Danielson MA, Kadirvel R, Cloft HJ, et al. Long-term patency of elastase-induced aneurysm model in rabbits. AJNR Am J Neuroradiol. 2006;27:139–41. [PMC free article] [PubMed] [Google Scholar]
- 38.Wang Y, Ma C, Xu N, Xu K, Wang H, Yu J, et al. An improved elastase-based method to create a saccular aneurysm rabbit model. Br J Neurosurg. 2013;27:779–82. doi: 10.3109/02688697.2013.799633. [DOI] [PubMed] [Google Scholar]
- 39.Franz C, Bender L, Dorn C, Sichtermann T, Minkenberg J, Franko M, et al. Platelet function testing using the multiplate analyzer after administration of aspirin in Aachen minipigs. PLoS One. 2022;17:e0275756. doi: 10.1371/journal.pone.0275756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Neuberger U, Moteva K, Vollherbst DF, Schönenberger S, Reiff T, Ringleb PA, et al. Tandem occlusions in acute ischemic stroke –Impact of antithrombotic medication and complementary heparin on clinical outcome and stent patency. J Neurointerv Surg. 2020;12:1088–93. doi: 10.1136/neurintsurg-2019-015596. [DOI] [PubMed] [Google Scholar]
- 41.Robertson L, Ghouri MA, Kovacs F. Antiplatelet and anticoagulant drugs for prevention of restenosis/reocclusion following peripheral endovascular treatment. Cochrane Database Syst Rev. 2012;2012:CD002071. doi: 10.1002/14651858.CD002071.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Murayama Y, Fujimura S, Suzuki T, Takao H. Computational fluid dynamics as a risk assessment tool for aneurysm rupture. Neurosurg Focus. 2019;47:E12. doi: 10.3171/2019.4.FOCUS19189. [DOI] [PubMed] [Google Scholar]
- 43.Fukazawa K, Ishida F, Umeda Y, Miura Y, Shimosaka S, Matsushima S, et al. Using computational fluid dynamics analysis to characterize local hemodynamic features of middle cerebral artery aneurysm rupture points. World Neurosurg. 2015;83:80–6. doi: 10.1016/j.wneu.2013.02.012. [DOI] [PubMed] [Google Scholar]
- 44.Mitome-Mishima Y, Yamamoto M, Yatomi K, Nonaka S, Miyamoto N, Urabe T, et al. Endothelial cell proliferation in swine experimental aneurysm after coil embolization. PLoS One. 2014;9:e89047. doi: 10.1371/journal.pone.0089047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Díaz L, Zambrano E, Flores ME, Contreras M, Crispín JC, Alemán G, et al. Ethical considerations in animal research: The principle of 3R's. Rev Invest Clin. 2020;73:199–209. doi: 10.24875/RIC.20000380. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.