

Summary
Iron‐refractory iron deficiency anaemia (IRIDA) is a rare hereditary microcytic anaemia characterized by partial or complete resistance to oral iron supplementation, caused by elevated plasma hepcidin levels resulting from pathogenic variants in the TMPRSS6 gene. Although intravenous iron supplementation is often effective, patient responses can vary significantly due to various factors, and potential side effects of this treatment remain unclear. Additionally, evidence‐based international guidelines for diagnosing and managing IRIDA are lacking. This review aims to provide patient‐tailored treatment strategies, informed by case studies and expert opinion, to address the specific therapeutic needs of both children and adults with IRIDA.
Keywords: hepcidin, iron distribution disorder, iron‐refractory iron deficiency anaemia, iron therapy
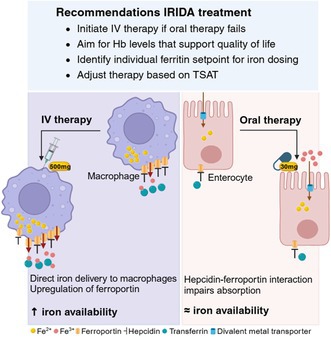
In iron‐refractory iron deficiency anaemia, inappropriately elevated hepcidin levels impair enteral iron absorption and iron release from macrophages by interacting with ferroportin. Oral iron supplements (containing ~30 mg Fe2+ per 100 mg) are generally ineffective due to this hepcidin–ferroportin interaction although, in some cases, this can be effective. Intravenous (IV) iron bypasses this barrier by delivering iron directly to macrophages. Subsequent ferroportin upregulation overcomes hepcidin inhibition, enabling iron release. Iron mobilization depends on the ferritin set point, the threshold for releasing iron from reticuloendothelial stores. As iron availability increases, haemoglobin levels will usually rise; however, normalizing haemoglobin is not the primary goal—the focus is on overall well‐being. When transferrin saturation begins to rise, the frequency of IV administrations can often be reduced.
INTRODUCTION
Iron‐refractory iron deficiency anaemia (IRIDA) is a rare hereditary microcytic anaemia caused by pathogenic variants in TMPRSS6, encoding matriptase‐2, a transmembrane protease that inhibits hepatic hepcidin synthesis via the Bone Morphogenetic Protein (BMP)/Small Mothers Against Decapentaplegic (SMAD) pathway. 1 , 2 Pathogenic TMPRSS6 variants lead to inappropriately elevated hepcidin levels relative to the body's iron status, especially circulating iron. 3
Clinically, IRIDA presents with hypochromic microcytic anaemia with markedly low serum iron and transferrin saturation (TSAT <10% or <15% with iron supplementation) in the absence of inflammation. 2 The phenotype is generally more pronounced in children, possibly due to their higher growth‐related iron demands or a different hepcidin set point relative to body iron levels. 4
As an iron distribution disorder, IRIDA is marked by relatively high iron levels in reticuloendothelial macrophages compared to the circulation and parenchymal cells, like hepatocytes. Importantly, elevated hepcidin alone does not confirm the diagnosis; it must be interpreted alongside the body's iron levels and inflammation status. In IRIDA, iron maldistribution is best reflected by a low TSAT/hepcidin ratio (<2.5th percentile for age and gender) (Table 1). 11 , 12 , 13 Another diagnostic hallmark is minimal or absent response to oral iron supplementation and incomplete response to intravenous (IV) iron therapy, with persistently low TSAT (Figure 1). 2 , 14
TABLE 1.
Characteristics of IRIDA.
| Clinical suspicion of IRIDA |
|---|
| Autosomal recessive inheritance a |
| Microcytic, hypochromic anaemia |
| Low circulating iron levels (serum iron and TSAT) in the absence of inflammation |
| Minimal or no response to oral iron therapy (Hb <1 g/dL in 4 weeks), partial response to IV therapy |
| More pronounced in childhood, tends to improve with ageing |
| Family history of microcytic anaemia refractory to oral iron therapy, especially in men |
| Laboratory findings | ||
|---|---|---|
| Ferritin | Variable b | |
| TSAT | <5%–10% (<15% post‐iron therapy) | |
| TSAT/hepcidin c | Male | <1.6%/nM |
| Female | <1.9%/nM (pre‐menopausal) | |
| <1.4%/nM (post‐menopausal) | ||
Abbreviations: IRIDA, iron refractory iron deficiency anaemia; TSAT, transferrin saturation.
Although IRIDA is typically considered an autosomal recessive disorder, a milder IRIDA phenotype has been reported in patients with a heterozygous genotype. 5
Ferritin levels in IRIDA patients are usually at the lower limit of the reference interval, but can be below this lower limit in cases of absolute iron deficiency. Ferritin levels above the higher limit of the reference interval may occur after IV iron therapy. However, relying solely on ferritin levels can be challenging, as ferritin is an acute‐phase protein that increases in response to inflammation or infection. This increase is likely driven by elevated hepcidin levels, which trap iron in macrophages, raising ferritin levels. Elevated ferritin can also result from other conditions, such as autoimmune diseases, chronic kidney disease, liver disease, metabolic syndrome (NASH, overweight, hypertension) and certain malignancies. 6 , 7 Note that ferritin assays lack standardization, meaning that levels may vary depending on the methodology used. 8 , 9
FIGURE 1.
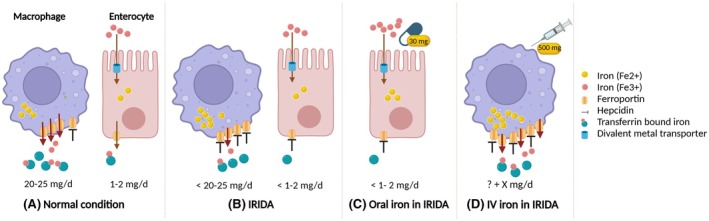
Schematic overview of effects of oral and IV iron therapy in IRIDA. (A) Macrophages release 20–25 mg of iron daily, mainly from the recycling of senescent erythrocytes. Enterocytes absorb 1–2 mg of dietary iron. Iron enters the circulation via the membrane‐bound exporter ferroportin, binds to transferrin and is delivered to iron‐requiring cells, including erythroid precursor cells. Each transferrin molecule can carry up two iron ions; for example, at a TSAT of 50%, each transferrin molecule typically carries one iron ion. (B) In IRIDA, inappropriately elevated hepcidin levels inhibit dietary iron uptake and iron release from macrophages by interacting with ferroportin, reducing circulating iron levels. (C) Oral iron supplements (containing usually 30 mg elemental iron per 100 mg of the compound) are generally ineffective in IRIDA. Hepcidin‐mediated inhibition traps iron in duodenal enterocytes, preventing its release into circulation and macrophages, and thus not significantly improving circulating iron levels. However, positive outcomes have been observed in younger children, although the studies are heterogeneous in terms of treatment regimens. (D) IV iron bypasses this barrier by delivering a significantly higher amount of elemental iron directly to macrophages, where it is unpacked from its carbohydrate shell. Ferroportin mRNA expression in macrophages is upregulated via the IRP/IRE system, overcoming hepcidin inhibition and enabling iron release into circulation while releasing macrophage iron loading. The extent of this release depends on the ferritin set point of a specific patient—the ferritin level at which iron is mobilized from reticuloendothelial stores—which tends to decrease with age and increase with the severity of TMPRSS6 defects.
The diagnosis of IRIDA is confirmed by identifying biallelic TMPRSS6 variants classified as (possibly) pathogenic (class 3 or higher), along with the characteristic clinical and biochemical profile (Table 1). 5 , 14 , 15 Although IRIDA is typically considered an autosomal recessive disorder, heterozygous TMPRSS6 variants can result in a milder phenotype with less need for IV therapy. 3 , 5 , 14 This guidance, however, focuses specifically on IRIDA due to biallelic TMPRSS6 variants.
Other causes of IRIDA, including gastro‐intestinal conditions (e.g. Helicobacter pylori infection, coeliac disease or atrophic gastritis), must be excluded. 16
Distinguishing IRIDA from absolute iron deficiency is essential. Absolute iron deficiency is characterized by both low iron stores and circulating iron, while IRIDA represents a form of functional iron deficiency, with adequate stores but limited erythropoietic availability due to impaired distribution (Table 2). 6 , 8 This results in iron‐restricted erythropoiesis, with relatively high ferritin levels compared to serum iron and TSAT, indicating iron sequestration in reticuloendothelial macrophages. 8 Over time, without adequate treatment, functional iron deficiency can progress to absolute iron deficiency.
TABLE 2.
Laboratory characteristics of common anaemias distinguishable from IRIDA.
| Iron deficiency anaemia (IDA) | Anaemia of chronic disease (ACD) | Mixed IDA + ACD | Iron refractory iron deficiency anaemia | |
|---|---|---|---|---|
| Haemoglobin | ↓ | ↓ | ↓ | ↓ |
| MCV | ↓ | ↓/= | ↓ | ↓ |
| Iron | ↓ | ↓ | ↓ | ↓ |
| Transferrin | ↑ | ↓ | =/↓ | ↑ |
| Ferritin c | ↓↓ (<15‐30 μg/L) | ↓/= (<100 μg/L) | = (<70–100 μg/L) | ↓/= (20–50 μg/L) a |
| TSAT | ↓ (<15%) | ↓ (<15%–20%) | ↓ (<15%–20%) | ↓↓ (usually <5%) |
| Hepcidin b | ↓↓ | ↑ (relative to TSAT) | =/↓ | ↑↑ (relative to TSAT) |
| sTfR | ↑↑ | ↓/= | =/↑ | ↑ |
| Effect iron therapy | Oral: ++ | Oral: − | Oral:+/− | Oral: − |
| IV: ++ | IV: +/− | IV:+/− | IV: +/− |
Note: This table provides laboratory characteristics of prevalent forms of anaemia that should be distinguished from IRIDA. Both ACD and IRIDA involve functional iron deficiency due to elevated hepcidin levels, leading to iron sequestration within macrophages (often reflected by normal to high ferritin levels). In both conditions, the hepcidin–ferroportin mechanism is disrupted and similarly affects treatment response. However, in ACD, additional factors such as reduced red blood cell survival or inhibited erythropoiesis due to cytokines can affect therapy outcomes. In mixed IDA + ACD, hepcidin levels depend on whether inflammation or iron deficiency predominates. In the presence of inflammation, severe anaemia may result in low hepcidin to enhance iron availability for erythropoiesis. ↑ increased, ↓ decreased, = within reference interval. Adjusted from Swinkels et al. 8
Abbreviations: Hb, haemoglobin; IRIDA, iron refractory iron deficiency anaemia; MCV, mean corpuscular volume; sTfR, soluble transferrin receptor; TSAT, transferrin saturation.
Ferritin levels can range widely. They are typically at the lower limit of the reference interval, but can be below this lower limit if untreated for years. After IV iron therapy or long‐term oral treatment, ferritin may be above the higher limit of the reference interval.
Note that worldwide ferritin assays lack standardization, meaning that reported levels may vary depending on the methodology used. 9
Hepcidin levels should be interpreted in the context of body iron levels (ferritin and/or TSAT). In IRIDA, hepcidin levels are disproportionately high relative to circulating iron levels (TSAT, serum iron), resulting in a low TSAT/hepcidin ratio.
Currently, no evidence‐based or consensus guidelines exist for treating IRIDA, and current management relies primarily on anecdotal case reports involving small patient series. This highlights the need for structured, evidence‐informed guidance. In this How to Treat, we present patient‐specific treatment strategies informed by available case evidence and our clinical expertise in managing IRIDA at Radboudumc, the national expertise centre for iron disorders in the Netherlands. Our approach aims to address the specific therapeutic needs of both children and adults with IRIDA.
IRIDA TREATMENT IN LITERATURE
A review of the literature on IRIDA treatment identified only case studies (see Supplemental Information S1 for literature search methodology). These studies reported diverse treatments—oral iron supplementation (with or without ascorbic acid), IV iron therapy and erythropoiesis‐stimulating agents (ESAs)—with highly variable outcomes (Table S1).
Oral iron therapy
Although high hepcidin levels in IRIDA generally reduce the effectiveness of oral iron supplementation, case studies reported variable haemoglobin responses. Positive outcomes were observed with higher doses or prolonged therapy, particularly in younger children or those with monoallelic or less severe biallelic TMPRSS6 defects (Table S1). 17 , 18 , 19 , 20 , 21 Interestingly, a 9‐month‐old girl initially unresponsive to oral iron showed improvement after adding ascorbic acid following a short course of IV iron therapy. 22 While other cases support this combination therapy, outcomes in the literature remain inconsistent, likely due to incompletely defined IRIDA cases. 23 , 24
These findings suggest that the effectiveness of oral iron therapy in IRIDA may depend on factors such as the IRIDA definition, treatment regimen, patient age, genotype (including genetic makeup beyond TMPRSS6) and concurrent therapies.
Intravenous iron
IV iron therapy generally showed more consistent efficacy than oral iron in increasing haemoglobin levels, although individual responses varied (Table S1). 14 , 17 , 25 , 26 , 27 , 28 This advantage is likely due to IV iron's higher elemental iron content and favourable pharmacokinetic profile. 29 While a single dose of oral iron generally provides about 20 mg of elemental iron daily (containing up to 30% elemental iron, with 10%–35% absorption), IV formulations like ferric carboxymaltose can deliver 500–1000 mg per dose, bypassing the intestinal hepcidin–ferroportin block by entering macrophages directly. Macrophages, with higher overall ferroportin expression than enterocytes, require significantly more hepcidin for comparable suppression of cellular iron release. 29 , 30 Furthermore, IV iron, by directly loading iron into macrophages, upregulates ferroportin via the cellular iron regulatory IRP/IRE (iron regulatory protein/iron responsive element) pathway, preventing intracellular iron toxicity. 31 Repeated IV iron administrations that elevate intracellular iron levels beyond a certain threshold facilitate effective, but not complete, iron mobilization from macrophages for erythropoiesis (Figure 1). 31 , 32
Despite the general effectiveness of IV iron therapy, case studies showed differences in administered doses, duration of effect and haemoglobin responses, even among patients with similar genotypes. 22 , 25 , 26 , 27 , 33 Higher doses or shorter intervals between administrations generally tended to further improve haemoglobin levels (Table S1). 17 , 21 , 26 Of note, published cases predominantly involved children with IRIDA, whose responses may differ from adults due to age‐related physiological differences.
Alternative therapies
There are limited case reports on using ESAs in IRIDA, with inconsistent haemoglobin responses. 21 , 33 ESAs may stimulate erythroferrone secretion, suppressing hepcidin synthesis and potentially improving cellular iron release. However, ESAs could also exacerbate functional iron deficiency due to unmet iron demand from increased erythropoiesis. Combining ESAs with IV iron may be beneficial, but evidence supporting this approach in IRIDA is lacking.
Given the central role of elevated hepcidin in IRIDA, novel oral iron formulations that bypass the enteral hepcidin–ferroportin pathway show promise for improving iron availability. For instance, nanotechnology‐based formulations have demonstrated efficacy in improving haemoglobin levels in populations with iron deficiency anaemia, including those with inflammatory bowel disease and chronic kidney disease. 34 , 35 Their improved bioavailability may allow for lower elemental iron doses, potentially reducing gastrointestinal side effects commonly associated with higher iron doses. However, most studies had relatively short follow‐up periods and lack direct comparison with oral ferrous salts, leaving their long‐term impact on iron stores and haemoglobin levels relative to conventional formulations unclear. 36 , 37
Another promising approach involves directly targeting the hepcidin–ferroportin axis, the underlying cause of IRIDA. This strategy has shown potential in preclinical research and clinical trials involving patients with inflammatory conditions characterized by elevated hepcidin levels, such as Castleman's disease and rheumatoid arthritis. 38 , 39 , 40
However, to the best of our knowledge, neither novel oral formulations nor hepcidin antagonists have been studied or approved for use in IRIDA.
CASE DESCRIPTIONS
Existing literature predominantly addresses treatment outcomes in children with IRIDA, while adults have distinct clinical needs and presentations, as illustrated in cases from our iron expertise centre (Figure 2). These cases provide insights into the pathophysiology underlying treatment variability, highlighting the need for individualized approaches in both adults and children.
FIGURE 2.
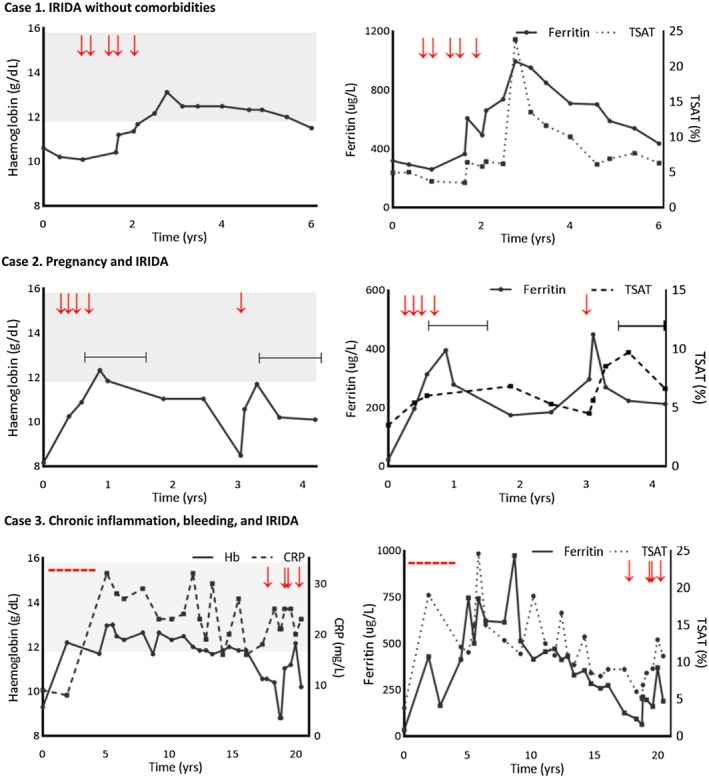
Course of haemoglobin, ferritin and TSAT levels in three female IRIDA patients. The left panels display Hb levels (with CRP for case 3); the right panels show ferritin and TSAT levels. Case 1: Hb and iron metrics over 6 years. This patient initially received IV iron therapy at irregular intervals due to being lost to follow up. At age 26 (6 years post‐diagnosis, time point t = 0), regular IV iron therapy was initiated. Over the subsequent years, she received a cumulative dose of 2500 mg of FCM via five 500 mg infusions, causing a sharp rise in ferritin (>900 μg/L) and TSAT (up to 25%). Despite persistently high ferritin (>700 μg/L), Hb only briefly peaked and remained within the lower normal range. Case 2: Hb and iron metrics over 4 years, including two pregnancies (shown by horizontal bars). At diagnosis (t = 0), this 32‐year‐old patient began monthly IV iron therapy. After a cumulative dose of 1700 mg FCM, the patient became pregnant (unaware at last administration). Particularly during the first pregnancy, TSAT remained stable and the Hb decrease was less pronounced than during non‐pregnancy periods. Case 3: Hb, CRP and iron metrics over 20 years. IV iron (totalling 5800 mg FS at 200 mg/dose) was administered every 2 months, maintaining ferritin >500 μg/L for nearly a decade, with Hb within the reference range. Diagnosis of IRIDA was made at t = 5 when she was 41 years old. Ferritin and TSAT varied widely, likely due to chronic inflammation (CRP ~25 mg/L). In the final years (following t = 15), heavy menstrual bleeding led to a Hb decline, requiring additional IV iron therapy (totalling 1700 mg FCM). Red arrows: IV iron administration; Grey‐shaded area: Hb reference interval. CRP, C‐reactive protein; FCM, ferric carboxymaltose; FS, iron saccharate; Hb, haemoglobin; TSAT, transferrin saturation.
Case 1 describes a female patient who presented with chronic, IRIDA since age 1. Initial diagnostics excluded gastrointestinal pathology and thalassaemia. Her anaemia was attributed to low iron intake or an iron incorporation disorder, but she was lost to follow up, preventing further evaluation. At age 20, she returned with symptoms and was diagnosed with TMPRSS6‐related IRIDA due to a homozygous frameshift variant (NM_153609.3: c.1904_1905dup; p.(Lys636Alafs*17)). She received IV iron therapy but again was lost to follow up. At age 26, she returned with clinical symptoms, normal‐high ferritin (260 μg/L) and low circulating iron (TSAT 3.5%, iron 2 μmol/L). IV therapy was reinitiated with two doses of 500 mg ferric carboxymaltose with a 1‐month interval, twice a year. After a cumulative dose of 1000 mg elemental iron, her iron parameters improved slightly. Subsequent infusions caused significant increases in ferritin and TSAT, with normalization of haemoglobin levels, after which therapy was stopped. Notably, haemoglobin levels remained within the reference interval for several years post‐therapy, with persistently elevated ferritin levels.
Conclusion: This case illustrates the importance of reaching a ferritin set point, marked by a rise in TSAT, indicating that iron is becoming available for erythropoiesis. In hindsight, IV treatment could have been stopped once ferritin reached approximately 700 μg/L, as haemoglobin was already improving. Careful titration of IV iron therapy to optimal haemoglobin levels for quality of life is essential to avoid unnecessary iron accumulation and potential macrophage dysfunction.
Case 2 involves an IRIDA patient who experienced two pregnancies. She was diagnosed with TMPRSS6‐related IRIDA at age 32, caused by a homozygous frameshift variant (NM_153609.3: c.497del; p.(Leu166Argfs*37)), after a lifelong history of iron‐refractory anaemia, requiring frequent IV iron therapy with limited response. Treatment was initiated with an initial dose of 200 mg ferric carboxymaltose, followed by 500 mg monthly. Unlike her early childhood, haemoglobin and ferritin levels and clinical symptoms improved. During treatment, she became pregnant, and IV therapy was discontinued. Remarkably, her iron parameters remained stable throughout pregnancy. Three years later, symptoms reoccurred. A single 500 mg dose of ferric carboxymaltose improved her condition, which stabilized again during a subsequent pregnancy.
Conclusion: This case highlights the potential effect of ageing on treatment response and underscores pregnancy‐related physiological suppression of hepcidin, which enhances iron availability for fetal–placental development, improving the IRIDA phenotype. 41
Case 3 describes a female IRIDA patient with chronic folliculitis who experienced iron‐refractory anaemia for years. Despite extensive diagnostics, including bone marrow biopsy and gastrointestinal endoscopy, no underlying causes were found. Her anaemia progressively worsened, requiring IV iron therapy every 2 months over a 5‐year period (cumulative dose: 5800 mg ferrioxide saccharate). During treatment, hepcidin levels were remarkably high, despite the absence of severe infection. At age 41, genotyping confirmed the diagnosis of TMPRSS6‐related IRIDA due to compound heterozygous missense variants (NM_153609.3: c.2383G>A; p.(Val795Ile); c.2105G>T; p.(Cys702Phe)) (Figure 2). Therapy was discontinued once haemoglobin levels normalized, which remained within the reference interval over the next decade, while ferritin and TSAT fluctuated, likely due to chronic inflammation episodes. Heavy menstrual bleeding resulted in haemoglobin decline, necessitating IV therapy again (cumulative dose: 1700 mg ferric carboxymaltose). However, ferritin levels further decreased post‐therapy.
Conclusion: This case illustrates the challenges of managing IRIDA in the context of chronic inflammation and additional factors like iron loss from menstrual bleeding. Fluctuating ferritin and TSAT levels, despite stable haemoglobin, suggest that inflammation complicates iron status assessment. As in Case 1, haemoglobin normalization was associated with excessively high ferritin levels. The post‐therapy ferritin level drop indicates that menstrual iron loss exceeded the benefits from iron supplementation.
EXPERT OPINION‐BASED TREATMENT GUIDANCE
Despite numerous case reports and studies on IRIDA pathophysiology, many questions remain about its optimal treatment. Here, we provide expert opinion‐based treatment guidance informed by the previously published IRIDA case reports, a comprehensive literature review on iron disorders and IRIDA pathophysiology and our clinical expertise in managing IRIDA patients in the Netherlands (Table 3).
TABLE 3.
Key recommendations for IRIDA treatment.
| Principles of IRIDA treatment |
|---|
|
Abbreviations: IRIDA, iron refractory iron deficiency anaemia; TSAT, transferrin saturation.
Oral iron therapy
Published case series showed that oral iron supplementation can be effective, especially in younger children with milder TMPRSS6 defects. 14 , 18 Although childhood cases often present a more pronounced phenotype, it is conceivable that an alternative hepcidin‐independent absorption mechanism might support oral iron efficacy, although evidence is lacking. Studies suggest higher doses may bypass the hepcidin‐mediated ferroportin block, improving haemoglobin levels. 18 , 19 Therefore, we recommend starting with a once‐daily dose of 3 mg/kg of elemental iron in children (Figure 3). Anecdotal reports showed positive effects at doses up to 10 mg/kg; however, if higher doses are ineffective, oral iron should be discontinued. 18 Since the maximum absorption capacity is around 25%, unabsorbed iron may accumulate in the colon, potentially causing adverse effects, disrupting the microbiota, and increasing the risk of infections, intestinal inflammation and metabolic syndrome. 37
FIGURE 3.
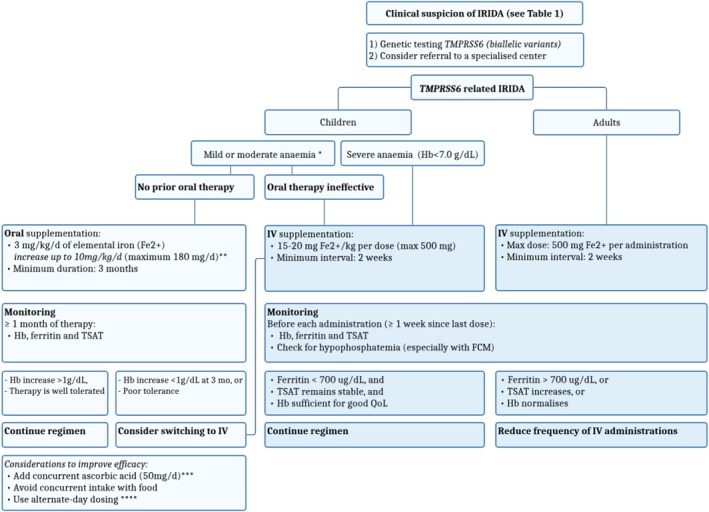
Flowchart of expert opinion‐based treatment guidance for IRIDA patients. This figure outlines treatment strategies for IRIDA in children and adults, based on expert opinion. Children: For mild to moderate anaemia without previous oral iron therapy, start once‐daily oral elemental iron (3 mg/kg/day, compared to the 1 mg/kg/day usually used for iron deficiency anaemia), titrating up to a maximum of 10 mg/kg/day based on evidence from case series suggesting better responses with higher doses. Minimize concurrent intake with specific foods (e.g. dairy products and fibres) and medications (e.g. calcium supplements, antacids, proton pump inhibitors) to prevent insoluble complexes that reduce iron availability. 42 Continue oral therapy for at least 3 months before considering IV iron therapy, as prolonged oral therapy may still be effective (Table S1). In iron deficiency anaemia, a 2‐g/dL Hb increase is expected within 4 weeks. 43 If oral iron therapy proves ineffective (including previous attempts) or severe anaemia is present, initiate IV iron therapy at 15–20 mg/kg per dose, up to a maximum of 500 mg per dose. Monitoring recommendations are consistent with adult guidelines. Adults: In adults, IRIDA often presents with a mild(er) phenotype, causing diagnostic delays with subsequent prolonged oral iron therapy before the final diagnosis of IRIDA is established. Therefore, IV iron therapy is recommended as first‐line treatment. Avoid targeting Hb normalization to prevent excessively high ferritin levels. Regularly monitor phosphate levels (at least after two administrations) during FCM therapy due to the risk of hypophosphataemia. Assessing the total iron deficit is not applicable for IRIDA patients, as it is an iron distribution disorder. *Reference intervals and definitions are age‐dependent; severe anaemia is defined according to the WHO guidelines. **Dosages are not applicable for neonates. ***Despite a recent trial found no benefit from adding ascorbic acid to oral iron therapy for iron deficiency anaemia, it may still be considered to improve iron absorption in IRIDA. 44 ****Alternate‐day dosing can reduce hepcidin‐mediated inhibition of iron uptake, which reduces iron absorption for approximately 24 h after iron intake. 45 FCM, ferric carboxymaltose; Hb, haemoglobin; IV, intravenous; QoL, quality of life; TSAT, transferrin saturation.
Although a recent clinical trial in adults with iron deficiency anaemia showed no added benefit from ascorbic acid, this may not exclude its potential benefit in IRIDA. 44 Moreover, reported cases showed varying outcomes with this combination therapy. 22 , 23 , 24 Iron should be taken apart from certain foods (e.g. dairy products, fibres) and medications (e.g. proton pump inhibitors, calcium supplements, antacids), which can reduce iron availability by forming insoluble complexes. 42 Alternate‐day dosing may reduce hepcidin‐mediated inhibition of iron uptake, which for iron‐deficient adult women has been described to last for approximately 24 h after iron intake. 45
In absolute iron deficiency anaemia, a weekly haemoglobin increase of approximately 0.8 g/dL is expected; however, in IRIDA, this haemoglobin increase in time is likely lower due to reduced iron availability. We define IRIDA non‐responders as those with less than a 1 g/dL haemoglobin increase after 4 weeks of oral therapy. As extended use appears more effective, oral supplementation should be continued for at least 3 months before considering switching to IV therapy. However, in practice, most patients diagnosed with IRIDA have already completed multiple unsuccessful attempts at oral iron supplementation. For these children, if they have been compliant with the prescribed therapy, reinitiating or extending oral therapy for 3 months is unnecessary. Instead, we recommend initiating IV iron therapy as soon as the diagnosis is confirmed.
IV iron therapy
Overall, reported case series as well as our three aforementioned cases demonstrate that IV treatment is generally effective, although responses vary significantly among patients (Figure 2). Our experience and case studies indicate that similar IV iron doses can result in different ferritin increases, and that ferritin levels do not consistently correlate with haemoglobin improvements across patients. We hypothesize that each IRIDA patient has an individual ferritin set point at which macrophages release iron into the circulation, making it available for erythropoiesis. This set point may be influenced by factors such as: (i) TMPRSS6 genotype, with severe variants increasing hepcidin synthesis and requiring a higher cumulative dose of IV iron, (ii) age, as treatment response has been described to improve with ageing, and (iii) concurrent conditions. For instance, pregnancy may improve iron availability by lowering hepcidin levels, while inflammation worsens IRIDA by increasing hepcidin levels. 46 , 47 Additionally, conditions causing absolute iron deficiency, such as menstrual bleeding, gastrointestinal malabsorption or limited dietary intake, can further worsen the phenotype. Therefore, establishing a universal ferritin target is inappropriate. Instead, treatment should focus on identifying the ferritin level that supports haemoglobin levels sufficient for an acceptable quality of life, enabling patients to carry out their daily activities. The haemoglobin level needed will vary between patients, making the primary goal to enhance daily functioning and overall quality of life rather than simply normalizing haemoglobin levels. Consequently, not only the target haemoglobin level but also the optimal ferritin level will differ among patients. IV iron should be carefully titrated to maintain this individualized ferritin level. Normalizing haemoglobin may result in excessively high ferritin levels (Figure 2, Case 1 and 3), indicating iron loading in the reticuloendothelial system in these patients, the long‐term effects of which are unknown.
Currently, no studies define the optimal frequency for IV iron therapy in IRIDA. Elevated hepcidin levels in IRIDA reduce ferroportin activity and cellular iron release, suggesting that higher hepcidin levels have a more significant impact. While large studies are lacking, one report showed that hepcidin levels increased within 6 h after a 200‐mg IV iron sucrose dose in an IRIDA case, returning to baseline after 1 week. 14 Research in chronic kidney disease (CKD) patients may also provide insights. 48 For instance, a randomized trial found that hepcidin levels increased significantly at the start of a 4‐weekly IV iron regimen, particularly with higher doses (e.g. 1000 mg versus 200 mg of ferric carboxymaltose). These elevated hepcidin levels persisted for 52 weeks, but the impact of subsequent doses on hepcidin diminished over time. 48 Based on these findings, we recommend administering frequent, smaller doses of IV iron (maximum dose: 500 mg elemental iron) at intervals of at least 2 weeks (Figure 3). Higher and more frequent dosing may further elevate hepcidin levels, potentially reducing the effectiveness of subsequent administrations. Moreover, lower dosing better allows personalized treatment in time.
Monitoring
Iron overload is a potential risk of IV iron therapy. Our experience suggests that IV iron therapy in IRIDA elevates ferritin levels without significantly affecting TSAT, indicating that iron is primarily stored in the reticuloendothelial system. An increase in TSAT suggests iron redistribution from the reticuloendothelial system to the circulation, signalling that the ferritin set point—the level at which iron becomes available for erythropoiesis and other (parenchymal) tissues—has been reached. While this iron redistribution improves iron availability and haemoglobin levels, it may also result in a decreased erythropoietic iron demand, potentially leading to toxic parenchymal iron overload, necessitating reduced treatment frequency.
Unlike inappropriately low‐hepcidin disorders such as HFE‐hereditary hemochromatosis, where iron accumulates in parenchymal tissues with a higher toxicity risk, IRIDA primarily results in iron overload in the reticuloendothelial macrophages. 49 Although the long‐term effects of such iron accumulation remain unclear, patients with (loss‐of‐function) ferroportin disease, who have similar biochemical profiles, typically do not experience severe complications despite excessive high ferritin levels. 49 Additionally, evidence from CKD patients suggests that excess reticuloendothelial iron, during at least a few years, is well tolerated. 50
Given the unknown long‐term risks, we recommend checking ferritin, TSAT and haemoglobin before each administration. If TSAT levels rise but the patient remains symptomatic with low haemoglobin requiring therapy, we advise reducing IV iron administration frequency. As IRIDA patients typically cannot achieve TSAT within the reference range due to hepcidin dysregulation, we recommend maintaining TSAT around 15%. In our experience, this percentage allows for sufficient iron availability for erythropoiesis without causing unnecessary excessive iron loading in the reticuloendothelial system. Importantly, the goal is not to normalize haemoglobin, as we cannot exclude that prolonged iron loading in the reticuloendothelial system may pose long‐term risks. Ferritin levels should be kept as low as possible while ensuring acceptable haemoglobin and quality of life.
General side effects of IV iron
Various IV formulations are available for the treatment of IRIDA. Older formulations, particularly high‐molecular‐weight dextran, were associated with serious adverse events like anaphylaxis and have been withdrawn from the market. 51 In contrast, newer formulations use carbohydrate shells that tightly bind iron, reducing labile iron and minimizing infusion reactions. 52 Current infusion reactions, often referred to as Fishbane reactions, occur in approximately 1 in 100–250 infusions and are usually self‐limiting, caused by transient‐free iron from rapid administration. 29 , 53 A multicentre cohort study found iron sucrose having the highest reaction rate (4.3%) and ferric carboxymaltose the lowest (1.4%), likely due to differences in carbohydrate core stability. 53 , 54 Serious anaphylactoid reactions are extremely rare, with an incidence ranging from 0.38 to 0.51 per 10,000 first administrations in a European post‐authorization study. 55
While no definitive studies address infection risk with IV iron in IRIDA, this remains an important consideration. Iron plays a crucial role in both pathogen reproduction and host immunity, and its sequestration within macrophages may theoretically increase infection risk from intracellular pathogens. However, randomized controlled trials involving haemodialysis patients, who typically have elevated hepcidin levels, suggest that high‐dose IV iron does not significantly increase infection risk compared to lower doses during the trial period. Nevertheless, the impact of ferritin levels exceeding 700 μg/L combined with low‐normal TSAT, however, remains unclear. 56
Moreover, we recommend monitoring phosphate levels in patients receiving ferric carboxymaltose, as this treatment is associated with renal phosphate‐wasting syndrome. This affects 51%–75% of non‐CKD patients in clinical trials, especially those with low ferritin and preserved kidney function. 51 , 57 This condition, characterized by hyperphosphaturic hypophosphatemia due to high fibroblast growth factor 23 (FGF‐23), leads to hypovitaminosis D, hypocalcaemia and secondary hyperparathyroidism, potentially causing irreversible osteomalacia. 58 If hypophosphatemia develops, switching to a different formulation is recommended, as this effect appears specific to ferric carboxymaltose. 57
CONCLUSION
In IRIDA, inappropriately elevated hepcidin levels impair oral iron availability for erythropoiesis, making IV therapy more effective as it partially bypasses the hepcidin–ferroportin block. Oral iron therapy should be attempted initially; however, if ineffective, IV therapy should be considered promptly to prevent under‐treatment, especially in paediatric patients. IV treatment should be carefully titrated to achieve acceptable haemoglobin levels while avoiding iron overloading macrophages, guided by ferritin, TSAT and haemoglobin levels. Monitoring serum phosphate levels is advised during ferric carboxymaltose therapy due to the risk of hypophosphatemia. While anti‐hepcidin therapies target the root cause, no such agents are currently approved for IRIDA.
AUTHOR CONTRIBUTIONS
This treatment guidance for IRIDA was developed with the expertise of all authors, who are all involved in the care of IRIDA patients. VH performed a literature search. All authors contributed to the discussion of data and information from literature and, as a team, developed an expert opinion for IRIDA treatment. VH analysed patient data and drafted the first version of the manuscript. AED, SEM and DWS provided a critical review of the manuscript. All authors approved the final version.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
Supporting information
Data S1.
ACKNOWLEDGEMENTS
We would like to thank Keros Therapeutics for providing salary support to VH, which contributed in part to making this work possible. However, Keros Therapeutics had no involvement in the study's design, data analysis, manuscript preparation or decision to submit this manuscript for publication.
Hoving V, Donker AE, Schols SEM, Swinkels DW. How I treat iron‐refractory iron deficiency anaemia—An expert opinion‐based treatment guidance for children and adults . Br J Haematol. 2025;206(4):1067–1076. 10.1111/bjh.20030
REFERENCES
- 1. Silvestri L, Nai A, Dulja A, Pagani A. Hepcidin and the BMP‐SMAD pathway: an unexpected liaison. Vitam Horm. 2019;110:71–99. [DOI] [PubMed] [Google Scholar]
- 2. Finberg KE. Iron‐refractory iron deficiency anemia. Semin Hematol. 2009;46(4):378–386. [DOI] [PubMed] [Google Scholar]
- 3. Finberg KE, Heeney MM, Campagna DR, Aydınok Y, Pearson HA, Hartman KR, et al. Mutations in TMPRSS6 cause iron‐refractory iron deficiency anemia (IRIDA). Nat Genet. 2008;40(5):569–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Donker AE, Galesloot TE, Laarakkers CM, Klaver SM, Bakkeren DL, Swinkels DW. Standardized serum hepcidin values in Dutch children: set point relative to body iron changes during childhood. Pediatr Blood Cancer. 2020;67(3):e28038. [DOI] [PubMed] [Google Scholar]
- 5. Hoving V, Korman SE, Antonopoulos P, Donker AE, Schols SEM, Swinkels DW. IRIDA phenotype in TMPRSS6 monoallelic‐affected patients: toward a better understanding of the pathophysiology. Genes (Basel). 2022;13(8):1309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Pasricha S‐R, Tye‐Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233–248. [DOI] [PubMed] [Google Scholar]
- 7. Baird‐Gunning J, Bromley J. Correcting iron deficiency. Aust Prescr. 2016;39(6):193–199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Swinkels DW. Iron metabolism. In: Rifai N, Chiu RWK, Young I, Burnham C‐AD, Wittwer CT, editors. Tietz Texbook of laboratory medicine. 7th ed. St. Louis (MO): Elsevier Saunders; 2023. [Google Scholar]
- 9. Swinkels DW, van Schrojenstein LM, Matlung HL, Weykamp C, Thelen M. Equivalence in clinical assessment of iron status requires ferritin assay standardisation before harmonisation of ferritin reference intervals. Lancet Haematol. 2024;11(10):e721. [DOI] [PubMed] [Google Scholar]
- 10. Diepeveen LE, Laarakkers CMM, Martos G, Pawlak ME, Uğuz FF, Verberne K, et al. Provisional standardization of hepcidin assays: creating a traceability chain with a primary reference material, candidate reference method and a commutable secondary reference material. Clin Chem Lab Med. 2019;57(6):864–872. [DOI] [PubMed] [Google Scholar]
- 11. van der Staaij H, Donker AE, Bakkeren DL, Salemans J, Mignot‐Evers LAA, Bongers MY, et al. Transferrin saturation/hepcidin ratio discriminates TMPRSS6‐related iron refractory iron deficiency anemia from patients with multi‐causal iron deficiency anemia. Int J Mol Sci. 2022;23(3):1917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hepcidinanalysis.com. Reference values: Internet; [cited 2024 Jun 11]. Available from: https://www.hepcidinanalysis.com/provided‐service/reference‐values/.
- 13. Heeney MM, Guo D, De Falco L, Campagna DR, Olbina G, Kao PP, et al. Normalizing hepcidin predicts TMPRSS6 mutation status in patients with chronic iron deficiency. Blood. 2018;132(4):448–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Donker AE, Schaap CC, Novotny VM, Smeets R, Peters TM, van den Heuvel BL, et al. Iron refractory iron deficiency anemia: a heterogeneous disease that is not always iron refractory. Am J Hematol. 2016;91(12):E482–E490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Donker AE, Raymakers RA, Vlasveld LT, van Barneveld T, Terink R, Dors N, et al. Practice guidelines for the diagnosis and management of microcytic anemias due to genetic disorders of iron metabolism or heme synthesis. Blood. 2014;123(25):3873–3886. quiz 4005. [DOI] [PubMed] [Google Scholar]
- 16. Hershko C, Camaschella C. How I treat unexplained refractory iron deficiency anemia. Blood. 2014;123(3):326–333. [DOI] [PubMed] [Google Scholar]
- 17. Sal E, Keskin EY, Yenicesu I, Bruno M, De Falco L. Iron‐refractory iron deficiency anemia (IRIDA) cases with 2 novel TMPRSS6 mutations. Pediatr Hematol Oncol. 2016;33(3):226–232. [DOI] [PubMed] [Google Scholar]
- 18. Khuong‐Quang D‐A, Schwartzentruber J, Westerman M, Lepage P, Finberg KE, Majewski J, et al. Iron refractory iron deficiency anemia: presentation with Hyperferritinemia and response to Oral iron therapy. Pediatrics. 2013;131(2):e620–e625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Beutler E, Van Geet C, te Loo DMWM, Gelbart T, Crain K, Truksa J, et al. Polymorphisms and mutations of human TMPRSS6 in iron deficiency anemia. Blood Cell Mol Dis. 2010;44(1):16–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Choi HS, Yang HR, Song SH, Seo J‐Y, Lee K‐O, Kim H‐J. A novel mutation Gly603Arg of TMPRSS6 in a Korean female with iron‐refractory iron deficiency anemia. Pediatr Blood Cancer. 2012;58(4):640–642. [DOI] [PubMed] [Google Scholar]
- 21. Lehmberg K, Grosse R, Muckenthaler MU, Altamura S, Nielsen P, Schmid H, et al. Administration of recombinant erythropoietin alone does not improve the phenotype in iron refractory iron deficiency anemia patients. Ann Hematol. 2013;92(3):387–394. [DOI] [PubMed] [Google Scholar]
- 22. Cau M, Galanello R, Giagu N, Melis MA. Responsiveness to oral iron and ascorbic acid in a patient with IRIDA. Blood Cells Mol Dis. 2012;48(2):121–123. [DOI] [PubMed] [Google Scholar]
- 23. Sourabh S, Bhatia P, Jain R. Favourable improvement in haematological parameters in response to oral iron and vitamin C combination in children with iron refractory iron deficiency anemia (IRIDA) phenotype. Blood Cells Mol Dis. 2019;75:26–29. [DOI] [PubMed] [Google Scholar]
- 24. Allison J, Drury L, Ford JB. Two novel TMPRSS6 variants in a compound heterozygous child with iron refractory iron deficiency anemia. J Pediatr Hematol Oncol. 2020;42(4):e238–e239. [DOI] [PubMed] [Google Scholar]
- 25. Malherbe JAJ, Cole CH. Double trouble: a case of fraternal twins with iron‐refractory iron‐deficiency anemia. Clin Case Reports. 2022;10(10):e6401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Maria Antonietta M, Milena C, Rita C, Gabriella S, Susanna B, Antonio C, et al. A mutation in the TMPRSS6 gene, encoding a transmembrane serine protease that suppresses hepcidin production, in familial iron deficiency anemia refractory to oral iron. Haematologica. 2008;93(10):1473–1479. [DOI] [PubMed] [Google Scholar]
- 27. Guillem F, Lawson S, Kannengiesser C, Westerman M, Beaumont C, Grandchamp B. Two nonsense mutations in the TMPRSS6 gene in a patient with microcytic anemia and iron deficiency. Blood. 2008;112(5):2089–2091. [DOI] [PubMed] [Google Scholar]
- 28. Huang DW, He GQ, Guo X, Wan Z, Gao J, Yang R. Iron‐refractory iron deficiency anemia with novel TMPRSS6 mutation. Indian J Pediatr. 2024;91(3):311. [DOI] [PubMed] [Google Scholar]
- 29. Girelli D, Ugolini S, Busti F, Marchi G, Castagna A. Modern iron replacement therapy: clinical and pathophysiological insights. Int J Hematol. 2018;107(1):16–30. [DOI] [PubMed] [Google Scholar]
- 30. Vlasveld LT, Dorine WS. Loss‐of‐function ferroportin disease: novel mechanistic insights and unanswered questions. Haematologica. 2018;103(11):1753–1755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Sukhbaatar N, Weichhart T. Iron regulation: macrophages in control. Pharmaceuticals (Basel). 2018;11(4):137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Nemeth E, Ganz T. Hepcidin‐Ferroportin interaction controls systemic iron homeostasis. Int J Mol Sci. 2021;22(12):6493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Ramsay AJ, Quesada V, Sanchez M, Garabaya C, Sardà MP, Baiget M, et al. Matriptase‐2 mutations in iron‐refractory iron deficiency anemia patients provide new insights into protease activation mechanisms. Hum Mol Genet. 2009;18(19):3673–3683. [DOI] [PubMed] [Google Scholar]
- 34. Pisani A, Riccio E, Sabbatini M, Andreucci M, Del Rio A, Visciano B. Effect of oral liposomal iron versus intravenous iron for treatment of iron deficiency anaemia in CKD patients: a randomized trial. Nephrol Dial Transplant. 2014;30(4):645–652. [DOI] [PubMed] [Google Scholar]
- 35. de Alvarenga Antunes CV, de Alvarenga Nascimento CR, da Rocha C, Ribeiro T, de Alvarenga AP, de Andrade CL, et al. Treatment of iron deficiency anemia with liposomal iron in inflammatory bowel disease: efficacy and impact on quality of life. International journal of. Clin Pharm. 2020;42(3):895–902. [DOI] [PubMed] [Google Scholar]
- 36. Ebea‐Ugwuanyi PO, Vidyasagar S, Connor JR, Frazer DM, Knutson MD, Collins JF. Oral iron therapy: current concepts and future prospects for improving efficacy and outcomes. Br J Haematol. 2024;204(3):759–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Pantopoulos K. Oral iron supplementation: new formulations, old questions. Haematologica. 2024;109(9):2790–2801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Nemeth E, Ganz T. Hepcidin and iron in health and disease. Annu Rev Med. 2023;74(1):261–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Ganz T, Nemeth E, Rivella S, Goldberg P, Dibble AR, McCaleb ML, et al. TMPRSS6 as a therapeutic target for disorders of erythropoiesis and iron homeostasis. Adv Ther. 2023;40(4):1317–1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Sagar P, Angmo S, Sandhir R, Rishi V, Yadav H, Singhal NK. Effect of hepcidin antagonists on anemia during inflammatory disorders. Pharmacol Ther. 2021;226:107877. [DOI] [PubMed] [Google Scholar]
- 41. van Santen S, Kroot JJ, Zijderveld G, Wiegerinck ET, Spaanderman ME, Swinkels DW. The iron regulatory hormone hepcidin is decreased in pregnancy: a prospective longitudinal study. Clin Chem Lab Med. 2013;51(7):1395–1401. [DOI] [PubMed] [Google Scholar]
- 42. Piskin E, Cianciosi D, Gulec S, Tomas M, Capanoglu E. Iron absorption: factors, limitations, and improvement methods. ACS Omega. 2022;7(24):20441–20456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Powers JM, Buchanan GR. Disorders of iron metabolism: new diagnostic and treatment approaches to iron deficiency. Hematol Oncol Clin North Am. 2019;33(3):393–408. [DOI] [PubMed] [Google Scholar]
- 44. Li N, Zhao G, Wu W, Zhang M, Liu W, Chen Q, et al. The efficacy and safety of vitamin C for iron supplementation in adult patients with iron deficiency anemia: a randomized clinical trial. JAMA Netw Open. 2020;3(11):e2023644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Stoffel NU, Zeder C, Brittenham GM, Moretti D, Zimmermann MB. Iron absorption from supplements is greater with alternate day than with consecutive day dosing in iron‐deficient anemic women. Haematologica. 2020;105(5):1232–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Koenig MD, Tussing‐Humphreys L, Day J, Cadwell B, Nemeth E. Hepcidin and iron homeostasis during pregnancy. Nutrients. 2014;6(8):3062–3083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Fisher AL, Nemeth E. Iron homeostasis during pregnancy. Am J Clin Nutr. 2017;106:1567S–1574S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Gaillard CA, Bock AH, Carrera F, Eckardt KU, Van Wyck DB, Bansal SS, et al. Hepcidin response to iron therapy in patients with non‐dialysis dependent CKD: an analysis of the FIND‐CKD trial. PLoS One. 2016;11(6):e0157063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Vlasveld LT, Janssen R, Bardou‐Jacquet E, Venselaar H, Hamdi‐Roze H, Drakesmith H, et al. Twenty years of Ferroportin disease: a review or an update of published clinical, biochemical, molecular, and functional features. Pharmaceuticals. 2019;12(3):132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Wish JB, Aronoff GR, Bacon BR, Brugnara C, Eckardt KU, Ganz T, et al. Positive iron balance in chronic kidney disease: how much is too much and how to tell? Am J Nephrol. 2018;47(2):72–83. [DOI] [PubMed] [Google Scholar]
- 51. Auerbach M, Macdougall IC. Safety of intravenous iron formulations: facts and folklore. Blood Transfus. 2014;12(3):296–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Gómez‐Ramírez S, Shander A, Spahn DR, Auerbach M, Liumbruno GM, Vaglio S, et al. Prevention and management of acute reactions to intravenous iron in surgical patients. Blood Transfus. 2019;17(2):137–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Caimmi S, Crisafulli G, Franceschini F, Liotti L, Bianchi A, Bottau P, et al. Hypersensitivity to intravenous iron preparations. Children (Basel). 2022;9(10):1473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Arastu AH, Elstrott BK, Martens KL, Cohen JL, Oakes MH, Rub ZT, et al. Analysis of adverse events and intravenous iron infusion formulations in adults with and without prior infusion reactions. JAMA Netw Open. 2022;5(3):e224488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Fortuny J, von Gersdorff G, Lassalle R, Linder M, Overbeek J, Reinold J, et al. Use of intravenous iron and risk of anaphylaxis: a multinational observational post‐authorisation safety study in Europe. Pharmacoepidemiol Drug Saf. 2021;30(10):1447–1457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Macdougall IC, White C, Anker SD, Bhandari S, Farrington K, Kalra PA, et al. Intravenous iron in patients undergoing maintenance hemodialysis. N Engl J Med. 2019;380(5):447–458. [DOI] [PubMed] [Google Scholar]
- 57. Schaefer B, Tobiasch M, Wagner S, Glodny B, Tilg H, Wolf M, et al. Hypophosphatemia after intravenous iron therapy: comprehensive review of clinical findings and recommendations for management. Bone. 2022;154:116202. [DOI] [PubMed] [Google Scholar]
- 58. Glaspy JA, Wolf M, Strauss WE. Intravenous iron‐induced hypophosphatemia: an emerging syndrome. Adv Ther. 2021;38(7):3531–3549. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1.