

ABSTRACT
Oral melanotic macules and primary oral malignant melanoma are distinct pigmented lesions that can present clinical challenges in diagnosis. While melanotic macules are generally benign, quite a few instances of progression to melanoma have been reported. We present the case of a 42-year-old female with gradually enlarging painless pigmented macules on her lips, diagnosed as oral melanotic macules after histopathological evaluation. Although no signs of melanocytic hyperplasia or dysplasia were found, the patient was closely monitored due to the lesion’s increasing size over 3 months. This case highlights the importance of distinguishing between benign pigmented lesions, which have a propensity to undergo malignant transformation from those that show no such tendency. Presences of histopathological features like atypical melanocytes and melanocytic hyperplasia/dysplasia in benign pigmented lesions are important markers for malignant transformation. Close clinical follow-up is essential to ensure timely intervention if the lesion exhibits suspicious changes.
Keywords: Malignant transformation, melanocytic dysplasia, melanoma, melanotic macule, peutz-jeghers syndrome, premalignant lesion
Introduction
Early detection and treatment of oral cancer significantly improve patient outcomes. Annually, about 377,713 new cases of oral cavity and lip cancers occur globally, leading to approximately 177,757 deaths.[1] India is known to have one of the highest incidences of oral cancer globally with 77,000 new cases reported every year.[1]
Oral melanotic macule and primary oral malignant melanoma are distinct oral pigmented lesions. The melanotic macule typically appears as a small, well-circumscribed, brown-to-black flat macule on the lip or mucous membranes, caused by increased melanin in the basal layer. Although generally benign, there has been a rare case reported where a benign macule progressed into malignant melanoma.[2] This creates a challenge in distinguishing between these lesions clinically.
Oral malignant melanoma, a rare neoplasm of melanocytes, accounts for less than 1% of melanomas and 0.5% of oral malignancies. It is aggressive with poor prognosis, having a 5-year survival rate of 10–25%.[3] Diagnosis is often delayed due to asymptomatic early stages, contributing to poor outcomes. Clinically, oral melanoma may resemble benign pigmented lesions, such as oral melanotic macules, making early diagnosis challenging.[4]
Histological examination is essential to differentiate between them. Oral melanomas exhibit atypical melanocyte proliferation at the epithelial-connective tissue junction, while oral melanotic macules show increased melanin without melanocyte proliferation.[5]
Melanocytic hyperplasia is another term that is characterized clinically by a flat, well-circumscribed macular lesion on the lips, buccal mucosa, and gingiva and is histologically characterized by melanocytic hyperplasia, that is, an actual increase in the number of melanocytes by proliferation. This is an important distinction and melanocytic hyperplasia can be considered as a transitional lesion between melanotic macule and melanoma.[2,4]
There is confusion as to whether a melanoma develops de novo or undergoes a transformation from a previously existing oral-pigmented lesion like a macule or melano-acanthoma. Many authors have suggested that the melanomas, which develop from an existing or pre-existing pigmented lesion usually undergo molecular changes (like melanocytic hyperplasia) induced by chemicals, stress, etc., or can be spontaneous or iatrogenic, before taking the form of an aggressive melanoma.[4]
Although melanotic macules and melanocytic hyperplasia are clinically benign lesions, few reported cases suggest potential malignant transformation, underscoring the importance of careful clinical and histological evaluation.[5] The primary care physicians will be amongst the first to encounter patients with oral-pigmented macules. Keeping in mind the potential of these pigmented lesions to undergo malignant transformation, primary care physicians play a pivotal role in identifying such lesions, providing primary care, and ensuring proper referral to higher centers. Herein we report a case of an oral melanotic macule.
Case Report
A 42-year-old female patient reported to the out-patient department (OPD) of a tertiary care center in Siliguri, West Bengal with a chief complaint of blackish discoloration in her upper and lower lip that has been gradually increasing in size since last 3 months [Figure 1]. She had no relevant medical or drug history. She reported that she did not have the black discoloration since birth; she noticed them approximately 5 years back when they appeared suddenly on both lips. She could not recall any history of trauma or external injury. Over the last 3 months, there has been a sudden increase in the size and extent of the lesion for which she reached out.
Figure 1.

Showing the extra-oral presentation of the patient
Clinical evaluation of the lesion revealed diffuse, flat, and circumscribed blackish pigmented macules measuring approximately 2 × 1 cm in the upper right labial mucosa in relation to 11, 12, and 13. Similar lesions were appreciated on both right and left lower labial mucosa, measuring from 0.5 × 1 cm in diameter. On palpation, both the lesions on the upper and lower labial mucosa appeared non-tender, non-scrappable, and no blanching was elicited on compression. Regional lymph nodes were non-palpable. A provisional diagnosis of melanotic macule was given [Figure 2].
Figure 2.
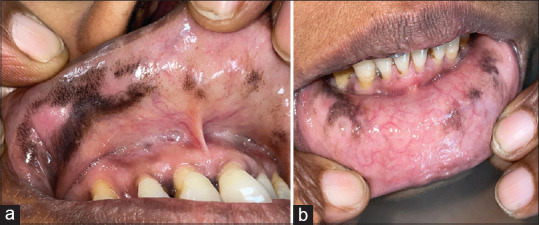
Showing the intra-oral presentation of the patient in the upper lip (a) and the lower lip (b)
As the lesion was slowly expanding during the last 3 months, there was a need to rule out melanocytic hyperplasia and/or melanoma. An incisional biopsy was performed on the lesion in the upper labial mucosa after obtaining informed consent from the patient. Haemotoxylin and eosin-stained specimens of the sub-site revealed the presence of stratified squamous epithelium backed by fibrous connective tissue stroma. The juxta-epithelial region shows the presence of diffuse melanin pigmentation along with the presence of melanocytes and melanophages (macrophages that engulf the melanin pigment). Multiple nests of melanin pigment with epithelial cells can be appreciated in the epithelium. No evidence of melanocytic hyperplasia or dysplasia could be appreciated [Figure 3]. A final diagnosis of oral melanotic macule was given.
Figure 3.
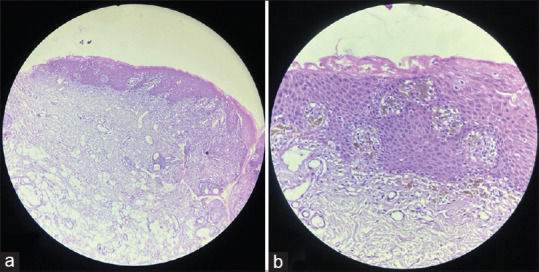
Showing the photomicrograph of the H and E stained section of the specimen that reveals the presence of stratified squamous epithelium backed by fibrous connective tissue stroma. The juxta-epithelial region shows the presence of diffuse melanin pigmentation along with the presence of melanocytes and melanophages under 10X (a) and 40× (b). Multiple nests of melanin pigment with epithelial cells can be appreciated in the epithelium
The patient was put under rigid follow-up. No change in lesion size or extent has been noted in the last 12 months.
Discussions
Melanocytes, derived from neuroectodermal cells, typically migrate to areas like the skin, retina, and uveal tract, which are all derived from ectodermal tissues. Although less frequently, melanocytes can also migrate to endodermal tissues such as the nasopharynx, larynx, esophagus, and oral cavity, allowing melanotic macules and/or melanoma to develop on mucosal surfaces, although it most commonly occurs on the skin.[6] Mucosal melanotic lesions (including melanomas) primarily appear in the head and neck region (55.4%), with a significant occurrence in the anal/rectal region (23.8%). Specific to the head and neck region, the nasal cavity, paranasal sinuses, and oral cavity are frequent sites.[7]
Although melanomas are rare, accounting for only 0.5% of all oral malignancies, the absence of a definitive precursor lesion and the rapid progression of oral melanoma highlight the importance of early detection and regular follow-up.[8] Oral melanotic macule has been historically considered a benign lesion without malignant potential. However, some case reports suggest that melanotic macules might carry a risk of developing into oral melanoma. Considering the high frequency of melanotic macules in the oral cavity, their potential for malignant transformation should be carefully monitored.[9]
The clinical significance of encountering an intra-oral pigmented lesion lies in ruling out melanoma, which is associated with a high mortality rate. Melanoma is an aggressive malignant neoplasm, characterized by uncontrolled proliferation of atypical melanocytes.[10] The exact cause of melanoma is not well understood, and it typically develops spontaneously (de novo). However, some studies have noted that a significant portion of oral melanoma patients (30%) presented with pigmented lesions months or even years before receiving a formal melanoma diagnosis.[11] Other reports suggest that 35–37% of oral melanoma patients had pre-existing pigmented lesions before their diagnosis, highlighting the importance of monitoring such lesions. Despite this correlation, many of these studies lack detailed histopathological data on these pre-existing pigmentations, complicating a clear understanding of their role in melanoma development.[8,11]
It has been postulated by researchers[2,3,4,9] that when the initial presentation of a lesion is that of a flat, well-circumscribed pigmented one, it harbors the inherent potential for malignant transformation. This can be histopathologically elicited as melanocytic hyperplasia. Unlike the previous concept, that melanomas develop de novo intra-orally, it can be hypothesized that melanomas are preceded by oral melanotic macules or melano-acanthoma, having melanocytic hyperplasia and/or dysplasia instead of having the same number of typical melanocytes with an increased tendency to synthesize melanin pigment. However, the possibility that melanomas can develop de novo is not completely being ruled out.[12]
As the present case report lacked evidence of melanocytic hyperplasia/dysplasia histologically, complete lesion excision was not done and she was only put under follow-up. Literature suggests that the development of melanocytic changes (atypical, hyperplasia, and dysplasia) can be induced by trauma, chemicals, drugs, radiation, stress, etc. In such instances, the lesion undergoes a drastic change in its size and extent. The criteria to clinically diagnose a rapidly spreading pigmented lesion are[13]
Diffuse outline
Sudden increase in size and extent
Deepening of the pigment color of the lesion
Raised lesion instead of a flat one
Nodular, rough, and irregular surface.
These changes should raise suspicion for malignant transformation of any pre-existing benign pigmented lesion and intervention should be mandated. During the course of the follow-up of the present case, no such changes could be elicited clinically.
Histopathological examinations are critical for diagnosing both oral melanotic macules and melanoma. In a typical case, the former will show typical melanocytes with an increased volume of melanin pigment that can be distributed throughout the epithelium and the latter will show increased melanin deposition along the basal cell layer, atypical melanocytes with nuclear pleomorphism, hyperchromatism, and the absence of rete ridges in the affected tissue. These abnormal cells often form prominent nests within the tissue.[8,13]
In terms of diagnostic tools, hematoxylin and eosin (H and E) staining, along with immunohistochemical staining using markers like HMB-45, S100, and Melan A, are essential for identifying oral melanoma. These tools are useful for distinguishing melanomas from other types of tumors but do not differentiate between melanomas and melanotic macules. In cases where lesions are large, biopsies from multiple areas are recommended to avoid missed diagnoses, which can result in poor prognosis due to late detection.[14]
A notable distinction between oral melanotic macule and primary oral melanoma was observed in terms of age, gender, and lesion location. Routine biopsies are recommended for suspected melanotic macules, particularly in men over 60 years, to exclude melanoma. While melanomas are more common on the palate and gingiva, melanotic macules are more frequently seen on the upper and lower lip, tongue, etc.[12]
Diffuse oral melanosis can also be observed in endocrine disorders like Cushing’s, Grave’s, and Addison’s disease but it is also accompanied by cutaneous bronze pigmentation. Peutz-jeghers syndrome consists of a triad of oral melanosis, intestinal polyposis, and cutaneous pigmentation. The patient reported in the present case showed no evidence of any cutaneous pigmentation, neither any evidence of endocrine deficiencies. Palatal melanosis is a common finding among smokers (normal/reverse). Another form of mucosal melanosis that is closely associated with auto-immune/vesiculobullous lesions in the healing stage is post-inflammatory pigmentation. The possibility of both can be ruled out in the present case as the patient gave no history of tobacco usage in any form; neither any vesiculobullous lesion could be identified intra-orally.[8,14]
Treatment for oral melanotic macule and melanoma involves surgical excision of the lesion, often combined with other therapies. The high morbidity and mortality in melanoma patients are primarily due to late diagnosis, with more than two-thirds identified at an advanced stage. Early diagnosis is critical for improving the prognosis. The clinical outcome for oral melanoma tends to be poor, with a 5-year disease-free survival rate ranging from 15% to 40%, largely due to late-stage detection. On early detection, a 5-year disease-free survival of 80–90% has been reported.[15] This difference is significant and herein lies the importance of early detection. If melanoma is preceded by any pigmented oral lesion, then early interception becomes possible. Thus proper understanding of the exact pathogenesis of melanoma is crucial in providing early detection. This paper has attempted to throw light on the same.
Oral melanotic lesions usually account for 15–20% of all the intra-oral lesions and more often than not, such pigmented lesions are first confronted by the primary care physicians.[16] Once the endocrine, post-inflammatory, and tobacco-related causes are excluded, it is imperative for primary care physicians to consider the inherent malignant potential of such pigmented lesions (melanotic macule/melano-acanthoma) to develop into melanoma and exercise caution with immediate effect for early detection and interception. The aggressive nature of oral melanoma makes it vital for primary care physicians to pay close attention to pigmented lesions in the oral cavity.
Conclusion
While oral melanotic macules have long been considered benign, emerging evidence suggests that some of these lesions may carry malignant potential. Given the poor prognosis of oral melanoma, early detection and treatment are essential. The clinical characteristics of melanotic macules observed in the present case report were consistent with existing literature, with a notable higher prevalence in women, typically in their fourth to fifth decade of life. Another relevant point that has been highlighted in the present case report is whether melanotic macules with melanocytic hyperplasia/dysplasia can be considered as premalignant lesions/precursor lesions/transitional lesions for the development of future melanomas.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of interest
There are no conflicts of interest.
Funding Statement
Nil.
References
- 1.Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. doi: 10.3322/caac.21660. [DOI] [PubMed] [Google Scholar]
- 2.Kahn MA, Weathers DR, Hoffman JG. Transformation of a benign oral pigmentation to primary oral melanoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:454–9. doi: 10.1016/j.tripleo.2005.01.018. [DOI] [PubMed] [Google Scholar]
- 3.Kaugars GE, Heise AP, Riley WT, Abbey LM, Svirsky JA. Oral melanotic macules: A review of 353 cases. Oral Surg Oral Med Oral Pathol. 1993;76:59–61. doi: 10.1016/0030-4220(93)90295-f. [DOI] [PubMed] [Google Scholar]
- 4.Gupta G, Williams RE, Mackie RM. The labial melanotic macule: A review of 79 cases. Br J Dermatol. 1997;136:772–5. [PubMed] [Google Scholar]
- 5.Mukherjee D. Pigmented lesions of the oral cavity –A brief review. J Dent Res Rev. 2020;7:228–31. [Google Scholar]
- 6.Allen AC, Spitz S. Malignant melanoma;A clinicopathological analysis of the criteria for diagnosis and prognosis. Cancer. 1953;6:1–45. doi: 10.1002/1097-0142(195301)6:1<1::aid-cncr2820060102>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 7.Resende NM, Vasques Bittencourt F, Gontijo B. Congenital melanocytic macule of the tongue: A 5-year follow-up. Dermatol Pract Concept. 2021;11:e2021122. doi: 10.5826/dpc.1104a122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shen ZY, Liu W, Bao ZX, Zhou ZT, Wang LZ. Oral melanotic macule and primary oral malignant melanoma: Epidemiology, location involved, and clinical implications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:e21–5. doi: 10.1016/j.tripleo.2011.02.040. [DOI] [PubMed] [Google Scholar]
- 9.Buchner A, Hansen LS. Melanotic macule of the oral mucosa. A clinicopathologic study of 105 cases. Oral Surg Oral Med Oral Pathol. 1979;48:244–9. doi: 10.1016/0030-4220(79)90011-2. [DOI] [PubMed] [Google Scholar]
- 10.Kumari N, Agarwal N, Tripathi P, Siddhartha V, Shukla S, Naaz S. Pigmented lesions of the oral cavity: A review. Saudi J Oral Dent Res. 2022;7:276–9. [Google Scholar]
- 11.Carlos-Bregni R, Contreras E, Netto AC, Mosqueda-Taylor A, Vargas PA, Jorge J, et al. Oral melanoacanthoma and oral melanotic macule: A report of 8 cases, review of the literature, and immunohistochemical analysis. Med Oral Patol Oral Cir Bucal. 2007;12:E374–9. [PubMed] [Google Scholar]
- 12.Ho KK, Dervan P, O’Loughlin S, Powell FC. Labial melanotic macule: A clinical, histopathologic, and ultrastructural study. J Am Acad Dermatol. 1993;28:33–9. doi: 10.1016/0190-9622(93)70005-e. [DOI] [PubMed] [Google Scholar]
- 13.Kim SH, Byun JS, Jung JK, Choi JK. Simultaneous occurrence of melanotic macule and melanoma in the oral cavity: A case report. J Oral Med Pain. 2020;45:71–8. [Google Scholar]
- 14.Umeda M, Komatsubara H, Shibuya Y, Yokoo S, Komori T. Premalignant melanocytic dysplasia and malignant melanoma of the oral mucosa. Oral Oncol. 2002;38:714–22. doi: 10.1016/s1368-8375(02)00008-8. [DOI] [PubMed] [Google Scholar]
- 15.Geum DH, Roh YC, Yoon SY, Kim HG, Lee JH, Song JM, et al. The impact factors on 5-year survival rate in patients operated with oral cancer. J Korean Assoc Oral Maxillofac Surg. 2013;39:207–16. doi: 10.5125/jkaoms.2013.39.5.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Patrick RJ, Fenske NA, Messina JL. Primary mucosal melanoma. J Am Acad Dermatol. 2007;56:828–34. doi: 10.1016/j.jaad.2006.06.017. [DOI] [PubMed] [Google Scholar]