

ABSTRACT
Introduction
“Delayed” antibody‐mediated xenograft rejection is one of the most important obstacles to clinical application of pig organ xenografts. The aim of this study was to assess the impact of a structured desensitization regimen including proteasome inhibition and next‐generation costimulation blockade on xenoreactive antibodies.
Methods
Rhesus macaques with moderate‐high pre‐treatment xenoreactive antibody titers (N = 2) were selected. Recipients received twice‐weekly carfilzomib (20 mg/m2), anti‐CD154 (20 mg/kg) every other week, and CD4 and CD20 lymphocyte cell depletion. Bone marrow was acquired to assess plasma cell depletion in response to proteasome inhibition. A flow cytometry‐based xenoreactive crossmatch assay was performed to assess levels of circulating xenoreactive antibodies.
Results
The desensitization regimen resulted in a >50% depletion of CD38+CD27+ bone marrow plasma cells; these changes were progressive over the duration of the desensitization treatment period. The desensitization strategy and plasma cell depletion resulted in a progressive reduction in anti‐pig IgG antibodies. Following xenotransplantation, both desensitized recipients demonstrated superior graft survival to a highly xenoreactive recipient (MST 30 days vs. 6 days), but neither desensitized recipient experienced prolonged graft survival.
Conclusions
A structured desensitization regimen including proteasome inhibition and costimulation blockade results in plasma cell depletion and resultant reduction in circulating xenoreactive anti‐pig IgG antibodies, with a modest improvement in xenograft survival. This desensitization regimen has promise for pig‐to‐NHP xenotransplant models.
Keywords: antibody, proteasome inhibition, xenotransplantation
1. Introduction
The presence of strong anti‐donor antibodies represents a formidable barrier in solid organ transplantation. For patients on the waiting list, broad levels of sensitization considerably prolong waiting times, and preformed anti‐donor antibodies increase the risk of antibody‐mediated rejection (ABMR) after receipt of a transplant [1]. For patients with an existing graft, de novo antibody formation poses the risk of graft injury and potential graft loss. ABMR contributes to both short‐ and long‐term injury in up to 10% of recipients [2].
ABMR is a significant barrier in xenotransplantation as well. Though screening for preformed xenoreactive IgG has been shown to mitigate early xenograft injury [3, 4], humans and nonhuman primates possess significant amounts of anti‐porcine antibodies recognizing both Gal and non‐Gal antigens. However, commonly used pre‐transplant desensitization therapies, including IVIG, plasmapheresis, and rituximab, do not impact the cellular source of IgG production [5].
It has been demonstrated that plasma‐cell‐based therapies using proteasome inhibition are an effective strategy for pre‐transplant desensitization, with sensitized transplant patients demonstrating a significant reduction in anti‐HLA antibody levels when used as part of a pre‐transplant desensitization strategy [5, 6, 7, 8, 9]. Carfilzomib, a second‐generation irreversible proteasome inhibitor, has shown promise in promoting IgG desensitization in human allotransplantation [5]. The aim of this study was to assess the efficacy of a proteasome inhibitor‐based multimodal desensitization protocol in a pig‐to‐nonhuman primate xenotransplant model, as well as the impact of this desensitization strategy on xenograft outcomes. We hypothesize that the proteasome inhibitor‐based desensitization will reduce humoral xenoreactivity and prolong xenograft survival among highly xenoreactive recipients.
2. Methods
2.1. Animals
The care and treatment of animals used in this study was conducted with the approval of the Emory University Institutional Animal Care and Use Committee in adherence with the Guide for the Care and Use of Laboratory Animals (Institute of Laboratory Animal Resources, National Research Council, US Department of Health and Human Services).
αGal knockout/CD55 transgenic pigs (α‐1,3‐galactosyltransferase knockout, human decay‐accelerating factor transgenic), aged 10–14 weeks, were obtained from the National Swine Resource and Research Center (University of Missouri‐Columbia, Columbia, MO, USA) to serve as kidney donors. Juvenile rhesus macaques (Macaca mulatta) were obtained from breeding colonies at Yerkes National Primate Research Center (Lawrenceville, GA, USA) or AlphaGenesis, Inc. (Yemassee, SC, USA).
Recipients were screened based on preformed IgG serum antibody levels against porcine αGal knockout cells using a flow cytometry‐based assay as described below. Monkeys were stratified as either low xenoreactive IgG antibody titer or moderate‐high xenoreactive IgG antibody titer.
2.2. Flow Cytometry‐Based Xenoreactive Crossmatch
Indian Rhesus Macaques (M. mulatta) were assessed for xenoreactive IgG antibody titer against porcine αGal knockout cells using a flow cytometric crossmatch (FCXM). Briefly, peripheral blood mononuclear cells (PBMCs) from αGal knockout/CD55 transgenic pigs (α‐1,3‐galactosyltransferase knockout, human decay‐accelerating factor transgenic) were incubated with IgM heat‐inactivated rhesus macaque serum, allowing for rhesus IgG coating of the cells. Cells were then stained with goat anti‐monkey IgG (KPL/SeraCare, Milford, MA, USA). Flow cytometry results were reported as molecules of equivalent soluble fluorochrome (MESF).
2.3. Desensitization Treatment Regimen
Two (2) immunologically naïve rhesus macaques with moderate‐high xenoreactive IgG antibody titers were selected for desensitization therapy. These macaques received in vivo treatment with a combination of carfilzomib (Selleck Chemicals LLC; Houston, TX, USA) 20 mg/m2 IV twice weekly, anti‐CD154 (clone 5C8, Nonhuman Primate Reagent Resource [NHPRR]; Boston, MA, USA) 20 mg/kg IV every other week [4, 10, 11, 12], and anti‐CD4mAb (clone CD4R1; NHPRR) 50 mg/kg IV and anti‐CD20mAb 50 mg/kg (clone 2B8R1; NHPRR) every 4 weeks (Figure 1). Xenoreactive FCXM antibody titer tests were conducted weekly during desensitization. Bone marrow biopsies of the recipient humerus were performed at regular intervals to assess plasma cell populations using a 20‐gauge CareFusion Bone Marrow Biopsy/Aspiration Needle.
FIGURE 1.
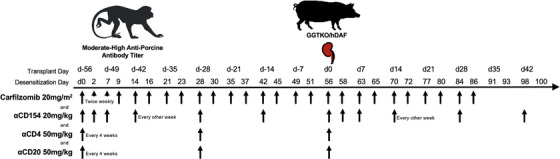
Proteasome inhibitor‐based desensitization protocol dosing regimen. Moderate‐high xenoreactive rhesus macaques received an 8‐week desensitization protocol including twice weekly carfilzomib, biweekly costimulation blockade (CD154 mAb), and CD4 and CD20 depleting antibody therapy every 4 weeks. Carfilzomib was continued for 4 weeks post‐transplant.
2.4. Rhesus Macaque Transplants
Donor transgenic pigs underwent bilateral nephrectomy on the day of transplantation (Division of Animal Resources, Emory University, Atlanta, GA, USA). The recipient rhesus macaques then underwent bilateral nephrectomy followed by life‐sustaining renal transplantation with a donor porcine kidney (Yerkes National Primate Research Center, Emory University, Atlanta, GA, USA). Post‐operatively, graft function was monitored with daily urine output assessment and weekly serum chemistries. Veterinary staff examined animals on a daily basis and was available for consultation. Peripheral blood and bone marrow were collected at regular intervals for cell subset analysis using single‐cell flow cytometry (FlowJo LLC; Ashland, OR, USA) and visual stochastic neighbor embedding (viSNE; Cytobank, Inc., Santa Clara, CA, USA). Quantitative cytomegalovirus (CMV) titers were measured weekly using a polymerase chain reaction‐based assay. Protocol renal biopsies under ultrasound guidance with a 20‐gauge CareFusion Achieve Soft Tissue Automatic Biopsy Needle were performed on post‐operative days (PODs) 14 and 35 as well as at times of suspected rejection. Biopsies were analyzed using standard H&E and immunohistochemistry and histologic analysis was performed by a blinded renal pathologist.
3. Results
3.1. Pre‐Transplant Plasma Cell Depletion and Desensitization
Prior to initiation of desensitization, high‐dimensional single‐cell analysis of the humerus bone marrow of both rhesus macaques revealed a robust CD19+CD20−CD38+CD27+IgM−IgD− cell population consistent with bone marrow antibody‐secreting plasma cells (Figure 2A, baseline). Administration of the combination proteasome inhibition‐costimulation blockade desensitization regimen resulted in a progressive reduction in the plasma cell compartment of each recipient during the 8‐week desensitization period. Bone marrow cell analysis by viSNE demonstrated a marked longitudinal change in the CD19 lineage repertoire during desensitization, with a decrease in a CD27+CD38+ memory ASC cell population and increased heterogeneity of the remaining CD19+ cells representing a less mature/differentiated B cell phenotype (Figure 2B).
FIGURE 2.
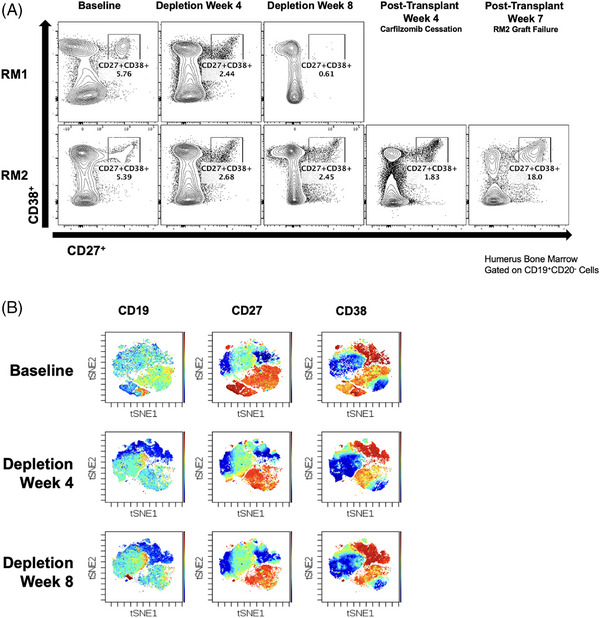
Bone marrow plasma cell sampling. Recipients on the desensitization protocol received protocol percutaneous humerus bone marrow biopsies every4 weeks during therapy. (A) Both recipients demonstrated a reduction in CD19+CD20−CD38+CD27+IgM−IgD− plasma cells during the course of their desensitization, which rebounded in RM2 after cessation of carfilzomib treatment. (B) Bone marrow biopsies demonstrated reduction in CD19+, CD27+, and CD38+ cells using viSNE analysis.
Following anti‐CD20 depleting antibody therapy, peripheral B cells remained nearly undetectable throughout the desensitization course (Figure S1). Concomitant plasma cell reduction via proteasome inhibition and B cell reduction via anti‐CD20 depleting therapeutic antibodies resulted in a reduction in circulating peripheral xenoreactive IgM and IgG as measured in the recipient serum (Figure 3). When compared to highly xenoreactive rhesus historic controls with early xenograft failure, recipients treated with the desensitization regimen had a notable reduction in IgG, with a 26.8% and 54.4% IgG reduction for RM1 and RM2, respectively, as well as IgM, with a 48.2% and 68.7% IgM reduction for RM1 and RM2, respectively. The post‐desensitization immunoglobulin levels approximated the levels of historic low xenoreactive rhesus historic controls who experienced prolonged xenograft survival.
FIGURE 3.
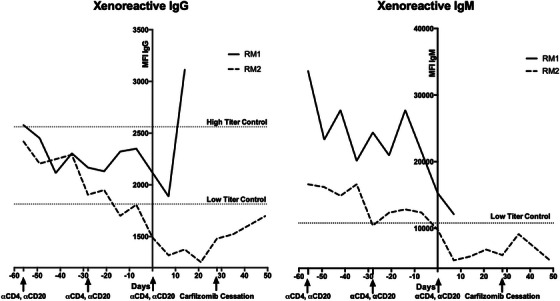
Xenoreactive IgG and IgM antibody titers. Recipients demonstrated a progressive reduction in both IgG and IgM xenoreactive antibody titers throughout the course of the pre‐transplant desensitization regimen. RM2 demonstrated rebound IgG after cessation of carfilzomib therapy.
During the pre‐transplant desensitization regimen, both recipients were noted to have low‐level CMV reactivation (data not shown), indicating nonspecific loss of protective immunity. Neither recipient demonstrated adverse clinical effects of viremia, and both were easily treated with antiviral (ganciclovir, valganciclovir) therapies to the resolution of viremia.
3.2. Post‐Desensitization Kidney Xenotransplant
Following the 8‐week desensitization protocol, both recipients underwent life‐sustaining renal xenotransplantation. Both desensitized recipients demonstrated superior graft survival to the highly xenoreactive control xenograft recipient (MST 30 days vs. 6 days), but neither desensitized recipient experienced prolonged graft survival to the degree of their low xenoreactive titer control counterparts (Figure 4A). RM1, the recipient with higher baseline xenoreactive IgG and IgM serum titer, demonstrated graft failure at post‐transplant Day 12 with histologic features consistent with acute antibody‐mediated xenorejection (ABMR), including severe interstitial hemorrhage, thrombotic microangiopathy (TMA), and arteritis (Figure 4B). RM2 demonstrated longer post‐transplant survival to 48 days before developing xenograft rejection, similarly, with histologic features consistent with acute ABMR. RM2's protocol renal biopsies at post‐transplant Days 14 and 25 demonstrated early vascular rejection, though the recipient's labs demonstrated adequate renal function. RM2 also demonstrated a progressive IgG reconstitution (Figure 3A) following cessation of proteasome inhibition at post‐transplant Week 4. This corresponded with a significant increase in bone marrow plasma cells between cessation of carfilzomib therapy at post‐transplant Week 4 and graft failure at post‐transplant Week 7 (Figure 2A).
FIGURE 4.
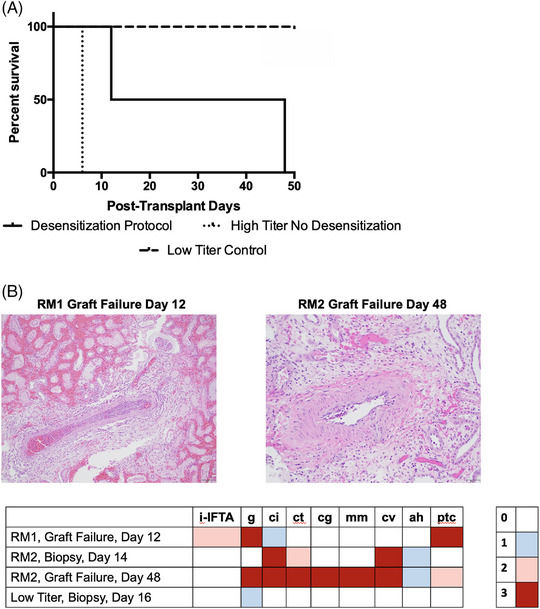
Xenograft survival and histology. (A) Desensitized recipients exhibited improved graft survival relative to highly xenoreactive controls (MST 30 vs. 6 days). (B) Histology at time of rejection revealed features consistent with ABMR in the desensitized recipients, while low‐titer controls had normal kidney architecture and physiology.
4. Discussion
Dual targeting of antibody‐secreting cells via a combination of proteasome inhibition, targeting the IgG‐producing plasma cell, and anti‐CD20, targeting the IgM‐producing B cell, resulted in relative reductions of circulating xenoreactive antibodies. The evidence provided in this study shows a significant reduction in levels of xenoreactive IgM antibodies, xenoreactive IgG antibodies, and IgG‐producing plasma cells within the bone marrow of monkeys treated with a proteasome inhibition‐based desensitization protocol. Xenotransplantation of the desensitized recipients yielded mixed results. Both desensitized recipients demonstrated superior graft survival to the highly xenoreactive control recipient, but neither was able to achieve long‐term xenograft survival. The results of this proteasome inhibitor‐based desensitization protocol study represent a potential avenue for reducing xenoreactive antibody levels, either as a pre‐operative induction strategy or as a post‐operative method to mediate chronic ABMR.
The results presented in this study are consistent with those observed with proteasome inhibition other nonhuman primate allotransplant models. Knechtle et al. demonstrated reductions in donor specific antibody (DSA), germinal center B cells and follicular helper T cells (Tfh) associated with combination bortezomib and costimulation blockade‐based desensitization [13, 14]. However, the opposite effect, with paradoxical increases in germinal center and Tfh activity, was observed in animals treated with bortezomib monotherapy [15]. Among allosensitized human patients treated with bortezomib monotherapy, Hara et al. demonstrated minimal reduction in xenoreactive antibody levels [16]. The observations in these studies, as well as the present study, elicit several critical questions will drive further xenotransplant desensitization studies. First, the previously mentioned studies all employed bortezomib, a first‐generation, reversible PI, which has reduced efficacy to the second‐generation, irreversible PI carfilzomib employed in the present study. The difference in reversible‐irreversible binding between the first‐ and second‐generation PIs may be more efficacious in constitutive inhibition of the proteasome effect. This is consistent with results recently reported by Tremblay et al. in an HLA‐sensitized human sample, where carfilzomib monotherapy leads to a >50% reduction in alloreactive antibody, 70% reduction in bone marrow plasma cells, and reduction in cPRA. Similar to the results in the present study, they also reported the development of rebound IgG antibody after cessation of carfilzomib therapy [5]. Second, concomitant treatment with PI and costimulation blockade yielded improved efficacy of PI therapy in reducing circulating DSA levels and inhibiting the humoral cellular machinery. Knechtle's recent experience using carfilzomib plus costimulation blockade as a desensitization regimen in the sensitized allotransplant setting has shown promise, with reductions in DSA and bone marrow plasma cells and improved allograft survival, though rebound DSA development and ABMR after cessation of PI therapy were again seen [17, 18]. This regimen has also been used to treat ABMR in their highly‐sensitized NHP allograft cohort [19]. Improved understanding of the immune mechanisms of costimulation blockade on this humoral compensation will further elucidate the translational impact of PI‐based desensitization regimens.
Proteasome inhibition interferes with cell homeostasis through dysregulation of ubiquitinated protein degradation, leading to accumulation of unfolded proteins and apoptotic cell death [20, 21]. While plasma cells are particularly susceptible given their high volume of immunoglobulin protein synthesis, other immune cells have shown susceptibility. There is also evidence that PIs may influence antibody production by B cells, apoptosis of activated T cells, reduced Th1 differentiation, cytokine expression, and maturation of dendritic cells [21, 22, 23]. It is postulated that a similar desensitization protocol could be used for the treatment of post‐transplant xenoreactive ABMR, though the long interval of desensitization therapy utilized in this study is a challenge to treatment of typically rapid‐onset xenograft rejection. PI therapy as rescue therapy for ABMR has previously been used in the post‐transplant human allotransplant, with promising results for early ABMR but mixed effects on late or chronic ABMR [24, 25, 26]. The variance in efficacy of proteasome inhibition for treatment of ABMR is presumed to be related to the heterogeneity in the ABMR spectrum and differences in underlying pathophysiology [21].
The limitations of this study should be noted. First, this is a single‐arm study of a small number of highly xenoreactive recipient, and we have not compared this desensitization protocol to alternative desensitization treatment schedules or therapies. Second, the longitudinal decrease in xenoreactive IgG and IgM antibodies is subject to in vitro artifacts in binding properties that may influence the median fluorescence intensity readings. To minimize these artifacts, serum samples were tested in serial dilutions to control for prozone effects, and longitudinal samples were tested retrospectively in batches to preclude day‐to‐day variations in test results.
5. Conclusion
In conclusion, this study demonstrates a beneficial impact of a proteasome inhibitor‐based desensitization regimen on reducing xenoreactive antibody levels and bone marrow plasma cell populations. Improved understanding of the immune mechanisms of xenoreactive ABMR with PI therapy, and further optimization of desensitization protocols, may improve xenograft survival by protecting organs from acute/chronic xenograft injury and dysfunction.
Supporting information
Supporting Information
{kind=link}
Acknowledgments
Research reported in this publication was supported by NIAID of the National Institutes of Health under award number 5U01AI126322 (A.B.A., A.J.T.).
Funding: Research reported in this publication was supported by NIAID of the National Institutes of Health under award number 5R01AI126322 (A.B.A.).
References
- 1. Montgomery R. A., Loupy A., and Segev D. L., “Antibody‐Mediated Rejection: New Approaches in Prevention and Management,” American Journal of Transplantation 18 (2018): 3–17, 10.1111/ajt.14584. [DOI] [PubMed] [Google Scholar]
- 2. Chehade H. and Pascual M., “The Challenge of Acute Antibody‐Mediated Rejection in Kidney Transplantation,” Transplantation 100, no. 2 (2016): 264–265, 10.1097/TP.0000000000000959. [DOI] [PubMed] [Google Scholar]
- 3. Higginbotham L., Mathews D., Breeden C. A., et al., “Pre‐Transplant Antibody Screening and Anti‐CD154 Costimulation Blockade Promote Long‐Term Xenograft Survival in a Pig‐to‐Primate Kidney Transplant Model,” Xenotransplantation 22, no. 3 (2015): 221–230, 10.1111/xen.12166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Kim S. C., Mathews D. V., Breeden C. P., et al., “Long‐Term Survival of Pig‐to‐Rhesus Macaque Renal Xenografts Is Dependent on CD4 T Cell Depletion,” American Journal of Transplantation 19, no. 8 (2019): 2174–2185, 10.1111/ajt.15329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tremblay S., Driscoll J. J., Rike‐Shields A., et al., “A Prospective, Iterative, Adaptive Trial of Carfilzomib‐Based Desensitization,” American Journal of Transplantation 20, no. 2 (2020): 411–421, 10.1111/ajt.15613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Dhillon M., Kobashigawa J. A., Kittleson M., et al., “Does Bortezomib Influence Pre‐Transplant Desensitization Therapy or Benefit Post‐Heart Transplant Outcomes for Highly Sensitized Patients?,” Clinical Transplantation 38, no. 1 (2024): e15165, 10.1111/ctr.15165. [DOI] [PubMed] [Google Scholar]
- 7. Fida N., Eagar T. N., Yun A. N., et al., “Effectiveness of Combined Plasma Cell Therapy and Costimulation Blockade Based Desensitization Regimen in Heart Transplant Candidates,” Clinical Transplantation 38, no. 2 (2024): e15249, 10.1111/ctr.15249. [DOI] [PubMed] [Google Scholar]
- 8. Philogene M. C., Sikorski P., Montgomery R. A., Leffell M. S., and Zachary A. A., “Differential Effect of Bortezomib on HLA Class I and Class II Antibody,” Transplantation 98, no. 6 (2014): 660–665, 10.1097/TP.0000000000000132. [DOI] [PubMed] [Google Scholar]
- 9. Woodle E. S., Shields A. R., Ejaz N. S., et al., “Prospective Iterative Trial of Proteasome Inhibitor‐Based Desensitization,” American Journal of Transplantation 15, no. 1 (2015): 101–118, 10.1111/ajt.13050. [DOI] [PubMed] [Google Scholar]
- 10. Adams A. B., Kim S. C., Martens G. R., et al., “Xenoantigen Deletion and Chemical Immunosuppression Can Prolong Renal Xenograft Survival,” Annals of Surgery 268, no. 4 (2018): 564–573, 10.1097/SLA.0000000000002977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Adams A. B., Lovasik B. P., Faber D. A., et al., “Anti‐C5 Antibody Tesidolumab Reduces Early Antibody‐Mediated Rejection and Prolongs Survival in Renal Xenotransplantation,” Annals of Surgery 274, no. 3 (2021): 473–480, 10.1097/SLA.0000000000004996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Anwar I. J., DeLaura I., Ladowski J. M., et al., “CD154 Blockade Effectively Controls Antibody‐Mediated Rejection in Highly Sensitized Nonhuman Primate Kidney Transplant Recipients,” Science Translational Medicine 17, no. 779 (2025): eadn8130, 10.1126/scitranslmed.adn8130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Knechtle S. J., Burghuber C. K., Manook M., et al., “Dual Targeting: Combining Costimulation Blockade and Bortezomib to Permit Kidney Transplantation in Sensitized Recipients,” American Journal of Transplantation 19, no. 3 (2019): 724–736, 10.1111/ajt.15067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Knechtle S. J., Kwun J., Burghuber C., et al., “Successful Desensitization With Proteasome Inhibition and Costimulation Blockade in Sensitized Nonhuman Primates,” Blood Advances 1, no. 24 (2017): 2115–2119, 10.1182/bloodadvances.2017010991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kwun J., Burghuber C., Manook M., et al., “Humoral Compensation After Bortezomib Treatment of Allosensitized Recipients,” Journal of the American Society of Nephrology 28, no. 7 (2017): 1991–1996, 10.1681/ASN.2016070727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hara H., Bentall A., Long C., et al., “Minimal Effect of Bortezomib in Reducing Anti‐Pig Antibodies in Human Leukocyte Antigen‐Sensitized Patients: A Pilot Study,” Xenotransplantation 20, no. 6 (2013): 429–437, 10.1111/xen.12052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Ezekian B., Schroder P. M., Mulvihill M. S., et al., “Pretransplant Desensitization With Costimulation Blockade and Proteasome Inhibitor Reduces DSA and Delays Antibody‐Mediated Rejection in Highly Sensitized Nonhuman Primate Kidney Transplant Recipients,” Journal of the American Society of Nephrology 30, no. 12 (2019): 2399–2411, 10.1681/ASN.2019030304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Manook M., Olaso D., Anwar I. J., et al., “Desensitization and Belatacept‐Based Maintenance Therapy in Pregnancy‐Sensitized Monkeys Receiving a Kidney Transplant,” Science Advances 9, no. 20 (2023): eadg1448, 10.1126/sciadv.adg1448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Schmitz R., Manook M., Fitch Z., et al., “Belatacept and Carfilzomib‐Based Treatment for Antibody‐Mediated Rejection in a Sensitized Nonhuman Primate Kidney Transplantation Model,” Frontiers in Transplantation 2 (2023): 1230393, 10.3389/frtra.2023.1230393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Basler M., Li J., and Groettrup M., “On the Role of the Immunoproteasome in Transplant Rejection,” Immunogenetics 71, no. 3 (2019): 263–271, 10.1007/s00251-018-1084-0. [DOI] [PubMed] [Google Scholar]
- 21. Shah N., Meouchy J., and Qazi Y., “Bortezomib in Kidney Transplantation,” Current Opinion in Organ Transplantation 20, no. 6 (2015): 652–656, 10.1097/MOT.0000000000000252. [DOI] [PubMed] [Google Scholar]
- 22. Eskandari S. K., Seelen M. A. J., Lin G., and Azzi J. R., “The Immunoproteasome: An Old Player With a Novel and Emerging Role in Alloimmunity,” American Journal of Transplantation 17, no. 12 (2017): 3033–3039, 10.1111/ajt.14435. [DOI] [PubMed] [Google Scholar]
- 23. Mulder A., Heidt S., Vergunst M., Roelen D. L., and Claas F. H., “Proteasome Inhibition Profoundly Affects Activated human B Cells,” Transplantation 95, no. 11 (2013): 1331–1337, 10.1097/TP.0b013e3182911739. [DOI] [PubMed] [Google Scholar]
- 24. Cicora F., Paz M., Mos F., and Roberti J., “Use of Bortezomib to Treat Anti‐HLA Antibodies in Renal Transplant Patients: A Single‐Center Experience,” Transplant Immunology 29, no. 1‐4 (2013): 7–10, 10.1016/j.trim.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 25. Gupta G., Abu Jawdeh B. G., Racusen L. C., et al., “Late Antibody‐Mediated Rejection in Renal Allografts: Outcome After Conventional and Novel Therapies,” Transplantation 97, no. 12 (2014): 1240–1246, 10.1097/01.TP.0000442503.85766.91. [DOI] [PubMed] [Google Scholar]
- 26. Nguyen S., Gallay B., and Butani L., “Efficacy of Bortezomib for Reducing Donor‐Specific Antibodies in Children and Adolescents on a Steroid Minimization Regimen,” Pediatric Transplantation 18, no. 5 (2014): 463–468, 10.1111/petr.12274. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information