

Abstract
Background
Achondroplasia is the most common form of disproportionate skeletal dysplasia. Recently, C-type natriuretic peptide analogue (vosoritide) was approved in numerous countries to increase annual growth velocity in patients with achondroplasia with open plates. This is a case report highlighting an atypical adverse event in a group of patients with achondroplasia using vosoritide for at least 3 months. This adverse event is reported for the first time in the literature. Among all vosoritide clinical trials, hypertrichosis was not described as a side effect.
Case presentation
The study included a total of 18 patients, all of whom were from Brazil. Among these patients, 16 identified as White, specifically Latin Americans of European descent, while the remaining 2 identified as being of African descent. All patients exhibited typical clinical features of achondroplasia, which were confirmed by the presence of the most common pathogenic variant in the FGFR3 gene, c.1138G>A (p.Gly380Arg). Out of 18 patients (11 girls and 7 boys) ranging in age from 2 to 10 years, 11 developed hypertrichosis (8 girls and 3 boys). Out of the 18 patients (61.1%) receiving regular subcutaneous vosoritide, 11 developed hypertrichosis, characterized by pigmented, thin, and short hair on the face, arms, abdomen, back, and legs. Hypertrichosis was clinically diagnosed by experienced pediatric endocrinologists. None of the patients exhibited signs of virilization, advanced bone age, or elevated androgen levels. The hypertrichosis resolved after discontinuation of treatment.
Conclusions
This unexpected pharmacological event, observed in a real-world setting, should be discussed with families prior to initiating treatment. Although hypertrichosis was not previously reported in clinical trials, it was not considered a serious adverse event. Further real-world data are needed to support therapeutic decisions and set appropriate expectations for families, patients, and healthcare providers. Additional evidence is required to better understand the pathophysiology underlying this phenomenon. In some cases, this undesirable adverse effect may influence clinical decision-making regarding treatment.
Keywords: Achondroplasia, Hypertrichosis, Adverse events, FGFR3, Vosoritide
Introduction
Achondroplasia (Ach) is the most common disproportionate skeletal dysplasia, characterized by short stature with rhizomelic shortening of the limbs, and other distinct clinical features [1]. Recently, it has been demonstrated that C-type natriuretic peptide (CNP) analogue treatment acts as a positive regulator of the signalling pathway downstream of FGFR3, promoting endochondral bone growth and increasing linear height velocity in patients with Ach [2]. The use of this treatment has been approved for children aged 6 months and older with open growth plates in Brazil, from birth in Japan, for children aged 5 years and older in the USA, and for those aged 2 years and older in Europe [3–5]. As a daily subcutaneous medication, the most commonly reported adverse events (AEs) are related to injection-site reactions [2]. We report an atypical AE in Ach patients treated with vosoritide, which has not been previously described in real-world patient reports or in any clinical trials related to the medication’s regulatory approvals.
Patient presentation
Eighteen patients with a confirmed molecular diagnosis of achondroplasia (c.1138G>A) initiated treatment with recombinant human C-type natriuretic peptide (vosoritide). All patients were Brazilian, including 16 of White ethnicity (Latin Americans of European descent) and 2 of African descent. The cohort ranged in age from 2 to 10 years, and all patients were in pre-pubertal stages at the start of treatment, with a majority being female (Table 1). Hypertrichosis, characterized by lightly pigmented, thin, and short hair on the face, arms, abdomen, back, and legs—without signs of virilization—was observed after at least 3 months of treatment and was primarily identified through physician examination. All patients received daily subcutaneous injections of vosoritide at a dosage of 15 µg/kg, in accordance with the approved prescribing guidelines.
Table 1.
Patient characteristics and hypertrichosis incidence
| Sex | Age at treatment initiation (years) | Treatment duration (months) | Hypertrichosis | Time to hypertrichosis onset (months) | |
|---|---|---|---|---|---|
| 1 | F | 6 | 16 | Yes | 9 |
| 2 | F | 5 | 15 | Yes | 6 |
| 3 | M | 7 | 17 | Yes | 9 |
| 4 | F | 7 | 16 | Yes | 8 |
| 5 | M | 9 | 15 | Yes | 6 |
| 6 | F | 6 | 14 | No | — |
| 7 | F | 2 | 9 | Yes | 6 |
| 8 | F | 10 | 9 | Yes | 3 |
| 9 | F | 3 | 11 | Yes | 3 |
| 10 | F | 2 | 9 | Yes | 3 |
| 11 | F | 10 | 10 | Yes | 3 |
| 12 | M | 9 | 9 | No | — |
| 13 | M | 10 | 9 | Yes | 6 |
| 14 | M | 6 | 9 | No | — |
| 15 | F | 2 | 9 | No | — |
| 16 | M | 10 | 7 | No | — |
| 17 | M | 10 | 9 | No | — |
| 18 | F | 9 | 5 | No | — |
F, female; M, male
Clinical findings
In this series, 11 out of 18 children (61.1%) exhibited varying degrees of hypertrichosis. None of the patients showed signs of virilization. No patient had hypotension or hyperhidrosis, and all reported mild injection-site reactions. Radiographs of the hand and wrist were obtained to assess bone age, and serum levels of adrenal androgens (androstenedione, 17-OH progesterone, dehydroepiandrosterone sulfate [DHEA-S], and testosterone) were measured in all patients. None had advanced bone age or elevated androgen levels. Hypertrichosis was characterized by the presence of short, thin hair, as observed in patient #8 after 3 months of vosoritide treatment (Fig. 1), and in patient #1 after 9 months of therapy (Fig. 2).
Fig. 1.
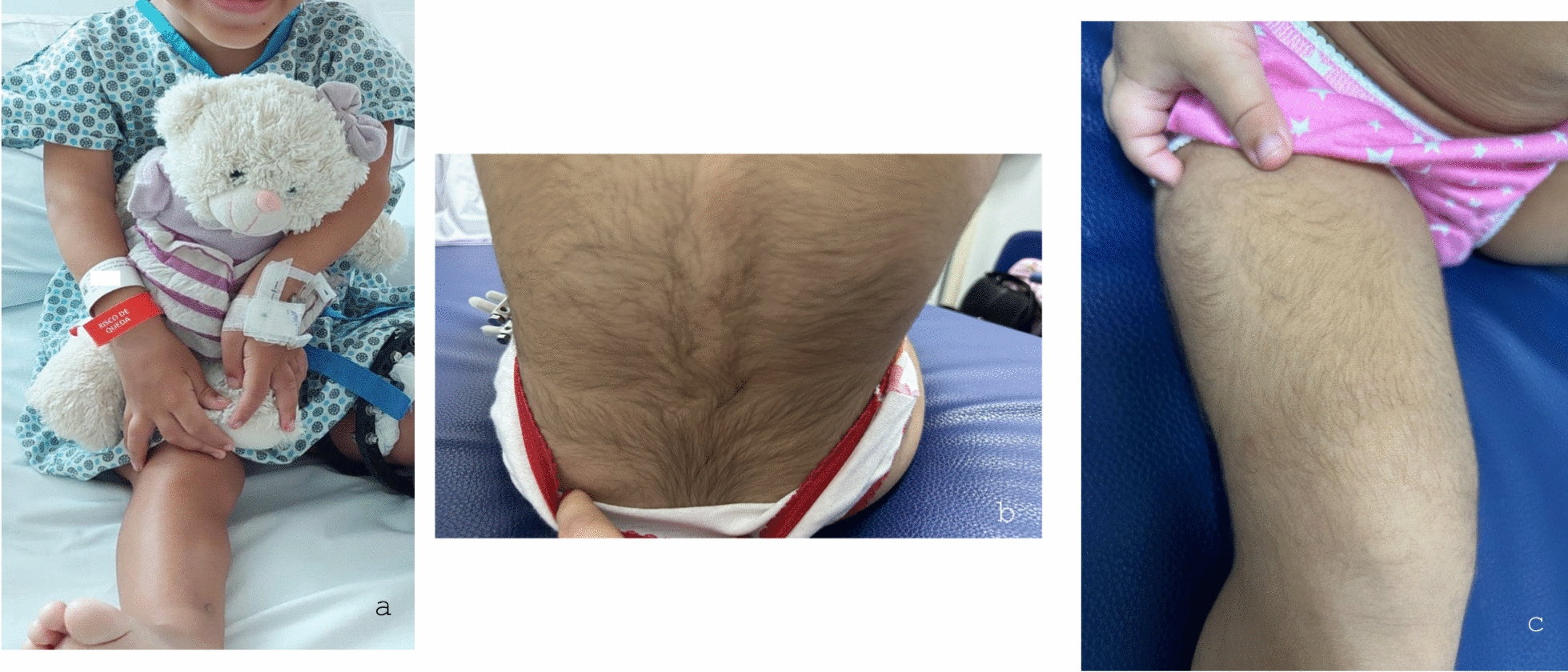
Patient #8 (10 years old, Tanner breast maturation 1, pubic hair 1). a Pre-treatment without hypertrichosis at baseline. b, c Post-treatment showing hypertrichosis after 3 months of treatment
Fig. 2.

Patient #1 (female, 6 years old, at Tanner stage breast maturation 1, pubic hair 1) with hyperthichosis after 9 months of treatment
Follow-up and outcomes
The child receiving vosoritide for the longest duration has been on treatment for 16 months. None of the patients discontinued treatment due to hypertrichosis. However, two patients temporarily interrupted treatment due to supply issues. In both cases, the excess hair fell out after 1 month without treatment. In one of these patients, reintroduction of vosoritide led to the regrowth of thin hair in the same body areas. The clinical follow-up protocol at our center was modified to include standardized photographs taken before and after the initiation of vosoritide treatment, to systematically document any changes in hair patterns.
Discussion
Hypertrichosis has been shown to occur with other medications such as diazoxide, a medication prescribed for hyperinsulinism and, just like vosoritide, it is a vasodilator. Diazoxide-induced hypertrichosis is associated with the activation of two K⁺-gated channels in the skin that influence hair growth: SUR1/KIR6.2 and, more specifically, SUR2B/KIR6.1 (also known as the ABCC9 and KCNJ8 genes) [6]. Although the mechanism of action of vosoritide cannot be directly compared with that of diazoxide, one proposed hypothesis for hypertrichosis is increased blood flow due to vasodilation. Vasodilators relax smooth muscles in blood vessels, leading to vessel widening and enhanced circulation. This increased blood flow delivers more oxygen, nutrients, and essential factors to tissues, including hair follicles, potentially supporting the anagen phase of hair growth. Additionally, mild inflammation induced by vasodilation may activate biological processes, such as the release of cytokines and growth factors, which could promote hair follicle regeneration [7].
Conclusions
Further evidence is required to better understand the pathophysiology underlying the association between vosoritide use and hypertrichosis. Studies involving a larger cohort of patients with achondroplasia (Ach) on vosoritide therapy should be published to provide additional insights. In our cohort, 61% of patients (11 out of 18) receiving vosoritide developed hypertrichosis. All other potential causes of hypertrichosis were ruled out following thorough clinical and laboratory evaluations. This adverse event was not documented in any regulatory agency prescribing information (the Food and Drug Administration [FDA], European Medicines Agency [EMA], and Brazilian Health Regulatory Agency [ANVISA]).
As hypertrichosis appears to be a relatively common pharmacological event, families should be informed about this possibility prior to initiating treatment. Although hypertrichosis was not considered a serious adverse event and was not previously reported in clinical trials, it highlights the need for further real-world data to guide therapeutic decisions and set appropriate expectations for families, patients, and healthcare providers.
Acknowledgements
We acknowledge the contribution of JCL, TSPCM, APB, and PCS.
Abbreviations
- CNP
C-type natriuretic peptide
- Ach
Achondroplasia
- FGFR3
Fibroblast Growth Factor receptor 3
- AE
Adverse events
Author contributions
All authors contributed to the manuscript.
Funding
Research funding by FioCruz.
Availability of data and materials
The datasets and materials used and/or analyzed during the current study are available from the corresponding author upon reasonable request, in compliance with Brazilian legislation, including the General Data Protection Law (Lei Geral de Proteção de Dados [LGPD], Law No. 13.709/2018), which ensures the ethical and legal handling of personal and research data;
Declarations
Ethics approval and consent to participate
This study protocol was reviewed and approved by the Research Ethics Committee of the Hospital Universitario Pedro Ernesto (approval number 60627622.9.0000.5259).
Consent for publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Informed consent
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
Not applicable.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Pauli RM. Achondroplasia: a comprehensive clinical review. Orphanet J Rare Dis. 2019;14(1):1. 10.1186/s13023-018-0972-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Savarirayan R, Tofts L, Irving M, et al. Once-daily, subcutaneous vosoritide therapy in children with achondroplasia: a randomised, double-blind, phase 3, placebo-controlled, multicentre trial. Lancet. 2020;396(10252):684–92. 10.1016/s0140-6736(20)31541-5. [DOI] [PubMed] [Google Scholar]
- 3.Vosoritida label in Brazil, ANVISA. https://consultas.anvisa.gov.br/#/medicamentos/25351440107202171/?nomeProduto=Voxzogo.
- 4.Vosoritide label (fda.gov). https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/214938s000lbl.pdf.
- 5.Vosoritide https://www.ema.europa.eu/en/medicines/human/EPAR/voxzogo.
- 6.Chen X. Efficacy and safety of diazoxide for treating hyperinsulinemic hypoglycemia: a systematic review and meta-analysis. PLoS ONE. 2021;16(2): e0246463. 10.1371/journal.pone.0246463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lin X, Zhu L, He J. Morphogenesis, growth cycle and molecular regulation of hair follicles. Front Cell Dev Biol. 2022;10: 899095. 10.12703/r/11-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets and materials used and/or analyzed during the current study are available from the corresponding author upon reasonable request, in compliance with Brazilian legislation, including the General Data Protection Law (Lei Geral de Proteção de Dados [LGPD], Law No. 13.709/2018), which ensures the ethical and legal handling of personal and research data;