

Abstract
The purpose of this study was to examine the influence of inter-limb leg lean tissue mass (LTM) asymmetry on stair climb (SC) performance in firefighters. Forty-one career firefighters (age=32.3±8.2 years, body mass=92.1±18.6 kg, stature=178.3±7.9 cm) visited the laboratory on one occasion and completed a whole body and leg composition assessment followed by a timed and weighted SC task. Percent body fat (%BF) and leg LTM were determined during a DEXA scan and regional thigh analysis. Asymmetry was assessed by the percent difference between limbs (dominant limb LTM – non-dominant limb LTM)/dominant limb LTM × 100) and a ±3% cut-off for asymmetry classification. Participants ascended and descended 26 stairs four times as quickly as possible while wearing a weighted (22kg) vest. Point biserial correlations were used to assess the relationship of inter-limb leg LTM asymmetry and SC performance before and after controlling for age and %BF. Results indicated that inter-limb leg LTM asymmetry was associated with longer SC task time (poorer performance) both before (r=0.432, P=0.005) and after (r=0.502, P=0.001) controlling for age and %BF. Our findings indicated that inter-limb leg LTM asymmetry negatively impacts firefighter SC performance, which may be improved with appropriate exercise interventions.
Keywords: Tactical, occupational health, body composition, occupational performance, aging
Practitioner Summary:
This study examined the influence of leg inter-limb lean tissue mass (LTM) asymmetry on SC performance in career firefighters. We found that inter-limb leg LTM asymmetry was associated with reduced SC performance, prior to and after controlling for age and percent body fat. Interventions that mitigate these asymmetries may improve occupational performance.
INTRODUCTION
Firefighters are paramount to public safety with over 360,000 career firefighters currently employed in the United States, protecting nearly 70% of the population (7). Occupational injuries are common within the fire service with over 60,000 firefighters being injured on duty in 2021 (5). These injuries result in a high economic burden, with subsequent expenses between $2.8 billion and $7.8 billion per year (25). One potential contributing factor is that these individuals are required to perform a number of critical and essential tasks in hazardous conditions while wearing personal protective equipment weighing around 22 kg (22). Specifically, the International Association of Fire Chiefs and International Association of Firefighters have identified eight critical firefighter tasks in the Candidate Physical Abilities Test (32). The stair climb (SC) task is often considered one of the most critical and challenging tasks. For example, previous studies have demonstrated a significant cardiometabolic response during the SC including near maximal heart rates and increased oxygen consumption and blood lactate levels (12,28,35). Further, simulated SC assessments have been shown to be reliable (28) and rated as a highly relevant occupational task among firefighters with a mean response of 3.6 on a 0 – 4 scale (0 = not relevant at all, 4 = very relevant) (31).
Inter-limb leg lean tissue mass (LTM) asymmetries occur when there are inter-limb differences in skeletal muscle mass. These asymmetries have been examined in various populations ranging from athletes to older adults (2,11,19,21). Previous studies have found leg inter-limb asymmetries adversely impact countermovement jump height (2), contribute to greater leg inter-limb strength differences (11), and are associated with reduced performance in common functional tasks (i.e., chair sit-to-stands, walking, timed-up-and-go) (18). Previous authors have suggested inter-limb leg LTM asymmetries are influenced by performing various tasks on a favored side over time (14,17,20,33). For example, Australian football players tend to have larger psoas muscle size in their kicking (favored) limb, when compared to their stance leg (14,33). It is possible firefighters are exposed to occupational tasks that are performed on a favored side such as specific victim drag techniques and/or asymmetric load carriage (1,14,33). Due to the unilateral limb demands during a SC task (29), inter-limb leg LTM asymmetries may negatively impact SC performance. For instance, previous authors (29) have indicated that inter-limb leg asymmetry adversely affects SC speed more than gait speed in older adults due to the higher demand on unilateral leg function. These previous studies indicate a need to assess and examine the relationship between inter-limb leg asymmetries and occupational performance in career firefighters. Therefore, the purpose of this study is to examine the relationship between inter-limb leg LTM differences and SC performance in career firefighters. We hypothesize that firefighters with greater LTM asymmetries will have reduced performance (longer time to completion) during a timed SC task.
MATERIALS and METHODS
Participants
Forty-one career male firefighters (all demographic data are in Table 1) volunteered for this investigation. All participants were apparently healthy and free of any known cardiovascular, neuromuscular, or metabolic diseases and indicated that they had not sustained any recent musculoskeletal injuries. Participants were excluded if they were a current smoker or had a history of surgery to the low back (e.g., spinal fusion) or lower extremities (e.g., joint replacement, ligament reconstruction). This study was approved by the University institutional review board (IRB #18-1458) for the protection of human subjects.
Table 1.
Mean ± standard deviation (SD) and range values for the demographic and performance variables.
| Mean ± SD | Range | |
|---|---|---|
| Age | 32.3 ± 8.2 | 20.0 – 50.0 |
| Stature (cm) | 178.3 ± 7.9 | 159.2 – 194.6 |
| Body mass (kg) | 92.1 ± 18.6 | 65.0 – 132.5 |
| BMI (kg/m2) | 28.8 ± 5.3 | 20.9 – 41.2 |
| % BF (%) | 24.1 ± 7.9 | 9.9 – 39.4 |
| Dominant leg mass (kg) | 11.9 ± 2.1 | 8.3 – 17.0 |
| Non-Dominant leg mass (kg) | 11.9 ± 2.0 | 8.7 – 16.7 |
| Leg asymmetry (%) | 0.5 ± 2.5 | −4.9 – 5.9 |
| SC time (seconds) | 74.7 ± 13.4 | 61.0 – 129.0 |
BMI – body mass index, % BF – percent body fat, SC – stair climb.
N = 41 male career firefighters
Experimental Design
Participants reported to the laboratory on one occasion following an eight-hour fast (excluding water). They were instructed to refrain from caffeine and smokeless tobacco for a minimum of 12 hours and abstain from vigorous lower-body exercise for a minimum of 48 hours prior to the visit. Each participant completed an informed consent document, a health history questionnaire, a body composition assessment, and a timed SC task with a weighted vest. Prior to the SC task, participants consumed a standardized meal (Carnation Breakfast Essentials High Protein 8 fl oz) to break their fast.
Body Composition
Stature and body mass were assessed using a calibrated clinical scale (Health o meter 2101 KL, Bridgeview, IL). Percent body fat (%BF) and leg lean tissue mass (LTM) were assessed using a daily calibrated dual energy x-ray absorptiometry (DEXA; GE Lunar iDXA, General Electric Medical Systems Ultrasound & Primary Care Diagnostics, Madison WI, USA) scan. Participants wore athletic clothing and removed any metal prior to the scan. Participants were instructed to lie supine and remain still throughout the duration of the scan per the manufacturer's guidelines. Leg LTM was determined by outlining both legs into regions of interest as described similarly in previous studies (9,23). Tracings for each leg started lateral to the iliac crest and moved diagonally through the femoral neck, continuing down the leg and below the foot, and connecting to the initial tracing at the iliac crest (see Figure 1). Asymmetry was assessed by subtracting the non-dominant limb LTM from the dominant limb LTM and then dividing by the LTM of the dominant limb and expressed as a percentage. Dominant limb was determined by asking participants which leg they would kick a ball with. A ±3% LTM cut-off was used as it has been shown to result in significant inter-limb leg strength differences (11).
Figure 1.
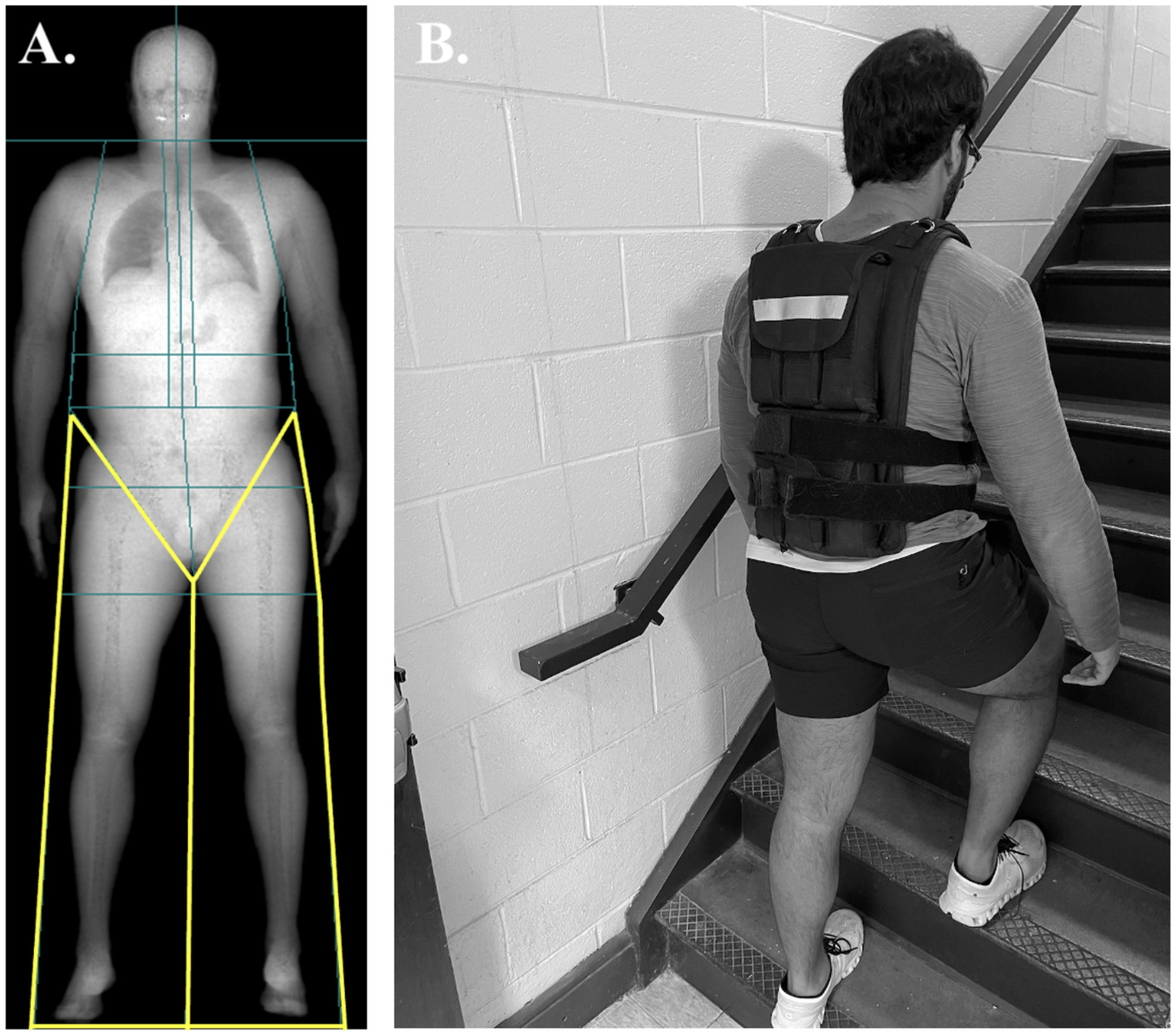
Examples of the boundaries (highlighted in yellow) used for the limb lean tissue mass analysis from a dual energy x-ray absorptiometry scan (A) and of the stair climb task with weighted vest (B).
Stair Climb Performance
All participants performed a timed SC task wearing a weighted vest as described previously (31). Prior to the assessment, participants were familiarized with the protocol by ascending 26 steps once without the weighted vest. After the familiarization, participants were fitted with a 22.73 kg weighted vest (Z Fitness Inc., San Jose, CA, USA) to simulate the weight of their personal protective equipment (PPE) and self-contained breathing apparatus (SCBA) (31). The vest was securely fastened around the torso and chest via Velcro straps to assure movement was minimized during the SC task. Following the verbal command (i.e., 3-2-1-GO), a timer started and participants began to ascend and descend 26 stairs that included a floor, followed by three separate flights of stairs (i.e. nine steps, nine steps, five steps) and a landing for each flight. Firefighters completed this four times for a total of 104 steps. They were instructed to touch each step (stair height – 18.5 cm) with one foot as quickly as possible without stopping or holding onto the railing. The timer stopped once both feet touched the floor of the bottom of the stairs.
Statistical Analysis
All descriptive data are presented as mean ± standard deviation. A point biserial correlation was used to assess the relationship between leg inter-limb asymmetry and SC task performance. Due to the large age range (7) and high prevalence of obesity among firefighters (30), an additional partial correlation controlling for age and %BF was employed to assess the relationship between inter-limb leg LTM asymmetry and SC task performance. As previous studies (4) have reported taller participants walk faster, we also examined the potential relationship of stature on SC performance. Outliers were identified and removed if they were greater than three standard deviations above the mean. All data were analyzed using R statistical language (version 4.1.2 R Core Team, 2022). An alpha level of 0.05 was utilized a priori to determine statistical significance.
RESULTS
All mean and standard deviation values for limb LTM, asymmetry, and SC variables are presented in Table 1. Our participants age and %BF were similar to and representative of career firefighters reported in previous studies (7,30). One participant was identified as an outlier (> 4 SD above the mean) for the SC time and was removed prior to analyses. The point biserial correlation indicated LTM asymmetry was associated with longer SC task time (poorer performance) (r = 0.432, P = 0.005). When adjusting for age and %BF, a similar positive relationship was observed between LTM asymmetry and SC time (r = 0.502, P = 0.001). Lastly, there was no significant relationship between participant stature and SC time (r = −0.095, P = 0.562).
DISCUSSION
Firefighters are required to perform a number of essential occupational activities (32), however, the SC is often considered one of the most critical and challenging tasks (34). The current study examined the impact of lower body LTM asymmetry on simulated SC performance in career firefighters. The primary findings of the current study indicated that inter-limb leg LTM asymmetry is significantly associated with impaired SC task performance (longer completion times) in career firefighters before and after accounting for age and %BF.
The finding that greater inter-limb leg LTM asymmetry is associated with reduced performance is in agreement with previous research in both athletic and older adult populations (2,11,18,21). For example, investigators have reported that greater inter-limb leg LTM asymmetries are associated with poorer countermovement jump height (2), greater inter-limb strength differences (unilateral isometric back squat on force plates) (11), poorer performance during common functional tasks (chair sit-to-stands, walking, timed-up-and-go) (18), and reduced lower-extremity function (400 m walk test, 30 sec chair sit-to-stands) (21). These authors (18,21) also noted that inter-limb leg LTM asymmetries likely contribute to limb strength/power capabilities that may impact subsequent performance. For example, Bell et al. (2) reported LTM asymmetry accounted for 20% of the variance in leg inter-limb force differences in collegiate athletes. Thus, it is possible that the inter-limb leg LTM asymmetry reported in the current study may have contributed to strength/power asymmetries whereby the weaker limb is unable to maintain the unilateral demands required during the weighted SC climb (24,29). This may be supported by Portegijis et al. (29) who reported leg inter-limb asymmetry adversely affects SC speed more than gait speed in older adults, given that the SC is a more challenging mobility task requiring a higher demand on unilateral leg function.
Previous studies have suggested inter-limb leg LTM differences occur as a result of the mechanical stress stimulating increases in muscle mass on the favored limb through chronic exposure to asymmetric tasks, and is commonly seen in athletic populations (14,17,20,33). For example, Australian football athletes tend to have greater psoas major muscle size in their dominant (kicking) leg compared to their contralateral (stance) limb, and field hockey athletes exhibit lower extremity asymmetries between their lead side and contralateral limb (14,17,33). We are unaware of any previous studies that have examined the impact of inter-limb leg LTM asymmetries on occupational performance in firefighters. Based on previous studies examining LTM in athletic populations (2,11), the muscle atrophy that occurs following injury (19), and recent work demonstrating the impact of firefighter demographics on performance during other simulated occupational tasks (22,31), it is possible that these asymmetries may exist due to chronically performing various firefighter tasks, injury history, age, and/or %BF.
Previous injury (i.e., ACL tear) can cause prolonged underloading resulting in muscle atrophy of the injured limb and the development of inter-limb leg LTM asymmetry (18,19). However, inter-limb leg LTM asymmetry reported in the current study may occur from repetitively performing occupational tasks targeting the favored side given that we excluded participants with any major musculoskeletal surgeries in the lower leg and back, any recent injuries, and found no impact of age and %BF when controlled for our in our analyses. For example, firefighters perform many occupational duties including specific victim drag techniques and asymmetric load carriage that may impact inter-limb leg LTM asymmetries. However, future work (e.g., occupational analysis) is needed to identify specific issues that cause LTM asymmetries in firefighters. Additionally, it is important to note that inter-limb leg LTM asymmetry accounted for 18.7 – 25.2% of the variance in SC time, which aligns with previous studies (2). Along with LTM asymmetries, it is likely additional physiological parameters such as lower extremity strength and power (31), aerobic capacity (12,15,26), and/or steadiness (31) may also be important contributors to SC performance. Therefore, future studies are needed to identify additional variables that further explain the remaining variance in firefighter SC performance. Lastly, it is important to note that previous investigations have utilized different percent asymmetry calculations (2,11). However, when using these calculations (2,11) to determine the ±3% threshold, there were no differences in the outcome (r = 0.432, P = 0.005, 7 asymmetry cases identified) between these methods and the asymmetry calculation used in the current paper.
Limitations and Future Research Considerations
Previous research has shown simulated SC performance to be reliable (28) and that using a weighted vest to simulate the impact of wearing firefighter PPE and SCBA during a SC task is occupationally relevant (31). However, given that prior investigations have noted wearing PPE or a SCBA results in minimal to significant alterations in balance performance (6,8,16,27), future investigations are needed to determine the impact of wearing PPE and/or SCBA versus a weighted vest on SC performance. While the aim of the current study examined the impact of inter-limb leg LTM asymmetries on performance, additional work is needed to determine the impact of asymmetries on firefighter injuries. Further, to increase the ability to test more firefighters at their departments, future studies are required to determine if field-based assessments of inter-limb leg LTM (e.g. bioelectrical impedance analysis) are suitable alternatives to examine asymmetries when compared to the DEXA-based assessments used in the current study.
Conclusion
The primary findings of the current study indicated that inter-limb leg LTM asymmetry (≥3%) is significantly associated with poorer SC task performance in career firefighters. These results highlight the importance of 1) monitoring inter-limb leg LTM over time to identify firefighters who have significant asymmetries that may impact performance and potential injury risk (13), and 2) implementing training strategies to minimize inter-limb leg asymmetries (3,10).
Figure 2.
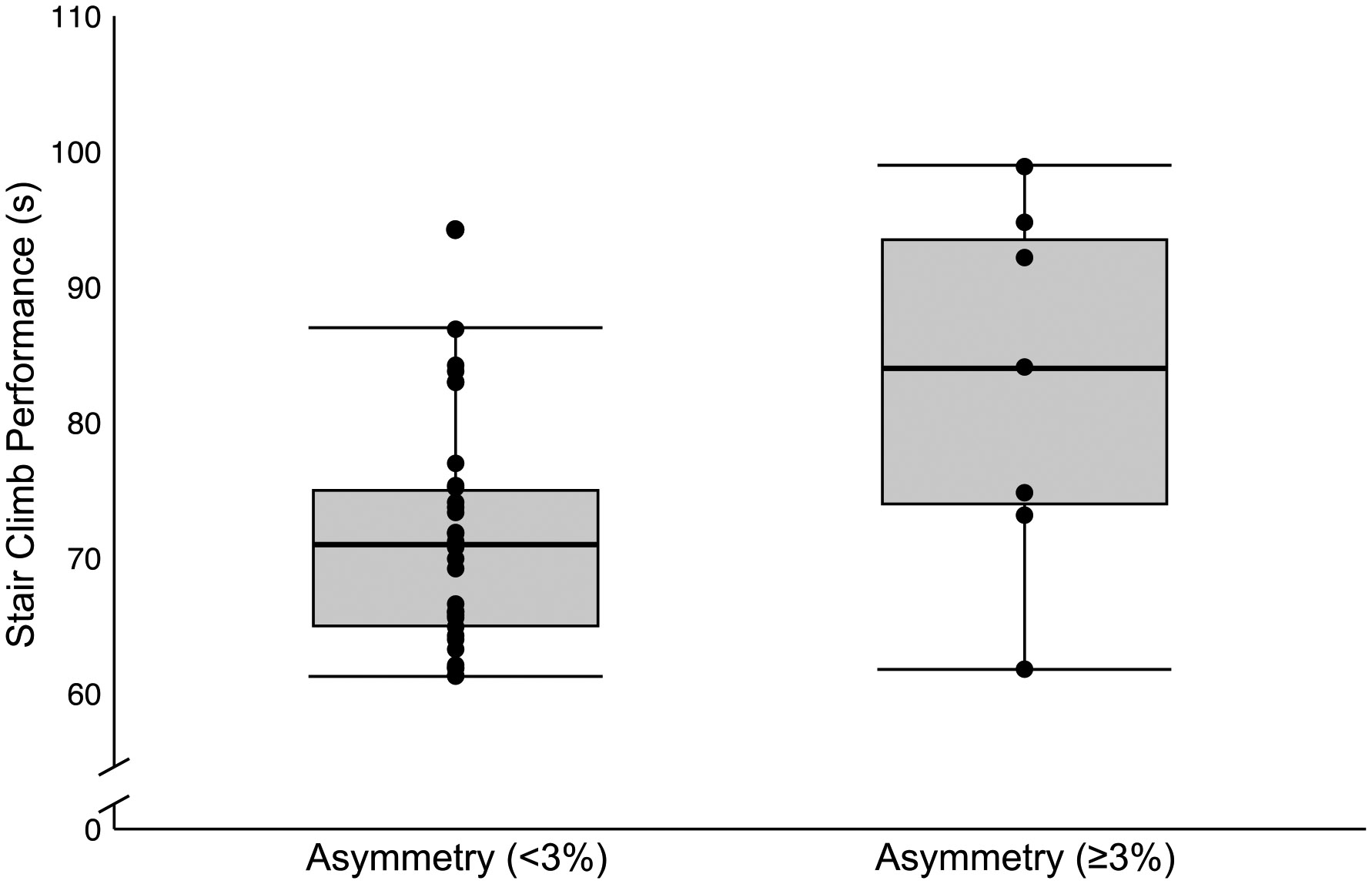
Box-and-whisker plots for asymmetry classification and stair climb time. Median values are marked with a bold line within the boxes. The lower and upper boundaries represent the 25th (Q1) and 75th (Q3) percentiles. The lower and upper whiskers indicate the value for (Q1 – [1.5 * Interquartile Range]) and (Q3 + [1.5 * Interquartile Range]), respectively. N = 40 male career firefighters.
Acknowledgments:
We would like to thank all the local fire departments who supported and participated in this project.
Funding:
This project was supported in part by a grant through the Centers of Disease Control and Prevention (#U19-OH012303).
Abbreviation:
- LTM
Lean tissue mass
- SC
Stair climb
- DEXA
Dual energy x-ray absorptiometry
- ACL
Anterior Cruciate Ligament
- %BF
Percent Body Fat
- PPE
Personal Protective Equipment
- BMI
Body Mass Index
Footnotes
Disclosure statement:
No conflicts of interests were reported by the authors.
References
- 1.Alvar BA, Sell K, Deuster PA, and National Strength & Conditioning Association (U.S.) (eds.). NSCA’s essentials of tactical strength and conditioning. Champaign, IL: Human Kinetics, 2017. [Google Scholar]
- 2.Bell DR, Sanfilippo JL, Binkley N, and Heiderscheit BC. Lean Mass Asymmetry Influences Force and Power Asymmetry During Jumping in Collegiate Athletes. Journal of Strength and Conditioning Research 28: 884–891, 2014.Available from: https://journals.lww.com/00124278-201404000-00002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bishop C, De Keijzer KL, Turner AN, and Beato M Measuring Interlimb Asymmetry for Strength and Power: A Brief Review of Assessment Methods, Data Analysis, Current Evidence, and Practical Recommendations. Journal of Strength and Conditioning Research 37: 745–750, 2023.Available from: https://journals.lww.com/10.1519/JSC.0000000000004384 [DOI] [PubMed] [Google Scholar]
- 4.Bohannon RW. Comfortable and maximum walking speed of adults aged 20—79 years: reference values and determinants. Age Ageing 26: 15–19, 1997.Available from: https://academic.oup.com/ageing/article-lookup/doi/10.1093/ageing/26.1.15 [DOI] [PubMed] [Google Scholar]
- 5.Campbell R and Hall S United States Firefighter Injuries in 2021. , 2022. [Google Scholar]
- 6.Colburn D, Russo L, Burkard R, and Hostler D Firefighter protective clothing and self contained breathing apparatus does not alter balance testing using a standard sensory organization test or motor control test in healthy, rested individuals. Applied Ergonomics 80: 187–192, 2019.Available from: https://linkinghub.elsevier.com/retrieve/pii/S0003687019300948 [DOI] [PubMed] [Google Scholar]
- 7.Fahy R, Evarts B, and Stein GP. US Fire Department Profile 2020. [Google Scholar]
- 8.Garner JC, Wade C, Garten R, Chander H, and Acevedo E The influence of firefighter boot type on balance. International Journal of Industrial Ergonomics 43: 77–81, 2013.Available from: https://linkinghub.elsevier.com/retrieve/pii/S0169814112001096 [Google Scholar]
- 9.Giuliani HK, Laffan MR, Trivisonno AJ, Gerstner GR, Mota JA, Arieta LR, et al. Measuring muscle quality: associations between echo intensity and normalized strength and power. Physiol Meas 42: 03NT01, 2021.Available from: https://iopscience.iop.org/article/10.1088/1361-6579/abea24 [DOI] [PubMed] [Google Scholar]
- 10.Gonzalo-Skok O, Tous-Fajardo J, Suarez-Arrones L, Arjol-Serrano JL, Casajús JA, and Mendez-Villanueva A Single-Leg Power Output and Between-Limbs Imbalances in Team-Sport Players: Unilateral Versus Bilateral Combined Resistance Training. International Journal of Sports Physiology and Performance 12: 106–114, 2017.Available from: https://journals.humankinetics.com/view/journals/ijspp/12/1/article-p106.xml [DOI] [PubMed] [Google Scholar]
- 11.Hart NH, Nimphius S, Spiteri T, and Newton RU. Leg strength and lean mass symmetry influences kicking performance in Australian football. J Sports Sci Med 13: 157–165, 2014. [PMC free article] [PubMed] [Google Scholar]
- 12.von Heimburg ED, Rasmussen AKR, and Medbø JI. Physiological responses of firefighters and performance predictors during a simulated rescue of hospital patients. Ergonomics 49: 111–126, 2006.Available from: https://www.tandfonline.com/doi/full/10.1080/00140130500435793 [DOI] [PubMed] [Google Scholar]
- 13.Helme M, Tee J, Emmonds S, and Low C Does lower-limb asymmetry increase injury risk in sport? A systematic review. Physical Therapy in Sport 49: 204–213, 2021.Available from: https://linkinghub.elsevier.com/retrieve/pii/S1466853X21000468 [DOI] [PubMed] [Google Scholar]
- 14.Hides J, Fan T, Stanton W, Stanton P, McMahon K, and Wilson S Psoas and quadratus lumborum muscle asymmetry among elite Australian Football League players. British Journal of Sports Medicine 44: 563–567, 2010.Available from: https://bjsm.bmj.com/lookup/doi/10.1136/bjsm.2008.048751 [DOI] [PubMed] [Google Scholar]
- 15.Huang C-J, Garten RS, Wade C, Webb HE, and Acevedo EO. Physiological responses to simulated stair climbing in professional firefighters wearing rubber and leather boots. Eur J Appl Physiol 107: 163–168, 2009.Available from: http://link.springer.com/10.1007/s00421-009-1092-8 [DOI] [PubMed] [Google Scholar]
- 16.Kong PW, Suyama J, Cham R, and Hostler D The Relationship Between Physical Activity and Thermal Protective Clothing on Functional Balance in Firefighters. Research Quarterly for Exercise and Sport 83: 546–552, 2012.Available from: http://www.tandfonline.com/doi/abs/10.1080/02701367.2012.10599144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Krzykała M. Dual Energy X-Ray Absorptiometry in Morphological Asymmetry Assessment among Field Hockey Players. Journal of Human Kinetics 25: 77–84, 2010.Available from: https://www.sciendo.com/article/10.2478/v10078-010-0034-1 [Google Scholar]
- 18.Lee EJ, Lee SA, Soh Y, Kim Y, Won CW, and Chon J Association between asymmetry in lower extremity lean mass and functional mobility in older adults living in the community: Results from the Korean Frailty and Aging Cohort Study. Medicine 98: e17882, 2019.Available from: https://journals.lww.com/10.1097/MD.0000000000017882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lepley LK, Davi SM, Burland JP, and Lepley AS. Muscle Atrophy After ACL Injury: Implications for Clinical Practice. Sports Health 12: 579–586, 2020.Available from: http://journals.sagepub.com/doi/10.1177/1941738120944256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lijewski M, Burdukiewicz A, Pietraszewska J, Andrzejewska J, and Stachoń A Asymmetry of Muscle Mass Distribution and Grip Strength in Professional Handball Players. IJERPH 18: 1913, 2021.Available from: https://www.mdpi.com/1660-4601/18/4/1913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mertz KH, Reitelseder S, Jensen M, Lindberg J, Hjulmand M, Schucany A, et al. Influence of between-limb asymmetry in muscle mass, strength, and power on functional capacity in healthy older adults. Scand J Med Sci Sports 29: 1901–1908, 2019.Available from: https://onlinelibrary.wiley.com/doi/10.1111/sms.13524 [DOI] [PubMed] [Google Scholar]
- 22.Mota JA, Barnette TJ, Gerstner GR, Giuliani HK, Tweedell AJ, Kleinberg CR, et al. Relationships Between Neuromuscular Function and Functional Balance Performance in Firefighters. Sci Rep 8: 15328, 2018.Available from: http://www.nature.com/articles/s41598-018-33555-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mota JA, Stock MS, and Thompson BJ. Vastus lateralis and rectus femoris echo intensity fail to reflect knee extensor specific tension in middle-school boys. Physiol Meas 38: 1529–1541, 2017.Available from: https://iopscience.iop.org/article/10.1088/1361-6579/aa791a [DOI] [PubMed] [Google Scholar]
- 24.Nadeau S, McFadyen BJ, and Malouin F Frontal and sagittal plane analyses of the stair climbing task in healthy adults aged over 40 years: what are the challenges compared to level walking? Clinical Biomechanics 18: 950–959, 2003.Available from: https://linkinghub.elsevier.com/retrieve/pii/S0268003303001797 [DOI] [PubMed] [Google Scholar]
- 25.National Institude of Standards and Technology. The Economic Consequences Of Firefighter Injuries and Their Prevention. [Google Scholar]
- 26.O’Connell ER, Thomas PC, Cady LD, and Karwasky RJ. Energy costs of simulated stair climbing as a job-related task in fire fighting. J Occup Med 28: 282–284, 1986. [PubMed] [Google Scholar]
- 27.P H. Effect of Protective Clothing and Fatigue on Functional Balance of Firefighters. J Ergonomics S2, 2014.Available from: http://www.omicsgroup.org/journals/effect-of-protective-clothing-and-fatigue-on-functional-balance-of-firefighters-2165-7556.S2-004.php?aid=21517 [Google Scholar]
- 28.Plat M-CJ, Frings-Dresen MHW, and Sluiter JK. Reproducibility and validity of the stair-climb test for fire fighters. Int Arch Occup Environ Health 83: 725–731, 2010.Available from: http://link.springer.com/10.1007/s00420-010-0518-2 [DOI] [PubMed] [Google Scholar]
- 29.Portegijs E, Sipilä S, Rantanen T, and Lamb SE. Leg Extension Power Deficit and Mobility Limitation in Women Recovering from Hip Fracture. American Journal of Physical Medicine & Rehabilitation 87: 363–370, 2008.Available from: https://journals.lww.com/00002060-200805000-00003 [DOI] [PubMed] [Google Scholar]
- 30.Poston WSC, Haddock CK, Jahnke SA, Jitnarin N, Tuley BC, and Kales SN. The Prevalence of Overweight, Obesity, and Substandard Fitness in a Population-Based Firefighter Cohort. Journal of Occupational & Environmental Medicine 53: 266–273, 2011.Available from: https://journals.lww.com/00043764-201103000-00008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ryan ED, Laffan MR, Trivisonno AJ, Gerstner GR, Mota JA, Giuliani HK, et al. Neuromuscular determinants of simulated occupational performance in career firefighters. Applied Ergonomics 98: 103555, 2022.Available from: https://linkinghub.elsevier.com/retrieve/pii/S0003687021002027 [DOI] [PubMed] [Google Scholar]
- 32.Sheaff AK, Bennett A, Hanson ED, Kim Y-S, Hsu J, Shim JK, et al. Physiological Determinants of the Candidate Physical Ability Test in Firefighters. Journal of Strength and Conditioning Research 24: 3112–3122, 2010.Available from: https://journals.lww.com/00124278-201011000-00030 [DOI] [PubMed] [Google Scholar]
- 33.Stewart S, Stanton W, Wilson S, and Hides J Consistency in size and asymmetry of the psoas major muscle among elite footballers. British Journal of Sports Medicine 44: 1173–1177, 2010.Available from: https://bjsm.bmj.com/lookup/doi/10.1136/bjsm.2009.058909 [DOI] [PubMed] [Google Scholar]
- 34.Taylor NAS, Dodd MJ, Taylor EA, and Donohoe AM. A Retrospective Evaluation of Injuries to Australian Urban Firefighters (2003 to 2012): Injury Types, Locations, and Causal Mechanisms. Journal of Occupational & Environmental Medicine 57: 757–764, 2015.Available from: https://journals.lww.com/00043764-201507000-00008 [DOI] [PubMed] [Google Scholar]
- 35.Taylor NAS, Fullagar HHK, Mott BJ, Sampson JA, and Groeller H Employment Standards for Australian Urban Firefighters: Part 1 The Essential, Physically Demanding Tasks. Journal of Occupational & Environmental Medicine 57: 1063–1071, 2015.Available from: https://journals.lww.com/00043764-201510000-00005 [DOI] [PubMed] [Google Scholar]