

Abstract
Categorical diagnosis, a pillar of the medical model, has not worked well in psychiatry where most diagnoses are still exclusively symptom based. Uncertainty continues about whether categories or dimensions work better for the assessment and treatment of idiopathic psychoses. The Bipolar Schizophrenia Network for Intermediate Phenotypes (B-SNIP) examined multiple cognitive and electrophysiological biomarkers across a large transdiagnostic psychosis data set. None of the variables supported neurobiological distinctiveness for conventional clinical psychosis diagnoses but showed a continuum of severity. Using numerical taxonomy of these data, B-SNIP identified three biological subtypes (Biotypes) agnostic to DSM diagnoses. Biotype-1 is characterized by reduced physiological response to salient stimuli, while Biotype-2 showed accentuated intrinsic (background or ongoing) neural activity and the worst inhibition. Biotype-3 cases are like healthy persons on many laboratory measures. These Biotypes differed in imaging and other electrophysiological measures not included in subgroup creation, illustrating external validation. The Biotypes solution also replicated in an independent sample of psychosis cases. Biotypes are differentiable by clinical characteristics, leading to a feasible algorithm for Biotype estimates. Identifying Biotypes may aid treatment selection and outcome prediction. As an example, preliminary cross-sectional B-SNIP data suggest that Biotype-1 cases may have physiological features that predict a more favorable response to clozapine. While psychosis Biotypes reveal physiological heterogeneity across cases with similar clinical characteristics, data also suggest a dimensional vulnerability for serious psychopathology that cuts across diagnostic boundaries. Both categorical and dimensional diagnostic approaches should be considered within idiopathic psychosis for optimum diagnosis, care, and research.
Keywords: Psychosis, Biotypes, Categorical, Dimensional, Classification, Cognition, Physiology
A patient calls their doctor about some niggling complaint or grave ailment. The medical staff ask questions, collect basic bodily information (e.g., height, weight, heart rate, and blood pressure), do a physical exam, and perhaps order laboratory tests like blood draws, an MRI, or maybe electroencephalography. At each step, the clinicians speculate about what is wrong. They have diagnostic hypotheses, including ones they consider more or less likely; the latter are called rule-outs. After pondering all the information, the medical team has the best guess they label a diagnosis.
This is not merely an intellectual exercise. The process of medical diagnosis provides the rational basis for treatment prescription. The patient hopes the medical team can devise a successful treatment plan, and the ailment disappears. The diagnosis may have a known etiology and pathology. However, a diagnosis does not guarantee a known cause or effective treatment, and a known etiology does not ensure a cure. Alternatively, the availability of an effective treatment does not require a known cause.
1. The Medical Model and Psychiatry
Every medical specialty walks this familiar diagnostic path. Psychiatry, at least conceptually, is no different from every other branch of medicine, with its diagnoses formalized in the DSM and ICD manuals. Those compendia are the field’s best diagnostic guesses based on expert consensus (Horwitz 2021). The current diagnostic systems for psychiatry are categorical, meaning one either does or does not have a specific diagnosis. Pure categorical systems assume qualitative differences between health and disease (you are healthy or not) and between conditions (you have this diagnosis, not that diagnosis).
Across the range of medical conditions, however, diagnosis is less specific than it sounds, undeniably less precise than most clinicians and patients hope. Not all diagnoses across all of medicine are like Huntington’s disease (an autosomal dominant mutation of the Huntingtin gene). There are many reasons for ambiguity. For instance, two patients with the same or very similar clinical presentations may have different pathologies and need different treatments. In this case, multiple causes yield similar clinical pictures, which is called etiological heterogeneity. Alternatively, two patients with different presentations may need the same treatment. This is when the same etiology yields different clinical pictures, called variable expressivity. Finally, unknown to the clinician, a patient could have two or more conditions simultaneously, with independent or interacting causes. For example, a person could qualify for both a major depression and a psychoactive substance use disorder. The clinician might attempt to decipher if one diagnosis (e.g., the depression) accounts for the other (e.g., the substance use), or vice versa, but there is no prohibition in nature against an organism carrying multiple etiologically different ailments simultaneously. These and other issues complicate medical diagnosis. Of course, etiological heterogeneity, variable expressivity, and concurrent conditions are just conjectures without evidence.
Psychiatry is considered rugged terrain for the so-called “medical model,” although psychiatry’s transition to this method was once considered a foregone conclusion (Guze 1992). The basic assumptions of this approach are simple: illnesses come in different forms that reflect cause, pathophysiology, population distribution, optimal treatments, and outcomes (Guze 1992; Zhang et al. 2023). For psychiatry, because the brain is the affected organ, this means using neuroscience as part of a larger biological context to understand specific deviations in brain functioning that undergird clinical conditions. In the early 1900s, psychiatry appeared primed to become a medical model discipline—neurosyphilis progressed from clinical syndrome to disease with a specific cause (the Treponema pallidum bacterium). Forty years passed from identifying neurosyphilis’ cause to the availability of penicillin as an effective treatment. Unfortunately, no matter how protracted, the hope that this success initiated a new age for psychiatric disease identification and treatment developments has yet to materialize in an uncomplicated form (Keshavan et al. 2013; Harrington 2019). As a result, most psychiatric maladies remain idiopathic, meaning their causes are unknown, their etiology is a mystery. So far, the medical model methodology has not evolved in psychiatry.
2. Psychiatry’s Commitment to Clinical Features for Diagnosis
Throughout its history general medicine also struggled with caverns of uncertainty and nosological confusion. Some of these lacunae were filled after decades, sometimes centuries, of wandering in the darkness. For instance, morbid edema, or dropsy, was once considered a legitimate medical diagnosis with certain, nonspecific treatment indications (Estes 1993). But clinicians made additional observations about dropsy that changed their understanding and approach. Consider this article from the 1837 New England Journal of Medicine:
You must be made aware that dropsy is to be considered as the prominent symptom of some morbid condition of the body. It is not an idiopathic disease, but is the result of some unwonted action, into the nature of which, before you search for your remedy, you must carefully inquire. To obtain a relief from the discharge of the fluid is of course an object of anxious consideration, but beyond this you must ascertain what has been the predisposing, what the executing cause, whether any other remedy may not be more effectual, whether the constitution of the individual is such that you may prescribe an agent which, when it does not produce good effects, may become the source of mischief, and, indeed, be more detrimental than the disease which you undertake to cure by it. (Sigmond 1837)
The same reasoning probably applies to the evaluation and treatment of serious psychiatric conditions with psychosis as a prominent clinical feature. Just substitute “psychosis” for “dropsy,” “brain” for “body,” and “delusions and hallucinations” for “the discharge of the fluid.” More precisely, the passage hints at psychiatry’s main impediment to implementing a medical model approach—the exclusive reliance on signs and symptoms for diagnosis. Even a medical clinic operator in remote Eagle, Alaska considered this a limitation. In John McPhee’s (1977) “Coming into the Country,” Elva Scott, who ran such an establishment out of her kitchen in the middle of the last century, said: “We don’t have laboratory tests. We treat on symptoms.”
The remainder of this document uses the above insightful passage from 1837 on dropsy as a motivating influence, in combination with what we learned from the Bipolar-Schizophrenia Network for Intermediate Phenotypes (B-SNIP) project. Our transparent title discloses that the theme is whether categories or dimensions seem most useful for treatment selection when diagnosing patients with an idiopathic psychosis. The second part of the title reveals that B-SNIP’s outcomes influenced our conclusions concerning this issue.
3. Early B-SNIP Hypotheses for Parsing Psychosis-Related Neurobiology
B-SNIP is a consortium of scientists spread across multiple academic centers (Tamminga et al. 2014, 2017). From its inception in 2008, the goal was to assemble neurobiological support for clinically defined, idiopathic psychosis diagnoses. It is believed that better etiological or physiological understanding paves the road to targeted and better treatments and improved standard of care (National Research Council 2011). From early in the project, and influenced by Craddock and Owen (2010), B-SNIP had two main questions germane to this journey.
First, there is evidence for continua of severity on both neurobiological and symptom features of relevance to psychosis. There is also a cognitive performance range across all humans, which is one of Craddock and Owen’s (2010) “domains of psychopathology.” A psychosis diagnosis is not required to capture this cognition dimension. Nevertheless, schizophrenia-like cases tend to fall at the deficit/severe and bipolar disorder-like cases at the surplus/mild ends of those distributions. B-SNIP wanted to know, given an idiopathic psychosis, if deficient cognition is a core feature of a schizophrenia diagnosis, as is often assumed (McCutcheon et al. 2023). If not, perhaps cognitive performance is more like a modifying feature across all psychosis rather than central to any specific clinically defined subgroup. This question was related to considering psychosis a “spectrum” that gradually shades from normal to subsyndromal to mild and severe clinical manifestations.
Second, Craddock and Owen (2010) postulated etiological factors at more basic levels of analysis (etiological “hits”), including genetic and neurobiological systems variations, all of which could be influenced by environmental and stochastic events. Some of these factors will necessarily affect where an individual falls along the domains of psychopathology. Other factors, however, could influence the specific clinical expression of psychosis given how they act on neuroanatomical and neurofunctional systems. There might be deviations in neurobiology that predispose to schizophrenia- or bipolar-like presentations. B-SNIP wanted to know if the multiple variations for where a person falls along the domains of psychopathology, combined with specific etiological hits, may cause the jumble of clinical manifestations observed across psychosis cases, even though there are discrete disease entities. This question addressed the possibility of etiological specificity within idiopathic psychosis, even if that specificity is distributed against a pleiomorphic psychopathology background.
4. B-SNIP Approach
The B-SNIP group assumed that there were three keys to successfully addressing the above questions. First, it was crucial to collect psychosis samples of sufficient size across DSM diagnosis (what is called transdiagnostic assessment) to capture representative clinical and neurobiological heterogeneity. Small samples probably account for inconsistent results in the psychosis literature, and almost certainly insufficiently capture hard-to-classify cases. Transdiagnostic assessment was necessary to evaluate specificity of any findings to individual DSM psychosis diagnoses.
This is different from the recent approach of, for instance, large genetics consortia (Singh et al. 2022; Trubetskoy et al. 2022). Those international efforts, that used to do things differently (Cross-Disorder Group of the Psychiatric Genomics et al. 2013), performed case-control comparisons for schizophrenia alone and then inferred, or at least strongly suggested, specificity of genetic findings to that diagnosis without comparison to other psychosis subgroups (e.g., schizoaffective disorder or bipolar disorder with psychosis). They then took the additional step of building schizophrenia specific models of, for instance, hippocampal functioning (Guo et al. 2023) without evaluating the model’s specificity across psychosis diagnoses. Their conclusions may be accurate, but it is impossible to know without transdiagnostic comparisons. The single diagnosis approach is not new and not unique to genetics; it has dominated and perhaps compromised psychosis research across measurement domains for years.
Second, psychosis relevant factors must be quantified at multiple levels of analysis using multiple approaches. At the very least, it was important to canvas neurocognitive and neuro-physiological correlates of psychosis. Deviations in psychosis cover at least those territories, and limiting probes to only one area would almost certainly yield an incomplete, and perhaps a completely inaccurate, geography of psychosis neurobiology. Therefore, we performed dense phenotyping across multiple levels of analysis (molecular measures, structural and functional brain imaging, psychophysiology, cognition, symptom assessments, social functioning evaluations, environmental factors). This approach has the best hope of evaluating whether DSM psychosis diagnoses approximate biological reality.
B-SNIP emphasized so-called neurobiological “endophenotypes” (see Thaker 2008), a term applied by Irving Gottesman to biomarkers that capture inherited predisposition (Gottesman and Gould 2003). The core of B-SNIP’s biomarker battery had the dual purpose of understanding neurobiology and familial liability for idiopathic psychosis. In the late 2000s, B-SNIP’s core measures were the most researched endophenotypes for addressing those issues. Emphasizing an intermediate level of neurobiological deviation also promoted shortening the logical distance between genes and clinical phenotypes. Findings could be probed and verified via associations with more molecular and more clinical and sociodemographic measures, developing and strengthening knowledge of the complex causal network, a common approach in quality biological research (Wilson 1998).
Third, B-SNIP assumed biofactors (i.e., multiple statistically integrated biomarkers), rather than biomarkers considered individually, would best capture psychosis-relevant features. Any single measure probably fails to precisely define any psychiatric disease. Given the state of knowledge, it is unrealistic to assume a single measure adequately assesses any brain function (e.g., auditory sensory registration, target detection, context updating in working memory, behavioral inhibition; behavioral response speed). Single measures of complex constructs are often used in experimental psychopathology and psychiatry, but this approach in psychosis biomarkers research was easily modified. B-SNIP statistically integrated multiple individual measures to assess brain functions of interest, enhancing signal-to-noise (e.g., antisaccade response latency and prosaccade latency both index speed of visual orienting; the auditory ERP N100 response during the paired-stimuli task is assessing a highly similar neural response as the N100 response during the auditory oddball task).
5. Central B-SNIP Biomarker Battery
Fair warning—this section is a detour. It provides summary information about measurements that anchor B-SNIP’s main taxonomic analyses (see Clementz et al. 2022 for complete details). They are the tasks and paradigms from which came dependent variables defining an intermediate location in the multilevel analysis hierarchy. They range from more cognitive to more physiological in nature. For those already familiar with the design, or those less interested in individual contours, skip to the next section’s presentation of B-SNIP’s fundamental DSM psychosis topography.
Brief Assessment of Cognition in Schizophrenia (BACS)
BACS covers multiple cognitive domains (Verbal Memory, Processing Speed, Reasoning and Problem Solving, Working Memory; Keefe et al. 2004, 2006, 2008) and provides an excellent measure of psychosis-related cognitive performance (Hill et al. 2013; Hochberger et al. 2016). Statistical integration over the subtests yielded one BACS biofactor.
Stop Signal Task (SST)
The SST measures efficiency and adequacy of cognitive control when response preparation and the subsequent movement requirement are conflicted (Lipszyc and Schachar 2010). Subjects see a “Go” cue to the left or right of central fixation. On a minority of trials, a “Stop” signal is presented. Participants are instructed to respond to the Go cue as quickly as possible unless they encounter the Stop signal. Psychosis cases on average respond more slowly and make more errors (Ethridge et al. 2014; Gotra et al. 2020). Statistical integration over reaction time and error variables yielded one SST bio-factor.
Pro- and Antisaccade Tasks
Prosaccades (looking at a visual cue) assess the speed of visual orienting, with psychosis cases having highly variable responses, from slower to faster than normal (Clementz et al. 1994; Clementz 1996; McDowell and Clementz 2001; Reilly et al. 2005). Subjects are simply asked to look quickly and accurately at a newly appearing visual stimulus. Alternatively, antisaccades assess at least two abilities: (i) inhibitory control, because the visual stimulus and required response location are incompatible and (ii) goal maintenance, because subjects must remember the response requirement over time (Hallett and Adams 1980; McDowell and Clementz 2001; Ethridge et al. 2009). Subjects look as quickly and accurately as possible to the mirror image location of a peripheral cue (same amplitude, opposite direction). On average, psychosis cases have delayed reaction times and increased error rates (Reilly et al. 2014; Huang et al. 2022). Statistical integration over saccade latency and percentage of error response variables yielded two saccade bio-factors, one for speed of visual orienting and one for antisaccade performance.
EEG During Auditory Paired-Stimuli and Oddball Paradigms
Neurophysiological brain responses to repetitive auditory stimuli (paired-stimuli task, used to measure what is sometimes called “p50 gating”; Freedman et al. 1987) and predetermined auditory targets randomly interspersed with nontarget auditory events (called an “oddball task”; Polich 2007) are commonly encountered in psychopathology research (Thaker 2008). These paradigms assess the neural dynamics of preparation for and recovery from auditory sensory activations, neural responses to stimulus salience, and neural differentiation of relevant from irrelevant auditory stimuli.
For the typical paired stimuli task, subjects passively listen to many auditory stimuli pairs with a short (500 ms) interval between the two stimuli and a long (8–10 s) interval between the pairs. This task ostensibly probes the ability to detect stimulus relevance (or reject stimulus irrelevance), a deficit in some psychosis cases (Adler et al. 1982; Freedman et al. 1987; Hamm et al. 2012, 2014). For a typical auditory oddball task, subjects listen to hundreds of auditory stimuli occurring every 1–1.5 s. Most of the stimuli are the same (e.g., 1000-Hz tones), and are called “standards.’ Some of the stimuli, randomly interspersed with the standards, are different (e.g., 1500-Hz tones), and are called ‘targets.’ Targets elicit a different brain response from the standards, with the most prominent the so-called p300 (a positive voltage waveform in the event-related brain potential most prominent over central parietal lobe sensors occurring 300–400 ms after stimulus onset). The p300 measures updating of information in working (or available) memory, a function that is deficient in many psychiatric conditions, including psychosis (Linden 2005; Polich 2007; Ethridge et al. 2012, 2015; Lundin et al. 2018; Parker et al. 2021).
Electroencephalography (EEG) data are quantified in multiple ways. The most common approach is to estimate neural responding from one or a few EEG sensors at a limited number of time points. From B-SNIP’s perspective, this approach unnecessarily restricts the rich EEG-recorded neural activity data that is distributed across the brain and unfolds in complex ways over time. Instead, B-SNIP maximizes the use of available information using many sensors and time points, with brain responses extracted from the temporal and frequency domains. Scoring data in the temporal domain yields information on the strength of brain signals in voltage units. These signals are typically used to measure event-related brain potentials (ERPs) at specific time points (50, 100, 200, or 300 ms after stimulus onset). Scoring in the frequency domain yields information on brain signals in particular frequency ranges (e.g., delta, theta, alpha, beta, and gamma); this information also can be quantified as a function of time (e.g., gamma activity in the first 100 msec after stimulus onset). Extracting both voltage and frequency provides more information on complex brain responses than is possible using either quantification approach alone. In B-SNIP’s latest iteration, statistical integration over EEG/ERP variables yielded four ERP magnitude biofactors and three intrinsic (background or nonspecific) activity biofactors.
6. DSM Psychosis Diagnoses as the Gold Standard
The initial B-SNIP goal was to identify neurobiological features (i) shared across or (ii) distinctive to the major DSM psychosis diagnosis categories (schizophrenia, schizoaffective disorder, bipolar disorder with psychosis). B-SNIP collected large numbers of patients, so any measures meeting those characteristics would be obvious. Over 13 years, using DSM-IV diagnoses, B-SNIP recruited more than 700 schizophrenia, 500 schizoaffective disorder, and 700 bipolar disorder cases, plus more than 900 people from the community without serious psychiatric conditions to serve as an anchor. We paid participants for the many hours over multiple days they spent providing hundreds of measures; nevertheless, the only way to justly compensate them is if B-SNIP products improve the standard of care.
The best currently published statement on the main outcomes is in Clementz et al. (2022). Participants came from two separate samples collected at least 5 years apart, with n > 900 in each sample. There were a few interesting results. First, every part of the data analysis path exhibited high repeatability. Second, the DSM psychosis diagnoses outcomes were highly similar between samples. Both outcomes are attractive and important because they highlight the analysis approach is structurally sound and that DSM-IV psychosis cases have a common pattern of deviations in relation to each other and the community sample.
The conclusions from DSM diagnosis comparisons are straightforward—because there is not much to tell. Despite remarkable consistencies between samples, DSM-IV schizophrenia, schizoaffective disorder, and bipolar disorder with psychosis did not seem to define obviously distinct neurobiological entities. Figure 1 shows the patterns across the main bio-factor classes as a function of DSM psychosis diagnosis, which describe a neurobiological continuum (schizophrenia < schizoaffective disorder < bipolar disorder < community sample), with considerable group overlap.
Fig. 1.
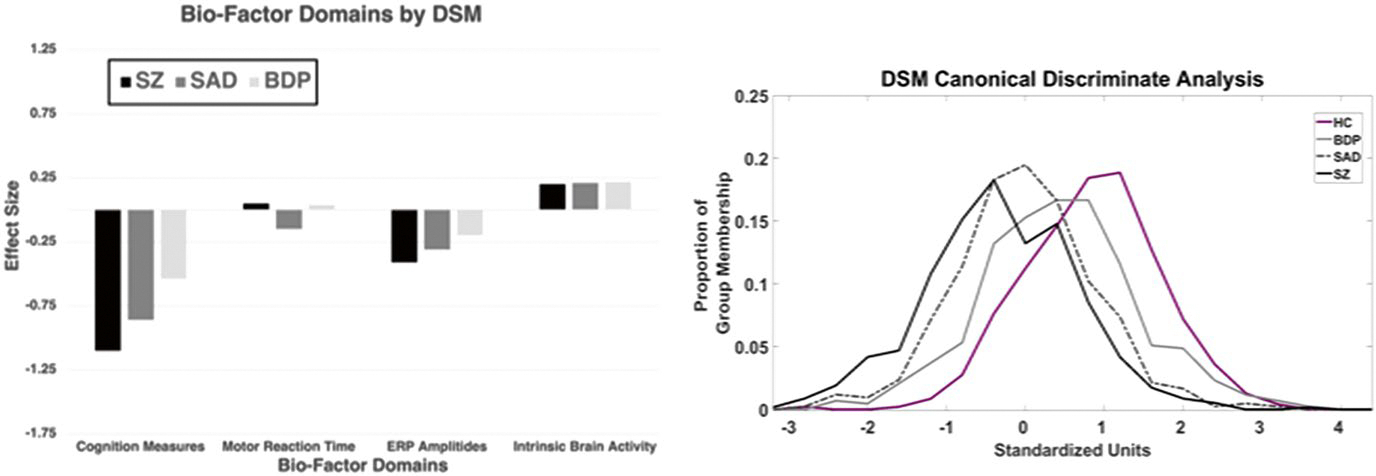
DSM Diagnoses. Left Plot: Glass effect sizes (y-axis) of the main bio-factor domains (x-axis) as a function of DSM psychosis diagnosis. The community sample is represented by the zero line. The Cognition Measures are an average of BACS, antisaccade, and stop signal variables, Motor Reaction Time is speed of responding to saccade targets, ERP Amplitudes are an average of measures indexing strength of neural response to auditory stimuli, and Intrinsic Brain Activity is an average of measures capturing nonspecific brain activity (not locked to processing of any stimulus). Right Plot: The outcome of a discriminant analyses to maximize group separation using all bio-factors. There was one significant function that differentiated the groups. The plot shows the proportion of cases within each group (y-axis) as a function of their standardized discriminant function scores (x-axis). SZ schizophrenia, SAD schizoaffective disorder, and BDP bipolar disorder with psychosis, HC community sample. (Adapted from Clementz et al. 2022)
There are three noteworthy features of Fig. 1. First, consistent with the published literature, psychosis cases have deficient values on cognition and ERP amplitudes (values below the mean of healthy persons). Second, the magnitudes of the between-psychosis group differences are modest. For cognition measures, schizophrenia and bipolar psychosis cases differ by less than 0.5 standard deviation units, with schizoaffective cases halfway between. For ERP amplitudes, the differences are more modest, and no psychosis group has a greater than 0.5 standard deviation separation from the healthy mean. Curiously, despite interest in intrinsic activity as a psychosis, perhaps a schizophrenia-specific, biomarker (Spencer 2014), there is little evidence such is the case in the complete B-SNIP sample when DSM diagnoses are the gold standards. Third, when using all bio-factors simultaneously to improve DSM group separations, the schizophrenia to bipolar disorder separation increases to about 0.90 standard deviation units, again with schizoaffective cases halfway between. This is a modest improvement over cognition alone. It seems unlikely even this amount of biomarker data which reveals no specificity to a DSM diagnosis, and takes days to collect and weeks to quantify, can improve treatment selection and outcome predictions for DSM diagnosis.
7. The Psychosis Spectrum
Before COVID, B-SNIP had annual in-person meetings to review the previous year’s work, what it meant, and routes to pursue in the next year and beyond. In addition to being wonderful bonding occasions, those gatherings stimulated the group’s most inventive discussions. In 2013, we were at the Institute of Living in Hartford staring at Fig. 1 data for B-SNIP1, the first iteration of our project. The undeniable conclusion was that the main DSM psychosis diagnoses described a severity continuum. That fact formed the backdrop for Craddock and Owens’ (2010) domains of psychopathology. The extraordinary outcome was that not a single variable supported the thesis that DSM psychosis diagnoses capture neurobiological distinctiveness. And this was not just true of Fig. 1 variables but extended to all measures in the database, including assessments of brain structure and function (Lui et al. 2015; Ivleva et al. 2017, 2020; Zhang et al. 2020; Guimond et al. 2021; Kelly et al. 2021; Xiao et al. 2022). At about this same time, former NIMH Director, Dr. Thomas Insel, succinctly concluded: “Biology never read that book [the DSM]” (Belluck and Carey 2013).
The B-SNIP archive includes measures of basic sensory processing, sensorimotor performance, inhibitory control, target detection, memory functions, general executive control abilities, and brain imaging. That is expansive terrain. But perhaps B-SNIP used the wrong laboratory measures to address diagnostic specificity, although measures were selected for their demonstrated success. Apparently, though, B-SNIP is not the only consortium struggling to detect the unique substructures of DSM diagnoses. The Psychiatric Genomics Consortium concluded that genetic data “strongly suggest that our [current] diagnostic categories do not define pathophysiological entities” (Sullivan et al. 2018, p. 25).
Dimensions describe the overwhelming majority of variance in psychological and psychiatric phenotypes (Haslam et al. 2020). For idiopathic psychosis, this was the unmistakable conclusion of everyone in that Institute of Living conference room. That deduction was clearly illustrated by an analysis pursued with Robert Gibbons, the Blum-Riese Professor of Statistics at the University of Chicago (Tamminga et al. 2021). The core of Dr. Gibbons’ approach was the observation that deficient cognition captured the majority of B-SNIP’s severity continuum. Cognitive performance is linked to many characteristics, including symptom severity and the structural and functional integrity of the brain (Green et al. 2000, 2004; Lui et al. 2010; McTeague et al. 2016; Zhang et al. 2018; Zhu et al. 2019). Such associations across multiple measurement domains in psychosis research specifically and psychopathology research generally inspired the theory of one transdiagnostic dimension accounting for a broad vulnerability to serious psychiatric syndromes (Goldberg 2015; McTeague et al. 2017; Caspi and Moffitt 2018).
Gibbons evaluated relationships between cognitive performance and other measurement domains across B-SNIP1 psychosis cases (n = 711), their relatives (n = 883), and healthy persons (n = 278). Those domains included: (i) structural MRI (397 Freesurfer variables characterizing cortical volume, surface area, and thickness across multiple regions) and (ii) neuropsychological-psychophysiology measurements (20 neuropsychological measures that were not part of the main cognition dimension, EEG/ERP, and ocular motor measures). Gibbons computed the subject-level relationships between cognitive performance and all those individual variables simultaneously to evaluate if they all fit a single function.
Figure 2 shows the plots averaged over variables within MRI and neuropsychology-psychophysiology domains. These plots have three interesting features. First, psychosis cases span the cognitive range but the overwhelming majority of broadly recruited healthy subjects occupy only the upper three quintiles. Second, the functions are statistically equivalent for probands, relatives, and healthy subjects. Finally, most measures were captured by the overall functions in Fig. 2: (i) 95.5% of MRI measures and 65% of neuropsychology-psychophysiology measures fit this function. The only logical conclusion is that most measurements of key psychosis-related extraclinical features capture a transdiagnostic neurocognition continuum.
Fig. 2.

Overall structural MRI (top plot) and cognition and neurophysiology (bottom plot) standard scores as a function of cognitive performance. The cognitive dimension is plotting in quintiles by different subject groups (healthy in blue, probands in orange, relatives of probands in yellow). When considering all measures in a set, all groups show declines in both MRI and neurophysiology and cognition from high to low cognitive performance levels. (From Tamminga et al. 2020)
8. Categories of Psychosis?
What would Guze think? Would he forego belief in the assumed existence and importance of categorical entities in psychiatry (Guze 1992)? The above data appear to reject, or at least mortally harm, the categorical thesis for the main psychosis diagnoses. Similar outcomes buttress critiques of categorical diagnostic systems throughout psychiatry. At some point, as any good neo-Popperian would agree (Lakatos 1978), one must surrender a failing programme. When considered across multiple levels of analysis, the DSM programme for psychosis is at the very least struggling.
The perpetuation of medical model-type classification in the face of contradictory evidence agitates impatience with DSM-type psychoses diagnostics specifically and across psychiatry generally. Psychiatry might be surrendering the benefits of laboratory tests because the medical model diagnostic approach for psychopathology is wrong. Perhaps, there are no discrete psychosis categories (Esterberg and Compton 2009). Maybe laboratory tests or biomarkers fail to differentiate discrete diagnoses because there are no such differentiations to make. The lack of clear demarcation between health and serious psychiatric conditions, and between conditions is, at the very least, awkward (Kendell and Jablensky 2003).
Clinicians might consider evaluating patients on quantitative measures shading from normal through subsyndromal to pathological levels of severity, rather than using fictive categories. The premise of dimensional approaches is that certain traits, symptoms, cognitive domains, or physiological parameters lie on measurable spectra independent of either pathology (because healthy people also fall on the dimensions) or current specific clinical diagnoses. B-SNIP outcomes using DSM diagnoses as the gold standard support this view. Heckers et al. (2013) even described an attractive model for psychosis presentations (see their Fig. 1) that includes assessments of delusions, hallucinations, disorganized speech, psychomotor behavior, negative symptoms, cognition, depression, and mania. We might have added a spoke for social functioning to Heckers’ psychosis assessment wheels. Kotov et al. (2020) statistically derived a “psychosis superspectrum” which may capture meaningful variance across genetics, environmental and psychopathology risk, neurobiology, treatment response, and outcome variables.
The assumption is that evaluating such dimensions will improve treatments that target domains of relevance for individual patients and is perhaps where biomarkers can have their best impact. Tailoring treatments for individual patients to the most relevant of the many possible ills, dysfunctions, and abnormalities that may befall the person seeking psychiatric care is unquestionably a laudable goal (Keshavan and Clementz 2023; Zhang et al. 2023). In medicine outside of psychiatry, there are dimensional scales used for treatment targeting (e.g., blood pressure for hypertension, lipoprotein profile for cholesterol, ejection fraction in heart failure, blood glucose level for diabetes, and pathologist ratings of tissue biopsies). Those laboratory measures have the benefit of being easily obtained and described to the patient, providing an index for evaluating a treatment’s effectiveness and determining when the patient is “cured.” Based on hope and evidence, the dimensional approach for psychiatry is worth careful consideration.
9. Critiques of Categories in Psychiatry
Numerous slings and arrows pierce the armaments of the psychiatric establishment’s categorical fortress. Critics decry the overlap of symptoms between different diagnoses, heterogeneity of clinical pictures within the same diagnosis, the high rates of psychiatric comorbidity, marginal reliability and stability, and the lack of external validators (Insel et al. 2010; Cuthbert and Insel 2013; Goldberg 2015; Guloksuz and van Os 2017, 2021; Hengartner and Lehmann 2017). They highlight that sophisticated and unimpeachable statistical analyses of complex and extensive clinical characteristics only reveal dimensional structure (Krueger et al. 2018; Kotov et al. 2020). Such analyses, which start at the level of clinical features, expose no evidence for cuts or points of rarity in the distribution of those integrated clinical distributions.
Many areas of clinical medicine outside of psychiatry, however, are also subject to these same critiques. Should psychiatry be concerned about the overlapping symptoms issue? Abdominal pain, cough, edema, fatigue, fever, and nausea — we could go on — are common complaints in general clinical medical practice and are features of multiple diseases and syndromes. How about heterogeneity of clinical presentations within a diagnosis? In typically insightful fashion, Wakefield (2022) addressed this critique:
Just to take a simple example all too close at hand: upon searching, I get a list of 16 possible COVID-19 symptoms ... if any two or more of them is considered cause for inferring possible disease ... there are 65,519 symptom profiles, many non-overlapping. (p. 13)
Wakefield (2022) also addressed the high rates of comorbidity criticism:
... about 77% of older individuals have two or more chronic physical disorders at any one time .... Given the high level of interaction and integration among psychological modules, dysfunction in one module could tend to cause unusual behavior or even dysfunction in another linked module, even though “pure” one-module dysfunctions are also possible. (p. 13)
For at least some idiopathic psychoses, there is overwhelming evidence that the troubling clinical manifestations are the end stage of a neurodevelopmental trajectory (Weinberger 1996; Insel 2010). Psychosis symptoms are not the disease, but the result of a condition to which the brain, the relevant organ system, is no longer able to adapt. Considered in this context, it is not unusual for persons with one chronic condition to accumulate other conditions over time. Alzheimer’s, Huntington’s, and Parkinson’s diseases start with circumscribed lesions, but the pathology extends to include considerable expanse of brain territory. Those invasions cause the accumulation of behavioral, cognitive, and emotional deviations that were not part of the presentation precipitating the initial diagnosis.
It is worrying when different clinicians see the same patient but disagree on the diagnosis. But it is often overlooked that the theoretical validity of a diagnosis is the square root of reliability. Even rater agreement of 0.50 means a 0.71 ceiling on validity, not a terrible start when bootstrapping a diagnostic definition. Nevertheless, psychiatry should expect and achieve better. There are also multiple chronic medical conditions where clinical pictures wax and wane (e.g., multiple sclerosis, lupus erythematosus, Parkinson’s, Alzheimer’s, neurosyphilis), sometimes as part of the natural course and sometimes because of treatments’ wavering efficacies.
So, are the above critiques fatal flaws of medical model-type, categorical systems for classifying all psychiatric conditions? The conclusion in most clinical medicine is not that complications eliminate the possibility of disease categories. Medical nosology evolves, with that evolution not necessarily eliminating, but rearranging, diagnostic criteria.
Progressions in syndrome or disease definitions are not just shuffling deck chairs on the Titanic. Familiar and commonly invoked historical instances of previously embraced diagnoses include dropsy, as mentioned above, and pyrexia (see Clementz 2022, for a brief analogy to psychosis). There are other examples of diagnostic evolution. For instance, seizures are a nonspecific and sometimes troubling indicator of neurological dysfunction, with multiple manifestations that can be rated from mild to severe (O’Donoghue et al. 1996), and often carry deleterious social and occupational consequences (O’Sullivan 2015, 2018, 2021). Knowledge of seizure etiology has improved from crude understanding and accompanying horrific treatments to the current ability to diagnose specific lesions and conditions with various treatment indications (Penfield 1977; Dittrich 2016; Espay et al. 2018). Diagnosis and treatment of seizures was modified by the upgrading of etiological knowledge. The traditional approach to cancer diagnosis and treatment is no longer tenable (Begg et al. 2013). An organ system affected by a tumor is an organizing principle now superseded in sophistication by the tumor’s molecular profile independent of the tumor’s bodily location. The conclusion from these instances was not that categories in epilepsy or cancer diagnoses were invented but that nosological refinements were required to improve treatment targeting and standard-of-care.
Why did medical diagnostics in the above cases advance standard of care while psychiatry is perpetually mired in conceptual debate? This is a complex and multiply determined question, but one issue deserves special consideration. Examples of evolution in medical diagnostics, as illustrated by the dropsy quote from 1837, at least raise the possibility that exclusive reliance on signs and symptoms is problematic for psychiatry.
In other medical realms, more mature and terraced understanding of mechanisms revealed how different syndromes and diseases yield superficially similar forms. Reaching mechanistic knowledge was tough without embracing etiological heterogeneity and variable expressivity of clinical pictures. The outcome of the DSM-II to DSM-III transition was a major event in the history of psychiatry (Horwitz 2021). But even contemporary diagnostic criteria still rely solely on clinical features, untethered from etiological or pathophysiological knowledge. Other branches of medicine reveal that “diagnoses based primarily on symptoms and signs has proven to be useful only up to a point” (Guze 1992, p. 45). Of course, unless there is evidence, it is only conjecture that a different approach can help identify psychosis categories linked to neurobiology. Robins and Guze (1970) selected schizophrenia to illustrate their classical validity approach. If there was a region of psychiatry where evidence for categories await discovery, its most serious conditions seemed like a decent place to start.
10. Psychosis Biotypes
How does a seasoned and responsible scientific team proceed when their primary thesis is refuted? One option is retirement. Another option is to consider the difference between a scientific hypothesis as stated in words and constructs used to test that hypothesis. Theories and associated hypotheses are subject to nuance and modification, just like medical diagnoses. The trick is knowing when there is substance behind modifying a theory versus maintaining a failing idea despite overwhelming and inarguable evidence to the contrary (Lakatos 1978). The former is part of a legitimate scientific enterprise.
A primary assumption of B-SNIP’s initial hypothesis was that DSM psychosis diagnoses estimate neurobiological entities. This issue was a matter of considerable debate for years, with arguments intensifying during the development of DSM-5 (Wexler 1992; Hyman 2010). What if this critical auxiliary hypothesis was wrong? If it was wrong, how could we know? What was the line beyond which signs and symptoms hinder the search for neurobiologically differentiable subgroups among idiopathic psychosis cases (e.g., Guze 1992)?
B-SNIP modified their approach by defining Guze’s “up to a point” as presence of an idiopathic psychosis, regardless of the diagnosis. This meant qualifying for a psychosis of unknown cause under DSM’s so-called Criterion A list, but other approaches could be used (e.g., Gibbons et al. 2022). B-SNIP then searched for neurobiologically homologous subgroups using all psychosis cases and variance across laboratory measures from the central biomarker battery. If cases neatly organized themselves into subgroups by cognition and physiology, then DSM diagnoses were the impediment. Figure 3 provides a pictorial representation of the strategy.
Fig. 3.

Psychosis is a characteristic of schizophrenia, schizoaffective disorder, and bipolar disorder with psychosis, all pathophysiologically complex diagnoses. These clinical diagnoses were not distinguishable by B-SNIP’s extensive biomarker panel. Psychosis subjects, therefore, were combined into a single group, independent of DSM diagnosis, and biomarker variables were used to define subgroups with shared neurobiological variance. Numerical taxonomy (the prism) identified subgroups, called Biotypes-1, -2, and -3. The groups had distinctive neurobiological characteristics, including on variables not used in their definition (called external validators). Neural characteristics as they segregate in these groups could be the basis for distinct molecular and therapeutic targets. (From Supplement in Clementz et al. 2016)
A key issue is how to meaningfully parse psychosis-relevant biomarker variance. There are many options, but B-SNIP selected a numerical taxonomy method called k-means clustering of bio-factors. This method forms groups of cases defined by their centroids (or center of mass) in the multiple bio-factor space, with all cases in a group being as close to their respective centroid as possible.
A source of worry for the B-SNIP crew was that most numerical taxonomy approaches, including k-means, yield a solution regardless of the true state of nature. The analytical team took numerous approaches to inoculate the outcomes against this critique from themselves and others. The details appear in Clementz et al. (2022), including an extensive supplementary methods and results. Multiple independent approaches quantitatively or quasi-quantitatively established that three psychosis subgroups best captured neurobiological variance among the bio-factors. B-SNIP1 had at least one first-degree biological relative for every psychosis case, and those relatives showed the same biofactor patterns as the cases to whom they were related (Clementz et al. 2016). Replication is always the best test of any outcome, and the three-subgroup solution repeated with high similarity (r = 0.95) using an independent sample of psychosis cases and community volunteers. The classification solutions also cross validated, as demonstrated by taking the algorithm calculated in the initial sample and applying it to the replication sample and vice versa; cases were sorted into the same subgroups with about 90% accuracy. Additionally, the B-SNIP team externally validated differences between the psychosis subgroups using measures not included in subgroup creation (Hudgens-Haney et al. 2017, 2018; Ivleva et al. 2017; Reininghaus et al. 2019; Guimond et al. 2021; Kelly et al. 2021; Clementz et al. 2022; Xiao et al. 2022); that work continues.
Figure 4 displays the same cases from Fig. 1 by their bio-factor-derived subgroups rather than by their DSM diagnosis. The B-SNIP PIs inspected a similar figure in that Institute of Living conference room back in 2013. In comparison to the DSM outcome, this solution was captivating. A flurry of animated discussions included contemplating subgroup names. The most conservative approach was to forgo descriptive terms, like “Kraepelinian psychosis.” After pondering numerous impractical alternatives, Carol Tamminga suggested “Biotypes,” for “biologically distinctive types.” In biology, “Biotype” refers to organisms sharing underlying defining features, like physiology or constitutional characteristics. We learned later that Andreasen (1987) was the first to use “Biotype” in the schizophrenia literature to juxtapose biology and clinical phenomenology. Given the limited understanding of these newly derived subgroups, “psychosis Biotypes” (capitalized because they are entities, not a general concept) offered a decent balance between providing a label and reification.
Fig. 4.

Biotypes. Left Plot: Glass effect sizes (y-axis) of the main bio-factor domains (x-axis) as a function of Biotype. The community sample is represented by the zero line. The Cognition Measures are an average of BACS, antisaccade, and stop signal variables, Motor Reaction Time is speed of responding to saccade targets, ERP Amplitudes are an average of measures indexing strength of neural response to auditory stimuli, and Intrinsic Brain Activity is an average of measures capturing nonspecific brain activity (not locked to processing of any stimulus). Right Plot: There were two discriminant functions that differentiated the psychosis Biotype groups. The first function on the x-axis captured “Neural Response Magnitude,” and the second function on the y-axis captured “Neural Disinhibition”. Frequency polygons show the proportion of cases by group at the bottom (Neural Response Magnitude) and right (Neural Disinhibition) of the central plot that shows the centroids and standard deviation ellipses by group. BT1 = Biotype-1, BT2 = Biotype-2, BT3 = Biotype-3; HC = community sample. (Adapted from Clementz et al. 2022)
There are five noteworthy conclusions to draw from the Biotypes solution. They all at least inspire questions about assumed knowledge concerning idiopathic psychosis. First, a dramatically different and replicable outcome from the DSM approach addresses previous inconsistencies in the literature. With cases sorted by Biotype, all biofactors appear uniquely interesting. Sometimes, this meant subgroup values below, sometimes above, and sometimes the same as the comparison sample. All such outcomes had been variously reported for DSM psychosis diagnoses. This illustrates the importance of using samples large and representative versus drawing conclusions from those small and unrepresentative. If the differences between Figs. 1 and 4 fail to make the point, Biotypes do not recapitulate, or even grossly estimate, DSM psychosis diagnoses (Fig. 5). The only possible exception is that bipolar disorder cases occur with higher frequency in Biotype-3, but over 50% of that neurobiological subgroup is still composed of schizophrenia and schizoaffective cases.
Fig. 5.

Percent of cases conditioning on an initial group classification. The left plot shows the percent of cases with a particular DSM diagnosis across Biotypes, and the right plot shows the percent of cases with a particular Biotype across DSM diagnoses (e.g., the values within the black SZ line sum to 100; the values within the blue BT1 line sum to 100). BT1 = Biotype-1, BT2 = Biotype-2, BT3 = Biotype-3, SZ = schizophrenia, SAD = schizoaffective disorder, and BDP = bipolar disorder with psychosis. (Adapted from Clementz et al. 2023)
Of related relevance, and second in the conclusions list, Biotype-3 cases are like the comparison sample on all biofactors, even though they qualified for an idiopathic psychosis. If any neurobiological features define Biotype-3, they are not specifically captured in this plot, a plot based on a generation’s worth of psychosis biomarker research using DSM targets. But as Henri Bergson famously said: “The eye sees only what the mind is prepared to comprehend.” The neuroscience of idiopathic psychosis has been dominated by DSM case-control comparisons since DSM-III. The field learned a lot but maybe overlooked important factors obscured by this approach to subgroup creation. For instance, only after epilepsy diagnosis advanced through improved understanding and better technology was it possible to identify that functional seizure cases may have unique neural signatures (Bègue et al. 2021; Perez et al. 2021; Weber et al. 2022).
The third curious conclusion from Figs. 4 and 5 is that Biotype-1 and Biotype-2 have roughly similar percentages of DSM psychosis diagnoses among their memberships. More than half of bipolar disorder cases are evenly split between Biotypes-1 and -2. Cognitive deficit is restricted to these two Biotypes and effectively absent from Biotype-3. This means that a nontrivial proportion of bipolar disorder cases are carrying cognitive deficits of the same magnitude as schizophrenia and schizoaffective cases and that about a third of both schizophrenia and schizoaffective cases are missing the cognitive deviations thought to characterize those conditions (McCutcheon et al. 2023). It is also possible that in the absence of psychosis, Biotype-3 cases would have even better cognition (Hochberger et al. 2018), making them super cognitive performers compared to community volunteers. Appraisal of constitutionally expected cognitive performance is not the way such evaluations are typically used in psychosis research and practice. Perhaps that should change.
The fourth conclusion relates to the undeniable ubiquity of a cognitive performance dimension when the analysis method is meant to produce such an outcome. The right half of Fig. 4 shows the canonical discriminant function dimensions that simplify visual presentation of the multiple biofactors distinguishing Biotypes. The discriminant analysis eases, but does not exactly recapitulate, the location of cases in hyperdimensional biofactor space. But the computations provide a direct comparison to the DSM discriminant analysis solution presented in the right half of Fig. 1 and reveal a 2–2.75 standard deviation separation between Biotype centroids in Cartesian space. The first dimension, on the x-axis, is labelled “neural magnitude response” because of its primary contributions from strength of ERP/EEG neural responses combined with general cognitive functioning—lower scores on this dimension mean deficient ability to generate a robust EEG/ERP signal and lower cognition scores. There is a clear continuum from Biotype-1 at the deficit end to Biotype-3 and healthy community volunteers at the surplus end—this contrasts with clear differentiations of Biotypes-1 and -2 and Biotype-3 and healthy persons when biofactors are considered individually. There is obviously a difference between using measures individually and a statistical approach that creates an efficient and integrated solution.
The fifth and most striking conclusion from Fig. 4 is the dramatic differences between Biotypes-1 and -2 on measures of brain physiology. Biotype-1 is characterized by low physiological activity across ERP and EEG measurements, while Biotype-2 has near normal ERP amplitudes but accentuated intrinsic (background or ongoing) neural activity. These deviations span paradigms, quantification approaches, ERP components with different neural source configurations and functional purposes (e.g., auditory and visual n100, auditory p300, auditory and visual steady-state stimulation), and different methods for quantifying intrinsic brain activity (voltage and frequency across rest periods between stimuli, during 5 min of unstructured EEG recording, and neural activity not locked to stimuli presentation during ERP tasks—so-called induced activity). They are also consistent during complex cognitive tasks and during efforts to drive auditory and visual systems (Hudgens-Haney et al. 2017, 2018; Clementz et al. 2022). Biotype-2’s accentuated neural activity is paired with more inhibition failures (Clementz et al. 2022), which makes for a nice cohesive story. These patterns capture stable differences between Biotype-1 and -2 cases in the absence of efforts to specifically modify those physiologies (Clementz et al. 2022).
In an analysis described in the DSM section, Robert Gibbons showed that an overwhelming percentage of structural MRI and cognition-psychophysiology variables fit and are apparently explained by an overall cognition dimension. Such an all-encompassing outcome may yield the impression there is no remaining meaningful variance to explain. As it happens, the ways this assumption are false compliments noteworthy knowledge of brain structural and functional deviations in idiopathic psychosis.
Gibbons exposed two complimentary findings for structural MRI measures. Variables statistically deviating from the primary cognition dimension include most measures of hippocampus on the one hand and brain space enlargements and/or lesions on the other (e.g., all ventricular volumes, white matter signal abnormalities, overall CSF). The entire hippocampal complex bilaterally shows a more devastating decline over cognitive performance than all other brain measures. The hippocampal complex is central to neurodevelopmental models of psychosis, so this outcome nicely compliments that literature (Tamminga et al. 2010; Jirsaraie et al. 2018; Guo et al. 2019). The distribution of brain space-lesion measures is shown in Fig. 6 and illustrate a discontinuity within psychosis cases at the deficit end of cognition. B-SNIP genetics data confirm the temporal horns of the lateral ventricles have a specific genome-wide significant hit with Neurexin 1 (NRXN1; Alliey-Rodriguez et al. 2019). NRXN1 supports synapse formation, and its complete deletion is associated with psychosis and autism (Duong et al. 2012; Schaaf et al. 2012). Perhaps the hippocampal complex and adjacent structural alterations are critical for indexing the specific etiology of a psychosis subgroup, an outcome only visible via analyses sidestepping DSM diagnoses.
Fig. 6.

MRI measures that deviate from the BANCC pattern. Brain space volumes are plotted by cognitive ability (in quintiles) and subject group (healthy in blue, probands in orange, relatives of probands in yellow). Brain space measures, like ventricular volume, are a set of variables that do not follow the overall pattern displayed in Fig. 11, with especially probands showing a marked deviation from the canonical pattern at the deficit end of cognitive ability. (From Tamminga et al. 2020)
Gibbons also revealed two complimentary findings within the psychophysiology variable set. Intrinsic brain activity, which captures a dramatic difference between Biotype-1 and Biotype-2 physiologies, deviates from the overall cognitive dimension (left half of Fig. 7). Healthy subjects with high cognitive performance have notably and substantially lower intrinsic activity than the other groups (blue arrow). Alternatively, ERP magnitudes to salient stimuli specifically index Biotype-1, and they track with the overall cognition function for probands and relatives but not for healthy people (right half of Fig. 7; black arrow). Healthy persons, but not probands and relatives, maintain ERP magnitudes across their cognition range. Signal fidelity is always a function of (i) background neural activity against which the signal-specific neural response is generated, and (ii) signal strength to salient stimuli. Even when psychosis cases generate a robust neural response to salient stimuli, their signal-to-noise (ERP magnitude/intrinsic activity) is lower than normal. This is also true for healthy persons in the middle range of cognitive performance because their background noise is higher than for their high cognitive performance compatriots. Signal-to-noise becomes especially dire in psychosis as cognition declines because background noise is higher than normal, and signals related to information processing are severely diminished.
Fig. 7.

EEG measures that deviate from the BANCC pattern. Intrinsic EEG activity (left plot) and ERP magnitudes like N100 and P300 (right plot) are displayed as a function of cognitive ability quintiles and subject group (healthy in blue, probands in orange, relatives of probands in yellow). Intrinsic activity does not follow the canonical pattern of Fig. 11 for any group; ERP magnitude does not follow this pattern for healthy persons, meaning they are able to generate ample ERP responses independent of cognitive ability, giving them an advantage in signal-to-noise ratio over a broader range of cognitive abilities. At the high end of cognitive ability, healthy persons have a decided signal-to-noise advantage given their very low intrinsic activities (blue arrow) in combination with robust neural responses to salient stimuli (black arrow). (From Tamminga et al. 2020)
Apparently, multimodal assessments are necessary to appreciate both the ubiquity of a cognitive performance dimension regardless of psychiatric status and that there are distinct psychosis-related deviations not captured by that dimension. There are measures of brain structure and function that deviate from the canonical pattern, what the B-SNIP crew calls “bio-indicators,” that may index diseases within what is now idiopathic psychosis. Bio-indicators are superimposed on the cognition dimension common to all humans and may parse specific etiologies from a multivariate-polygenic background. These outcomes are at least consistent with Craddock and Owen’s (2010) formulation of domains of psychopathology and the concept of additional etiological hits superimposed on those dimensions.
11. Clinical Implications of Psychosis Biotypes
Biotypes are mixtures of DSM diagnoses, and the patterns of their neurobiological deviations are obscured by the traditional clinically defined diagnoses. Possibly essential practical differences between these approaches are illustrated by three complementary bits of evidence. The first bit is related to clinical differentiators of psychosis Biotypes. The first step in every medical evaluation is thorough description of clinical presentation, during which clinicians generate diagnostic hypotheses based on interview and observations. In some settings, like Elva Scott’s Alaskan kitchen and many rural community mental health centers, access to high technology diagnostic equipment is limited. To be widely practically useful, neurobiologically-derive psychosis Biotypes must be differentiated by easily ratable clinical characteristics, at least to a first approximation. Again, with Robert Gibbons, B-SNIP tested whether efficient clinical characterization of psychosis Biotypes is possible, a true attempt at a bottom-up (really, middle-up) derivation of unique clinical classifiers.
Gibbons and his University of Chicago collaborator Ishanu Chattopadhyay’s ensemble decision tree model expertise paid dividends (Clementz et al. 2023). They discovered that the sensitivities, specificities, and areas under the curve for efficient clinical differentiations of psychosis Biotypes are uniformly high (in the 0.80 range). Only 10–11 clinical ratings are needed to efficiently assign a case to a Biotype. The top clinical characteristics for differentiating psychosis Biotypes, in order of importance, are difficulty in abstract thinking, social functioning, conceptual disorganization, severity of hallucinations, stereotyped thinking, suspiciousness, unusual thought content, lack of spontaneous speech, and severity of delusions. Ratings of social involvement and clinical signs of cognition, thinking, and speech deviations are most important for differential Biotype categorization. The conclusion is that anyone can derive a Biotype estimate using a simple clinical assessment.
The associated algorithm (called ADEPT) is adaptive, so the influence of items, and the order in which they are assessed, is unique to an individual case. Nevertheless, Biotypes-1 and -2 are remarkable for their more abnormal scores in relation to Biotype-3, with Biotype-2 the most clinically deviant. The constellation of clinical features most important for Biotypes differentiation are not captured by any current scale for initial classification or evaluating treatment outcomes. They are combinations of social functioning and traditional positive, negative, and general psychopathology qualities. Typical instruments for tracking clinical outcomes (e.g., PANSS, BPRS) may add noise to assessments requiring a different, but empirically derived, type of precision.
Biotypes have differentiating clinical characteristics, so diagnosticians in any setting can identify neurobiologically defined subgroups to facilitate comparative investigations of etiology and clinical utility. Here is where we encounter the second and third bits of possibly useful complimentary evidence. The physiological differences between Biotypes offer specific treatment targets not provided by any other currently available scheme for subgrouping psychosis cases. The only way to determine improved efficacy for treatment selection is to directly compare available schemes. This is the heart of the scientific enterprise.
Biotype-1 and -2 cases have equivalently poor signal-to-noise (Hudgens-Haney et al. 2017, 2018), the former due to deficient neural responses to salient stimuli and the latter due to accentuated intrinsic or background brain activity (Figs. 4 and 7). Both types of cases need signal-to-noise adjustments, but the means to achieve that end theoretically differ. Medalia et al. (2019) used a sensory training paradigm that should specifically enhance ERP magnitudes, and they modestly improved signal processing and cognition in a mixed group of schizophrenia participants. The second bit of information comes from pilot data where the B-SNIP team slightly modified Medalia’s case selection approach. They differentiated between Biotype-1 and other cases, assuming only Biotype-1 would be affected by an intervention targeting one of their main physiological deviations. Only 26 participants have so far participated, but the intermediate results are promising. Figure 8 shows the change in neural response magnitudes between baseline and after 16 (midpoint) and 32 (post-exposure) sensory intervention sessions. Only Biotype-1 cases show an enhancement, while a mixed group of Biotype-2 and -3 cases show essentially no change on a function where they need no adjustment. A variation on this sensory training procedure for Biotype-2 cases may modify their signal-to-noise by reducing intrinsic brain activity but have no effect on overall sensory functioning for Biotype-1’s.
Fig. 8.
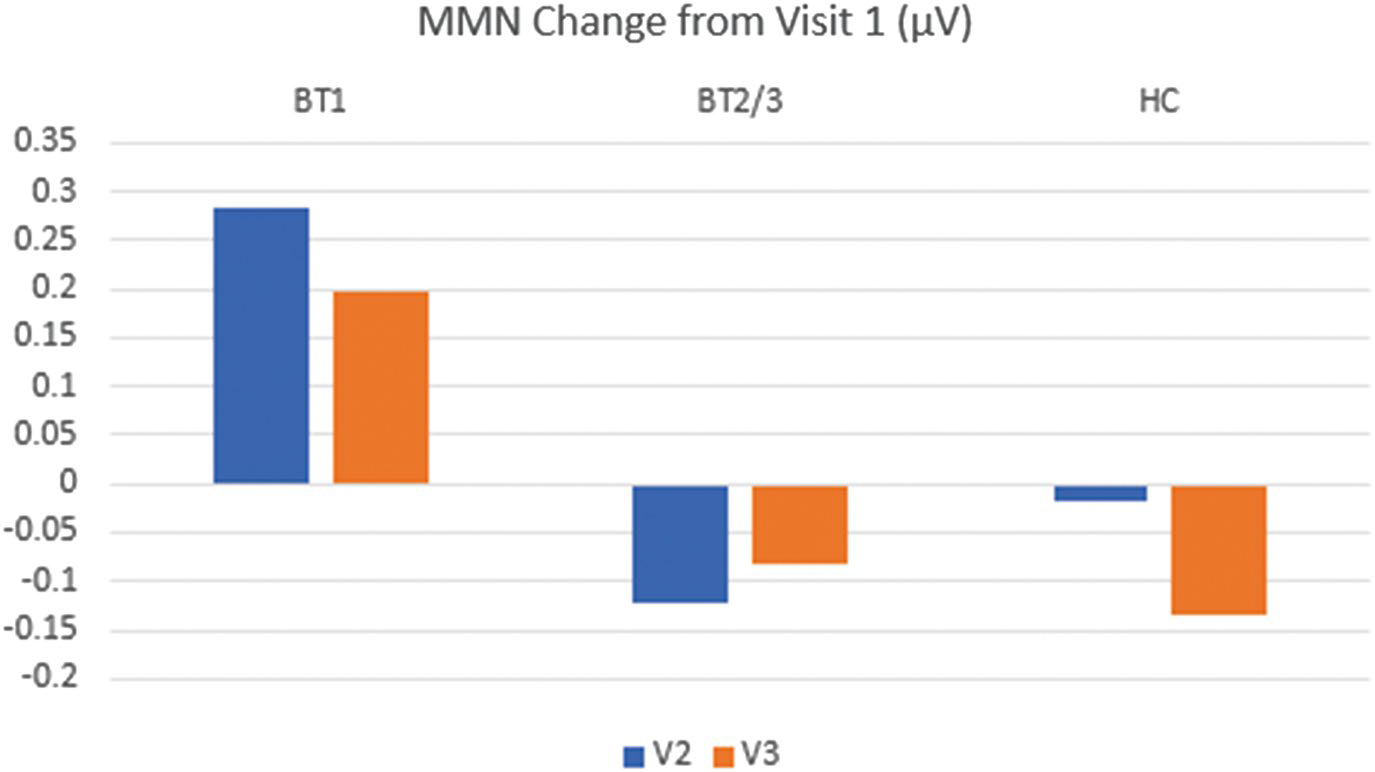
Mismatch negative changes following 16 (V2) and 32 (V3) sensory intervention exposures among Biotype-1 (BT1), a mixed group of Biotype-2 and -3 (BT2/3), and HC (healthy community) participants. Values above zero indicate enhancement
The final bit of complimentary information relates to another Biotypes-specific treatment target. Clozapine is the most effective antipsychotic drug (Keshavan et al. 2022), but is underused because of the possible occurrence of troubling side effects and sometimes complex administration (Leung et al. 2022). If there was a means to identify responsive cases in advance, clozapine could be used more decisively. Clozapine’s unique antipsychotic action remains unexplained. However, we know that unlike other antipsychotics, clozapine increases alpha and theta electroencephalography power in a resting state (Raymond et al. 2022). These neural oscillation frequencies are main components of a B-SNIP bio-factor.
As it happens, B-SNIP has cases off and on clozapine across psychosis Biotypes; their patterns of intrinsic activity are displayed in Fig. 9. The largest percentage of cases are not taking clozapine, and those cases show the pattern of intrinsic activity deviation captured in Fig. 4. Across all psychosis cases, taking clozapine is associated with higher levels of intrinsic activity, mirroring the literature. The most intriguing outcome, however, is that Biotype-1 cases on clozapine are at the level of healthy subjects, but Biotype-2 and -3 cases on clozapine are farther from normal. These data are not from a treatment trial; subjects were not randomly assigned to treatment groups. Nevertheless, this outcome is consistent with the archival literature, and at least suggests the possibility that Biotype-1 cases may have physiology that predicts their uniquely favorable response to clozapine (see Tamminga et al. 2021). This hypothesis is the subject of an ongoing clinical trial by the B-SNIP team.
Fig. 9.

The heads plots show a flattened top-down view of EEG alpha activity recorded from 64 sensors arranged around the head. Darker blue (Biotype-1) means weaker and darker red (Biotype-2) means stronger signals. The bar chart shows intrinsic EEG activity on the y-axis for Biotypes-1, -2, and - 3 in relation to healthy level of brain response (at 0 on the y-axis). Biotype groups are separated by those off and on clozapine. There is a main effect of drug. Biotype-1 s on clozapine are at normal level of intrinsic activity. Biotype-2 s on clozapine are dramatically high on intrinsic activity. Biotype-3 s on clozapine are at typical Biotype-2 levels of intrinsic activity deviation
12. Categories or Dimensions of Psychosis?
People outside of psychiatry, including medical professionals in other disciples, are surprised that laboratory and biomarker information are not required to make psychiatric diagnoses. They are puzzled that laboratory data are not routinely used to inform treatment or track course and outcome. Elva Scott might have thought all of psychiatry borders the Yukon Territory. At present, psychiatry’s legitimacy depends on the clinician’s observational acumen and a belief in the patient’s report of their complaint, free from etiological or any other defining biological knowledge. Except for limited physiology or laboratory information supporting, but not diagnostic of, some substance-related and neurocognitive disorders, a psychiatric clinician may use laboratory tests to eliminate but not to rule in a diagnosis. Moreover, even if the cause of, for instance, substance-related and neurocognitive disorders is assumed (substance ingestion or brain insult/injury), the mechanisms by which any clinical features arise from these causes remain enigmatic.
The above presentation suggests some possible reasons for this state-of-affairs and approaches that may help resolve this less-than-ideal situation for clinicians, but especially for patients. The reasons for this situation may also at least partially explain why psychiatry is perpetually immersed in the categories versus dimensions debate. Following is a list of issues for the reader’s consideration:
Schizophrenia was changed to a reality distortion diagnosis at the time of DSM-III, dramatically altering the concept from its historical core of an affect-self-volition syndrome (Clementz 2023). Hallucinations and delusions are common across psychiatric and neurological conditions. They are not so useful for differential diagnosis except for determining if a case has a psychosis. Modification of the schizophrenia construct had the lingering effect of perpetuating the belief that psychosis symptoms—clinically analogous to dropsy, headache, pyrexia, or seizures—are the main defining characteristics of a single psychiatric illness.
The effect of this historical modification appears to be that DSM diagnostic criteria for idiopathic psychosis inadvertently created a clinical severity scale rather than one based on unique differentiating features. This scale includes a prominent cognition dimension that captures most variables used in psychosis research. This is consistent with multiple studies over many levels of analysis, including B-SNIP data presented above. One conclusion is that most measures and paradigms used in psychosis research, traceable to DSM-III’s approach to schizophrenia diagnosis, index a single construct that is part of the human condition. This outcome also helped foster the belief that there are no disease categories within psychosis. This may be true, but the evidence upon which such conclusions are based appears insufficient for that task. This circumstance may have changed recently with DSM-5’s elimination of preference for Schneiderian first-rank symptoms in schizophrenia diagnosis (Carpenter 2013), but it is too soon to know.
Psychosis is a manifestation of the brain failing to adapt to a pathological circumstance. The difference between psychosis and, for instance, pyrexia (Clementz 2022), is that there is a recognized mechanism for fever generation. Antipsychotic medications importantly and undeniably helpfully treat reality distortions, analogous to fever reducers, but not the historical core features of schizophrenia (affect-self-volition disturbances). Richard Wyatt et al. (1988) succinctly summarized a similar position in the very first issue of Schizophrenia Research. However, identifying a clear psychosis mechanism independent of any specific psychosis diagnosis, would focus clinicians and researchers on a troubling clinical manifestation that requires immediate relief, like is the case for dropsy or pyrexia. In the meantime, investigators could vigorously search for underlying causes of those troubling clinical manifestations, as was so nicely outlined in the dropsy quote from 1837. To accomplish this differentiation, the field must embrace the difference between a dramatic clinical event and the etiology responsible for that event. The B-SNIP team took a step in this direction (Stan et al. 2019). There is a specific association between psychosis symptoms and cortical thickness in a contiguous cluster of brain regions spanning temporal, parietal and inferior frontal lobes — the thinner the cortex in those regions, the higher the psychosis symptom scores, independent of a patient’s subgroup membership. This is a general neurobiological link to severity of psychosis.
B-SNIP demonstrated the possibility of deriving neurobiological subgroups of psychosis with unique defining features. It was necessary to bypass DSM psychosis diagnoses to do so. Psychosis Biotypes yield specific etiological possibilities and treatment targets that are not derivable from any other available approach. This does not mean B-SNIP fortuitously derived the correct diagnostic model; the solution is a function of the variables used and methods applied. The best scientists spend their careers believing even their cherished theories are wrong, but they might be a little more correct than what people used to think. The B-SNIP outcomes yield testable hypotheses in the spirit of Platt’s strong inference (Platt 1964; Carpenter et al. 1993). David Quammen once wrote that science is not about providing answers but asking better questions. That is what we have tried to accomplish in this presentation and what B-SNIP have tried to do with their work.
Psychosis Biotypes illustrate at the very least physiological heterogeneity. For instance, Biotypes-1 and -2 have similar clinical characteristics, but they apparently come by those features via different patterns of brain deviations. They have superficially similar signs and symptoms, but B-SNIP was nevertheless able to derive a clinical evaluation efficiently differentiating those subgroups. Starting with clinical features, rather than neurobiology, did not offer the same level of combined neurobiological and clinical specificity. Even negative symptoms are not neurobiologically homogeneous (Hudgens-Haney et al. 2020). Biomarker fingerprints of Kraepelin’s “weakening of the wellsprings of volition” are apparently more diverse than is described by clinical definitions alone. It is an empirical question whether a purely top down or a B-SNIP-like middle-up approach to identifying specific types of patients is important for treatment targeting and mapping meaningful course and outcome. The B-SNIP team are vigorously evaluating this issue.
There is apparently a dimensional vulnerability for serious psychopathology that does not respect diagnostic boundaries. Some latent neurocognitive construct possesses strong gravitational attraction for capturing components in its orbit. Still, the ubiquity and influence of that dimension does not prove a lack of specific disease categories. For instance, general intelligence is measured with excellent psychometric properties. The normal population distribution of general intelligence is ideal for statistics, reveals strong polygenic inheritance, and predicts other features in dominant Western culture. Intellectual disability is defined by scoring beyond an arbitrary cutoff on this intelligence distribution. When considering persons below that cutoff as belonging to a syndrome, intellectual disability appears to be a complex and highly pleiomorphic polygenic phenotype (Carpenter et al. 1993; Mitchell 2012). Nevertheless, there are multiple distinct factors (many of them genetic, not necessarily familial) that cause an intellectual ability score to fall beyond the arbitrary cut line. The ability to detect many of these specific genetic etiologies is a function of improved technology (Gilissen et al. 2014). Discontinuity in an overall distribution was not required for either the identification or proof of these specific etiologies; they are hidden by the smoothed overall intelligence distribution. Improved technology is also known to change diagnoses from unknown to specific and treatable in other neurological disorders (O’Sullivan 2018). The polygenic and purely dimensional hypothesis for intellectual disability is refuted by the cases with identifiable specific etiologies. Mark Lenzenweger (2015, 2018), an intellectual descendent of Paul Meehl, made a similar and important argument regarding the schizotypy construct.
This sounds great for intellectual disability, seizure disorders, and other real medical illnesses, but can it possibly apply to idiopathic psychosis? Before their identification, cases with 22q11 deletion syndrome (Bassett and Chow 2008; Vorstman et al. 2015) or anti-NMDA receptor encephalitis (Dalmau et al. 2019) were buried within idiopathic psychosis. Some of us wonder about patients who we remember as anti-NMDA-like from years before the awareness generated by Susannah Cahalan’s (2012) Brain on Fire. There may be more autoimmune conditions that can account for additional confusing neurological manifestations (Dalmau et al. 2017). In B-SNIP psychosis cases, brain space volumes show a discontinuity at the deficit end of cognition, as shown in Fig. 6 above. It turns out those cases are largely Biotype-1 (80%). Whether this pattern hints at a specific etiology for a neurobiologically defined psychosis subtype remains to be verified. The final answer likely is more complicated than there is only a dimension of psychosis (Esterberg and Compton 2009; Guloksuz and van Os 2017, 2021) or an all-encompassing p-factor (Caspi and Moffitt 2018).
The B-SNIP outcomes, regardless of their eventual veridicality for psychosis diagnosis, required transdiagnostic assessment and probes of at least neurocognitive and neuro-physiological deviations. Disentangling the mechanisms for psychosis manifestations and the pathophysiologies underlying disruptions of neural systems is probably not a single variable, single domain, or single level of analysis problem.
- When considering B-SNIP outcomes in the context of an extensive psychosis literature, it seems the best conclusion is that categorical and dimensional diagnostic approaches have their place within idiopathic psychosis (Fulford and Handa 2018). This position reflects the method for determining treatment in the rest of medicine. Understanding the mechanism(s) for psychosis symptom development and the distinct etiologies creating them will require an integrated and open-minded approach. Of course, doing what is best for patients is always the primary concern. In 1983, Alex McBirney of the University of Oregon was asked to reflect on his main area of scientific investigation, igneous rocks, and its integration with the newish theory of plate tectonics. Maybe if the psychosis field embraces a spirit of cooperation, it can avoid Dr. McBirney’s acerbic supposition about his own discipline:The increasing awareness of ... deficiency ... in current literature makes the task of forecasting the direction of research for the coming decade an easy one. I predict that our present confusion ... will rise to undreamed-of levels of sophistication. (McBirney 1983, p. 689)
Acknowledgements
This paper is devoted to the memory of John Adrian Sweeney, Ph.D., our mentor, colleague, and friend. Dr. Sweeney was a founding member of B-SNIP, and made important contributions to this and many other B-SNIP papers. We miss him personally and professionally. Preparation of this paper was partially supported by the following grants: R01 MH124806, R01 MH124803, R01 MH095888, R01 MH119069, and P50 DA051361.
Contributor Information
Brett A. Clementz, Departments of Psychology and Neuroscience, BioImaging Research Center, University of Georgia, Athens, GA, USA
Michal Assaf, Department of Psychiatry, Olin Neuropsychiatric Research Center, Hartford, CT, USA.
John A. Sweeney, Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati, Cincinnati, OH, USA
Elliot S. Gershon, Departments of Psychiatry and Human Genetics, University of Chicago, Chicago, IL, USA
Sarah K. Keedy, Department of Psychiatry and Behavioral Neuroscience, University of Chicago, Chicago, IL, USA
S. Kristian Hill, Department of Psychology, Rosalind Franklin University of Medicine and Science, North Chicago, IL, USA.
Elena I. Ivleva, Department of Psychiatry, UT Southwestern Medical School, Dallas, TX, USA
Carol A. Tamminga, Department of Psychiatry, UT Southwestern Medical School, Dallas, TX, USA
Jennifer E. McDowell, Departments of Psychology and Neuroscience, Owen Institute for Behavioral Research, University of Georgia, Athens, GA, USA
Matcheri S. Keshavan, Department of Psychiatry, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA
Robert D. Gibbons, Departments of Medicine and Public Health Sciences, University of Chicago, Chicago, IL, USA
William T. Carpenter, Department of Psychiatry, Maryland Psychiatric Research Center, University of Maryland School of Medicine, Baltimore, MD, USA
Godfrey D. Pearlson, Departments of Psychiatry and Neuroscience, Olin Neuropsychiatric Research Center, Institute of Living, Hartford Hospital, and Yale University School of Medicine, Hartford, CT, USA
References
- Adler LE, Pachtman E, Franks RD, Pecevich M, Waldo MC, Freedman R. Neurophysiological evidence for a defect in neuronal mechanisms involved in sensory gating in schizophrenia. Biol Psychiatry. 1982;17(6):639–54. [PubMed] [Google Scholar]
- Alliey-Rodriguez N, Grey TA, Shafee R, Asif H, Lutz O, Bolo NR, Padmanabhan J, Tandon N, Klinger M, Reis K, Spring J, Coppes L, Zeng V, Hegde RR, Hoang DT, Bannai D, Nawaz U, Henson P, Liu S, Gage D, McCarroll S, Bishop JR, Hill S, Reilly JL, Lencer R, Clementz BA, Buckley P, Glahn DC, Meda SA, Narayanan B, Pearlson G, Keshavan MS, Ivleva EI, Tamminga C, Sweeney JA, Curtis D, Badner JA, Keedy S, Rapoport J, Liu C, Gershon ES. NRXN1 is associated with enlargement of the temporal horns of the lateral ventricles in psychosis. Transl Psychiatry. 2019;9(1):230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andreasen NC. The diagnosis of schizophrenia. Schizophr Bull. 1987;13(1):9–22. [DOI] [PubMed] [Google Scholar]
- Bassett AS, Chow EW. Schizophrenia and 22q11.2 deletion syndrome. Curr Psychiatry Rep 2008;10(2):148–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Begg CB, Zabor EC, Bernstein JL, Bernstein L, Press MF, Seshan VE. A conceptual and methodological framework for investigating etiologic heterogeneity. Stat Med. 2013;32(29):5039–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bègue I, Nicholson TR, Kozlowska K, LaFrance WC, Levenson JL, Rapaport MH, Carson AJ, Perez DL. Psychiatry’s modern role in functional neurological disorder: join the renaissance. Psychol Med. 2021;51(12):1961–3. [DOI] [PubMed] [Google Scholar]
- Belluck P, Carey B. Psychiatry’s new guide is out of touch with science, experts say. New York Times. 2013. [Google Scholar]
- Cahalan S Brain on fire: my month of madness. New York: Free Press; 2012. [Google Scholar]
- Carpenter WT. The psychoses in DSM-5 and in the near future. Am J Psychiatry. 2013;170(9):961–2. [DOI] [PubMed] [Google Scholar]
- Carpenter WT Jr, Buchanan RW, Kirkpatrick B, Tamminga C, Wood F. Strong inference, theory testing, and the neuroanatomy of schizophrenia. Arch Gen Psychiatry. 1993;50(10):825–31. [DOI] [PubMed] [Google Scholar]
- Caspi A, Moffitt TE. All for one and one for all: mental disorders in one dimension. Am J Psychiatry. 2018;175(9):831–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clementz BA. The ability to produce express saccades as a function of gap interval among schizophrenia patients. Exp Brain Res. 1996;111(1):121–30. [DOI] [PubMed] [Google Scholar]
- Clementz BA. Psychosis and fever revisited. Schizophr Res. 2022;242:17–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clementz BA. The Carpenter-Strauss quest to save schizophrenia: how DSM shifted the construct from its historical core. Biomark Neuropsychiatry. 2023;9:100061. [Google Scholar]
- Clementz BA, McDowell JE, Zisook S. Saccadic system functioning among schizophrenia patients and their first-degree biological relatives. J Abnorm Psychol. 1994;103(2):277–87. [PubMed] [Google Scholar]
- Clementz BA, Sweeney JA, Hamm JP, Ivleva EI, Ethridge LE, Pearlson GD, Keshavan MS, Tamminga CA. Identification of distinct psychosis biotypes using brain-based biomarkers. Am J Psychiatry. 2016;173(4):373–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clementz BA, Parker DA, Trotti RL, McDowell JE, Keedy SK, Keshavan MS, Pearlson GD, Gershon ES, Ivleva EI, Huang LY, Hill SK, Sweeney JA, Thomas O, Hudgens-Haney M, Gibbons RD, Tamminga CA. Psychosis biotypes: replication and validation from the B-SNIP Consortium. Schizophr Bull. 2022;48(1):56–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clementz BA, Chattopadhyay I, Trotti RL, Parker DA, Gershon ES, Hill SK, Ivleva EI, Keedy SK, Keshavan MS, McDowell JE, Pearlson GD, Tamminga CA, Gibbons RD. Clinical characterization and differentiation of B-SNIP psychosis biotypes: algorithmic diagnostics for efficient prescription of treatments (ADEPT)-1. Schizophr Res. 2023;260:143–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craddock N, Owen MJ. The Kraepelinian dichotomy – going, going... but still not gone. Br J Psychiatry. 2010;196(2):92–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cross-Disorder Group of the Psychiatric Genomics Consortium, Lee SH, Ripke S, Neale BM, Faraone SV, Purcell SM, Perlis RH, Mowry BJ, Thapar A, Goddard ME, Witte JS, Absher D, Agartz I, Akil H, Amin F, Andreassen OA, Anjorin A, Anney R, Anttila V, Arking DE, Asherson P, Azevedo MH, Backlund L, Badner JA, Bailey AJ, Banaschewski T, Barchas JD, Barnes MR, Barrett TB, Bass N, Battaglia A, Bauer M, Bayes M, Bellivier F, Bergen SE, Berrettini W, Betancur C, Bettecken T, Biederman J, Binder EB, Black DW, Blackwood DH, Bloss CS, Boehnke M, Boomsma DI, Breen G, Breuer R, Bruggeman R, Cormican P, Buccola NG, Buitelaar JK, Bunney WE, Buxbaum JD, Byerley WF, Byrne EM, Caesar S, Cahn W, Cantor RM, Casas M, Chakravarti A, Chambert K, Choudhury K, Cichon S, Cloninger CR, Collier DA, Cook EH, Coon H, Cormand B, Corvin A, Coryell WH, Craig DW, Craig IW, Crosbie J, Cuccaro ML, Curtis D, Czamara D, Datta S, Dawson G, Day R, De Geus EJ, Degenhardt F, Djurovic S, Donohoe GJ, Doyle AE, Duan J, Dudbridge F, Duketis E, Ebstein RP, Edenberg HJ, Elia J, Ennis S, Etain B, Fanous A, Farmer AE, Ferrier IN, Flickinger M, Fombonne E, Foroud T, Frank J, Franke B, Fraser C, Freedman R, Freimer NB, Freitag CM, Friedl M, Frisen L, Gallagher L, Gejman PV, Georgieva L, Gershon ES, Geschwind DH, Giegling I, Gill M, Gordon SD, Gordon-Smith K, Green EK, Greenwood TA, Grice DE, Gross M, Grozeva D, Guan W, Gurling H, De Haan L, Haines JL, Hakonarson H, Hallmayer J, Hamilton SP, Hamshere ML, Hansen TF, Hartmann AM, Hautzinger M, Heath AC, Henders AK, Herms S, Hickie IB, Hipolito M, Hoefels S, Holmans PA, Holsboer F, Hoogendijk WJ, Hottenga JJ, Hultman CM, Hus V, Ingason A, Ising M, Jamain S, Jones EG, Jones I, Jones L, Tzeng JY, Kahler AK, Kahn RS, Kandaswamy R, Keller MC, Kennedy JL, Kenny E, Kent L, Kim Y, Kirov GK, Klauck SM, Klei L, Knowles JA, Kohli MA, Koller DL, Konte B, Korszun A, Krabbendam L, Krasucki R, Kuntsi J, Kwan P, Landen M, Langstrom N, Lathrop M, Lawrence J, Lawson WB, Leboyer M, Ledbetter DH, Lee PH, Lencz T, Lesch KP, Levinson DF, Lewis CM, Li J, Lichtenstein P, Lieberman JA, Lin DY, Linszen DH, Liu C, Lohoff FW, Loo SK, Lord C, Lowe JK, Lucae S, MacIntyre DJ, Madden PA, Maestrini E, Magnusson PK, Mahon PB, Maier W, Malhotra AK, Mane SM, Martin CL, Martin NG, Mattheisen M, Matthews K, Mattingsdal M, McCarroll SA, McGhee KA, McGough JJ, McGrath PJ, McGuffin P, McInnis MG, McIntosh A, McKinney R, McLean AW, McMahon FJ, McMahon WM, McQuillin A, Medeiros H, Medland SE, Meier S, Melle I, Meng F, Meyer J, Middeldorp CM, Middleton L, Milanova V, Miranda A, Monaco AP, Montgomery GW, Moran JL, Moreno-De-Luca D, Morken G, Morris DW, Morrow EM, Moskvina V, Muglia P, Muhleisen TW, Muir WJ, Muller-Myhsok B, Murtha M, Myers RM, Myin-Germeys I, Neale MC, Nelson SF, Nievergelt CM, Nikolov I, Nimgaonkar V, Nolen WA, Nothen MM, Nurnberger JI, Nwulia EA, Nyholt DR, O’Dushlaine C, Oades RD, Olincy A, Oliveira G, Olsen L, Ophoff RA, Osby U, Owen MJ, Palotie A, Parr JR, Paterson AD, Pato CN, Pato MT, Penninx BW, Pergadia ML, Pericak-Vance MA, Pickard BS, Pimm J, Piven J, Posthuma D, Potash JB, Poustka F, Propping P, Puri V, Quested DJ, Quinn EM, Ramos-Quiroga JA, Rasmussen HB, Raychaudhuri S, Rehnstrom K, Reif A, Ribases M, Rice JP, Rietschel M, Roeder K, Roeyers H, Rossin L, Rothenberger A, Rouleau G, Ruderfer D, Rujescu D, Sanders AR, Sanders SJ, Santangelo SL, Sergeant JA, Schachar R, Schalling M, Schatzberg AF, Scheftner WA, Schellenberg GD, Scherer SW, Schork NJ, Schulze TG, Schumacher J, Schwarz M, Scolnick E, Scott LJ, Shi J, Shilling PD, Shyn SI, Silverman JM, Slager SL, Smalley SL, Smit JH, Smith EN, Sonuga-Barke EJ, Clair DS, State M, Steffens M, Steinhausen HC, Strauss JS, Strohmaier J, Stroup TS, Sutcliffe JS, Szatmari P, Szelinger S, Thirumalai S, Thompson RC, Todorov AA, Tozzi F, Treutlein J, Uhr M, van den Oord EJ, Van Grootheest G, Van Os J, Vicente AM, Vieland VJ, Vincent JB, Visscher PM, Walsh CA, Wassink TH, Watson SJ, Weissman MM, Werge T, Wienker TF, Wijsman EM, Willemsen G, Williams N, Willsey AJ, Witt SH, Xu W, Young AH, Yu TW, Zammit S, Zandi PP, Zhang P, Zitman FG, Zollner S, Devlin B, Kelsoe JR, Sklar P, Daly MJ, O’Donovan MC, Craddock N, Sullivan PF, Smoller JW, Kendler KS, Wray NR, International Inflammatory Bowel Disease Genetics Consortiuim. Genetic relationship between five psychiatric disorders estimated from genome-wide SNPs. Nat Genet. 2013;45(9):984–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuthbert BN, Insel TR. Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med. 2013;11:126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dalmau J, Geis C, Graus F. Autoantibodies to synaptic receptors and neuronal cell surface proteins in autoimmune diseases of the central nervous system. Physiol Rev. 2017;97(2):839–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dalmau J, Armangué T, Planagumà J, Radosevic M, Mannara F, Leypoldt F, Geis C, Lancaster E, Titulaer MJ, Rosenfeld MR, Graus F. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. Lancet Neurol. 2019;18(11):1045–57. [DOI] [PubMed] [Google Scholar]
- Dittrich L Patient H.M.: a story of memory, madness and family secrets. New York: Random House; 2016. [Google Scholar]
- Duong L, Klitten LL, Møller RS, Ingason A, Jakobsen KD, Skjødt C, Didriksen M, Hjalgrim H, Werge T, Tommerup N. Mutations in NRXN1 in a family multiply affected with brain disorders: NRXN1 mutations and brain disorders. Am J Med Genet B Neuropsychiatr Genet. 2012;159B(3):354–8. [DOI] [PubMed] [Google Scholar]
- Espay AJ, Aybek S, Carson A, Edwards MJ, Goldstein LH, Hallett M, LaFaver K, LaFrance WC, Lang AE, Nicholson T, Nielsen G, Reuber M, Voon V, Stone J, Morgante F. Current concepts in diagnosis and treatment of functional neurological disorders. JAMA Neurol. 2018;75(9):1132–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Esterberg ML, Compton MT. The psychosis continuum and categorical versus dimensional diagnostic approaches. Curr Psychiatry Rep. 2009;11(3):179–84. [DOI] [PubMed] [Google Scholar]
- Estes JW. Dropsy. In: Kiple KF, editor. The Cambridge world history of human disease. Cambridge: Cambridge University Press; 1993. p. 689–96. [Google Scholar]
- Ethridge LE, Brahmbhatt S, Gao Y, McDowell JE, Clementz BA. Consider the context: blocked versus interleaved presentation of antisaccade trials. Psychophysiology. 2009;46(5):1100–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ethridge LE, Hamm JP, Shapiro JR, Summerfelt AT, Keedy SK, Stevens MC, Pearlson G, Tamminga CA, Boutros NN, Sweeney JA, Keshavan MS, Thaker G, Clementz BA. Neural activations during auditory oddball processing discriminating schizophrenia and psychotic bipolar disorder. Biol Psychiatry. 2012;72(9):766–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ethridge LE, Soilleux M, Nakonezny PA, Reilly JL, Hill SK, Keefe RS, Gershon ES, Pearlson GD, Tamminga CA, Keshavan MS, Sweeney JA. Behavioral response inhibition in psychotic disorders: diagnostic specificity, familiality and relation to generalized cognitive deficit. Schizophr Res. 2014;159(2–3):491–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ethridge LE, Hamm JP, Pearlson GD, Tamminga CA, Sweeney JA, Keshavan MS, Clementz BA. Event-related potential and time-frequency endophenotypes for schizophrenia and psychotic bipolar disorder. Biol Psychiatry. 2015;77(2):127–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman R, Adler LE, Gerhardt GA, Waldo M, Baker N, Rose GM, Drebing C, Nagamoto H, Bickford-Wimer P, Franks R. Neurobiological studies of sensory gating in schizophrenia. Schizophr Bull. 1987;13(4):669–78. [DOI] [PubMed] [Google Scholar]
- Fulford KWM, Handa A. Categorical and/or continuous? Learning from vascular surgery. World Psychiatry. 2018;17(3):304–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons RD, Chattopadhyay I, Meltzer HY, Kane JM, Guinart D. Development of a computerized adaptive diagnostic screening tool for psychosis. Schizophr Res. 2022;245:116–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilissen C, Hehir-Kwa JY, Thung DT, van de Vorst M, van Bon BW, Willemsen MH, Kwint M, Janssen IM, Hoischen A, Schenck A, Leach R, Klein R, Tearle R, Bo T, Pfundt R, Yntema HG, de Vries BB, Kleefstra T, Brunner HG, Vissers LE, Veltman JA. Genome sequencing identifies major causes of severe intellectual disability. Nature. 2014;511(7509):344–7. [DOI] [PubMed] [Google Scholar]
- Goldberg D Psychopathology and classification in psychiatry. Soc Psychiatry Psychiatr Epidemiol. 2015;50(1):1–5. [DOI] [PubMed] [Google Scholar]
- Gotra MY, Hill SK, Gershon ES, Tamminga CA, Ivleva EI, Pearlson GD, Keshavan MS, Clementz BA, McDowell JE, Buckley PF, Sweeney JA, Keedy SK. Distinguishing patterns of impairment on inhibitory control and general cognitive ability among bipolar with and without psychosis, schizophrenia, and schizoaffective disorder. Schizophr Res. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psychiatry. 2003;160(4):636–45. [DOI] [PubMed] [Google Scholar]
- Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “right stuff”? Schizophr Bull. 2000;26(1):119–36. [DOI] [PubMed] [Google Scholar]
- Green MF, Kern RS, Heaton RK. Longitudinal studies of cognition and functional outcome in schizophrenia: implications for MATRICS. Schizophr Res. 2004;72(1):41–51. [DOI] [PubMed] [Google Scholar]
- Guimond S, Gu F, Shannon H, Kelly S, Mike L, Devenyi GA, Chakravarty MM, Sweeney JA, Pearlson G, Clementz BA, Tamminga C, Keshavan M. A diagnosis and biotype comparison across the psychosis spectrum: investigating volume and shape amygdala-hippocampal differences from the B-SNIP study. Schizophr Bull. 2021;47(6):1706–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guloksuz S, van Os J. The slow death of the concept of schizophrenia and the painful birth of the psychosis spectrum. Psychol Med. 2017:1–16. [DOI] [PubMed] [Google Scholar]
- Guloksuz S, van Os J. Waiting for the funeral of “schizophrenia” and the baby shower of the psychosis spectrum. Front Psych. 2021;12:618842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo JY, Ragland JD, Carter CS. Memory and cognition in schizophrenia. Mol Psychiatry. 2019;24(5):633–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo J, Rothman DL, Small SA. Why hippocampal glutamate levels are elevated in schizophrenia. JAMA Psychiatry. 2023;80(3):274–5. [DOI] [PubMed] [Google Scholar]
- Guze SB. Why psychiatry is a branch of medicine. New York: Oxford University Press; 1992. [Google Scholar]
- Hallett PE, Adams BD. The predictability of saccadic latency in a novel voluntary oculomotor task. Vis Res. 1980;20(4):329–39. [DOI] [PubMed] [Google Scholar]
- Hamm JP, Ethridge LE, Shapiro JR, Stevens MC, Boutros NN, Summerfelt AT, Keshavan MS, Sweeney JA, Pearlson G, Tamminga CA, Thaker G, Clementz BA. Spatiotemporal and frequency domain analysis of auditory paired stimuli processing in schizophrenia and bipolar disorder with psychosis. Psychophysiology. 2012;49(4):522–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamm JP, Ethridge LE, Boutros NN, Keshavan MS, Sweeney JA, Pearlson GD, Tamminga CA, Clementz BA. Diagnostic specificity and familiality of early versus late evoked potentials to auditory paired stimuli across the schizophrenia-bipolar psychosis spectrum. Psychophysiology. 2014;51(4):348–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrington A Mind fixers : psychiatry’s troubled search for the biology of mental illness. New York: W.W. Norton & Company; 2019. [Google Scholar]
- Haslam N, McGrath MJ, Viechtbauer W, Kuppens P. Dimensions over categories: a meta-analysis of taxometric research. Psychol Med. 2020;50(9):1418–32. [DOI] [PubMed] [Google Scholar]
- Heckers S, Barch DM, Bustillo J, Gaebel W, Gur R, Malaspina D, Owen MJ, Schultz S, Tandon R, Tsuang M, Van Os J, Carpenter W. Structure of the psychotic disorders classification in DSM-5. Schizophr Res. 2013;150(1):11–4. [DOI] [PubMed] [Google Scholar]
- Hengartner MP, Lehmann SN. Why psychiatric research must abandon traditional diagnostic classification and adopt a fully dimensional scope: two solutions to a persistent problem. Front Psych. 2017;8:101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill SK, Reilly JL, Keefe RS, Gold JM, Bishop JR, Gershon ES, Tamminga CA, Pearlson GD, Keshavan MS, Sweeney JA. Neuropsychological impairments in schizophrenia and psychotic bipolar disorder: findings from the bipolar-schizophrenia network on intermediate phenotypes (B-SNIP) study. Am J Psychiatry. 2013;170(11):1275–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hochberger WC, Hill SK, Nelson CL, Reilly JL, Keefe RS, Pearlson GD, Keshavan MS, Tamminga CA, Clementz BA, Sweeney JA. Unitary construct of generalized cognitive ability underlying BACS performance across psychotic disorders and in their first-degree relatives. Schizophr Res. 2016;170(1):156–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hochberger WC, Combs T, Reilly JL, Bishop JR, Keefe RSE, Clementz BA, Keshavan MS, Pearlson GD, Tamminga CA, Hill SK, Sweeney JA. Deviation from expected cognitive ability across psychotic disorders. Schizophr Res. 2018;192:300–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horwitz AV. DSM : a history of psychiatry’s bible. Baltimore: Johns Hopkins University Press; 2021. [Google Scholar]
- Huang LY, Jackson BS, Rodrigue AL, Tamminga CA, Gershon ES, Pearlson GD, Keshavan MS, Keedy SS, Hill SK, Sweeney JA, Clementz BA, McDowell JE. Antisaccade error rates and gap effects in psychosis syndromes from bipolar-schizophrenia network for intermediate phenotypes 2 (B-SNIP2). Psychol Med. 2022;52(13):2692–701. [DOI] [PubMed] [Google Scholar]
- Hudgens-Haney ME, Ethridge LE, Knight JB, McDowell JE, Keedy SK, Pearlson GD, Tamminga CA, Keshavan MS, Sweeney JA, Clementz BA. Intrinsic neural activity differences among psychotic illnesses. Psychophysiology. 2017;54(8):1223–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hudgens-Haney ME, Ethridge LE, McDowell JE, Keedy SK, Pearlson GD, Tamminga CA, Keshavan MS, Sweeney JA, Clementz BA. Psychosis subgroups differ in intrinsic neural activity but not task-specific processing. Schizophr Res. 2018;195:222–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hudgens-Haney ME, Clementz BA, Ivleva EI, Keshavan MS, Pearlson GD, Gershon ES, Keedy SK, Sweeney JA, Gaudoux F, Bunouf P, Canolle B, Tonner F, Gatti-McArthur S, Tamminga CA. Cognitive impairment and diminished neural responses constitute a biomarker signature of negative symptoms in psychosis. Schizophr Bull. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyman SE. The diagnosis of mental disorders: the problem of reification. Annu Rev Clin Psychol. 2010;6:155–79. [DOI] [PubMed] [Google Scholar]
- Insel TR. Rethinking schizophrenia. Nature. 2010;468(7321):187–93. [DOI] [PubMed] [Google Scholar]
- Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, Sanislow C, Wang P. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry. 2010;167(7):748–51. [DOI] [PubMed] [Google Scholar]
- Ivleva EI, Clementz BA, Dutcher AM, Arnold SJM, Jeon-Slaughter H, Aslan S, Witte B, Poudyal G, Lu H, Meda SA, Pearlson GD, Sweeney JA, Keshavan MS, Tamminga CA. Brain structure biomarkers in the psychosis biotypes: findings from the bipolar-schizophrenia network for intermediate phenotypes. Biol Psychiatry. 2017;82(1):26–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ivleva EI, Turkozer HB, Sweeney JA. Imaging-based subtyping for psychiatric syndromes. Neuroimaging Clin N Am. 2020;30(1):35–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jirsaraie RJ, Sheffield JM, Barch DM. Neural correlates of global and specific cognitive deficits in schizophrenia. Schizophr Res. 2018;201:237–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keefe RS, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The brief assessment of cognition in schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. 2004;68(2–3):283–97. [DOI] [PubMed] [Google Scholar]
- Keefe RS, Poe M, Walker TM, Harvey PD. The relationship of the Brief Assessment of Cognition in Schizophrenia (BACS) to functional capacity and real-world functional outcome. J Clin Exp Neuropsychol. 2006;28(2):260–9. [DOI] [PubMed] [Google Scholar]
- Keefe RS, Harvey PD, Goldberg TE, Gold JM, Walker TM, Kennel C, Hawkins K. Norms and standardization of the brief assessment of cognition in schizophrenia (BACS). Schizophr Res. 2008;102(1–3):108–15. [DOI] [PubMed] [Google Scholar]
- Kelly S, Guimond S, Pasternak O, Lutz O, Lizano P, Cetin-Karayumak S, Sweeney JA, Pearlson G, Clementz BA, McDowell JE, Tamminga CA, Shenton ME, Keshavan MS. White matter microstructure across brain-based biotypes for psychosis – findings from the bipolar-schizophrenia network for intermediate phenotypes. Psychiatry Res Neuroimaging. 2021;308:111234. [DOI] [PubMed] [Google Scholar]
- Kendell R, Jablensky A. Distinguishing between the validity and utility of psychiatric diagnoses. Am J Psychiatry. 2003;160(1):4–12. [DOI] [PubMed] [Google Scholar]
- Keshavan MS, Clementz BA. Precision medicine for psychosis: a revolution at the interface of psychiatry and neurology. Nat Rev Neurol. 2023;19:193–4. [DOI] [PubMed] [Google Scholar]
- Keshavan MS, Clementz BA, Pearlson GD, Sweeney JA, Tamminga CA. Reimagining psychoses: an agnostic approach to diagnosis. Schizophr Res. 2013;146(1–3):10–6. [DOI] [PubMed] [Google Scholar]
- Keshavan MS, Bishop DL, Coconcea C, Bishop JR. Clozapine, an update. Schizophr Res. 2022;248:168–70. [DOI] [PubMed] [Google Scholar]
- Kotov R, Jonas KG, Carpenter WT, Dretsch MN, Eaton NR, Forbes MK, Forbush KT, Hobbs K, Reininghaus U, Slade T, South SC, Sunderland M, Waszczuk MA, Widiger TA, Wright AGC, Zald DH, Krueger RF, Watson D, Workgroup HU. Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): I. Psychosis superspectrum. World Psychiatry. 2020;19(2):151–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger RF, Kotov R, Watson D, Forbes MK, Eaton NR, Ruggero CJ, Simms LJ, Widiger TA, Achenbach TM, Bach B, Bagby RM, Bornovalova MA, Carpenter WT, Chmielewski M, Cicero DC, Clark LA, Conway C, DeClercq B, DeYoung CG, Docherty AR, Drislane LE, First MB, Forbush KT, Hallquist M, Haltigan JD, Hopwood CJ, Ivanova MY, Jonas KG, Latzman RD, Markon KE, Miller JD, Morey LC, Mullins-Sweatt SN, Ormel J, Patalay P, Patrick CJ, Pincus AL, Regier DA, Reininghaus U, Rescorla LA, Samuel DB, Sellbom M, Shackman AJ, Skodol A, Slade T, South SC, Sunderland M, Tackett JL, Venables NC, Waldman ID, Waszczuk MA, Waugh MH, Wright AGC, Zald DH, Zimmermann J. Progress in achieving quantitative classification of psychopathology. World Psychiatry. 2018;17(3):282–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lakatos I The methodology of scientific research programmes. Cambridge/New York: Cambridge University Press; 1978. [Google Scholar]
- Lenzenweger MF. Thinking clearly about schizotypy: hewing to the schizophrenia liability core, considering interesting tangents, and avoiding conceptual quicksand. Schizophr Bull. 2015;41(Suppl 2):S483–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lenzenweger MF. Schizotypy, schizotypic psychopathology, and schizophrenia: hearing echoes, leveraging prior advances, and probing new angles. Schizophr Bull. 2018;44(suppl_2):S564–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung JG, de Leon J, Frye MA, Singh B, Coates R, McElroy SL. The modernization of clozapine: a recapitulation of the past in the United States and the view forward. J Clin Psychopharmacol. 2022;42(6):565–80. [DOI] [PubMed] [Google Scholar]
- Linden DE. The p300: where in the brain is it produced and what does it tell us? Neuroscientist. 2005;11(6):563–76. [DOI] [PubMed] [Google Scholar]
- Lipszyc J, Schachar R. Inhibitory control and psychopathology: a meta-analysis of studies using the stop signal task. J Int Neuropsychol Soc. 2010;16(6):1064–76. [DOI] [PubMed] [Google Scholar]
- Lui S, Li T, Deng W, Jiang L, Wu Q, Tang H, Yue Q, Huang X, Chan RC, Collier DA, Meda SA, Pearlson G, Mechelli A, Sweeney JA, Gong Q. Short-term effects of antipsychotic treatment on cerebral function in drug-naive first-episode schizophrenia revealed by “resting state” functional magnetic resonance imaging. Arch Gen Psychiatry. 2010;67(8):783–92. [DOI] [PubMed] [Google Scholar]
- Lui S, Yao L, Xiao Y, Keedy SK, Reilly JL, Keefe RS, Tamminga CA, Keshavan MS, Pearlson GD, Gong Q, Sweeney JA. Resting-state brain function in schizophrenia and psychotic bipolar probands and their first-degree relatives. Psychol Med. 2015;45(1):97–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lundin NB, Bartolomeo LA, O’Donnell BF, Hetrick WP. Reduced electroencephalogram responses to standard and target auditory stimuli in bipolar disorder and the impact of psychotic features: analysis of event-related potentials, spectral power, and inter-trial coherence. Bipolar Disord. 2018;20(1):49–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McBirney AR. Geology—past and future. Geology. 1983;11(12):679–91. [Google Scholar]
- McCutcheon RA, Keefe RSE, McGuire PK. Cognitive impairment in schizophrenia: aetiology, pathophysiology, and treatment. Mol Psychiatry. 2023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDowell JE, Clementz BA. Behavioral and brain imaging studies of saccadic performance in schizophrenia. Biol Psychol. 2001;57(1–3):5–22. [DOI] [PubMed] [Google Scholar]
- McPhee J Coming into the country. New York: Farrar, Straus and Giroux; 1977. [Google Scholar]
- McTeague LM, Goodkind MS, Etkin A. Transdiagnostic impairment of cognitive control in mental illness. J Psychiatr Res. 2016;83:37–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McTeague LM, Huemer J, Carreon DM, Jiang Y, Eickhoff SB, Etkin A. Identification of common neural circuit disruptions in cognitive control across psychiatric disorders. Am J Psychiatry. 2017;174(7):676–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Medalia A, Saperstein AM, Qian M, Javitt DC. Impact of baseline early auditory processing on response to cognitive remediation for schizophrenia. Schizophr Res. 2019;208:397–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell KJ. What is complex about complex disorders? Genome Biol. 2012;13(1):237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National-Research-Council. Toward precision medicine: building a knowledge network for biomedical research and a new taxonomy of disease. Washington, DC: The National Academies Press; 2011. [PubMed] [Google Scholar]
- O’Donoghue MF, Duncan JS, Sander JW. The National Hospital Seizure Severity Scale: a further development of the Chalfont Seizure Severity Scale. Epilepsia. 1996;37(6):563–71. [DOI] [PubMed] [Google Scholar]
- O’Sullivan S Is it all in your head?: True stories of imaginary illness. New York: Other Press; 2015. [Google Scholar]
- O’Sullivan S Brainstorm: detective stories from the world of neurology. New York: Other Press; 2018. [Google Scholar]
- O’Sullivan S The sleeping beauties : and other stories of mystery illness. New York: Pantheon Books; 2021. 1 online resource [Google Scholar]
- Parker DA, Trotti RL, McDowell JE, Keedy SK, Hill SK, Gershon ES, Ivleva EI, Pearlson GD, Keshavan MS, Tamminga CA, Clementz BA. Auditory oddball responses across the schizophrenia-bipolar spectrum and their relationship to cognitive and clinical features. Am J Psychiatry. 2021;178(10):952–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penfield W No man alone: a neurosurgeon’s life. Boston: Little, Brown; 1977. [Google Scholar]
- Perez DL, Nicholson TR, Asadi-Pooya AA, Bègue I, Butler M, Carson AJ, David AS, Deeley Q, Diez I, Edwards MJ, Espay AJ, Gelauff JM, Hallett M, Horovitz SG, Jungilligens J, Kanaan RAA, Tijssen MAJ, Kozlowska K, LaFaver K, LaFrance WC, Lidstone SC, Marapin RS, Maurer CW, Modirrousta M, Reinders AATS, Sojka P, Staab JP, Stone J, Szaflarski JP, Aybek S. Neuroimaging in functional neurological disorder: state of the field and research agenda. Neuroimage Clin. 2021;30:102623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Platt JR. Strong inference: certain systematic methods of scientific thinking may produce much more rapid progress than others. Science. 1964;146(3642):347–53. [DOI] [PubMed] [Google Scholar]
- Polich J Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol. 2007;118(10):2128–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raymond N, Lizano P, Kelly S, Hegde R, Keedy S, Pearlson GD, Gershon ES, Clementz BA, Tamminga CA, Keshavan M. What can clozapine’s effect on neural oscillations tell us about its therapeutic effects? A scoping review and synthesis. Biomark Neuropsychiatry. 2022;6:100048. [Google Scholar]
- Reilly JL, Harris MS, Keshavan MS, Sweeney JA. Abnormalities in visually guided saccades suggest corticofugal dysregulation in never-treated schizophrenia. Biol Psychiatry. 2005;57(2):145–54. [DOI] [PubMed] [Google Scholar]
- Reilly JL, Frankovich K, Hill S, Gershon ES, Keefe RS, Keshavan MS, Pearlson GD, Tamminga CA, Sweeney JA. Elevated antisaccade error rate as an intermediate phenotype for psychosis across diagnostic categories. Schizophr Bull. 2014;40(5):1011–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reininghaus U, Bohnke JR, Chavez-Baldini U, Gibbons R, Ivleva E, Clementz BA, Pearlson GD, Keshavan MS, Sweeney JA, Tamminga CA. Transdiagnostic dimensions of psychosis in the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP). World Psychiatry. 2019;18(1):67–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins E, Guze SB. Establishment of diagnostic validity in psychiatric illness: its application to schizophrenia. Am J Psychiatry. 1970;126(7):983–7. [DOI] [PubMed] [Google Scholar]
- Schaaf CP, Boone PM, Sampath S, Williams C, Bader PI, Mueller JM, Shchelochkov OA, Brown CW, Crawford HP, Phalen JA, Tartaglia NR, Evans P, Campbell WM, Tsai AC, Parsley L, Grayson SW, Scheuerle A, Luzzi CD, Thomas SK, Eng PA, Kang SH, Patel A, Stankiewicz P, Cheung SW. Phenotypic spectrum and genotype-phenotype correlations of NRXN1 exon deletions. Eur J Hum Genet. 2012;20(12):1240–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sigmond GG. On the use of digitalis in dropsy. Boston Med Surg J. 1837;17(14):213–20. [Google Scholar]
- Singh T, Poterba T, Curtis D, Akil H, Al Eissa M, Barchas JD, Bass N, Bigdeli TB, Breen G, Bromet EJ, Buckley PF, Bunney WE, Bybjerg-Grauholm J, Byerley WF, Chapman SB, Chen WJ, Churchhouse C, Craddock N, Cusick CM, DeLisi L, Dodge S, Escamilla MA, Eskelinen S, Fanous AH, Faraone SV, Fiorentino A, Francioli L, Gabriel SB, Gage D, Gagliano Taliun SA, Ganna A, Genovese G, Glahn DC, Grove J, Hall MH, Hämäläinen E, Heyne HO, Holi M, Hougaard DM, Howrigan DP, Huang H, Hwu HG, Kahn RS, Kang HM, Karczewski KJ, Kirov G, Knowles JA, Lee FS, Lehrer DS, Lescai F, Malaspina D, Marder SR, McCarroll SA, McIntosh AM, Medeiros H, Milani L, Morley CP, Morris DW, Mortensen PB, Myers RM, Nordentoft M, O’Brien NL, Olivares AM, Ongur D, Ouwehand WH, Palmer DS, Paunio T, Quested D, Rapaport MH, Rees E, Rollins B, Satterstrom FK, Schatzberg A, Scolnick E, Scott LJ, Sharp SI, Sklar P, Smoller JW, Sobell JL, Solomonson M, Stahl EA, Stevens CR, Suvisaari J, Tiao G, Watson SJ, Watts NA, Blackwood DH, Børglum AD, Cohen BM, Corvin AP, Esko T, Freimer NB, Glatt SJ, Hultman CM, McQuillin A, Palotie A, Pato CN, Pato MT, Pulver AE, St Clair D, Tsuang MT, Vawter MP, Walters JT, Werge TM, Ophoff RA, Sullivan PF, Owen MJ, Boehnke M, O’Donovan MC, Neale BM, Daly MJ. Rare coding variants in ten genes confer substantial risk for schizophrenia. Nature. 2022;604(7906):509–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spencer KM. Time to be spontaneous: a renaissance of intrinsic brain activity in psychosis research? Biol Psychiatry. 2014;76(6):434–5. [DOI] [PubMed] [Google Scholar]
- Stan AD, Tamminga CA, Han K, Kim JB, Padmanabhan J, Tandon N, Hudgens-Haney ME, Keshavan MS, Clementz BA, Pearlson GD, Sweeney JA, Gibbons RD. Associating psychotic symptoms with altered brain anatomy in psychotic disorders using multidimensional item response theory models. Cereb Cortex. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan PF, Agrawal A, Bulik CM, Andreassen OA, Børglum AD, Breen G, Cichon S, Edenberg HJ, Faraone SV, Gelernter J, Mathews CA, Nievergelt CM, Smoller JW, O’Donovan MC, P. G. Consortium. Psychiatric genomics: an update and an agenda. Am J Psychiatry. 2018;175(1):15–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamminga CA, Stan AD, Wagner AD. The hippocampal formation in schizophrenia. Am J Psychiatry. 2010;167(10):1178–93. [DOI] [PubMed] [Google Scholar]
- Tamminga CA, Pearlson G, Keshavan M, Sweeney J, Clementz B, Thaker G. Bipolar and schizophrenia network for intermediate phenotypes: outcomes across the psychosis continuum. Schizophr Bull. 2014;40(Suppl 2):S131–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamminga CA, Pearlson GD, Stan AD, Gibbons RD, Padmanabhan J, Keshavan M, Clementz BA. Strategies for advancing disease definition using biomarkers and genetics: the bipolar and schizophrenia network for intermediate phenotypes. Biol Psychiatry Cogn Neurosci Neuroimaging. 2017;2(1):20–7. [DOI] [PubMed] [Google Scholar]
- Tamminga CA, Clementz BA, Pearlson G, Keshavan M, Gershon ES, Ivleva EI, McDowell J, Meda SA, Keedy S, Calhoun VD, Lizano P, Bishop JR, Hudgens-Haney M, Alliey-Rodriguez N, Asif H, Gibbons R. Biotyping in psychosis: using multiple computational approaches with one data set. Neuropsychopharmacology. 2020;46:143–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamminga CA, Pearlson G, Gershon E, Keedy S, Hudgens-Haney ME, Ivleva EI, Parker DA, McDowell JE, Clementz BA. Using psychosis biotypes and the Framingham model for parsing psychosis biology. Schizophr Res. 2021;242:132–4. [DOI] [PubMed] [Google Scholar]
- Thaker GK. Neurophysiological endophenotypes across bipolar and schizophrenia psychosis. Schizophr Bull. 2008;34(4):760–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trubetskoy V, Pardiñas AF, Qi T, Panagiotaropoulou G, Awasthi S, Bigdeli TB, Bryois J, Chen CY, Dennison CA, Hall LS, Lam M, Watanabe K, Frei O, Ge T, Harwood JC, Koopmans F, Magnusson S, Richards AL, Sidorenko J, Wu Y, Zeng J, Grove J, Kim M, Li Z, Voloudakis G, Zhang W, Adams M, Agartz I, Atkinson EG, Agerbo E, Al Eissa M, Albus M, Alexander M, Alizadeh BZ, Alptekin K, Als TD, Amin F, Arolt V, Arrojo M, Athanasiu L, Azevedo MH, Bacanu SA, Bass NJ, Begemann M, Belliveau RA, Bene J, Benyamin B, Bergen SE, Blasi G, Bobes J, Bonassi S, Braun A, Bressan RA, Bromet EJ, Bruggeman R, Buckley PF, Buckner RL, Bybjerg-Grauholm J, Cahn W, Cairns MJ, Calkins ME, Carr VJ, Castle D, Catts SV, Chambert KD, Chan RCK, Chaumette B, Cheng W, Cheung EFC, Chong SA, Cohen D, Consoli A, Cordeiro Q, Costas J, Curtis C, Davidson M, Davis KL, de Haan L, Degenhardt F, DeLisi LE, Demontis D, Dickerson F, Dikeos D, Dinan T, Djurovic S, Duan J, Ducci G, Dudbridge F, Eriksson JG, Fañanás L, Faraone SV, Fiorentino A, Forstner A, Frank J, Freimer NB, Fromer M, Frustaci A, Gadelha A, Genovese G, Gershon ES, Giannitelli M, Giegling I, Giusti-Rodríguez P, Godard S, Goldstein JI, González Peñas J, González-Pinto A, Gopal S, Gratten J, Green MF, Greenwood TA, Guillin O, Gülöksüz S, Gur RE, Gur RC, Gutiérrez B, Hahn E, Hakonarson H, Haroutunian V, Hartmann AM, Harvey C, Hayward C, Henskens FA, Herms S, Hoffmann P, Howrigan DP, Ikeda M, Iyegbe C, Joa I, Julià A, Kähler AK, Kam-Thong T, Kamatani Y, Karachanak-Yankova S, Kebir O, Keller MC, Kelly BJ, Khrunin A, Kim SW, Klovins J, Kondratiev N, Konte B, Kraft J, Kubo M, Kučinskas V, Kučinskiene ZA, Kusumawardhani A, Kuzelova-Ptackova H, Landi S, Lazzeroni LC, Lee PH, Legge SE, Lehrer DS, Lencer R, Lerer B, Li M, Lieberman J, Light GA, Limborska S, Liu CM, Lönnqvist J, Loughland CM, Lubinski J, Luykx JJ, Lynham A, Macek M, Mackinnon A, Magnusson PKE, Maher BS, Maier W, Malaspina D, Mallet J, Marder SR, Marsal S, Martin AR, Martorell L, Mattheisen M, McCarley RW, McDonald C, McGrath JJ, Medeiros H, Meier S, Melegh B, Melle I, Mesholam-Gately RI, Metspalu A, Michie PT, Milani L, Milanova V, Mitjans M, Molden E, Molina E, Molto MD, Mondelli V, Moreno C, Morley CP, Muntané G, Murphy KC, Myin-Germeys I, Nenadić I, Nestadt G, Nikitina-Zake L, Noto C, Nuechterlein KH, O’Brien NL, O’Neill FA, Oh SY, Olincy A, Ota VK, Pantelis C, Papadimitriou GN, Parellada M, Paunio T, Pellegrino R, Periyasamy S, Perkins DO, Pfuhlmann B, Pietiläinen O, Pimm J, Porteous D, Powell J, Quattrone D, Quested D, Radant AD, Rampino A, Rapaport MH, Rautanen A, Reichenberg A, Roe C, Roffman JL, Roth J, Rothermundt M, Rutten BPF, Saker-Delye S, Salomaa V, Sanjuan J, Santoro ML, Savitz A, Schall U, Scott RJ, Seidman LJ, Sharp SI, Shi J, Siever LJ, Sigurdsson E, Sim K, Skarabis N, Slominsky P, So HC, Sobell JL, Söderman E, Stain HJ, Steen NE, Steixner-Kumar AA, Stögmann E, Stone WS, Straub RE, Streit F, Strengman E, Stroup TS, Subramaniam M, Sugar CA, Suvisaari J, Svrakic DM, Swerdlow NR, Szatkiewicz JP, Ta TMT, Takahashi A, Terao C, Thibaut F, Toncheva D, Tooney PA, Torretta S, Tosato S, Tura GB, Turetsky BI, Üçok A, Vaaler A, van Amelsvoort T, van Winkel R, Veijola J, Waddington J, Walter H, Waterreus A, Webb BT, Weiser M, Williams NM, Witt SH, Wormley BK, Wu JQ, Xu Z, Yolken R, Zai CC, Zhou W, Zhu F, Zimprich F, Atbaşoğlu EC, Ayub M, Benner C, Bertolino A, Black DW, Bray NJ, Breen G, Buccola NG, Byerley WF, Chen WJ, Cloninger CR, Crespo-Facorro B, Donohoe G, Freedman R, Galletly C, Gandal MJ, Gennarelli M, Hougaard DM, Hwu HG, Jablensky AV, McCarroll SA, Moran JL, Mors O, Mortensen PB, Müller-Myhsok B, Neil AL, Nordentoft M, Pato MT, Petryshen TL, Pirinen M, Pulver AE, Schulze TG, Silverman JM, Smoller JW, Stahl EA, Tsuang DW, Vilella E, Wang SH, Xu S, Adolfsson R, Arango C, Baune BT, Belangero SI, Børglum AD, Braff D, Bramon E, Buxbaum JD, Campion D, Cervilla JA, Cichon S, Collier DA, Corvin A, Curtis D, Forti MD, Domenici E, Ehrenreich H, Escott-Price V, Esko T, Fanous AH, Gareeva A, Gawlik M, Gejman PV, Gill M, Glatt SJ, Golimbet V, Hong KS, Hultman CM, Hyman SE, Iwata N, Jönsson EG, Kahn RS, Kennedy JL, Khusnutdinova E, Kirov G, Knowles JA, Krebs MO, Laurent-Levinson C, Lee J, Lencz T, Levinson DF, Li QS, Liu J, Malhotra AK, Malhotra D, McIntosh A, McQuillin A, Menezes PR, Morgan VA, Morris DW, Mowry BJ, Murray RM, Nimgaonkar V, Nöthen MM, Ophoff RA, Paciga SA, Palotie A, Pato CN, Qin S, Rietschel M, Riley BP, Rivera M, Rujescu D, Saka MC, Sanders AR, Schwab SG, Serretti A, Sham PC, Shi Y, Clair DS, Stefánsson H, Stefansson K, Tsuang MT, van Os J, Vawter MP, Weinberger DR, Werge T, Wildenauer DB, Yu X, Yue W, Holmans PA, Pocklington AJ, Roussos P, Vassos E, Verhage M, Visscher PM, Yang J, Posthuma D, Andreassen OA, Kendler KS, Owen MJ, Wray NR, Daly MJ, Huang H, Neale BM, Sullivan PF, Ripke S, Walters JTR, O’Donovan MC, Consortium IS, PsychENCODE PE, Consortium I, Consortium S, S. W. G. o. t. P. G. Consortium. Mapping genomic loci implicates genes and synaptic biology in schizophrenia. Nature. 2022;604(7906):502–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vorstman JA, Breetvelt EJ, Duijff SN, Eliez S, Schneider M, Jalbrzikowski M, Armando M, Vicari S, Shashi V, Hooper SR, Chow EW, Fung WL, Butcher NJ, Young DA, McDonald-McGinn DM, Vogels A, van Amelsvoort T, Gothelf D, Weinberger R, Weizman A, Klaassen PW, Koops S, Kates WR, Antshel KM, Simon TJ, Ousley OY, Swillen A, Gur RE, Bearden CE, Kahn RS, Bassett AS, I. C. o. B. a. B. i. q. D. Syndrome. Cognitive decline preceding the onset of psychosis in patients with 22q11.2 deletion syndrome. JAMA Psychiatry. 2015;72(4):377–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wakefield JC. Klerman’s “credo” reconsidered: neo-Kraepelinianism, Spitzer’s views, and what we can learn from the past. World Psychiatry. 2022;21(1):4–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weber S, Heim S, Richiardi J, Van De Ville D, Serranová T, Jech R, Marapin RS, Tijssen MAJ, Aybek S. Multi-Centre classification of functional neurological disorders based on resting-state functional connectivity. Neuroimage Clin. 2022;35:103090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinberger DR. On the plausibility of “the neurodevelopmental hypothesis” of schizophrenia. Neuropsychopharmacology. 1996;14(3 Suppl):1S–11S. [DOI] [PubMed] [Google Scholar]
- Wexler BE. Beyond the Kraepelinean dichotomy. Biol Psychiatry. 1992;31(6):539–41. [DOI] [PubMed] [Google Scholar]
- Wilson EO. Consilience : the unity of knowledge. New York: Knopf: Distributed by Random House; 1998. [Google Scholar]
- Wyatt RJ, Alexander RC, Egan MF, Kirch DG. Schizophrenia, just the facts. What do we know, how well do we know it? Schizophr Res. 1988;1(1):3–18. [DOI] [PubMed] [Google Scholar]
- Xiao Y, Liao W, Long Z, Tao B, Zhao Q, Luo C, Tamminga CA, Keshavan MS, Pearlson GD, Clementz BA, Gershon ES, Ivleva EI, Keedy SK, Biswal BB, Mechelli A, Lencer R, Sweeney JA, Lui S, Gong Q. Subtyping schizophrenia patients based on patterns of structural brain alterations. Schizophr Bull. 2022;48(1):241–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang W, Li S, Wang X, Gong Y, Yao L, Xiao Y, Liu J, Keedy SK, Gong Q, Sweeney JA, Lui S. Abnormal dynamic functional connectivity between speech and auditory areas in schizophrenia patients with auditory hallucinations. Neuroimage Clin. 2018;19:918–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang W, Lei D, Keedy SK, Ivleva EI, Eum S, Yao L, Tamminga CA, Clementz BA, Keshavan MS, Pearlson GD, Gershon ES, Bishop JR, Gong Q, Lui S, Sweeney JA. Brain gray matter network organization in psychotic disorders. Neuropsychopharmacology. 2020;45(4):666–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang W, Sweeney JA, Bishop JR, Gong Q, Lui S. Biological subtyping of psychiatric syndromes as a pathway for advances in drug discovery and personalized medicine. Nature Mental Health. 2023;1(2):88–99. [Google Scholar]
- Zhu Y, Womer FY, Leng H, Chang M, Yin Z, Wei Y, Zhou Q, Fu S, Deng X, Lv J, Song Y, Ma Y, Sun X, Bao J, Wei S, Jiang X, Tan S, Tang Y, Wang F. The relationship between cognitive dysfunction and symptom dimensions across schizophrenia, bipolar disorder, and major depressive disorder. Front Psych. 2019;10:253. [DOI] [PMC free article] [PubMed] [Google Scholar]