

Abstract
Study Design: A retrospective cohort study. Background and objective: There are no data on changes in cervical sagittal alignment and curvature after second and third surgeries in patients with multilevel cervical degenerative diseases (CDD). This study aimed to explore these changes following multiple decompression and reconstruction surgeries. Methods: 145 patients with multilevel CDD were enrolled based on medical records extracted from 2015 to 2023. They were divided into three groups according to the number of surgeries. 63 patients underwent first decompression and reconstruction surgery (Group 1), 53 patients underwent second surgery (Group 2) and 29 patients underwent third surgery (Group 3). Clinical parameters (Japanese Orthopedic Association (JOA) score for neural functional recovery, visual analogue scale (VAS) and neck disability index (NDI) for neck pain) and radiologic parameters (T1 slope (T1S), cervical lordosis (C2-7CL), C2-7 sagittal vertical axis (C2-7SVA)) were reviewed and analyzed. Results: The mean period between final surgery and last follow-up was more than 12 months. There were significant differences among 3 groups in terms of operation time, blood loss and hospital stay (P < 0.001). Functional scores changed significantly after decompression surgeries (P < 0.001) in 3 groups. Radiographic parameters increased after surgery in group 1 (P < 0.001), while C2-7CL and T1S decreased after second and third surgery in group 2 and group 3 (P < 0.001). Comparing with group 1, there were significant differences showed in terms of C2-7CL, T1S, NDI and VAS in group 2 and group 3 (P < 0.05), NDI and VAS were significantly larger in group3 compare with group 2 (P < 0.05). Conclusion: Multiple surgeries may exacerbate cervical lordosis loss and increase axial pain, necessitating cautious surgical planning for multilevel CDD.
Keywords: Degenerative cervical diseases, surgery, C2-7CL
Introduction
Cervical sagittal alignment is an important indicator of degeneration and stability, and plays a very important role in the development of degenerative diseases [1]. As known, cervical parameters including C2-7CL, C2-7SVA and T1S vary continuously and dynamically, and as degeneration progresses, changes in cervical radiological parameters demonstrate that C2-7CL decreases and C2-7SVA increases, and yet, the variation of T1S is with dramatic nondeterminacy in patients with CDD [2].
Radiological parameters are the imaging manifestations of cervical sagittal alignment and balance [2,3]. Previous studies demonstrated biomechanical balance between cervical anterior and posterior structures changed after decompression and reconstruction surgeries, consequently, cervical sagittal radiological parameters, including C2-7CL, C2-7SVA and T1S were modified significantly in patients with CDD [4,5]. Postoperative complications, such as axial pain, fat liquefaction and infection, which affect cervical alignment directly or circuitously, increased with multiple invasive procedures in clinical practices. Regardless of surgical approaches, cervical curvature improved after first anterior and posterior decompression and reconstruction surgeries. Literatures reported C2-7CL and T1S increased after first cervical procedure, though, there was no theoretical data about the change of cervical sagittal alignment and curvature after more than one surgery performed in existing studies [2-5].
Accordingly, in order to explore the change of cervical curvature and alignment after more than one surgery in CDD patients, we compared and analyzed the clinical functional outcomes and radiological parameters of three groups patients with different number of surgeries in this study.
Materials and methods
Participants
Written informed consent was acquired from each patient prior to the study, and the study was approved by the Ethics Committee. Multilevel CDD patients who underwent once, twice and thrice decompression and reconstruction surgeries, and presented integrated clinical data in the department of spine surgery between January 2015 and December 2022 were recruited. Groups were divided into groups according to the number of operations, first surgery as group 1, second surgery as group 2 and third surgery as group 3. The procedure techniques included anterior cervical discectomy and fusion (ACDF), hybrid technique of anterior cervical corpectomy and fusion (ACCF), and posterior reconstruction included laminoplasty (LAMP) and laminectomy with fusion (LF). The inclusion criteria were: (I) adult patients with a diagnosis of CDD and preoperative multilevel impairment confirmed by MRI; (II) underwent once, twice and thrice decompression and reconstruction surgeries and integrated clinical data; (III) established a follow-up period longer than 12 months after final surgery and the final neurological functions were satisfied. The exclusion criteria were: (I) underwent other spine surgeries before the surgeries performed in hospital; (II) T1 vertebral body blocked by sternum or ribs on lateral X-ray radiographs when standing with a neutral position and looking straight forward to maintain a horizontal gaze; (III) history of osteoporosis, trauma, tumor, or infection of the cervical spine.
Surgical technique
All surgeries were conducted by the same senior surgeon. Soft collars were worn for 3 months in these patients after surgery. The anterior decompression and reconstruction techniques include classical ACDF, hybrid technique is a combination of discectomy and corpectomy. Posterior approach techniques include laminoplasty (LAMP), and laminectomy with fusion (LF).
ACDF was performed with the standardized right-sided Robinson-Smith anterior approach. Incision was performed using a right-sided approach at the appropriate cervical level. Following division of platysma, blunt dissection was performed until deep prevertebral fascia was reached. Following a second fluoroscopy, the hyperplastic osteophyte, degenerative disc and posterior longitudinal ligament were removed. The cages filled with bone fragments were inserted into the intervertebral space. The vertebral body of the decompression area was fixed by the titanium plate. Corpectomy was performed using a highspeed bur carefully. Uncinate processes were used as reference points to determine the width of the corpectomy. The posterior longitudinal ligament was removed by using a Kerrison rongeur until exposure of the dura mater was achieved. The decompressed segment was measured so an appropriately sized Tantalum trabecular metal (TTM) designed to match the anatomy of the adjacent end plates could be placed.
LAMP was performed on patients in a prone position with head fixed using the Mayfield head holder. The lamina and spinous processes were exposed by a posterior midline approach, and the side with relatively severe clinical symptoms and/or radiographic compression was selected as the open side, where the outer and inner cortical margins were both drilled using a high-speed drill. The inner cortical margin of the hinge side was preserved, and the lamina was lifted from the open side toward the hinge side and fixed in an expanded position with 8-12 mm miniplates. LF was performed in a prone position. The spinous processes, laminae, facet joints, and transverse processes were exposed by a posterior midline approach that was similar to laminoplasty. Subsequently, the lateral mass screws and prebending titanium rods were placed at the target segment, followed by a resection of the lamina and ligamentum flavum. Autologous bone grafts from the lamina were placed adjacent to the bilateral joints to facilitate fusion.
Clinical and radiographic evaluation
Data were collected before surgery and at the time of final follow-up. The Japanese Orthopedic Association (JOA) score is a standardized tool for assessing neurological function in patients with spinal cord injuries, encompassing motor, sensory, and bladder functions, where a higher score indicates better function. Neck Disability Index (NDI) is a questionnaire assessing functional status in cervical spine disorder patients, comprising 10 items with a total score of 50, where higher scores indicate greater disability. Visual analog scale (VAS) is a tool for assessing pain intensity, where patients mark their pain level on a 10 cm line, with 0 being no pain and 10 being the worst pain. Scoring systems were used for clinical assessment of neurological outcomes. Complications including dysphagia, hematoma, axial pain, cerebrospinal fluid leakage, C5 paralysis, infection, and deterioration in neurologic deficits were recorded, and rates of each complication was calculated for comparison among groups.
The cervical sagittal parameters were measured on the lateral X-ray radiographs (Figure 1): cervical lordosis (C2-7CL) was determined by measuring the angle between the C2 and C7 lower endplates; C2-7 SVA was determined by measuring the distance between the C2 plumb line and the posterior superior endplate of C7; T1 slope was determined by measuring the angle between the horizontal plane and the T1 upper endplate.
Figure 1.
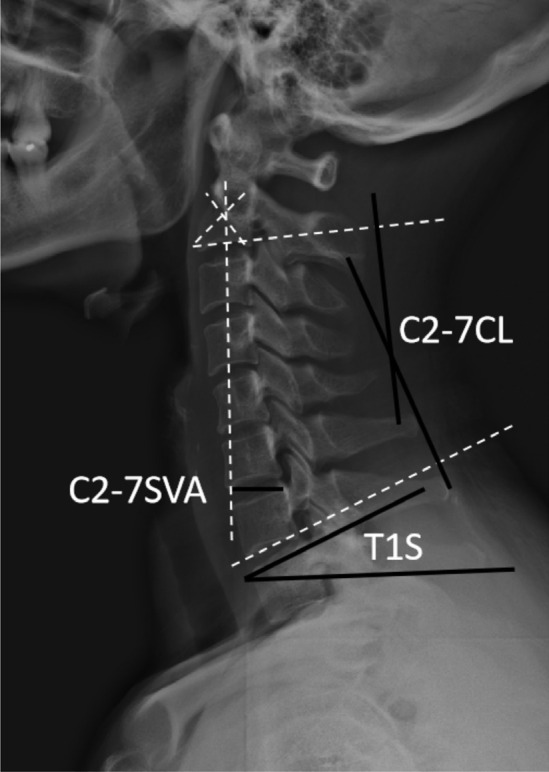
Cervical sagittal parameters: 1) cervical lordosis (C2-7CL): the angle between the C2 and C7 lower endplates; 2) C2-7 SVA: the distance between the C2 plumb line and the posterior superior endplate of C7; 3) T1S: the angle between the horizontal plane and the T1 upper endplate.
Statistical analysis
Statistical analysis was performed using SPSS version 26.0 (IBM, Armonk, New York, USA, version 11), with P value < 0.05 considered statistically significant. Continuous variables were calculated as mean value ± standard deviations (SD), and categorical variables were calculated as frequencies. Chi-square analysis was performed to compare categorical variables among groups. Non-parametric analysis, independent and paired t test was used to compare the continuous variables in and among the three groups.
Results
Demographics
The baseline characteristics of the patient populations were summarized in Table 1. Group 1 included 63 patients (41 males and 22 females) with an average age of 64.7±10.0 years (43-76 years), group 2 included 53 patients (35 males and 18 females) with an average age of 65.3±9.1 years (45-77 years) and group 3 included 29 patients (17 males and 12 females) with an average age of 65.6±9.3 years (45-78 years). All patients were followed up more than 12 months after final surgery. The sex ratio, average age and follow-up time were not statistically different (P > 0.05), while the differences demonstrated were statistically significant in terms of operation time, blood loss and hospital study (P < 0.001) among groups.
Table 1.
Demographic data of the patients in two groups (mean ± SD)
| Characteristic | NO=1 | NO=2 | NO=3 | χ2/F | p |
|---|---|---|---|---|---|
| Sex (male/female), n | 41/22 | 35/18 | 17/12 | 0.717 | 0.699 |
| Age (years) | 64.7±10.0 | 65.3±9.1 | 65.6±9.3 | 1.332 | 0.267 |
| Op-time (min) | 124.6±8.2 | 130.6±17.9a | 138.9±16.3a,b | 10.272 | 0.000 |
| Blood loss (ml) | 129.8±39.7 | 251.9±73.4a | 277.6±60.6a | 92.407 | 0.000 |
| Hospital stay (days) | 8.2±1.4 | 10.9±1.5a | 11.6±1.3a,b | 76.595 | 0.000 |
| Follow-up (months) | 22.5±5.3 | 20.7±6.3 | 21.4±3.9 | 1.451 | 0.238 |
Note: NO: number of operations;
compared with NO=1, P < 0.05;
compared with NO=2, P < 0.05.
Comparison of clinical and radiographic measurements
The clinical outcomes and radiographic parameters were summarized in Table 2. The radiological parameters, JOA score, VAS-neck score and NDI were not significantly different among groups (P > 0.05) before and after surgeries. At the final follow-up, clinical and radiological parameters in each group changed significantly different compared with preoperative items except C2-7SVA in NO=2 and NO=3 group. C2-7CL and T1S decreased in NO=2 (P < 0.001) and NO=3 (P < 0.001) group, and the values of C2-7CL and T1S were smaller than NO=1 group (P < 0.01). NDI and VAS decreased significantly (P < 0.001) in each group, and the values of NDI and VAS were larger than NO=1 group (P < 0.05).
Table 2.
Clinical and radiographic outcomes in two groups (mean ± SD)
| Parameters | Pre-operation | Final follow-up | t | p |
|---|---|---|---|---|
| NO=1 | ||||
| C2-7 CL (°) | 17.5±5.3 | 20.6±7.7 | -3.841 | 0.000 |
| C2-7 SVA (mm) | 18.9±6.5 | 22.1±6.9 | -5.278 | 0.000 |
| T1S (°) | 24.5±6.8 | 32.6±7.9 | -13.691 | 0.000 |
| JOA | 10.1±1.7 | 15.1±1.3 | -19.119 | 0.000 |
| NDI | 46.6±6.5 | 26.5±6.8 | 16.581 | 0.000 |
| VAS | 2.6±1.2 | 0.9±0.7 | 10.249 | 0.000 |
| NO=2 | ||||
| C2-7 CL (°) | 17.7±5.4 | 11.6±4.3a | 7.260 | 0.000 |
| C2-7 SVA (mm) | 20.6±5.1 | 21.0±5.9 | -0.462 | 0.646 |
| T1S (°) | 24.4±8.1 | 20.5±3.1a | 3.307 | 0.002 |
| JOA | 9.9±2.1 | 15.0±1.3 | -16.004 | 0.000 |
| NDI | 47.1±7.2 | 30.3±4.5a | 16.090 | 0.000 |
| VAS | 2.6±1.1 | 1.9±0.9a | 3.3644 | 0.000 |
| NO=3 | ||||
| C2-7 CL (°) | 18.2±3.4 | 10.2±3.1a | 8.825 | 0.000 |
| C2-7 SVA (mm) | 19.1±7.5 | 20.0±4.6 | -0.697 | 0.491 |
| T1S (°) | 25.6±5.6 | 20.0±3.1a | 4.896 | 0.000 |
| JOA | 10.2±2.5 | 14.8±1.3 | -7.802 | 0.000 |
| NDI | 47.5±5.2 | 33.2±4.3a,b | 12.786 | 0.000 |
| VAS | 3.0±0.7 | 2.4±0.7a,b | 3.016 | 0.005 |
Note: NO: number of operations;
compared with NO=1, P < 0.05;
compared with NO=2, P < 0.05.
Analysis of complications
Invasive wound healed well in all cases. Postoperative complications were compared and summarized in Table 3. There was no difference showed in terms of dysphagia, epidural hematoma, C5 palsy, fat liquefaction, infection, neurologic deficit, graft dislodgement and subsidence among three groups (P > 0.05). Incidences of cerebrospinal fluid leakage (CFL), axial pain and total complications were significantly different among groups (P < 0.01), and the incidence rates increased with the number of surgeries.
Table 3.
Postoperative complications in two groups
| Complications (n) | NO=1 | NO=2 | NO=3 | χ2 | p |
|---|---|---|---|---|---|
| dysphagia | 1/62 | 1/52 | 2/27 | 2.323 | 0.313 |
| epidural hematoma | 0/63 | 0/53 | 0/29 | - | - |
| C5 palsy | 0/63 | 2/51 | 2/27 | 3.842 | 0.146 |
| SFL | 0/63 | 2/51 | 4/25 | 9.553 | 0.008 |
| axial pain | 0/63 | 3/50 | 11/18 | 34.283 | 0.000 |
| fat liquefaction | 0/63 | 1/52 | 1/28 | 1.894 | 0.388 |
| infection | 0/63 | 0/53 | 0/29 | - | - |
| neurologic deficit | 0/63 | 0/53 | 1/28 | 4.028 | 0.133 |
| graft dislodgement | 0/63 | 0/53 | 0/29 | - | - |
| subsidence | 0/63 | 0/53 | 0/29 | - | - |
| Total | 1/62 | 5/48 | 21/29 | 70.393 | 0.000 |
Discussion
Cervical degenerative diseases (CDD) leads radiculopathy and myelopathy function impairments [1], and changes cervical sagittal alignment, which can help to evaluate disease severity, formulate an appropriate preoperative strategies, predict prognosis, and guide rehabilitation exercises. With deterioration of physiological manifestations, cervical sagittal alignment turns from normal lordotic to straight, sigmoid and kyphotic, and finally, cervical balance may change subsequently [6,7]. As cervical imbalance may lead neurofunction deterioration, neck pain and decrease the quality of life, more attention has been paid to cervical sagittal alignment. Hence, first surgery treatment routinely performed after failure from conservative therapy seems quite necessary (Figure 2).
Figure 2.

Anterior cervical hybrid surgery of C3/4, C4/5 discectomy and C6 corpectomy. Before surgery, C2-7CL was 17.3, C2-7SVA was 15.8 mm and T1S was 21.1. At the 12-month follow-up, C2-7CL was 21.2, C2-7SVA was 20.4 mm and T1S was 33.2.
Cervical surgeries can restore the disordered conditions of abnormal neurofunction and imbalance, although, the invasive disadvantages cannot be ignored [8,9]. As is known that the key procedures of discectomy, corpectomy, antedisplacement, laminoplasty and laminectomy are decompression and reconstruction, which are trigger factors of neural functional recovery. However, poor neurofunction recoveries of were subjected after procedures implementation in a portion of patients with multilevel CDD, which resulted from massive and complex causative factors. Additionally, severe dysfunction manifestations and complex physiopathologic etiological elements resulted in a second or third cervical surgery [9,10]. In this study, some patients suffered second (Figure 3) and third (Figure 4) decompression and reconstruction surgery who got poor neural functional recovery were enrolled in group 2 and group 3, and fortunately, those patients got satisfied clinical outcomes were met the inclusion criteria.
Figure 3.

First surgery of C5/6 discectomy and C4 corpectomy, and second surgery of open-door laminoplasty of C3-C7. Before surgery, C2-7CL was 16.2, C2-7SVA was 18.8 mm and T1S was 23.0. At the 12-month follow-up, C2-7CL was 12.1, C2-7SVA was19.4 mm and T1S was 21.1.
Figure 4.

First surgery of open-door laminoplasty of C3-C7, second surgery of laminectomy of C3-C7 with lateral mass fixation, and third surgery of C4 corpectomy. Before surgery, C2-7CL was 14.9, C2-7SVA was 17.7 mm and T1S was 21.5. At the 12-month follow-up, C2-7CL was 10.7, C2-7SVA was 20.5 mm and T1S was 22.5.
Cervical surgeries can change sagittal alignment and curvature, as radiographic findings show alterations in radiological parameters [2,3,11,12]. Cervical structures are remolded inevitably after invasive procedures [2,3,13], and the number of cervical surgeries aggravated worse damages. Furthermore, the more serious damages of bone structures and soft tissues, the greater changes of cervical sagittal alignment and curvature demonstrated. In other words, the changes of cervical biomechanical environment after surgeries are closely related to sagittal alignment and curvature theoretically and logically. Previous studies illustrated cervical curvature changed after first surgery for multilevel CDD, conducting C2-7CL decreased and C2-7SVA increased, no matter anterior or posterior approach invasive treatment [14,15]. In our study, the variation of cervical sagittal alignment was consistent with the above characterization data in group 1, while, the variations were different in other groups, whom underwent more than once surgery.
Cervical sagittal curvature changes after first invasive intervention [2,3], yet the data of second and third surgery have not been reported according to clinical investigation [16,17]. Perspectives in literatures on cervical sagittal curvature change are always consistent in terms of first surgery for patients with CDD [2,3], and cervical procedures could improve nervous dysfunction and subaxial sagittal balance [18,19]. According to radiological examination after first cervical surgery, parameters including C2-7CL, T1S and C2-7SVA increases simultaneously [20,21]. Surgeries change the biomechanical environments of cervical spine, and multiple surgeries damage the bone and soft tissue structures more seriously [22-24]. Therefore, straight cervical spine and more complications may be the explainations of changes of cervical radiological parameters unexpectedly uncommon in group 2 and group 3 in our study.
Cervical sagittal alignment was linearized after multiple surgeries, manifesting C2-7CL and T1S decreased, while cervical sagittal balance maintain a dynamic stability. Although, previous studies reported many different perspectives about postoperative complications and revision surgery [25-27], multiple surgeries for CDD were rarely reported in available literatures [28,29]. In this study, comparing with preoperative values in CDD patients, C2-7CL and T1S were significantly decreased, and C2-7SVA changed without significance in group 2 and group 3. The characteristics were contrary based on clinical practices and theoretical study. In terms of complications, incidence rates of cerebrospinal fluid leakage (CFL) and axial pain in group 2 and group 3 were higher than group 1, and total incidence rates were significantly different among three groups. Therefore, conclusions were drawn from the data and phenomena that multiple cervical surgeries can impair physiological function, and increase the loss of cervical lordosis and incidence rates of complications in multilevel CDD.
The present study has several limitations. Firstly, it was a retrospective and single-centered study. Secondly, this study is a summarization and representation of a clinical data and phenomenon, and there is no longer follow-up and biomechanical evidence to support it. Thirdly, the compensatory mechanism of cervicothoracic junction and soft tissues cannot be ignored after cervical surgeries. Therefore, further prospective, randomized controlled and multicentered clinical trials, and biomechanical experimental researches should be conducted to confirm these findings.
Conclusions
Cervical decompression and reconstruction surgeries can improve dysfunction and change sagittal alignment. Multiple surgeries increased the loss of C2-7CL and T1S, which may be vital iatrogenic factors in terms of high incidences of complications. Therefore, thoughtful strategies should be developed when multilevel CDD patients needed surgical treatments. The events cannot be done that high incidences of complications exchanged for improved neurological function.
Acknowledgements
This study was supported by Shanghai Hongkou District Clinical Key Specialty (HKLCZD2024B03).
Disclosure of conflict of interest
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- 1.Gallagher DO, Taghlabi KM, Bondar K, Saifi C. Degenerative cervical myelopathy: a concept review and clinical approach. Clin Spine Surg. 2024;37:1–8. doi: 10.1097/BSD.0000000000001463. [DOI] [PubMed] [Google Scholar]
- 2.Chen S, Deng Y, Liu H, Wu T, Huang K, He J, Wang B. Cervical sagittal balance after consecutive three-level hybrid surgery versus anterior cervical discectomy and fusion: radiological results from a single-center experience. J Orthop Surg Res. 2023;18:345. doi: 10.1186/s13018-023-03819-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu C, Zhu W, Li Y, Li X, Shi B, Kong C, Lu S. How does cervical sagittal profile change after the spontaneous compensation of global sagittal imbalance following one- or two-level lumbar fusion. BMC Musculoskelet Disord. 2024;25:387. doi: 10.1186/s12891-024-07518-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Huang K, Wang Q, Rong X, Wu T, Ding C, Meng Y, Yin W, Liu H, Wang B. Biomechanical effects on the prostheses and vertebrae of three-level hybrid surgery: a finite element study. Orthop Surg. 2024;16:2019–2029. doi: 10.1111/os.14125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Xu H, Liu Z, Yang Y, Miao J, Wang B, Yang C. Biomechanical comparison of different surgical strategies for skip-level cervical degenerative disc disease: a finite element study. Spine (Phila Pa 1976) 2024;49:E262–E271. doi: 10.1097/BRS.0000000000005050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bębenek A, Godlewski B. Anterior cervical discectomy and fusion (ACDF) with and without plating: a comparison of radiological and clinical outcomes. Adv Clin Exp Med. 2024;33:881–888. doi: 10.17219/acem/172062. [DOI] [PubMed] [Google Scholar]
- 7.Wichmann TO, Bech-Azeddine R, Norling AL, Einarsson HB, Rasmussen MM. Comparison of outcomes and complications between one- and two-level anterior cervical discectomy and fusion: a population-based study of 410 patients. Br J Neurosurg. 2024;38:928–933. doi: 10.1080/02688697.2021.2005778. [DOI] [PubMed] [Google Scholar]
- 8.Xu R, Bydon M, Macki M, De la Garza-Ramos R, Sciubba DM, Wolinsky JP, Witham TF, Gokaslan ZL, Bydon A. Adjacent segment disease after anterior cervical discectomy and fusion: clinical outcomes after first repeat surgery versus second repeat surgery. Spine (Phila Pa 1976) 2014;39:120–6. doi: 10.1097/BRS.0000000000000074. [DOI] [PubMed] [Google Scholar]
- 9.Veeravagu A, Cole T, Jiang B, Ratliff JK. Revision rates and complication incidence in single- and multilevel anterior cervical discectomy and fusion procedures: an administrative database study. Spine J. 2014;14:1125–31. doi: 10.1016/j.spinee.2013.07.474. [DOI] [PubMed] [Google Scholar]
- 10.Roth SG, Robles Ortiz MJ, Vulapalli M, Riew KD. Revision strategies for cervical disc arthroplasty. Clin Spine Surg. 2023;36:411–418. doi: 10.1097/BSD.0000000000001542. [DOI] [PubMed] [Google Scholar]
- 11.Wang B, Qu R, Liu Z, Zhao N, Pan S, Chen X, Zhao Y, Dang L, Zhou H, Wei F, Sun Y, Zhou F, Jiang L. Comparison of postoperative pain and surgical outcomes between three types of modified muscle-sparing laminoplasty and conventional laminoplasty for multilevel degenerative cervical myelopathy. Global Spine J. 2025;15:1801–1812. doi: 10.1177/21925682241265625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Johansen TO, Holmberg ST, Danielsen E, Rao V, Salvesen ØO, Andresen H, Carmen VLA, Solberg TK, Gulati S, Nygaard ØP. Long-term results after surgery for degenerative cervical myelopathy. Neurosurgery. 2024;94:454–460. doi: 10.1227/neu.0000000000002712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoelen TA, Willems PC, Loenen A, Meisel HJ, Wang JC, Jain A, Buser Z, Arts JJ AO Spine Knowledge Forum Degenerative. The evidence for the use of osteobiologics in hybrid constructs (anterior cervical discectomy and fusion and total disc replacement) in multilevel cervical degenerative disc disease: a systematic review. Global Spine J. 2024;14:120S–128S. doi: 10.1177/21925682221150795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bębenek A, Dominiak M, Godlewski B. Cervical sagittal balance: impact on clinical outcomes and subsidence in anterior cervical discectomy and fusion. Biomedicines. 2023;11:3310. doi: 10.3390/biomedicines11123310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schmeiser G, Bergmann JI, Papavero L, Kothe R. Surgical treatment of multilevel degenerative cervical myelopathy: open-door laminoplasty and fixation via unilateral approach. A feasibility study. J Neurol Surg A Cent Eur Neurosurg. 2022;83:494–501. doi: 10.1055/s-0041-1739224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Akgün MY, Ateş Ö, Tepebaşili MA, Günerbüyük C, Özer AF. Clinical parameters of laminoplasty and laminectomy with fusion in the treatment of cervical spondylosis and analysis of postoperative sagittal balance. Turk J Med Sci. 2023;53:1458–1464. doi: 10.55730/1300-0144.5713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hiyama A, Katoh H, Sakai D, Sato M, Tanaka M, Nukaga T, Watanabe M. Correlation analysis of sagittal alignment and skeletal muscle mass in patients with spinal degenerative disease. Sci Rep. 2018;8:15492. doi: 10.1038/s41598-018-33867-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chambers JS, Kropp RG, Gardocki RJ. Reoperation rates and patient-reported outcomes of single and two-level anterior cervical discectomy and fusion. Arch Orthop Trauma Surg. 2023;143:265–268. doi: 10.1007/s00402-021-04056-y. [DOI] [PubMed] [Google Scholar]
- 19.Steinle AM, Nian H, Pennings JS, Bydon M, Asher A, Archer KR, Gardocki RJ, Zuckerman SL, Stephens BF, Abtahi AM. Complications, readmissions, revisions, and patient-reported outcomes in patients with parkinson disease undergoing elective spine surgery: a propensity-matched analysis. Spine (Phila Pa 1976) 2022;47:1452–1462. doi: 10.1097/BRS.0000000000004401. [DOI] [PubMed] [Google Scholar]
- 20.Xu C, Zhang Y, Dong M, Wu H, Yu W, Tian Y, Cao P, Chen H, Wang X, Shen X, Liu Y, Yuan W. The relationship between preoperative cervical sagittal balance and clinical outcome of laminoplasty treated cervical ossification of the posterior longitudinal ligament patients. Spine J. 2020;20:1422–1429. doi: 10.1016/j.spinee.2020.05.542. [DOI] [PubMed] [Google Scholar]
- 21.Hung CW, Wu MF, Yu GF, Ko CC, Kao CH. Comparison of sagittal parameters for anterior cervical discectomy and fusion, hybrid surgery, and total disc replacement for three levels of cervical spondylosis. Clin Neurol Neurosurg. 2018;168:140–146. doi: 10.1016/j.clineuro.2018.03.003. [DOI] [PubMed] [Google Scholar]
- 22.Joo PY, Jayaram RH, McLaughlin WM, Ameri B, Kammien AJ, Arnold PM, Grauer JN. Four-level anterior versus posterior cervical fusions: perioperative outcomes and five-year reoperation rates: outcomes after four-level anterior versus posterior cervical procedures. N Am Spine Soc J. 2022;10:100115. doi: 10.1016/j.xnsj.2022.100115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shahzad H, Alvarez PM, Pallumeera M, Bhatti N, Yu E, Phillips FM, Khan SN, Singh VK. Exploring the incidence and risk factors of reoperation for symptomatic adjacent segment disease following cervical decompression and fusion. N Am Spine Soc J. 2023;17:100305. doi: 10.1016/j.xnsj.2023.100305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li X, Yu H, Welle K, Gathen M, Zhang L, Xiao J, Kabir K. Comparative effectiveness and safety of open-door laminoplasty, French-door laminoplasty, laminectomy and fusion, andlaminectomy alone for multilevel degenerative cervical myelopathy: a bayesian network analysis. Adv Ther. 2022;39:117–139. doi: 10.1007/s12325-021-01980-8. [DOI] [PubMed] [Google Scholar]
- 25.Ouyang H, Hu Y, Hu W, Zhang H, Sun Z, Tang Y, Jiang Y, Chen J, Dong S, Li W, Tian Y. Incidences, causes and risk factors of unplanned reoperations within 30 days of spine surgery: a single-center study based on 35,246 patients. Spine J. 2022;22:1811–1819. doi: 10.1016/j.spinee.2022.07.098. [DOI] [PubMed] [Google Scholar]
- 26.Nakashima H, Kanemura T, Satake K, Ito K, Ouchida J, Morita D, Ando K, Kobayashi K, Ishiguro N, Imagama S. Reoperation for late neurological deterioration after laminoplasty in individuals with degenerative cervical myelopathy: comparison of cases of cervical spondylosis and ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976) 2020;45:E909–E916. doi: 10.1097/BRS.0000000000003408. [DOI] [PubMed] [Google Scholar]
- 27.Park MS, Ju YS, Moon SH, Kim TH, Oh JK, Makhni MC, Riew KD. Reoperation rates after surgery for degenerative cervical spine disease according to different surgical procedures: national population-based cohort study. Spine (Phila Pa 1976) 2016;41:1484–1492. doi: 10.1097/BRS.0000000000001581. [DOI] [PubMed] [Google Scholar]
- 28.Altorfer FCS, Kelly MJ, Avrumova F, Zhu J, Abjornson C, Lebl DR. Reasons for revision surgery after cervical disk arthroplasty based on medical device reports maintained by the US food and drug administration. Spine (Phila Pa 1976) 2024;49:1417–1425. doi: 10.1097/BRS.0000000000005060. [DOI] [PubMed] [Google Scholar]
- 29.Jentzsch T, Wetzel OT, Malhotra AK, Lozano CS, Massicotte EM, Spirig JM, Fehlings MG, Farshad M. Cervical kyphosis after posterior cervical laminectomy with and without fusion. Eur Spine J. 2024;33:3109–3116. doi: 10.1007/s00586-024-08260-3. [DOI] [PubMed] [Google Scholar]