

Abstract
Obesity independently increases AF risk and negatively affects the outcomes of catheter ablation. This review examines the relationship between obesity and AF, focusing on structural and electrical remodelling. Multiple studies demonstrate worse ablation outcomes in patients with obesity. Pre-ablation weight loss improves outcomes and maintaining weight loss post-ablation is equally important. Risk factor modification programmes show promise, however they require a large investment in resources. Less intensive strategies focusing on diet and exercise have shown mixed results. Glucagon-like peptide-1 receptor agonists have been identified as potential adjunct therapies. They have multiple effects, including preferential reduction of epicardial adipose tissue and an anti-inflammatory action. Further research is needed to establish their efficacy in improving ablation outcomes. This review highlights the importance of weight management in AF treatment and suggests potential monitoring strategies using cardiac imaging. Future studies may shift the paradigm for the management of AF patients with obesity who are undergoing ablation.
Keywords: Ablation, atrial fibrillation, emerging therapies, duration of therapy, obesity, risk factors
Central Illustration: Flow Chart Summarising the Approach to a Patient with AF and Obesity, with Focus on the Structured Weight Loss Programmes (European Society of Cardiology ABC Approach).

This structured weight loss approach can reverse an AF phenotype and improve outcomes from rhythm control therapies. ABC = anticoagulation, better symptom control, comorbidities.
AF is the most common arrhythmia in clinical practice and its prevalence is increasing. The estimated number of patients with AF globally was 33.5 million in 2010 and this rose to 50 million in 2020.1,2 The estimated lifetime risk of AF among people in Europe was one in four in 2006, rising to one in three in 2020.3 A similar projected prevalence has been estimated for the US population from 5.2 million in 2010 to 12.1 million in 2030.4 AF is associated with higher morbidity and mortality. Quality of life (QoL) is impaired due to a wide array of symptoms, including lethargy, palpitations, dyspnoea, sleeping difficulties and psychosocial distress. Patients with AF are four times as likely to require cardiovascular hospitalisation compared to propensity-matched controls and suffer from higher rates of heart failure and stroke.5 AF is an independent predictor of all-cause mortality, with a two-fold adjusted increase in death.6
Mirroring this, the prevalence of obesity is rising rapidly and brings with it an exponential risk of cardiovascular morbidity and mortality. Globally, the estimated prevalence of obesity (BMI ≥30) increased from 3.2% in 1975 to 10.8% in 2014 in men, and from 6.4% to 14.9% in women.7 In 2019, more than half (53%) of the European population was overweight (BMI ≥25 kg/m2).8 In the US, the prevalence of adult obesity was 42% in 2017–2018.9 While it is well-known that obesity is an upstream risk factor for hypertension, diabetes and obstructive sleep apnoea (OSA), the independent impact ofobesity on incidence, recurrence and management of AF is less appreciated. Both European (anticoagulation, better symptom control, comorbidities) and American (lifestyle and risk factor modification) guidelines on the management of AF recommend weight loss before ablation; however, it is less clear how that may be best achieved and over what time course.3,10,11
The aim of this article is to review the available evidence, including emerging therapies that may optimise patient outcomes.
Obesity and Onset of AF
Multiple epidemiological studies have shown a strong association between obesity and the risk of developing AF, although there are many potential confounding factors, including hypertension, diabetes and dyslipidaemia. However, a smaller number of studies have investigated the effect of obesity independent of associated risk factors by recruiting metabolically healthy obese (MHO) patients, defined as having a BMI above 30 but without associated metabolic conditions (Supplementary Table 1).12-14 MHO is characterised by normal insulin sensitivity blood pressure and lipid profiles. Crucially, obesity should be understood as a complex continuum instead of a binary condition. MHO may progress to metabolically unhealthy obesity (MUO) over time unless preventive interventions are not initiated early.
In a Swedish population-based longitudinal study of 4,021 participants with a mean follow-up of 13.6 years, obesity was associated with an increased risk of AF independent of other risk factors (HR 1.75; 95% CI [1.11–2.74]).12 A study that used a national health insurance database of a large population of 389,321 participants in Korea confirmed that MHO individuals had an increased risk of AF (HR 1.3; 95% CI [1.14–1.48]).13 Of importance, a quarter of this cohort became metabolically unhealthy during a mean follow-up of 7.5 ± 1.5 years. The question whether MHO individuals and MUO individuals carry the same risk of AF was investigated in another population-based prospective study of 47,670 participants from Norway.14 Compared to people with a normal weight (BMI <25 kg/m2), both MHO and MUO individuals had a HR of 1.6 for the development of AF and the risk increased according to the severity of obesity. This growing evidence suggests that obesity is an independent risk factor for AF.
Obesity and Persistence of AF
It has long been established that AF starts with the rapid firing of ectopic foci (triggers) from myocyte sleeves within the pulmonary veins.15 Typically, these present as short attacks and can spontaneously resolve with or without treatment. For these triggers to set off persistent AF, conditions (referred to as substrates) must be favourable. Substrates can be structural, such as inflammation, scarring and changes in pressure or volume, or electrical, such as changes in conduction velocity and voltage in the atria. A trigger initiates AF and the substrate enables it to persist. This interplay between triggers and substrate governs the clinical course of AF and obesity is a common interlocutor (Figure 1).
Figure 1: Obesity as an Independent Risk Factor in Promoting AF.

Obesity and Cardiac Structure and Function
Left atrial (LA) dilatation, whether measured by diameter or volume, and impaired LA function, are known to be important substrates that promote persistent AF. These changes are common in obesity and precede the onset of AF. The prevalence of LA enlargement in obesity ranges from 9.8% to 37% by LA diameter on 2D echocardiography, and obesity is a more important driver for this change than hypertension.16,18 Similar changes are seen on echocardiography in MHO participants, who have a significantly larger LA dimension than people with a normal weight.19 Obese patients have impaired LA global strain which is a measure of how good the left atrium can stretch and contract during a cardiac cycle measured by speckle-tracking echocardiography which tracks tiny dots or speckles all over the left atrium (-10.5 ± 3.7%), compared to non-obese patients (-13.1 ± 5.1%; p=0.004).20 Further, obesity is associated with impaired reservoir (the ability of the LA to store pulmonary venous return during left ventricular (LV) contraction and isovolumetric relaxation) and conduit LA function (the ability of the LA to transport blood passively into left ventricle) (Figure 2).21
Figure 2: Left Atrial Strain.
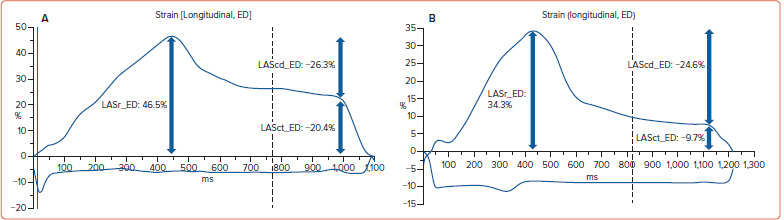
A: a patient with BMI <25 and B: a patient with BMI >30. Compared to a patient with normal BMI in panel A, the patient with obesity in panel B shows lower reservoir function (34.3% versus 46.5%), lower conduit function (-24.6% versus -26.3%) and lower contraction function (-9.7 versus -20.4%). In strain analysis, the negative sign before the number denotes shortening of cardiac muscles whereas the positive lengthening of cardiac muscles rather than positive or negative values. ED = end diastole; LAScd = left atrial (LA) strain conduit function; LASct = LA strain contraction function; LASr = left atrial strain reservoir function.
Changes in the LA are likely to be secondary to impaired LV diastolic function and LV hypertrophy. Multiple studies have confirmed that diastolic dysfunction is common in obesity, reflected in a higher pressure half-time, lower deceleration slope, high peak A velocity, lower E/A ratio, prolonged isovolumetric relaxation time, and a lower peak systolic velocity of the lateral mitral annulus.22,26 Post-mortem studies of obese individuals reported higher heart weight, LV wall thickness and more frequent dilated cardiomyopathy.27 These changes were corroborated by a meta-analysis of 15 echocardiographic studies that reported obese patients were 4.2-fold more likely to have LV hypertrophy than non-obese patients.28
Obesity, Inflammation and AF
Epicardial adipose tissue (EpAT) and the myocardium are developed from splanchnic mesoderm and receive their blood supply through the coronary arteries.29 By contrast, paracardial fat develops from the primitive thoracic mesenchyme and blood is supplied from branches of the internal mammary artery.29 Unlike paracardial fat, there is no fascia between EpAT and the myocardium, meaning that EpAT is in direct contact and can share microcirculation and local interactions.30 EpAT relation to AF is particularly important. EpAT is positively correlated with BMI.31,32 Moreover, multiple studies have reported a close relationship between the extent of EpAT and incidence, duration and recurrence of AF.33-37 EpAT can be measured using echocardiography, CT or cardiovascular MRI with low inter- and intra-observer variability (Figure 3).35,38-40
Figure 3: Cardiac MRI Showing Epicardial Adipose Tissue.

A: patient with BMI <25; B: patient with BMI >30. Yellow stars = epicardial adipose tissue; white arrow = visceral pericardium; blue arrow = parietal pericardium.
EpAT contributes to the development and progression of AF through effects including inflammation and fibrosis. In relation to inflammation, Mazurek et al. compared the inflammatory activity of EpAT and skin adipose tissue (SAT) using samples harvested from elective coronary artery bypass graft (CABG) surgery. Higher levels of inflammatory cytokines such as interleukin (IL)-1b, IL-6 and tumour necrosis factor (TNF)-α were found in EpAT samples (p<0.001).41 Fain et al. replicated these findings to show that EpAT secreted a higher level of IL-1β and TNF-α compared to sternal, abdominal and leg SATs.42 Irrespective of underlying coronary artery disease or hypertension, EpAT from overweight/obese patients showed higher levels of IL-1, IL-6, TNF-α and interferon-g compared to lean controls (p<0.01).43
In relation to fibrosis, the atrial myocardium in rats was exposed to the samples of EpAT and SAT from patients undergoing CABG by Venteclef et al.44 Compared to SAT, EpAT secreted activin A (p=-0.0002), a profibrotic maker, which induced both interstitial and peripheral fibrosis of the rat atria. In a human study comparing EpAT, SAT and pericardial adipose tissue from patients with sinus rhythm and AF undergoing CABG, the expression of connective tissue growth factor was higher in the EpAT of AF patients than in the SAT and PAT of AF patients and the EpAT of patients with sinus rhythm.45 In a study of right atrial appendage tissue excised from patients undergoing CABG with AF, Nalliah et al. reported higher local EpAT volume to be associated with more fibrosis, slower conduction and lateralisation of connexin40 (an important human atrial gap junction protein that regulates successful propagation of action potentials through the myocardium) than in patients in sinus rhythm.46 The lack of fascia between EpAT and the myocardium allows these mediators or ‘adipokines’ to have a local (paracrine) effect, acting as drivers for arrhythmias both in animal models and in human studies.43,47,48 (Supplementary Table 2 for multimodality assessment of persistent AF substrate in obese AF patients).
Obesity and Electrical Remodelling
Obesity-dependent changes in LA conduction velocity and voltage have been reported in animal studies.49,50 In ovine studies, sheep were fed with hay and high-energy pellets to induce progressive weight gain. This resulted in progressive LA electrical remodelling. Obese sheep developed lower LA conduction velocity, decreased LA voltage, higher LA pressure and more extensive fibrosis. These electrical changes were replicated in obese patients with AF and may be reversible with weight loss.51 In a study of 30 sheep fed over 72 weeks until they were obese, Mahajan et al. showed that with 30% weight reduction, these changes could be reversed resulting in higher conduction velocity, a fall in LA pressure and a reduction in LA fibrosis.52 It is not known, however, whether weight loss in humans can achieve similar reverse remodelling of atrial substrates.
Obesity and Outcome from Ablation
It is well established that obese patients have lower procedural success (usually defined as evidence of AF in a 12-lead ECG or Holter monitoring in previous research studies) and higher complication rates following catheter ablation for AF (Supplementary Table 3). In brief, recurrence of AF following radiofrequency ablation increased by 15% for each 5 kg/m2 increase in BMI (risk ratio 1.15; 95% CI [1.08–1.22]; heterogeneity, 53%) in a meta-analysis of 26 cohort studies.53 Similarly, Ding et al. reported a 1–5% increased risk of recurrence with every increase of one unit of BMI.54 It is important to note that this effect did not seem to be replicated in studies with cryoablation probably because the majority of the study populations were paroxysmal AF (PAF) patients.55,56 Further studies are required to answer which ablation strategy delivers the most benefit to this group of patients.
Effect of Weight Loss on AF Ablation
Weight Loss Before Ablation
There is growing evidence of the benefit of weight loss before ablation for obese patients. A recent meta-analysis of seven cohort studies by Zhao et al. reported that every 10% weight loss from baseline significantly reduced the chance of recurrence (RR 0.54; 95% CI [0.33–0.88]).57 Of the seven studies, four used lifestyle modification and one used bariatric surgery pre-ablation and the duration of intervention varied from 6 to 22 months (Table 1). Weight loss is not only linked to the success of the procedure but a further meta-analysis of six cohort studies showed an extended effect beyond 12 months in reducing recurrence (RR 0.49; 95% CI [0.31–0.80]).58 Moreover, a significant improvement in outcome accrues from less than 10% weight loss compared to no weight loss at all in longer-term follow-up (RR 0.39; 95% CI [0.31–0.49]). Maintaining a lower weight and not gaining weight is also crucial after ablation. Fluctuation in BMI <1 unit after ablation should be the goal for patients (change in BMI <1 unit versus a change in BMI ≥1 unit OR 0.4; 95% CI [0.18–0.9]).59 For daily clinical practice, patients should be advised to achieve some weight loss at least 3–6 months before offering AF ablation and maintaining this weight within 1 unit of BMI after ablation.
Table 1: Studies Investigating the Effect of Weight Reduction on AF Ablation Outcome.
| Authors | Study Design | Population | Before versus After Ablation (Duration) | Weight Loss Method | Ablation Method | Comparators | Effect on Recurrence |
|---|---|---|---|---|---|---|---|
| Mohanty et al. 201861 | Prospective cohort study | n=90 Age = 62 ±9 years Men = 71% Longstanding PeAF = 100% |
Before for 12 months | Lifestyle | RF | Median 24.9 kg weight loss versus no change |
At 1 year No difference |
| Jia et al. 201959 | Prospective cohort study | n=333 Age: 28-87 years PAF: 59% |
After for 12 months |
Lifestyle | RF |
|
At 12 months OR 0.4; 95% CI 0.18–0.9 |
| Akhtar et al. 202358 | Systematic review and meta-analysis | 6 cohort studies | Before: 5 studies (for 3 to 24 months) | Lifestyle: 4 Bariatric surgery: 1 |
Mixed |
|
Beyond 12 months RR 0.49; 95% CI [0.31–0.80] RR 0.39; 95% CI [0.31–0.49] |
| Gessler et al. 2023 (SORT-AF)60 |
Randomised control trial | n=133 Age: 60 ± 10 years Men: 43% Persistent AF: 57% |
After for 6 months |
Lifestyle | RF: 94% CB: 6% |
BMI at 12 months 34.9 ± 2.6 to 33.4 ± 3.6 versus 34.8 ± 3.0 to 34.5 ± 3.6 | At 12 months No difference |
| Goldberger et al. 2023 (LEAF-AF)62 | Randomised cohort trial | n=59 Age: 62 ± 9 Men: 63% PeAF: 80% |
Before for 3 months |
Lifestyle and liraglutide | NR | ≥3–10% weight loss versus <3% weight loss | At 6 months for PeAF 93% versus 59%; p=0.04 |
| Zhao et al. 202357 | Systematic review and meta-analysis | 7 cohort studies | Before: 5 studies (for 6–22 months) After: 2 studies (for 36 months) | Lifestyle: 4 Bariatric surgery: 1 NR: 2 |
RF | Every 10% weight reduction from baseline | RR 0.54; 95% CI [0.33–0.88] |
CB = Cryoablation; D = change; MA = meta-analysis; NR = Not reported, PeAF=persistent AF; RF = Radiofrequency; SR = systematic review.
Weight Loss After Ablation
Losing weight after AF ablation does not have a similar beneficial effect on recurrence. Gessler et al. randomised 133 patients either to a structured weight reduction programme in a specialised obesity department for the duration of 6 months or a control group.60 Hypertension, diabetes and sleep apnoea were optimised according to current guidelines before ablation in both groups. With implantable monitoring, neither AF burden (defined as the percentage of AF during the observed period) at 3 and 12 months or AF recurrence at 12 months were not significantly different between intervention (BMI changing from 34.9 ± 2.6 to 33.4 ± 3.6 at 12 months) and the control group (no change to BMI). Until further studies investigate a head-to-head comparison between pre-ablation versus post-ablation weight loss, the evidence supports weight loss before ablation and maintenance post-ablation.
Timing the Weight Loss
Weight loss before ablation must be achieved in a timely fashion as the beneficial effect appears to be lost in those with persistent AF for more than 12 months. Despite significant weight loss (19.1–56.7 kg) with lifestyle modification for 1 year before ablation in a prospective cohort study, the single-procedure recurrence rate was similar between the weight loss and no weight loss group at 1 year (63.8% versus 59.3%; p=0.68).61 Recent data published have indicated that a better outcome may be achieved by interventions (lifestyle modification and drug therapy) being limited to only 3 months before ablation (Table 1). This will be discussed further below.62
Strategies for Weight Loss Before Ablation
The ideal programme to improve ablation outcomes would include interventions that target multiple risk factors, including timely weight reduction, optimisation of hypertension and diabetes, treatment of OSA, reduction of alcohol intake, smoking cessation and increasing physical activity. Such risk factor management (RFM) programmes have been tested but are resource intensive. The outcomes of these studies are shown in Table 2. For example, Gessler et al. tested a programme led by an endocrinologist in a specialised obesity department that required participants to attend twice a month for nutritional advice, physical training and cognitive behavioural therapy.60 Before undergoing ablation, all participants were investigated for sleep disordered breathing and control of hypertension and diabetes was optimised, and the programme continued for 6 months following successful ablation.
Table 2: Studies Investigating the Effect of risk factor modification on AF Ablation Outcome.
| Reference | Study design | Population | Before versus after Ablation | Comparator | Ablation Method | Effect on Weight | Effect on Recurrence |
|---|---|---|---|---|---|---|---|
| Resource Intensive | |||||||
| ARREST-AF 201464 | Prospective cohort study | n=165 Age: 58.4 ± 10.8 years Men: 56% Paroxysmal AF: 65% |
Before 9.8 ± 7.1 months After 41.6 ± 12.5 months |
RFM versus control | RF | BMI at final follow-up RFM: 33.5 ± 4.6 to 29.1 ± 3.9 versus control; 32.1 ± 4.7 to 31.8 ± 4.9 |
At final follow-up multiple procedures arrhythmia free survival RFM: 87% versus control: 17.8% |
| LEGACY 201563 | Prospective cohort study | n=355 Age: 65 ± 11 years Men: 64% PAF: 53% |
Before Not reported Total duration 48.4 ± 18.2 |
RFM | RF | Weight loss groups ≥10% WL versus 3–8% WL versus <3% WL or WG | At final follow-up, total arrhythmia-free survival 86.2% versus 65.5% versus 39.6% success rate |
| SORT-AF 202160 | Randomised control trial | n=133 Age: 60 ±10 years Men: 43% PAF: 43% |
After for 6 months |
RFM versus control | RF: 94% CB: 6% |
BMI at 12 months RFM: 34.9 ± 2.6 to 33.4 ± 3.6 versus control 34.8 ± 3.0 to 34.5 ± 3.6 | At 12 months No difference |
| Less Resource Intensive | |||||||
| Mohanty et al. 201861 | Prospective cohort study | n=90 Age: 62 ± 9 years Men: 71% LSPeAF: 100% |
Before for 12 months |
Meal plans by dietitian versus control | RF | Weight loss at 12 months Meal plans -24.9 kg WL, -19.1 to 56.7 kg versus control -0.9 kg WL, -2.3 to 1.4 kg |
At 12 months No difference |
| Ding et al. 202066 | Feasibility study | n=92 Age: 64.6 ± 9.1 years Men: 56% PAF: 43% |
Before for 6 months After patient’s choice |
IF with 5:2 diet versus control | RF: 76% CB: 24% |
BMI before ablation IF 36.5 ± 4 to 33.7 ± 4.2 versus control: no significant change | At 12 months, AF recurrence No difference |
CB = cryoablation; IF = intermittent fasting; LSPeAF = longstanding persistent AF; RF = radiofrequency ablation; RFM = risk factor modification programme; WG = weight gain; WL = weight loss.
A similar approach using a structured motivational and goal-directed programme was employed in the ARREST-AF and LEGACY studies.63,64 The research team supported a dedicated physician to run the programme that included dietary advice, meal replacement sachets and a lifestyle journal (recording diet, weight, blood pressure and exercise). A review occurred every 3 months with additional visits as needed (for the whole duration of the study up to 48 months). Sleep-disordered breathing, hypertension, diabetes and lipids were closely monitored and optimised according to current guidelines. Behavioural support was offered to smokers and counselling follow-ups were provided for those with an excessive alcohol intake.
Less resource-intensive strategies have also been tested, limited to dietary and exercise advice with other risk factors managed by the treating electrophysiologist or a registered nurse with input from a dietitian. The outcomes of these studies are shown in Table 2. For example, the PENN AF Care study was managed by a registered nurse, supported by a cardiac electrophysiologist and tested intermittent fasting and counselling with a dietitian to achieve more than 5% body weight loss from baseline over 6–12 months.61,65,66 The focus of the study was on obesity and OSA, although records were made of the participants’ diet, alcohol and tobacco consumption and physical activity.65 In a variation of this more focused approach, dietitians prepared personalised meal plans to reduce daily calorie intake and participants were asked to perform moderate intensity exercise (150 min/week).61 However, this approach has not been tested in larger randomised controlled studies.
Drug Therapy for Weight Loss and Ablation: the Future?
Recent studies have led to the approval of glucagon-like peptide 1 analogues/receptor agonists (GLP-1/RAs) for use as an adjunct to weight loss. GLP-1RAs mimic the function of the natural hormones called incretins that slow gastric emptying, delay absorption of food, increase satiety, inhibit the release of glucagon and stimulate insulin production. On average, those who take GLP-1RAs lose weight from 0.64–6.5 kg over a 1-year period.67 The first approved GLP-1RAs, such as exenatide and liraglutide, require once or twice-daily administration and were followed by longer-acting versions, such as dulaglutide, exenatide once weekly, semaglutide and tirzepatide (a glucose-dependent insulinotropic polypeptide receptor and GLP-1 receptor co-agonist), which are suitable for once-weekly administration (Supplementary Table 4).
This group of drugs, however, exert pleiotropic effects that make them attractive for short-term use to improve outcomes of ablation in obese patients. However, a recent animal study using swine suggests GLP-1RAs have a direct chronotropic effect on the heart via a calcium signalling response.68 Indirect benefits include not only weight loss and improved diabetic control but also improved blood pressure control, for example, liraglutide achieved a greater reduction in systolic blood pressure (-4.6 versus -1.5 mmHg; p=0.002) and reduction in HbA1C(-0.22 versus -0.06%; p=0.0001) than orlistat.69
Mechanistic studies suggest benefits that go beyond an impact on weight loss. For example, a randomised, double-blind placebo-controlled phase IV trial of liraglutide found a preferential reduction of the visceral adipose tissue over 40 weeks (mean difference -10.86%; 95% CI [-6.97–-14.75]; p<0.001) compared to placebo.70 Additionally, liraglutide preferentially lowered EpAT thickness with a treatment duration as early as 3 months in diabetic patients, an effect also seen with semaglutide.71-73 As discussed earlier, this is important in AF due to the reduction in paracrine and endocrine effects of this EpAT and visceral adipose tissue that increase inflammation. An anti-inflammatory effect of these drugs is supported by studies that found lower proinflammatory markers such as TNF-α (-1.33 versus 0.00 pg/ml), IL-6 (-0.78 versus +0.04 pg/ml), and high-sensitivity C-reactive protein (1.55 versus 0.46 µg/ml; p<0.05) in patients treated with liraglutide over 12 weeks.74 Furthermore, the slow progression of fibrosis was reported in patients with non-alcoholic fatty liver disease treated with liraglutide compared with placebo, therefore further studies are needed to investigate GLP-1Ras’ effect on human atria, especially on anti-fibrosis.75 Although the major cardiovascular risk reduction effect is observed in patients without diabetes treated with GLP-1RAs reported in a recent meta-analysis of 10 randomised controlled trials, few studies confirm or refute its benefit on patients with AF.76 These widespread positive effects raise the possibility that short-duration therapy may improve outcomes of AF ablation in association with risk factor management programmes.
Importance of Weight Loss Regardless of Ablation
As obesity is also an upstream risk factors for other morbidities such as hypertension, diabetes and obstructive sleep apnoea, reduction in weight can optimise the outcomes from these conditions. Hypertension is a well-recognised risk factor (RR 1.5; 95% CI [1.42–1.58]) in the development of AF in a recent systematic review of 56 cohort studies.77 A similar effect was reported in patients with diabetes (RR 1.39; 95% CI [1.1–1.75]; p=0.000) in another meta-analysis.78 OSA also promotes the risk of AF (RR 1.7; 95% CI [1.53–1.89]) as highlighted in a recent meta-analysis.57 Therefore, weight loss for conditions can in turn lower the risk of AF and its progression.
Weight management can also deliver fewer AF episodes, symptoms and a lower burden at 1 year.79 This seems to have a long-term effect of up to 5 years if maintained weight loss without fluctuation with the potential reversal of AF phenotype (persistent to paroxysmal, paroxysmal to sinus rhythm).63,80,81 A weight reduction strategy, therefore, can be considered as a preventive approach for AF progression even before ablation.
Conclusion
Obesity without other associated risk factors is an independent risk factor in AF. The success of catheter ablation is substantially decreased by obesity. The importance of weight management including RFM is highlighted in recently published international guidelines. This review discussed the available evidence that pre-ablation weight loss for at least 3–6 months and weight maintenance post-ablation is crucial for better outcomes from ablation. Moreover, changes in cardiac investigations can potentially be useful to monitor the progress and regress of weight management when selecting an appropriate ablation candidate. Further studies on RFM using newer adjunct therapies might shift the paradigm for the management of obese AF patients in the future.
Clinical Perspective
Pre-ablation weight loss of at least 5–10% from baseline over 3–6 months appears crucial for improved ablation outcomes in obese AF patients.
Conventional imaging techniques have not proven to be reliable in assessing left atrial substrate prior to ablation.
Short-term use of GLP-1 receptor agonists show promise in improving ablation outcomes, potentially through rapid visceral fat reduction, and anti-inflammatory and pleiotropic effects.
Maintaining weight loss within one unit of BMI after ablation appears important for long-term arrhythmia-free survival in patients with obesity.
Structured risk factor management programmes, including dietary interventions and exercise, may enhance patient selection and ablation success rates in patients with obesity.
Supplementary Material
Acknowledgments
RPS and MK contributed equally to this work.
References
- 1.Benjamin EJ, Muntner P, Alonso A et al. Heart disease and stroke statistics — 2019 update: a report from the American Heart Association. Circulation. 2019;139:e56–e528. doi: 10.1161/CIR.0000000000000659. [DOI] [PubMed] [Google Scholar]
- 2.Chugh SS, Havmoeller R, Narayanan K et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129:837–47. doi: 10.1161/CIRCULATIONAHA.113.005119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hindricks G, Potpara T, Dagres N et al. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2020;42:373–498. doi: 10.1093/eurheartj/ehaa612. [DOI] [PubMed] [Google Scholar]
- 4.Colilla S, Crow A, Petkun W et al. Estimates of current and future incidence and prevalence of atrial fibrillation in the US adult population. Am J Cardiol. 2013;112:1142–7. doi: 10.1016/j.amjcard.2013.05.063. [DOI] [PubMed] [Google Scholar]
- 5.Kim MH, Johnston SS, Chu B-C et al. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011;4:313–20. doi: 10.1161/CIRCOUTCOMES.110.958165. [DOI] [PubMed] [Google Scholar]
- 6.Benjamin EJ, Wolf PA, D’Agostino RB et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. doi: 10.1161/01.cir.98.10.946. [DOI] [PubMed] [Google Scholar]
- 7.NCD Risk Factor Collaboration (NCD-RisC) Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387:1377–96. doi: 10.1016/S0140-6736(16)30054-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eurostat. Overweight and obesity – BMI statistics. 2024. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Overweight_and_obesity_-_BMI_statistics (accessed 7 October 2024)
- 9.Hales CM, Carroll MD, Fryar CD Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief. 2020. pp. 1–8. [PubMed]
- 10.Joglar JA, Chung MK, Armbruster AL ACC/AHA/ACCP/ HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/ American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2023. pp. 109–279. [DOI] [PMC free article] [PubMed]
- 11.Van Gelder IC, Rienstra M, Bunting KV et al. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45:3314–414. doi: 10.1093/eurheartj/ehae176. [DOI] [PubMed] [Google Scholar]
- 12.Nyström PK, Carlsson AC, Leander K et al. Obesity, metabolic syndrome and risk of atrial fibrillation: a Swedish, prospective cohort study. PLoS One. 2015;10:e0127111. doi: 10.1371/journal.pone.0127111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lee H, Choi EK, Lee SH et al. Atrial fibrillation risk in metabolically healthy obesity: a nationwide populationbased study. Int J Cardiol. 2017;240:221–7. doi: 10.1016/j.ijcard.2017.03.103. [DOI] [PubMed] [Google Scholar]
- 14.Feng T, Vegard M, Strand LB et al. Metabolically healthy obesity and risk for atrial fibrillation: the HUNT study. Obesity (Silver Spring) 2019;27:332–8. doi: 10.1002/oby.22377. [DOI] [PubMed] [Google Scholar]
- 15.Haïssaguerre M, Jaïs P, Shah DC et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–66. doi: 10.1056/NEJM199809033391003. [DOI] [PubMed] [Google Scholar]
- 16.Sasson Z, Rasooly Y, Gupta R, Rasooly I. Left atrial enlargement in healthy obese: prevalence and relation to left ventricular mass and diastolic function. Can J Cardiol. 1996;12:257–63. [PubMed] [Google Scholar]
- 17.Movahed MR, Saito Y. Obesity is associated with left atrial enlargement, E/A reversal and left ventricular hypertrophy. Exp Clin Cardiol. 2008;13:89–91. [PMC free article] [PubMed] [Google Scholar]
- 18.Stritzke J, Markus MRP, Duderstadt S et al. The aging process of the heart: obesity is the main risk factor for left atrial enlargement during aging the Monica/KORA (monitoring of trends and determinations in cardiovascular disease/cooperative research in the region of Augsburg) study. J Am Coll Cardiol. 2009;54:1982–9. doi: 10.1016/j.jacc.2009.07.034. [DOI] [PubMed] [Google Scholar]
- 19.Fernandes-Cardoso A, Santos-Furtado M, Grindler J et al. Epicardial fat thickness correlates with P-wave duration, left atrial size and decreased left ventricular systolic function in morbid obesity. Nutr Metab Cardiovasc Dis. 2017;27:731–8. doi: 10.1016/j.numecd.2017.05.009. [DOI] [PubMed] [Google Scholar]
- 20.Cichoń M, Wieczorek J, Wybraniec M et al. Left atrial function in obese and non-obese patients undergoing percutaneous pulmonary vein isolation. Heart Vessels. 2019;34:343–51. doi: 10.1007/s00380-018-1243-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chirinos JA, Sardana M, Satija V et al. Effect of obesity on left atrial strain in persons aged 35–55 years (the Asklepios study). Am J Cardiol. 2019;123:854–61. doi: 10.1016/j.amjcard.2018.11.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pascual M, Pascual DA, Soria F et al. Effects of isolated obesity on systolic and diastolic left ventricular function. Heart. 2003;89:1152–6. doi: 10.1136/heart.89.10.1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ku CS, Lin SL, Wang DJ et al. Left ventricular filling in young normotensive obese adults. Am J Cardiol. 1994;73:613–5. doi: 10.1016/0002-9149(94)90347-6. [DOI] [PubMed] [Google Scholar]
- 24.Herszkowicz N, Barbato A, Salvi W et al. Contribution of Doppler echocardiography to the evaluation of systolic and diastolic function of obese women versus a control group. Arq Bras Cardiol. 2001;76:189–96. doi: 10.1590/s0066-782x2001000300002. [DOI] [PubMed] [Google Scholar]
- 25.Tanalp AC, Bitigen A, Cevik C et al. The role of tissue Doppler study in the assessment of left ventricular dysfunction in obesity. Acta Cardiol. 2008;63:541–6. doi: 10.2143/AC.63.5.2033218. [DOI] [PubMed] [Google Scholar]
- 26.Yaseen RI, Ahmed MK, Hamed WA. Assessment of abnormal LV myocardial deformation properties in obese patients by 2D based strain and strain rate imaging. Egypt Heart J. 2015;67:183–91. doi: 10.1016/j.ehj.2014.04.005. [DOI] [Google Scholar]
- 27.Wong C, Marwick TH. Obesity cardiomyopathy: pathogenesis and pathophysiology. Nat Clin Pract Cardiovasc Med. 2007;4:436–43. doi: 10.1038/ncpcardio0943. [DOI] [PubMed] [Google Scholar]
- 28.Cuspidi C, Rescaldani M, Sala C, Grassi G. Left-ventricular hypertrophy and obesity: a systematic review and metaanalysis of echocardiographic studies. J Hypertens. 2014;32:16–25. doi: 10.1097/HJH.0b013e328364fb58. [DOI] [PubMed] [Google Scholar]
- 29.Sacks HS, Fain JN. Human epicardial adipose tissue: a review. Am Heart J. 2007;153:907–17. doi: 10.1016/j.ahj.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 30.Iacobellis G, Corradi D, Sharma AM. Epicardial adipose tissue: anatomic, biomolecular and clinical relationships with the heart. Nat Clin Pract Cardiovasc Med. 2005;2:536–43. doi: 10.1038/ncpcardio0319. [DOI] [PubMed] [Google Scholar]
- 31.Iacobellis G, Willens HJ, Barbaro G, Sharma AM. Threshold values of high-risk echocardiographic epicardial fat thickness. Obesity (Silver Spring) 2008;16:887–92. doi: 10.1038/oby.2008.6. [DOI] [PubMed] [Google Scholar]
- 32.Alexopoulos N, McLean DS, Janik M et al. Epicardial adipose tissue and coronary artery plaque characteristics. Atherosclerosis. 2010;210:150–4. doi: 10.1016/j.atherosclerosis.2009.11.020. [DOI] [PubMed] [Google Scholar]
- 33.Wong CX, Sun MT, Odutayo A et al. Associations of epicardial, abdominal, and overall adiposity with atrial fibrillation. Circ Arrhythm Electrophysiol. 2016;9:e004378. doi: 10.1161/CIRCEP.116.004378. [DOI] [PubMed] [Google Scholar]
- 34.Wong CX, Abed HS, Molaee P et al. Pericardial fat is associated with atrial fibrillation severity and ablation outcome. J Am Coll Cardiol. 2011;57:1745–51. doi: 10.1016/j.jacc.2010.11.045. [DOI] [PubMed] [Google Scholar]
- 35.Bertaso AG, Bertol D, Duncan BB, Foppa M. Epicardial fat: definition, measurements and systematic review of main outcomes. Arq Bras Cardiol. 2013;101:e18–28. doi: 10.5935/abc.20130138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wong CX, Ganesan AN, Selvanayagam JB. Epicardial fat and atrial fibrillation: current evidence, potential mechanisms, clinical implications, and future directions. Eur Heart J. 2017;38:1294–302. doi: 10.1093/eurheartj/ehw045. [DOI] [PubMed] [Google Scholar]
- 37.Douglass E, Greif S, Frishman WH. Epicardial fat: pathophysiology and clinical significance. Cardiol Rev. 2017;25:230–5. doi: 10.1097/CRD.0000000000000153. [DOI] [PubMed] [Google Scholar]
- 38.Mahajan R, Kuklik P, Grover S et al. Cardiovascular magnetic resonance of total and atrial pericardial adipose tissue: a validation study and development of a 3 dimensional pericardial adipose tissue model. J Cardiovasc Magn Reson. 2013;15:73. doi: 10.1186/1532-429X-15-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Vach M, Luetkens JA, Faron A et al. Association between single-slice and whole heart measurements of epicardial and pericardial fat in cardiac MRI. Acta Radiol. 2023;64:2229–37. doi: 10.1177/02841851211054192. [DOI] [PubMed] [Google Scholar]
- 40.Golukhova EZ, Bulaeva NI, Alexandrova SA et al. Quantification of epicardial adipose tissue by computed tomographic scanning as a prognostic criterion of atrial fibrillation recurrence after catheter ablation. Kardiologiia. 2023;63:3–10. doi: 10.18087/cardio.2023.8.n2168. [DOI] [PubMed] [Google Scholar]
- 41.Mazurek T, Zhang L, Zalewski A et al. Human epicardial adipose tissue is a source of inflammatory mediators. Circulation. 2003;108:2460–6. doi: 10.1161/01.CIR.0000099542.57313.C5. [DOI] [PubMed] [Google Scholar]
- 42.Fain JN, Sacks HS, Bahouth SW et al. Human epicardial adipokine messenger RNAs: comparisons of their expression in substernal, subcutaneous, and omental fat. Metabolism. 2010;59:1379–86. doi: 10.1016/j.metabol.2009.12.027. [DOI] [PubMed] [Google Scholar]
- 43.Vyas V, Blythe H, Wood EG et al. Obesity and diabetes are major risk factors for epicardial adipose tissue inflammation. JCI Insight. 2021;6:e145495. doi: 10.1172/jci.insight.145495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Venteclef N, Guglielmi V, Balse E et al. Human epicardial adipose tissue induces fibrosis of the atrial myocardium through the secretion of adipo-fibrokines. Eur Heart J. 2015;36:795–805a. doi: 10.1093/eurheartj/eht099. [DOI] [PubMed] [Google Scholar]
- 45.Wang Q, Xi W, Yin L et al. Human epicardial adipose tissue cTGF expression is an independent risk factor for atrial fibrillation and highly associated with atrial fibrosis. Sci Rep. 2018;8:3585. doi: 10.1038/s41598-018-21911-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Nalliah CJ, Bell JR, Raaijmakers AJA et al. Epicardial adipose tissue accumulation confers atrial conduction abnormality. J Am Coll Cardiol. 2020;76:1197–211. doi: 10.1016/j.jacc.2020.07.017. [DOI] [PubMed] [Google Scholar]
- 47.Ernault AC, Meijborg VMF, Coronel R. Modulation of cardiac arrhythmogenesis by epicardial adipose tissue: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021;78:1730–45. doi: 10.1016/j.jacc.2021.08.037. [DOI] [PubMed] [Google Scholar]
- 48.Ernault AC, Verkerk AO, Bayer JD et al. The secretome of atrial epicardial adipose tissue facilitates reentrant arrhythmias by myocardial remodeling. Heart Rhythm. 2022;19:1461–70. doi: 10.1016/j.hrthm.2022.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Abed HS, Samuel CS, Lau DH et al. Obesity results in progressive atrial structural and electrical remodeling: implications for atrial fibrillation. Heart Rhythm. 2013;10:90–100. doi: 10.1016/j.hrthm.2012.08.043. [DOI] [PubMed] [Google Scholar]
- 50.Mahajan R, Lau DH, Brooks AG et al. Electrophysiological, electroanatomical, and structural remodeling of the atria as consequences of sustained obesity. J Am Coll Cardiol. 2015;66:1–11. doi: 10.1016/j.jacc.2015.04.058. [DOI] [PubMed] [Google Scholar]
- 51.Munger TM, Dong YX, Masaki M et al. Electrophysiological and hemodynamic characteristics associated with obesity in patients with atrial fibrillation. J Am Coll Cardiol. 2012;60:851–60. doi: 10.1016/j.jacc.2012.03.042. [DOI] [PubMed] [Google Scholar]
- 52.Mahajan R, Lau DH, Brooks AG et al. Atrial fibrillation and obesity: reverse remodeling of atrial substrate with weight reduction. JACC Clin Electrophysiol. 2021;7:630–41. doi: 10.1016/j.jacep.2020.11.015. [DOI] [PubMed] [Google Scholar]
- 53.Liu F, Song T, Hu Q et al. Body mass index and atrial fibrillation recurrence post ablation: a systematic review and dose-response meta-analysis. Front Cardiovasc Med. 2022;9:999845. doi: 10.3389/fcvm.2022.999845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ding WY, Yang PS, Jang E et al. Impact of abdominal obesity on outcomes of catheter ablation in Korean patients with atrial fibrillation. Int J Clin Pract. 2021;75:e14696. doi: 10.1111/ijcp.14696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Weinmann K, Bothner C, Rattka M et al. Pulmonary vein isolation with the cryoballoon in obese atrial fibrillation patients – Does weight have an impact on procedural parameters and clinical outcome? Int J Cardiol. 2020;316:137–42. doi: 10.1016/j.ijcard.2020.06.001. [DOI] [PubMed] [Google Scholar]
- 56.Malaspina D, Brasca F, Iacopino S et al. Cryoablation for pulmonary veins isolation in obese patients with atrial fibrillation compared to nonobese patients. Pacing Clin Electrophysiol. 2021;44:306–17. doi: 10.1111/pace.14149. [DOI] [PubMed] [Google Scholar]
- 57.Zhao H, Li X, Yu P et al. Association between weight loss and outcomes in patients undergoing atrial fibrillation ablation: a systematic review and dose-response metaanalysis. Nutr Metab (Lond) 2023;20:5. doi: 10.1186/s12986-023-00724-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Akhtar KH, Jafry AH, Beard C et al. The effect of weight loss on recurrence of atrial fibrillation after catheter ablation: a systematic review and meta-analysis. J Cardiovasc Electrophysiol. 2023;34:2514–26. doi: 10.1111/jce.16090. [DOI] [PubMed] [Google Scholar]
- 59.Jia ZX, Jiang C, Lu SX et al. Association between weight control and recurrence of atrial fibrillation after catheter ablation in overweight and obese patients [in Chinese]. Zhonghua Xin Xue Guan Bing Za Zhi. 2019;47:595–601. doi: 10.3760/cma.j.issn.0253-3758.2019.08.002. [DOI] [PubMed] [Google Scholar]
- 60.Gessler N, Willems S, Steven D et al. Supervised Obesity Reduction Trial for AF ablation patients: results from the SORT-AF trial. Europace. 2021;23:1548–58. doi: 10.1093/europace/euab122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Mohanty S, Mohanty P, Natale V et al. Impact of weight loss on ablation outcome in obese patients with longstanding persistent atrial fibrillation. J Cardiovasc Electrophysiol. 2018;29:246–53. doi: 10.1111/jce.13394. [DOI] [PubMed] [Google Scholar]
- 62.Goldberger JJ, Mitrani RD, Baez-García C et al. Pre-ablation weight loss as a predictor of atrial fibrillation ablation outcome in the Liraglutide Effect on Atrial Fibrillation (LEAF) Study. Heart Rhythm. 2023;20:1079. doi: 10.1016/j.hrthm.2023.04.029. [DOI] [Google Scholar]
- 63.Pathak RK, Middeldorp ME, Meredith M et al. Long-term effect of goal-directed weight management in an atrial fibrillation cohort: a long-term follow-up study (LEGACY). J Am Coll Cardiol. 2015;65:2159–69. doi: 10.1016/j.jacc.2015.03.002. [DOI] [PubMed] [Google Scholar]
- 64.Pathak RK, Middeldorp ME, Lau DH et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. 2014;64:2222–31. doi: 10.1016/j.jacc.2014.09.028. [DOI] [PubMed] [Google Scholar]
- 65.Yaeger A, Keenan BT, Cash NR et al. Impact of a nurse-led limited risk factor modification program on arrhythmia outcomes in patients with atrial fibrillation undergoing catheter ablation. J Cardiovasc Electrophysiol. 2020;31:423–31. doi: 10.1111/jce.14336. [DOI] [PubMed] [Google Scholar]
- 66.Yew Ding W, Kozhuharov N. Hao Chin S et al. Feasibility of weight loss in obese atrial fibrillation patients attending a specialist arrhythmia clinic and its impact on ablation outcomes. J Arrhythm. 2020;36:984–90. doi: 10.1002/joa3.12432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Brown E, Heerspink HJL, Cuthbertson DJ, Wilding JPH. SGLT2 inhibitors and GLP-1 receptor agonists: established and emerging indications. Lancet. 2021;398:262–76. doi: 10.1016/S0140-6736(21)00536-5. [DOI] [PubMed] [Google Scholar]
- 68.Lubberding AF, Veedfald S, Achter JS et al. GLP-1 increases heart rate by a direct action on the sinus node. Cardiovasc Res. 2024;120:1427–41. doi: 10.1093/cvr/cvae120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Astrup A, Carraro R, Finer N et al. Safety, tolerability and sustained weight loss over 2 years with the once-daily human GLP-1 analog, liraglutide. Int J Obes (Lond) 2012;36:843–54. doi: 10.1038/ijo.2011.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Neeland IJ, Marso SP, Ayers CR et al. Effects of liraglutide on visceral and ectopic fat in adults with overweight and obesity at high cardiovascular risk: a randomised, doubleblind, placebo-controlled, clinical trial. Lancet Diabetes Endocrinol. 2021;9:595–605. doi: 10.1016/S2213-8587(21)00179-0. [DOI] [PubMed] [Google Scholar]
- 71.Iacobellis G, Mohseni M, Bianco SD, Banga PK. Liraglutide causes large and rapid epicardial fat reduction. Obesity (Silver Spring) 2017;25:311–6. doi: 10.1002/oby.21718. [DOI] [PubMed] [Google Scholar]
- 72.Zhao N, Wang X, Wang Y et al. The effect of liraglutide on epicardial adipose tissue in type 2 diabetes. J Diabetes Res. 2021;2021:5578216. doi: 10.1155/2021/5578216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Iacobellis G, Villasante Fricke AC. Effects of semaglutide versus dulaglutide on epicardial fat thickness in subjects with type 2 diabetes and obesity. J Endocr Soc. 2020;4:bvz042. doi: 10.1210/jendso/bvz042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Armstrong MJ, Hull D, Guo K et al. Glucagon-like peptide 1 decreases lipotoxicity in non-alcoholic steatohepatitis. J Hepatol. 2016;64:399–408. doi: 10.1016/j.jhep.2015.08.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Armstrong MJ, Gaunt P, Aithal GP et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet. 2016;387:679–90. doi: 10.1016/S0140-6736(15)00803-X. [DOI] [PubMed] [Google Scholar]
- 76.Singh S, Garg A, Tantry US et al. Safety and efficacy of glucagon-like peptide-1 receptor agonists on cardiovascular events in overweight or obese non-diabetic patients. Curr Probl Cardiol. 2024;49:102403. doi: 10.1016/j.cpcardiol.2024.102403. [DOI] [PubMed] [Google Scholar]
- 77.Aune D, Mahamat-Saleh Y, Kobeissi E et al. Blood pressure, hypertension and the risk of atrial fibrillation: a systematic review and meta-analysis of cohort studies. Eur J Epidemiol. 2023;38:145–78. doi: 10.1007/s10654-022-00914-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Huxley RR, Filion KB, Konety S, Alonso A. Meta-analysis of cohort and case–control studies of type 2 diabetes mellitus and risk of atrial fibrillation. Am J Cardiol. 2011;108:56–62. doi: 10.1016/j.amjcard.2011.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Abed HS, Wittert GA, Leong DP et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310:2050–60. doi: 10.1001/jama.2013.280521. [DOI] [PubMed] [Google Scholar]
- 80.Middeldorp ME, Pathak RK, Meredith M et al. PREVEntion and regReSsive Effect of weight-loss and risk factor modification on Atrial Fibrillation: the REVERSE-AF study. Europace. 2018;20:1929–35. doi: 10.1093/europace/euy117. [DOI] [PubMed] [Google Scholar]
- 81.Al-Kaisey AM, Kalman JM. Obesity and atrial fibrillation: epidemiology, pathogenesis and effect of weight loss. Arrhythm Electrophysiol Rev. 2021;10:159–64. doi: 10.15420/aer.2021.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.