

Abstract
Cirsoid aneurysms, a subtype of arteriovenous fistulas (AVF), of the scalp are rare pathological lesions characterized by abnormal fistulous connections between superficial arteries and draining veins without intervening capillary beds. We present a case report of a cirsoid aneurysm located on the scalp, treated at our tertiary care center using percutaneous endovascular intervention with injection embolics. This report highlights the challenges posed by complex vascular anatomy and high shunt flow in the treatment of such lesions involving the head and neck. We discuss the rationale for selecting the treatment approach, emphasizing the importance of a patient-specific strategy to achieve successful obliteration of the abnormal vascular connections. Our experience underscores the efficacy of transarterial and/or transvenous embolization using appropriate embolic materials in the management of cirsoid aneurysms. This case report contributes to the existing literature on treatment options for scalp AVFs, providing insights into optimizing outcomes in these rare but clinically significant lesions.
Keywords: Cirsoid aneurysm, Arteriovenous fistula, Endovascular embolization
Introduction
Cirsoid aneurysms, also known as arteriovenous fistulas (AVFs) of the scalp, are rare vascular abnormalities characterized by abnormal connections between superficial arteries and veins, bypassing the capillary bed [1,2]. These lesions may be congenital or acquired, with trauma being a frequent trigger, leading to high-flow vascular shunts within the scalp [3].
The superficial temporal and occipital arteries are the most commonly implicated feeders in cirsoid aneurysms due to their superficial and prolonged courses, although any scalp vessel may be involved. Clinically, these aneurysms present as pulsatile, progressively enlarging scalp masses, often accompanied by headache, tinnitus, and intermittent bleeding [[4], [5], [6]].
Diagnosis relies on imaging modalities such as computed tomography angiography (CTA) or diagnostic cerebral angiography, although physical examination often provides the initial clue [2,7]. However, due to the rarity of these lesions and the paucity of case reports in the literature, there are no established protocols for their investigation, diagnosis, or management. This lack of standardized approaches often results in misdiagnosis and suboptimal treatment, particularly when lesions are managed as straightforward excisions without preoperative embolization [8,9].
We present the case of a 24-year-old man with a superior tarsal cirsoid aneurysm who was successfully treated with percutaneous endovascular embolization. This case highlights the importance of accurate diagnosis, multidisciplinary collaboration, and tailored endovascular strategies in managing these complex vascular anomalies, while also contributing to the broader understanding of their diagnosis and treatment.
Case presentation
A 24-year-old male presented with a pulsatile mass above the right supraorbital region. The patient reported a prior history of trauma with ecchymosis of the right eyelid 2 years earlier but denied visual disturbances. Physical examination revealed a 2 cm fluctuant, pulsatile mass above the right eyelid with a normal ophthalmological examination.
Noncontrast computed tomography of the head revealed a 1.8 cm hyperdense supraorbital mass without evidence of calvarial fracture, acute hemorrhage, or significant mass effect. A subsequent contrast-enhanced maxillofacial CT further delineated a high-flow vascular lesion with a nidus in the right supraorbital region (Fig. 1). Cerebral angiography confirmed a 2.6 × 2.5 × 2.4 cm early filling venous structure with arterialized blood shunting in the superior tarsal region, supplied by branches of the right middle meningeal artery, internal maxillary artery, and superficial temporal artery, with venous drainage through the supratrochlear and angular veins into the external jugular system (Fig. 2).
Fig. 1.

Contrast-enhanced CT of the head at the level of the orbits demonstrates a large, avidly enhancing vascular malformation along the right temporal scalp, with a nidus in the right supraorbital region.
Fig. 2.
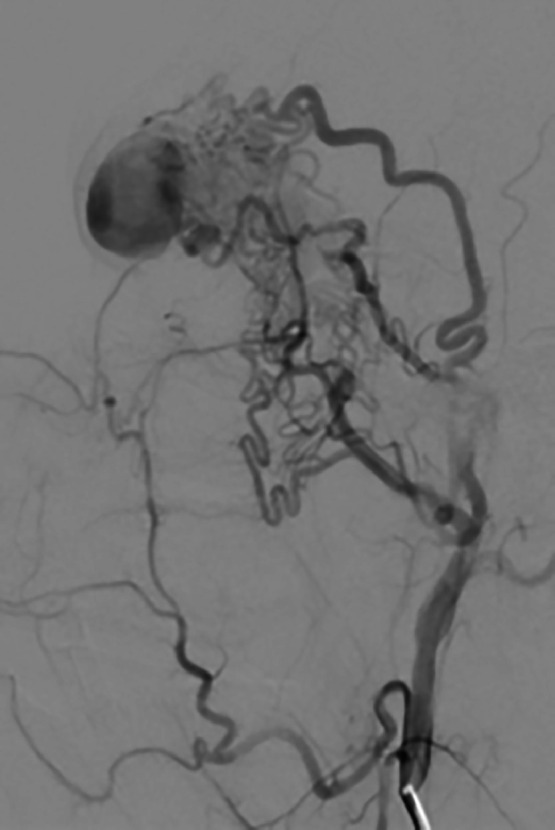
Subselective lateral angiogram of the internal maxillary artery shows vascular supply to the right supraorbital cirsoid malformation, draining into multiple venous territories.
Given the risk of progressive enlargement and potential complications, a multidisciplinary neuro interventional team opted for percutaneous endovascular embolization. Under fluoroscopic guidance, arterial access was established via the right common femoral artery. Angiographic evaluation of the right external carotid artery demonstrated early venous shunting. A 3-dimensional dynamic CT with right external carotid injection confirmed the arteriovenous fistula’s arterial feeders and venous drainage pattern (Fig. 3). Embolization was performed in a stepwise manner using a Scepter XC balloon microcatheter system (MicroVention, Inc., California, USA), delivering Onyx 34 liquid embolic agent (Medtronic, Inc., Minnesota, USA) into the feeding branches of the middle meningeal and superficial temporal arteries. The distal access catheter was positioned in the proximal orbital segment, and Onyx 34 was injected with the balloon inflated, leading to embolization of the draining vein (Fig. 4). Postembolization angiography confirmed occlusion of the pseudoaneurysm from the middle meningeal artery. Persistent supply from the middle deep temporal and superior palatal arteries was identified. Due to vessel tortuosity, selective catheterization of the middle deep temporal artery was unsuccessful, so Gelfoam slurry (Pfizer, Inc., New York, USA) was deployed to reduce shunting. A Concerto 3 × 8 mm coil (Medtronic, Inc., Minnesota, USA) was placed to protect the lateral branch of the superficial temporal artery before final embolization with Onyx 34. Postprocedural angiography confirmed complete occlusion of the AVF with no residual shunting (Fig. 5).
Fig. 3.

3D rotational angiogram demonstrates right periorbital arteriovenous fistula (A). Lateral projection right external carotid artery angiogram demonstrates multiple feeders to the fistula pouch from the right superficial temporal artery (B).
Fig. 4.

Lateral projection angiogram through the Scepter XC balloon catheter demonstrates supply to the fistula from the right superficial temporal artery branch that is catheterized (A). Lateral projection right superficial temporal artery angiogram through a distal access catheter demonstrates supply to the fistula from the superficial temporal artery frontal branches (B). Lateral projection right superficial temporal artery angiogram through a DAC catheter demonstrates occlusion of supply to the fistula from the superficial temporal artery frontal branches with onyx cast (C).
Fig. 5.
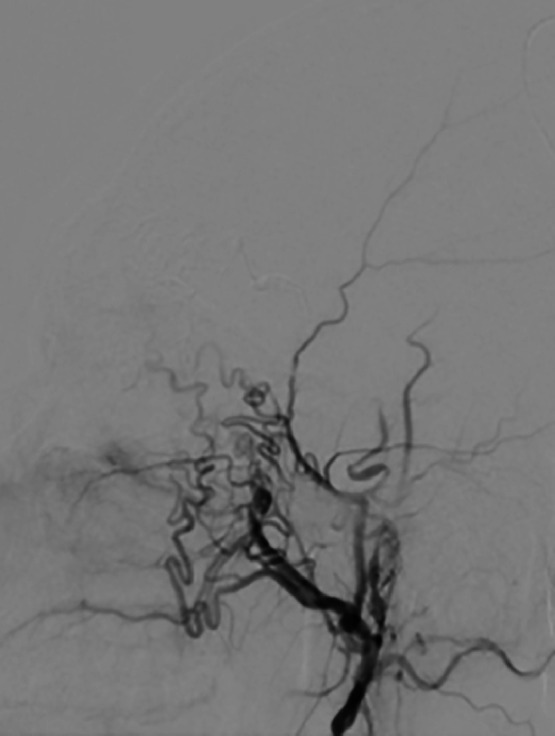
Lateral angiogram of the internal maxillary artery postembolization demonstrates nonvisualization of the cirsoid malformation, consistent with complete embolization.
One-week postprocedure, angiography confirmed complete AVF occlusion with no residual filling. Color Doppler ultrasound demonstrated no discernible flow within the lesion. The patient remained asymptomatic and was discharged with instructions for routine monitoring. Subsequently, the patient underwent cirsoid resection (Fig. 6).
Fig. 6.

Intraoperative image following embolization shows a large bulbar mass that was completely excised with minimal bleeding.
Discussion
The management of cirsoid aneurysms presents a challenge due to their complex vascular architecture and high-flow dynamics. These lesions are characterized by the presence of an AVF, which creates a direct high-flow shunt of arterial blood into the venous system. This abnormal communication leads to progressive dilatation, thickening, and tortuosity of the affected veins.
Clinically, cirsoid aneurysms are often confused with low-flow vascular malformations such as hemangiomas, cavernomas, and sinus pericranii. Misdiagnosis can lead to inappropriate treatment, such as attempted excision without preoperative embolization, resulting in uncontrollable hemorrhage, incomplete resection, and recurrence [[10], [11], [12]].
Catheter angiography remains the gold standard for diagnosing cirsoid aneurysms, as it provides detailed visualization of the vascular anatomy, identifies feeding arteries and draining veins, and excludes intracranial involvement. This modality also offers the added benefit of enabling endovascular treatment at the time of diagnosis. Complementary imaging techniques, such as CTA, magnetic resonance imaging and magnetic resonance angiography, further aid in preoperative planning by delineating the relationship of the lesion to surrounding structures [[13], [14], [15]].
Surgical excision has been the most common method of managing cirsoid aneurysms. However, this approach carries a significant risk of uncontrollable perioperative hemorrhage, particularly when performed without preoperative embolization [5,8].
Endovascular embolization is a widely utilized treatment approach, with arterial embolization and venous occlusion being the 2 primary techniques. The objective of intervention, regardless of the approach, is to eliminate the arteriovenous communication and prevent recurrence [2,16].
Arterial embolization remains the most common approach due to its ability to selectively target feeding arteries, effectively reducing arterial inflow. This technique employs various embolic agents, including liquid embolics (e.g., Onyx 34), coils, and vascular plugs, to achieve precise occlusion of the vascular anomaly [17]. Conversely, venous occlusion is preferred when arterial inflow is relatively simple, permitting direct closure of the venous outflow and immediate cessation of the fistula. Although venous embolization is considered safer due to a lower risk of nontarget embolization, studies suggest that a combination of arterial and venous approaches results in superior outcomes [2,17].
The success of endovascular treatment depends on meticulous procedural planning and the careful selection of embolic agents. In this case, the use of Onyx 34, Gelfoam slurry, and coils allowed for durable occlusion of the lesion while minimizing complications. Future advancements in embolic technology and imaging guidance will continue to refine treatment strategies for these complex vascular lesions, optimizing both safety and efficacy.
Conclusion
The management of cirsoid aneurysms requires a multidisciplinary approach, with accurate diagnosis and tailored treatment strategies being paramount to achieving successful outcomes. Endovascular embolization, particularly with the use of liquid embolics and adjunctive materials, has proven to be a safe and effective treatment modality. This case highlights the importance of integrating advanced imaging techniques and endovascular interventions in the management of complex vascular lesions, contributing to the broader understanding of their diagnosis and treatment.
Patient consent
Informed written consent was obtained from the patients.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Consent for publication was obtained for every individual person’s data included in the study.
Footnotes
Competing Interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments: This study did not receive any funds.
References
- 1.Tiwary S.K., Khanna R., Khanna AK. Craniofacial cirsoid aneurysm: 2-stage treatment. J Oral Maxillofac Surg. 2007;65(3):523–525. doi: 10.1016/j.joms.2005.10.066. [DOI] [PubMed] [Google Scholar]
- 2.Sofela A., Osunronbi T., Hettige S. Scalp Cirsoid Aneurysms: case illustration and systematic review of literature. Neurosurgery. 2020;86(2):E98–e107. doi: 10.1093/neuros/nyz303. [DOI] [PubMed] [Google Scholar]
- 3.Tauro L.F., Suhith G., Shetty P., Rao D. Cirsoid aneurysm of scalp. J Neurosci Rural Pract. 2012;3(1):95–96. doi: 10.4103/0976-3147.91976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shenoy S.N., Raja A. Scalp arteriovenous malformations. Neurol India. 2004;52(4):478–481. [PubMed] [Google Scholar]
- 5.Visser A., FitzJohn T., Tan S.T. Surgical management of arteriovenous malformation. J Plast Reconstr Aesthet Surg. 2011;64(3):283–291. doi: 10.1016/j.bjps.2010.05.033. [DOI] [PubMed] [Google Scholar]
- 6.Richter G.T., Suen JY. Pediatric extracranial arteriovenous malformations. Curr Opin Otolaryngol Head Neck Surg. 2011;19(6):455–461. doi: 10.1097/MOO.0b013e32834cd57c. [DOI] [PubMed] [Google Scholar]
- 7.Goel V., Verma A.K., Singh S., Puri SK. Cirsoid aneurysm of scalp: demonstration on CT angiography (CTA) BMJ Case Rep. 2013;2013 doi: 10.1136/bcr-2013-202459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Karki M., Roka YB. Surgical excision of Cirsoid aneurysm of the scalp: case series and review of the literature. World Neurosurg. 2021;155:e600–e6e4. doi: 10.1016/j.wneu.2021.08.102. [DOI] [PubMed] [Google Scholar]
- 9.Albuquerque Sousa L.H., Maranha Gatto L.A., Demartini Junior Z., Koppe G.L. Scalp Cirsoid Aneurysm: an updated systematic literature review and an illustrative case report. World Neurosurg. 2018;119:416–427. doi: 10.1016/j.wneu.2018.08.098. [DOI] [PubMed] [Google Scholar]
- 10.Gupta R., Kayal A. Scalp arteriovenous malformations in young. J Pediatr Neurosci. 2014;9(3):263–266. doi: 10.4103/1817-1745.147587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hasturk A.E., Erten F., Ayata T. Giant non-traumatic arteriovenous malformation of the scalp. Asian J Neurosurg. 2012;7(1):39–41. doi: 10.4103/1793-5482.95698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chowdhury F.H., Haque M.R., Kawsar K.A., Sarker M.H., Momtazul Haque A.F. Surgical management of scalp arterio-venous malformation and scalp venous malformation: an experience of eleven cases. Indian J Plast Surg. 2013;46(1):98–107. doi: 10.4103/0970-0358.113723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Senoglu M., Yasim A., Gokce M., Senoglu N. Nontraumatic scalp arteriovenous fistula in an adult: technical report on an illustrative case. Surg Neurol. 2008;70(2):194–197. doi: 10.1016/j.surneu.2007.04.018. [DOI] [PubMed] [Google Scholar]
- 14.MO Fard, Yousofnejad O., Heydari M. Traumatic arteriovenous malformation of the superficial temporal artery. Adv Biomed Res. 2017;6:82. doi: 10.4103/2277-9175.210663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Worm P.V., Ruschel L.G., Roxo M.R., Camelo R. Giant scalp arteriovenous malformation. Rev Assoc Med Bras (1992) 2016;62(9):828–830. doi: 10.1590/1806-9282.62.09.828. [DOI] [PubMed] [Google Scholar]
- 16.Albuquerque Sousa L.H., Maranha Gatto L.A., Demartini Junior Z., Koppe G.L. Scalp Cirsoid Aneurysm: an updated systematic literature review and an illustrative case report. World Neurosurg. 2018;119:416–427. doi: 10.1016/j.wneu.2018.08.098. [DOI] [PubMed] [Google Scholar]
- 17.Gupta A.K., Purkayastha S., Bodhey N.K., Kapilamoorthy T.R., Krishnamoorthy T., Kesavadas C., et al. Endovascular treatment of scalp cirsoid aneurysms. Neurol India. 2008;56(2):167–172. doi: 10.4103/0028-3886.41995. [DOI] [PubMed] [Google Scholar]