

Abstract
Background
Thyroid eye disease is an autoimmune inflammatory condition of the orbital and periorbital tissues. Orbital radiotherapy is an anti‐inflammatory treatment used in the treatment of active thyroid eye disease. It is administered as an outpatient procedure in 10 to 12 fractionated doses.
Objectives
To assess the effectiveness and adverse events of orbital radiotherapy in thyroid eye disease. The effectiveness was dependent on the level of 'success' of the intervention predefined in each randomised controlled trial (RCT).
Search methods
We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2012, Issue 2), MEDLINE (January 1950 to March 2012), EMBASE (January 1980 to March 2012), Latin American and Caribbean Literature on Health Sciences (LILACS) (January 1982 to March 2012), the metaRegister of Controlled Trials (mRCT) (www.controlled‐trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not restrict the electronic searches for trials by date or language. We last searched the electronic databases on 12 March 2012. We screened reference lists of reports of included studies, other reviews and book chapters to find additional trials. We contacted trial investigators and experts in the field to identify additionally published studies.
Selection criteria
We included RCTs of orbital radiotherapy versus sham radiotherapy or other interventions enrolling adults, with a minimum of three months' follow‐up and an endpoint of two years or less post treatment.
Data collection and analysis
Two review authors independently assessed trial quality and extracted data. Trial authors were contacted for missing data. The risk ratio was used for our primary outcome. For our secondary outcomes, the odds ratio and mean difference were reported where possible.
Main results
We obtained full‐text copies of nine potential studies and included five trials with a total of 244 participants in this review. Orbital radiotherapy was compared to sham radiotherapy in two studies and to glucocorticoids in three studies, as a monotherapy or combination therapy. There was heterogeneity (as defined in our protocol) of trial outcome measures. Our primary outcome of a composite score was used in the two trials comparing radiotherapy versus sham radiotherapy and showed a risk ratio of success of 1.92 (95% confidence interval (CI) 1.27 to 2.91) in favour of orbital radiotherapy. The primary outcome was not used in the other three trials.
Authors' conclusions
This review found that orbital radiotherapy is more effective than sham radiotherapy for the treatment of mild‐to‐moderate thyroid eye disease. In a single trial no difference between radiotherapy and steroid monotherapy was found. A meta‐analysis of our secondary outcome of disease severity was not possible but results from individual trials suggest a better outcome with combination treatment with steroids versus steroids alone. No significant changes in quality‐of‐life scores following treatment with radiotherapy versus alternative treatments were found. Short‐term adverse events related to radiotherapy that were reported were local and mild but long‐term data were lacking and development of retinal changes following radiotherapy was not reported on.
Keywords: Adult, Female, Humans, Male, Anti‐Inflammatory Agents, Anti‐Inflammatory Agents/therapeutic use, Graves Ophthalmopathy, Graves Ophthalmopathy/drug therapy, Graves Ophthalmopathy/radiotherapy, Methylprednisolone, Methylprednisolone/therapeutic use, Prednisolone, Prednisolone/therapeutic use, Quality of Life, Randomized Controlled Trials as Topic, Steroids, Steroids/therapeutic use
Plain language summary
Orbital therapy for adult thyroid eye disease
Thyroid eye disease is a condition that is still not fully understood but results in inflammation of the eye and the tissues around the eye. It can cause changes in appearance (such as puffiness and redness of eyelids and conjunctiva, 'starey' eyes and misaligned eyes), discomfort, double vision and decreased vision. Orbital radiotherapy is a treatment given to reduce the inflammation and its associated changes. It is given in an outpatient setting and as the dose is divided into smaller daily doses it often involves up to 12 visits. This review included five randomised controlled trials involving 244 participants. A combined analysis of trials using our primary outcome showed that the 'risk' of success in a patient who received radiotherapy was 1.92 times that of a patient who did not receive radiotherapy. Single studies suggested that orbital radiotherapy in combination with steroids had a better outcome than steroids alone. There was no significant change in quality‐of‐life information collected in the orbital radiotherapy groups compared to the other groups. The short‐term adverse events reported in the trials were mild and localised to the area of treatment (redness of skin and temporal hair loss). However, trial methodology may have led to a decreased rate of adverse events from radiotherapy. Three trials excluded diabetic patients and these patients have been reported, in the literature, to be at higher risk of developing radiation retinopathy and of having progression of pre‐existing diabetic retinopathy. Some studies did not report on retinal changes at all.
Background
Description of the condition
Thyroid eye disease (TED) affects 25% to 50% of patients with Graves' disease (Bahn 1993), which is approximately 400,000 people in the UK (Cawood 2004). Clinically, it is characterised by an aching sensation behind the eyes, swelling and redness of the eyelids and conjunctiva, protrusion of the eyes (proptosis) and double vision. In a small minority (6%) of patients vision is also threatened by compression of the optic nerve (Bartalena 2000). TED is therefore a visually disabling and cosmetically disfiguring condition that significantly impairs quality of life (Terwee 2002).
The cellular and molecular basis remains incompletely understood and it has long been postulated that the common link between Graves' disease and TED is a misdirected immune response targeting the thyroid‐stimulating hormone receptor (TSHr), although insulin‐like growth factor receptor 1 (IGFR1) has also been shown to play a role (Smith 2003). There is an increasing amount of basic research being carried out on TED and the intricacies of disease mechanism are continuing to unfold. We will provide a simplified summary for the purpose of this systematic review. B cells and T cells, which are part of the body's immune system, respond to an autoimmune signal and migrate to the orbit. This signal is presumably multifactorial and is likely to be due to both environmental and genetic risk factors (Stan 2010). It results in T‐cell driven inflammation and B cells are also stimulated to produce autoantibodies against the TSHr and IGFR1 (Lehmann 2007), which are expressed on orbital fibroblasts (Bahn 2010). The result is the release of further cytokines and chemokines that perpetuate the proinflammatory immune response. Fibroblasts also secrete glycosaminoglycans (Smith 2004), which as well as being hydrophilic, have subclasses that can differentiate into myofibrocytes (muscle fibre precursors) and adipocytes (fat cells) (Van Steensel 2010). Clinically, these changes are manifest as extraocular muscle enlargement and an increase in the volume of orbital fat, which is readily demonstrated on magnetic resonance imaging (MRI) and computed tomography (CT) scans. The globe is pushed forwards, if the surrounding anatomy allows it to be, which is seen as proptosis. If the globe is prevented from this 'self decompression' a vicious cycle of orbital congestion arises as venous outflow is obstructed by rising intraorbital pressure (Bahn 2010).
The initial active phase of TED is typically followed, after one to three years, by an inactive 'burnt out' phase during which fibrosis and scarring of the orbital contents occurs (Rundle 1945). Hence, there is an early window of opportunity to modify the natural history of the disease by suppressing the immune response, and corticosteroids have been used to treat TED for over 40 years with response rates of 63% to 77% (Bartalena 2000). Additional immunomodulatory therapies may also be used in some centres, but there is little evidence regarding their efficacy.
A key challenge in the management of TED is reliably differentiating between active and 'burnt out' disease (EUGOGO 2006b), and the diagnostic classification most commonly used for this purpose is the clinical activity score (CAS), which has an 80% positive‐predictive value for the outcome of immunosuppressive treatment (Mourits 1997). In addition, there are multiple grading systems for classifying disease severity (EUGOGO 2006a) based on cumulative functional and anatomical measures (Perros 1993; Prummel 1989; Werner 1977), and composite scores, which grade the success or failure of interventions using a defined number of criteria, are also commonly used in the evaluation of treatments for active TED (Marcocci 2001; Mourits 2000; Prummel 2004). Once the disease has 'burnt out', residual abnormalities are managed surgically with operations to reduce proptosis (orbital decompression), minimise diplopia (strabismus surgery) and correct the position and appearance of the eyelids. Surgery is used in the active phase in sight‐threatening conditions that are not responding to medical therapy such as optic neuropathy or corneal ulceration/perforation.
Description of the intervention
Orbital radiotherapy has been used to treat TED for over 60 years (Bartalena 2000). Treatment is administered on an outpatient basis, typically involving 10 to 12 visits over a 2‐ to 2.5‐week period. The dose given is traditionally 20 Gy divided in 2 Gy fractions (Marquez 2001) but some centres do use lower doses. Great care is taken to ensure that exposure is limited to the orbits. In some centres a plastic face shell is made for each patient to ensure that their position does not change between treatment sessions.
How the intervention might work
Radiotherapy is thought to reduce inflammation by preventing the replication of lymphocytes through disruption of their DNA. At the low doses used in the treatment of TED it may also specifically downregulate orbital macrophage activation (Hildebrandt 1998). In addition, radiotherapy reduces the production of water‐attracting molecules (glycosaminoglycans), which are overexpressed in TED and therefore helps to counteract orbital fluid retention and consequently tissue swelling is reduced (Kahaly 1988).
Why it is important to do this review
There is great controversy about the benefits of radiotherapy for TED (Bartalena 2004; Feldon 2001). The evidence for its use is largely based on retrospective and uncontrolled studies, which suggest that 60% of patients have a positive response (Bartalena 2000), but it is difficult to ascertain whether this is a direct result of treatment or simply a reflection of expected clinical improvement in the regressive phase of the disease. The few available randomised controlled trials (RCTs) are of varying quality and have reported conflicting results (Gorman 2001; Mourits 2000; Prummel 1993; Prummel 2004). Consequently, clinical practice varies widely across the UK, Europe (EUGOGO 2006b) and in the USA. This is widely acknowledged in the literature, but an international study has not been carried out. The National Institute for Health and Clinical Excellence (NICE) have produced guidelines for the use of orbital radiotherapy in TED and have only recommended its use where other treatments have failed or have caused significant side effects (NICE guidelines 2005). A systematic review is required to raise the standard of information available to both patients and healthcare professionals.
Objectives
To review current evidence from RCTs for the effectiveness and short‐term adverse events of orbital radiotherapy in adult TED when compared to sham radiotherapy, other interventions and glucocorticoids.
Methods
Criteria for considering studies for this review
Types of studies
We included RCTs with a minimum of three months follow‐up and an endpoint of two years or less post treatment. Paired and unpaired studies were analysed separately.
Types of participants
We included adults (aged 18 years old or above) with clinically diagnosed TED.
Types of interventions
We included:
orbital radiotherapy of any dose and duration versus sham radiotherapy
orbital radiotherapy of any dose and duration versus other interventions
orbital radiotherapy combined with glucocorticoids versus glucocorticoids alone
Types of outcome measures
Primary outcomes
We considered primary outcomes at a minimum of three months and a maximum of two years post treatment.
Composite Outcome Score (Marcocci 2001; Mourits 2000; Prummel 2004) ‐ ordinal score.
Composite scores grade clinical success or failure using a defined number of criteria (see Table 1). Success and failure were defined by the individual trials as composite scores are heterogeneous. Our outcome was the proportion of successes compared to the proportion of non‐responders and treatment failures.
1. Composite outcome score criteria.
| Criteria |
| Major criterion |
| †Changes in the maximum eye movement in specified directions (measured in degrees, ≥ 8 degrees) |
| †Change in Gorman diplopia score (none ‐ no double vision, intermittent ‐ double vision when tired or reported but not evident, inconstant ‐ double vision in certain directions of gaze, constant ‐ double vision in primary position or requiring a prism) |
| †Change in visual acuity (Snellen acuity or converted Snellen acuity) |
| Minor criterion |
| †Change in soft tissue inflammation (predefined change in the appearance of the eyelids, conjunctiva, caruncle (which is the pink tissue in the medial corner of the eye), or a combination graded mild (1), moderate (2) or severe (3) according to a standardised colour atlas (Dickinson 2001) or eyelid swelling alone (none, mild, moderate, severe) |
| †Change of palpebral/lid aperture (distance between upper and lower eyelid at the point midway across the pupil) of > 2 mm |
| †Change in proptosis (protrusion of eyeball) of > 2 mm |
| Change in CAS |
| Subjective improvement (predefined grading) |
| †Used in more than 1 study |
Mourits 2000
Prummel 2004
|
CAS: clinical activity score
Secondary outcomes
We considered secondary outcomes at a minimum of three months and a maximum of two years post treatment.
Number of post‐treatment rehabilitative surgical procedures to correct functional disability (e.g. eyelid operations to reduce exposure of the cornea, squint operations for double vision, orbital decompression operations to reduce the proptosis)
Disease Severity Score ‐ total eye score (see Table 2) (Prummel 1989) ‐ a continuous score
2. Modified NOSPECS and total eye score (TES).
| NOSPECS class | Criteria | TES equivalent |
| Class 0 | No signs or symptoms | 0 |
| Class 1 | Only signs (lid retraction, lid lag) | 1 |
| Class 2 | Soft tissue involvement | |
| Grade 0: absent | 0 | |
| Grade a: minimal | 2 | |
| Grade b: moderate | 4 | |
| Grade c: marked | 6 | |
| Class 3 | Proptosis | |
| Grade 0: < 20 mm (original score < 23 mm) |
0 | |
| Grade a: 20 to 21 mm (original score 23 to 24 mm) |
3 | |
| Grade b: 21.5 to 24 mm (original score 25 to 27 mm) |
6 | |
| Grade c: > 24 mm (original score > 28 mm) |
9 | |
| Class 4 | Eye muscle involvement | |
| Grade 0: absent | 0 | |
| Grade a: limitation in extremes | 4 | |
| Grade b: evident restriction of movement | 8 | |
| Grade c: fixation of globes | 12 | |
| Class 5 | Corneal involvement | |
| Grade 0: absent | 0 | |
| Grade a: stippling/staining of cornea with fluorescein drops | 5 | |
| Grade b: ulceration of cornea | 10 | |
| Grade c: clouding, necrosis, perforation of cornea | 15 | |
| Class 6 | Sight loss (Snellen acuity stated in American units) | |
| Class 0: better than 20/30 | 0 | |
| Class a: 20/30 to 20/60 | 6 | |
| Class b: 20/60 to 20/200 | 12 | |
| Class c: worse than 20/200 | 18 | |
| Individual class values added together to give total eye score |
(NOSPECS score, an ordinal score, (Werner 1977) or Ophthalmopathy index, a continuous score (Perros 1993), if total eye score not present), which assess how severe the changes due to TED are (see Table 2; Table 3).
3. Ophthalmopathy index.
| Involvement | Criteria | Score |
| Soft tissue involvement | Mild | 1 |
| Moderate | 2 | |
| Severe | 3 | |
| Proptosis (in mm) | 16 | 0.2 |
| 17 | 0.4 | |
| 18 | 0.6 | |
| 19 | 0.8 | |
| 20 | 1.0 | |
| 21 | 2.0 | |
| 22 | 3.0 | |
| > 23 | 4.0 | |
| Palpebral aperture (distance between upper and lower eyelids at mid‐pupil point) (in mm) | 8 | 0.15 |
| 9 | 0.45 | |
| 10 | 0.75 | |
| 11 | 1.05 | |
| 12 | 1.35 | |
| 13 | 1.65 | |
| 14 | 1.95 | |
| 15 | 2.25 | |
| 16 | 2.55 | |
| 17 | 2.85 | |
| 18 | 3 | |
| Difference between intraocular pressure looking straight ahead and that in upgaze | 1 | 0.1 |
| 2 | 0.2 | |
| 3 | 0.3 | |
| 4 | 0.4 | |
| 5 | 0.5 | |
| 6 | 0.6 | |
| 7 | 0.7 | |
| 8 | 0.8 | |
| 9 | 0.9 | |
| 10 | 1.0 | |
| Diplopia (double vision) (grades defined in composite score table) |
Intermittent | 1 |
| Inconstant | 2 | |
| Constant | 3 | |
| Corneal involvement | Initial lesions | 1 |
| Ulcers | 2 | |
| Clouding/perforation | 3 | |
| Optic neuropathy (optic nerve damage) | ||
| Abnormal visual evoked potential detected when vision better than 6/12 | 3 | |
| (Snellen visual acuity expressed as fraction (e.g. 6/12 = 0.5)) | 0.5 to 0.9 | 5 |
| 0.1 to 0.4 | 7 | |
| < 0.1 | 9 |
Disease Activity Score ‐ CAS (Mourits 1989), a continuous score that assesses how active the disease is (see Table 4).
4. Clinical activity score.
| Criteria | (Each score 1 point) |
| Pain | Pain on eye movement in the last 4 weeks |
| Painful, oppressive feeling on or behind eye globe in the last 4 weeks | |
| Redness | Conjunctival redness |
| Eyelid redness | |
| Swelling | Chemosis (fluid under conjunctiva) |
| Swollen caruncle (pink tissue in medial corner of eye next to nose) | |
| Eyelid oedema | |
| Increasing proptosis of > 2 mm during a period of 1 to 3 months | |
| Impaired function | Decreasing visual acuity of > 1 Snellen line (using a pinhole to obtain best corrected visual acuity) during a period of 1 to 3 months |
| Decreasing eye movement of greater than or equal to 5 degrees during a period of 1 to 3 months |
Adverse outcomes
Adverse events (e.g. reaction to trial medication, effect on patient's liver function or full blood count, development of secondary ocular or non‐ocular disorders such as cataracts, retinopathy, head and neck malignancy in particular lymphoma)
Study withdrawal due to intolerance of study intervention
Economic data
We summarised the direct and indirect costs of rehabilitative interventions such as surgery and medical treatments and any other economic data in the included studies.
Quality‐of‐life data
Quality‐of‐life measurement (a continuous score) was summarised using validated questionnaires available from individual studies (Terwee 2001).
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) 2012, Issue 2, part of The Cochrane Library. www.thecochranelibrary.com (accessed 12 March 2012), MEDLINE (January 1950 to March 2012), EMBASE (January 1980 to March 2012), Latin American and Caribbean Literature on Health Sciences (LILACS) (January 1982 to March 2012), the metaRegister of Controlled Trials (mRCT) (www.controlled‐trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not restrict the search for trials by language or date. We last searched the electronic databases on 12 March 2012.
See: Appendices for details of search strategies for CENTRAL (Appendix 1), MEDLINE (Appendix 2), EMBASE (Appendix 3), LILACS (Appendix 4), mRCT (Appendix 5), ClinicalTrials.gov (Appendix 6) and the ICTRP (Appendix 7).
Searching other resources
We searched the reference lists of reports of included studies, other reviews and book chapters to find references to additional trials. We contacted trial investigators and experts in the field to identify additionally published and unpublished studies.
Data collection and analysis
Selection of studies
Two review authors independently assessed the titles and abstracts of all reports identified by the searches. RR and SM worked independently to screen the titles and abstracts that resulted from the searches. Each report was labelled as (a) definitely exclude, (b) unsure or (c) definitely include. The full texts of abstracts labelled as 'unsure' were reassessed according to the inclusion criteria for this review. Differences between the two review authors' assessments were resolved through discussion or by involving a third person to adjudicate. Studies labelled as 'definitely exclude' were excluded from the review and those labelled as 'definitely include' were assessed for methodological quality. Trial authors were contacted for clarification where necessary. Attempts were made to obtain further information about any trial that had been published only as an abstract. If a full report was not available, the abstract was excluded at this stage.
Data extraction and management
RR and SM worked independently to extract the following information from the trial reports and entered the data into RevMan (Review Manager 2011):
details of participants: age, gender, setting, number in each group, comparability at baseline
details of interventions: dosage, schedule, comparison group
outcomes: primary and secondary outcomes, adverse effects
other information: funding
primary and secondary outcome data. If reports used different methods for assessing outcomes, the method described most often was selected for analysis and all other measurements were converted where possible
Assessment of risk of bias in included studies
As per guidance given in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) we examined the following different types of biases: selection, performance, detection and attrition by assessing randomisation, concealment of allocation and blinding (masking).
Two review authors working independently assessed trial quality as follows:
1. The method that was used to generate the random sequence within the trials was graded as follows:
(A) low risk: computer random number generator, random number table, shuffled cards or envelopes
(B) unclear: not stated in report
(C) high risk: no sequence or alternation, case record numbers, dates of birth, days of the week
Any trial graded as (C) on randomisation was excluded.
2. Allocation concealment: the mechanism of implementing the randomisation schedule was graded as follows:
(A) low risk: centralized randomisation by central office or pharmacy, sequential administration of pre‐numbered or coded containers to enrolled participants, on‐site computer system (provided that the computer file containing the assignments is locked), serially numbered sealed opaque envelopes, other approaches that appear to offer adequate concealment, combined with the statement that the person who generated the allocation did not administer it
(B) unclear: list, table or envelopes used but no qualifying statement, an apparently adequate concealment but other information in the report suggests that concealment may not have been adequate
(C) high risk: any allocation that is entirely transparent before allocation.
3. Blinding (masking)
We assessed masking of participants, providers of care and outcome assessment (for each outcome). Each of these were graded:
(A) low risk
(B) unclear
(C) high risk
4. Incomplete outcome data assessed
We documented missing outcome data and exclusions from the analysis. Trials were graded according to whether the analysis was intention‐to‐treat (ITT) as follows:
(A) low risk: ITT done
(B) unclear
(C) high risk: ITT not done
We were not masked to trial results or publication details during the quality assessment. Disagreements between review authors were documented and discussed. Study authors were contacted for clarification on any item scored 'unclear', or where there was disagreement between authors on the grading.
Measures of treatment effect
Our primary outcome measure was success defined by a composite outcome score. We used risk ratios (RRs) as our measure of treatment effect. Information on secondary outcomes was only collated.
Unit of analysis issues
Studies using both eyes of participants were analysed separately to those where a single eye had been studied and compared to the other eye. As TED is a systemic condition and treatment has an effect systemically, those trials using observation of one eye compared to the other in the same individual are likely to find differing results to those comparing one participant with another acting as a control (the radiotherapy could have had an effect on the control eye both by direct low‐dose unintentional radiation of the contralateral orbit and by the radiotherapy acting on lymphocytes that could circulate to the other orbit).
Composite scores, disease activity and disease severity were assessed on highest scoring eye. Quality of life, economic data and adverse events were assessed on the individual.
Dealing with missing data
Where possible investigators were contacted if there were missing data. Any missing data that was unobtainable were assumed to be 'missing at random'.
Assessment of heterogeneity
We assessed for heterogeneity between studies by careful review of papers to identify important methodological differences that might lead to methodological heterogeneity. If the studies appeared similar, we assessed consistency between them by examination of the I2 statistic. If the I2 statistic was less than 50% and no clinical heterogeneity had been determined we performed a meta‐analysis where studies had collected data on the primary endpoint.
Assessment of reporting biases
We aimed to investigate the potential influence of publication bias by examining funnel plots, but as there were insufficient eligible trials this could not be done.
Data synthesis
We used the individual trial's predefined success and failure and compared the proportion of patients/eyes who improved to those that remained the same or worsened. The RRs for dichotomous data model were used when meta‐analyzing the data. In general we used the random‐effects model unless there were fewer than three trials when the fixed‐effect model was used.
Subgroup analysis and investigation of heterogeneity
If the studies were inconsistent in how they assessed their outcomes or if heterogeneity was detected we did not pool the data but instead presented a narrative review. Heterogeneity of all forms was assessed as indicated in the 'Assessment of heterogeneity' section.
Sensitivity analysis
We conducted sensitivity analyses to assess the robustness of results when we: 1. excluded studies of lower methodological quality (scoring C (high risk) on randomisation) 2. excluded unpublished studies
Results
Description of studies
Results of the search
The electronic searches yielded a total of 567 reports of studies (Figure 1). After deduplication the Trials Search Co‐ordinator scanned 401 records and discarded 249 records because they were not relevant to the scope of the review. We screened the title and abstracts of the remaining 152 references. Of these records 22 were in Spanish, one author (SM) reviewed the Spanish abstracts and we excluded all of these abstracts as none met the inclusion criteria. Of the remaining 130 abstracts we excluded 17 as they were review papers. We reviewed the remaining reports and 15 abstracts related to RCTs comparing radiotherapy to sham treatment or to another intervention were potentially eligible for inclusion. We excluded trials comparing different dosing regimens of radiotherapy as they did not meet our inclusion criteria. Of the 15 eligible abstracts, one was a comment on a randomised trial and five were duplicate reports, leaving nine studies for detailed review. We obtained the full papers for these and two review authors (RR and SM) reviewed them independently. Any discrepancies were discussed between the two review authors, and a third review author (CB) was consulted if they were not resolved. At this stage, we excluded four further studies; one that used adjuvant steroids in the radiotherapy arm of the study only (Antonelli 1992), and one that used the patient's untreated eye as the control arm with subsequent cross‐over treatment (Gorman 2001). In the latter, the radiotherapy could have had an effect on the control eye both by direct low‐dose unintentional radiation of the contralateral orbit and by the radiotherapy acting on lymphocytes, which could circulate to the other orbit and have had an effect on the control eye and, as such, the controls were not suitably independent. One study (Sterker 2009) was excluded as it was a retrospective study. Another study (Li 2008) stated that participants were randomly divided into treatment groups. We contacted the trialists for further details but were informed that the study was not an RCT.
1.

Results from searching for studies for inclusion in the review.
This left five trials that met the inclusion criteria. The characteristics of these studies and the quality of the studies are described below.
Included studies
See the 'Characteristics of included studies' table for further details.
Participants
The five included RCTs randomised a total of 244 participants (sample size range 16 to 88). Of these 199 were female. The mean age in the radiotherapy group ranged from 42 to 64 years old, and from 45 to 49 years old in the comparison group. The number of smokers was not reported in the earliest two studies (Bartalena 1983; Prummel 1993), but ranged from 31.2% to 66.7% in the latter three (Mourits 2000; Ng 2005; Prummel 2004). Treatment of TED prior to the study was an exclusion criterion in four out of the five studies and was not reported on in one study (Bartalena 1983). Treated patients had moderately severe TED in four studies and mild TED in one study. Presence of optic neuropathy was an exclusion criterion in three studies (Prummel 1993; Prummel 2004; Mourits 2000) and was only included in one study if the patient refused surgery or surgery was contraindicated (Ng 2005). In the earliest study (Bartalena 1983) the inclusion of participants with optic neuropathy was not specified but in the data given two patients in the radiotherapy group had sight loss from optic nerve involvement and none of the control group did.
Types of interventions
Orbital radiotherapy was compared to sham treatment in two studies (Mourits 2000; Prummel 2004) and compared to glucocorticoid treatment in three studies (Bartalena 1983; Ng 2005; Prummel 1993). Two of these studies involved glucocorticoid administration to the radiotherapy arm of the study as well as the control (Bartalena 1983; Ng 2005).
Types of outcome measures
Two studies used a composite outcome score (Mourits 2000; Prummel 2004) and two used the NOSPECS and total eye scores (Ng 2005; Prummel 1993). The ophthalmopathy score was only used in one study (Bartalena 1983). The CAS was described in 1997 and therefore not used in the earlier two studies (Bartalena 1983; Prummel 1993). However, two later studies did use CAS as an outcome (Mourits 2000; Prummel 2004). Only one study used the Graves Ophthalmopathy ‐ Quality of Life questionnaire (Prummel 2004) and three recorded the Subjective Eye Score (Mourits 2000; Ng 2005; Prummel 1993). Health economic data was reported in one trial (Prummel 2004).
Final outcomes were assessed at different time points. Two studies used 24 weeks as the final endpoint (Mourits 2000; Prummel 1993) and two assessed the outcome at one year (Ng 2005; Prummel 2004). The earliest study (Bartalena 1983) did not define a specific time point and instead used the final follow‐up subsequent to discontinuation of steroid. This ranged from 12 to 28 months, with a mean of 19 months, in the randomised combination therapy group, and 18 months in the steroid control group. The treatment itself lasted five to six months making the total follow‐up from the start of treatment range from 17 to 34 months.
Excluded studies
We excluded four studies (Antonelli 1992; Gorman 2001; Li 2008; Sterker 2009) and details can be found in the 'Characteristics of excluded studies' table.
Risk of bias in included studies
Allocation
Random sequence generation
Randomisation was carried out according to lists in two studies (Prummel 1993; Prummel 2004) and random numbers in one study (Bartalena 1983). One study used an external randomisation service (Mourits 2000) but the exact details of how this was carried out were not described. The most recent study (Ng 2005) stated that randomisation was used but did not report how.
Allocation concealment
Allocation concealment was adequate in two studies (Mourits 2000; Prummel 2004) but unclear in the remaining three (Bartalena 1983; Ng 2005; Prummel 1993).
Blinding
Three studies (Mourits 2000; Prummel 1993; Prummel 2004) were double‐masked. The other two were single‐masked with the assessor unaware of treatment allocation (Bartalena 1983; Ng 2005). However, patients were aware of their allocation and this could have led to bias in their reporting of symptoms.
Incomplete outcome data
Bartalena 1983 did not specifically mention dropouts, withdrawals or protocol deviations, but all patients did have an outcome reported. Authors of the steroid versus radiotherapy trial (Prummel 1993) stated that patients without sufficient follow‐up were excluded and replaced. Two studies excluded one patient each who died or withdrew prior to the first postintervention assessment without replacement (Mourits 2000; Ng 2005). An ITT analysis was carried out by two studies, including one of the above (Ng 2005; Prummel 2004), by either including protocol deviations or using the last observation carried forwards (LOCF) principle for participants who did not complete the study. In one study they stated that the LOCF was only used if patients had a minimum of four‐week post baseline data (Ng 2005).
Selective reporting
One study did not have a defined temporal endpoint (Bartalena 1983) and therefore outcome measures were taken 17 to 34 months after the initiation of the intervention, reducing the comparability of results. Another study did not report on adverse events (Prummel 2004), and, despite attempting to obtain this data directly from the study group, we were unable to do so as the first study author was deceased and the study documents destroyed.
Effects of interventions
Orbital radiotherapy versus sham treatment
Two studies compared orbital radiotherapy and sham treatment; one enrolling moderately active TED (Mourits 2000) and one investigating treatment of mild disease (Prummel 2004). Our primary outcome of composite outcome score was used in both, although the major and minor criteria used were not identical. We recorded the number of patients meeting the predefined composite success criteria in both studies, the analysis of which showed an RR of success of 1.92 (95% confidence interval (CI) 1.27 to 2.91; Analysis 1.1) in favour of orbital radiotherapy. Our secondary outcome of number of rehabilitative surgeries was similar in the radiotherapy group (47; Mourits 2000 and 27; Prummel 2004) and the sham treatment group (45; Mourits 2000 and 30; Prummel 2004) for both studies.
1.1. Analysis.
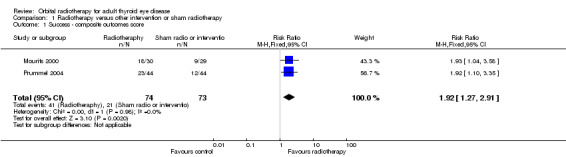
Comparison 1 Radiotherapy versus other intervention or sham radiotherapy, Outcome 1 Success ‐ composite outcomes score.
Prummel 2004 also assessed the change in CAS (our co‐secondary outcome) from baseline to 12 months and found a mean reduction of ‐0.84 (standard deviation (SD) 1.15) in the orbital radiotherapy group and a mean reduction of ‐1.19 (SD 1.53) in the sham group. However, this difference was not significant (0.35; 95% CI ‐0.22 to 0.92).
Orbital radiotherapy versus steroids
Only one study was identified which randomised orbital radiotherapy without steroids to oral prednisolone (Prummel 1993), and, as such, a meta‐analysis was not possible. The study involved patients with moderately severe TED. The primary outcome of composite outcome score was not assessed by this group but secondary outcomes of disease severity and number of rehabilitative surgeries were recorded. An improvement in NOSPECS at 24 weeks was seen in 13 out of 28 patients (46%) in the radiotherapy group and 14 out of 28 (50%) in the oral steroid group. However, this was not significant (odds ratio (OR) 0.87; 95% CI 0.30 to 2.47). The number of rehabilitative operations performed after treatment was similar between the radiotherapy and steroid groups (20 (71%) and 22 (79%), respectively).
Orbital radiotherapy combined with steroids versus steroids alone
Two studies randomised patients to orbital radiotherapy combined with oral steroids versus oral steroids in isolation to explore radiotherapy as a combination treatment as compared to steroids alone (Bartalena 1983; Ng 2005). Both enrolled patients with moderately active TED. As the studies did not use our primary outcome score of a composite outcome score a meta‐analysis could, once again, not be performed. Our secondary outcome of disease severity was recorded for both. However, as only one study reported the total eye score, no meta‐analysis could be performed of this (Ng 2005). In addition, although both studies did use the NOSPECS score, data on the randomised patients could not be separated from that of non‐randomised patients in Bartalena 1983, preventing further comparative analysis.
Bartalena 1983 compared orbital cobalt radiotherapy with methylprednisolone to methylprednisolone alone (n = 24). However, a further 24 non‐randomised patients treated with combined radiotherapy and methylprednisolone were also reported on (total n = 48). We extracted the data on the classification of improvement and initial and final Ophthalmopathy Index on the randomised patients only. This revealed a mean reduction of ‐4.8 (SD 1.5) in the group treated with orbital radiotherapy in combination with intravenous steroids as compared to ‐3.2 (SD 0.94) in the group treated with intravenous steroids alone (P < 0.005 by Student's unpaired two‐tailed t‐test); resulting in a mean difference between the groups of ‐1.60 (95% CI ‐2.60 to ‐0.60). The study group used predefined criteria to measure response, taken from a radiotherapy study carried out between 1968 and 1972 (Donaldson 1973). This was similar to a composite score, using changes in symptoms, signs and functional capacity, but lacking objective definitions. Bartalena et al. found an excellent response in four patients in the combination group but none in the steroid alone group. A good response was reported in six patients in the combination group compared to four in the steroid group. Slight response and no response were seen in two and none of the combination group, respectively, and six and two of the steroid alone group. By comparing an excellent and good response with a slight or no response, using a Chi2 analysis, they found a significance of < 0.01.
Ng 2005 investigated the use of intravenous steroids with and without radiotherapy in a small cohort of 16 patients and reported on 15 of them at 52 weeks (one of the steroid alone group died prior to first assessment from community acquired pneumonia). The mean age of the combination group was higher than those in the intravenous steroid group (64.1 years old versus 48.3 years old). A similar number of patients needed an increase in steroids due to deterioration of total eye score of four or more (3/7 steroid only group (43%), 4/8 combination therapy group (50%)). The improvement in NOSPECS class was greater in the combination group as compared to the control group (7/8 (88%) versus 2/7 (29%) for soft tissue changes, 7/8 (88%) versus 2/7 (29%) for ocular motility and 5/8 (63%) versus 0/7 (0%) for patients showing 'normal eye movement'). The mean change in total eye score was therefore significantly greater in the combination group (‐11.75; 95% CI ‐18.13 to ‐5.37) as opposed to the steroid monotherapy group (‐5.00; 95% CI ‐7.72 to ‐2.28) (P = 0.029).
Adverse events
All but one study reported the adverse events experienced by their study participants (Bartalena 1983; Mourits 2000; Ng 2005; Prummel 1993). These are described in the adverse events table (Analysis 3.1). Almost all of these related to steroid treatment with only three cases of transient redness of the skin and two cases of transient local hair loss reported with radiotherapy. One study, looking at prednisolone versus radiotherapy, commented that their follow‐up was too short for detecting long‐term radiotherapy side effects (Prummel 1993). There were no comments on development of retinopathy. Of the five studies, three excluded patients with diabetes (Mourits 2000; Prummel 1993; Prummel 2004) and one excluded patients with pre‐existing diabetic retinopathy (Ng 2005). Bartalena 1983 did not state that they excluded diabetics and 'retinoscopy' (fundoscopy) was performed as they assessed optic nerve changes. In their report of side effects there was no comment on development of radiation retinopathy or diabetic retinopathy.
3.1. Analysis.
Comparison 3 Adverse events, Outcome 1 Side effects.
| Side effects | |
|---|---|
| Study | |
| Bartalena 1983 | cushingoid features of 'most cases' with methyl pred alone or in combination |
| Bartalena 1983 | 1 depressive pscyhosis (methylprednisolone) |
| Bartalena 1983 | 1 developed diabetic syndrome (methylprednisolone) |
| Bartalena 1983 | 1 moderate increase in intraocular tension (methylprednisolone) |
| Bartalena 1983 | (No cataracts from radiotherapy in the 26 month follow up) |
| Mourits 2000 | 3 radiotherapy group had transient redness of skin |
| Mourits 2000 | 2 radiotherapy group had transient local hair loss |
| Mourits 2000 | |
| Mourits 2000 | |
| Mourits 2000 | |
| Ng 2005 | steroids withdrawn prematurely in 1 of the steroid group due to recurrent Ramsay ‐ Hunt syndrome |
| Ng 2005 | steroids withdrawn early in 1 combination treatment group due to gastric discomfort |
| Ng 2005 | 3 to 4 in each group developed moon face, weight gain, transient leucocytosis , hyperlipidaemia due to steroids |
| Ng 2005 | 2‐3 had hot flushes, gastro‐intestinal upset, hypertension, insomnia, eye or nose infections due to steroids. 1 developed acne due to steroids |
| Ng 2005 | 3 in combined treatment group experienced mild exacerbation of peri‐orbital swelling & transient redness of eyes, 3 had temporal hair loss |
| Prummel 1993 | mean body weight increased from 71 (95% CI 67‐75)kg to 73(68‐78)kg in prednisolone group |
| Prummel 1993 | 1 prednisolone group developed severe depression and 1 developed recurrent herpes zoster |
| Prummel 1993 | 2 prednisolone group developed hypertension; severe pyrosis developed in 5 prednisolone group and 2 radiotherapy group, 2 prednisolone patients developed hirsuitism, 3 prednisolone group developed behavioural changes, weight gain of greater than 2kg in 12 prednisolone group and 3 in radiotherapy group. 14 prednisolone group developed cushingoid face |
| Prummel 1993 | |
| Prummel 1993 | no side effects in 3 prednisolone group and 13 radiotherapy group |
| Prummel 2004 | No comment on side‐effects or adverse events |
| Prummel 2004 | |
| Prummel 2004 | |
| Prummel 2004 | |
| Prummel 2004 | |
Quality‐of‐life assessment
One study did attempt to assess the change in the quality of life using the GO‐QoL (Graves Ophthalmopathy ‐ Quality of Life), Euro‐QoL, SIP (Sickness Impact Profile) and MOS‐24 (Medical Outcomes Study Short‐form General Health Survey) questionnaires (Prummel 2004). They were unable to assess the first 23 of their 88 patients and, in the remaining patients, the response rate at baseline was 92% and that at 12 months was 85%. As they had incomplete data on 42% of patients their quality‐of‐life assessment lacked power for further analysis. However, there was no obvious difference in quality of life between those treated with radiotherapy and those who received sham radiotherapy. The subjective eye score recorded in one study comparing radiotherapy to steroids (Prummel 1993), and one comparing combination radiotherapy/steroid treatment to steroids alone (Ng 2005) was slightly higher in the control arm (1.3 versus 1.2, 1 versus 0.8). However, this was not significant.
Health economic analysis
Only one study (Prummel 2004) reviewed the cost of management of mild TED with radiotherapy treatment and without. Their estimated costs of radiotherapy and follow‐up care during the first year after such treatment were Euros 5007 per person for radiotherapy and Euros 4465 per person for sham.
Discussion
Summary of main results
This Cochrane review has demonstrated that there is great heterogeneity of outcome measures used in TED treatment trials. This has prevented a meta‐analysis using data from all of the identified studies. Only two studies could be combined, both investigating radiotherapy versus sham treatment in mild‐to‐moderate thyroid‐associated orbitopathy (Mourits 2000; Prummel 2004). The proportion of patients reaching predefined success criteria as defined by the composite outcome score was found to favour treatment with radiotherapy in this setting (RR 1.92; 95% CI 1.27 to 2.91). However, the proportion of rehabilitative procedures necessary was similar between the two groups. The only included RCT comparing radiotherapy to oral prednisolone, also in mild‐to‐moderate patients, did not demonstrate a difference between disease progression or the number of rehabilitative procedures required by patients, in the two groups, suggesting that radiotherapy was as effective as steroid monotherapy.
Two studies compared treatment with radiotherapy plus steroids versus steroids alone (Bartalena 1983; Ng 2005). Although these studies could not be combined due to differences in outcome measures, the number of patients who improved in NOSPECS, Ophthalmopathy index or total eye score was greater in the combination therapy group than the steroid monotherapy group in both cases. This difference was found to be statistically significant in one study. Although one of these studies did enrol two patients with severe sight‐threatening disease (Bartalena 1983), this was insufficient to comment on the effect of radiotherapy on this subgroup.
The effect on quality of life was difficult to assess. Validated questionnaires were used in one study (Prummel 2004) and due to poor response they did not have sufficient power for analysis. Review of the scores did not reveal an obvious trend in quality‐of‐life difference between the two groups. Costs of treatment were only assessed in one study, which showed that in mild disease the cost of radiotherapy was 12% greater than sham treatment.
Adverse events were common but mild, and were almost always attributable to the steroids involved in the trials. Radiotherapy was found to have local short‐term adverse events such as transient loss of hair or redness. The only two systemic short‐term adverse events reported with radiotherapy (weight gain and leukocytosis) were seen in both the treatment and control arms of the studies involved, suggesting that they may not have been directly related to the radiotherapy. Development of retinopathy was not reported on in any of the five studies. Four studies excluded diabetic patients or those with pre‐existing diabetic retinopathy and this may have affected the incidence of retinal changes. The follow‐up of these studies was too short to confirm or dispute the theoretical risk of induction of malignancies with radiotherapy.
In summary, this review has found that orbital radiotherapy is more effective than sham radiotherapy for the treatment of mild‐to‐moderate TED and that a difference between radiotherapy and steroid monotherapy was not found in any single trial. One of our secondary outcomes of disease severity (total eye score, NOSPECS score and Ophthalmopathy index) also suggested a better outcome of combination treatment with steroids versus steroids alone, although a large meta‐analysis looking at this aspect was not possible. However, significant changes in quality‐of‐life scores following treatment with radiotherapy versus alternative treatments were not found. Short‐term adverse events related to radiotherapy were local and mild supporting its safe use although long‐term data are lacking and the development of retinal changes was not reported on.
Overall completeness and applicability of evidence
The studies described above relate to patients with mild or moderate TED. Patients with severe TED, including those with optic neuropathy, were excluded in three trials (Mourits 2000; Prummel 1993; Prummel 2004) and included in Ng 2005 if the patient refused surgery or surgery was contraindicated. The study that included all TED severities only had two patients with optic neuropathy, both of which were in the combination‐treatment group (Bartalena 1983).
Adverse events were documented in four of five studies. Although most of the effects relating to radiotherapy were infrequent, local and mild, the numbers involved in these studies were insufficient to comment on the risks of radiotherapy accurately. Furthermore, many of the reported effects of radiotherapy are long‐term and would not necessarily have been appreciated during the two‐year study period. As such, this review fails to inform about rare but significant complications of orbital radiotherapy adequately.
The issue of long‐term side effects of orbital radiotherapy has been addressed in four studies involving a total of 597 participants (Gorman 2002; Marcocci 2003; Marquez 2001; Wakelkamp 2004). Of these studies, three were uncontrolled. One (Gorman 2002) was a continuation of an RCT of orbital radiotherapy in TED that was excluded from this review due to trial design. The authors reviewed the 37 surviving patients out of the 42 enrolled in the trial at three years. Two patients died of non‐head and neck cancer, one was lost to follow‐up and two could not participate. Of the remaining three studies, only one used a control group of patients treated with other modalities (Wakelkamp 2004). The range of mean follow‐up for the four studies was three to 11 years (with one study including patients with up to 29 years follow‐up). No head or neck tumours developed during the follow‐up period in any study. In one study two patients died of haematological malignancies (Wakelkamp 2004) but one was in the irradiated group and one in the non‐irradiated group. The incidence of cataract development was reported in three of the studies and ranged from 10% to 34% (Marcocci 2003; Marquez 2001; Wakelkamp 2004). The highest value was actually found in non‐irradiated patients in one study, with irradiated patients manifesting a cataract incidence of 30%. These high rates were attributed to a highly sensitive cataract grading system (Wakelkamp 2004). The authors also commented that the majority of patients in both arms of this study received glucocorticoid treatment and this is known to be associated with posterior subcapsular cataract formation. In one study (Marcocci 2003), the authors found an increase in cataract formation in patients that received radiotherapy via cobalt unit of 18% versus the collimation of radiotherapy with linear accelerator of 8%, which is the method used now. A separate retrospective study (Schaefer 2002) of patients receiving bilateral orbital radiation for TED between 1963 and 1978 (n = 250, median follow‐up of 31 years) calculated a survival curve for the patients they were able to obtain follow‐up data on and compared this to an age‐adapted survival curve and a cancer‐specific survival curve. There was no significant difference between survival rates.
Radiation retinopathy has also been described following radiotherapy treatment for TED. Of the 546 patients who received radiotherapy in these four studies, 36 developed retinal changes (6%) believed to be related to the radiotherapy (Table 5). The presence of co‐existing diabetes, hypertension, or both and a dose of 30 Gy were found to be associated with the development of retinopathy in two studies (Marquez 2001; Wakelkamp 2004) and implied in two (Marcocci 2003; Robertson 2003). Uveitis was considered a possible risk factor for vascular changes in one patient who developed de novo retinal changes (Robertson 2003). One study comparing those that had received radiotherapy to those that had not with a mean follow‐up of 11 years (SD three years) found the mortality levels to be similar in the two groups, at 27/159 (17%) in the irradiated group and 10/86 (12%) in the non‐irradiated group (P = 0.264) (Wakelkamp 2004). One case report published in 1998 reported transitory visual loss following radiotherapy (Nygaard 1998).
5. Retinopathy findings in long‐term follow‐up studies.
| Study | Important exclusions | Assessment of retinopathy | Number of patients with retinal changes thought to be due to irradiation therapy | Important study findings |
| Marquez 2001 | Retrospective review of notes | 2/197 | Logistic regression analysis found a radiation dose of 30 Gy to correlate with retinopathy (P = 0.02) | |
| Gorman 2002 | Diabetes mellitus excluded | Photographs and FFA Only 37 patients had an FFA at baseline and 3 years |
3 Unclear if out of 42 patients irradiated or 37 with FFA |
(Robertson 2003) Of the 3 patients who developed de novo changes, 2 had no retinal changes at baseline. Of these 1 had labile hypertension and borderline glucose levels and 1 had a history of uveitis, which were implied as risk factors for vascular changes |
| Marcocci 2003 | Fundoscopy and FFA where necessary | 2/204 (13 "minimal signs of hypertensive retinopathy" 2 "possibly related to orbital irradiation") |
1 in 7 (14%) had concurrent diabetes mellitus and hypertension 1 of 31 (3%) had hypertension alone None of the 11 diabetic patients without hypertension or the 155 without diabetes or hypertension developed retinal changes |
|
| Wakelkamp 2004 | Assessed by retinal photographs (3 non‐irradiated not photographed) |
27/103 irradiated group | Diabetes mellitus had an RR of 21.0 (95% CI 3.0 to 179.0) |
CI: confidence interval FFA: Fundal fluorescein angiograms RR: risk ratio
TED is a disease that significantly affects peoples' self‐esteem and mental state. As such, quality‐of‐life changes are an essential part of monitoring treatment. Only one study addressed this by using validated questionnaires, and did not have the power to comment on any changes due to low numbers (Prummel 2004). Consequently, conclusions regarding this are lacking in this review and will have to be addressed in future research. Similarly, the cost implications of orbital radiotherapy remain poorly assessed, with only one study considering this (Prummel 2004). As such, the existing data only reflects the cost in one country and also does not assess the long‐term cost implications. Further studies in other countries would give a better indication of the true cost of radiotherapy treatment in TED management.
Quality of the evidence
Overall 244 participants were randomised in the five studies analysed in this review. Each study was an RCT and therefore level one evidence. However, there were some sources of bias in the studies with unclear allocation concealment in three studies and with two of the studies only being single‐masked. Furthermore, only two studies attempted an ITT analysis. Combining the five studies into a meta‐analysis was not possible due to differences in the study designs and outcome measures used by the different authors.
Potential biases in the review process
Three review authors (RR, RL, CB) of this Cochrane review are investigators in an existing TED treatment trial, the Combined Immunosuppression and Radiotherapy in Thyroid Eye Disease (CIRTED) trial. This trial is investigating the use of azathioprine and radiotherapy as dual and triple therapy with glucocorticoids in moderate TED. The results of this trial remain concealed to all authors at present. The design of the trial may have influenced the outcome measures used in this review but these are internationally accepted and validated elsewhere. The trial committee members encourage further trials to use these validated outcomes of disease severity and activity and quality of life, to enable a meta‐analysis of results, and have published their protocol in an open‐access e‐journal (Rajendram 2008).
Agreements and disagreements with other studies or reviews
In general the literature regarding the use of radiotherapy in TED has remained inconclusive, with authors often sceptical and calling for further high‐level evidence (McNab 2002; Mourits 2002). Some have suggested a benefit predominantly in extraocular muscle impairment (Bradley 2008; Stiebel‐Kalish 2009) but not in proptosis, eyelid retraction and soft tissue inflammation. Our Cochrane review did not investigate the effect on these areas individually but the composite scores, which included these signs in conjunction with ocular motility, did show a beneficial effect of radiotherapy.
Other reviews have agreed with our findings and report an overall favourable response to radiotherapy in comparison to sham radiotherapy and as combination therapy with glucocorticoids (Behbehani 2004; Stiebel‐Kalish 2009; Wei 2008). All of the reviews agreed with our findings that orbital radiotherapy is a relatively safe procedure when carried out correctly and at the widely used 20 Gy in 10 fractions. Despite no development of head or neck tumours in any long‐term study some authors have only recommended orbital radiotherapy in older patients due to the theoretical risk of carcinogenesis (Behbehani 2004).
One of the prompts for conducting this Cochrane review was the publication of NICE guidelines on orbital radiotherapy in TED (NICE guidelines 2005). NICE only recommend orbital radiotherapy if other treatments have failed or the patient has significant side effects to them.
One of the four studies (Gorman 2001) NICE used for evidence showed no difference in outcome for radiotherapy versus sham radiotherapy. This is a study we excluded and one that has been criticised for its inclusion criteria (Feldon 2001). This Cochrane review, although limited, disagrees with the NICE recommendations as it found that radiotherapy was equivalent to glucocorticoid treatment alone and that combination with radiotherapy and glucocorticoids has increased efficacy and therefore orbital radiotherapy should not be reserved for second‐line treatment.
Authors' conclusions
Implications for practice.
This small systematic review would support the use of orbital radiotherapy as monotherapy for moderate TED in current practice. As a meta‐analysis of orbital radiotherapy combined with steroids versus steroids alone could not be carried out this review cannot comment on its use as a combination therapy, even though single studies favoured dual therapy. The studies did not include severe TED and therefore the review cannot recommend whether radiotherapy should be used in these patients or not. The cost effectiveness of radiotherapy in TED cannot be discussed as the cost was only assessed in one study from one country in the context of mild TED and found a 12% increase in cost compared to sham. Further studies investigating cost effectiveness in regard to moderate, as well as mild disease, and comparison to other interventions are needed before this can be taken into account.
Implications for research.
The review has significant implications for research as it highlights the variation in inclusion criteria, outcome measures and study design currently used in trials assessing treatments for TED. This range reflects the subjective nature of much of the condition and the lack of obvious objective outcome measures. It also reflects the variable natural history of the disease and presentations. However, future research into this area must try and use more universal inclusion criteria, parallel study designs and reproducible outcome measures, which will permit meta‐analysis of studies to be undertaken. Specific areas of research include the impact of the disease and treatments on patients' quality of life as well as health economics. The use of radiotherapy in severe TED has not been explored but enrolling patients with significant sight‐threatening pathology that could become permanent would have ethical issues.
Acknowledgements
The Cochrane Eyes and Vision Group (CEVG) Trials Search Co‐ordinator created and ran the electronic search strategies. We thank Lelio Baldeschi for commenting on the review and Kostas Boboridis, Ann Ervin and Elizabeth Ssemanda for their comments on the protocol for the review. We also thank Taixiang Wu for contacting trialists on the Li 2008 study and Anupa Shah, Managing Editor for CEVG for her assistance throughout the review process.
Richard Wormald (Co‐ordinating Editor for CEVG) acknowledges financial support for his CEVG research sessions from the Department of Health (UK) through the award made by the National Institute for Health Research to Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology. The views expressed in this publication are those of the authors and not necessarily those of the Department of Health.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Graves Disease #2 MeSH descriptor Graves Ophthalmopathy #3 grave* near ophthalm* #4 grave* near orbitopath* #5 (thyroid*) near (ophthalm* or eye*) #6 basedow* next disease* #7 (#1 OR #2 OR #3 OR #4 OR #5 OR #6) #8 MeSH descriptor Radiotherapy #9 radiotherap* or irrad* #10 (#8 OR #9) #11 (#7 AND #10)
Appendix 2. MEDLINE (OvidSP) search strategy
1. randomized controlled trial.pt. 2. (randomized or randomised).ab,ti. 3. placebo.ab,ti. 4. dt.fs. 5. randomly.ab,ti. 6. trial.ab,ti. 7. groups.ab,ti. 8. or/1‐7 9. exp animals/ 10. exp humans/ 11. 9 not (9 and 10) 12. 8 not 11 13. exp graves disease/ 14. exp graves ophthalmopathy/ 15. (grave$ adj3 ophthalm$).tw. 16. (grave$ adj3 orbitopath$).tw. 17. ((ophthalm$ or eye$) adj3 thyroid$).tw. 18. (basedow$ adj3 disease$).tw. 19. or/13‐18 20. exp radiotherapy/ 21. (radiotherap$ or irrad$).tw. 22. or/20‐21 23. 19 and 22 24. 12 and 23
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville (Glanville 2006).
Appendix 3. EMBASE (OvidSP) search strategy
1. exp randomized controlled trial/ 2. exp randomization/ 3. exp double blind procedure/ 4. exp single blind procedure/ 5. random$.tw. 6. or/1‐5 7. (animal or animal experiment).sh. 8. human.sh. 9. 7 and 8 10. 7 not 9 11. 6 not 10 12. exp clinical trial/ 13. (clin$ adj3 trial$).tw. 14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 15. exp placebo/ 16. placebo$.tw. 17. random$.tw. 18. exp experimental design/ 19. exp crossover procedure/ 20. exp control group/ 21. exp latin square design/ 22. or/12‐21 23. 22 not 10 24. 23 not 11 25. exp comparative study/ 26. exp evaluation/ 27. exp prospective study/ 28. (control$ or prospectiv$ or volunteer$).tw. 29. or/25‐28 30. 29 not 10 31. 30 not (11 or 23) 32. 11 or 24 or 31 33. exp graves disease/ 34. exp endocrine ophthalmopathy/ 35. (grave$ adj3 ophthalm$).tw. 36. (grave$ adj3 orbitopath$).tw. 37. (thyroid adj3 ophthalm$).tw. 38. (basedow$ adj3 disease$).tw. 39. or/33‐38 40. exp radiotherapy/ 41. (radiotherap$ or irrad$).tw. 42. or/40‐41 43. 39 and 42 44. 32 and 43
Appendix 4. LILACS search strategy
grave$ or thyroid or basedow$ and ophthalm$ or orbit$ or disease or TED and radiotherap$ or irrad$
Appendix 5. metaRegister of Controlled Trials search strategy
(thyroid eye disease) and radiotherapy
Appendix 6. ClinicalTrials.gov search strategy
Thyroid Eye Disease AND Radiotherapy
Appendix 7. ICTRP search strategy
graves OR thyroid OR ophthalmopathy = Condition AND radiotherapy = Intervention
Data and analyses
Comparison 1. Radiotherapy versus other intervention or sham radiotherapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Success ‐ composite outcomes score | 2 | 147 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.92 [1.27, 2.91] |
| 2 Number of rehabilitative operations | Other data | No numeric data | ||
| 3 NOSPECS improvement at 24 weeks | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Clinical Activity Score ‐ change from baseline to 12 months | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
1.2. Analysis.
Comparison 1 Radiotherapy versus other intervention or sham radiotherapy, Outcome 2 Number of rehabilitative operations.
| Number of rehabilitative operations | |||
|---|---|---|---|
| Study | Intervention | Number of patients | Number of patients needing operations |
| Mourits 2000 | radiotherapy | 30 | 47 (total no of ops ‐ may be > 1 per pt) |
| Mourits 2000 | sham radiotherapy | 29 | 45 (total no of ops) |
| Prummel 1993 | radiotherapy | 28 | 20 |
| Prummel 1993 | steroid | 28 | 22 |
| Prummel 2004 | radiotherapy | 44 | 27 |
| Prummel 2004 | sham radiotherapy | 44 | 30 |
1.3. Analysis.

Comparison 1 Radiotherapy versus other intervention or sham radiotherapy, Outcome 3 NOSPECS improvement at 24 weeks.
1.4. Analysis.

Comparison 1 Radiotherapy versus other intervention or sham radiotherapy, Outcome 4 Clinical Activity Score ‐ change from baseline to 12 months.
Comparison 2. Radiotherapy plus steroids versus steroids.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Change in total eye score from baseline to 52 weeks | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 NOSPECS change from baseline to 52 weeks | Other data | No numeric data | ||
| 3 Ophthalmopathy Index change from baseline to final visit | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
2.1. Analysis.

Comparison 2 Radiotherapy plus steroids versus steroids, Outcome 1 Change in total eye score from baseline to 52 weeks.
2.2. Analysis.
Comparison 2 Radiotherapy plus steroids versus steroids, Outcome 2 NOSPECS change from baseline to 52 weeks.
| NOSPECS change from baseline to 52 weeks | ||||||
|---|---|---|---|---|---|---|
| Study | Treatment group | Parameter | Improvement | Static | Worse | Total No. of Participants |
| Ng 2005 | Radiotherapy & steroids | Soft Tissue | 7 | 1 | 0 | 8 |
| Ng 2005 | Steroids | Soft Tissue | 2 | 5 | 0 | 7 |
| Ng 2005 | Radiotherapy & steroids | Ocular Motility | 7 ('normal eye motion' 5) |
1 | 0 | 8 |
| Ng 2005 | Steroids | Ocular Motility | 2 ('normal eye motion' 0) |
4 | 1 | 7 |
2.3. Analysis.

Comparison 2 Radiotherapy plus steroids versus steroids, Outcome 3 Ophthalmopathy Index change from baseline to final visit.
Comparison 3. Adverse events.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Side effects | Other data | No numeric data |
Comparison 4. Change in quality of life between baseline and 12 months of treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 GO‐QoL (Graves Ophthalmopathy ‐ Quality of Life) | Other data | No numeric data | ||
| 2 MOS‐24 (Medical Outcomes Study Short‐form General Health Survey) | Other data | No numeric data | ||
| 3 SIP (Sickness Impact Profile) | Other data | No numeric data | ||
| 4 Euro‐QoL | Other data | No numeric data | ||
| 5 Subjective eye score | Other data | No numeric data |
4.1. Analysis.
Comparison 4 Change in quality of life between baseline and 12 months of treatment, Outcome 1 GO‐QoL (Graves Ophthalmopathy ‐ Quality of Life).
| GO‐QoL (Graves Ophthalmopathy ‐ Quality of Life) | ||||
|---|---|---|---|---|
| Study | Control mean(SD) | Radiotherapy mean (SD) | Difference (95% CI) | |
| Prummel 2004 | visual functioning | 10.5 (16.8) | 8.2 (15.8) | ‐2.3 (‐11.5 to 6.7) |
| Prummel 2004 | appearance | 5.5 (16.6) | 6.7 (17.2) | 1.2 (‐8.4 to 10.7) |
4.2. Analysis.
Comparison 4 Change in quality of life between baseline and 12 months of treatment, Outcome 2 MOS‐24 (Medical Outcomes Study Short‐form General Health Survey).
| MOS‐24 (Medical Outcomes Study Short‐form General Health Survey) | ||||
|---|---|---|---|---|
| Study | Control mean (SD) | Radiotherapy mean (SD) | Difference(95% CI) | |
| Prummel 2004 | physical functioning | ‐1.4 (19.4) | ‐0.3 (11.2) | 1.1 (‐7.8 to 9.9) |
| Prummel 2004 | role functioning | 2.0 (20.3) | 6.7 (18.1) | 4.7 (‐6.1 to 15.5) |
| Prummel 2004 | social functioning | ‐3.2 (23.6) | ‐1.5 (23.9) | 1.7 (‐11.7 to 15.0) |
| Prummel 2004 | mental health | ‐3.8 (17.1) | 2.3 (19.1) | 6.1 (‐1.4 to 16.4) |
| Prummel 2004 | general health perceptions | ‐3.4 (16.3) | 0.2 (16.0) | 3.6 (‐5.5 to 12.7) |
| Prummel 2004 | bodily pain | ‐1.0 (31.9) | ‐1.0 (32.8) | 0.04 (‐18.2 to 18.2) |
| Prummel 2004 | vitality | ‐0.4 (17.4) | 3.3 (13.3) | 3.7 (‐5.0‐12.4) |
4.3. Analysis.
Comparison 4 Change in quality of life between baseline and 12 months of treatment, Outcome 3 SIP (Sickness Impact Profile).
| SIP (Sickness Impact Profile) | ||||
|---|---|---|---|---|
| Study | Control mean (SD) | Radiotherapy mean (SD) | Difference (95% CI) | |
| Prummel 2004 | social interaction | 1.2 (14.3) | 3.5 (12.8) | 2.4 (‐5.3 to 10.0) |
| Prummel 2004 | household management | 3.8 (19.3) | 0.8 (12.4) | ‐3.1 (‐12.2 to 6.0) |
| Prummel 2004 | leisure pastimes & recreation | 5.0 (22.2) | 7.4 (16.3) | 2.4 (‐8.6 to 13.4) |
4.4. Analysis.
Comparison 4 Change in quality of life between baseline and 12 months of treatment, Outcome 4 Euro‐QoL.
| Euro‐QoL | |||
|---|---|---|---|
| Study | Control mean (SD) | Radiotherapy mean (SD) | Difference (95% CI) |
| Prummel 2004 | 3.2 (14.3) | 1.2 ( 14.5) | ‐2.0 (‐11.9 to 7.9) |
4.5. Analysis.
Comparison 4 Change in quality of life between baseline and 12 months of treatment, Outcome 5 Subjective eye score.
| Subjective eye score | ||
|---|---|---|
| Study | mean change in control group (SD) | mean change in experimental group (SD) |
| Ng 2005 | +1.3 (0.9) (steroids) | +1.2 (0.8) (steroids & radiotherapy) |
| Prummel 1993 | +1(steroids) | +0.8 (radiotherapy) |
Comparison 5. Health economic analysis.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Cost of treatment | Other data | No numeric data |
5.1. Analysis.
Comparison 5 Health economic analysis, Outcome 1 Cost of treatment.
| Cost of treatment | ||
|---|---|---|
| Study | Intervention | cost per patient in Euros |
| Prummel 2004 | radiotherapy | 5007 |
| Prummel 2004 | sham‐irradiation | 4465 |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bartalena 1983.
| Methods | RCT | |
| Participants | 48 discussed but only 24 randomised (12 intervention, 12 control) consecutive patients | |
| Interventions | Intervention: radiotherapy (10 daily doses of 200 rads) + IV steroids (70 to 80 mg methylprednisolone for 3 weeks, dose tapered by 5 mg weekly until a daily dosage of 20 mg then reduced by 2.5 to 5 mg every 2 to 3 weeks and stopped at 5 to 6 months) Control: IV steroids (as above) |
|
| Outcomes | Clinical grading of treatment result as "excellent, good, slight and no response" Soft tissue changes Proptosis (mm) Ophthalmopathy Index |
|
| Notes | Radiotherapy + IV steroid group: n = 12, mean age 42 years; mean duration of TED 25 months, mean follow‐up after steroid cessation 19 months (range 12 to 25 months) IV steroid group: n = 12, mean age 46 years, mean duration of TED 26 months, mean follow‐up after steroid cessation 18 months (range 12 to 28 months) CT carried out Source of funding not stated |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients "were randomly assigned by the use of random numbers". |
| Allocation concealment (selection bias) | Unclear risk | This information was not reported in the trial. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | The ophthalmologist evaluating eye changes after therapy was unaware of the type of treatment used. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 24 patients are included in the results but the paper is not explicit in describing the duration of follow‐up for these or whether any dropped out early. |
Mourits 2000.
| Methods | Placebo‐controlled RCT | |
| Participants | 60 participants (30 intervention, 30 control) consecutive patients, moderately severe Graves' orbitopathy (worse eye motility impairment causing diplopia, or proptosis of ≥ 23 mm or moderate‐to‐severe lid swelling or combination of these), ages 20 to 75 years, only local treatment for orbitopathy, euthyroid for 3 months prior to enrolment | |
| Interventions | Intervention: radiotherapy 20 Gy in 10 fractions over 12 days Control: sham radiotherapy |
|
| Outcomes | Lid aperture (mm) Eyelid swelling (no swelling, mild, moderate, severe swelling) documented with photographs Proptosis (mm) Uniocular eye movements (degrees) Field of binocular single vision CAS (0 to 10) Subjective eye score (1 to 10, 10 worst possible) Composite outcome (major criteria ‐ improvement in diplopia grade, improvement in eye movement of 8 degrees or more; minor criteria change of 2 mm or more in lid aperture, change in proptosis of 2 mm or more, change in eyelid swelling); success 1 or more major criteria or 2 minor |
|
| Notes | CT scans performed No comment on funding made |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | External randomisation office (the data centre of the Netherlands Integral Cancer Center). |
| Allocation concealment (selection bias) | Low risk | External randomisation office (the data centre of the Netherlands Integral Cancer Center). Placebo‐controlled. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 placebo patient withdrew before the first session radiotherapy/sham and was excluded from the analysis as they had not commenced treatment. |
Ng 2005.
| Methods | RCT | |
| Participants | 16 participants (8 intervention, 8 control) Moderate‐to‐severe Graves ophthalmopathy (NOSPECS class 2 grade a, b, c plus 1 or more of the following: class 3 grade b, c; class 4 grade a, b, c; class 6 grade a, b, c); euthyroid when recruited, optic nerve compression "only recruited if refused surgery or if surgery contra‐indicated"; ages 20 to 80 years |
|
| Interventions | Intervention: radiotherapy (20 Gy 10 fractions over 2 weeks) + IV steroids (500 mg IV methylprednisolone 3 days then 0.7 mg/kg oral prednisolone daily for 4 weeks, then reduction by 5 mg per week until 5 mg once daily reached, then 2.5 mg for 1 week) Control: IV steroids (500 mg IV methylprednisolone 3 days then 0.7 mg/kg oral prednisolone daily for 4 weeks, then reduction by 5 mg per week until 5 mg once daily reached, then 2.5 mg for 1 week) |
|
| Outcomes | NOSPECS Total eye score (0 to 45) Subjective eye score (1 to 5, with 1 being the worst and 5 being the best) Extraocular muscle thickness on CT/MRI (cm) Assessment at 52 weeks |
|
| Notes | Source of funding not stated | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stated participants randomised but does not state how. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Single‐masked (assessor masked). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 patient in steroid group died of hospital acquired pneumonia 3 weeks before initiation of treatment prior to first post‐intervention assessment (week 4) therefore his results were excluded in the efficacy analysis. ITT analysis provided at least 1 set of post‐baseline efficacy data at week 4 for the remaining participants. LOCF principle used in those that did not complete the study. |
Prummel 1993.
| Methods | Placebo‐controlled RCT | |
| Participants | 56 participants (28 intervention, 28 controls) consecutive untreated moderately severe graves orbitopathy patients, 20 to 70 years old, euthyroid 2 months prior to trial | |
| Interventions | Intervention: radiotherapy (10 divided fractions of 2 Gy daily over 2 weeks) Control: oral prednisolone (60 mg for 2 weeks, 40 mg for 2 weeks, 30 mg for 4 weeks, 20 mg for 4 weeks then decreasing by 2.5 mg per week) |
|
| Outcomes | NOSPECS score Total eye score Eye muscle score (0 to 5) based on number of muscles enlarged, degree of enlargement in coronal plane, extent of enlargement along length of muscle Subjective eye score (1 to 10, 1 being the worst and 10 being the best) Overall response at 24 weeks' post treatment used at endpoint Palpebral aperture (mm) Duction eye movements (degrees) |
|
| Notes | No comment on funding CT scans obtained |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation list. |
| Allocation concealment (selection bias) | High risk | Randomisation list with no statement regarding concealment of previous and following allocation. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐masked. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 9 patients (6 in prednisolone group) forgot 1 or 2 capsules during study. 1 prednisolone patient did not take medication during the last 3 weeks of treatment, 1 did not take placebo for 2 weeks ‐ "both were retained in the analysis". |
Prummel 2004.
| Methods | Placebo‐controlled RCT | |
| Participants | 88 (44 intervention, 44 control), consecutive untreated mild Graves orbitopathy (defined as having a mild extraocular eye muscle motility disturbance, mostly elevation, using an age‐specific nomogram with or without mild or moderate eyelid swelling),18 to 75 years old, euthyroid 2 months prior to trial | |
| Interventions | Intervention: 10 divided fractions of 2 Gy daily over 2 weeks Control: sham radiotherapy |
|
| Outcomes | Composite outcome Major criteria
Minor criteria
A response to treatment was defined as 'very good' in the case of an improvement in at least 2 major criteria, as 'good' in the case of an improvement in 1 major criterion, as 'fair' in the case of an improvement in 2 minor criteria, as 'no change' in the case of no changes or a change in only 1 minor criteria, and as 'worse' in the case of a deterioration in at least 1 major or 2 minor criteria Quality‐of‐life assessment Health economic assessment CAS |
|
| Notes | Quality‐of‐life assessment "could not be assessed in the first 23 patients" and had a 92% response given at baseline and 85% at 12 months and therefore not sufficiently powered Work supported by grant from the Dutch Healthcare Insurance Board (OG 94/038) 3, 6 and 12 months assessments |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation with blocks of 4 patients. |
| Allocation concealment (selection bias) | Low risk | Coded sealed opaque envelopes. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐masked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ITT. When a patient was prematurely withdrawn from the study, in the case of a decrease in visual acuity of 2 or more Snellen lines, an increase in proptosis of 3 mm or more, or a decrease in eye muscle motility of 10 degrees or more, all outcomes measures were assessed at that time, and the patient was analysed according to the last value carried forwards principle. |
CAS: clinical activity score CT: computed tomography ITT: intention‐to‐treat IV: intravenous LOCF: last observation carried forwards mm: millimetres MRI: magnetic resonance imaging RCT: randomised controlled trial TED: thyroid eye disease
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Antonelli 1992 | Patients were randomised to orbital radiotherapy, oral steroids and intravenous immunoglobulin (treatment group) versus intravenous immunoglobulin only (control group). Therefore there were 2 differing treatment modalities between groups. |
| Gorman 2001 | 1 orbit was treated and the other used as a control (lymphocytes affected by radiotherapy would circulate throughout body and therefore this is not appropriate) |
| Li 2008 | The authors were contacted and they stated that this was not an RCT |
| Sterker 2009 | Retrospective study |
Contributions of authors
Conceiving the review: the review was originally conceived by Mr Michael Wearne (MW), consultant ophthalmologist. RR and CB took over the review.
Undertaking manual searches: RR.
Screening search results: RR, SM.
Organising retrieval of papers: Cochrane Eyes and Vision Group Trials Search Co‐ordinator.
Screening retrieved papers against inclusion criteria: RR, SM.
Appraising quality of papers: CB, RR, SM.
Extracting data from papers: CB, RR, SM.
Writing to authors of papers for additional information: RR.
Providing additional data about papers: RR.
Data management for the review
Entering data into RevMan: CB, RR, SM.
Analysis of data: CB, RR, SM.
Interpretation of data
Providing a methodological perspective: CB.
Providing a clinical perspective: RR, SM, RL.
Providing a policy perspective: RR, SM, RL.
Providing a consumer perspective: RR, SM, RL.
Writing the review: RR, SM, RL, CB.
Providing general advice on the review: CB, RR.
Performing previous work that was the foundation of the current study: MW.
Sources of support
Internal sources
Moorfields Eye Hospital NHS Foundation Hospital, UK.
External sources
No sources of support supplied
Declarations of interest
The three authors (RR, CB, RL) are investigators in an RCT of medical treatment for TED.
New
References
References to studies included in this review
Bartalena 1983 {published data only}
- Bartalena L, Marcocci C, Chiovato L, Laddaga M, Lepri G, Andreani D, et al. Orbital cobalt irradiation combined with systemic corticosteroids for Graves' ophthalmopathy: comparison with systemic corticosteroids alone. Journal of Clinical Endocrinology and Metabolism 1983;56(6):1139‐44. [DOI] [PubMed] [Google Scholar]
Mourits 2000 {published data only}
- Mourits MP, Kempen‐Hartveld ML, Garcia MB, Koppeschaar HP, Tick L, Terwee CB. Radiotherapy for Graves' orbitopathy: randomised placebo‐controlled study. Lancet 2000;355(9124):1505‐9. [DOI] [PubMed] [Google Scholar]
Ng 2005 {published data only}
- Ng CM, Yuen HK, Choi KL, Chan MK, Yuen KT, Ng YW, et al. Combined orbital irradiation and systemic steroids compared with systemic steroids alone in the management of moderate‐to‐severe Graves' ophthalmopathy: a preliminary study. Hong Kong Medical Journal 2005;11(5):322‐30. [PubMed] [Google Scholar]
Prummel 1993 {published data only}
- Prummel MF, Mourits MP, Blank L, Berghout A, Koornneef L, Wiersinga WM. Randomized double‐blind trial of prednisone versus radiotherapy in Graves' ophthalmopathy. Lancet 1993;342(8877):949‐54. [DOI] [PubMed] [Google Scholar]
Prummel 2004 {published data only}
- Prummel MF, Terwee CB, Gerding MN, Baldeschi L, Mourits MP, Blank L, et al. A randomized controlled trial of orbital radiotherapy versus sham irradiation in patients with mild graves' ophthalmopathy. Journal of Clinical Endocrinology and Metabolism 2004;89(1):15‐20. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Antonelli 1992 {published data only}
- Antonelli A, Saracino A, Alberti B, Canapicchi R, Cartei F, Lepri A, et al. High‐dose intravenous immunoglobulin treatment in Graves' ophthalmopathy. Acta Endocrinologica 1992;126(1):13‐23. [DOI] [PubMed] [Google Scholar]
Gorman 2001 {published data only}
- Gorman CA, Garrity JA, Fatourechi V, Bahn, RS, Petersen IA, Stafford SL, et al. A prospective, randomized, double‐blind, placebo‐controlled study of orbital radiotherapy for Graves' ophthalmopathy. Ophthalmology 2001;108(9):1523‐34. [DOI] [PubMed] [Google Scholar]
Li 2008 {published data only}
- Li LL, Wang F, Zhang Y, Sun R. Observation of curative effect of triamcinolone acetomide retrobular injection combined with orbital radiation on TAO. International Journal of Ophthalmology 2008;8(9):1860‐2. [Google Scholar]
Sterker 2009 {published data only}
- Sterker I, Tegetmeyer H, Papsdorf K, Fuhrer‐Sakel D. Effect of combined intravenous glucocorticoids and orbital radiotherapy in restoring driving competency in patients with Graves' orbitopathy. Hormone and Metabolic Research 2009;41(5):391‐6. [DOI] [PubMed] [Google Scholar]
Additional references
Bahn 1993
- Bahn RS, Heufelder AE. Pathogenesis of Graves' ophthalmopathy. New England Journal of Medicine 1993;329(20):1468‐75. [DOI] [PubMed] [Google Scholar]
Bahn 2010
- Bahn RS. Graves' ophthalmopathy. New England Journal of Medicine 2010;362(8):726‐38. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bartalena 2000
- Bartalena L, Pinchera A, Marcocci C. Management of Graves' ophthalmopathy: reality and perspectives. Endocrine Reviews 2000;21(2):168‐99. [DOI] [PubMed] [Google Scholar]
Bartalena 2004
- Bartalena L, Marcocci C, Pinchera A. Orbital radiotherapy for Graves' ophthalmopathy. Journal of Clinical Endocrinology and Metabolism 2004;89(1):13‐4. [DOI] [PubMed] [Google Scholar]
Behbehani 2004
- Behbehani R, Sergott RC, Savino PJ. Orbital radiotherapy for thyroid‐related orbitopathy. Current Opinion in Ophthalmology 2004;15(6):479‐82. [DOI] [PubMed] [Google Scholar]
Bradley 2008
- Bradley EA, Gower EW, Bradley DJ, Meyer DR, Cahill KV, Custer PL, et al. Orbital radiation for graves ophthalmopathy: a report by the American Academy of Ophthalmology. Ophthalmology 2008;115(2):398‐409. [DOI] [PubMed] [Google Scholar]
Cawood 2004
- Cawood T, Moriarty P, O'Shea D. Recent developments in thyroid eye disease. BMJ 2004;329(7462):385‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dickinson 2001
- Dickinson AJ, Perros P. Controversies in the clinical evaluation of active thyroid‐associated orbitopathy: use of a detailed protocol with comparative photographs for objective assessment. Clinical Endocrinology 2001;55(3):283‐303. [DOI] [PubMed] [Google Scholar]
Donaldson 1973
- Donaldson SS, Bagshaw MA, Kriss JP. Supervoltage orbital radiotherapy for Graves' ophthalmopathy. Journal of Clinical Endocrinology and Metabolism 1973;37(2):276‐85. [DOI] [PubMed] [Google Scholar]
EUGOGO 2006a
- The European Group on Graves' Orbitopathy (EUGOGO), Wiersinga WM, Perros P, Kahaly GJ, Mourits MP, Baldeschi L, Boboridis K, et al. Clinical assessment of patients with Graves' orbitopathy: the European Group on Graves' Orbitopathy recommendations to generalists, specialists and clinical researchers. European Journal of Endocrinology 2006;155(3):387‐9. [DOI] [PubMed] [Google Scholar]
EUGOGO 2006b
- The European Group of Graves' Orbitopathy, Perros P, Baldeschi L, Boboridis K, Dickinson AJ, Hullo A, Kahaly GJ, et al. A questionnaire survey on the management of Graves' orbitopathy in Europe. European Journal of Endocrinology 2006;155(2):207‐11. [DOI] [PubMed] [Google Scholar]
Feldon 2001
- Feldon SE. Radiation therapy for Graves' ophthalmopathy: trick or treat?. Ophthalmology 2001;108(9):1521‐2. [DOI] [PubMed] [Google Scholar]
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso‐Stefinovic J. How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130‐6. [PMC free article] [PubMed] [Google Scholar]
Gorman 2002
- Gorman CA, Garrity JA, Fatourechi V, Bahn RS, Petersen IA, Stafford SL, et al. The aftermath of orbital radiotherapy for graves' ophthalmopathy. Ophthalmology 2002;109(11):2100‐7. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hildebrandt 1998
- Hildebrandt G, Seed MP, Freemantle CN, Aslam CAS, Colville‐Nash PR, Trott KR. Mechanisms of the anti‐inflammatory activity of low‐dose radiation therapy. International Journal of Radiation Biology 1998;74(3):367‐78. [DOI] [PubMed] [Google Scholar]
Kahaly 1988
- Kahaly G, Beyer J. Immunosuppressant therapy of thyroid eye disease. Klinische Wochenschrift 1988;66(21):1049‐59. [DOI] [PubMed] [Google Scholar]
Lehmann 2007
- Lehmann GM, Feldon SE, Smith TJ, Phipps RP. Immune mechanisms in thyroid eye disease. Thyroid 2007;18(9):959‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marcocci 2001
- Marcocci C, Bartalena L, Tanda ML, Manetti L, Dell'Unto E, Rocchi R, et al. Comparison of the effectiveness and tolerability of intravenous or oral glucocorticoids associated with orbital radiotherapy in the management of severe Graves' ophthalmopathy: results of a prospective, single‐blind, randomized study. Journal of Clinical Endocrinology and Metabolism 2001;86(8):3562‐7. [DOI] [PubMed] [Google Scholar]
Marcocci 2003
- Marcocci C, Bartalena L, Rocchi R, Marino M, Menconi F, Morabito E, et al. Long‐term safety of orbital radiotherapy for Graves' ophthalmopathy. Journal of Clinical Endocrinology and Metabolism 2003;88(8):3561‐6. [DOI] [PubMed] [Google Scholar]
Marquez 2001
- Marquez SD, Lum BL, McDougall IR, Katkuri S, Levin PS, MacManus M, et al. Long‐term results of irradiation for patients with progressive Graves' ophthalmopathy. International Journal of Radiation Oncology, Biology, Physics 2001;51(3):766‐74. [DOI] [PubMed] [Google Scholar]
McNab 2002
- McNab AA. Does radiotherapy have a role in the management of thyroid orbitopathy?. British Journal of Ophthalmology 2002;86(1):106‐7. [PubMed] [Google Scholar]
Mourits 1989
- Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, Gaag R. Clinical criteria for the assessment of disease activity in Graves' ophthalmopathy: a novel approach. British Journal of Ophthalmology 1989;73(8):639‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mourits 1997
- Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with Graves' ophthalmopathy. Clinical Endocrinology 1997;47(1):9‐14. [DOI] [PubMed] [Google Scholar]
Mourits 2002
- Mourits MP. Does radiotherapy have a role in the management of thyroid orbitopathy ‐ View 2. British Journal of Ophthalmology 2002;86(1):104‐6. [PubMed] [Google Scholar]
NICE guidelines 2005
- National Institute for Health and Clinical Excellence. Retrobulbar irradiation for thyroid eye disease. www.nice.org.uk/ip257overview 2005 (accessed March 2012).
Nygaard 1998
- Nygaard B, Specht L. Transitory blindness after retrobulbar irradiation of Graves ophthalmopathy. Lancet 1998;351(9104):725‐6. [DOI] [PubMed] [Google Scholar]
Perros 1993
- Perros P, Crombie AL, Matthews JN, Kendall‐Taylor P. Age and gender influence the severity of thyroid‐associated ophthalmopathy: a study of 101 patients attending a combined thyroid‐eye clinic. Clinical Endocrinology 1993;38(4):367‐72. [DOI] [PubMed] [Google Scholar]
Prummel 1989
- Prummel MF, Mourits MP, Berghout A, Krenning EP, Gaag R, Koornneef L, et al. Prednisone and cyclosporine in the treatment of severe Graves' ophthalmopathy. New England Journal of Medicine 1989;321(20):1353‐9. [DOI] [PubMed] [Google Scholar]
Rajendram 2008
- Rajendram R, Lee RW, Potts MJ, Rose GE, Jain R, Olver JM, et al. Protocol for the combined immunosuppression & radiotherapy in thyroid eye disease (CIRTED) trial: a multi‐centre, double‐masked, factorial randomised controlled trial. Trials 2008;9:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2011 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Robertson 2003
- Robertson DM, Buettner H, Gorman CA, Garrity JA, Fatourechi V, Bahn RS, et al. Retinal microvascular abnormalities in patients treated with external radiation for graves ophthalmopathy. Archives of Ophthalmology 2003;121(5):652‐7. [DOI] [PubMed] [Google Scholar]
Rundle 1945
- Rundle F, Wilson C. Development and course of exophthalmos and ophthalmoplegia in Graves' disease with special reference to the effect of thyroidectomy. Clinical Science 1945;5:177‐94. [PubMed] [Google Scholar]
Schaefer 2002
- Schaefer U, Hesselmann S, Micke O, Schueller P, Bruns F, Palma C, et al. A long‐term follow‐up study after retro‐orbital irradiation for Graves' ophthalmopathy. International Journal of Radiation Oncology, Biology, Physics 2002;52(1):192‐7. [DOI] [PubMed] [Google Scholar]
Smith 2003
- Smith TJ. The putative role of fibroblasts in the pathogenesis of Graves' disease: evidence for the involvement of the insulin‐like growth factor‐1 receptor in fibroblast activation. Autoimmunity 2003;36:409‐15. [DOI] [PubMed] [Google Scholar]
Smith 2004
- Smith TJ, Hoa N. Immunoglobulins from patients with Graves' disease induce hyaluronan synthesis in their orbital fibroblasts through the self‐antigen, insulin‐like growth factor‐I receptor. Journal of Clinical Endocrinology and Metabolism 2004;89(10):5076‐80. [DOI] [PubMed] [Google Scholar]
Stan 2010
- Stan MN, Bahn RS. Risk factors for development or deterioration of Graves' ophthalmopathy. Thyroid 2010;20(7):777‐83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stiebel‐Kalish 2009
- Stiebel‐Kalish H, Robenshtok E, Hasanreisoglu M, Ezrachi D, Shimon I, Leibovici L. Treatment modalities for Graves' ophthalmopathy: systematic review and metaanalysis. Journal of Clinical Endocrinology and Metabolism 2009;94(8):2708‐16. [DOI] [PubMed] [Google Scholar]
Terwee 2001
- Terwee CB, Dekker FW, Mourits MP, Gerding MN, Baldeschi L, Kalmann R, et al. Interpretation and validity of changes in scores on the Graves' ophthalmopathy quality of life questionnaire (GO‐QOL) after different treatments. Clinical Endocrinology 2001;54(3):391‐8. [DOI] [PubMed] [Google Scholar]
Terwee 2002
- Terwee C, Wakelkamp I, Tan S, Dekker F, Prummel MF, Wiersinga W. Long‐term effects of Graves' ophthalmopathy on health‐related quality of life. European Journal of Endocrinology 2002;146(6):751‐7. [DOI] [PubMed] [Google Scholar]
Van Steensel 2010
- Steensel L, Dik WA. The orbital fibroblast: a key player and target for therapy in Graves' ophthalmopathy. Orbit 2010;29(4):202‐6. [DOI] [PubMed] [Google Scholar]
Wakelkamp 2004
- Wakelkamp IM, Tan H, Saeed P, Schlingemann RO, Verbraak FD, Blank LE, et al. Orbital irradiation for Graves' ophthalmopathy: is it safe? A long‐term follow‐up. Ophthalmology 2004;111(8):1557‐62. [DOI] [PubMed] [Google Scholar]
Wei 2008
- Wei RL, Cheng JW, Cai JP. The use of orbital radiotherapy for Graves' ophthalmopathy: quantitative review of the evidence. Ophthalmologica 2008;222(1):27‐31. [DOI] [PubMed] [Google Scholar]
Werner 1977
- Werner SC. Modification of the classification of the eye changes of Graves' disease: recommendations of the Ad Hoc Committee of the American Thyroid Association. Journal of Clinical Endocrinology and Metabolism 1977;44(1):203‐4. [DOI] [PubMed] [Google Scholar]