

Abstract
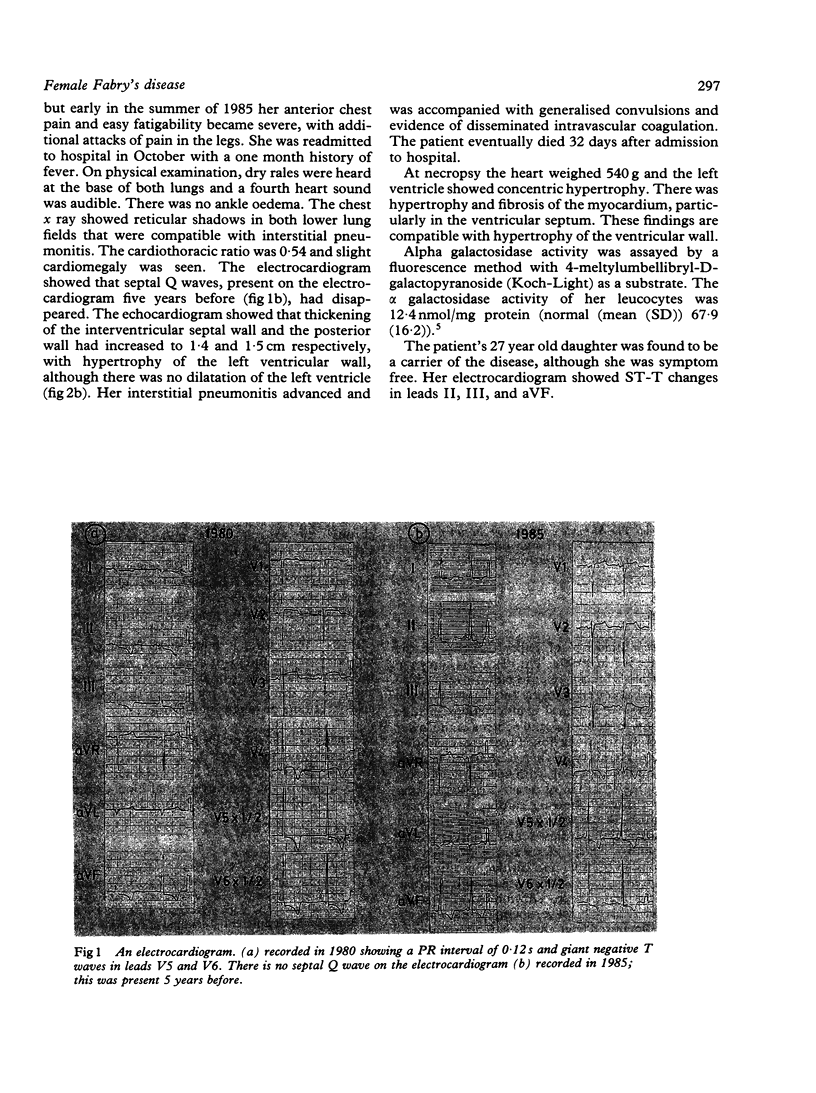
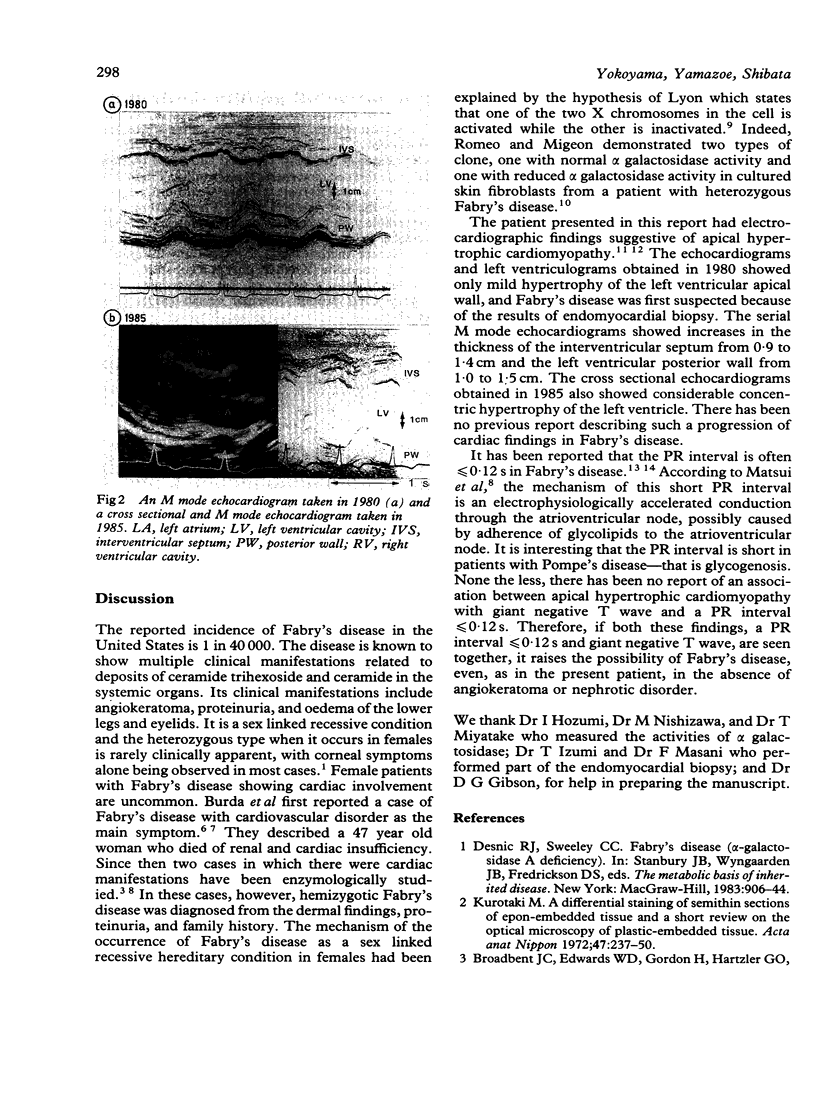
A 55 year old woman with heterozygous Fabry's disease presented with cardiac symptoms. The electrocardiogram showed a PR interval of 0.12 s and giant negative T waves, suggesting apical hypertrophic cardiomyopathy. Endomyocardial biopsy, however, revealed myelin like substances characteristic of Fabry's disease. Increasing thickness of the left ventricular wall was seen by echocardiography over a period of five years. A deficiency of alpha galactosidase activity in the leucocytes confirmed the diagnosis of Fabry's disease, although this patient had neither angiokeratoma or proteinuria. The possibility of Fabry's disease should be considered in patients with cardiomegaly of unknown cause and the following electrocardiographic abnormalities: a PR interval less than or equal to 0.12 s, high voltage QRS complexes in the left precordial leads, and giant negative T waves.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Applefeld M. M., Billingsley L. M., Tucker H. J., Fiset P. Q fever endocarditis--a case occurring in the United States. Am Heart J. 1977 May;93(5):669–670. [PubMed] [Google Scholar]
- Broadbent J. C., Edwards W. D., Gordon H., Hartzler G. O., Krawisz J. E. Fabry cardiomyopathy in the female confirmed by endomyocardial biopsy. Mayo Clin Proc. 1981 Oct;56(10):623–628. [PubMed] [Google Scholar]
- Burda C. D., Winder P. R. Angiokeratoma corporis diffusum universale (Fabry's disease) in female subjects. Am J Med. 1967 Feb;42(2):293–301. doi: 10.1016/0002-9343(67)90027-7. [DOI] [PubMed] [Google Scholar]
- Kurotaki M. [Differential staining of epon-resin-embedded tissue for light microscopy observation (including review of the literature on general technics of semi-thin sectioning)]. Kaibogaku Zasshi. 1972 Jun;47(3):237–250. [PubMed] [Google Scholar]
- LYON M. F. Gene action in the X-chromosome of the mouse (Mus musculus L.). Nature. 1961 Apr 22;190:372–373. doi: 10.1038/190372a0. [DOI] [PubMed] [Google Scholar]
- Matsui S., Murakami E., Takekoshi N., Hiramaru Y., Kin T. Cardiac manifestations of Fabry's disease. Report of a case with pulmonary regurgitation diagnosed on the basis of endomyocardial biopsy findings. Jpn Circ J. 1977 Sep;41(9):1023–1036. [PubMed] [Google Scholar]
- Rodriguez F. H., Jr, Hoffmann E. O., Ordinario A. T., Jr, Baliga M. Fabry's disease in a heterozygous woman. Arch Pathol Lab Med. 1985 Jan;109(1):89–91. [PubMed] [Google Scholar]
- Romeo G., Migeon B. R. Genetic inactivation of the alpha-galactosidase locus in carriers of Fabry's disease. Science. 1970 Oct 9;170(3954):180–181. doi: 10.1126/science.170.3954.180. [DOI] [PubMed] [Google Scholar]
- Sakamoto T., Tei C., Murayama M., Ichiyasu H., Hada Y. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle. Echocardiographic and ultrasono-cardiotomographic study. Jpn Heart J. 1976 Sep;17(5):611–629. doi: 10.1536/ihj.17.611. [DOI] [PubMed] [Google Scholar]
- Suzuki K. Enzymic diagnosis of sphingolipidoses. Methods Enzymol. 1978;50:456–488. doi: 10.1016/0076-6879(78)50049-9. [DOI] [PubMed] [Google Scholar]
- Toole J. F. Informed consent. Circulation. 1973 Jul;48(1):1–4. doi: 10.1161/01.cir.48.1.1. [DOI] [PubMed] [Google Scholar]
- Yamaguchi H., Ishimura T., Nishiyama S., Nagasaki F., Nakanishi S., Takatsu F., Nishijo T., Umeda T., Machii K. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): ventriculographic and echocardiographic features in 30 patients. Am J Cardiol. 1979 Sep;44(3):401–412. doi: 10.1016/0002-9149(79)90388-6. [DOI] [PubMed] [Google Scholar]