

Abstract
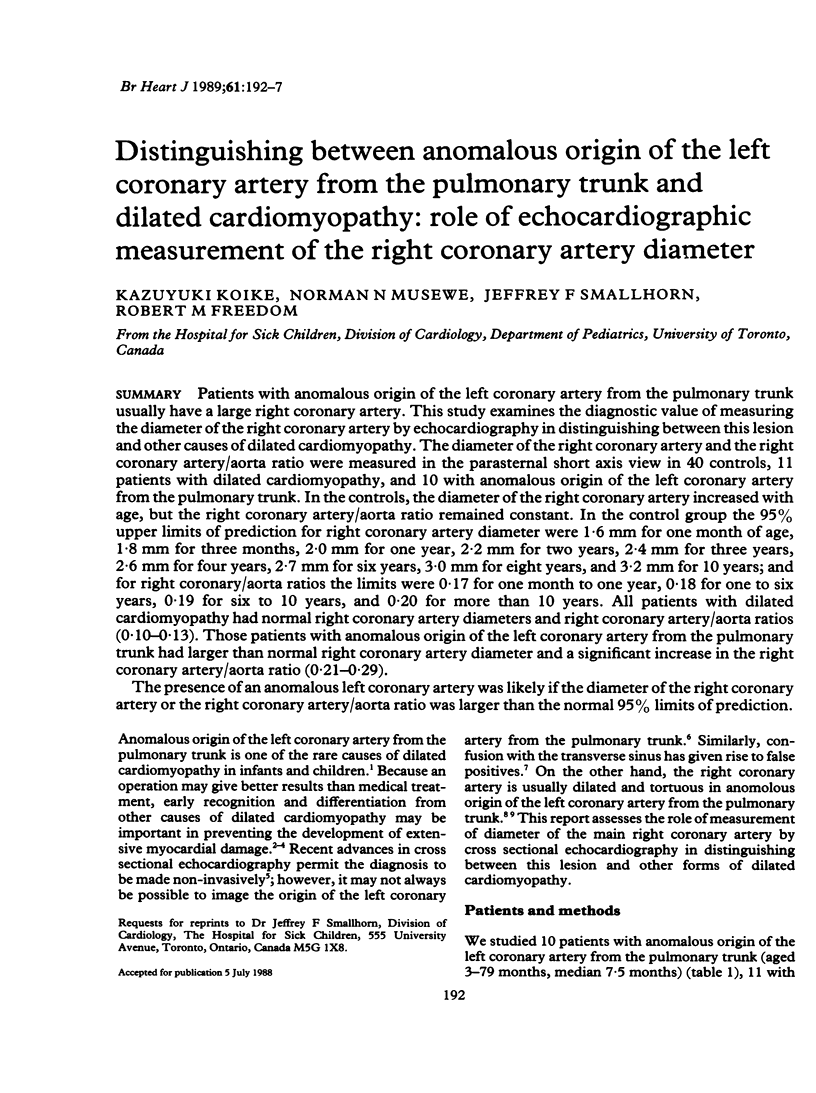
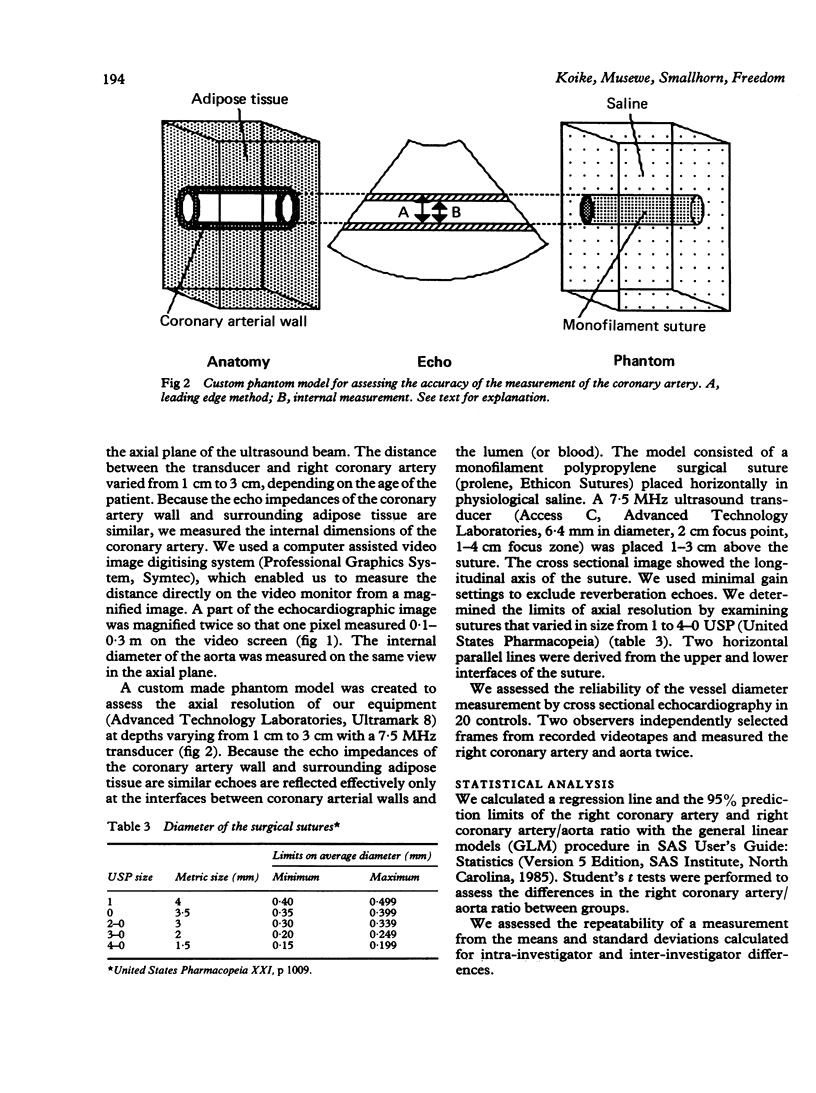
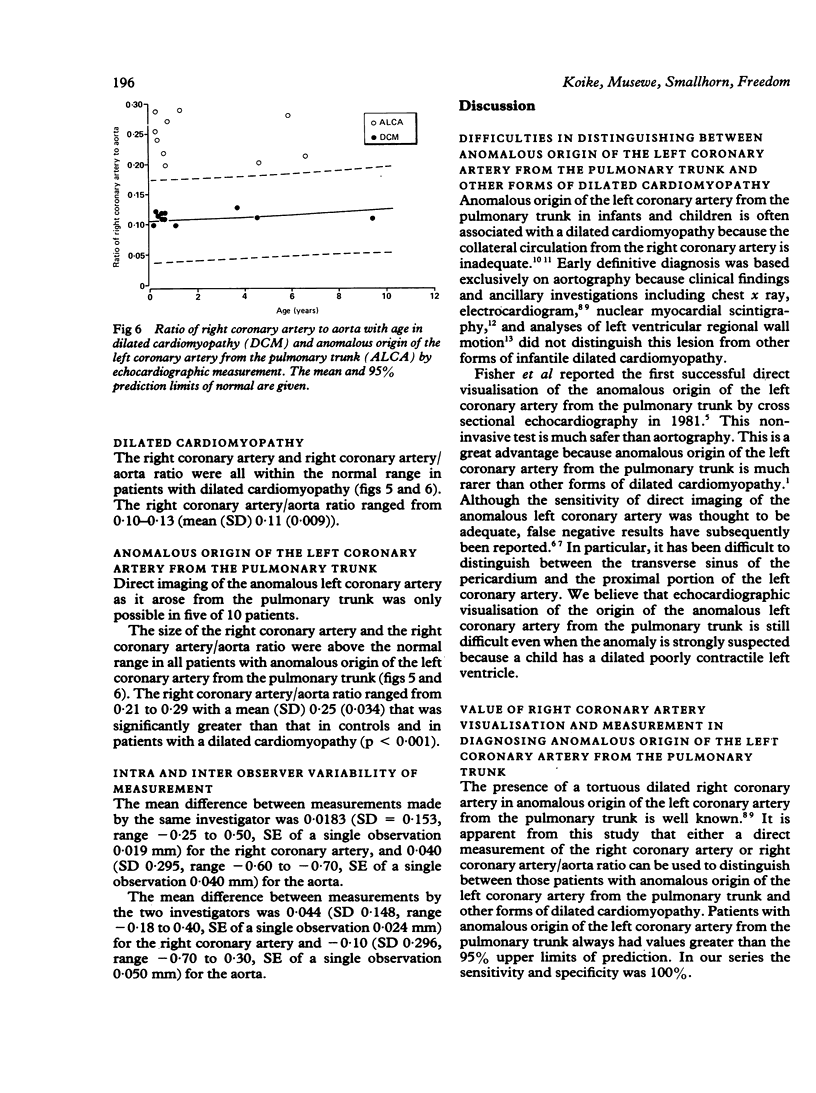
Patients with anomalous origin of the left coronary artery from the pulmonary trunk usually have a large right coronary artery. This study examines the diagnostic value of measuring the diameter of the right coronary artery by echocardiography in distinguishing between this lesion and other causes of dilated cardiomyopathy. The diameter of the right coronary artery and the right coronary artery/aorta ratio were measured in the parasternal short axis view in 40 controls, 11 patients with dilated cardiomyopathy, and 10 with anomalous origin of the left coronary artery from the pulmonary trunk. In the controls, the diameter of the right coronary artery increased with age, but the right coronary artery/aorta ratio remained constant. In the control group the 95% upper limits of prediction for right coronary artery diameter were 1.6 mm for one month of age, 1.8 mm for three months, 2.0 mm for one year, 2.2 mm for two years, 2.4 mm for three years, 2.6 mm for four years, 2.7 mm for six years, 3.0 mm for eight years, and 3.2 mm for 10 years; and for right coronary/aorta ratios the limits were 0.17 for one month to one year, 0.18 for one to six years, 0.19 for six to 10 years, and 0.20 for more than 10 years. All patients with dilated cardiomyopathy had normal right coronary artery diameters and right coronary artery/aorta ratios (0.10-0.13). Those patients with anomalous origin of the left coronary artery from the pulmonary trunk had larger than normal right coronary artery diameter and a significant increase in the right coronary artery/aorta ratio (0.21-0.29). The presence of an anomalous left coronary artery was likely if the diameter of the right coronary artery or the right coronary artery/aorta ratio was larger than the normal 95% limits of prediction.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arjunan K., Daniels S. R., Meyer R. A., Schwartz D. C., Barron H., Kaplan S. Coronary artery caliber in normal children and patients with Kawasaki disease but without aneurysms: an echocardiographic and angiographic study. J Am Coll Cardiol. 1986 Nov;8(5):1119–1124. doi: 10.1016/s0735-1097(86)80390-4. [DOI] [PubMed] [Google Scholar]
- Askenazi J., Nadas A. S. Anomalous left coronary artery originating from the pulmonary artery. Report on 15 cases. Circulation. 1975 Jun;51(6):976–987. doi: 10.1161/01.cir.51.6.976. [DOI] [PubMed] [Google Scholar]
- Caldwell R. L., Hurwitz R. A., Girod D. A., Weyman A. E., Feigenbaum H. Two-dimensional echocardiographic differentiation of anomalous left coronary artery from congestive cardiomyopathy. Am Heart J. 1983 Oct;106(4 Pt 1):710–716. doi: 10.1016/0002-8703(83)90092-3. [DOI] [PubMed] [Google Scholar]
- Cottrill C. M., Davis D., McMillen M., O'Connor W. N., Noonan J. A., Todd E. P. Anomalous left coronary artery from the pulmonary artery: significance of associated intracardiac defects. J Am Coll Cardiol. 1985 Jul;6(1):237–242. doi: 10.1016/s0735-1097(85)80282-5. [DOI] [PubMed] [Google Scholar]
- Driscoll D. J., Nihill M. R., Mullins C. E., Cooley D. A., McNamara D. G. Management of symptomatic infants with anomalous origin of the left coronary artery from the pulmonary artery. Am J Cardiol. 1981 Mar;47(3):642–648. doi: 10.1016/0002-9149(81)90549-x. [DOI] [PubMed] [Google Scholar]
- EDWARDS J. E. THE DIRECTION OF BLOOD FLOW IN CORONARY ARTERIES ARISING FROM THE PULMONARY TRUNK. Circulation. 1964 Feb;29:163–166. doi: 10.1161/01.cir.29.2.163. [DOI] [PubMed] [Google Scholar]
- Fisher E. A., Sepehri B., Lendrum B., Luken J., Levitsky S. Two-dimensional echocardiographic visualization of the left coronary artery in anomalous origin of the left coronary artery from the pulmonary artery. Pre- and postoperative studies. Circulation. 1981 Mar;63(3):698–704. doi: 10.1161/01.cir.63.3.698. [DOI] [PubMed] [Google Scholar]
- Gutgesell H. P., Pinsky W. W., DePuey E. G. Thallium-201 myocardial perfusion imaging in infants and children. Value in distinguishing anomalous left coronary artery from congestive cardiomyopathy. Circulation. 1980 Mar;61(3):596–599. doi: 10.1161/01.cir.61.3.596. [DOI] [PubMed] [Google Scholar]
- KEITH J. D. The anomalous origin of the left coronary artery from the pulmonary artery. Br Heart J. 1959 Apr;21(2):149–161. doi: 10.1136/hrt.21.2.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Midgley F. M., Watson D. C., Jr, Scott L. P., 3rd, Kuehl K. S., Perry L. W., Galioto F. M., Jr, Ruckman R. N., Shapiro S. R. Repair of anomalous origin of the left coronary artery in the infant and small child. J Am Coll Cardiol. 1984 Dec;4(6):1231–1234. doi: 10.1016/s0735-1097(84)80142-4. [DOI] [PubMed] [Google Scholar]
- Pinsky W. W., Gillette P. C., Duff D. F., Wanderman N., Morriss J. H., Mullins C. E., McNamara D. G. Anomalous origin of left coronary artery from the pulmonary artery with ventricular septal defect. Circulation. 1978 May;57(5):1026–1030. doi: 10.1161/01.cir.57.5.1026. [DOI] [PubMed] [Google Scholar]
- Rein A. J., Colan S. D., Parness I. A., Sanders S. P. Regional and global left ventricular function in infants with anomalous origin of the left coronary artery from the pulmonary trunk: preoperative and postoperative assessment. Circulation. 1987 Jan;75(1):115–123. doi: 10.1161/01.cir.75.1.115. [DOI] [PubMed] [Google Scholar]
- Robinson P. J., Sullivan I. D., Kumpeng V., Anderson R. H., Macartney F. J. Anomalous origin of the left coronary artery from the pulmonary trunk. Potential for false negative diagnosis with cross sectional echocardiography. Br Heart J. 1984 Sep;52(3):272–277. doi: 10.1136/hrt.52.3.272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross R. S. The next 30 years--will the progress continue? Circulation. 1980 Jul;62(1):1–7. doi: 10.1161/01.cir.62.1.1. [DOI] [PubMed] [Google Scholar]
- Wesselhoeft H., Fawcett J. S., Johnson A. L. Anomalous origin of the left coronary artery from the pulmonary trunk. Its clinical spectrum, pathology, and pathophysiology, based on a review of 140 cases with seven further cases. Circulation. 1968 Aug;38(2):403–425. doi: 10.1161/01.cir.38.2.403. [DOI] [PubMed] [Google Scholar]