

Abstract
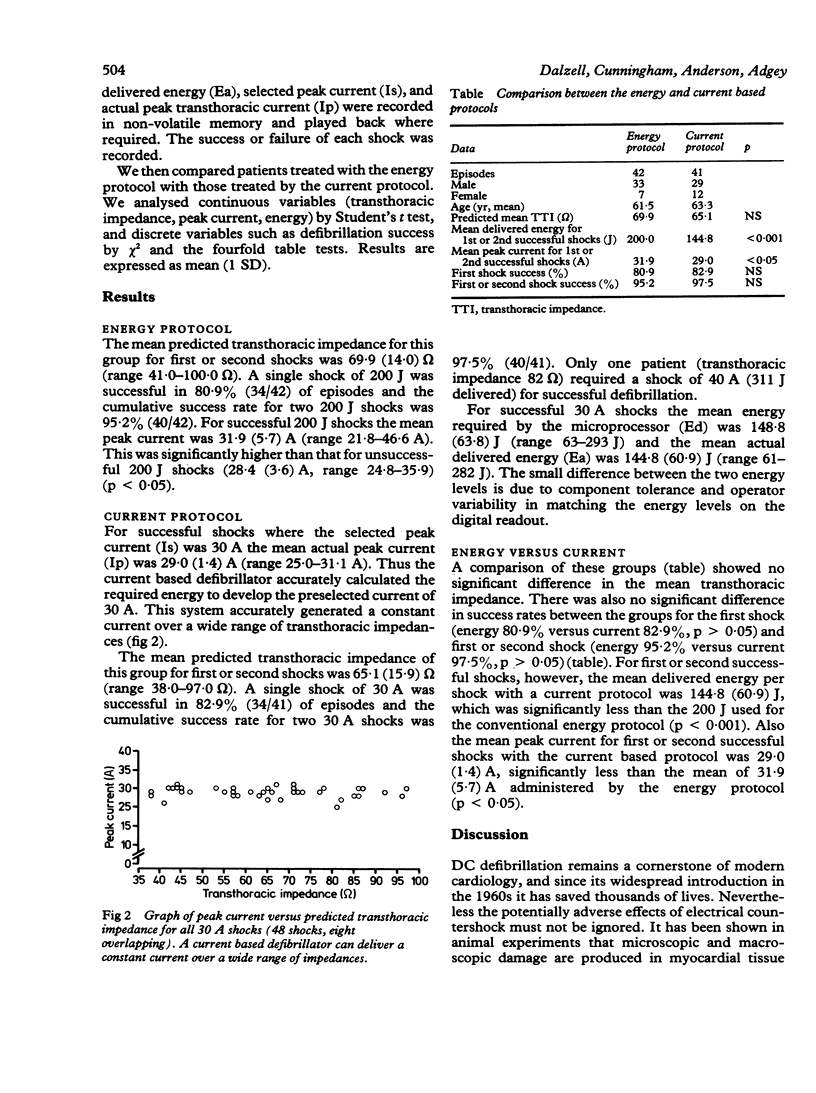
Intramyocardial current flow is a critical factor in successful ventricular defibrillation. The main determinants of intramyocardial current flow during transthoracic countershock are the selected energy and the transthoracic impedance of the patient. To optimise the success of the first shock and to titrate energy dosage according to each patient's transthoracic impedance, a microprocessor controlled current based defibrillator was developed. It was compared with a conventional energy based protocol of 200 J (delivered energy), 200 J, then 360 J if required in 42 consecutive episodes of ventricular fibrillation in 33 men and seven women. The mean (SD) predicted transthoracic impedance was 69.9 (14.0) omega. First shock success with the standard protocol was 80.9%, and first or second shock success was 95.2%. The microprocessor controlled current based defibrillator automatically measured transthoracic impedance and calculated the energy required to develop a selected current in each patient. A current protocol of 30 A, 30 A, then 40 A, if required, was used in 29 men and 12 women with 41 episodes of ventricular fibrillation. Transthoracic impedance (mean 65.1 (15.9) omega) was similar to that in the energy protocol group and success rates for first shock (82.9%) and first or second shocks (97.5%) were also similar. The mean delivered energy per shock with the current based defibrillator for first or second shock success was significantly less (144.8 J) with the energy protocol (200 J). The mean peak current of successful shocks was also significantly reduced (29.0 v 31.9 A). A current based defibrillator titrates energy according to transthoracic impedance; it has a success rate comparable to conventional defibrillators but it delivers significantly less energy and current per shock.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Geddes L. A., Tacker W. A., Jr, Schoenlein W., Minton M., Grubbs S., Wilcox P. The prediction of the impedance of the thorax to defibrillating current. Med Instrum. 1976 May-Jun;10(3):159–162. [PubMed] [Google Scholar]
- Geddes L. A., Tacker W. A., Jr Ventricular fibrillation and defibrillation. Australas Phys Eng Sci Med. 1983 Jan-Mar;6(1):9–19. [PubMed] [Google Scholar]
- Hoyt R., Grayzel J., Kerber R. E. Determinants of intracardiac current in defibrillation. Experimental studies in dogs. Circulation. 1981 Oct;64(4):818–823. doi: 10.1161/01.cir.64.4.818. [DOI] [PubMed] [Google Scholar]
- Jones J. L., Jones R. E. Postshock arrhythmias--a possible cause of unsuccessful defibrillation. Crit Care Med. 1980 Mar;8(3):167–171. doi: 10.1097/00003246-198003000-00016. [DOI] [PubMed] [Google Scholar]
- Karch S. B., Billingham M. E. Morphologic effects of defibrillation: a preliminary report. Crit Care Med. 1984 Oct;12(10):920–921. doi: 10.1097/00003246-198410000-00020. [DOI] [PubMed] [Google Scholar]
- Machin J. W. Thoracic impedance of human subjects. Med Biol Eng Comput. 1978 Mar;16(2):169–178. doi: 10.1007/BF02451918. [DOI] [PubMed] [Google Scholar]
- Monzón J. E., Guillén S. G. Current defibrillator: new instrument of programmed current for research and clinical use. IEEE Trans Biomed Eng. 1985 Nov;32(11):928–934. doi: 10.1109/TBME.1985.325625. [DOI] [PubMed] [Google Scholar]
- Patton J. N., Allen J. D., Pantridge J. F. The effects of shock energy, propranolol, and verapamil on cardiac damage caused by transthoracic countershock. Circulation. 1984 Feb;69(2):357–368. doi: 10.1161/01.cir.69.2.357. [DOI] [PubMed] [Google Scholar]
- Patton J. N., Pantridge J. F. Current required for ventricular defibrillation. Br Med J. 1979 Feb 24;1(6162):513–514. doi: 10.1136/bmj.1.6162.513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas E. D., Ewy G. A., Dahl C. F., Ewy M. D. Effectiveness of direct current defibrillation: role of paddle electrode size. Am Heart J. 1977 Apr;93(4):463–467. doi: 10.1016/s0002-8703(77)80409-2. [DOI] [PubMed] [Google Scholar]
- Van Vleet J. F., Tacker W. A., Jr, Geddes L. A., Ferrans V. J. Acute cardiac damage in dogs given multiple transthoracic shocks with a trapezoidal wave-form defibrillator. Am J Vet Res. 1977 May;38(5):617–626. [PubMed] [Google Scholar]
- Warner E. D., Dahl C., Ewy G. A. Myocardial injury from transthoracic defibrillator countershock. Arch Pathol. 1975 Jan;99(1):55–59. [PubMed] [Google Scholar]
- Weaver W. D., Cobb L. A., Copass M. K., Hallstrom A. P. Ventricular defibrillation -- a comparative trial using 175-J and 320-J shocks. N Engl J Med. 1982 Oct 28;307(18):1101–1106. doi: 10.1056/NEJM198210283071801. [DOI] [PubMed] [Google Scholar]
- Wickline S. A., Thomas L. J., 3rd, Miller J. G., Sobel B. E., Perez J. E. Sensitive detection of the effects of reperfusion on myocardium by ultrasonic tissue characterization with integrated backscatter. Circulation. 1986 Aug;74(2):389–400. doi: 10.1161/01.cir.74.2.389. [DOI] [PubMed] [Google Scholar]
- Zipes D. P., Fischer J., King R. M., Nicoll A deB, Jolly W. W. Termination of ventricular fibrillation in dogs by depolarizing a critical amount of myocardium. Am J Cardiol. 1975 Jul;36(1):37–44. doi: 10.1016/0002-9149(75)90865-6. [DOI] [PubMed] [Google Scholar]