

Abstract
Objectives:
Challenges in implementing telemedicine disproportionately affect patients served in safety-net settings. Few studies have elucidated pragmatic team-based strategies for successful telemedicine implementation in primary care, especially with a safety-net population.
Study Design:
We conducted in-depth semi-structured qualitative interviews with primary care clinicians and staff in a large urban safety-net health care system on the facilitators, challenges, and impact of implementing team workflows for synchronous telemedicine video and audio-only visits. Interviews were analyzed using modified grounded theory with multi-stage coding.
Results:
Four themes emerged from 11 interviews: (1) Having a dedicated individual preparing patients for video visits is a prerequisite for the successful introduction of video visits to patients with limited digital literacy. (2) Healthcare maintenance for video and audio-only visits benefit from standardized workflows and communication. (3) The increased flexibility and accessibility of telemedicine visits were perceived benefits to patient care, despite barriers for subsets of patients. (4) Telemedicine visits generally have a positive impact on work experience for clinicians and staff due to increased efficiency, despite audio-only visits feeling less engaging.
Conclusions:
Understanding how to strategically use team-based workflows to expand video visit access while ensuring care quality of all telemedicine visits will allow primary care practices to maximize telemedicine’s benefits to patients in the safety-net setting.
Précis:
Telemedicine in safety net primary care faces particular challenges. Consistent team-based workflows can support video visit implementation and healthcare maintenance in telemedicine visits.
Introduction:
The COVID-19 pandemic spurred health care systems to rapidly transform telemedicine from an uncommon innovation in most outpatient settings to a fundamental modality of care.1–3 Prior to reimbursement changes during the pandemic, using telemedicine to deliver synchronous care via video and audio visits was especially rare among safety-net clinics providing primary care to low-resource populations.4–6 The challenges of telemedicine implementation disproportionately affect safety-net institutions and their patients. Patients who identify as racial/ethnic minorities, have limited English proficiency, or have lower socioeconomic status face increased barriers to accessing telemedicine, including lower device, internet and data access, and limitations in digital literacy.8–15 The “digital divide” between those with and without resources to access technology-based health innovations impacts many of the same populations already affected by health inequities.16–19 Thus, the medical community has highlighted the importance of addressing equity in telemedicine access to help reduce existing disparities in health care delivery and outcomes rather than exacerbate them.20,21
Given primary care’s foundational role in improving population health and narrowing health disparities,22,23 understanding barriers and facilitators to telemedicine implementation for safety-net primary care settings is particularly relevant.24 Studies from diverse primary care settings typically depict patient or clinician perspectives on general benefits and challenges of telemedicine or patterns of utilization.25–37 One study noted that practices and clinicians drive more variation in video visit use than patients,27 suggesting that systemic factors impact telemedicine adoption. However, few studies detail telemedicine implementation in the context of primary care teams and population health management, especially with a safety-net population.
Furthermore, studies often focus on clinician or system leader perspectives,26,29–32 with fewer featuring clinic staff perspectives despite the importance of teams in primary care. Team-based care adapts roles and workflows for the optimal contribution of non-physician team members to meet patient care needs,38 and there is a need to understand how best to incorporate primary care team members into telemedicine workflows.39 To bridge these gaps and better elucidate pragmatic strategies for successful implementation of video and audio visits, we assessed clinician and staff perspectives on the facilitators, challenges, and impact of implementing team-based telemedicine workflows into safety-net primary care.
Methods:
Setting/population:
This study was conducted in a large urban clinic network serving an ethnically diverse, publicly insured patient population with a large proportion of patients primarily speaking non-English languages. In this network of 14 primary care clinic sites, telemedicine visits, defined as synchronous video or phone visits with a medical provider, were not offered as a routine form of care prior to the COVID-19 pandemic.
The three sites serving as the study setting included two community-based family medicine clinics and one internal medicine residency teaching clinic. These sites were selected due to their piloting of two telemedicine workflows. One workflow supported video visit implementation through a video visit “support pool” to which clinicians and staff could refer patients needing video visit orientation. The support pool consisted of volunteers who called patients ahead of time to guide them through the process of starting a video visit. The other workflow incorporated healthcare maintenance (preventive and chronic care tasks) into video and audio-only telemedicine visits by using standardized “virtual rooming” where medical assistants called patients to coordinate health care maintenance tasks in advance of telemedicine visits. Workflow details are provided in Appendices 1–2.
During the study period, audio-only visits represented 31.5 % of all primary care visits in the network, and 35.6% of visits at the 3 pilot sites. Video visit prevalence in the network was much lower at 0.35% of all visits. At the pilot sites, video visit prevalence was 1.3% for the community-based sites and 0.4% at the residency site.
Study design:
We performed in-depth qualitative interviews with clinicians and staff at the 3 clinics. Participants were recruited using a purposive sampling strategy to include clinicians, medical assistants, and managers with experience using the telemedicine workflows. Researchers invited eligible participants via email or phone to take part in a Zoom interview. The interview instrument was designed using stakeholder input on the relevant clinic workflows (see Appendix 3). Verbal consent was obtained at the time of the interview.
The one-on-one semi-structured interviews were conducted between October 2021 and April 2022, until the research team observed no new concepts arising from interviews, suggesting thematic saturation.40 Interviews were audio recorded, deidentified and transcribed verbatim using auto-transcription followed by review by the interviewer for accuracy. The study protocol was approved by the UCSF Institutional Review Board (Study # 11–08048).
Analysis:
Coding and thematic development were conducted in an iterative process. Interviews were dual-coded using modified grounded theory with multi-stage coding.41 Analysis was conducted by the interviewer and a trained research associate. The analysis team reviewed a sample of 3 transcripts to identify recurrent ideas and organize them into a codebook, which was piloted and refined with additional transcripts. To calibrate between coders, team members independently coded a subset of 4 transcripts, then met to identify and resolve discrepancies. They then used the codebook to code each transcript, and met weekly to review and discuss coding decisions until consensus was reached. An additional transcript was dual-coded and reconciled later in the coding process to avoid drift in inter-coder consistency. Dual-coded interviews were entered into Atlas.ti (Version 9.1.7.0, Atlas.ti Scientific Software Development, GmbH). Common themes were identified and reviewed to describe within-group and between-group variations. Final themes were selected based on prevalence among interviewees and relevance for implementing telemedicine workflows.
To organize the final themes with an implementation science lens, we used the Practical Implementation Sustainability Model (PRISM) framework, which describes multilevel contextual factors relevant to program implementation.42–44 The PRISM model is a framework to evaluate how health care interventions interact with the external environment, intervention design, implementation and sustainability infrastructure, and the multilevel recipients of an intervention to influence program reach, effectiveness, adoption, implementation, and maintenance.42–44
Results:
Of 19 people across the 3 clinics invited to take part in this study, 11 participated, for a response rate of 57.9%. These included 4 primary care clinicians, 5 medical assistants, 1 nursing manager and 1 practice manager. At least one clinician and one medical assistant from each clinic were interviewed. Participants had worked at their sites for an average of 5 years, ranging from 7 months to 10 years.
Four themes emerged, corresponding to the impact of telemedicine workflow implementation on video visit uptake, healthcare maintenance, patient care, and clinician/staff experience, respectively. Within the PRISM framework, the first two themes correspond to the implementation and sustainability infrastructure domain, while the latter two mapped to the patient and organizational perspectives and characteristics (Figure 1). Representative quotes are summarized in Table 1. Non-clinicians are referred to as “staff” for simplicity.
Figure 1.
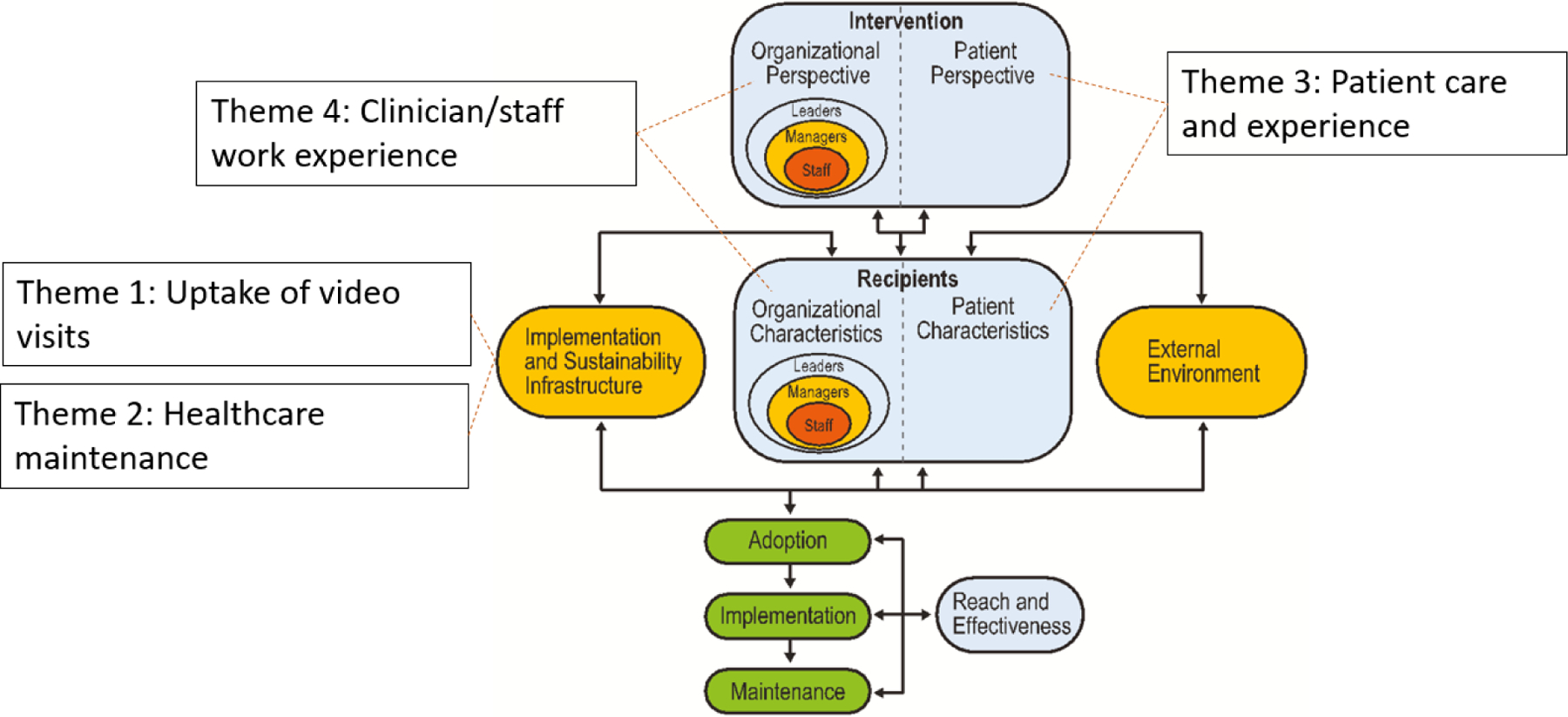
Thematic areas mapped to the The Practical Robust Implementation Sustainability Model (PRISM).42–44
Table 1.
Representative quotes by theme
| Subtheme (interviewees reporting) |
Representative quotes |
|---|---|
|
Theme 1: Having a dedicated individual preparing patients for video visits is a prerequisite for the successful introduction of video visits to patients with limited digital literacy.
PRISM domain: Implementation and sustainability infrastructure | |
|
A dedicated staff role to orient patients to using video visits was essential (4/4 clinicians, 3/7 staff) |
“At the beginning, MEAs were going the extra mile trying to help the patients get into Zoom and telling them how to do it. But it took too long, like over 20 minutes trying to go back and forth and explain over the phone, which was not doable, because the provider gets behind, patients get frustrated, the MEAs get frustrated… they don’t have time to assist them because they’re also seeing the patients that are in person. So, that has not worked.” (Staff) “I think clinicians are really looking for that support, they cannot take on the [video visit] operations. It needs to be shared across the team and what we really realized is we don’t have the workforce for this. Our team of medical assistants, front desk staff, PCP, nurses is beyond saturated and beyond capacity, and it really felt difficult to ask them to absorb new workflows and new operations around [video visits]… we need a workforce that specifically can manage [video workflows], has the skills for it, and has the capacity for it… anything that outsources some of the support that patients need.” (Clinician) |
|
The video visit support workflow was a helpful resource for supporting patients to use video visits (2/4 clinicians, 3/7 staff) |
“I’ve had several experiences offering the [video visit] support…I believe the pool is very helpful to help the patient set up.” (Staff) “All you have to do is just connect them to Zoom. And give the iPad to the provider, nothing else. You don’t have to call in advance, you don’t have to set them up, …we have [the video visit support] pool for that.” (Staff) |
|
Offering of video visits was a barrier (3/4 clinicians, 2/7 staff) |
“We’ve seen a couple people try video visits… where occasionally there’s a patient who’s really good on video or asks for it, or clinician who asks for it… we have not seen it integrated into regular scheduled visits…We’ve seen very little uptake.” (Clinician) “There really hasn’t been all that much buy in, which is something we’re working on, like basically other staff hasn’t started booking video visits. So right now we’re working on ramping up …we haven’t done enough to think about [offering them regularly].“ (Clinician) |
|
Theme 2: Healthcare maintenance for telemedicine visits benefited from standardized workflows and communication for medical assistant virtual rooming.
PRISM domain: Implementation and sustainability infrastructure | |
|
Virtual rooming workflows allowed close approximation of healthcare maintenance quality during telemedicine visits (3/4 clinicians, 4/7 staff) |
“I think since we have the workflow… we can make sure we can help patient to update all the health maintenance…[The quality is] almost the same.” (Staff) “Something like a pap I think definitely gets done more in person. But for mammo, and FIT… and the diabetic eye stuff as well, those are done I think at almost the same rate.” (Clinician) “[The chronic care and health care maintenance] wasn’t as good for sure. It was a lot more relying on the provider. So I think it’s a lot better now that we have the virtual rooming.” (Clinician) |
|
Clear workflows and communication helpful with successful implementation (2/4 clinicians, 2/7 staff) |
“Writing things down as a workflow helps, because it helps make it clear about what the job expectation is… having an algorithmic workflow about what was supposed to get documented where, that was helpful and the provider working on this got a lot of feedback so that helped get buy-in from the medical assistant team. I think the time where I saw it [improve] was when the provider and the MA teams met about it a couple of times, so heard from each side about what was working and not working, and why some of these things were important, and acknowledging where some of the difficulties were and trying to work around them, that’s where I feel the consistency was happening the most.” (Clinician) |
|
Staff shortages/ turnover are a barrier to successful implementation (3/4 clinicians, 4/7 staff) |
“We also have seen a lot of staff turnover during this time, so you know there’s some MEAs that are really comfortable and there’s others that are still learning the workflows of the clinic. We’ve had newer MEAs that are filling in, or that we’re borrowing from other clinics. So I think staffing challenges have played a role in why this continues to be variable… due to ongoing staffing challenges, our MEAs currently don’t have administrative time, which is when they would usually do these sorts of calls.” (Clinician) |
|
Logistical barriers to healthcare maintenance existed for telemedicine visits compared to in-person visits (4/4 clinicians, 4/7 staff) |
“I think it for the most part the medical assistants do call and do the virtual rooming… but it does sometimes get missed, if they’re doing something like a blood draw, or doing shots … Just because sometimes the in person things get precedent... Some of the things that we do, I would say in general, the in-person is done slightly more consistently …a lot of the time it’s because of the [flow], where the medical assistant doesn’t get to it.” (Clinician) |
|
Theme 3: The increased flexibility and accessibility of telemedicine visits were perceived benefits to patient care, despite barriers for subsets of patients.
PRISM domains: Patient perspective and characteristics | |
|
Telemedicine options provide increased flexibility and accessibility to patients (4/4 clinicians, 7/7 staff) |
“I think it’s really been great to be able to offer this flexibility, I think before it …[would] take a long time to schedule in person, and patients would have to take time or have someone watch their children, or if they’re caretakers for older adults …it was another barrier for coming in. And a blood pressure visit could be very, very simple, but then having the requirement to have them come in and find parking, that would definitely make it sort of a clunky slow process, whereas right now it feels like we’re able to respond in many cases better to our patients’ needs…it doesn’t seem like it’s burdensome for them so I feel like I’m able to offer more options [in] our flexibility and following up with people’s care.” (Clinician) “I feel like it’s really cool to give them different options. …[Some patients] are like, “I really can’t take off a day”, but they would be able to do a phone call at their breaktime or lunchtime. …they don’t have to struggle so much coming here. And you know, things happen along the way, and instead of rescheduling an appointment, they can just talk over the phone.” (Staff) |
|
Some patient subgroups have more barriers to telemedicine, including elderly or those with limited digital literacy (3/4 clinicians, 7/7 staff) |
“The older patients will not be able to log in and or have a computer, or, or they don’t know how to use their phones, or they don’t have smartphones. …We do have a lot of patients that are really hard to get a hold of on the phone. They work, so they don’t answer, or they change their numbers often or if they don’t change it, sometimes they’re not using them. …some of them don’t even have their voicemail setup so it’s hard to even leave them a message.” (Staff) |
|
Telemedicine was a more efficient format for care in certain scenarios (3/4 clinicians, 2/7 staff) |
“When we first started doing telephone visits I think there was a lot of lack of experience with what could be done over the telephone or video… as we started doing more of them we realized that we could do different types of visits that we hadn’t thought would be that useful…for example like blood pressure visits … we got the green light to allow for patients to report their blood pressures that they measure at home, we found that we could do a lot of visits actually based on over the phone or video. So I think we’ve just become more experienced and more flexible with using video visits for different things.” (Clinician) “A lot of people who we would get blood work on and then we’d be like “oh we’ll just call you if anything’s abnormal.” And then they would call in and ask to talk to the [advice line], and that was a lot of extra phone calls or extra work, and so now that we can be like, ‘Okay, we’re going to schedule a telephone call to go over your results in like a week or two,’ patients seem to really like that.” (Clinician) |
|
Improved protocols to appropriately triage among visit formats are needed (2/4 clinicians, 1/7 staff) |
“I think we did a lot of phone visits where it was clear that the person needed to come in for an urgent medical reason…for example for something like… a red eye or something that just was virtually impossible to evaluate by phone.” (Clinician) “What’s working is the doctors kind of seeing if that patient really needs to come in. And kind of triaging what the next appointment would be like. Is it really necessary to have them come in, or can we do this over the phone?” (Staff) |
|
Theme 4: Telemedicine visits generally have a positive impact on work experience for clinicians and staff due to increased efficiency, despite audio-only visits feeling less engaging.
PRISM domain: Organizational perspective and characteristics | |
|
Telemedicine brings increased flexibility or efficiency in clinic flow (4/4 clinicians, 6/7 staff) |
“For telephone or video we don’t need to wait until the patient arrives, we can call ahead of the appointment…But if all the patients are in clinic, we have to wait until the patient arrives, then we can start, or we need to find an exam room. Now the time management is much easier, or less stressful for the MEA.” (Staff) “I feel like telehealth has definitely made work less exhausting. I think because telehealth visits, for the most part, they feel like there are clearer limits and boundaries on what you can do…fewer additional agenda items get added on the telehealth visits, so it does make visits seem to go more efficiently and quickly. And that overall is helpful for my day.” (Clinician) “Sometimes if the first patient or the [next] one haven’t shown up yet, the provider can go move on to the phone visit, and get the visit started. That saves more time and gets the clinic [running] smoother.” (Staff) “The doctor can always do a phone call while you’re still waiting for patients to come in. Sometimes you have patients that run late to their appointment. And the doctor has a phone call, so she can always call that patient as she’s waiting for that in-person to come in. So it’s more flexibility.” (Staff) |
|
Involving medical assistants in healthcare maintenance for telemedicine visits is helpful to reduce burnout (3/4 clinicians) |
“Now that the MAs are doing [these workflows] it doesn’t make me feel like the entire [telemedicine ] visit is on me, when there’s a medical assistant involved in doing a component of that… initially in the pandemic it felt like those visits were actually all on the provider, and that was hard. Because you’re both trying to do a visit and do the medical assistant part.” (Clinician) “I really think the virtual rooming is super helpful. I think it’s always a balance …everyone’s really busy, but of course it’s nice for providers when the MEAs are really taking responsibility for the care gaps ...As long as they have time to do it, of course.” (Clinician) |
|
Audio-only visits feel less engaging (2/4 clinicians, 2/7 staff) |
“When I have telehealth only days …I end the day with my charts finished generally, and I don’t have as many things hanging over me after the clinic is done, that makes me feel less burnout …But there’s also a part of me, after I’m done with the phone visits…where I just don’t find it as rewarding. Like if I have a phone-only half day, it’s great, I’ll be done earlier, but I don’t feel like I’ve connected with patients in the same way, and I don’t feel like I’ve helped in the same way. …I think probably the video component would add back some of that.” (Clinician) “I found it really, really challenging to take care of complicated patients without ever meeting them in person. And I found it really, really difficult to build rapport with them and build trust with them…only over the phone. In the times that I did use video visits, I really liked it and I felt like just making a face to face connection was so helpful. And there was just something, maybe cognitively for me as a clinician, that when I could put a face and a voice to a patient, I could remember them and understand them so much better.” (Clinician) |
Note: For the purposes of the interviews, the terms telehealth and telemedicine were used interchangably to refer to synchronouse phone/video visits. Quotes were edited for length or clarity but not content.
Theme 1: Having a dedicated individual preparing patients for video visits is a prerequisite for the successful introduction of video visits to patients with limited digital literacy. (Implementation and sustainability infrastructure)
7/11 interviewees identified that having a dedicated staff role to orient patients with limited digital literacy to using video visits was essential. They described that while initially, medical assistants or clinicians helped with this, the amount of time needed to help patients through the process became unfeasible to balance with existing duties: “What we really realized is we don’t have the workforce for this. Our team of medical assistants, front desk staff, PCP, nurses is beyond saturated and beyond capacity …we need a workforce that specifically can manage [video visit orientation], has the skills for it, and has the capacity for it… anything that outsources the support patients need.” (Clinician)
5/11 interviewees described the video visit support pool as a helpful resource for supporting patients to use video visits. 2 staff noted this was limited by whether the patients were contacted in time for their video visits. 6/11 of the interviewees observed barriers at the upstream stage of offering video visits to patients: “There really hasn’t been all that much buy in … basically other staff hasn’t started booking video visits. …we haven’t done enough to think about [offering them regularly].” (Clinician)
Theme 2: Healthcare maintenance for telemedicine visits benefited from standardized workflows and communication for medical assistant virtual rooming. (Implementation and sustainability infrastructure)
All interviewees from the community-based sites (3 clinicians and 4 staff) reported that the medical assistant virtual rooming workflows improved healthcare maintenance quality for telemedicine visits. 4 interviewees described that with the virtual rooming workflows, the perceived difference between in-person and telemedicine preventive care was small or negligible: “Since we have the workflow… we can make sure we help patients update all [their] health maintenance…[The quality is] almost the same. (Staff)
Among the community-based clinics, 3 clinicians and 1 staff member commented that standardized virtual rooming workflows facilitated consistent completion of healthcare maintenance tasks for telemedicine visits: “Writing things down as a workflow helps, it helps make it clear about what the job expectation is …Where I saw it [improve] was when the provider and the MA teams met about it, heard from each side about what was working and not working, why some of these things were important, and acknowledging where some of the difficulties were and trying to work around them.” (Clinician)
In contrast, interviewees from the teaching clinic site reported more challenges with consistency of the workflows, with variability in how often preventive care was completed for telemedicine visits.
7/11 interviewees from all three clinics described medical assistant staffing shortages or turnover as a barrier to successfully implementing standardized preventive care workflows for telemedicine visits.
7/11 of interviewees reported logistical barriers to healthcare maintenance being done for telemedicine visits compared to in-person visits. These included patients needing to be scheduled to return for in-person preventive care tasks (i.e. vaccines or cervical cancer screening), and perceived decreased priority of virtual rooming workflows when medical assistants were busy with in-person patient tasks.
Theme 3: The increased flexibility and accessibility of telemedicine visits were perceived benefits to patient care, despite barriers for subsets of patients. (Patient perspective and characteristics)
11/11 interviewees observed increased visit flexibility and accessibility as key patient care benefits of having telemedicine options, especially for younger patients, patients less able to take time off from work or caregiving responsibilities, and those with mobility difficulties. For example, one clinician reported, “It’s really been great to be able to offer this flexibility… we’re able to respond in many cases better to our patients’ needs.” (Clinician) Many staff members and clinicians specifically noted the benefits of being able to switch from in-person to a telemedicine visit when last minute circumstances would have otherwise led to a no show or cancellation: “[Patients] don’t have to struggle so much coming here…[if] things happen along the way, instead of rescheduling an appointment, they can just talk over the phone.” (Staff)
10/11 interviewees also noted patient subgroups with more barriers to telemedicine, including elderly patients and patients with low digital literacy.
4/11 interviewees also observed that telemedicine visits seemed to be more useful than in-person visits for care delivery in certain scenarios. For example, 2/4 clinicians described telemedicine as a good format for discussion of results with patients, when previously this might only be done at the patient’s proactive request. Another clinician discussed improved uses of telemedicine visits over time: “When we first started doing telephone visits I think there was a lot of lack of experience with what could be done… as we started doing more of them we realized that we could do different types of visits that we hadn’t thought would be that useful, for example like blood pressure visits …we found that we could do a lot of visits over the phone or video.” (Clinician)
3/11 interviewees also identified the need to improve protocols to identify the most appropriate visit format. 2/4 clinicians raised concerns about delays when an issue is attempted to be addressed over telemedicine but actually requires an in-person evaluation: “We would see patients who had been mis-triaged to a telephone for a red eye or something that just was virtually impossible to evaluate by phone.” (Clinician)
Theme 4: Telemedicine visits generally have a positive impact on work experience for clinicians and staff due to increased efficiency, despite audio-only visits feeling less engaging. (Organizational perspective and characteristics)
10/11 interviewees described telemedicine visits as bringing more efficiency into the clinic schedule and flow. 4/7 staff specifically described the flexible timing of telemedicine visits as helpful: “We don’t need to wait until the patient arrives, we can call ahead… time management is much easier, or less stressful for the MEA.” (Staff)
3/4 clinicians reported that telemedicine visits had a positive impact on burnout or work exhaustion due to these benefits: “Telehealth has definitely made work less exhausting… visits seem to go more efficiently and quickly. And that overall is helpful for my day.” (Clinician)
The 3 clinicians from the community-based sites described the involvement of medical assistants in healthcare maintenance for telemedicine visits as helpful for reducing burnout: “It doesn’t make me feel like the entire visit is on me… initially in the pandemic it felt like those visits were actually all on the provider, and that was hard, because you’re both trying to do a visit and do the medical assistant part.” (Clinician)
2/4 clinicians and 2/7 staff also commented that phone visits had less sense of connection or relationship compared to in-person visits. The clinicians reported that this resulted in less joy in practice, but also that video visits could be more rewarding than audio-only visits: “I found it really difficult to build rapport with [new patients] and build trust...over the phone. In the times that I did use video visits, I really liked it and I felt like just making a face to face connection was so helpful… I could remember them and understand them so much better.” (Clinician)
Discussion:
We identified key facilitators and barriers for the strategic incorporation of two telemedicine workflows in busy, under-resourced safety-net primary care clinics. Pertinent to the implementation and sustainability infrastructure domain of PRISM, we found that optimizing telemedicine in public delivery systems requires dedicated support staff to orient patients to video visits. A few prior studies have called for devoting resources to providing digital navigators to overcome video visit barriers,35,45–47 and this study provides supporting evidence for this need, especially in settings where limited digital literacy is more common.
Our findings also suggest that dedicated navigation support is necessary but insufficient without additional workflows to consistently offer video visit options to patients. There has been evidence of lower rates of offering video versus audio-only options to certain populations – e.g., Hispanic, non-primary English speaking, and Medi-caid/Medicare dually eligible patients -- even after controlling for access to a smartphone/tablet and home internet.5 This is consistent with literature on disparities in offering other technological health innovations, such as patient portals.48 Thus, further development and evaluation of workflows to ensure standardized offering of video visit options and support will be an important step in operationalizing video visits effectively and equitably.20
Consistent use of team-based workflows is also an important contributor to the delivery of healthcare maintenance during both video and audio visits. One study in a large integrated health system found that patients with telemedicine exposure had better rates of chronic disease and counseling-based preventive care metrics,49 suggesting that these components of primary care can translate effectively to telemedicine formats. This study elaborates on prior literature on using team-based care in telemedicine by highlighting the importance of workflows specifically standardizing healthcare maintenance in telemedicine visits.39 Interviewees from the community-based sites that reported higher consistency of these workflows noted that clear role expectations and opportunities for team communication faciliated successful implementation. Clinicians from these sites also described that the healthcare maintenance workflows helped reduce exhaustion or burnout, further supporting the value of investment in team-based telemedicine workflows.
In the patient and organizational domains of PRISM, our findings aligned with those previously reported in non-safety-net settings,28–30,33–36 with flexibility, accessibility, and efficiency being major benefits of telemedicine visits despite certain limitations and barriers. For safety net populations where patients commonly face increased structural barriers to accessing in-person health care, such as transportation issues or limited ability to take time off from work, the flexibility of telemedicine options may provide particularly important accessibility benefits. The interviewee descriptions of using telemedicine effectively for certain visits and for efficient clinic flow support further development of best practices for strategically triaging to telemedicine visit formats.
Limitations of this study include relatively limited staff and clinician experience with video visits compared to audio visits, due to low video visit volume during the study course. Further perspectives obtained with scaled-up video visit volumes could offer additional insights into impact of telemedicine on care delivery, for example, whether video visits would ameliorate the reduction in clinicians’ perceived rapport and engagement during audio-only visits. Also, our sample size was small, although our patient and organizational perspective findings corroborated well with other studies, supporting our assessment of thematic saturation.
This work highlights the importance of designating and funding specific staff to provide telemedicine support for video visits, as well as sufficient staffing to consistently implement healthcare maintenance workflows for telemedicine visits of both phone and video formats. Equitably supporting patients to engage in video visits, while simultaneously ensuring high-quality preventive and chronic care on both phone and video visits, will be important as decisions evolve around reimbursement for different visit types.13,50 Further research should examine optimal workflows for consistently and equitably offering video visits to patients in safety-net settings. The noted difficulties with consistently implementing team-based workflows in the large teaching clinic compared to the community-based sites in this study suggest that future work should give attention to the particular nuances of telemedicine implementation in more complex primary care settings, such as residency clinics.
Clinicians and staff in this study recognized the challenges, but also the value and facilitators of providing telemedicine care to often marginalized populations. Continuing to understand how to strategically use team-based workflows to expand video visit access while ensuring care quality of all telemedicine visits will allow primary care practices to maximize telemedicine’s flexibility and benefits to patients in the safety-net setting.
Takeaway points:
Clinicians and staff in safety net primary care clinics recognized that team-based workflows can help expand video visit access and improve healthcare maintenance in telemedicine visits.
Dedicated staff providing navigation support for video visits are necessary for safety net populations to access video visits.
Workflows to consistently and equitably offer video visit options to patients are also needed.
Standardized team-based workflows and communication facilitate healthcare maintenance in telemedicine visits.
Ensuring high-quality preventive and chronic care on both phone and video visits will be important as patients continue to face barriers to video visit access.
Funding sources:
This work was supported by the Tides Foundation, in collaboration with the Center for Care Innovations and California Health Care Foundation [TF2007-093073], and the University of California, San Francisco Population Health and Health Equity Scholars Program.
Appendix 1. Video visit support pool script

Appendix 2. Telemedicine healthcare maintenance workflow

Appendix 3: Provider/staff interview guide
Questions
What type of work do you currently do in the clinic?
- Let’s start with some background on how telehealth is being used at your clinic.
- How often are different visit types are being used currently [in person, video, phone]? Which types are being used most/least?
- How has this changed since the beginning of the pandemic?
- For a typical in person visit, how is preventive care (like cancer screenings or immunizations) usually done for a patient? What about for a phone visit? For a video visit?
- Probe: Who starts/prompts this care? When/how?
- How has this changed since the beginning of the pandemic?
- For a typical phone visit, how is chronic care (like getting diabetes care for patients with diabetes) usually done? What about for a video visit?
- Probe: Who starts/prompts this care? When/how?
- How does this differ from an in person visit?
- How has this changed since the beginning of the pandemic?
- At your clinic, how do you typically prepare patients for their phone visits (e.g., informed them what to expect from the phone visit, remind them to have their home monitoring/medications/questions prepared, other)?
- Who does this? When/how?
- How has this changed since the beginning of the pandemic?
- At your clinic, how do you typically prepare patients for their telehealth video visits (e.g., helped them download an app, walk through how to log on for a visit, other)?
- Who does this? When/how?
- How has this changed since the beginning of the pandemic?
In addition to what we just discussed in terms of changes between use of telehealth at the start of the pandemic and now [LIST CHANGES DISCUSSED ABOVE], in what other ways has your clinic’s use of telehealth evolved?
- How has the response to telehealth been at your clinic from the perspective of [interviewee’s role]?
- How has it impacted your daily work?
- Has this changed over the course of the pandemic?
- Are there some telehealth workflows in the clinic that are working well? Others that are NOT working well? Why/why not?
- In what ways, if any, have the clinic’s telehealth workflows made your job easier?
- In what ways, if any, have the clinic’s telehealth workflows made your job harder?
- In your view, how has the shift to telehealth impacted:
- Quality of care
- Access to care for different patient populations (probe: unstable housing, non-English speakers, undocumented, uninsured)
- Feeling exhausted or burned out at work?
Anything important we have left out of the discussion that would help us understand the impact of telehealth at your clinic?
Contributor Information
Marianna Kong, University of California, San Francisco.
Rachel Willard-Grace, University of California, San Francisco.
Elaine Khoong, University of California, San Francisco.
Anjana Sharma, University of California, San Francisco.
Monjori Mukerjee, University College Dublin.
George Su, University of California, San Francisco.
Delphine Tuot, University of California, San Francisco.
References:
- 1.Mehrotra A, Ray K, Brockmeyer DM, Barnett ML, Bender JA. Commentary; Rapidly converting to “virtual practices”: outpatient care in the era of Covid-19. NEJM Catalyst, Innovations in Care Delivery. Published Apr 1, 2020. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0091 [Google Scholar]
- 2.Keesara S, Jonas A, Schulman K. Covid-19 and health care’s digital revolution. N Engl J Med 2020;382:e82. [DOI] [PubMed] [Google Scholar]
- 3.Shachar C, Engel J, Elwyn G. Implications for telehealth in a postpandemic future: regulatory and privacy issues. JAMA 2020;323:2375–6. [DOI] [PubMed] [Google Scholar]
- 4.Lin CC, Dievler A, Robbins C, Sripipatana A, Quinn M, Nair S. Telehealth In Health Centers: Key Adoption Factors, Barriers, And Opportunities. Health Aff (Millwood) 2018. Dec;37(12):1967–1974. [DOI] [PubMed] [Google Scholar]
- 5.Benjenk I, Franzini L, Roby D, Chen J. Disparities in Audio-only Telemedicine Use Among Medicare Beneficiaries During the Coronavirus Disease 2019 Pandemic. Med Care. 2021. Nov 1;59(11):1014–1022. doi: 10.1097/MLR.0000000000001631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Uscher-Pines L, Sousa J, Jones M, et al. Telehealth Use Among Safety-Net Organizations in California During the COVID-19 Pandemic. JAMA 2021;325(11):1106–1107. doi: 10.1001/jama.2021.0282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Beheshti L, Kalankesh LR, Doshmangir L, Farahbakhsh M. Telehealth in Primary Health Care: A Scoping Review of the Literature. Perspect Health Inf Manag 2022. Jan 1;19(1):1n. [PMC free article] [PubMed] [Google Scholar]
- 8.Khoong EC, Butler BA, Mesina O, Su G, DeFries TB, Nijagal M, Lyles CR. Patient interest in and barriers to telemedicine video visits in a multilingual urban safety-net system. J Am Med Inform Assoc 2020. Nov 4:ocaa234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goel MS, Brown TL, Williams A, Hasnain-Wynia R, Thompson JA, Baker DW. Disparities in enrollment and use of an electronic patient portal. Journal of general internal medicine. 2011;26(10):1112–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.George S, Hamilton A, Baker RS. How do low-income urban African Americans and Latinos feel about telemedicine? A diffusion of innovation analysis. International journal of telemedicine and applications. 2012;2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gordon NP, Hornbrook MC. Differences in access to and preferences for using patient portals and other eHealth technologies based on race, ethnicity, and age: a database and survey study of seniors in a large health plan. Journal of medical Internet research. 2016;18(3):e50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jaffe DH, Lee L, Huynh S, Haskell TP. Health Inequalities in the use of telehealth in the United States in the lens of COVID-19. Popul Health Manag 2020;23:368–77. [DOI] [PubMed] [Google Scholar]
- 13.Khoong EC. Policy considerations to ensure telemedicine equity. Health Affairs. 2022;41(5): 643–646. doi: 10.1377/hlthaff.2022.00300 [DOI] [PubMed] [Google Scholar]
- 14.Lyles CR, Wachter RM, Sarkar U. Focusing on digital health equity. JAMA 2021;326(18):1795–6. [DOI] [PubMed] [Google Scholar]
- 15.Zahnd WE, Bell N, Larson AE. Geographic, racial/ethnic, and socioeconomic inequities in broadband access. J Rural Health. 2022. Jun;38(3):519–526. doi: 10.1111/jrh.12635. [DOI] [PubMed] [Google Scholar]
- 16.Ye S, Kronish I, Fleck E, Fleischut P, Homma S, Masini D, Moise N. Telemedicine Expansion During the COVID-19 Pandemic and the Potential for Technology-Driven Disparities. J Gen Intern Med 2021. Jan;36(1):256–258. doi: 10.1007/s11606-020-06322-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Smith B, Magnani JW. New technologies, new disparities: The intersection of electronic health and digital health literacy. Int J Cardiol 2019. Oct 1;292:280–282. doi: 10.1016/j.ijcard.2019.05.066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hsu J, Huang J, Kinsman J, Fireman B, Miller R, Selby J, et al. Use of e-Health services between 1999 and 2002: A growing digital divide. Journal of the American Medical Information Association. 2005;12(2):164–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Agency for Healthcare Research and Quality. 2018 National Health Quality and Disparities Report. AHRQ Pub. No. 19–0070. 2019. Accessed Nov 16, 2020. https://www.ahrq.gov/research/findings/nhqrdr/nhqdr18/index.html. [Google Scholar]
- 20.Lyles CR, Sharma AE, Fields JD, Getachew Y, Sarkar U, Zephyrin L. Centering Health Equity in Telemedicine. Ann Fam Med 2022. Jul-Aug;20(4):362–367. doi: 10.1370/afm.2823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nouri S, Khoong EC, Lyles CR, Karliner L. Addressing equity in telemedicine for chronic disease management during the Covid-19 Pandemic. NEJM Catalyst, Innovations in Care Delivery. Published May 4, 2020. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0123 [Google Scholar]
- 22.Starfield B, Shi L, Macinko J. Contribution of primary care to health systems and health. Milbank Q 2005;83(3):457–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.National Academies of Sciences, Engineering, and Medicine. Implementing High-Quality Primary Care: Rebuilding the Foundation of Health Care. The National Academies Press; 2021. [PubMed] [Google Scholar]
- 24.Shuemaker JC, Phillips RL, Newton WP. Clinical quality measures in a post-pandemic world: measuring what matters in family medicine (ABFM). Ann Fam Med 2020;18(4):380–382. doi: 10.1370/afm.2564 [DOI] [Google Scholar]
- 25.Gomez T, Anaya YB, Shih KJ, Tarn DM. A Qualitative Study of Primary Care Physicians’ Experiences With Telemedicine During COVID-19. J Am Board Fam Med 2021. Feb;34(Suppl):S61–S70. doi: 10.3122/jabfm.2021.S1.200517. [DOI] [PubMed] [Google Scholar]
- 26.Sharma AE, Khoong EC, Sierra M, Rivadeneira NA, Nijagal MA, Su G, Lyles CR, DeFries T, Tuot DS, Sarkar U. System-Level Factors Associated With Telephone and Video Visit Use: Survey of Safety-Net Clinicians During the Early Phase of the COVID-19 Pandemic. JMIR Form Res 2022. Mar 10;6(3):e34088. doi: 10.2196/34088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rodriguez JA, Betancourt JR, Sequist TD, Ganguli I. Differences in the use of telephone and video telemedicine visits during the COVID-19 pandemic. Am J Manag Care. 2021. Jan;27(1):21–26. doi: 10.37765/ajmc.2021.88573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Srinivasan M, Asch S, Vilendrer S, Thomas SC, Bajra R, Barman L, Edwards LM, Filipowicz H, Giang L, Jee O, Mahoney M, Nelligan I, Phadke AJ, Torres E, Artandi M. Qualitative Assessment of Rapid System Transformation to Primary Care Video Visits at an Academic Medical Center. Ann Intern Med 2020. Oct 6;173(7):527–535. doi: 10.7326/M20-1814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Donnelly C, Mills C, Gill S, Mehta K, Ashcroft R. The experience of primary care teams during the early phase of COVID-19: A qualitative study of primary care practice leaders in Ontario, Canada. BMC Prim Care. 2022. Nov 22;23(1):294. doi: 10.1186/s12875-022-01907-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gomez T, Anaya YB, Shih KJ, Tarn DM. A Qualitative Study of Primary Care Physicians’ Experiences With Telemedicine During COVID-19. J Am Board Fam Med 2021. Feb;34(Suppl):S61–S70. doi: 10.3122/jabfm.2021.S1.200517. [DOI] [PubMed] [Google Scholar]
- 31.Rabinowitz G, Cho LD, Benda NC, Goytia C, Andreadis K, Lin JJ, Horowitz C, Kaushal R, Ancker JS, Poeran J. The Telemedicine Experience in Primary Care Practices in the United States: Insights From Practice Leaders. Ann Fam Med 2023. May-Jun;21(3):207–212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Etz RS, Solid CA, Gonzalez MM, Britton E, Stange KC, Reves SR. Telemedicine in Primary Care: Lessons Learned About Implementing Health Care Innovations During the COVID-19 Pandemic. Ann Fam Med 2023. Jul-Aug;21(4):297–304. doi: 10.1370/afm.2979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hall TL, Connelly L, Staton EW, Holtrop JS, Sieja A, Knierim K, Holmstrom H. Points of Concordance, Points of Discordance: A Qualitative Examination of Telemedicine Implementation. J Am Board Fam Med 2022. May-Jun;35(3):517–526. doi: 10.3122/jabfm.2022.03.210325. [DOI] [PubMed] [Google Scholar]
- 34.Cunningham AT, Felter J, Smith KR, Sifri R, Arenson C, Patel A, Kelly EL. Burnout and Commitment After 18 Months of the COVID-19 Pandemic: A Follow-Up Qualitative Study with Primary Care Teams. J Am Board Fam Med 2023. Jan 2:jabfm.2022.220226R1. doi: 10.3122/jabfm.2022.220226R1. [DOI] [PubMed] [Google Scholar]
- 35.Leung PB, Nahid M, Rusli M, et al. Factors associated with never having had a video visit. J Am Board Fam Med 2022;35:634–637. [DOI] [PubMed] [Google Scholar]
- 36.Wray CM, Tang J, Shah S, Nguyen OK, Keyhani S. Sociodemographics, social vulnerabilities, and health factors associated with telemedicine unreadiness among US adults. J Gen Intern Med 2021;1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lindenfeld Z, Berry C, Albert S, Massar R, Shelley D, Kwok L, Fennelly K, Chang JE. Synchronous Home-Based Telemedicine for Primary Care: A Review. Med Care Res Rev 2023. Feb;80(1):3–15. [DOI] [PubMed] [Google Scholar]
- 38.Ghorob A, Bodenheimer T. Sharing the care to improve access to primary care. N. Engl. J. Med 2012;366(21):1955–1957. [DOI] [PubMed] [Google Scholar]
- 39.Sinsky CA, Jerzak JT, Hopkins KD. Telemedicine and Team-Based Care: The Perils and the Promise. Mayo Clin Proc 2021. Feb;96(2):429–437. doi: 10.1016/j.mayocp.2020.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Marshall MN. Sampling for qualitative research. Fam Pract 1996(6);13:522–5. [DOI] [PubMed] [Google Scholar]
- 41.Strauss A, Corbin J. Basics of Qualitative Research. Thousands Oaks, CA: Sage Publications. 1998. [Google Scholar]
- 42.RE-AIM [Internet]. Welcome to RE-AIM and PRISM: implementation in context; 2021. [cited 2021 June 16]. Available from: https://www.re-aim.org/. [Google Scholar]
- 43.Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf 2008. Apr;34(4):228–43. doi: 10.1016/s1553-7250(08)34030-6. [DOI] [PubMed] [Google Scholar]
- 44.McCreight MS, Rabin BA, Glasgow RE, Ayele RA, Leonard CA, Gilmartin HM, Frank JW, Hess PL, Burke RE, Battaglia CT. Using the Practical, Robust Implementation and Sustainability Model (PRISM) to qualitatively assess multilevel contextual factors to help plan, implement, evaluate, and disseminate health services programs. Transl Behav Med 2019. Nov 25;9(6):1002–1011. doi: 10.1093/tbm/ibz085. [DOI] [PubMed] [Google Scholar]
- 45.Garg A, Goyal S, Thati R, Thati N. Implementation of Telemedicine in a Tertiary Hospital-Based Ambulatory Practice in Detroit During the COVID-19 Pandemic: Observational Study. JMIR Public Health Surveill 2021. Jan 8;7(1):e21327. doi: 10.2196/21327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Anaya YB, Bañuelos Mota A, Hernandez GD, Osorio A, Hayes-Bautista DE. Post-Pandemic Telehealth Policy for Primary Care: An Equity Perspective. J Am Board Fam Med 2022. May-Jun;35(3):588–592. doi: 10.3122/jabfm.2022.03.210509. [DOI] [PubMed] [Google Scholar]
- 47.Wisniewski H, Gorrindo T, Rauseo-Ricupero N, Hilty D, Torous J. The Role of Digital Navigators in Promoting Clinical Care and Technology Integration into Practice. Digit Biomark. 2020. Nov 26;4(Suppl 1):119–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Richwine C, Johnson C, Patel V. Disparities in patient portal access and the role of providers in encouraging access and use. J Am Med Inform Assoc 2023. Jan 18;30(2):308–317. doi: 10.1093/jamia/ocac227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Baughman DJ, Jabbarpour Y, Westfall JM, et al. Comparison of Quality Performance Measures for Patients Receiving In-Person vs Telemedicine Primary Care in a Large Integrated Health System. JAMA Netw Open. 2022;5(9):e2233267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Westby A, Nissly T, Gieseker R, Timmins K, Justesen K. Achieving Equity in Telehealth: “Centering at the Margins” in Access, Provision, and Reimbursement. J Am Board Fam Med 2021. Feb;34(Suppl):S29–S32. doi: 10.3122/jabfm.2021.S1.200280. [DOI] [PubMed] [Google Scholar]