

Abstract
Loop diuretics are a cornerstone in the management of fluid overload in critically ill patients; however, their use is often complicated by variable pharmacokinetics and the phenomenon of diuretic resistance. This narrative review comprehensively examines the pharmacokinetic properties of loop diuretics and discusses the implications of altered pharmacokinetics due to factors such as organ dysfunction, fluid shifts, and concomitant medications, highlighting the challenges in achieving therapeutic targets. Furthermore, we explore the adverse events associated with loop diuretic administration, including electrolyte imbalances and ototoxicity. The review delves into the concept of diuretic resistance, exploring its multifactorial origins, including altered pharmacodynamics and increased compensatory mechanisms. Various strategies to overcome diuretic resistance are presented, including combination therapy with other diuretics, optimizing dosing regimens, and utilizing novel pharmacological agents. Given the complexity of loop diuretic therapy in critically ill patients, a tailored approach is crucial for optimizing fluid management and mitigating adverse effects. This review aims to inform clinicians about the nuances of loop diuretic use in critical care settings, providing insights into pharmacological strategies and clinical considerations essential for enhancing patient outcomes.
Key Points
| LDs are widely prescribed medications characterized by distinct pharmacokinetic and pharmacodynamic profiles, yet their use remains largely stereotypical. However, the careful consideration of dosing strategies and the modality of administration are essential in critically ill patients to provide clinical benefits. |
| Diuretic resistance occurs when a patient with fluid overload becomes refractory to conventional diuretic therapy, regardless of whether the patient is naïve to diuretics or has been previously treated. Managing diuretic resistance involves key challenges: (a) identifying the correct diuretic dose required to exceed the efficacy threshold and (b) developing strategies to maintain effective diuresis when there is little-to-no response, even with increased dosing. |
| The absence of high-quality studies with sufficient power does not allow for the recommendation of the coadministration of furosemide and albumin or suggest continuous intravenous infusion instead of the bolus. |
Introduction
Furosemide is one of the most frequently prescribed medications in the intensive care unit (ICU) [1, 2], known for several indications, including the management of congestive heart failure, treatment of fluid overload, maintenance of fluid balance, and evaluation of renal function through the furosemide stress test. While its impact on patient mortality is minimal, the use of furosemide to maintain fluid balance has been shown to reduce hospital readmissions in patients with congestive heart failure [3].
Furosemide was the first loop diuretic (LD) approved by the US Food and Drug Administration (FDA) in 1966, followed by ethacrynic acid (EA) in 1967, bumetanide in 1983, and torsemide in 1993 [4]. These agents are indicated for the treatment of clinical manifestations of heart, liver, or renal failure. Although there is limited evidence demonstrating that furosemide is superior to other loop diuretics, it remains the preferred choice within its class [1]. In addition, LD have a favorable therapeutic index, and their adverse effects can be easily managed or mitigated owing to their practicality and safety profile.
The purpose of this article is to critically reevaluate this class of medications, which are frequently administered in clinical practice without a standardized algorithm. Despite the widespread use of LD, there are few guidelines regarding the most appropriate diuretic strategy in critically ill patients [5]. By examining current practices and identifying gaps in the existing approaches, this article aims to highlight the need for evidence-based guidelines that can improve patient outcomes and minimize risks associated with individualized treatment plans.
Material and Methods of Literature Search
We performed a comprehensive search of the PubMed, OVID, and Embase databases, filtering papers with the following keywords: “loop diuretics,” “adults intensive care unit,” “adult critically ill patients”, “diuretic resistance,” and “PK/PD characteristics.” Titles and abstracts were screened, and reference lists were reviewed to identify additional relevant articles. Selected articles were further evaluated for clinical aspects such as the mechanism of action, pharmacokinetics of loop diuretics, diuretic resistance, and strategies to overcome it. The search was limited to articles published from 1 January 2000 till October 31 2024, only in English, involving humans in critical care units. All references were downloaded for consolidation, and duplicates were eliminated before further analysis. Owing to the volume of literature, four experienced authors in critical care medicine (C.Z., Y.L., A.V., and J.F.) conducted the research and determined the eligibility of all studies identified in the initial search. A consensus among three authors (V.S., G.G., and R.P.) approved the final list. Ultimately, this narrative review analyzed 25 articles published in English involving only humans in critical care units.
Discussion
Mechanism of Action
Diuretics are mainly classified by their site of action within the nephron, which closely relates to their efficacy. Except for spironolactone and its analogs, all diuretics act on the luminal side of tubular cells. Their secretion into the tubular lumen involves distinct transport mechanisms: loop diuretics (LDs) and thiazides rely ontorganic anion Transporters (OATs) and multidrug resistance-associated protein 4, while amiloride and triamterene use organic cation transporters (OCTs). LDs and hydrochlorothiazide are taken up at the basolateral membrane via these transporters and delivered to the tubular fluid through apical transporters in a two-step transcellular process. A small amount of furosemide is also filtered through the glomerulus; however, owing to its high protein binding (> 98%), only a minimal fraction undergoes filtration. This strong plasma protein binding supports its tubular secretion and enhances its diuretic effect. In contrast, spironolactone and other aldosterone antagonists are not transported by organic transporters but instead act on cytosolic receptors. LDs inhibit the cotransport isoform 2 of sodium (Na+), potassium (K+), and chloride ions (Cl−) (NKCC-2) across the cell membrane along the ascending limb of the loop of Henle and the macula densa [6, 7] (Fig. 1). The NKCC-2 is electrically neutral and becomes activated when all four binding sites are occupied. Once Na+ enters the tubular cell from one side, it is subsequently extruded into the systemic circulation through the Na+/K+-ATPase-dependent transporter located in the basolateral membrane, thereby creating a favorable electrochemical gradient. For Na+ to enter the cell from the luminal side, where its concentration is lower, it relies on Na+/K+-ATPase pumps that actively expel Na+ from the opposite side of the tubular cell [6–8]. The luminal membrane of the thick segment of the loop of Henle exhibits high permeability to K+ owing to the presence of renal outer medullary potassium (ROMK) channels on the luminal membrane of the tubular cells, which serve as apical pathways for recycling potassium. On the basolateral side, chloride channels (CLCKb) facilitate the passage of Cl− across the basolateral membrane. At this stage, the potential difference across the membrane achieves a state of equilibrium, resulting in hyperpolarization for K+. Conversely, at the opposite pole of the cell, the basolateral membrane’s permeability to Cl− leads to depolarization. This combination of hyperpolarization of the luminal membrane and depolarization of the basolateral membrane gives rise to a potential difference of approximately 10 mV, with the luminal side being positive and the interstitial space being negative. This potential difference repels divalent cations such as Ca2+ and Mg2+; however, it also serves as an important driving force for their transport via paracellin-1 through the paracellular route [7, 8].
Fig. 1.

The mechanism of action of the Loop diuretics. ROMK renal outer medullary potassium
The loop of Henle is virtually impermeable to water, as it lacks aquaporins in contrast to other segments of the proximal tubule. Consequently, water is not reabsorbed at this level, while sodium and chloride are symported, leading to a dilution of tubular fluid by 25–35% owing to the removal of Na+ and Cl− [6, 8]. If the ion symport mechanism is blocked by LDs, this percentage of Na+ is not reabsorbed, remaining in the tubular fluid as it progresses to the collecting duct. There, it may be reabsorbed to a limited extent under the influence of aldosterone, eliminating K+. The Na+ that remains in the tubular fluid osmotically drags water along with it, which accounts for the diuretic effect of LD as well as side effects such as hyponatremia, hypokalemia, hypocalcemia, and hypomagnesemia [7, 8].
Several inhibitors of the NKCC-2 symporter exhibit additional effects in the proximal tubule. For instance, furosemide possesses weak carbonic anhydrase-inhibiting activity, resulting in increased urinary excretion of bicarbonate (HCO3−) and phosphate. In contrast, EA and bumetanide lack carbonic anhydrase-inhibiting activity [9].
Pharmacokinetics of Loop Diuretics
Table 1 shows the pharmacokinetic characteristics of LDs. Furosemide, bumetanide, EA, and torsemide are rapidly absorbed following oral administration, achieving peak concentrations (Cmax) approximately 30 to 120 min postingestion. In contrast, when administered intravenously, the effects of furosemide and EA are nearly immediate [8–10].
Table 1.
The pharmacokinetic characteristics of loop diuretics
| Characteristic | Furosemide | Bumetanide | Torsemide | Ethacrynic acid |
|---|---|---|---|---|
| Bioavailability (%) | 10–100 | 80–100 | 80–100 | 100 |
| Affected by food | Yes | Yes | No | No |
| Half-life (h) | 1.5–2 | 1 | 3–4 | 30–160 |
| In renal dysfunction | 2.8 | 1.6 | 4–5 | |
| In hepatic dysfunction | 2.5 | 2.3 | 8 | |
| In heart failure | 2.7 | 1.3 | 6 | |
| Onset (min) oral | 30–60 | 30–60 | 30–60 | 30 |
| Onset (min) intravenous | 5 | 2–3 | 10 | 5 |
| Protein bound (%) | 91–98 | 97 | 99 | 98 |
| Metabolism | Kidney 85%, 40% furosemide glucuronide (active), and saluamine 4-chloro 5-sulfamoylanthranilic acid; liver 10–15% | 45% secreted unchanged; urinary and biliary metabolites are formed by oxidation | Liver +++ (CYP2C8 and CYP2C9 hydroxylation, oxidation and reduction); 20% unchanged in urine | Liver |
| Elimination | Urine | Urine 80%, bile 2% | Feces 70-80%, urine 20-30% | Bile, urine |
| Oral to intravenous conversion§§ | 2:1 | 1:1 | 1:1 | 1:1 |
| Suggested enteral dose (bolo mg)/maintenance dose (mg/daily) [19] | 20–40 mg/40–240 mg | 0.5–1 mg/1–5 mg | 5–10mg/10–200mg | 50–100 mg/50–400 mg given one to four times daily, though typical doses are 50–200 mg daily |
| Suggested i.v. dose bolo/maintenance dose (mg/daily) and frequency [19, 20]a | 10–20 mg/80–600 mg |
1 mg/0.5–1 mg every 8–24 h Max 10 mg/day |
10 mg/10–20 mg Max 200 mg/day |
50 mg or 0.5–1 mg/kg ×1 dose Max 100 mg ×1 dose (if necessary, may do 1 additional dose 8–12 h later) |
CYP cytochrome, i.v., intravenous
aExcluding Furosemide stress test
The bioavailability of torsemide and bumetanide after oral administration is around 80%, while EA has an approximate bioavailability of 100%. Conversely, furosemide’s bioavailability is considerably lower and highly variable, ranging from 10% to 90%, and is significantly influenced by concurrent food intake. Consequently, when transitioning from intravenous to oral administration, the doses of torsemide and bumetanide should remain unchanged, whereas the dose of furosemide should be doubled to account for its variable absorption [8, 10].
The half-life (t½) of Furosemide is relatively short, at approximately 90 min; however, its duration of action can extend up to about 6 h following oral administration. This extended duration is likely due to gastrointestinal absorption occurring at a rate slower than its half-life, a phenomenon referred to as “absorption limited kinetics.” This limitation does not apply to torsemide and bumetanide, both of which exhibit rapid oral absorption. Indeed, although food slows and lowers the peak plasma concentration of bumetanide, it does not significantly affect the total amount absorbed or excreted, indicating only a minor impact on its overall bioavailability—especially when compared with furosemide [11]. Similarly, coadministration of torsemide with a high-fat, high-carbohydrate meal reduces its absorption rate without altering the extent of absorption, half-life, or renal clearance. These modest pharmacokinetic changes do not influence the drug’s diuretic efficacy, as the relationship between urinary sodium excretion and drug levels, as well as total electrolyte and urine output, remain unaffected [12].
EA has a half-life of approximately 30 min, which can vary from 12 to 160 min following intravenous administration [8, 10]. Similar to furosemide, the diuretic effect of EA is relatively short-lived. The drug is efficiently metabolized and eliminated by both the liver and kidneys, thereby preventing accumulation, even with multiple doses [9].
Approximately 40% of a furosemide dose is excreted unchanged in the urine and undergoes metabolic modification through glucuronidation in the kidneys. In contrast, torsemide and bumetanide are primarily eliminated via the liver before urinary excretion. For furosemide, metabolic variations among patients can influence the drug’s half-life, particularly in individuals with acute kidney injury (AKI) or chronic kidney disease (CKD), where renal excretion and glucuronidation may be impaired. Conversely, the half-lives of torsemide and bumetanide remain relatively stable in patients with renal dysfunction. After intravenous administration of EA, approximately one-third is excreted by the liver, while two-thirds are eliminated by the kidneys. The drug recovered from the urine is roughly distributed into three fractions: the unchanged parent compound, a cysteine adducts, and an unstable, chemically uncharacterized metabolite [9].
LDs display a steep dose–response curve. Below a certain plasma concentration (threshold), the natriuretic and diuretic effects are minimal; however, above this threshold, the response increases rapidly. At higher concentrations, a plateau is reached, wherein further increases in plasma concentration do not correspond to an enhanced effect. This dose–response relationship underpins the recommendation to double the dose if there is no response to initial diuretic administration [7, 8, 13].
In critically ill patients, however, the threshold for reaching the plateau is difficult to define owing to altered extracellular volume expansion and pathologic organ functions, which affects the pharmacokinetics and pharmacodynamics of the diuretics. For instance, the area under the curve for a specific intravenous dose of furosemide and a theoretical equipotent oral dose may be comparable; nevertheless, the time to surpass the natriuretic threshold can vary owing to pathological conditions affecting this threshold. This variability explains why intravenous doses of LDs that achieve higher peak levels may remain effective when equipotent oral doses lose efficacy [8, 13].
Indeed, the natriuretic threshold, defined as the luminal concentration necessary to elicit a significant diuretic response, depends not only on pharmacokinetics parameters but also on the actual patient’s clinical conditions or comorbidities. In critically ill patients, fluid accumulation, organ edema, and impaired cardiac or renal function notably impact LD efficacy. Intestinal edema, as occurs also in heart failure or nephrotic syndrome, but simply owing to fluid accumulation, can impair the enteral absorption of LDs, necessitating intravenous administration to avoid diuretic resistance. Furthermore, as in heart failure, an impaired cardiac index leads to altered renal perfusion, increased intraparenchymal pressure, and neurohormonal activation. These conditions result in diuretic resistance (DR), and the necessity of higher doses or combination therapies to overcome diminished responsiveness.
In acute or chronic kidney disease, decreased glomerular filtration rate (GFR) and competition with endogenous anions for OAT-mediated secretion elevate the threshold dose needed for efficacy. About 15–20% of the furosemide dose is delivered into the tubular fluid in patients with stage 5 CKD. This diminished tubular secretion is due to the elevated level of endogenous organic anions that interfere with furosemide secretion via organic acid transporters in the proximal tubule [14].
Hypoalbuminemia reduces the plasma concentration of loop diuretics available for secretion into the renal tubules. Additionally, the substantial protein loss in urine (proteinuria) might lead to loop diuretics binding to albumin within the tubular fluid, potentially reducing their availability to interact with the Na+-K+-2Cl− cotransporter in the thick ascending limb [15].
Collectively, these conditions underscore the importance of understanding the complex interplay between LD pharmacology and pathophysiological states to optimize therapeutic outcomes.
LDs can cause hearing loss in human at very high doses > 1 g or infusion rate > 250 mg/h; this risk is greater in patients with GFR < 20 ml/min/1.73m2 or concurrent administration of other ototoxic drugs (e.g., gentamicin and cisplatin) [7]. Furosemide ototoxicity involves NKCC-2 cotransporters in the inner ear stria vascularis encoded by the gene SLC12A2 and seems to be more linked to speed to infusion and the peak levels than the total dose. Deafness usually occurs 10–20 min after intravenous administration and is usually reversible and of short duration (1–24 h) [9].
LDs led to distinct pathological alterations in the cochlea, notably the development of oedematous spaces within the stria vascularis epithelium. This process results in a swift decline of the endolymphatic potential and ultimately causes the loss of cochlear microphonic potential, summating potential, and compound action potential. These diuretics also affect strial adenylate cyclase and Na+/K+-ATPase while inhibiting the Na+-K+-2Cl− cotransporter found in the stria vascularis. However, recent findings suggest that one of the earliest observable effects in vivo is a reduction of blood flow to the vessels supplying the cochlear lateral wall. Although EA does not result in damage to the stria vascularis under laboratory conditions, the changes noted in Na+/K+-ATPase and the Na+-K+-2Cl− cotransporter in living organisms may be secondary effects arising from ischemia and anoxia in the stria. Additionally, recent studies have revealed the presence of renin in pericytes surrounding the stria arterioles, indicating that diuretics may cause localized vasoconstriction through the secretion of renin and subsequent formation of angiotensin. The tight junctions of the blood–cochlea barrier serve to protect the cochlea from toxic molecules and pathogens. However, when diuretics provoke a temporary ischemic state, this barrier can become compromised, allowing harmful substances or pathogens to penetrate the cochlea [16]. These factors may account for instances of permanent hearing loss following the administration of EA, contributing to its diminished clinical application [9]. Angiotensin-converting enzyme (ACE) inhibitors may provide a protective effect against cochlear ischemia and damage caused by ototoxic drugs, such as cisplatin [17]. Blocking this system could reduce ischemic damage and oxidative stress in the cochlea, potentially lowering the risk of ototoxicity. However, their protective effect in the context of furosemide ototoxicity has not been extensively explored. Oxygen inhalation, the coadministration of triamterene (a potassium-sparing diuretic), iodinated benzoic acid derivatives such as diatrizoate and probenecid, and organic acids such as sodium salicylate and penicillin G have been demonstrated to attenuate the ototoxicity from diuretics. Despite these potential interventions, pharmacological treatments are generally not of major clinical significance, as the ototoxicity caused by diuretics is typically short-lived [18].
LDs can cause hyperuricemia and hyperglycemia and can increase the level of low-density lipoprotein cholesterol and triglycerides while decreasing high-density lipoprotein cholesterol. All these actions are reversible upon cessation of administration. Allergic interstitial nephritis may occur with chronic use of sulfa-containing LDs [9].
Furosemide and bumetadine contain a sulfonamide moiety, whereas torsemide is a sulfonyl urea. In patients who are suspected to be allergic to sulfa, EA should be used because it does not contain sulfa [9].
Diuretic Resistance
Diuretic resistance occurs when a patient with fluid overload becomes refractory to conventional diuretic therapy, regardless of whether the patient is naïve to diuretics or has been previously treated. The factors contributing to diuretic resistance can be categorized into three main groups: (1) pharmacokinetic properties of the drugs, (2) coadministration of other medications that inhibit the action of loop diuretics, and (3) coexistence of organ failure, particularly acute or chronic renal failure.
Owing to their short half-life, initial natriuresis typically diminishes within the first 3–6 h following administration, resulting in an interval (16–21 h) in which the diuretic effect is essentially absent, but sufficient for the kidneys to compensate the acute electrolyte and water losses that occur after diuretic administration [8, 23]. At steady state, postdiuretic Na+ retention may be observed, characterized by excretion rates falling below baseline levels once the effects of the previously administered diuretic have waned. This condition persists until a subsequent diuretic dose is administered. Following any therapeutically active dose, natriuresis tends to decrease as extracellular fluid volume diminishes, a phenomenon commonly referred to as “braking,” which is particularly noted in patients undergoing chronic diuretic treatment. The phenomenon underscores the presence of both functional and structural adaptive processes in critically ill patients [8, 23]. Specifically, there is an upregulation of proteins involved in renal Na+ absorption [23]. Consequently, the increased release of Na+ into the distal tubular segments, which occurs owing to the inhibition of NKCC-2 in the ascending limb of the loop of Henle, subsequently stimulates the activity of Na+/Cl− channels. This process is also linked to an elevated number of Na+/K+-ATPase pumps in the basolateral membrane of tubular cells. These structural modifications significantly impair the effectiveness of LDs, particularly in patients with chronic diuretic therapy [8, 23]. In summary, the braking phenomenon represents a remodeling of the distal nephron, characterized by hypertrophy and hyperplasia resulting from increased Na+ release, elevated levels of angiotensin II and aldosterone, and alterations in K+ balance. The consequences of this remodeling include an enhanced transport capacity of the distal tubules, enabling them to compete more effectively with the ascending loop of Henle [8, 23]. Consequently, as more Na+ is extruded from the loop, a greater amount is reabsorbed distally, leading to a decrease in net natriuresis [8, 23]. Functional compensatory response is postdiuretic sodium retention, where the kidneys avidly retain sodium after the diuretic effect of a LD has waned, counteracting the initial sodium loss. This can be triggered by the activation of the renin–angiotensin–aldosterone system (RAAS) and the sympathetic nervous system in response to the diuretic-induced volume changes. Increased proximal tubular sodium reabsorption has also been observed as a compensatory mechanism that can limit the overall efficacy of loop diuretics. Chloride depletion, a potential consequence of LD therapy, can contribute to diuretic braking by stimulating sodium reabsorption in the distal nephron. Furthermore, the increased delivery of sodium to the macula densa as a result of loop diuretic action can trigger tubuloglomerular feedback, leading to a reduction in GFR and renal blood flow, which may subsequently limit the diuretic efficacy. These compensatory renal mechanisms highlight the dynamic interplay between loop diuretics and the kidney’s intrinsic regulatory systems, often contributing to diuretic resistance and necessitating adjustments in treatment strategies (Fig. 2). To mitigate this adaptive response and restore diuretic efficacy, it is beneficial to add a second diuretic from a different class, such as a thiazide diuretic.
Fig. 2.
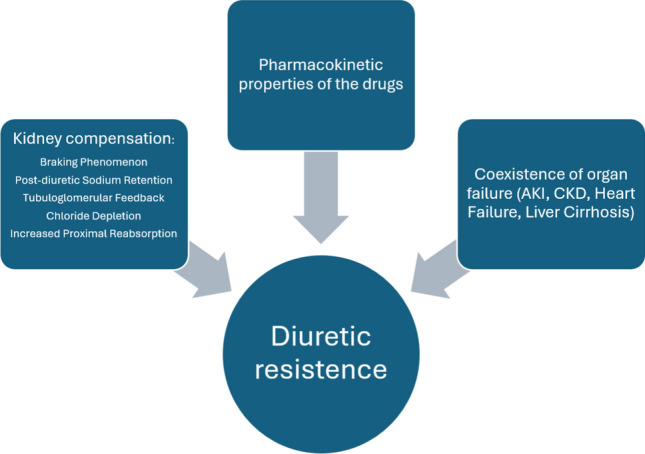
Mechanisms of diuretic resistance. The kidney employs several compensatory mechanisms that can influence the response to loop diuretics, particularly with chronic use. Furthermore, coadministration of other medications, and coexistence of organ failure, particularly acute or chronic renal failure, can affect the loop diuretics’ effects
OAT type 1 and 3 can be inhibited by coadministered drugs, particularly nonsteroidal antiinflammatory drugs (NSAIDs). The mechanism by which LD inhibit Na+ reabsorption involves their action at the level of the macula densa. This inhibition stimulates the secretion of renin and promotes the production of prostaglandins through cyclooxygenase 2. Prostaglandin E2, in turn, acts on the renal tubules, enhancing natriuresis and inhibiting Na+ reabsorption along the ascending limb of the loop of Henle and within the collecting duct. However, NSAIDs block this prostaglandin-mediated action [7, 8, 13, 23]. Reported half-maximal inhibitory concentration values indicate comparable affinities of OAT1 and OAT3 for diuretics, cephalosporins, and NSAIDs, whereas OAT2 shows generally lower affinity for these compounds [24, 25]. Furosemide and bendroflumethiazide have been shown to inhibit tracer uptake via mOat1 and mOat3 in a concentration-dependent manner, consistent with their behavior as substrates of these transporters [25]. Consequently, drug–drug interactions at OAT1 and OAT3—particularly with coadministered β-lactam penicillins or thiazide diuretics—may impair renal drug clearance and increase the risk of adverse effects. Moreover, furosemide-induced alterations in tubular ion transport may further influence the reabsorption of other positively charged compounds, such as certain antibiotics, through effects on the luminal electrochemical gradient.
LDs also inhibit NKCC-1 channels, which are expressed in vascular smooth muscle cells. This inhibition contributes to afferent arteriolar vasodilation, helping to maintain glomerular filtration rate (GFR) even in the context of reduced extracellular volume. Importantly, this compensatory adaptation relies on the production of prostaglandins, an effect that can be compromised using NSAIDs [13, 23].
Several studies have reported a high incidence of DR, ranging from 50% to 70%, in patients with renal syndromes [3]. OATs in the ascending limb of the loop of Henle and the proximal convoluted tubule also mediate the reabsorption of uric acid and weak anions. Kidney failure and other conditions leading to persistent renal hypoperfusion can result in the progressive accumulation of organic anions, which compete with diuretics for active secretion and transport to their sites of action. Additionally, in the context of metabolic acidosis, the depolarization of the cell membrane may further reduce the activity of OATs [23].
How Can We Face Diuretic Resistance?
From a practical perspective, two different issues arise in the management of critically ill patients regarding diuretic therapy: (1) determining the appropriate diuretic dose needed to surpass the efficacy threshold and (2) defining strategies to sustain diuresis in the absence of a response despite escalating doses. One previously mentioned approach involves combining LDs with a thiazide diuretic to mitigate the braking phenomenon. Alternatively, LDs can be administered alongside albumin, or they may be given as boluses rather than through continuous infusion. These strategies are inherently grounded in pharmacokinetic principles.
Diuretic resistance (DR) is associated with an elevated risk of mortality [26], particularly in patients in the ICU with severe heart failure or fluid overload. The assessment of DR relies on a combination of the clinician’s subjective evaluation of inadequate drug efficacy and quantitative indicators from the patient, such as urine output. However, there is presently no universally accepted definition of DR [3] that can be consistently applied in clinical practice or utilized in the design of clinical studies.
In a retrospective study that used the publicly available deidentified Medical Information Mart for Intensive Care III (MIMIC-III) database, Coté et al. considered adult patients admitted to ICU for more than 24 h and treated with a dose of furosemide greater than 1 mg/kg/24 h. They explored the effectiveness of the following interventions: mode of furosemide administration (continuous infusion versus intermittent), incremental dosing of diuretics, use of albumin, or addition of a second class of diuretics. The primary endpoint of the study was diuresis within the first 24 h, while secondary efficacy endpoints included fluid balance over 24 h and weight change at 24 and 48 h. Safety endpoints encompassed electrolyte abnormalities and acid–base balance. The results showed that doses of furosemide greater than 2, 3, or 4 mg/kg/die resulted in a progressive increase in urine output over 24 h. Additionally, continuous infusion was associated with greater urine output over 24 h, improved fluid balance, and greater weight loss within the same period [27]. The addition of a second diuretic—such as thiazides, mineralocorticoid antagonists, or carbonic anhydrase inhibitors—resulted in a modest increase in 24-h urine output and varied according to the class of diuretic administered, with thiazide diuretics demonstrating a more pronounced urine output. Additionally, the combination of furosemide with albumin was associated with a positive fluid balance, a reduction in diuresis over the 24-h period, and no significant change in body weight [27].
Continuous infusion of furosemide represents a strategic approach to mitigate the effects of the drug’s pharmacokinetics. There are several compelling reasons to consider continuous infusion of furosemide: it minimizes fluctuations in serum concentration, addresses the limitations associated with the drug’s short half-life, facilitates more predictable and consistent diuresis, mitigates the risk of developing diuretic resistance by eliminating the postdiuretic rebound effect that may activate compensatory renal mechanisms, and ultimately enhances hemodynamic stability in the patient.
In a meta-analysis focusing on cardiac patients, the primary efficacy endpoint of diuretic therapy was the change in body weight, despite this parameter is typically regarded as a secondary endpoint in clinical practice. Notably, continuous infusion of furosemide was shown to be more effective than bolus administration [28].
Ng et al., in a meta-analysis involving patients in the ICU, assessed not only the different methods of furosemide administration (continuous infusion versus bolus administration) but also an adaptive dosing strategy based on the observed diuretic response (increasing or decreasing the dose as necessary). They found that the dose-adjustment strategy was superior in enhancing diuresis compared with the mere comparison of continuous infusion versus bolus administration, especially in hemodynamically unstable patients. Furthermore, subgroup analyses revealed that this targeted therapeutic approach was associated with a reduction in ICU length of stay compared with patients who did not receive this strategy [29].
It is crucial to highlight that all studies included in these meta-analyses identified ICU and hospital mortality as primary endpoints related to the administration of furosemide, whether given as a continuous infusion or in bolus form. Consequently, the sample size calculations in these studies were based on these endpoints, rather than on measures of diuretic efficacy. Furthermore, the target populations exhibited considerable heterogeneity, as did the protocols for furosemide administration.
Another explored strategy to mitigate DR involves the administration of furosemide in combination with albumin. LDs, particularly furosemide, are bound by approximately 95% to plasma proteins, with albumin as principal transporter. In cases of hypoalbuminemia, the distribution volume of furosemide increases, resulting in a reduced amount of albumin-bound furosemide available for the proximal tubules. As a result, in patients with severe hypoalbuminemia, the efficacy of the diuretic may be compromised. Elevating albumin levels prior to or concurrently with furosemide administration may enhance its therapeutic effect.
Studies have indicated that the infusion of albumin alone can lead to increased diuresis, likely owing to an elevation in intravascular volume, improving hemodynamic parameters [30] and consequent increase in the estimated GFR (eGFR) and the effective renal plasma flow [31, 32]. A meta-analysis encompassing only randomized controlled trials, albeit heterogeneous in terms of target populations, compared the combined administration of furosemide and albumin to albumin alone. This analysis revealed that coadministration resulted in an increase in urine volume of 231.0 ml within the first 8 h and 276.6 ml within 24 h postadministration. A similar enhancement was noted in natriuresis, with Na+ excretion increasing by 15.9 mEq within the first 8 h and 23.4 mEq over 24 h [33]. The doses of furosemide and albumin utilized across the individual studies exhibited considerable variability, and the meta-analysis did not demonstrate a significant association between dosage and therapeutic effect. Specifically, in studies where high doses (> 100 mg) of furosemide were administered, no apparent benefit was observed from the concomitant use of albumin.
However, in a subgroup analysis, patients with nephrotic syndrome showed a significant increase in diuresis both in the initial 8 h (378.4 ml) and over a 24-h period (420.5 ml), without significant changes in natriuresis [33]. This finding is inconsistent with previous research, which proposed a physiological rationale indicating that albumin administration might be counterproductive in such patients. Specifically, albuminuria could result in the albumin accumulation in the renal tubules, binding free and biologically active furosemide, thereby inhibiting the interaction with its site of action [34].
Furosemide dosages have been reported to range between 40 mg and 220 mg, accompanied by equimolar amounts of salt-poor albumin [35]. The administration of both albumin and furosemide either occurred simultaneously or involved albumin being given before furosemide. The specific dosage of furosemide and the timing of albumin administration relative to furosemide are critical factors; the administration of higher doses of furosemide may reduce the effectiveness of albumin. Additionally, it has been shown that albumin reaches its peak impact on intravascular volume expansion within 30 to 60 min after administration [35]. Therefore, giving albumin prior to furosemide may enhance diuresis more effectively than using furosemide alone, as evidenced by findings from Na et al. [36]
In summary, the effect of albumin on loop diuretic response is context-dependent. In hypoalbuminemic states, the reduced availability of albumin-bound furosemide may impair delivery to the tubular lumen, diminishing its diuretic effect. Clinical studies and meta-analyses suggest that the coadministration of albumin with furosemide may enhance diuresis in hypoalbuminemic patients, particularly those with nephrotic syndrome, by restoring effective renal drug delivery and improving hemodynamics [33].However, albuminuria may lead to tubular accumulation of albumin, which can sequester furosemide intraluminally and limit its action. In contrast, in patients with normal serum albumin levels, no significant benefit has been observed from albumin coadministration [38]. Thus, the impact of albumin on loop diuretic efficacy reflects a balance between improved systemic delivery and potential intratubular binding effects [33].
In an adult ICU setting, furosemide is occasionally substituted with EA administration when its effectiveness diminishes.
EA is declared 30% less potent than furosemide [7], even though the superiority of one agent over the other in terms of the improvement of urine output or serum creatinine has not been demonstrated [37]. By contrast, furosemide was found more effective in the reduction of B-type natriuretic peptide, blood urea nitrogen, and weight after 3 days of continuous infusion to manage fluid overload in cardiac intensive care [37].
Numerous randomized controlled trials and meta-analyses have indicated that achieving sustained diuresis is more effective with continuous administration rather than with intermittent bolus dosing. However, the efficacy of bolus administration is influenced by both the timing and frequency of the doses, as close-set boluses may coincide with the half-life of furosemide. Notably, there appear to be no significant differences between the two administration methods regarding mortality, length of hospital stay, or incidence of electrolyte disturbances [38].
Conclusions
LDs are widely prescribed medications characterized by distinct pharmacokinetic and pharmacodynamic profiles, yet their use remains largely stereotypical. To enhance their therapeutic efficacy, clinicians should be more attentive to these unique properties. In the absence of high-quality studies with sufficient power, clear recommendations regarding the coadministration of furosemide and albumin or the preference for continuous versus bolus administration cannot be made (Table 2).
Table 2.
Final recommendations on loop diuretic use in critically ill patients
| Recommendation | Details |
|---|---|
| Individualized dosing | Tailor dosing based on patient-specific factors (e.g., organ function, fluid balance, and comorbidities) rather than relying on stereotypical regimens. To optimize dose–response while minimizing risk of toxicity, a ceiling furosemide dose of 6 mg/kg/day is usually desired |
| Threshold identification | Carefully identify the minimum effective dose needed to surpass the natriuretic threshold, especially in resistant patients. To optimize dose–response while minimizing risk of toxicity, a ceiling furosemide dose of 6 mg/kg/day is usually desired |
| Use of combination therapy | Combine loop diuretics with thiazides or other classes in resistant cases to overcome the braking phenomenon |
| Continuous vs. bolus infusion | Continuous infusion may offer more stable diuretic response and fewer fluctuations; however, evidence for mortality benefit is lacking |
| Albumin co-administration | Consider albumin only in hypoalbuminemic patients, particularly those with nephrotic syndrome; avoid routine use |
| Monitor for resistance | Regularly assess response via urine output and fluid balance; escalate therapy when resistance is observed |
| Caution in hypoalbuminemia and kidney dysfunction | Adjust dose and route (prefer i.v.) to compensate for reduced drug delivery and bioavailability |
| No clear superiority between loop diuretics | Furosemide remains first-line owing to familiarity; ethacrynic acid may be used when sulfa allergy is suspected, but it is less potent |
Acknowledgements
Our deepest gratitude to the esteemed Italian American, Leonardo Domiziano Zanza, for his invaluable assistance in revising and editing our manuscript.
Declarations
Funding
Open access funding provided by Università degli Studi di Roma Tor Vergata within the CRUI-CARE Agreement.
Conflict of Interest
All authors declared to have no financial or nonfinancial interests that are directly or indirectly related to this work.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Availability of Data and Material
The data presented in this study are available upon request from the corresponding author.
Code Availability
Not applicable.
Author Contributions and Consent for Publication
F.F. conceptualized and drafted the review. C.Z., Y.L., A.V., and J.F. performed the paper selection, quality assessment, and data extraction. R.P. and G.G. edited the draft of review. V.S. and M.T. adjudicated in case of disagreement. All authors reviewed, edited, and consented to publish the review.
References
- 1.Giamello JD, Savioli G, Longhitano Y, Ferrari F, D’Agnano S, Esposito C, Tesauro M, Zanza C. The role of acetazolamide in critical care and emergency medicine. J Geriatr Cardiol. 2024;21(11):E1085–95. 10.26599/1671-5411.2024.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.McCoy IE, Chertow GM, Chang TI-H. Patterns of diuretic use in the intensive care unit. PLoS ONE. 2019;14: e0217911. 10.1371/journal.pone.0217911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fernandez Hazim C, Duarte G, Urena AP, Jain S, Mishra R, Vittorio TJ, Rodriguez-Guerra M. Diuretic resistance and the role of albumin in congestive heart failure. Drugs Context. 2023;12:1–8. 10.7573/dic.2023-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ferrari F, Milla P, Sartori M, Zanza C, Tesauro M, Longhitano Y, De Silvestri A, Abbruzzese C, De Rosa S, Lassola S, Samoni S, Brendolan A, Zanella M, Scaravilli V, Grasselli G, Arpicco S, Ronco C. Antibiotics removal during continuous renal replacement therapy in septic shock patients: mixed modality versus “expanded haemodialysis.” Clin Pharmacokinet. 2024;63(8):1167–76. 10.1007/s40262-024-01397-w. (Epub 2024 Aug 5 PMID: 39102092). [DOI] [PubMed] [Google Scholar]
- 5.Escudero VJ, Mercadal J, Molina-Andújar A, Piñeiro GJ, Cucchiari D, Jacas A, Carramiñana A, Poch E. New insights into diuretic use to treat congestion in the icu: beyond furosemide. Front Nephrol. 2022. 10.3389/fneph.2022.879766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Puschett JB. Pharmacological classification and renal actions of diuretics. Cardiology. 1994;84:4–13. 10.1159/000176450. [DOI] [PubMed] [Google Scholar]
- 7.La Via L, Marino A, Cuttone G, Nunnari G, Deana C, Tesauro M, Voza A, Planinsic R, Longhitano Y, Zanza C. Critical care pharmacology of antiretroviral therapy in adults. Eur J Drug Metab Pharmacokinet. 2025;50(2):105–18. 10.1007/s13318-025-00934-7. Epub 2025 Feb 12. PMID: 39937350; PMCID: PMC11882694. [DOI] [PMC free article] [PubMed]
- 8.Ellison DH. Clinical pharmacology in diuretic use. Clin J Am Soc Nephrol. 2019;14:1248–57. 10.2215/CJN.09630818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Molnar J, Somberg JC. The clinical pharmacology of ethacrynic acid. Am J Ther. 2009;16:86–92. 10.1097/MJT.0b013e318195e460. [DOI] [PubMed] [Google Scholar]
- 10.Halstenson CE, Matzke GR. Bumetanide: a new loop diuretic (Bumex, Roche Laboratories). Drug Intell Clin Pharm. 1983;17:786–97. 10.1177/106002808301701101. [DOI] [PubMed] [Google Scholar]
- 11.McCrindle JL, Li Kam Wa TC, Barron W, Prescott LF. Effect of Food on the absorption of frusemide and bumetanide in man. Br J Clin Pharmacol. 1996;42:743–6. 10.1046/j.1365-2125.1996.00494.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kramer WG. Effect of food on the pharmacokinetics and pharmacodynamics of torsemide. Am J Ther. 1995;2:499–503. 10.1097/00045391-199506000-00010. [DOI] [PubMed] [Google Scholar]
- 13.Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, LeWinter MM, Deswal A, Rouleau JL, Ofili EO, et al. Diuretic strategies in patients with acute decompensated heart failure. New Eng J Med. 2011;364:797–805. 10.1056/NEJMoa1005419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tamargo J, Segura J, Ruilope LM. Diuretics in the treatment of hypertension. Part 2: loop diuretics and potassium-sparing agents. Expert Opin Pharmacother. 2014;15:605–21. 10.1517/14656566.2014.879117. [DOI] [PubMed] [Google Scholar]
- 15.Shankar SS, Brater DC. Loop diuretics: from the Na-K-2Cl transporter to clinical use. Am J Physiol Renal Physiol. 2003;284:F11–21. 10.1152/ajprenal.00119.2002. [DOI] [PubMed] [Google Scholar]
- 16.Ding D, Liu H, Qi W, Jiang H, Li Y, Wu X, Sun H, Gross K, Salvi R. Ototoxic effects and mechanisms of loop diuretics. J Otol. 2016;11:145–56. 10.1016/j.joto.2016.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shalkami A-GS, Hassan MIA, Abd El-Ghany AA. Perindopril regulates the inflammatory mediators, nf-κb/tnf-α/il-6, and apoptosis in cisplatin-induced renal dysfunction. Naunyn Schmiedebergs Arch Pharmacol. 2018;391:1247–55. 10.1007/s00210-018-1550-0. [DOI] [PubMed] [Google Scholar]
- 18.Oishi N, Talaska AE, Schacht J. Ototoxicity in dogs and cats. Vet Clin N Am. 2012;42:1259–71. 10.1016/j.cvsm.2012.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Felker GM, Mentz RJ. Diuretics and ultrafiltration in acute decompensated heart failure. J Am Coll Cardiol. 2012;59:2145–53. 10.1016/j.jacc.2011.10.910. [DOI] [PubMed] [Google Scholar]
- 20.Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, et al. ACCF/AHA guideline for the management of heart failure. Circulation. 2013;2013:128. 10.1161/CIR.0b013e31829e8776. [Google Scholar]
- 21.Zanza C, Saglietti F, Tesauro M, Longhitano Y, Savioli G, Balzanelli MG, Romenskaya T, Cofone L, Pindinello I, Racca G, Racca F. Cardiogenic Pulmonary Edema in Emergency Medicine. Adv Respir Med. 2023;91(5):445–63.10.3390/arm91050034. PMID: 37887077; PMCID: PMC10604083. [DOI] [PMC free article] [PubMed]
- 22.Desai A, Voza G, Paiardi S, Teofilo FI, Caltagirone G, Pons MR, Aloise M, Kogan M, Tommasini T, Savevski V, Stefanini G, Angelini C, Ciccarelli M, Badalamenti S, De Nalda AL, Aghemo A, Cecconi M, Martinelli Boneschi F, Voza A, Humanitas COVID-19 task force. The role of anti-hypertensive treatment, comorbidities and early introduction of LMWH in the setting of COVID-19: a retrospective, observational study in Northern Italy. Int J Cardiol. 2021;1(324):249–54. 10.1016/j.ijcard.2020.09.062. (Epub 2020 Sep 25. PMID: 32980434; PMCID: PMC7516574). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ellison DH. Diuretic resistance: physiology and therapeutics. Semin Nephrol. 1999;19:581–97. [PubMed] [Google Scholar]
- 24.Zanza C, Facelli V, Romenskaya T, Bottinelli M, Caputo G, Piccioni A, Franceschi F, Saviano A, Ojetti V, Savioli G, Longhitano Y. Lactic Acidosis Related to Pharmacotherapy and Human Diseases. Pharmaceuticals (Basel). 2022 Nov 30;15(12):1496. doi: 10.3390/ph15121496 [DOI] [PMC free article] [PubMed]
- 25.Vallon V, Rieg T, Ahn SY, Wu W, Eraly SA, Nigam SK. Overlapping in vitro and in vivo specificities of the organic anion transporters oat1 and oat3 for loop and thiazide diuretics. Am J Physiol Renal Physiol. 2008;294:F867–73. 10.1152/ajprenal.00528.2007. [DOI] [PubMed] [Google Scholar]
- 26.Neuberg GW, Miller AB, O’Connor CM, Belkin RN, Carson PE, Cropp AB, Frid DJ, Nye RG, Pressler ML, Wertheimer JH, et al. Diuretic resistance predicts mortality in patients with advanced heart failure. Am Heart J. 2002;144:31–8. 10.1067/mhj.2002.123144. [DOI] [PubMed] [Google Scholar]
- 27.Côté J-M, Bouchard J, Murray PT, Beaubien-Souligny W. Diuretic strategies in patients with resistance to loop-diuretics in the intensive care unit: a retrospective study from the MIMIC-III Database. J Crit Care. 2021;65:282–91. 10.1016/j.jcrc.2021.06.009. [DOI] [PubMed] [Google Scholar]
- 28.Kuriyama A, Urushidani S. Continuous versus intermittent administration of furosemide in acute decompensated heart failure: a systematic review and meta-analysis. Heart Fail Rev. 2019;24:31–9. 10.1007/s10741-018-9727-7. [DOI] [PubMed] [Google Scholar]
- 29.Ng KT, Velayit A, Khoo DKY, Mohd Ismail A, Mansor M. Continuous infusion versus intermittent bolus injection of furosemide in critically ill patients: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2018;32:2303–10. 10.1053/j.jvca.2018.01.004. [DOI] [PubMed] [Google Scholar]
- 30.Phakdeekitcharoen B, Boonyawat K. The added-up albumin enhances the diuretic effect of furosemide in patients with hypoalbuminemic chronic kidney disease: a randomized controlled study. BMC Nephrol. 2012;13:92. 10.1186/1471-2369-13-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ghafari A, Mehdizadeh A, Alavi-Darazam I, Rahimi E, Kargar C, Sepehrvand N. Co-administration of albumin-furosemide in patients with the nephrotic syndrome. Saudi J Kidney Dis Transpl. 2011;22(3):471–5. PMID: 21566302. [PubMed]
- 32.Fliser D, Zurbrüggen I, Mutschler E, Bischoff I, Nussberger J, Franek E, Ritz E. Coadministration of albumin and furosemide in patients with the nephrotic syndrome. Kidney Int. 1999;55:629–34. 10.1046/j.1523-1755.1999.00298.x. [DOI] [PubMed] [Google Scholar]
- 33.Kitsios GD, Mascari P, Ettunsi R, Gray AW. Co-administration of furosemide with albumin for overcoming diuretic resistance in patients with hypoalbuminemia: a meta-analysis. J Crit Care. 2014;29:253–9. 10.1016/j.jcrc.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 34.Chalasani N, Gorski CJ, Horlander JC, Craven R, Hoen H, Maya J, Brater CD. Effects of albumin/furosemide mixtures on responses to furosemide in hypoalbuminemic patients. J Am Soc Nephrol. 2001;12:1010–6. 10.1681/ASN.V1251010. [DOI] [PubMed] [Google Scholar]
- 35.Duffy M, Jain S, Harrell N, Kothari N, Reddi A. Albumin and furosemide combination for management of edema in nephrotic syndrome: a review of clinical studies. Cells. 2015;4:622–30. 10.3390/cells4040622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Na KY, Han JS, Kim YS, Ahn C, Kim S, Lee JS, Bae KS, Jang IJ, Shin SG, Huh W, et al. Does albumin preinfusion potentiate diuretic action of furosemide in patients with nephrotic syndrome? J Korean Med Sci. 2001;16:448. 10.3346/jkms.2001.16.4.448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Han J, Li N, Wang Y. Ethacrynic acid vs. furosemide in patients with fluid overload associated with cardiac intensive care. Int J Pharmacol. 2018;15:129–36. 10.3923/ijp.2019.129.136. [Google Scholar]
- 38.Joannidis M, Klein SJ, Ostermann M. 10 Myths about frusemide. Intensive Care Med. 2019;45:545–8. 10.1007/s00134-018-5502-4. [DOI] [PubMed] [Google Scholar]