

ABSTRACT
Background
Individuals with Down syndrome (DS) have an elevated likelihood of challenges with executive function (EF) throughout the lifespan, and syndrome‐informed intervention approaches that strengthen these foundations during early childhood may be beneficial. This single group baseline versus postintervention pilot study presents findings from the implementation of a syndrome‐informed, parent‐mediated intervention designed to support the development of EF in preschool‐aged children with DS (EXPO: Executive Function Play Opportunities).
Method
Participants were 34 children aged 3–7 years old with DS and their caregivers. The full sample participated in a novel 12‐week parent‐mediated intervention focused on building working memory, inhibitory control, cognitive flexibility and planning skills. Participants were evaluated at baseline and poststudy for feasibility outcomes and preliminary evidence of intervention efficacy.
Results
Activities were feasible for families to implement and appropriate for the developmental range of participants in the study. Preliminary evidence of efficacy was observed via laboratory‐based EF outcome measures. Within‐sample heterogeneity in response to intervention was also observed.
Conclusions
EXPO is feasible for a larger trial in its current form. Additional intervention modifications may further increase the potential impact of EXPO by addressing heterogeneity in presentations among young children with DS.
Keywords: Down syndrome, executive function, parent‐mediated intervention, pilot study
Over the past several decades, a body of research has characterised phenotypic profiles of behavioural and developmental outcomes in neurogenetic syndromes associated with intellectual disability, such as Down syndrome (DS; Dykens 1995; Hodapp 1997). A promising recent direction for this research is the translation of phenotype‐related findings into tailored interventions and educational applications. Syndrome‐informed intervention offers a personalised approach that accounts for common strengths and challenges associated with specific conditions. Previous work has demonstrated that targeted syndrome‐informed activities are feasible for facilitating early skill development in DS, such as reaching behaviour in infants (Fidler et al. 2021). Such an approach may also benefit critical cognitive skills, like executive functions (EFs), that are areas of known vulnerability in conditions associated with intellectual disability.
DS is associated with challenges in EF throughout all phases of the lifespan (Daunhauer et al. 2014; Lanfranchi et al. 2010; Loveall et al. 2017). EF consists of cognitive regulatory processes that shape adaptive, organised thinking and action (Blair et al. 2005). Most EF models include (but are not limited to) the constructs of working memory, inhibitory control and cognitive flexibility, with some including the higher order dimension of planning and aspects of emotion regulation (Blair et al. 2005; Carlson et al. 2013; Zelazo and Cunningham 2007). EF is associated with adaptive skill development and academic achievement in children with DS and employment outcomes in adults with DS (Onnivello et al. 2022; Tomaszewski et al. 2018; Will et al. 2017), which are related to independence and quality of life (Dean et al. 2018; Graves et al. 2020). Furthermore, EF is associated with levels of autonomy and important skills of independence such as reading and using a telephone in adolescents and adults with DS (Fontana et al. 2024). Precursors of atypical development in EF are detectable during infancy and early childhood in DS (Daunhauer et al. 2014; Schworer et al. 2022). However, intervention approaches have not proactively aimed to strengthen EF foundations in DS by capitalising on early neuroplasticity. Effective EF intervention could support adaptive developmental cascades in young children with DS, promoting greater independence and self‐determination across the lifespan.
Promising research indicates that EF skills can be modified through early intervention in the general population (Diamond 2012). However, these EF interventions have not been adapted or validated for use with children with DS and frequently involve cognitive and language demands that are barriers to participation. Consequently, young children with DS may be missing the opportunity to strengthen cognitive regulatory foundations before transitioning to primary grade education. An adapted approach to meet the needs of children with DS is necessary to remove these barriers.
A novel parent‐mediated intervention called ‘Executive Function Play Opportunities’ (EXPO; see Lanfranchi et al. 2024) was developed to address these needs. The design of EXPO accounts for specific developmental needs associated with early development in DS by selecting appropriate intervention targets and incorporating syndrome‐informed activities that accommodate cognitive, language and motor‐related challenges. EXPO is a 12‐week intervention divided into six 2‐week blocks: play foundations, working memory, inhibition, cognitive flexibility, planning and consolidation. Each block includes 6–10 play‐based activities designed for parent–child engagement, with each activity designed to promote the development of a targeted EF skill in an intrinsically motivating manner. For example, activities in the working memory block involve hiding and then remembering the location of a favourite toy or recalling sequences of joyful greeting gestures (high fives; waves). Families are instructed to select three to four EXPO activities per block from the provided options, with the goal of engaging in activity play sessions at least five times throughout the block. Families are encouraged to repeat activities as often as desired within the block to support skill acquisition. All activities are brief (15–20 min per session) and guided by EXPO Activity Cards that describe materials needed and steps for each activity. Tasks are designed to be implemented at three difficulty levels to account for individual differences among children, and options are provided for modifying task difficulty levels as children gain proficiency within a task. Parents meet weekly with an EXPO Coach, who provides information about EF and the EXPO programme structure, offers guidance on the timing and implementation of activities, provides feedback and offers suggestions for strategies and modifications to enhance accessibility and child engagement in the programme.
EXPO was developed over 2 years through a cross‐national collaboration that started with focus groups with caregivers of young children with DS. A formative evaluation of Version 1.0 materials was conducted by cross‐national DS clinical experts and the programme was then refined into EXPO Version 2.0 (for additional detail, see Lanfranchi et al. 2024; Walsh et al. 2024). Notably, although EXPO is designed to meet the needs of young children with DS based on group‐level findings, a key feature that guided its development was addressing within‐DS heterogeneity related to biomedical and neurodevelopmental complexity (Karmiloff‐Smith et al. 2016; Onnivello et al. 2023). This heterogeneity informed the decision to make EXPO activities adjustable based on a child's current skills and abilities.
1. CONSORT Guidelines
A critical next stage of intervention development for EXPO is evaluating its feasibility and preliminary efficacy through a pilot study. Pilot studies assess the feasibility of an intervention—whether it can be implemented on a larger scale and if any modifications are necessary—and trial novel interventions on a small scale (Eldridge, Lancaster, et al. 2016). Such an evaluation is necessary to determine whether EXPO is appropriate for a larger randomised controlled trial or if additional intervention refinement is necessary (Eldridge, Lancaster, et al. 2016). The present study adheres to current consensus guidelines by applying the Consolidated Standards of Reporting Trials (CONSORT) extension for pilot trials to evaluate EXPO 2.0 (Eldridge, Chan, et al. 2016), following recommendations for nonrandomised pilot studies outlined by Lancaster and Thabane (2019).
2. Current Study
The primary aim of this pilot study was to evaluate the feasibility of EXPO 2.0, focusing on group‐level outcomes including participant retention, adherence, developmental appropriateness and preliminary efficacy. A secondary objective was to characterise heterogeneity in response to intervention to inform the further refinement of EXPO Version 3.0 for a randomised controlled treatment trial. Parental appraisals of the acceptability of EXPO are reported elsewhere (Colaianni et al. 2025 and Walsh et al. 2025).
1. Method
1.1. Participants and Study Design
A single‐group, baseline versus poststudy design was used to evaluate the feasibility of EXPO 2.0 for families of young children with DS. All participants had immediate access to the EXPO 2.0 programme. The a priori target sample size for this pilot was an n of 34–40 children with DS, which was similar to other feasibility studies with children with neurodevelopmental disabilities (e.g., Fidler et al. 2021; Stadnick et al. 2015). Eligibility criteria to participate were a diagnosis of DS established through caregiver report of medical confirmation and a chronological age (CA) between 3.00 and 7.99 years at the start of the trial. Caregivers were required to live with and spend several hours per day interacting with the child. Families were recruited in the United States and Italy and were required to be English speaking in the United States and Italian speaking in Italy. Child participant inclusion criteria were the ability to sit unsupported for at least 1 min and the ability to share attention to objects with their caregiver, assessed through caregiver report. A member of the research team obtained caregiver written consent for their child to participate in laboratory visits and intervention activities.
Recruitment for EXPO began in September 2022, and a total of 39 families of children with parent report of a confirmed DS diagnosis were screened for participation between November 2022 and July 2023. Of these, 38 eligible families enrolled in the intervention pilot trial (United States n = 18; Italy n = 20). Thirty‐six participating caregivers were parents (28 mothers, 5 fathers and 3 mother/father couples), one was a sister and one was a grandparent. Four families (10.5%) started EXPO and withdrew before completing the programme. Figure 1 shows participant flow through the study. Child participants had an average CA of 5.4 years (min = 3.0, 1 max = 7.8, sd = 1.2) and an average MA of 27.8 months (min = 5.0, max = 55.0, sd = 8.0). Participant CA and MA did not differ by site (t = −0.32, p = 0.75 and t = 0.78, p = 0.44, respectively). Child demographics and biomedical characteristics are reported in Table 1. Subgroups of the participants in the present study are also included in Colaianni et al. 2025 and Walsh et al. 2025, which describe site‐specific acceptability and household implementation dimensions.
FIGURE 1.

Participant flow through the EXPO 2.0 pilot study.
TABLE 1.
Participant demographics.
| Child characteristics | |
|---|---|
| Mean CA in years (SD) | 5.4 (1.2) |
| Sex, n (%) | |
| Male | 19 (50%) |
| Female | 19 (50%) |
| DS type, n (%), n = 3 missing | |
| Nondisjunction/trisomy 21 | 26 (68.4%) |
| Mosaic | 1 (2.6%) |
| Translocation | 2 (5.3%) |
| Unknown/not sure | 6 (15.8%) |
| Race, n (%), n = 1 missing | |
| White | 35 (92.1%) |
| Asian | 1 (2.6%) |
| Egyptian | 1 (2.6%) |
| Ethnicity, n (%), n = 20 missing | |
| Hispanic or Latino | 2 (5.3%) |
| Not Hispanic or Latino | 15 (39.5%) |
| Unknown/prefer not to answer | 1 (2.6%) |
| Medical history, n (%), n = 1 missing | |
| Premature birth | 15 (39.5%) |
| Congenital heart defect | 16 (42.1%) |
| Hearing problems | 4 (10.5%) |
| Vision or eye problems | 19 (50%) |
| Sleep apnoea | 9 (23.7%) |
| Autism Spectrum Disorder | 0 (0%) |
| Attention Deficit and/or Hyperactivity Disorder | 0 (0%) |
| Obsessive Compulsive Disorder | 0 (0%) |
1.2. Procedure
EXPO 2.0 was piloted at two cross‐national sites, one in the United States and one in Italy. Families were given identical materials to implement the programme, provided in the native language of the participant (English or Italian). Child participants completed a baseline assessment visit in a laboratory setting that included standardised measures of development and performance‐based EF tasks that have been evaluated for use with young children with DS. These assessments are detailed below. Caregivers completed questionnaires at baseline and participated in an interview that focused on family routines, helping the research team gain a better understanding of each household's context for implementing EXPO.
At the baseline laboratory visit, caregivers downloaded a secure data‐collection mobile phone application that they used to log information about each EXPO activity completed. Activity log entries were automatically uploaded to a secure data management system (REDCap; Harris et al. 2009) that coaches and research staff could access. A primary caregiver implemented the intervention activities at home with their child over a 12‐week period and logged activity information. Weekly coaching sessions, lasting 30 min each, were held between the caregiver and a member of the research team throughout the intervention. These sessions were scheduled based on the family's availability and convenience and took place primarily via video call, with phone calls used if video was not possible. Following the intervention period, families returned to the laboratory for a postintervention visit consisting of the same assessments collected at baseline.
1.3. Measures
1.3.1. Background/Medical History
Caregivers provided information about their child's sex, race, ethnicity, DS diagnosis type and biomedical conditions.
1.3.2. Activity Log
Parents used a mobile phone application to record information about each activity implementation.
1.3.3. EF Outcome Measures
Developmentally appropriate measures of EF were administered to participants at baseline and postintervention, with measures scored by examiners in vivo.
1.3.3.1. Working Memory
In the Garage Game (Pinks et al. 2023), the examiner hid a set of cars in toy garages and encouraged the child to find one car at a time until all cars were found. Responses were coded for novel (correct) versus repeated (incorrect) search locations. The number of cars hidden started at three and increased to six across three trials. Participants could find a maximum of 12 cars across trials if they did not reach a stop rule in Set 1 or 2 (i.e., three consecutive incorrect responses). Scoring: A repetitive search rate was calculated by dividing the total incorrect searches by the total number of cars searched for. For example, if a child attempted all three sets, they searched for 12 cars in total. If that child repeated a search location three times, their repetitive search rate was 3/12 or 0.25. Participants who did not pass the practice trial or who did not respond to test trials were assigned a rate of ‘2’ for analyses. Scores range from 2 (minimum) to 0 (maximum). Lower scores indicate more advanced working memory (Pinks et al. 2023).
1.3.3.2. Inhibition
In the prohibition task, the examiner presented the child with a visually appealing rainmaker toy and instructed the child to wait until they said ‘go’ before playing with it, while gesturing by shaking their head ‘no.’ The examiner then placed the toy in front of the child and waited for 30 s before ending the trial and allowing the child to play with the toy. Scoring: Latency to touch the toy was timed in vivo by examiner. Coders rated scores independently through video recordings to verify examiner accuracy. Scores range from 0 s (minimum) to 30 s (maximum) (Walsh et al. 2023).
1.3.3.3. Flexibility/Shifting
In the Adapted Reverse Categorisation task (van Deusen et al. 2023), examiners instructed participants to sort 10 toys following a colour‐congruent rule (red ones in a red bucket and yellow ones in a yellow bucket). If children sorted more than six toys correctly (indicating task comprehension), they were instructed to shift to a colour‐incongruent rule (yellow ones in the red bucket and red ones in the yellow bucket) for 10 sorts. Scoring: The number of items that were correctly sorted in the colour‐incongruent phase, ranging from 0 to 10, was calculated. To provide additional differentiation among participant performances at more foundational levels, children who passed fewer than three colour‐congruent items were assigned a ‘−2’ for analyses, and children scoring 4–5 correct in the colour‐congruent phase were assigned a score of ‘−1’. Scores range from −2 (minimum) to 10 (maximum) (as per van Deusen et al. 2023).
1.3.4. Developmental Status
Due to differences in the availability of norm‐referenced measures in different languages and cross‐national regions, two measures of child developmental status were utilised for this study. The Stanford–Binet Intelligence Scales, 5th Edition Abbreviated Battery IQ (SB‐5; Roid 2003), was administered in the United States, and the Griffiths Scales of Child Development, 3rd Edition Foundations of Learning Scale (Griffiths III; Stroud et al. 2016), was administered in Italy. Although this strategy allowed for the use of one type of transformed score (age equivalent scores) across both measures, limitations of this approach are considered in Section 4. Mental age (MA) in this study was derived from these age equivalent scores.
1.4. Data Analysis
All analyses were conducted in the R statistical computing environment (R Core Team 2022). An intent‐to‐treat approach was used when evaluating outcome measures, with all enrolled participants included in the analyses regardless of withdrawal status or engagement with the programme. In accordance with CONSORT guidelines for pilot studies, the following feasibility and implementation outcomes were assessed: (a) proportion of eligible participants enrolled and reasons for nonparticipation; (b) proportion of participants retained in the study; (c) intervention adherence (i.e., 100% when families completed 5 or more activities per block); (d) coaching attendance; (e) developmental appropriateness (i.e., percentage of activity sessions taking place across difficulty levels and whether observed differences were accounted for by child characteristics); (f) outcome measure distributional issues; and (g) preliminary efficacy.
Preliminary efficacy was estimated using paired t tests for the EF outcome measures administered at baseline and intervention exit along with Hedges' g statistics of effect size, an adjusted version of Cohen's d measure of effect size that corrects for bias in small samples (Cumming 2013). Regression models were conducted to evaluate whether gains in the outcome measures were predicted by child characteristics or intervention dosage. The percentage of children with gains in single or multiple areas of EF and those with no gains in EF from baseline to postintervention was calculated. Violin plots with statistical details were created to explore patterns of response on the EF outcome measures (Patil 2021).
2. Results
2.1. Primary Implementation Outcomes
2.1.1. Intervention Adherence
Families logged an average of 68.5 activities across the 12 weeks of the EXPO 2.0 pilot, or 11.4 activities per block. The total number of activities that families logged ranged from 6 to 211. Out of 38 families, 31 (81.6%) completed an average of 5 activities per block, and 18 (47.4%) completed 5 activities in all six blocks. Unlogged activities were not included in analyses, which is noted as a limitation in Section 4. Although the number of activities completed did not significantly differ by block, F(5, 161.96) = 2.01, p = 0.08, a linear mixed model analysis demonstrated that families participated in fewer activities in two of the latter blocks (flexibility: Estimate = −2.24, p = 0.05; consolidation: Estimate = −2.77, p = 0.02) in comparison with the first block (foundations). Most participating families (73.7%; n = 28) attended all 12 coaching sessions. On average, participants attended 11.05 coaching sessions (min = 5, max = 12).
2.1.2. Developmental Appropriateness
Logged activities were distributed almost evenly across the three levels of task difficulty, with 33.0% completed at the first level, 32.6% at the second level and 34.4% at the third level. A mixed model was fit to determine whether the difficulty level of logged activities differed as a function of child characteristics, with fixed effects for CA, MA, sex and race and random effects for each participant. There was evidence of a difference in difficulty completion by CA (F[1, 28.78] = 5.37, p = 0.03) and sex (F[1, 28.23] = 4.72, p = 0.04). Higher CA was associated with greater difficulty (t = 2.32, p = 0.03). Female participants had a higher mean activity difficulty than male participants (mean difference = 0.27, p = 0.04).
2.1.3. EF Outcome Measures Performance Distributions
Table 2 reports the distributions of EF outcome measure scores at baseline, including minimum and maximum values, the number and percentage of participants at extreme score values and the skewness and kurtosis of the measures.
TABLE 2.
EF outcome measure distributions at baseline.
| Measure | Minimum score | Maximum score | Minimum score n (%) | Maximum score n (%) | Skew | Kurtosis |
|---|---|---|---|---|---|---|
| Garage Game a | 2 | 0 | 4 (10.5%) | 8 (21.1%) | 1.41 | 0.70 |
| Adapted Reverse Categorisation b | −2 | 10 | 5 (13.2%) | 12 (31.6%) | −0.03 | −1.89 |
| Prohibition | 0 s | 30 s | 8 (21.1%) | 16 (42.1%) | 0.21 | −1.93 |
Lower scores on the garage game indicate better working memory skills.
See Section 1.3.3.3 for negative score interpretation and scoring procedures.
2.1.4. Preliminary Efficacy
Table 3 presents changes in EF outcome measures from baseline to poststudy. Participants at the group level made improvements on two of the three performance‐based laboratory measures: Garage Game (t[33] = 2.10, p = 0.04, Hedges' g = 0.35) and Adapted Reverse Categorisation (t[31] = 4.56, p = 0.02, Hedges' g = −0.43). Despite selecting measures designed to capture performances with validity in this population, a small number of participants scored at the ceiling for one or more of the measures at the baseline visit and thus could not show gains on these measures. Participants who scored ‘ceiling at baseline’ are accounted for in analyses when applicable. When ‘ceiling‐at‐baseline’ participants were removed, the effects were stronger: Garage Game (t[27] = 2.37, p = 0.02, Hedges' g = 0.44) and Adapted Reverse Categorisation (t[21] = −2.66, p = 0.01, Hedges' g = −0.55). Removing ‘ceiling‐at‐baseline’ participants, 80.0% made gains on at least one of the three EF outcome measures, 61.5% made gains in working memory, 54.5% made gains in flexibility and 38.9% made gains in inhibition.
TABLE 3.
Changes in EF‐related outcomes from baseline to postassessment.
| Dependent variable | Baseline mean (SD) | Poststudy mean (SD) | t‐test statistic (p value) | Hedges' g |
|---|---|---|---|---|
| Garage Game a | 0.53 (0.63) | 0.40 (0.57) | 2.10 (0.04) | 0.35 |
| Adapted Reverse Categorisation | 4.56 (5.07) | 5.71 (4.61) | −2.49 (0.02) | −0.43 |
| Prohibition | 14.1 (14.0) | 12.6 (13.8) | 0.77 (0.45) | 0.13 |
Lower scores on the garage game indicate better working memory skills.
Regression models accounting for EF outcome scores at baseline did not provide evidence that the total number of activities completed by families, both across the intervention and within the relevant EF block, was predictive of improvement on the EF outcome tasks (p values > 0.1).
2.2. Secondary Outcome
2.2.1. Response Heterogeneity
Visualisations of participant performances on EF outcome measures at baseline and poststudy can be seen in Figures 3, 4, 5. Overall group‐level improvements were observed for two of the three EF outcome measures (see Table 4); however, one fifth of participants made no improvements when excluding those with ‘ceiling‐at‐baseline’ scores. Moreover, a small number of participants demonstrated floor effects postintervention. Out of 34 participants who completed postintervention measures, two (5.9%) scored at the floor of Adapted Reverse Categorisation, three (8.8%) scored at the floor of the Garage Game and seven (20.6%) scored at the floor of the prohibition. Gains in EF from baseline to postintervention varied across age groups, as demonstrated in Figure 2. Age groups were formed by rounding each child's age down to the nearest whole year, creating 1‐year CA bins. The oldest age group (7‐year‐olds, n = 2) showed no improvements on the EF tasks. In contrast, children aged 3–6 years made notable gains, with approximately 50%–80% of each age group demonstrating improvement on one or more EF tasks.
FIGURE 3.

Changes in participant working memory outcome from baseline to postintervention. Note: Lower scores indicate stronger working memory performances.
FIGURE 4.

Changes in participant inhibition outcome from baseline to postintervention. Note: Higher scores indicate stronger inhibition performances.
FIGURE 5.
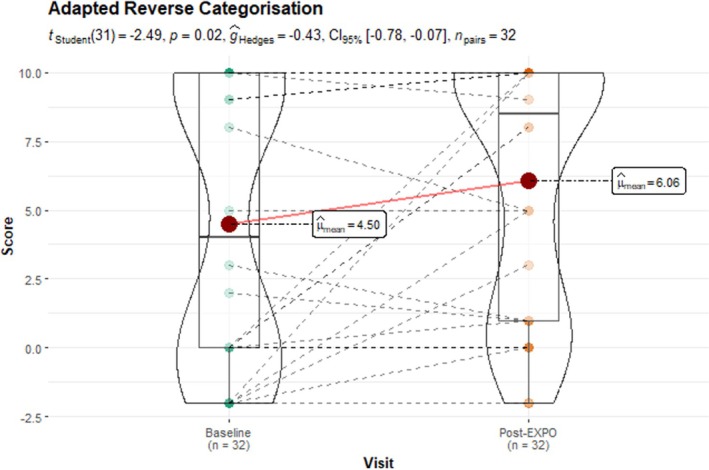
Changes in participant shifting outcome from baseline to postintervention. Note: Higher scores indicate stronger cognitive flexibility performances.
TABLE 4.
Participant gain patterns.
| Outcome Gains | n | % a | % out of participants who were not ‘ceiling at baseline’ |
|---|---|---|---|
| Total participants with gains | 23 | 70.6 | 80.0 |
| WM only | 6 | 17.6 | 23.1 |
| Flexibility only | 4 | 11.8 | 18.2 |
| Inhibition only | 3 | 8.8 | 16.7 |
| WM + Flexibility | 7 | 20.6 | 24.1 |
| WM + Inhibition | 3 | 8.8 | 10.3 |
| Flexibility + Inhibition | 1 | 2.9 | 3.7 |
| WM + Flexibility + Inhibition | 0 | 0.0 | 0.0 |
| Total participants with no gains | 10 | 29.4 | — |
| Scored at ceiling of all baseline outcome measures | 4 | 11.8 | — |
Percentage out of participants who completed outcome measures at baseline and poststudy (n = 34).
FIGURE 2.

Number of EF tasks demonstrating gains by participant CA. (A) Total number of EF task gains without accounting for ceiling effects at baseline. (B) Total number of EF task gains accounting for ceiling effects on the Garage Game task at baseline. (C) Total number of EF task gains accounting for ceiling effects on the Adapted Reverse Categorisation (ARC) task at baseline. (D) Total number of EF task gains accounting for ceiling effects on the prohibition task at baseline.
3. Discussion
This study is the first to evaluate the feasibility, developmental appropriateness and preliminary efficacy of EXPO, a novel parent‐mediated intervention designed to strengthen early EF skills in young children with DS. Families at two sites participated in a pilot trial of EXPO Version 2.0, a 12‐week course of activities involving play‐ and routine‐based opportunities to strengthen aspects of EF, including working memory, inhibitory control and cognitive flexibility. Results demonstrated that EXPO 2.0 activities were feasible for families to implement and appropriate for the developmental range of child participants in the study. Preliminary evidence of efficacy was observed for two of three laboratory‐based EF outcome measures in group‐level analyses, and the majority of participants (80.0%) made gains on at least one of the three laboratory‐based EF outcome measures when ceiling effects at baseline were accounted for. A within‐sample evaluation of response heterogeneity suggests that EXPO efficacy may be enhanced by further refinement of EXPO into an adaptive intervention that accounts for early versus slower response patterns among young children with DS.
Phenotypic patterns of strength and challenge associated with DS informed this intervention in several important ways: EF was selected as an intervention target based on prior evidence of early developmental vulnerabilities in DS (see Fidler et al. 2023), intervention activities were developed accounting for the broader pattern of relative strengths and challenges generally associated with DS (see Daunhauer and Fidler 2011) and the EF outcome measures selected have been validated for use with young children with DS (Pinks et al. 2023; van Deusen et al. 2023; Walsh et al. 2023).
3.1. Feasibility
The primary findings from this study related to the feasibility of implementing EXPO activities. The vast majority of families interested in participation enrolled in the study and sustained participation through to intervention exit. Analysis of participation patterns demonstrated that families adhered to guidelines regarding frequency of implementation, which entailed five or more activities per block for six blocks. Nearly all families participated in all weekly coaching sessions. These findings suggest that the design of EXPO successfully removed barriers to EF intervention implementation for families and that activities were designed in ways that promoted family engagement, which may lead to more opportunities for practice and the accumulation and consolidation of skills over time. A potential barrier to feasibility in community settings is access to mobile phones and the internet. Although most materials were provided in hard copy, paper‐based activity logging could serve as an alternative to mobile app‐based logging in areas with restricted access to smart phones or the internet. Coaching is a critical component of EXPO that was piloted primarily via video calls, but phone calls could serve as a feasible alternative in situations where access to video calls is limited. Overall, this intervention could be readily adapted to accommodate the needs of various families, given its low cost, minimal material requirements and at‐home parent‐mediated design.
3.2. Preliminary Efficacy
Statistically significant overall group‐level improvements in EF on near‐transfer lab tasks were observed for two of the three EF outcome measures administered, with 80% of participants making gains on at least one EF dimension from baseline to exit when ceiling‐at‐baseline performances were accounted for. These findings have translational relevance, as recent work demonstrates that performance on syndrome‐informed laboratory measures of EF in DS is associated with adaptive behaviour performances longitudinally (van Deusen et al. 2024). Though no far transfer effects were evaluated in this pilot study, future work should evaluate EXPO's potential effects on activities of daily living and the practical use of communication and social skills in real‐world settings.
It is notable that group level improvements were observed for working memory and cognitive flexibility laboratory measures but not inhibitory control. This finding necessitates the examination of EXPO inhibitory control activities to ensure they provide adequate opportunities for strengthening this dimension in the 2.0 version of EXPO. Although it may be that EXPO activities truly did not impact this EF dimension, additional evaluation of the inhibitory control outcome measure itself (the prohibition task) is warranted as well, as it may not have sensitively captured gains. Inhibitory control was measured with an early childhood prohibition task requiring the child to resist a prepotent response to access an enticing toy (Walsh et al. 2023). This type of task has shown adequate psychometric properties in young children with DS once goal‐directed actions become more flexible and frequent (Walsh et al. 2023). However, goal‐directed behaviour is often an area of relative delay for young children with DS, and prior to the onset of frequent and flexible goal‐directed action, inhibitory control may not be adequately measured through prohibition tasks. A critical next step for further evaluation of EXPO involves the selection of alternative measures of inhibitory control that are not contingent upon the presence of a high degree of goal‐directed initiations. Future work should also increase the number of tasks assessing EF performance to capture additional manifestations of EF and more rigorously evaluate efficacy.
3.3. Heterogeneity of Responses
A secondary aim of this study was to evaluate heterogeneity in response to intervention. Overall group‐level findings are necessary for establishing an evidence base for this novel intervention, and its appropriateness for young children with DS within the targeted developmental window for EXPO activities. However, it is critical to highlight that gains were not observed for 20% of participants from baseline to exit (when ceiling‐at‐baseline participants were removed). Thus, although overall group‐level findings were observed for both working memory and cognitive flexibility and some individual gains were observed for inhibitory control, a smaller subgroup of participants showed no evidence of intervention response. For some participants, the lack of overall gains may be attributed to ceiling effects on certain measures at baseline. This is evidenced in Figure 2, where those who did not show gains on EF measures but achieved the highest possible score on a measure are categorised in ‘ceiling effects’ groups. This categorisation helped account for the limitation that ceiling effects may have imposed, potentially masking improvements that participants made in EXPO.
Additional evaluation of nonresponse patterns is warranted to determine its interaction with child dimensions such as degree of developmental delay and cooccurring neurodevelopmental conditions. The original intent of the development of EXPO was to tailor an intervention to young children with DS, including those who demonstrate greater neurodevelopmental complexity. Therefore, a critical next step in the intervention development process is to transform EXPO into an adaptive intervention that can be further tailored based on initial response to intervention. Alternative pathways through EXPO may provide a longer intervention timeline beyond 12 weeks or adapt EXPO activities to involve more practice of foundational play skills that facilitate participation in activities designed to strengthen EF.
3.4. Strengths and Limitations
Although additional intervention and outcome measure refinement are warranted, this preliminary implementation provides promising evidence that tailoring early EF interventions in syndrome‐informed ways can lead to observable and quantifiable changes in laboratory‐based assessments of working memory and cognitive flexibility. A primary strength of this study is its ecological validity. By examining the feasibility and preliminary efficacy of a home‐based, parent‐mediated intervention specifically designed for young children with DS, the study benefits from a high level of relevance to real‐world settings. The intervention was informed by focus groups with caregivers of young children with DS, ensuring that it addressed the unique needs and circumstances of the target population. This design approach enhances the likelihood that the findings will be applicable and beneficial for refining the intervention for further use in everyday contexts. In addition, the study included measures of EF that have been validated for use with young children with DS, maximising the opportunity to capture preliminary treatment effects, although further evaluation of the prohibition task as an inhibition endpoint is warranted. Nonetheless, for working memory and cognitive flexibility, performance‐based laboratory measures appear to have captured near‐transfer changes in processing efficiency. Although some ceiling and floor effects were observed, the outcome measures can be readily modified to better capture efficacy in future trials.
An inherent limitation of pilot trials is their smaller scale compared to full‐scale randomised controlled trials. The current pilot study involved a smaller sample size and utilised a single‐group design without randomisation or a comparison group. This limits the ability to generalise findings and assess the effectiveness of EXPO with the same level of rigour as larger trials. The EF gains that were observed could be the result of participants ‘practising’ the outcome measures at the two time points. However, the outcome measures chosen for this study did not show significant practice effects when evaluated for use with young children with DS (Pinks et al. 2023; van Deusen et al. 2023; Walsh et al. 2023), suggesting that the improvements observed in this study were likely the result of the intervention and not practice effects from the baseline visit. Future larger scale trials should seek greater characterisation of the dosage, intensity and intervention components contributing to group‐level and individual patterns of response to intervention.
Several additional limitations should be noted. Due to cross‐national differences in the use of norm‐referenced early development standardised measures, overall developmental status was evaluated using different measures in the US and Italian participant sites. This approach allowed for the use of more localised and well‐established measures specific to the collaborating study teams; however, the comparability of age equivalent scores generated by the two measures is unknown. As such, the interpretation of MA‐related descriptions and findings should be approached with some measure of caution. In addition, activity completion data were collected through parent logs using a mobile phone application, allowing parents to record activities in real time and minimising the likelihood of missing data. However, at least one family reported inconsistencies in logging activities after the initial week of the programme, suggesting potential underreporting of the number of activities completed. Additionally, distributional issues were observed for the selected EF outcome measures, with ceiling effects present for each EF assessment, indicating that some participants performed at the highest level possible at the start of the intervention. Lastly, fidelity of activity implementation was not systematically assessed in this pilot study, with fidelity informally evaluated by coaches during coaching sessions through review of the previous week's activities. Future studies should include more formalised and standardised evaluations of fidelity. These limitations highlight the need for improved measurement tools and approaches in future research.
3.5. Future Directions
Although EXPO was originally designed to meet the needs of young children with DS, the programme may be beneficial for other groups of children as well. EXPO focused on removing barriers to participation for a specific subgroup of children by starting with phenotype‐related findings from the current literature and stakeholder insight. It is possible that the accommodations developed for children with DS could also benefit children with other neurodevelopmental conditions that are associated with EF challenges. Furthermore, additional dimensions of EF, such as emotion regulation, may serve as important intervention targets for young children with DS. Future research should explore expanding the scope of early intervention to include these and other relevant aspects of EF for this population.
4. Conclusions
This pilot study of EXPO demonstrated group‐level improvements in young children with DS for two of the three laboratory‐based outcome measures administered. Moreover, data visualisations highlighted response patterns that were predominantly in the direction of improvement on measures of cognitive flexibility and working memory. Results also identify a subgroup of children who demonstrated difficulties with EF tasks at baseline and continue to demonstrate similar difficulties at intervention exit. These results suggest that EXPO is feasible for a larger trial, but further refinement of EXPO into an adaptive intervention that meets the needs of even more children in this population is warranted.
Ethics Statement
Informed consent was obtained from the caregiver of each participant in this study. The study protocol was approved by the Colorado State University Institutional Review Board and the University of Padua Ethics Committee. All project procedures conform to the guidelines for the protection of human subjects in research.
Conflicts of Interest
The authors declare no conflicts of interest.
Acknowledgements
The authors would like to thank the families and community members who contributed to the development of this intervention by providing their time, support and insights.
Pinks, Miranda E. , Walsh, Madison M. , Colaianni, S. , Onnivello, S. , Marcolin, C. , Looney, S. , Rossi, E. , Pulina, F. , Prince, Mark A. , Riggs, Nathaniel R. , Hepburn, S. , Daunhauer, Lisa A. , Kaylyn, V. , Lanfranchi, S. , and Fidler, Deborah J. (2025) Feasibility and Preliminary Efficacy of an Executive Function Intervention for Young Children With Down Syndrome. Journal of Intellectual Disability Research, 69: 546–557. 10.1111/jir.13234.
Funding: This study was supported by the Fondation Jérôme Lejeune (2061) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (1R61HD115161‐01).
Endnotes
One participant had a CA of 2.97 at the baseline visit and turned 3 prior to initiating intervention activities.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
- Blair, C. , Zelazo P. D., and Greenberg M. T.. 2005. “The Measurement of Executive Function in Early Childhood.” Developmental Neuropsychology 28, no. 2: 561–571. [DOI] [PubMed] [Google Scholar]
- Carlson, S. M. , Zelazo P. D., and Faja S.. 2013. “Executive Function.” In The Oxford Handbook of Developmental Psychology, edited by Zelazo P. D., vol. 1. Oxford University Press. [Google Scholar]
- Colaianni, S. , Walsh M. M., Onnivello S., et al. 2025. “Acceptability of a Novel Parent‐Mediated Executive Function Intervention for Young Children With Down Syndrome in Italy.” Journal of Applied Research in Intellectual Disabilities 38, no. 2: e70038. 10.1111/jar.70038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cumming, G. 2013. Understanding the new Statistics: Effect Sizes, Confidence Intervals, and Meta‐Analysis. Routledge. [Google Scholar]
- Daunhauer, L. A. , and Fidler D. J.. 2011. “The Down Syndrome Behavioral Phenotype: Implications for Practice and Research in Occupational Therapy.” Occupational Therapy in Health Care 25, no. 1: 7–25. [DOI] [PubMed] [Google Scholar]
- Daunhauer, L. A. , Fidler D. J., Hahn L., Will E., Lee N. R., and Hepburn S. L.. 2014. “Profiles of Everyday Executive Functioning in Young Children With Down Syndrome.” American Journal on Intellectual and Developmental Disabilities 119, no. 4: 303–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dean, E. E. , Shogren K. A., Hagiwara M., and Wehmeyer M. L.. 2018. “How Does Employment Influence Health Outcomes? A Systematic Review of the Intellectual Disability Literature.” Journal of Vocational Rehabilitation 49, no. 1: 1–13. 10.3233/JVR-180950. [DOI] [Google Scholar]
- Diamond, A. 2012. “Activities and Programs That Improve Children's Executive Functions.” Current Directions in Psychological Science 21, no. 5: 335–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dykens, E. M. 1995. “Measuring Behavioral Phenotypes: Provocations From the “New Genetics”.” American Journal of Mental Retardation 99, no. 5: 522–532. [PubMed] [Google Scholar]
- Eldridge, S. M. , Chan C. L., Campbell M. J., et al. 2016. “CONSORT 2010 Statement: Extension to Randomised Pilot and Feasibility Trials.” BMJ 355: 1−29. 10.1136/bmj.i5239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eldridge, S. M. , Lancaster G. A., Campbell M. J., et al. 2016. “Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework.” PLoS ONE 11, no. 3: e0150205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fidler, D. , Schworer E., Needham A., et al. 2021. “Feasibility of a Syndrome‐Informed Micro‐Intervention for Infants With Down Syndrome.” Journal of Intellectual Disability Research 65, no. 4: 320–339. [DOI] [PubMed] [Google Scholar]
- Fidler, D. J. , Daunhauer L. A., Schworer E., and Patel L.. 2023. “Executive Function in Down Syndrome: Links to Adaptation and Treatment Implications.” In The Oxford Handbook of Down Syndrome and Development, edited by Burack J. A., Edgin J., and Abbeduto L., 305–331. Oxford University Press. [Google Scholar]
- Fontana, M. , Pellizzoni S., and Passolunghi M. C.. 2024. “The Relationship Between Different Levels of Autonomy, Inhibition Dimensions and Working Memory in People With Down Syndrome.” International Journal of Disability, Development and Education 72, no. 1: 102–116. 10.1080/1034912X.2024.2337171. [DOI] [Google Scholar]
- Graves, R. J. , Zlomke K., Graff J. C., and Hall H. R.. 2020. “Adaptive Behavior of Adults With Down Syndrome and Their Health‐Related Quality of Life.” Advances in Neurodevelopmental Disorders 4, no. 1: 27–35. [Google Scholar]
- Harris, P. A. , Taylor R., Thielke R., Payne J., Gonzalez N., and Conde J. G.. 2009. “Research Electronic Data Capture (REDCap)—A Metadata‐Driven Methodology and Workflow Process for Providing Translational Research Informatics Support.” Journal of Biomedical Informatics 42, no. 2: 377–381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hodapp, R. M. 1997. “Direct and Indirect Behavioral Effects of Different Genetic Disorders of Mental Retardation.” American Journal on Mental Retardation 102, no. 1: 67–79. [DOI] [PubMed] [Google Scholar]
- Karmiloff‐Smith, A. , Al‐Janabi T., D'Souza H., et al. 2016. “The Importance of Understanding Individual Differences in Down Syndrome.” F1000Research 5: 1−10. 10.12688/f1000research.7506.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lancaster, G. A. , and Thabane L.. 2019. “Guidelines for Reporting Non‐Randomised Pilot and Feasibility Studies.” Pilot and Feasibility Studies 5, no. 1: 114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanfranchi, S. , Jerman O., dal Pont E., Alberti A., and Vianello R.. 2010. “Executive Function in Adolescents With Down Syndrome.” Journal of Intellectual Disability Research 54, no. 4: 308–319. [DOI] [PubMed] [Google Scholar]
- Lanfranchi, S. , Onnivello S., Walsh M., et al. 2024. “Considerations for Developing Syndrome‐Informed Early Interventions for Children with Neurogenetic Conditions.” International Review of Research in Developmental Disabilities 67: 45–69. 10.1016/bs.irrdd.2024.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loveall, S. J. , Conners F. A., Tungate A. S., Hahn L. J., and Osso T. D.. 2017. “A Cross‐Sectional Analysis of Executive Function in Down Syndrome From 2 to 35 Years.” Journal of Intellectual Disability Research 61, no. 9: 877–887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onnivello, S. , Colaianni S., Pulina F., et al. 2022. “Executive Functions and Adaptive Behaviour in Individuals With Down Syndrome.” Journal of Intellectual Disability Research 66, no. 1–2: 32–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onnivello, S. , Schworer E. K., Prince M. A., Daunhauer L. A., and Fidler D. J.. 2023. “Early Developmental Profiles Among Infants With Down Syndrome.” Journal of Intellectual Disability Research 67, no. 3: 228–238. [DOI] [PubMed] [Google Scholar]
- Patil, I. 2021. “Visualizations With Statistical Details: The ‘ggstatsplot’ Approach.” Journal of Open Source Software 6, no. 61: 3167. [Google Scholar]
- Pinks, M. E. , van Deusen K., Prince M. A., et al. 2023. “Psychometric Evaluation of a Working Memory Assessment Measure in Young Children With Down Syndrome.” Research in Developmental Disabilities 139: 104564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Core Team . 2022. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. https://www.R‐project.org. [Google Scholar]
- Roid, G. H. 2003. Stanford Binet Intelligence Scales. Fifth ed. Riverside Publishing. [Google Scholar]
- Schworer, E. K. , Fidler D. J., Kaur M., Needham A. W., Prince M. A., and Daunhauer L. A.. 2022. “Infant Precursors of Executive Function in Down Syndrome.” Journal of Intellectual Disability Research 66, no. 1–2: 108–120. [DOI] [PubMed] [Google Scholar]
- Stadnick, N. A. , Stahmer A., and Brookman‐Frazee L.. 2015. “Preliminary Effectiveness of Project ImPACT: A Parent‐Mediated Intervention for Children With Autism Spectrum Disorder Delivered in a Community Program.” Journal of Autism and Developmental Disorders 45, no. 7: 2092–2104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stroud, L. , Foxcroft C., Green E., et al. 2016. Griffiths Scales of Child Development (3rd Edition) Part I: Overview, Development, and Psychometric Properties. Hogrefe Ltd. [Google Scholar]
- Tomaszewski, B. , Fidler D. J., Talapatra D., and Riley K.. 2018. “Adaptive Behaviour, Executive Function and Employment in Adults With Down Syndrome.” Journal of Intellectual Disability Research 62, no. 1: 41–52. [DOI] [PubMed] [Google Scholar]
- van Deusen, K. , Prince M. A., Thurman A. J., et al. 2023. “Evaluating an Adapted Reverse Categorisation Task to Assess Cognitive Flexibility in Young Children With Down Syndrome.” Journal of Intellectual Disability Research 67, no. 8: 734–745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Deusen, K. , Prince M. A., Walsh M. M., et al. 2024. “Laboratory‐Based Measures of Executive Function and Daily Living Skills in Young Children With Down Syndrome: Informing Future Interventions.” Journal of Intellectual Disability Research 68: 1301–1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh, M. M. , van Deusen K., Prince M. A., et al. 2023. “Preliminary Psychometric Properties of an Inhibition Task in Young Children With Down Syndrome.” Journal of Intellectual Disabilities 29: 5–23. 10.1177/17446295231218776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walsh, M. M. , Pinks M. E., Colaianni S., et al. 2025. “A Mixed‐Method Evaluation of the Usability and Acceptability of a Novel Parent‐Mediated Intervention for Young Children With Down Syndrome in the US.” Manuscript submitted for publication.
- Walsh, M. M. , Van Deusen K., Pinks M. E., et al. 2024. “Parent Perspectives on Parent‐Mediated Intervention for Young Children With Down Syndrome.” Journal of Applied Research in Intellectual Disabilities 37, no. 6: e13307. 10.1111/jar.13307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Will, E. , Fidler D. J., Daunhauer L. A., and Gerlach‐McDonald B.. 2017. “Executive Function and Academic Achievement in Primary—Grade Students With Down Syndrome.” Journal of Intellectual Disability Research 61, no. 2: 181–195. 10.1111/jir.12313. [DOI] [PubMed] [Google Scholar]
- Zelazo, P. D. , and Cunningham W. A.. 2007. “Executive Function: Mechanisms Underlying Emotion Regulation.” In Handbook of Emotion Regulation, edited by Gross J. J., 135–158. Guilford Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.