

ABSTRACT
Music appears universally in human infancy with self‐evident effects: as many parents know intuitively, infants love to be sung to. The long‐term effects of parental singing remain unclear, however. In an offset‐design exploratory 10‐week randomized trial conducted in 2023 (110 families of young infants, M age = 3.67 months, 53% female, 73% White), the study manipulated the frequency of infant‐directed singing via a music enrichment intervention. Results, measured by smartphone‐based ecological momentary assessment (EMA), show that infant‐directed singing causes general post‐intervention improvements to infant mood, but not to caregiver mood. The findings show the feasibility of longitudinal EMA (retention: 92%; EMA response rate: 74%) of infants and the potential of longer‐term and higher‐intensity music enrichment interventions to improve health in infancy.
Keywords: ecological momentary assessment, EMA, infancy, infant‐directed song, music, parenting
Decades of research have demonstrated the profound impact of the quality of early life experiences on lifelong physical and mental health (Fries et al. 2005; Shonkoff et al. 2012). Building on Bowlby's (1969) work on attachment, evidence from a wide variety of approaches and across diverse populations shows that consistent warmth, care, and responsiveness provided by caregivers is a key feature of healthy caregiving and positive infant‐caregiver relationships (Schore 2005; Stams et al. 2002).
Children face very different chances of receiving the benefits of a caring and nurturing infant‐caregiver relationship, however. Factors related to risk and resilience, such as caregiver characteristics (e.g., age, sex, personality, marital status), cultural background, and socioeconomic circumstances, together mediated by differential access to resources and opportunities, interact to shape the variability in early life experiences (Roubinov and Boyce 2017). Moreover, contextual factors, such as poor marital relationship quality (Dennis and Ross 2006) and inadequate social support (Reid and Taylor 2015), are associated with increased risk of postpartum depression, affecting caregiver responsiveness and sensitivity towards infants (Feldman et al. 2009).
The high degree of variability in early home environments presents an opportunity to improve outcomes for young infants and their families. In particular, simple, low‐cost, and low‐tech interventions that involve only modest adjustments to infant care practices hold particular promise given their ease of uptake. For example, increasing early skin‐to‐skin contact (e.g., kangaroo care) has demonstrated numerous health benefits for both premature and full‐term infants worldwide (Feldman et al. 2014; Moore et al. 2012). In this paper, we report an exploratory randomized trial of a high‐potential but relatively unexplored type of enrichment: singing interventions for caregivers of young infants.
Music permeates the early lives of infants, particularly through their interactions with caregivers (e.g., Trehub and Hannon 2006; Mehr and Krasnow 2017). Caregivers universally sing to their infants in the course of child‐rearing (Mehr et al. 2019; Singh and Mehr 2023), throughout infancy (Yan et al. 2021), and regardless of family socioeconomic status (Mehr 2014; Custodero and Johnson‐Green 2003; Fancourt and Perkins 2018c). Such infant‐directed singing has robust cross‐cultural regularities (Hilton et al. 2022; Yurdum et al. 2023; Mehr et al. 2019), including multimodal features that combine voice, touch, eye contact, and movement, which infants may reciprocate via visual attention, cooing, smiling, and moving their hands and legs (Malloch and Trevarthen 2009). These interactive behaviors may support a variety of communicative functions (Trehub and Gudmundsdottir 2019; Mehr et al. 2021), including signaling social information (Mehr et al. 2016; Mehr and Spelke 2017) or parental investment (Kotler et al. 2019; Mehr and Krasnow 2017; Mehr et al. 2017), enhancing social bonds (Fancourt and Perkins 2018b), and promoting meaningful social interactions in families (Lense et al. 2022; Malloch 1999).
It may be unsurprising, then, that music in general, and infant‐directed singing in particular, has profound effects on infant mood and well‐being. Infants, who are notoriously poor at emotional self‐regulation, rely heavily on their caregivers; and infant‐directed singing is effective in regulating infant mood and arousal on a short‐term basis. For example, after a still‐face procedure, parent‐produced familiar infant‐directed songs reduced infant distress and arousal levels more effectively than speech (Cirelli and Trehub 2020). Similarly, in an open‐ended listening task, infants listened to singing for more than twice as long before initiating sustained crying, relative to speech listening (Corbeil et al. 2016). While familiar songs accelerate infants' recovery from distress (Cirelli and Trehub 2020), even unfamiliar, foreign lullabies calm infants, as measured by heart rate, electrodermal activity, and pupillometry (Bainbridge et al. 2021).
The benefits of early musical engagement may extend beyond infants to caregivers themselves. Music may aid in the regulation of caregivers' own arousal levels (Cirelli et al. 2020), reduce caregiving‐related stress (Cho and Ilari 2021), or contribute to positive home environments (Byrn and Hourigan 2010). Moreover, active musical engagement has been proposed to foster communication, emotional bonding, and a sense of security and attachment between caregivers and infants (Fancourt and Perkins 2018b; Gerry et al. 2012; Persico et al. 2017; Steinberg et al. 2021). Any of these may well promote well‐being in caregivers alongside that of their infants.
Singing therefore has potential as an enrichment intervention, as its short‐term effects could in principle work cumulatively, leading to improved health outcomes in infants and caregivers. Only a few longitudinal experiments have tested this possibility. For instance, year‐long participation in parent–child music enrichment programs led to enhanced quality of parent–child interactions (Smith et al. 2024). Additionally, 10‐week group singing programs have reduced both psychological and biological markers of depression, anxiety, and stress, while also strengthening bonds between parents with postnatal depression and their infants (Bind et al. 2023; Fancourt and Perkins 2018a; Perkins et al. 2018).
Here, we report a 6‐week randomized trial of young infant‐caregiver dyads, wherein we experimentally manipulated the frequency of infant‐directed singing via a music enrichment intervention. We measured outcomes primarily with smartphone‐based ecological momentary assessment (EMA), a method that samples infant behavior in real time via brief, repeated‐measures surveys that caregivers complete daily at random intervals (e.g., de Barbaro et al. 2023; Franchak 2019). This approach provides comprehensive snapshots of highly fluctuating family dynamics and routines over time, minimizing parent recall bias (a vulnerability of prior music intervention studies) and enhancing ecological validity (van den Heuvel et al. 2021; Stone et al. 2007).
1. Method
1.1. Participants
All participants provided informed consent under a protocol approved by the Yale University Institutional Review Board (protocol #2000035858). We advertised the study via in‐person visits to baby fairs, distribution of flyers at local daycare centers, preschools, and delivery hospitals, and an announcement on public radio in New Haven, Connecticut. Online recruitment efforts targeted social media groups for expecting and new parents, along with online communities related to early childhood education. The inclusion criteria required participants to have a smartphone, to communicate and complete surveys in English, and to be a primary caregiver of the focal infant. Participants were primarily located in the United States and New Zealand (see Table 1), but as the study took place entirely online, there were no geographical constraints.
TABLE 1.
Demographic characteristics of the sample.
| Characteristics | n | % of sample |
|---|---|---|
| Country of residence | ||
| United States of America | 60 | 54.5 |
| New Zealand | 38 | 34.5 |
| Canada | 10 | 9.1 |
| Singapore | 1 | 0.9 |
| Sweden | 1 | 0.9 |
| Parent's country of birth | ||
| United States of America | 53 | 48.2 |
| New Zealand | 27 | 24.5 |
| Canada | 7 | 6.4 |
| South Korea | 7 | 6.4 |
| United Kingdom of Great Britain and Northern Ireland | 3 | 2.7 |
| India | 2 | 1.8 |
| Australia | 1 | 0.9 |
| China | 1 | 0.9 |
| El Salvador | 1 | 0.9 |
| France | 1 | 0.9 |
| Germany | 1 | 0.9 |
| Hong Kong (SAR) | 1 | 0.9 |
| Iraq | 1 | 0.9 |
| Malaysia | 1 | 0.9 |
| Saudi Arabia | 1 | 0.9 |
| Spain | 1 | 0.9 |
| Zimbabwe | 1 | 0.9 |
| Parent's race/ethnicity | ||
| White/European/New Zealand European | 80 | 72.7 |
| Asian | 20 | 18.2 |
| Black or African American | 2 | 1.8 |
| Māori | 1 | 0.9 |
| More than one race | 6 | 5.5 |
| I'd prefer not to say | 1 | 0.9 |
| Parent's highest level of education | ||
| High school or equivalent | 4 | 3.6 |
| Vocational/technical school (2 year) | 2 | 1.8 |
| Some college/university | 9 | 8.2 |
| College/university graduate | 49 | 44.5 |
| Master's degree (MA or equivalent) | 32 | 29.1 |
| Doctoral degree (PhD or equivalent) | 5 | 4.5 |
| Professional degree (MD, JD, etc.) | 9 | 8.2 |
| Current household ıncome (USD) | ||
| Over $150,000 | 31 | 28.2 |
| $100,000 to $150,000 | 25 | 22.7 |
| $75,000 to $99,999 | 26 | 23.6 |
| $50,000 to $74,999 | 14 | 12.7 |
| Below $50,000 | 9 | 8.2 |
| I'd prefer not to say | 5 | 4.5 |
| Number of children | ||
| 1 | 68 | 61.8 |
| 2 | 29 | 26.4 |
| 3 | 9 | 8.2 |
| 4 or more | 4 | 3.6 |
Note: Participants in New Zealand reported their household income in New Zealand dollars, so their responses have been converted to the approximate equivalent US‐dollar category. The US‐based and New Zealand‐based versions of the demographics surveys included slightly different race labels, in line with local guidelines. For simplicity, we have combined the (US‐based) category “White” and (New Zealand‐based) category “European/New Zealand European.”
Of the 120 participants initially recruited, two withdrew from the study due to time constraints. Eight participants were excluded due to low completion rates, having responded to fewer than 50% of EMA pings either for two consecutive weeks during the study period or by the end of the study (an exclusion criterion determined before data collection began). This resulted in a final sample size of 110, indicating a retention rate of 91.7%. We report information about the excluded participants in Text S1.
While we aimed to recruit only infants under 6 months of age, considering the significant role of early parent‐infant interactions on subsequent development and well‐being, recruitment challenges led us to include some older infants. The sample included a small number of infants between 6 and 9 months of age but is skewed to include more young infants than older ones (see Figure S1 for a histogram of infant ages). The participating infants were, on average, 3.67 months old at the start of the study (range: 0.17–8.93 months, interquartile range: 2.12 months). Five infants were born preterm (i.e., more than 3 weeks before their due date), and 58 of the infants were female (52.7%). We did not collect medical information about the infant, as our inclusion criteria were broad.
Caregivers were predominantly mothers (M age = 33.5 years; 104 female, 6 male) and were mostly White, highly educated, and socioeconomically advantaged (see Table 1 for demographics). Most participants had some degree of musical training; only 18 participants reported having had no formal musical training (see Table S1). At three points during the study, caregivers reported how they split caregiving with their partner or other adults (including daycare) on a typical day. Most caregivers (n = 103) reported providing at least 50% of childcare at all three time points.
Participant incentives included digital gift cards, a baby songbook, and baby clothing (a total value of approximately US$70), distributed over the course of the study. We also informed caregivers at the outset of the study that they would receive a personalized report summarizing their survey responses at the end of the study. This approach, inspired by gamified citizen science (e.g., Long et al. 2023; Liu et al. 2023), served as an additional motivation for study completion. An example report is in Figure S2.
1.2. Study Structure
We used an offset randomized design, with participants assigned to either a manipulation (n = 54) or control group (n = 56). The main portion of the study was 6 weeks long (Figure 1), with a pre‐test period (Week 1), a four‐week intervention period (Weeks 2–5), and a post‐test period (Week 6). Participation continued for four additional weeks following the post‐test, to provide an identical intervention period for the control group, so as to avoid biases stemming from group assignment. For group assignment, US participants were randomly assigned using a random number generator. By chance, this resulted in imbalanced sizes of the two groups in the US sample. To address this, we used random assignment with proportional weighting for the New Zealand sample, so as to arrive at evenly sized groups when recruitment was complete. EMA data were collected throughout the trial (see Section 1.3). Data collection took place from February to December 2023.
FIGURE 1.
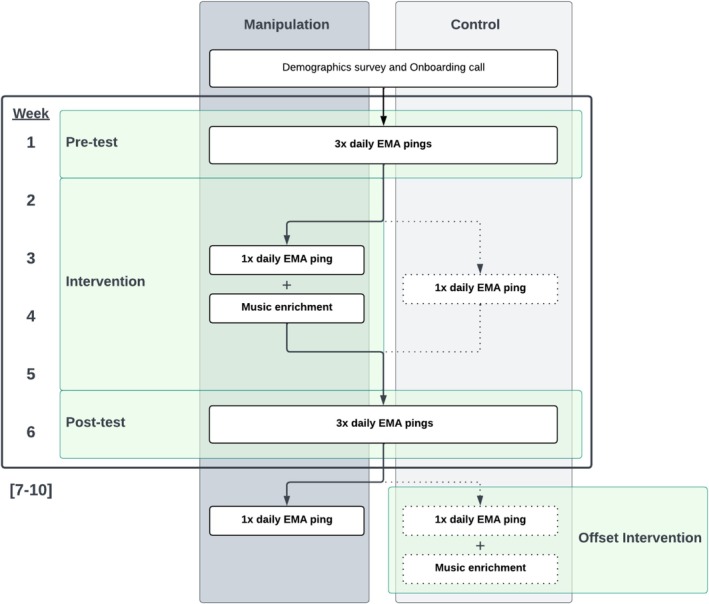
Structure of the experiment. We conducted an offset‐design randomized trial with a one‐week pre‐test, a four‐week intervention, and a one‐week post‐test (see the areas highlighted in green). This main study period was followed by four further weeks of study participation to accommodate the offset intervention period (for the control group). The left and right columns indicate the study flow for the manipulation and control groups, respectively. Both groups received the same number of EMA pings and followed identical procedures, except during the intervention period (Weeks 2–5), during which the manipulation group participated in the music enrichment intervention along with their daily EMA pings, while the control group only completed the EMA pings and had no intervention.
The study began with a one‐on‐one onboarding video call, where a designated researcher provided an overview of the study, guided participants in configuring their smartphones to receive EMA pings, and answered any questions. Participants were required to be physically present with their infants during the onboarding session to safeguard against fraudulent participation, a common concern in online developmental studies (Perkel 2020). The same researcher continued to serve as the participant's point of contact throughout the rest of the study.
1.3. Measures
The primary measures of infant and caregiver health were collected via EMA. We used a varied ping schedule, where caregivers received three EMA surveys per day during the pre‐test (Week 1) and post‐test (Week 6), delivered at randomly selected times in the morning, afternoon, and evening; and one EMA survey per day at all other times during the study, delivered at a randomly selected time during waking hours. In total, caregivers received 98 EMA surveys across the 10 weeks of the study. We did not require a minimum time between responses so as to maximize the amount of data we could analyze. EMA data collection was conducted either via The Person Project, a smartphone app developed by authors H.S. and D.T.; or via Qualtrics surveys accessed via URLs in text messages distributed with Inclivio (https://inclivio.com). Complete details about EMA methods are in Text S2.
The EMA surveys measured characteristics of infant and caregiver health in the 2–3 h prior to the ping, including 12 items on (1) infant mood, measured by valence and arousal; (2) infant distress and recovery, assessed through a pictorial scale of infant fussiness (Adams et al. 2019), and details on soothing techniques and duration for recovery; (3) caregiver mood and stress, measured by self‐assessed valence, impact, and rationality using the 3D Mind Model approach to mental state assessment (Thornton and Tamir 2020), along with self‐reported levels of caregiving‐related stress; and (4) musical behavior, measured by the frequency of caregivers' engagement with focus behaviors (i.e., singing and music listening). Every ping included an item asking whether the caregiver was with the infant during the 2–3 h prior to the ping. If the caregiver answered “No”, then no items were presented concerning the infant's state (see Text S3 for detail about this procedure and the full text of the EMA surveys). We also included questions concerning the previous day, such as the estimated frequency of infant‐directed singing, the frequency of infant night waking, and the duration taken to fall back asleep. During the pre‐test and post‐test, these previous‐day questions were only displayed once per day. The full text of the EMA surveys is in Text S3.
We also collected data in four longer‐form surveys spread throughout the study for analysis in a different paper comparing EMA responses to retrospective surveys; they are not reported here.
1.4. Music Enrichment Intervention
The goal of the intervention was to increase the frequency of infant‐directed singing in daily life while also expanding caregivers' repertoire of songs. We aimed to do so by teaching participants new songs to sing at home and providing materials designed to encourage more singing, in general, in the course of their caregiving. We did not collect data regarding the exact content or acoustic features of songs caregivers chose to sing to their infants, as we were interested in the effects of increased singing in whatever form caregivers felt was appropriate.
During the intervention, participants were given access to six instructional videos of unfamiliar songs presented in karaoke style, with lyrics synchronized to a bouncing ball indicating the rhythm (all videos are available at https://github.com/themusiclab/musical‐babies). These were displayed to participants either in The Person Project app or on YouTube (i.e., at private URLs), depending on the type of EMA caregivers used (see Text S2). Three videos were sent at the start of the intervention, with an additional three delivered halfway through. The songs were sourced from vintage songbooks and online archives of folk songs for children, then adapted for simplicity and ease of singing, especially for caregivers with limited music training. This process involved rewriting and arranging lyrics and melodies. The songs were recorded and produced by members of the research team who had extensive experience in early childhood music education (E.C., E.E., and S.A.M.).
Additionally, participants received an infant‐friendly songbook of their choice from a provided list (i.e., the Ditty Bird Musical Book series, Cali's Books series), delivered to their homes at the outset of the intervention. These books featured infant‐pressable buttons that activated song playback, accompanied by vibrant illustrations and lyrics.
Last, to further motivate caregivers to sing more to their infants, we sent weekly email newsletters to participants in the manipulation group during the intervention. The newsletters introduced ideas to incorporate singing into daily caregiving routines; highlighted the significance of singing in infancy; and presented research findings relevant to the benefits of musical parenting, in an easy‐to‐understand format. The control group received the same newsletters in the offset intervention period, but did not receive any newsletters during the main intervention.
To sustain participants' engagement over the four‐week intervention, the research team maintained regular communication with participants via text messages and emails. These check‐ins provided study updates, addressed any technical issues with the survey app, and reminded participants to complete missed surveys. Caregivers were not discouraged from singing outside of the intervention period; the intervention should be understood as supplementing existing levels of singing in the home, as opposed to suppressing such behaviors at non‐intervention periods or in the control group.
1.5. Compliance
Participants responded to a median of 72 out of 98 scheduled pings, for an overall response rate of 73.7%, with a higher rate outside of the pre‐ and post‐test periods (i.e., when only receiving one EMA ping per day; 78.4%) than during the pre‐ and post‐test periods (i.e., when receiving three EMA pings per day; 67.9%). This compliance rate is comparable to those reported in other infant EMA studies, including one‐week studies with intensive daily pings (de Barbaro et al. 2023; Wenze et al. 2023; Franchak 2019) and longitudinal studies lasting up to 16 weeks with less intensive pings (Allen et al. 2018; Franchak et al. 2024; Corpuz et al. 2023). We then fit linear models to test whether any demographic variables predicted compliance, using a bootstrap procedure with 1000 resamples to obtain robust estimates of the model coefficients.
Participants' response rates were unrelated to infant age at the start of the study (p = 0.44), total income (p = 0.95), number of siblings (p = 0.56), or the caregivers' scores on a postpartum depression inventory (Cox et al. 1987; p = 0.4). The proportion of unanswered pings was slightly higher in the control group, although this difference did not reach significance at pre‐test (p = 0.29), intervention (p = 0.09), or post‐test (p = 0.08). Given the comparable levels of missingness in the two groups, we assume that nonresponse represents missing data at random and did not attempt to account for missingness in our analyses.
To assess responsiveness to EMA pings, we calculated response latency by subtracting the time of the ping from the time participants opened the survey on their smartphone. The median response latency was approximately 20 min (high intensity weeks = 16 min; low intensity weeks = 23 min); this analysis was only available for participants whose pings were distributed by text message. A mixed‐effects time‐series model that accounted for autoregression across the 6 weeks of the study (with data averaged per day when multiple datapoints were available) showed that latency increased with infant age ( = 0.09, SE = 0.04, p = 0.02).
2. Results
2.1. Music Enrichment Increases the Frequency of Infant‐Directed Singing
We began by asking whether the intervention worked; namely, whether we succeeded in increasing the frequency of infant‐directed singing in the manipulation group, relative to the control group. Two EMA items addressed this question in different ways.
First, every EMA ping included an item asking caregivers whether they had sung to their infant in the preceding 2–3 h. They could respond “Yes” or “No”; the question was only asked of caregivers who reported having been with their infant in the previous 2–3 h (92.7% of all available data, see Measures). We dropped data where the caregiver indicated in the same EMA ping that their infant was sick (12.2% of data). Here and throughout, we computed weekly average scores using all available data from each participant.
Consistent with previous research using daylong audio recordings from infants' home environments (Hippe et al. 2024; Lerma‐Arregocés and Pérez‐Moreno 2024; Mendoza and Fausey 2021), music frequently featured in infants' and caregivers' lives even prior to the intervention. At pre‐test, caregivers reported having sung to their infants in the previous 2–3 h in 64.5% of surveys (SD = 22.5%). Caregivers also reported often playing recorded music to their infants (M = 38.4%, SD = 25.7%) and playing music for their own enjoyment (M = 31.7%, SD = 27.3%).
The intervention caused a clear increase in the frequency of infant‐directed song (Figure 2, left panel), with no difference between groups at pre‐test (proportion of “Yes” responses in manipulation group: M = 0.64, SD = 0.24; in control group: M = 0.65, SD = 0.22; Wilcoxon Rank‐Sum Test, W = 1461, p = 0.85), and a large (d = 0.61), statistically significant difference at post‐test (proportion of “Yes” responses in manipulation group: M = 0.77, SD = 0.2; in control group: M = 0.64, SD = 0.24; Wilcoxon Rank‐Sum Test, W = 1841, p = 0.003). Note that during post‐test, caregivers were no longer actively encouraged to sing more to their infants: Week 5 was the last week of the intervention. The effect of the intervention therefore persisted for at least 1 week beyond the intervention itself.
FIGURE 2.
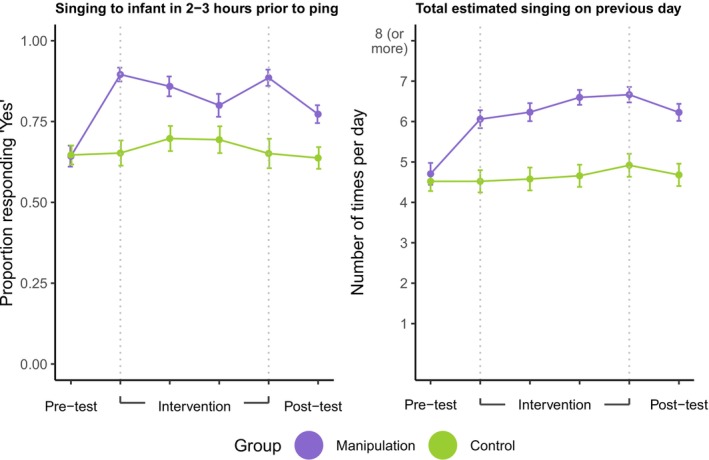
Music enrichment increases the frequency of infant‐directed singing. The plots depict responses to two items: “Did you sing to [baby] in the last 2–3 h?”, where “[baby]” was replaced by the infant's name (left panel), asked up to three times per day with response options “Yes” or “No”; and “If you had to guess, how many times did you sing to [baby] yesterday?” (right panel), asked once per day with response options ranging from “1” to “8 or more times”. There was a sharp increase in infant‐directed singing for the manipulation group, but not the control group, as measured by both items; the increase persisted through the full intervention and was maintained in the post‐test week. The tick marks on the x‐axis indicate the study week; Weeks 1 and 6 correspond to pre‐ and post‐test, respectively, while Weeks 2 through 5 span the intervention period. Note that for ease of visualization, here we plot weekly averages (points) and their corresponding standard errors of the mean (error bars), without accounting for temporal autocorrelation in responses over time. As such, the SEM values may be overestimating the precision of each estimate.
A mixed‐effects time‐series model that accounted for autoregression across the 6 weeks of the study (with data averaged per day when multiple datapoints were available) showed a significant group‐by‐time interaction ( = 0.26, SE = 0.12, p = 0.02). These effects were specific to infant‐directed singing, as we did not find comparable interaction effects for other music‐related variables that were also reported in the same EMA surveys, such as playing recorded music for the infant ( = −0.16, SE = 0.12, p = 0.18); or caregivers' personal music listening ( = 0.00, SE = 0.12, p = 0.98) in the 2–3 h preceding the EMA ping.
Notably, the absolute frequency of infant‐directed singing was substantial in the manipulation group: by the last week of the intervention, the proportion of times a caregiver had recently sung to their infant when they received an EMA ping was 0.89—almost all of the time—relative to 0.65 in the control group.
Second, caregivers reported an estimate of how many times they had sung to their infant on the previous day (“If you had to guess, how many times did you sing to [baby] yesterday?”) on an 8‐point scale ranging from “1” to “8 or more times”. Here too we found a clear effect of the intervention (Figure 2, right panel), with no group‐level difference at pre‐test (Wilcoxon Rank‐Sum Test, W = 1582.5, p = 0.56), a significant difference at post‐test (Wilcoxon Rank‐Sum Test, W = 2118.5, p < 0.001), and a significant group‐by‐timepoint interaction (Mixed‐effects time‐series model, = 0.03, SE = 0.01, p < 0.0001) indicating an estimated average increase of 0.28 singing episodes per week in the manipulation group (roughly 3.5% of the scale per week, for a cumulative total of 20.8% after the 6 weeks of intervention). While caregiver reports summarizing the previous day's singing with an integer may not be optimally precise, at the post‐test period these effects represented a 1.48 unit increase in absolute daily estimates of singing behavior (SD = 2.19).
Thus, convergent evidence demonstrates that the intervention succeeded at its primary goal, namely, to experimentally manipulate caregivers' infant‐directed singing in daily life.
2.2. Music Enrichment Increases the Use of Singing Specifically in the Context of Soothing Infants
Given the well‐known role of music in soothing or calming infants (e.g., Bainbridge et al. 2021), we wondered whether the intervention had not only general effects on the use of infant‐directed singing, but also specific effects in the context of soothing.
It did. In each EMA survey, we asked participants if their infant was fussy in the last 2–3 h. If so, they indicated all soothing techniques they used in response, from a list of 12 different techniques (e.g., feeding, changing a diaper, shushing, playing recorded music, singing; the full list is in Text S3). Parents reported that their infant was fussy (and not sick) in 41% of instances.
While the use of most soothing techniques remained more or less constant over the course of the study, in the manipulation group there was a large increase in the proportion of time caregivers used singing in response to fussy infants (Figure 3, left panel; pre‐test: M = 0.42, SD = 0.33; average across intervention: M = 0.63, SD = 0.40; post‐test: M = 0.61, SD = 0.35). While singing was the third most frequently used soothing technique among the 12 different techniques (both at pre‐test and overall), following movement‐based soothing (i.e., picking‐up, bouncing, rocking, or swinging) and feeding, singing was the only technique with increased caregiver use as a result of the intervention, an increase of 19 percentage points from pre‐test to post‐test (Wilcoxon Signed Rank Test, V = 769, p = 0.001).
FIGURE 3.
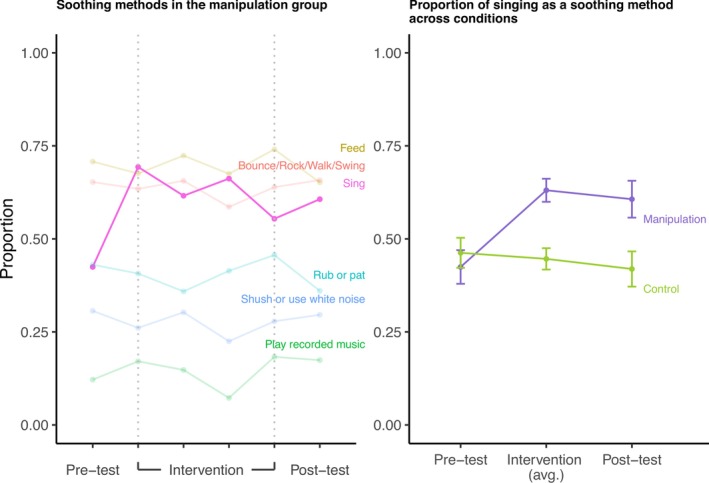
Music enrichment alters parent responses to infant fussiness. In each EMA ping, we asked the parent if their infant was fussy in the previous 2–3 h; if they answered “Yes”, then we asked how they attempted to soothe the infant. The left panel illustrates the proportion of responses in the manipulation group for six soothing techniques (of 12 available options; see Text S3). Tick marks indicate the study week; Weeks 1 and 6 correspond to pre‐ and post‐test, respectively, whereas Weeks 2 through 5 span the intervention period. Singing in response to fussiness was the only soothing technique out of 12 that showed a substantive increase in usage from pre‐ to post‐test. This increase was specific to the manipulation group, as shown in the right panel, which rescales the data as a proportion of all responses and averages across the four intervention weeks (Weeks 2–5). In the manipulation group, parents used singing in response to fussiness more than half of the time. The points indicate mean scores across the given week(s) and error bars denote standard errors of the mean.
No such increase was observed in the control group; however, there, the singing response stayed relatively flat (Wilcoxon Signed Rank Test, V = 365.5, p = 0.4; Figure 3, right panel). The cross‐group difference at post‐test was statistically significant (Wilcoxon Rank‐Sum Test, W = 1642.5, p = 0.006). Notably, we did not observe a group‐level difference at post‐test in the frequency of playing recorded music to infants, indicating that the effect did not reflect a general increase in the use of music to soothe infants (Wilcoxon Rank‐Sum Test, W = 1274.5, p = 0.85). Rather, it was specific to singing.
Thus, music enrichment not only increased the overall use of infant‐directed singing in daily life, but specifically influenced how caregivers responded to infant fussiness. We note here that caregivers were not explicitly instructed to use music in the context of soothing. The newsletters provided general suggestions for incorporating music into many different infant care contexts, one of which was soothing; the specific increase of the use of music in this context suggests that the decision to use music for soothing was likely an intuitive one.
2.3. Infant‐Directed Singing Improves Infant Mood but Not Caregiver Mood
As music has been shown to affect a variety of affect‐ and arousal‐related variables in infants in the short term (e.g., Bainbridge et al. 2021; Cirelli and Trehub 2020; Corbeil et al. 2016), a key question for this randomized trial is whether such effects are cumulative. Does music enrichment produce lasting effects on infant affect?
To study this question, we focused primarily on caregiver evaluations of infant mood, reported using a sliding scale from Negative (0) to Positive (100). In each EMA survey, caregivers rated their infant's mood during the last 2–3 h. Caregivers only responded if they had been with their infant during that time.
Importantly, this item does not measure caregivers' perceptions of infants' moods in response to singing. Rather, the item measures perceptions of infant mood in general.
To account for participant variability in scale usage, we z‐scored mood ratings within participants. We then computed a weekly average score for each infant. Consistent with other research showing less frequent crying as infants grow older (Barr 1990), infants showed improvements in mood from pre‐ to post‐test, on average (mean difference = 0.25; Wilcoxon Signed Rank Test, V = 4128, p < 0.0001).
These improvements were moderated by the manipulation group; however, (Figure 4, left panel). At pre‐test, the two groups did not differ (in z‐scores, manipulation group: M = −0.10, SD = 0.41; control group: M = −0.11, SD = 0.30; Wilcoxon Rank‐Sum Test, W = 1520, p = 0.58), but at post‐test, the intervention had caused a significant difference in infant mood, with the manipulation group approximately 0.18 standard deviations higher (manipulation group: M = 0.24, SD = 0.32; control group: M = 0.06, SD = 0.32; Wilcoxon Rank‐Sum Test, W = 1822, p = 0.004).
FIGURE 4.
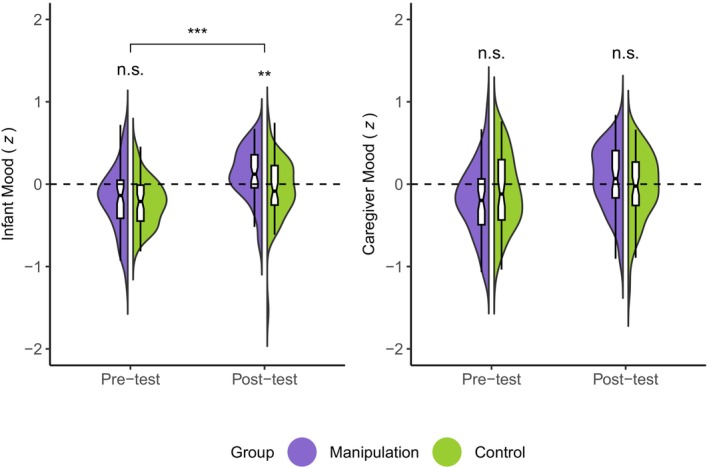
Music enrichment improves infant mood but not caregiver mood. In each EMA ping, caregivers were asked to report their infant's mood and their own mood during the previous 2–3 h, both on a 100‐point slider anchored at “Very negative” and “Very positive”. We normalized responses within participants to account for individual differences in scale use. While the average mood of infants in the two groups did not differ at pre‐test, it did at post‐test, with significantly more positive mood reports in the manipulation group (left panel). We did not observe the same pattern for caregiver mood (right panel). The half‐violins depict the distributions of weekly mean mood ratings from each of the two groups, weighted by participant. The shaded area in the half‐violins represents kernel density estimates; the boxplots denote the median (horizontal line), 95% confidence interval (notches), and interquartile range (edges of the boxes). The significance stars above the violins denote the between‐groups comparison at a given time point. The horizontal bar denotes the significant group‐by‐time interaction in the time‐series model. *p < 0.05, **p < 0.01, ***p < 0.001.
A mixed‐effects time‐series model (using untransformed data and daily averages of individuals' responses when multiple datapoints were available) that accounted for autoregression showed a significant group‐by‐time interaction ( = 0.18, SE = 0.05, p < 0.001). In the manipulation group, each week of intervention was associated with a 1.56‐unit increase in the 100‐point mood scale for infants in the manipulation group (p < 0.001), or roughly one tenth of a SD increase per week of intervention.
We tested the robustness of this effect by asking whether it repeated in two subsets of the main sample: a first cohort, recruited mainly in the United States from February to June 2023; and a second cohort, recruited mainly in New Zealand from June to December 2023. Mixed‐effects time‐series models revealed the same expected group‐by‐time interaction in both the first ( = 0.12, SE = 0.06, p = 0.04) and second cohorts ( = 0.32, SE = 0.10, p = 0.001).
Caregivers also rated how energetic their infants were in the previous 2–3 h, using a similar scale to the mood item; we found no corresponding effects on this measure, suggesting the effects of music enrichment are specific to infant mood and do not generalize to infant arousal.
We proceeded by analyzing data concerning caregiver mood for two reasons. First, improvements to infant mood might well translate to improvements in caregiver mood since happier infants are easier to look after than fussier ones. Second, a concern with the infant mood result is the potential for contamination in caregiver self‐reports: they might erroneously report happier infants when they themselves felt happier. Because this experiment relies on caregiver EMA data, we are unable to directly assess infant mood in isolation from the caregiver.
We addressed these issues with several analyses of caregivers' responses to ratings of their own mood, completed in the same EMA surveys and using the same normalization approach as the infant mood item. In contrast to infant mood, we found no differences between groups at pre‐test (Figure 4, right panel; manipulation group: M = −0.15, SD = 0.46; control group: M = −0.02, SD = 0.48; Wilcoxon Rank‐Sum Test, W = 1213, p = 0.18) or post‐test (manipulation group: M = 0.14, SD = 0.43; control group: M = 0.03, SD = 0.48; Wilcoxon Rank‐Sum Test, W = 1543, p = 0.29). This absence of effect suggests that the effect of music enrichment on caregiver self‐reports of infant mood does not erroneously represent an effect on caregiver mood.
Infant mood and caregiver mood were moderately and positively correlated, however (Spearman's rank correlation; r = 0.39, p < 0.0001), and adding caregiver mood as a predictor to the mixed model regressing condition and day number on infant mood weakened the time‐by‐group interaction enough that it no longer reached statistical significance (p = 0.09). While the correlation between infant and caregiver mood could indicate a true relation between these variables, a response bias, or both, we found no evidence for a difference in the size of the correlation across the manipulation and control groups ( = 0.01, p = 0.59); this suggests that any reporting biases, should they exist, are not attributable to the intervention.
To further assess the degree of potential confounding between infant and caregiver mood reports, we tested whether each of the infant and caregiver mood self‐reports correlated with other measures that should be expected to be more strongly linked to caregiver mood than infant mood. Two variables in the daily EMA surveys met this criterion: a measure of how socially connected caregivers felt (from “Very lonely” to “Very connected”) and a measure of the perceived stress of caregiving (“How stressful have you found parenting in the last 2–3 h?”).
The association of social connection and caregiver mood ( = 0.44, p < 0.0001) was both stronger and in the opposite direction of the association between social connection and infant mood ( = −0.08, p = 0.02; interaction: = 0.002, p < 0.0001; autoregressive time series model with untransformed mood data). Similarly, while both infant ( = −0.017, p < 0.0001) and caregiver mood ( = −0.019, p < 0.0001) predicted how stressful caregivers found parenting, the interaction between the two mood variables was statistically significant ( = 0.0001, p < 0.0001), indicating a significantly stronger relation between caregiver mood and parenting stress than between caregiver mood and infant mood. These results suggest that our measures of infant mood and caregiver mood tapped into substantively different phenomena and were not fully confounded.
In sum, we found a causal effect of music enrichment on infant mood, but not caregiver mood, despite the two mood measures being correlated with one another. It is possible that increasing the frequency of infant‐directed singing may improve both infants' and caregivers' moods, whether directly (e.g., singing makes caregivers feel positive) or indirectly (e.g., having a happier infant makes caregivers feel positive). If so, putative effects on caregiver mood are small enough that they could not be reliably detected in this brief intervention study.
3. Discussion
We report evidence that a brief singing intervention increases the frequency of infant‐directed singing, that caregivers intuitively extend this musical behavior specifically to the context of soothing their infants, and that these changes in the home musical environment cause improvements to infant mood in general. This suggests that the immediate effects of music on infants' moods (e.g., Bainbridge et al. 2021; Cirelli et al. 2020; Cirelli and Trehub 2020; Corbeil et al. 2016; Shenfield et al. 2003) may be cumulative, leading to longer‐term effects.
Importantly, the effect of the music enrichment intervention on infant mood was detected in EMA data collected regardless of whether the caregiver had recently sung to the infant (i.e., as opposed to measuring infants' mood responses to singing in particular). This implies that infant‐directed singing improved infant mood in general, in a one‐week post‐test period that followed the intervention (at which time we were no longer telling caregivers to sing to their infants). The present findings therefore substantiate a causal relation between an enriched musical environment and general improvements in infant mood.
Moreover, while this result is supported only by caregiver‐observational data, several considerations suggest that the findings reflect robust changes in infant affect. First, the data were collected with EMA, instead of retrospective surveys, and therefore are unlikely to be contaminated by recall bias (Stone and Shiffman 2002; Reis 2012). Second, the results largely replicated internally, in two separate samples recruited in two different countries, and therefore are unlikely to reflect the caregiving practices of only one community. Third, we found no corresponding effect of the intervention on caregiver mood, suggesting that caregivers' self‐reports of infant mood did not simply reflect caregivers' own mood, as they might in the presence of a reporting bias. Fourth, the modest correlation between caregiver reports of infant mood and their own mood was of a comparable size in both the manipulation and control groups, suggesting that a social‐desirability effect (e.g., where parents who had experienced the intervention reported higher infant mood because they felt obligated to do so) did not account for the main effects. Future studies can more precisely investigate the validity of infant mood assessment via EMA by supplementing the method with direct, independent lab‐based or home‐based observations of infant mood and behavior, psychophysiological measures of infant arousal, and so on.
Infant mood is an important issue for caregivers as it is closely linked to parenting stress (Oddi et al. 2013), caregiver‐infant bonding and attachment (Nolvi et al. 2016; Takács et al. 2020), and subsequently the infants' social and emotional development (Steele et al. 2008; Shaw and Dallos 2005). These associations raise the possibility that general improvements in infant mood, caused by altering the home music environment in young families, could subsequently cause other positive health‐related outcomes. While we did not observe any such effects here (such as an improvement in caregiver mood), we note that this study had only a brief (4‐week), low‐intensity, self‐directed intervention. A longer‐term, higher‐intensity intervention, perhaps with direct music instruction from a qualified teacher, may well uncover more widespread effects. These could potentially generalize to other health domains that are tightly related to caregivers' well‐being, such as the frequency of infant night waking, the duration of crying bouts, the ease with which caregivers can calm their infants when upset, or levels of caregiver stress.
Infant‐directed singing is a multifaceted mode of communication and interaction, including a variety of distinct musical attributes, such as exaggerated melodic contours, high pitch variability, repetitive rhythmic patterns (e.g., Malloch and Trevarthen 2009; Hilton et al. 2022); in conjunction with other caregiving behaviors, such as increased physical proximity, infant‐directed attention, touch, rocking, and infant‐directed speech (Mehr and Krasnow 2017; Mehr et al. 2021; Trehub and Gudmundsdottir 2019). We cannot yet know which of these specific characteristics or behaviors are the ones that caused improvements in infant mood, as the intervention likely altered all of them. Future randomized trials that include active control groups may determine the degree to which singing specifically alters infant temperament, over and above the many positive caregiving behaviors that are associated with singing.
We note that prior to the intervention, music was already well integrated into daily routines in many families in our sample, with parents reporting several instances of singing to their infants each day, on average. This aligns with previous research highlighting the widespread use of music, especially singing, in infancy (Yan et al. 2021; Custodero et al. 2003; Fancourt and Perkins 2018c; Ilari 2005), although a recent report using more precise measurement of the home auditory environment (via daylong audio recordings) found surprisingly low rates of music exposure across infancy (Hippe et al. 2024). Despite the pre‐existing musical engagement, the brief intervention led to a further increase in both the frequency of daily singing and its use for soothing fussy infants, as reflected in EMA reports, while no significant changes in music listening frequency were observed. If the limited musical input reported by Hippe et al. (2024) better reflects infants' environmental norms, the potential effects of music enrichment interventions may be underestimated here, in fact.
We also note several limitations of our sample. Demographic factors, such as education and socioeconomic status, can closely shape parenting behaviors and attitudes (Bradley and Corwyn 2002), including their everyday use of music with infants. As the majority of our participants were White, highly educated, and socially or economically advantaged, it is not yet clear whether the longer‐term effects of music enrichment will generalize to other populations. The inclusion of more diverse samples is essential for future studies.
On a methodological note, our findings demonstrate the feasibility of long‐term EMA studies in young infants and their caregivers. We observed that consistent engagement in the study over a 10‐week period, while learning from the intervention and integrating that learning into caregivers' daily routines with young infants, was manageable for caregivers, based on the low level of attrition and high level of compliance. EMA is commonly used in studies of adults but is relatively underused by developmentalists; when used, studies are typically short, spanning less than 2 weeks (e.g., de Barbaro et al. 2023; Franchak 2019; Wenze et al. 2023). While latency to ping response did vary in our data, including an increase in response time as infants grew older, very few families dropped out of the study (i.e., a retention rate of 92%), despite our asking caregivers to respond to nearly 100 surveys in 10 weeks.
We believe the EMA method complements traditional laboratory‐based or retrospective survey designs because it enables the collection of repeated, naturalistic observations of infant and caregiver behaviors and psychological states, which fluctuate both daily and over extended periods. Although infant EMA research is limited by infants' inability to report on their own behaviors and mental states (i.e., caregivers are responsible for assessing and reporting their infants' moods), analyses of the relations between caregiver‐reported infant mood and caregiver mood may provide some optimism that the recruitment of caregivers as “scientist‐observers” does not imply compromised data quality. As such, we encourage the research community to consider EMA in infant studies.
Last, we note that the primary caregivers of young infants studied here were quite happy to engage with a multi‐week music intervention, despite having relatively little music training, on average; and despite being presumably quite busy, stressed‐out primary caregivers of young infants. At the end of the study, the vast majority of caregivers reported that they would continue singing to their infants after the study (90.3%), and self‐reported their overall experience in the study as positive, particularly appreciating the opportunities to actively incorporate music into their daily lives and experience the positive impacts singing had on their infants as well as themselves (see Text S4 for further information and results from the exit survey). These findings, combined with the ease of carrying out the intervention, its very low cost, and its other reported effects, suggest a strong potential for music enrichment to improve infant and caregiver health.
Author Contributions
S.A.M. conceived of the research, provided funding, supervised the study team, and coordinated all research activities. D.I.T. provided funding for the Person Project data collection platform. E.C., L.Y., E.E., B.M., and S.A.M. contributed to the study design and materials development, including the music enrichment intervention. E.L., M.B., P.B., and B.M. provided research assistance. C.B.H. led the implementation of the study on the Person Project data collection platform, with additional contributions from H.S., S.A.M., and D.I.T. E.L. and S.A.M. implemented the study on the Inclivio data collection platform. E.C., L.Y., E.E., and E.L. collected data and managed all communication with participants. L.Y. wrote analysis code, with additional contributions from E.C., C.B.H., and S.A.M. C.B.H. conducted a review of the code and statistical analyses. L.Y., E.C., and S.A.M. designed the figures. E.C., L.Y., and S.A.M. wrote the manuscript, and all authors edited or approved it.
Supporting information
Data S1.
Acknowledgments
We thank the families for their participation; Stacey Sinclair, Epi Torres, Katie Ippolito, and Nicole Shelton for their support on The Person Project; Anna Bergson, S. Atwood, and Anya Keomurjian for research assistance; Danilo Lombardo for assisting with producing music enrichment intervention materials; and the members of The Music Lab for helpful discussions and feedback. Jerome Kagan, who passed away in May 2021, contributed early ideas that led to this work in lively conversation with S.A.M. Open access publishing facilitated by The University of Auckland, as part of the Wiley ‐ The University of Auckland agreement via the Council of Australian University Librarians.
Funding: This research was supported by grants from the US National Institutes of Health (DP5OD024566 and R21HD113998), the Royal Society of New Zealand Te Apārangi (Rutherford Discovery Fellowship RDF‐UOA2103), and the University of Auckland (Research Development Fund and Early Career Research Excellence Award) to S.A.M. The Person Project was supported by a grant from Princeton University (Eric and Wendy Schmidt Transformative Technology Fund) to D.I.T.
Eun Cho and Lidya Yurdum have contributed equally.
Contributor Information
Eun Cho, Email: eun.cho@yale.edu.
Lidya Yurdum, Email: lidya.yurdum@yale.edu.
Samuel A. Mehr, Email: sam@yale.edu.
Data Availability Statement
A fully reproducible manuscript; data; analysis and visualization code; and other materials are available at https://github.com/themusiclab/musical‐babies and is permanently archived at https://doi.org/10.5281/zenodo.15181606. Analyses were exploratory and not preregistered.
References
- Adams, E. L. , Marini M. E., Brick T. R., Paul I. M., Birch L. L., and Savage J. S.. 2019. “Ecological Momentary Assessment of Using Food to Soothe During Infancy in the INSIGHT Trial.” International Journal of Behavioral Nutrition and Physical Activity 16: 79. 10.1186/s12966-019-0837-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen, A. , Tosun N., Carlson S., and Allen S.. 2018. “Postpartum Changes in Mood and Smoking‐Related Symptomatology: An Ecological Momentary Assessment Investigation.” Nicotine & Tobacco Research 20: 681–689. 10.1093/ntr/ntx118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bainbridge, C. M. , Bertolo M., Youngers J., et al. 2021. “Infants Relax in Response to Unfamiliar Foreign Lullabies.” Nature Human Behaviour 5: 256–264. 10.1038/s41562-020-00963-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barr, R. G. 1990. “The Normal Crying Curve: What Do we Really Know?” Developmental Medicine and Child Neurology 32: 356–362. 10.1111/j.1469-8749.1990.tb16949.x. [DOI] [PubMed] [Google Scholar]
- Bind, R. H. , Sawyer K., Hazelgrove K., et al. 2023. “Feasibility, Clinical Efficacy, and Well‐Being Outcomes of an Online Singing Intervention for Postnatal Depression in the UK: SHAPER‐PNDO, a Single‐Arm Clinical Trial.” Pilot and Feasibility Studies 9, no. 1: 131. 10.1186/s40814-023-01360-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowlby, J. 1969. Attachment and Loss. Vol. I. Basic Books. [Google Scholar]
- Bradley, R. H. , and Corwyn R. F.. 2002. “Socioeconomic Status and Child Development.” Annual Review of Psychology 53: 371–399. 10.1146/annurev.psych.53.100901.135233. [DOI] [PubMed] [Google Scholar]
- Byrn, M. D. , and Hourigan R.. 2010. “A Comparative Case Study of Music Interactions Between Mothers and Infants.” Contributions to Music Education 37: 65–79. [Google Scholar]
- Cho, E. , and Ilari B. S.. 2021. “Mothers as Home DJs: Recorded Music and Young Children's Well‐Being During the Covid‐19 Pandemic.” Frontiers in Psychology 12: 637569. 10.3389/fpsyg.2021.637569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cirelli, L. K. , Jurewicz Z. B., and Trehub S. E.. 2020. “Effects of Maternal Singing Style on Mother‐Infant Arousal and Behavior.” Journal of Cognitive Neuroscience 32: 1213–1220. 10.1162/jocn_a_01402. [DOI] [PubMed] [Google Scholar]
- Cirelli, L. K. , and Trehub S. E.. 2020. “Familiar Songs Reduce Infant Distress.” Developmental Psychology 56: 861–868. 10.1037/dev0000917. [DOI] [PubMed] [Google Scholar]
- Corbeil, M. , Trehub S. E., and Peretz I.. 2016. “Singing Delays the Onset of Infant Distress.” Infancy 21: 373–391. 10.1111/infa.12114. [DOI] [Google Scholar]
- Corpuz, R. , Kotov D. A., and Donovan R. L.. 2023. “Earlier Sexual Debut Predicts Higher (Not Lower) Levels of Father Care Measured Across 12 Weeks: An Experience Sampling Study.” Frontiers in Psychology 14: 1199735. 10.3389/fpsyg.2023.1199735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox, J. L. , Holden J. M., and Sagovsky R.. 1987. “Detection of Postnatal Depression: Development of the 10‐Item Edinburgh Postnatal Depression Scale.” British Journal of Psychiatry 150: 782–786. 10.1192/bjp.150.6.782. [DOI] [PubMed] [Google Scholar]
- Custodero, L. A. , and Johnson‐Green E. A.. 2003. “Passing the Cultural Torch: Musical Experience and Musical Parenting of Infants.” Journal of Research in Music Education 51: 102–114. 10.2307/3345844. [DOI] [Google Scholar]
- Custodero, L. A. , Rebello Britto P., and Brooks‐Gunn J.. 2003. “Musical Lives: A Collective Portrait of American Parents and Their Young Children.” Journal of Applied Developmental Psychology 24: 553–572. 10.1016/j.appdev.2003.08.005. [DOI] [Google Scholar]
- de Barbaro, K. , Micheletti M., Yao X., Khante P., Johnson M., and Goodman S.. 2023. “Infant Crying Predicts Real‐Time Fluctuations in Maternal Mental Health in Ecologically Valid Home Settings.” Developmental Psychology 59: 733–744. 10.1037/dev0001530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennis, C.‐L. , and Ross L.. 2006. “Women's Perceptions of Partner Support and Conflict in the Development of Postpartum Depressive Symptoms.” Journal of Advanced Nursing 56: 588–599. 10.1111/j.1365-2648.2006.04059.x. [DOI] [PubMed] [Google Scholar]
- Fancourt, D. , and Perkins R.. 2018a. “Effect of Singing Interventions on Symptoms of Postnatal Depression: Three‐Arm Randomised Controlled Trial.” British Journal of Psychiatry 212: 119–121. 10.1192/bjp.2017.29. [DOI] [PubMed] [Google Scholar]
- Fancourt, D. , and Perkins R.. 2018b. “The Effects of Mother–Infant Singing on Emotional Closeness, Affect, Anxiety, and Stress Hormones.” Music & Science 1: 205920431774574. 10.1177/2059204317745746. [DOI] [Google Scholar]
- Fancourt, D. , and Perkins R.. 2018c. “Maternal Engagement With Music up to Nine Months Post‐Birth: Findings From a Cross‐Sectional Study in England.” Psychology of Music 46: 238–251. 10.1177/0305735617705720. [DOI] [Google Scholar]
- Feldman, R. , Granat A., Pariente C., Kanety H., Kuint J., and Gilboa‐Schechtman E.. 2009. “Maternal Depression and Anxiety Across the Postpartum Year and Infant Social Engagement, Fear Regulation, and Stress Reactivity.” Journal of the American Academy of Child & Adolescent Psychiatry 48: 919–927. 10.1097/CHI.0b013e3181b21651. [DOI] [PubMed] [Google Scholar]
- Feldman, R. , Rosenthal Z., and Eidelman A. I.. 2014. “Maternal‐Preterm Skin‐To‐Skin Contact Enhances Child Physiologic Organization and Cognitive Control Across the First 10 Years of Life.” Biological Psychiatry 75: 56–64. 10.1016/j.biopsych.2013.08.012. [DOI] [PubMed] [Google Scholar]
- Franchak, J. M. 2019. “Changing Opportunities for Learning in Everyday Life: Infant Body Position Over the First Year.” Infancy 24: 187–209. 10.1111/infa.12272. [DOI] [PubMed] [Google Scholar]
- Franchak, J. M. , Kadooka K., and Fausey C. M.. 2024. “Longitudinal Relations Between Independent Walking, Body Position, and Object Experiences in Home Life.” Developmental Psychology 60: 228–242. 10.1037/dev0001678. [DOI] [PubMed] [Google Scholar]
- Fries, A. B. W. , Ziegler T. E., Kurian J. R., Jacoris S., and Pollak S. D.. 2005. “Early Experience in Humans Is Associated With Changes in Neuropeptides Critical for Regulating Social Behavior.” Proceedings of the National Academy of Sciences 102: 17237–17240. 10.1073/pnas.0504767102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerry, D. , Unrau A., and Trainor L. J.. 2012. “Active Music Classes in Infancy Enhance Musical, Communicative and Social Development.” Developmental Science 15: 398–407. 10.1111/j.1467-7687.2012.01142.x. [DOI] [PubMed] [Google Scholar]
- Hilton, C. B. , Moser C. J., Bertolo M., et al. 2022. “Acoustic Regularities in Infant‐Directed Speech and Song Across Cultures.” Nature Human Behaviour 6: 1545. 10.1101/2020.04.09.032995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hippe, L. , Hennessy V., Ramirez N. F., and Zhao T. C.. 2024. “Comparison of Speech and Music Input in North American Infants' Home Environment Over the First 2 Years of Life.” Developmental Science 27: e13528. 10.1111/desc.13528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ilari, B. 2005. “On Musical Parenting of Young Children: Musical Beliefs and Behaviors of Mothers and Infants.” Early Child Development and Care 175: 647–660. 10.1080/0300443042000302573. [DOI] [Google Scholar]
- Kotler, J. , Mehr S. A., Egner A., Haig D., and Krasnow M. M.. 2019. “Response to Vocal Music in Angelman Syndrome Contrasts With Prader‐Willi Syndrome.” Evolution and Human Behavior 40: 420–426. 10.1016/j.evolhumbehav.2019.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lense, M. D. , Shultz S., Astésano C., and Jones W.. 2022. “Music of Infant‐Directed Singing Entrains Infants' Social Visual Behavior.” Proceedings of the National Academy of Sciences 119: e2116967119. 10.1073/pnas.2116967119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lerma‐Arregocés, D. , and Pérez‐Moreno J.. 2024. “Musical Communication Among Parents and Their Children: An Analysis Tool to Study Their Interaction.” International Journal of Music Education 42: 409–424. 10.1177/02557614231174033. [DOI] [Google Scholar]
- Liu, J. , Hilton C. B., Bergelson E., and Mehr S. A.. 2023. “Language Experience Predicts Music Processing in a Half‐Million Speakers of Fifty‐Four Languages.” Current Biology 33: 1916–1925.e4. 10.1016/j.cub.2023.03.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Long, B. , Simson J., Buxó‐Lugo A., Watson D. G., and Mehr S. A.. 2023. “How Games Can Make Behavioural Science Better.” Nature 613: 433–436. 10.1038/d41586-023-00065-6. [DOI] [PubMed] [Google Scholar]
- Malloch, S. N. 1999. “Mothers and Infants and Communicative Musicality.” Musicae Scientiae 3: 29–57. 10.1177/10298649000030S104. [DOI] [Google Scholar]
- Malloch, S. N. , and Trevarthen C.. 2009. Communicative Musicality: Exploring the Basis of Human Companionship. Oxford University Press. [Google Scholar]
- Mehr, S. A. 2014. “Music in the Home: New Evidence for an Intergenerational Link.” Journal of Research in Music Education 62: 78–88. 10.1177/0022429413520008. [DOI] [Google Scholar]
- Mehr, S. A. , Kotler J., Howard R. M., Haig D., and Krasnow M. M.. 2017. “Genomic Imprinting Is Implicated in the Psychology of Music.” Psychological Science 28: 1455–1467. 10.1177/0956797617711456. [DOI] [PubMed] [Google Scholar]
- Mehr, S. A. , and Krasnow M. M.. 2017. “Parent‐Offspring Conflict and the Evolution of Infant‐Directed Song.” Evolution and Human Behavior 38: 674–684. 10.1016/j.evolhumbehav.2016.12.005. [DOI] [Google Scholar]
- Mehr, S. A. , Krasnow M. M., Bryant G. A., and Hagen E. H.. 2021. “Origins of Music in Credible Signaling.” Behavioral and Brain Sciences 44: e60. 10.1017/S0140525X20000345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehr, S. A. , Singh M., Knox D., et al. 2019. “Universality and Diversity in Human Song.” Science 366: 957–970. 10.1126/science.aax0868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehr, S. A. , Song L. A., and Spelke E. S.. 2016. “For 5‐Month‐Old Infants, Melodies Are Social.” Psychological Science 27: 486–501. 10.1177/0956797615626691. [DOI] [PubMed] [Google Scholar]
- Mehr, S. A. , and Spelke E. S.. 2017. “Shared Musical Knowledge in 11‐Month‐Old Infants.” Developmental Science 21, no. 2: e12542. 10.1111/desc.12542. [DOI] [PubMed] [Google Scholar]
- Mendoza, J. K. , and Fausey C. M.. 2021. “Everyday Music in Infancy.” Developmental Science 24: e13122. 10.31234/osf.io/sqatb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore, E. R. , Anderson G. C., Bergman N., and Dowswell T.. 2012. “Early Skin‐to‐Skin Contact for Mothers and Their Healthy Newborn Infants.” In Cochrane Database of Systematic Reviews, edited by The Cochrane Collaboration , CD003519. John Wiley & Sons, Ltd. 10.1002/14651858.CD003519.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolvi, S. , Karlsson L., Bridgett D. J., Pajulo M., Tolvanen M., and Karlsson H.. 2016. “Maternal Postnatal Psychiatric Symptoms and Infant Temperament Affect Early Mother‐Infant Bonding.” Infant Behavior and Development 43: 13–23. 10.1016/j.infbeh.2016.03.003. [DOI] [PubMed] [Google Scholar]
- Oddi, K. B. , Murdock K. W., Vadnais S., Bridgett D. J., and Gartstein M. A.. 2013. “Maternal and Infant Temperament Characteristics as Contributors to Parenting Stress in the First Year Postpartum.” Infant and Child Development 22: 553–579. 10.1002/icd.1813. [DOI] [Google Scholar]
- Perkel, J. M. 2020. “Mischief‐Making Bots Attacked My Scientific Survey.” Nature 579: 461. 10.1038/d41586-020-00768-0. [DOI] [PubMed] [Google Scholar]
- Perkins, R. , Yorke S., and Fancourt D.. 2018. “How Group Singing Facilitates Recovery From the Symptoms of Postnatal Depression: A Comparative Qualitative Study.” BMC Psychology 6: 41. 10.1186/s40359-018-0253-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Persico, G. , Antolini L., Vergani P., Costantini W., Nardi M. T., and Bellotti L.. 2017. “Maternal Singing of Lullabies During Pregnancy and After Birth: Effects on Mother–Infant Bonding and on Newborns' Behaviour. Concurrent Cohort Study.” Women and Birth 30: e214–e220. 10.1016/j.wombi.2017.01.007. [DOI] [PubMed] [Google Scholar]
- Reid, K. M. , and Taylor M. G.. 2015. “Social Support, Stress, and Maternal Postpartum Depression: A Comparison of Supportive Relationships.” Social Science Research 54: 246–262. 10.1016/j.ssresearch.2015.08.009. [DOI] [PubMed] [Google Scholar]
- Reis, H. T. 2012. “Why Researchers Should Think “Real‐World”: A Conceptual Rationale.” In Handbook of Research Methods for Studying Daily Life, 3–21. Guilford Press. [Google Scholar]
- Roubinov, D. S. , and Boyce W. T.. 2017. “Parenting and SES: Relative Values or Enduring Principles?” Current Opinion in Psychology 15: 162–167. 10.1016/j.copsyc.2017.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schore, A. N. 2005. “Back to Basics.” Pediatrics in Review 26: 204–217. 10.1542/pir.26.6.204. [DOI] [PubMed] [Google Scholar]
- Shaw, S. K. , and Dallos R.. 2005. “Attachment and Adolescent Depression: The Impact of Early Attachment Experiences.” Attachment & Human Development 7: 409–424. 10.1080/14616730500365902. [DOI] [PubMed] [Google Scholar]
- Shenfield, T. , Trehub S. E., and Nakata T.. 2003. “Maternal Singing Modulates Infant Arousal.” Psychology of Music 31: 365–375. 10.1177/0305735603031400. [DOI] [Google Scholar]
- Shonkoff, J. P. , Garner A. S., Siegel B. S., et al. 2012. “The Lifelong Effects of Early Childhood Adversity and Toxic Stress.” Pediatrics 129: e232–e246. 10.1542/peds.2011-2663. [DOI] [PubMed] [Google Scholar]
- Singh, M. , and Mehr S. A.. 2023. “Universality, Domain‐Specificity and Development of Psychological Responses to Music.” Nature Reviews Psychology 2: 333–346. 10.1038/s44159-023-00182-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, A. R. , Salley B., Hanson‐Abromeit D., et al. 2024. “The Impact of a Community‐Based Music Program During Infancy on the Quality of Parent–Child Language Interactions.” Child Development 95: 481–496. 10.1111/cdev.14005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stams, G.‐J. J. M. , Juffer F., and van IJzendoorn M. H.. 2002. “Maternal Sensitivity, Infant Attachment, and Temperament in Early Childhood Predict Adjustment in Middle Childhood: The Case of Adopted Children and Their Biologically Unrelated Parents.” Developmental Psychology 38, no. 5: 806. 10.1037/0012-1649.38.5.806. [DOI] [PubMed] [Google Scholar]
- Steele, H. , Steele M., and Croft C.. 2008. “Early Attachment Predicts Emotion Recognition at 6 and 11 Years Old.” Attachment & Human Development 10: 379–393. 10.1080/14616730802461409. [DOI] [PubMed] [Google Scholar]
- Steinberg, S. , Shivers C. M., Liu T., Cirelli L. K., and Lense M. D.. 2021. “Survey of the Home Music Environment of Children With Various Developmental Profiles.” Journal of Applied Developmental Psychology 75: 101296. 10.1016/j.appdev.2021.101296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone, A. A. , and Shiffman S.. 2002. “Capturing Momentary, Self‐Report Data: A Proposal for Reporting Guidelines.” Annals of Behavioral Medicine 24: 236–243. 10.1207/S15324796ABM2403_09. [DOI] [PubMed] [Google Scholar]
- Stone, A. A. , Shiffman S., Atienza A. A., et al. 2007. “Historical Roots and Rationale of Ecological Momentary Assessment (EMA).” In The Science of Real‐Time Data Capture: Self‐Reports in Health Research, edited by Stone A. A., Shiffman S., and Nebeling A. A., 3–10. Oxford University Press. [Google Scholar]
- Takács, L. , Smolík F., Kaźmierczak M., and Putnam S. P.. 2020. “Early Infant Temperament Shapes the Nature of Mother‐Infant Bonding in the First Postpartum Year.” Infant Behavior and Development 58: 101428. 10.1016/j.infbeh.2020.101428. [DOI] [PubMed] [Google Scholar]
- Thornton, M. A. , and Tamir D. I.. 2020. “People Represent Mental States in Terms of Rationality, Social Impact, and Valence: Validating the 3d Mind Model.” Cortex 125: 44–59. 10.1016/j.cortex.2019.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trehub, S. E. , and Gudmundsdottir H. R.. 2019. “Mothers as Singing Mentors for Infants.” In The Oxford Handbook of Singing, edited by Welch G. F., Howard D. M., and Nix J., 454–470. Oxford University Press. 10.1093/oxfordhb/9780199660773.013.25. [DOI] [Google Scholar]
- Trehub, S. E. , and Hannon E. E.. 2006. “Infant Music Perception: Domain‐General or Domain‐Specific Mechanisms?” Cognition 100: 73–99. 10.1016/j.cognition.2005.11.006. [DOI] [PubMed] [Google Scholar]
- van den Heuvel, M. , Bülow A., Heininga V., et al. 2021. “Tracking Infant Development With a Smartphone: A Practical Guide to the Experience Sampling Method.” Frontiers in Psychology 12: 703743. 10.3389/fpsyg.2021.703743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenze, S. J. , Battle C. L., Huntley E. D., Gaugler T. L., and Kats D.. 2023. “Ecological Momentary Assessment of Postpartum Outcomes in Mothers of Multiples: Lower Maternal‐Infant Bonding, Higher Stress, and More Disrupted Sleep.” Archives of Women's Mental Health 26: 361–378. 10.1007/s00737-023-01317-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yan, R. , Jessani G., Spelke E., de Villiers P., de Villiers J., and Mehr S.. 2021. “Across Demographics and Recent History, Most Parents Sing to Their Infants and Toddlers Daily.” Philosophical Transactions of the Royal Society, B: Biological Sciences 376, no. 1840: 20210089. 10.1098/rstb.2021.0089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yurdum, L. , Singh M., Glowacki L., et al. 2023. “Universal Interpretations of Vocal Music.” Proceedings of the National Academy of Sciences 120: e2218593120. 10.1073/pnas.2218593120. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1.
Data Availability Statement
A fully reproducible manuscript; data; analysis and visualization code; and other materials are available at https://github.com/themusiclab/musical‐babies and is permanently archived at https://doi.org/10.5281/zenodo.15181606. Analyses were exploratory and not preregistered.