

Abstract
Background
Head impacts are common in contact sports such as boxing and occur at times of elevated core body and brain temperatures induced by the exercise. Following impact, elevated brain temperature may lead to the development of exacerbated brain injury that can be monitored by blood biomarkers. Blood-brain biomarkers S100B and glial fibrillary acidic protein (GFAP) reflect glial injury; neurofilament light (NFL), axonal injury; and Neuron-Specific Enolase (NSE) and Tubulin-associated unit (tau), neuronal injury. Time to peak levels post injury for these biomarkers varies. Levels of S100B l peak early post injury, while NSE, GFAP, and tau are regarded as subacute markers, and NFL shows prolonged increases. We attempt to cover a large spectrum of first week postfight alterations in blood-brain biomarkers and their response to head-neck cooling.
Objective
We hypothesized that acute head-and-neck cooling, recently shown to shorten return-to-play in concussed ice hockey players, applied acutely following a boxing bout, is associated with an attenuated concentration of blood biomarkers and improved symptom rating.
Methods
The trial is academically driven and funded by external and hospital research funds. Young, healthy elite boxers aged ≥18 years are recruited. Before, and immediately after a competitive boxing bout consisting of 2 or 3 rounds of 2 minutes each, blood samples are drawn. Boxers are randomized to intervention or control management by 1:1 allocation before baseline testing. After the initial postfight blood sample is drawn and symptom rating using the Sports Concussion Assessment Tool-5 (SCAT-5) has been collected, the boxers receive either acute selective head-and-neck cooling for 45 minutes or routine postfight management. The number of head impacts is counted in all boxers on match video recordings. In both groups, blood samples are drawn 45 minutes after the initial postbout blood sample, as well as 3 and 6 days post fight. At all blood sampling time points, the number of symptoms (NOS) and symptom severity score (SSS) are assessed using the symptom rating part of the SCAT-5. The primary endpoint is the difference in biomarker levels (GFAP, NFL, tau, UCH-L1, neuronal-specific enolase) immediately post fight and preintervention, to those obtained at 6 days post fight. The postfight SCAT-5 NOS and SSS are secondary endpoints.
Results
Recruitment started in November 2021 and is ongoing. So far, 41 boxers have been included: 20 controls and 21 cooled. Data collection started in October 2024 following the completion of blood sample analysis. We expect to recruit more boxers before the middle of 2025, but challenges with recruitment may limit this.
Conclusions
There is no treatment available for boxing-induced brain injury. Biomarkers are surrogate yet objective markers of brain injury, and the head-and-neck cooling treatment may attenuate the concentration of brain injury–related biomarkers as well as reduce symptoms induced by head impacts attained during a boxing fight.
Trial Registration
ClinicalTrials.gov NCT06386484; https://clinicaltrials.gov/study/NCT06386484
International Registered Report Identifier (IRRID)
DERR1-10.2196/68954
Keywords: sports concussion, biomarker, boxing, glial fibrillary acidic protein, neurofilament-light
Introduction
Background
Trauma to the head is common in many contact sports, including boxing [1]. If the trauma to the head, or the body with energy transmitted to the head, is sufficient to induce a range of clinical symptoms and signs that may or may not involve loss of consciousness, a sport-related concussion (SRC) has occurred [2]. In boxing, participants both receive and deliver, on average, 32-40 blows to the head during a typical bout [3]. Those blows are referred to as repetitive head impacts (RHI) [4,5]. RHI differs from the definition of SRC by the absence of the acute symptoms typically observed following an SRC. However, similar to after several SRCs cumulative effects of RHI include early-phase changes in brain function and increased risk for neurodegenerative disorders at long-term. Neuropathological consequences of RHIs in boxing have been comprehensively investigated in previous studies, illustrating structural alterations to the brain [2,6]. More specifically, RHI may lead to cognitive impairment, mood disorders, and motor control problems [7-9].
Several studies have shown that retired athletes who have sustained multiple RHI and SRCs during their career may develop chronic traumatic encephalopathy (CTE), a progressive neurodegenerative disease associated with memory loss, depression, personality changes, and dementia [1,8,10-13]. At present, CTE can only be diagnosed post mortem where key findings include irregular aggregation of phosphorylated tau protein at the depths of cortical sulci [8].
In sports, strenuous exercise leads to elevated core body and brain temperature [14], which may exacerbate the brain injury induced by head impacts. Recently, we showed that selective head-and-neck cooling for 45 minutes, aiming to rapidly normalize the elevated brain temperature, applied acutely post SRC in elite ice hockey players, resulted in earlier return-to-play and a smaller proportion of players with prolonged symptoms following the SRC [15]. However, there is a lack of objective outcome measures for assessing the effects of head-and-neck cooling in athletes.
There is a growing body of literature on the use of biomarkers of brain injury in athletes. In Olympic boxers, levels of cerebrospinal fluid biomarkers such as S100 calcium-binding protein (S100B), Tubulin-associated unit (Tau), Neurofilament light (NFL), and Glial fibrillary acid protein (GFAP) were collected at baseline, 1-6 days post fight, and 14 days after RHI attained in a boxing bout [16,17]. In addition, the biomarkers showed both acute and cumulative effects of the impacts, with a lack of normalization of NFL and GFAP after the rest period, which may indicate an ongoing injury process [16,17]. In addition, inflammatory biomarkers such as tumor necrosis factor-alpha, interleukin 6, and muscle injury biomarkers (alanine aminotransferase and aspartate aminotransferase), and creatinine increased in male elite boxers following a fight [18].
When boxing and mixed martial arts (MMA) were compared, retired boxers had higher plasma GFAP levels, and active boxers had higher plasma NFL than MMA fighters [19]. In addition, serum NFL levels were elevated both at 7-10 days post bout and after 3 months of rest in boxers compared to controls. This study also observed a significant increase in NFL at 7-10 days post bout comparing levels obtained after a high number of head impacts (more than 15 hits to the head or experienced grogginess during or after bout) to those obtained after fewer head impacts (fewer than 15 head hits) [20]. These studies indicate that selected biomarkers may remain elevated during the first postinjury week. In this randomized trial, we hypothesized that biomarkers could serve as an objective marker for the efficacy of selective head-and-neck cooling on attenuating brain injury in elite boxers, assessed by blood biomarkers immediately before and during the first 6 days after a competitive boxing fight.
Objectives
Research Hypothesis
The research hypothesis was that acute and selective head-and-neck cooling immediately after a boxing bout attenuated brain injury as evident by a reduced concentration of brain injury-related biomarker levels during the first postfight week.
Study Objectives
The primary objective was to determine whether selective head-and-neck cooling attenuates the concentration of brain injury biomarkers.
The secondary objectives were as follows:
To determine whether selective head-and-neck cooling improves symptom rating using the Sports Concussion Assessment Tool-5 (SCAT-5).
To determine whether any biomarker increase post fight, compared to baseline levels, is associated with the number of head impacts.
To determine any adverse event associated with the head-and-neck cooling.
Methods
Participants, Interventions, and Outcomes
Study Setting
The study will take place predominantly in the southern parts of Sweden due to logistical reasons, aiming for the feasibility of follow-up with biomarkers at distinct postfight time points. Blood samples will be collected at the site of the competitive boxing tournament or the local boxing clubs and transferred to the biobank at Lund University Hospital. All data will be collected in Sweden. The trial is academically driven by local funding. The trial will be conducted at Lund University, Lund, Sweden.
Trial Design
The head-and-neck Cooling of Brain temperature In BOXing (COBIBOX) trial is designed as a randomized, controlled, open, single-center superiority trial with 2 parallel groups and a primary endpoint of biomarker changes during the first 6 postfight days. Clinical secondary outcome assessments of a number of symptoms (NOS) and symptom severity score (SSS) using the symptom rating part of the SCAT-5 is performed during the initial 6 postinjury days. Randomization will be performed in blocks with 1:1 allocation.
Eligibility Criteria
Eligibility criteria are listed in Textbox 1.
Inclusion and exclusion criteria.
Inclusion criteria
Male and female elite boxers <40 years old and ≥18 years old.
Cleared for participation by the medical staff of the Swedish Boxing Association before the boxing bout.
Informed consent by each participant before the competitive event.
Exclusion criteria
>40 years old or <18 years old.
Participation in competitive fights, match-sparring, or any training causing additional head impacts during the 6-day postfight follow-up period after being included in the study.
History of autoimmune neurological diseases or a neurodegenerative disorder.
History of previous traumatic brain injury resulting in an intracranial hemorrhage.
Procedures and Measurements
All boxing clubs are thoroughly informed of the protocol before study initiation and before each tournament. Boxers between the ages of 18 and 40 years are included. At each tournament, allocation to the treatment takes place on the first morning, and the boxers are randomized 1:1 by a randomly drawn paper slip with a sign that the boxer will receive either selective head-and-neck cooling or routine postfight medical surveillance by an on-site physician. The selective head-and-neck cooling is to be initiated within 10 minutes post fight with a duration of a minimum of 45 minutes. After the boxer completes the fight (Figures 1 and 2), he or she follows the researcher to the cooling station and continues the head-and-neck cooling protocol. In some boxing events, a boxer may participate in two bouts if they win their first bout (Figure 2). The next day, during the finals, they will undergo the same protocol as on their first day, including SCAT-5 assessments and blood sample collection [21]. As mentioned in Figure 2, the start of intervention or return to play protocol starts after their last fight.
Figure 1.

Boxers that participate in direct final bouts or single-fight events will only engage in one boxing bout. SCAT-5: Sports Concussion Assessment Tool-5.
Figure 2.
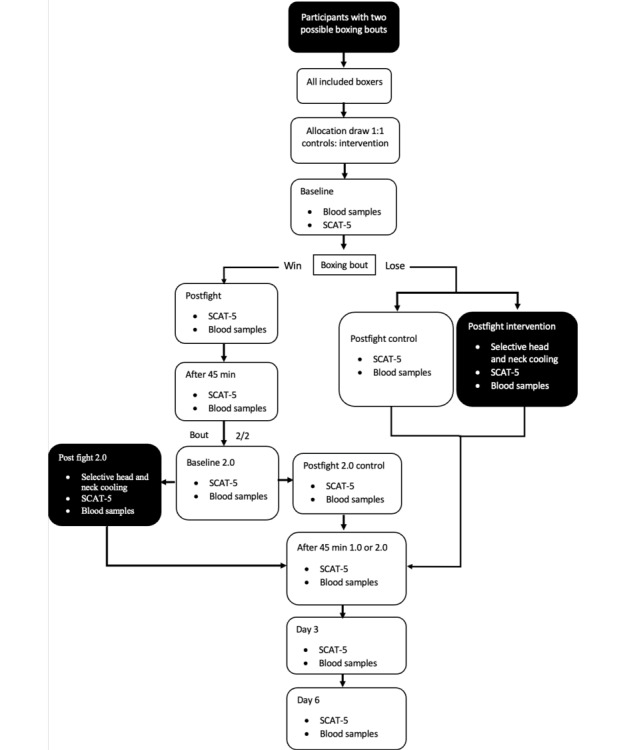
Boxers who participate in tournaments can either fight one or two boxing bouts, depends on whether they win or lose. SCAT-5: Sports Concussion Assessment Tool-5.
Participants will be randomly allocated to either the control or intervention group, involving selective head-and-neck cooling. Baseline SCAT-5 and blood samples will be collected. Subsequently, postfight SCAT-5 and blood samples will be collected for both groups. In addition, the intervention group will undergo selective head-and-neck cooling for 45 minutes. Following this, both the control and intervention groups will follow the same protocol, undergoing SCAT-5 and blood sample collection at 45 minutes post fight, as well as on day 3 and day 6 for follow-up (Figure 1).
The selective head-and-neck cooling takes place after the last boxing bout (dark-colored boxes). For a boxer who fights bout 2/2, new baseline SCAT 5 and blood samples will be collected, shown as baseline 2.0 in Figure 2.
The PolarCap System consists of a portable cooling system, designed to reduce brain temperature by controlled cooling of the scalp and neck with a circulating coolant (PolarCap Coolant, PolarCool AB). The coolant is maintained at 0 °C and flows through a silicone-based head cap. An insulating neoprene cover is put on top of the cap for isolation. The players are allowed to relax (sitting or supine) as long as the cooling head cap and neoprene cover remain in place on the head [22] Should the boxer experience discomfort and wish to discontinue the intervention, the cap is removed and the athlete is excluded from the study. All boxers follow the return-to-fight protocol. The standardized protocol is to return to physical exercise during the first 6 postfight days. During this time, the boxer may do all forms of physical exercise except sparring, match fight, or other activities resulting in impacts to the head or body (Figure 3).
Figure 3.

(A) The PolarCap unit is a powerful mobile cooling system. (B) The Polar Coolant is transported through the silicone head cap. (C) To insulate against the cold, a neoprene cover is applied on top of the cap.
Blood samples are collected at the following time points for all participants: the morning of the first boxing fight on day 1 (baseline, at rest), immediately after the fight, 45 minutes after the fight, and after 3 and 6 days in all boxers. The blood samples obtained at 3 and 6 days post fight will be drawn by a study nurse or a researcher (AaH) at the participants’ boxing club. The samples are transported to the hospital in a mobile refrigerator to maintain a temperature of 5-8 °C. Thereafter the serum samples are centrifuged at 3000 rpm, at 4 °C for 10 minutes, after which 800-1200 µL is transferred using a pipet to 2-mL tubes and stored at –80 °C.
At each time point for blood sample collection, boxers are also administered the SCAT-5 questionnaire, which is a self-report questionnaire with information on 22 different symptoms, each with a severity grading of 0-6, where 0 indicates no symptoms and 5-6 indicates severe symptoms. The maximum total score is 132. All boxing bouts are video-recorded for later analysis. The total hits per bout, strikes to the head, strikes to the body, and visible evidence of neurological disturbance (loss of consciousness, impaired balance or coordination, vacant expression, etc) will be assessed. After completion of the study, the boxers will be interviewed by phone to answer questions about their previous boxing, knock-out, and concussion history. The timeline for enrollment intervention and assessments across the study is visualized in Table 1 (SPIRIT [Standard Protocol Items: Recommendations for Interventional Trials] checklist in Multimedia Appendix 1).
Table 1.
Timeline of enrollment, intervention, and assessment during the study period.
| Procedures | Study period | Post allocation | Close-out | |||||||||
|
|
Enrollment | Preallocation | Allocation |
|
|
|||||||
| Time point | –t1 | Baseline | 0 | Post fight | 45 min post fight | Day 3 | Day 6 | 1 week post fight | ||||
| Enrollment | ✓ |
|
|
|
|
|
|
|
||||
|
|
Eligibility screen | ✓ |
|
|
|
|
|
|
|
|||
|
|
Informed consent | ✓ |
|
|
|
|
|
|
|
|||
|
|
Basic medical examination | ✓ |
|
|
|
|
|
|
|
|||
|
|
Allocation |
|
|
✓ |
|
|
|
|
|
|||
| Interventions |
|
|
|
|
|
|
|
|
||||
|
|
Selective head and neck cooling (Aa) |
|
|
|
✓ |
|
|
|
|
|||
|
|
Return to fight protocol (A+Bb) |
|
|
|
✓ | ✓ | ✓ | ✓ |
|
|||
|
|
Collecting blood sample |
|
✓ |
|
✓ | ✓ | ✓ | ✓ |
|
|||
| Assessments (SCAT-5c) |
|
|
|
|
|
|
|
|
||||
|
|
SCAT-5 |
|
✓ |
|
|
|
|
|
|
|||
|
|
SCAT-5 follow-up |
|
|
|
✓ | ✓ | ✓ | ✓ |
|
|||
|
|
Boxing history |
|
|
|
|
|
|
|
✓ | |||
aA: intervention group.
bB: control group.
cSCAT-5: Sport Concussion Assessment Tool-5.
Ethical Considerations
The study outlined in this article will be carried out in accordance with the Declaration of Helsinki. Regional ethics committee approval in Lund, Sweden (decision number Dnr 2022/06195) was obtained. Before their enrollment in the trial, all study participants will provide written informed consent. Each participant signs the form, containing comprehensive study details. Approval from the Swedish Boxing Association to include amateur and professional boxers registered in the Swedish Boxing Association (SBA) in the study will be received before the study is initiated. Forms describing the study are sent to all boxing clubs in southern Sweden that would participate in the tournaments and have enrolled boxers over 18 years old. All participants are informed of their right to terminate their participation in the study at any given time without the need to provide a reason for doing so. All questionnaires and data collection methods were reviewed and approved by the Swedish Ethical Review Authority in Uppsala, Sweden. The submitted protocol to the Swedish Ethical Review Authority included detailed information on the intervention, data confidentiality, blood collection, blood sample storage, and measures to ensure the protection of participants’ privacy. A study protocol was provided with the ethical application. All participants' data are anonymized from the time of inclusion, before allocation, by assigning a code containing letters and numbers. This code will be attached to the participants’ blood samples and SCAT-5 score files. Each participant will receive a compensation of 1000 SEK (US $104.53) for their time, inconvenience, and any potential discomfort associated with participation. The consent information emphasizes the voluntary nature of participation, including the possibility of opting out at any stage. It also specifies who will obtain informed consent from the participants. Specific contact information for the research team is provided to participants for any questions or concerns. The informed consent consists of 10 detailed points. It begins with a request for participation that describes what the boxers will be involved in. The background and aim section explains the purpose of the study and the facts supporting it. The study procedure outlines the collection of SCAT-5 questionnaires, blood samples, and the possibility of cooling. Biomarker collection is covered by the biobank policies and includes the category of biomarkers that will be analyzed. The risk section highlights any potential risks associated with participation. Handling personal data explains data protection measures in accordance with GDPR, while data management and privacy further detail how data are stored and covered under GDPR. The insurance section clarifies the responsible parts that ensure the participants during the study. Voluntary participation ensures that participants are informed of their right to opt out at any time, even after inclusion. Finally, the responsible staff section provides information about the staff in charge and their contact details.
Study Population
A total of 14 boxing clubs whose fighters enrolled in 5-7 boxing events in southern Sweden will be contacted and informed about the study and its inclusion criteria.
Allocation
After all boxers have approved participation in the study during the tournament, and signed the informed consent, the study staff makes an allocation on paper slips that equals the number of participants. Then the boxers randomly, by drawing a paper slip, receive either a sign for receiving head-and-neck cooling (C=cooling) or NC (no cooling; Figures 1-2). All allocations are finalized a minimum of 3 hours before the start of the tournaments.
The enrollment of participants will be done by a researcher (AaH) aided by boxing coaches.
After the boxing bout, and after the boxer is evaluated for red flags mandating transport to the nearest hospital, the boxer is brought to the intervention station to apply the PolarCap system as previously described.
Personnel Responsible for Informed Consent
Informed consent documents will be sent for approval to the Swedish Boxing Association, after which those will be distributed to each club. A responsible researcher and physician (AaH) will inform the participants verbally and in written form, either days before the competition or on the same day. Each participant will be informed about the study, informed of the possibility to withdraw from participation at any time, and provided time to ask questions. Before randomization, each participant signs the informed consent form.
Biomarker Analysis
Venous blood is collected in 3.5 mL serum and EDTA plasma tubes generated at room temperature and stored in a mobile refrigerator at 4-8 ºC until centrifuged at 4 ºC for 10 minutes at 3000 rpm. The remaining supernatant is transferred to 2 mL cryotubes and stored at –80 oC until analyzed. Once the study has been completed, blood biomarkers for brain injury (S100B, GFAP, tau forms, NFL, and NSE) will be measured in coded samples using an established single-molecule array (for GFAP, tau, and NFL) by Quanterix and electrochemiluminescence immunoassays (for S100B and NSE) by Roche Diagnostics immunoassays [23] in the Clinical Neurochemistry Laboratory by board-certified laboratory technicians who will be blinded to the intervention.
Data Collection
The SCAT-5 form will be filled out at the time of biomarker analysis and used as a secondary endpoint of the study. The boxing bouts take place either in events consisting of single bouts for each boxer or in tournaments where 2 bouts are possible (semifinal and final). For boxers participating in two bouts at the same event, the baseline, postfight, and 45-minute postfight scores and biomarker tests will be retaken. Values related to the second fight will be considered in the analysis. The analysis of symptom severity scores obtained by SCAT-5 at the set timeline will facilitate the interpretation of outcomes between the boxers independent of their previous boxing history after the completed 6-day follow-up. Boxing history will be obtained by phone call interview at the 6-day follow-up or on-site. The follow-up for days 3 and 6 will be organized by the local clubs before the first postmatch training session, or at the study hospital.
Sample Size and Statistical Power
Based on previous reports, an approximately 10% increase in key biomarkers is observed after a concussion in athletes [16]. We hypothesized a 20% reduction of biomarker level by acute head-and-neck cooling. We assumed equal variance of the cooled and control groups. The selected power was set to 0.8. Power analysis was conducted using the following formula:
 |
[24]
Based on the power calculations, a total number of 20 participants per group is expected to yield sufficient statistical power. Since dropouts and missed sample times can be anticipated we aim for group sizes of 25 per group.
Recruitment
Participants are recruited by one researcher (AaH) by sending information about the study to the Swedish Boxing Association which approves participation, in written form or verbally. Thereafter the study must be approved by the organizers of the boxing tournament. Finally, the recruitment of boxers who fulfill the inclusion criteria and sign the written consent form after verbal and written information about the study is provided.
Adverse Events
Any adverse events reported by the participant during the study period are noted and reported. Specifically, any deviation from the protocol (eg, sample time point, duration of head-and-neck cooling) will be noted. Symptoms, such as headache, nausea, and dizziness, are reported to the medical doctor and study researcher (AaH), although these symptoms may also be caused by the SRC per se [15]. No adverse events are expected, based on our previous study where 61 elite ice hockey players were cooled without any reported adverse events [15].
Results
The study flow is presented in Figures 1 and 2. The study began in November 2021 and is expected to be completed before the summer of 2025 (Figure 4). Based on our sample size calculations, we aim to recruit approximately 40-50 participants. The first results are anticipated to be submitted for publication in the Autumn of 2025. This study evaluates the effectiveness of selective head and neck cooling in reducing blood-brain biomarkers and SCAT-5 scores during the first week after a boxing bout. Recruitment started on November 4, 2021. Approximate completion of final recruitment is expected in the first weeks of January 2025 (protocol version 1.0, 2024-04-01).
Figure 4.

All allocation and randomization occur after signed informed consent and before baseline testing.
The 3 excluded boxers, whose opponents dropped out, went through baseline SCAT-5 testing and blood sample collection. The participant who experienced nausea and vomiting chose to withdraw from participation in the study after his boxing bout before any further testing (Figure 4).
Discussion
Principal Findings
During a boxing fight, boxers typically attain a high number of blows to the head, which may lead to brain injuries. Due to the strenuous activity, these blows occur at a time of elevated core body temperature, which may exacerbate the brain injury. There are no approved treatments for boxing-induced brain injuries. A blow to the head may lead to an elevation of blood biomarker concentrations that reflect the degree of the brain injury caused by the impact. There is an increasing interest in these biomarkers that include markers for large caliber axon injury (NFL), neuronal injury (NSE, tau), and glial injury (S100B, GFAP). Our present study may show whether the level of biomarkers is related to the number of hits or concussions received, the symptom development after the fight, and most importantly the effects of the cooling intervention.
Head-and-neck cooling was shown to decrease brain temperature measured by magnetic resonance imaging (MRI) [25], and improved cognitive outcome when applied acutely post concussion [26]. In a recent clinical trial including 132 concussed ice hockey players, a shorter recovery time was observed after acute selective head-and-neck cooling for at least 45 minutes [15]. A shorter recovery was also observed when cooling was initiated up to 8 days post concussion [27]. To provide an objective outcome measure for the cooling intervention in the present study, the primary outcome is blood biomarker levels, of which GFAP, NFL, S100B, and tau may be the most important. The chosen time points for collecting blood-brain biomarkers aim to assess the early-phase biomarker response to boxing matches, with subsequent evaluation of the head and neck cooling effect and its potential early impact. S100B is associated with an acute astrocytic response, which typically peaks within hours, followed by GFAP with a peak of 24 hours [28]. This makes postfight day 3 a valuable time point to capture a delayed peak or sustained elevation of the selected biomarkers. While NFL levels may remain elevated at longer time points post fight, we had to use 6 days as our latest evaluation time point. This is based on the guidelines of the Swedish Boxing Association, which prohibit boxers from competing or having fights within 6 days of their most recent tournament. Thus, many boxers are assigned to match sparring or other tournaments after 6 days.
The selection of biomarkers in the present trial is based on several previous studies [29,30], mainly in traumatic brain injury and neurodegenerative disorders [19]. Currently, both tau isoforms and GFAP are used in the prediction and diagnosis of neurodegenerative diseases, particularly Alzheimer disease, and S100B in mild traumatic brain injury guidelines [31-33].
In numerous reports on mild, moderate, or severe traumatic brain injury, blood and CSF biomarkers have been used at different time points postinjury [29]. Following boxing bouts, tau, NFL, GFAP, and S100B are all increased in the early phase after boxing. Of these, NFL, GAP, and tau are increased several weeks to months post fight [16,17,34].
In addition, strenuous exercise has been reported to increase biomarkers such as S100B [35,36]), while leading to a reduction in GFAP and no alteration in NF-L levels [37]. When comparing strenuous exercise to contact sports such as boxing, boxers showed a significant increase in biomarker levels, particularly in GFAP and NFL [17].
Blood S100B levels were significantly elevated in both competitive boxers and high-level exercised athletes such as runners [16,38]. These findings argue that boxing causes the elevation of concentration of several biomarkers reflecting the brain injury, and is associated with lead to long-term neurological consequences.
The role of brain temperature in acute brain injury has been evaluated in numerous trials. In particular, elevated brain temperature may negatively impact functional and neurological outcomes following traumatic brain injury [39,40]. While systemic hypothermia has not been associated with improved outcomes in severe traumatic brain injury, we hypothesized that controlling body temperature may be an important factor in the recovery of boxing-induced brain injury. The primary aim of head-and-neck cooling is not to provide cerebral hypothermia, it is to attenuate exercise-induced hyperthermia and to rapidly normalize the elevated brain temperature.
During exercise, elevated temperature is associated with a higher demand for oxygen and energy metabolism in the brain [41,42], resulting in exacerbation of the injury mechanism initiated by head impacts during boxing. We hypothesize that brain cooling can rapidly normalize brain temperature, thereby reducing metabolic demand resulting in attenuated secondary injury and leading to beneficial effects for the recovery phase after a fight.
Should this explorative study provide evidence of the beneficial effects of head-neck cooling, a multicenter study (preferably with later postfight time points) is warranted.
Strengths and Limitations
The present study has the potential to objectively evaluate the effect of head-and-neck cooling on blood biomarker levels. Moreover, it can provide unique results on biomarker concentration changes following repeated head impacts at several time points post fight.
Outliers in biomarker concentrations are expected, although since each boxer will be his or her control, percentage changes from baseline can be calculated. A 20% reduction of biomarker concentrations is reasonable based on the rapid application of head-and-neck cooling. The potential placebo effect of cooling on symptom ratings is also taken into consideration by using objective biomarker concentrations, highlighting the necessity of biomarker assessment to evaluate cooling’s physiological impact.
Conclusion
This study is structured to evaluate early-phase objective and subjective changes in boxers during the first week post fight, and to study the effects of head-and-neck cooling on these changes. In conclusion, the present trial may provide objective biomarker evidence for the role of attenuating cerebral hyperthermia by selective head-and-neck cooling acutely following a boxing bout.
Acknowledgments
The results of this trial will be presented in an appropriate scientific journal after the trial is completed. Open-access funding is provided by Lund University. Swedish Research Council for Sport Science, Hans-Gabriel and Alice Trolle-Wachtmeister (HGATW) Foundation for Medical Research, the Alborada Trust, Swedish Brain Foundation, and hospital ALF funds (all to NM). HZ is a Wallenberg Scholar and a Distinguished Professor at the Swedish Research Council supported by grants from the Swedish Research Council (#2023-00356; #2022-01018 and #2019-02397), the European Union’s Horizon Europe research and innovation program under grant agreement number 101053962, and Swedish State Support for Clinical Research (#ALFGBG-71320). The authors wish to thank Marit Bäckström for administrative assistance.
Abbreviations
- COBIBOX
Cooling of Brain temperature In BOXing
- CTE
chronic traumatic encephalopathy
- GFAP
glial fibrillary acid protein
- MRI
magnetic resonance imaging
- MMA
mixed martial arts
- NSE
neuron specific enolase
- NFL
Neurofilament light
- NOS
number of symptoms
- RHI
repetitive head impacts
- S100B
S100 calcium-binding protein
- SCAT-5
Sports Concussion Assessment Tool-5
- SRC
sport-related concussion
- SBA
Swedish Boxing Association
- SPIRIT
Standard Protocol Items: Recommendations for Interventional Trials
- SSS
symptom severity score
- Tau
tubulin-associated unit
SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) checklist COBIBOX.
Data Availability
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions: NM contributed to funding acquisition. AaH, YT, and NM assisted with conceptualization. AaH handled formal analysis. AaH, HZ, and KB contributed to investigation. NM, AaH, YT, HZ, and KB assisted with methodology. AaH handled project administration. NM handled supervision. AaH and NM contributed to validation. AaH and NM assisted with visualization and writing original draft. AaH, YT, HZ, KB, and NM contributed to writing–review and editing.
Conflicts of Interest: YT is a scientific advisor for PolarCool Inc. Lund, Sweden. NM previously was a scientific advisor for PolarCool Inc. Lund, Sweden. Polar Cool provides the cooling helmet, although has not influenced the design of the study protocol. HZ has served at scientific advisory boards and as a consultant for Abbvie, Acumen, Alector, Alzinova, ALZPath, Amylyx, Annexon, Apellis, Artery Therapeutics, AZTherapies, Cognito Therapeutics, CogRx, Denali, Eisai, Merry Life, Nervgen, Novo Nordisk, Optoceutics, Passage Bio, Pinteon Therapeutics, Prothena, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Alzecure, Biogen, Cellectricon, Fujirebio, Lilly, Novo Nordisk, and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). KB has served as a consultant, on advisory boards, or data monitoring committees for Abcam, Axon, Biogen, and JOMDD/Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Prothena, Roche Diagnostics, and Siemens Healthineers, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. IR has served on advisory boards and given talks sponsored by Biogen, Bayer, Merck, Roche, GlaxoSmithKline, TEVA, Sanofi, and UCB.
References
- 1.Bernick C, Banks S, Phillips M, Lowe M, Shin W, Obuchowski N, Jones S, Modic M. Professional fighters brain health study: rationale and methods. Am J Epidemiol. 2013 Jul 15;178(2):280–6. doi: 10.1093/aje/kws456.kws456 [DOI] [PubMed] [Google Scholar]
- 2.Patricios JS, Schneider KJ, Dvorak J, Ahmed OH, Blauwet C, Cantu RC, Davis GA, Echemendia RJ, Makdissi M, McNamee M, Broglio S, Emery CA, Feddermann-Demont N, Fuller GW, Giza CC, Guskiewicz KM, Hainline B, Iverson GL, Kutcher JS, Leddy JJ, Maddocks D, Manley G, McCrea M, Purcell LK, Putukian M, Sato H, Tuominen MP, Turner M, Yeates KO, Herring SA, Meeuwisse W. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. Br J Sports Med. 2023 Jun;57(11):695–711. doi: 10.1136/bjsports-2023-106898.57/11/695 [DOI] [PubMed] [Google Scholar]
- 3.Davis P, Benson PR, Pitty JD, Connorton AJ, Waldock R. The activity profile of elite male amateur boxing. Int J Sports Physiol Perform. 2015 Jan;10(1):53–7. doi: 10.1123/ijspp.2013-0474.2013-0474 [DOI] [PubMed] [Google Scholar]
- 4.Erlanger DM. Exposure to sub-concussive head injury in boxing and other sports. Brain Inj. 2015;29(2):171–4. doi: 10.3109/02699052.2014.965211. [DOI] [PubMed] [Google Scholar]
- 5.Goldfinger MH, Ling H, Tilley BS, Liu AKL, Davey K, Holton JL, Revesz T, Gentleman SM. The aftermath of boxing revisited: identifying chronic traumatic encephalopathy pathology in the original Corsellis boxer series. Acta Neuropathol. 2018 Dec;136(6):973–974. doi: 10.1007/s00401-018-1926-8. https://europepmc.org/abstract/MED/30377771 .10.1007/s00401-018-1926-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McKee AC, Daneshvar DH, Alvarez VE, Stein TD. The neuropathology of sport. Acta Neuropathol. 2014 Jan;127(1):29–51. doi: 10.1007/s00401-013-1230-6. https://europepmc.org/abstract/MED/24366527 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mackay DF, Russell ER, Stewart K, MacLean JA, Pell JP, Stewart W. Neurodegenerative Disease Mortality among Former Professional Soccer Players. N Engl J Med. 2019 Nov 07;381(19):1801–1808. doi: 10.1056/NEJMoa1908483. https://europepmc.org/abstract/MED/31633894 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McKee AC, Stein TD, Huber BR, Crary JF, Bieniek K, Dickson D, Alvarez VE, Cherry JD, Farrell K, Butler M, Uretsky M, Abdolmohammadi B, Alosco ML, Tripodis Y, Mez J, Daneshvar DH. Chronic traumatic encephalopathy (CTE): criteria for neuropathological diagnosis and relationship to repetitive head impacts. Acta Neuropathol. 2023 Apr;145(4):371–394. doi: 10.1007/s00401-023-02540-w. https://europepmc.org/abstract/MED/36759368 .10.1007/s00401-023-02540-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lember LM, Ntikas M, Mondello S, Wilson L, Di Virgilio TG, Hunter AM, Kobeissy F, Mechref Y, Donaldson DI, Ietswaart M. The Use of Biofluid Markers to Evaluate the Consequences of Sport-Related Subconcussive Head Impact Exposure: A Scoping Review. Sports Med Open. 2024 Jan 25;10(1):12. doi: 10.1186/s40798-023-00665-6. https://europepmc.org/abstract/MED/38270708 .10.1186/s40798-023-00665-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Di Virgilio TG, Ietswaart M, Wilson L, Donaldson DI, Hunter AM. Understanding the Consequences of Repetitive Subconcussive Head Impacts in Sport: Brain Changes and Dampened Motor Control Are Seen After Boxing Practice. Front Hum Neurosci. 2019;13:294. doi: 10.3389/fnhum.2019.00294. https://europepmc.org/abstract/MED/31551732 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ling H, Morris HR, Neal JW, Lees AJ, Hardy J, Holton JL, Revesz T, Williams DDR. Mixed pathologies including chronic traumatic encephalopathy account for dementia in retired association football (soccer) players. Acta Neuropathol. 2017 Mar;133(3):337–352. doi: 10.1007/s00401-017-1680-3. https://europepmc.org/abstract/MED/28205009 .10.1007/s00401-017-1680-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Batty GD, Frank P, Kujala UM, Sarna SJ, Valencia-Hernández Carlos A, Kaprio J. Dementia in former amateur and professional contact sports participants: population-based cohort study, systematic review, and meta-analysis. EClinicalMedicine. 2023 Jul;61:102056. doi: 10.1016/j.eclinm.2023.102056. https://linkinghub.elsevier.com/retrieve/pii/S2589-5370(23)00233-X .S2589-5370(23)00233-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alosco ML, Mariani ML, Adler CH, Balcer LJ, Bernick C, Au R, Banks SJ, Barr WB, Bouix S, Cantu RC, Coleman MJ, Dodick DW, Farrer LA, Geda YE, Katz DI, Koerte IK, Kowall NW, Lin AP, Marcus DS, Marek KL, McClean MD, McKee AC, Mez J, Palmisano JN, Peskind ER, Tripodis Y, Turner RW, Wethe JV, Cummings JL, Reiman EM, Shenton ME, Stern RA, DIAGNOSE CTE Research Project Investigators Developing methods to detect and diagnose chronic traumatic encephalopathy during life: rationale, design, and methodology for the DIAGNOSE CTE research project. Alzheimers Res Ther. 2021;13(1):136. doi: 10.1186/s13195-021-00872-x. https://alzres.biomedcentral.com/articles/10.1186/s13195-021-00872-x .10.1186/s13195-021-00872-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Racinais S, Cocking S, Périard Julien D. Sports and environmental temperature: From warming-up to heating-up. Temperature (Austin) 2017;4(3):227–257. doi: 10.1080/23328940.2017.1356427. https://europepmc.org/abstract/MED/28944269 .1356427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Al-Husseini A, Fazel Bakhsheshi M, Gard A, Tegner Y, Marklund N. Shorter Recovery Time in Concussed Elite Ice Hockey Players by Early Head-and-Neck Cooling: A Clinical Trial. J Neurotrauma. 2023 Jun;40(11-12):1075–1085. doi: 10.1089/neu.2022.0248. [DOI] [PubMed] [Google Scholar]
- 16.Neselius S, Zetterberg H, Blennow K, Marcusson J, Brisby H. Increased CSF levels of phosphorylated neurofilament heavy protein following bout in amateur boxers. PLoS One. 2013;8(11):e81249. doi: 10.1371/journal.pone.0081249. https://dx.plos.org/10.1371/journal.pone.0081249 .PONE-D-13-28774 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Neselius S, Brisby H, Theodorsson A, Blennow K, Zetterberg H, Marcusson J. CSF-biomarkers in Olympic boxing: diagnosis and effects of repetitive head trauma. PLoS One. 2012;7(4):e33606. doi: 10.1371/journal.pone.0033606. https://dx.plos.org/10.1371/journal.pone.0033606 .PONE-D-11-24988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kılıc Y, Cetin HN, Sumlu E, Pektas MB, Koca HB, Akar F. Effects of Boxing Matches on Metabolic, Hormonal, and Inflammatory Parameters in Male Elite Boxers. Medicina (Kaunas) 2019 Jun 18;55(6):288. doi: 10.3390/medicina55060288. https://www.mdpi.com/resolver?pii=medicina55060288 .medicina55060288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bernick C, Shan G, Ritter A, Ashton NJ, Blennow K, Lantero-Rodriguez J, Snellman A, Zetterberg H. Blood biomarkers and neurodegeneration in individuals exposed to repetitive head impacts. Alzheimers Res Ther. 2023 Oct 12;15(1):173. doi: 10.1186/s13195-023-01310-w. https://alzres.biomedcentral.com/articles/10.1186/s13195-023-01310-w .10.1186/s13195-023-01310-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shahim P, Zetterberg H, Tegner Y, Blennow K. Serum neurofilament light as a biomarker for mild traumatic brain injury in contact sports. Neurology. 2017 May 09;88(19):1788–1794. doi: 10.1212/WNL.0000000000003912. https://europepmc.org/abstract/MED/28404801 .WNL.0000000000003912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Echemendia RJ, Meeuwisse W, McCrory P, Davis GA, Putukian M, Leddy J, Makdissi M, Sullivan SJ, Broglio SP, Raftery M, Schneider K, Kissick J, McCrea M, Dvořák Jiří, Sills AK, Aubry M, Engebretsen L, Loosemore M, Fuller G, Kutcher J, Ellenbogen R, Guskiewicz K, Patricios J, Herring S. The Sport Concussion Assessment Tool 5th Edition (SCAT5): Background and rationale. Br J Sports Med. 2017 Jun;51(11):848–850. doi: 10.1136/bjsports-2017-097506.bjsports-2017-097506 [DOI] [PubMed] [Google Scholar]
- 22.Gard A, Tegner Y, Bakhsheshi MF, Marklund N. Selective head-neck cooling after concussion shortens return-to-play in ice hockey players. Concussion. 2021 Apr 15;6(2):CNC90. doi: 10.2217/cnc-2021-0002. https://europepmc.org/abstract/MED/34084556 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Posti JP, Riikka SKT, Lagerstedt L, Dickens AM, Hossain I, Mohammadian M, Ala-Seppälä H, Frantzén J, van Gils M, Hutchinson PJ, Katila AJ, Maanpää H-R, Menon DK, Newcombe VF, Tallus J, Hrusovsky K, Wilson DH, Gill J, Sanchez J-C, Tenovuo O, Zetterberg H, Blennow K. Correlation of Blood Biomarkers and Biomarker Panels with Traumatic Findings on Computed Tomography after Traumatic Brain Injury. Journal of Neurotrauma. 2019 Jan 01;36(14):2178–2189. doi: 10.1089/neu.2018.6254. https://www.liebertpub.com/doi/10.1089/neu.2018.6254 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Serdar CC, Cihan M, Yücel Doğan, Serdar MA. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem Med (Zagreb) 2021 Feb 15;31(1):010502. doi: 10.11613/BM.2021.010502. https://europepmc.org/abstract/MED/33380887 .bm-31-1-010502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Walter A, Finelli K, Bai X, Johnson B, Neuberger T, Seidenberg P, Bream T, Hallett M, Slobounov S. Neurobiological effect of selective brain cooling after concussive injury. Brain Imaging Behav. 2018 Jun;12(3):891–900. doi: 10.1007/s11682-017-9755-2.10.1007/s11682-017-9755-2 [DOI] [PubMed] [Google Scholar]
- 26.Smith MA, McNinch NL, Chaney D, Shauver L, Murray T, Kline P, Lesak A, Franco-MacKendrick L, Scott L, Logan K, Ichesco IK, Liebig C, Congeni J. Reduced concussion symptom burden in early adolescent athletes using a head-neck cooling device. Clin J Sport Med. 2024;34(3):247–255. doi: 10.1097/JSM.0000000000001198. https://europepmc.org/abstract/MED/38180057 .00042752-990000000-00172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Congeni J, Murray T, Kline P, Bouhenni R, Morgan D, Liebig C, Lesak A, McNinch NL. Preliminary Safety and Efficacy of Head and Neck Cooling Therapy After Concussion in Adolescent Athletes: A Randomized Pilot Trial. Clin J Sport Med. 2022 Jul 01;32(4):341–347. doi: 10.1097/JSM.0000000000000916. https://europepmc.org/abstract/MED/34009790 .00042752-202207000-00002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.O'Brien WT, Spitz G, Xie B, Major BP, Mutimer S, Giesler LP, Bain J, Evans LJ, Duarte Martins B, Piantella S, Alhassan A, Brady S, Cappellari D, Somma V, McColl T, Symons GF, Gore T, Sun M, Kuek T, Horan S, Bei M, Ponsford JL, Willmott C, Reyes J, Ashton NJ, Zetterberg H, Mitra B, O'Brien TJ, Shultz SR, McDonald SJ. Biomarkers of Neurobiologic Recovery in Adults With Sport-Related Concussion. JAMA Netw Open. 2024 Jun 03;7(6):e2415983. doi: 10.1001/jamanetworkopen.2024.15983. https://europepmc.org/abstract/MED/38848061 .2819700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hossain I, Marklund N, Czeiter E, Hutchinson P, Buki A. Blood biomarkers for traumatic brain injury: A narrative review of current evidence. Brain Spine. 2024;4:102735. doi: 10.1016/j.bas.2023.102735. https://linkinghub.elsevier.com/retrieve/pii/S2772-5294(23)01023-8 .S2772-5294(23)01023-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Meier TB, Huber DL, Bohorquez-Montoya L, Nitta ME, Savitz J, Teague TK, Bazarian JJ, Hayes RL, Nelson LD, McCrea MA. A Prospective Study of Acute Blood-Based Biomarkers for Sport-Related Concussion. Ann Neurol. 2020 Jun;87(6):907–920. doi: 10.1002/ana.25725. https://europepmc.org/abstract/MED/32215965 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mattsson N, Zetterberg H, Janelidze S, Insel PS, Andreasson U, Stomrud E, Palmqvist S, Baker D, Tan Hehir CA, Jeromin A, Hanlon D, Song L, Shaw LM, Trojanowski JQ, Weiner MW, Hansson O, Blennow K, ADNI Investigators Plasma tau in Alzheimer disease. Neurology. 2016 Oct 25;87(17):1827–1835. doi: 10.1212/WNL.0000000000003246. https://europepmc.org/abstract/MED/27694257 .WNL.0000000000003246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gill J, Latour L, Diaz-Arrastia R, Motamedi V, Turtzo C, Shahim P, Mondello S, DeVoto C, Veras E, Hanlon D, Song L, Jeromin A. Glial fibrillary acidic protein elevations relate to neuroimaging abnormalities after mild TBI. Neurology. 2018 Oct 09;91(15):e1385–e1389. doi: 10.1212/WNL.0000000000006321. https://europepmc.org/abstract/MED/30209234 .WNL.0000000000006321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Biberthaler P, Linsenmeier U, Pfeifer KJ, Kroetz M, Mussack T, Kanz KG, Hoecherl EFJ, Jonas F, Marzi I, Leucht P, Jochum M, Mutschler W. Serum S-100B concentration provides additional information fot the indication of computed tomography in patients after minor head injury: a prospective multicenter study. Shock. 2006 May;25(5):446–53. doi: 10.1097/01.shk.0000209534.61058.35.00024382-200605000-00004 [DOI] [PubMed] [Google Scholar]
- 34.Zetterberg H, Hietala MA, Jonsson M, Andreasen N, Styrud E, Karlsson I, Edman A, Popa C, Rasulzada A, Wahlund L, Mehta PD, Rosengren L, Blennow K, Wallin A. Neurochemical aftermath of amateur boxing. Arch Neurol. 2006 Sep;63(9):1277–80. doi: 10.1001/archneur.63.9.1277.63/9/1277 [DOI] [PubMed] [Google Scholar]
- 35.Oris C, Kahouadji S, Durif J, Bouvier D, Sapin V. S100B, Actor and Biomarker of Mild Traumatic Brain Injury. Int J Mol Sci. 2023 Apr 01;24(7):6602. doi: 10.3390/ijms24076602. https://www.mdpi.com/resolver?pii=ijms24076602 .ijms24076602 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Morris JK, Kueck PJ, Kemna RE, Green ZD, John CS, Winter M, Billinger SA, Vidoni ED. Biomarker Responses to Acute Exercise and Relationship with Brain Blood Flow. J Alzheimers Dis. 2024;97(1):283–292. doi: 10.3233/JAD-230766.JAD230766 [DOI] [PubMed] [Google Scholar]
- 37.Bazarian JJ, Abar B, Merchant-Borna K, Pham DL, Rozen E, Mannix R, Kawata K, Chou Y, Stephen S, Gill JM. Effects of Physical Exertion on Early Changes in Blood-Based Brain Biomarkers: Implications for the Acute Point of Care Diagnosis of Concussion. J Neurotrauma. 2023 Apr;40(7-8):693–705. doi: 10.1089/neu.2022.0267. https://europepmc.org/abstract/MED/36200628 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Otto M, Holthusen S, Bahn E, Söhnchen N, Wiltfang J, Geese R, Fischer A, Reimers CD. Boxing and running lead to a rise in serum levels of S-100B protein. Int J Sports Med. 2000 Nov;21(8):551–5. doi: 10.1055/s-2000-8480. [DOI] [PubMed] [Google Scholar]
- 39.Hinson HE, Rowell S, Morris C, Lin AL, Schreiber MA. Early fever after trauma: Does it matter? J Trauma Acute Care Surg. 2018 Jan;84(1):19–24. doi: 10.1097/TA.0000000000001627. https://europepmc.org/abstract/MED/28640776 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pegoli M, Zurlo Z, Bilotta F. Temperature management in acute brain injury: A systematic review of clinical evidence. Clin Neurol Neurosurg. 2020 Oct;197:106165. doi: 10.1016/j.clineuro.2020.106165.S0303-8467(20)30508-4 [DOI] [PubMed] [Google Scholar]
- 41.Rasmussen P, Nybo L, Volianitis S, Møller K, Secher NH, Gjedde A. Cerebral oxygenation is reduced during hyperthermic exercise in humans. Acta Physiol (Oxf) 2010 May;199(1):63–70. doi: 10.1111/j.1748-1716.2010.02084.x.APS2084 [DOI] [PubMed] [Google Scholar]
- 42.Wang H, Wang B, Jackson K, Miller CM, Hasadsri L, Llano D, Rubin R, Zimmerman J, Johnson C, Sutton B. A novel head-neck cooling device for concussion injury in contact sports. Transl Neurosci. 2015;6(1):20–31. doi: 10.1515/tnsci-2015-0004. https://europepmc.org/abstract/MED/28123788 .tnsci-2015-0004 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) checklist COBIBOX.
Data Availability Statement
The datasets generated or analyzed during this study are available from the corresponding author on reasonable request.