

Abstract
The capacity of government agencies to develop effective policy responses to external shocks is an important area of focus for health policy processes, as illustrated by the coronavirus (COVID-19) pandemic. However, few empirical studies exploring the subnational capacity of governments and the influence of institutional, organizational and political factors in shaping the policy response to complex emergencies have been conducted. The purpose of this study is to examine the governance capacity to develop and implement a policy response to a major health emergency—COVID-19—in Tamil Nadu, India, and to understand the factors shaping governance capacity during the first and second waves (2020–21). Tamil Nadu offers a useful case for exploring governance capacity due to its long-standing public health institutions and previous experiences with disaster and outbreak response. We utilized three sources of data: (1) a review of key policy documents (n = 164); (2) a review of English-language media articles in the Indian press (n = 336); and (3) in-depth interviews with senior decision makers, technical experts and other stakeholders (n = 10). We present four key findings from this analysis. Firstly, Tamil Nadu’s institutional framework enabled state-level governance capacity during an emergency of massive complexity, allowing for flexibility and nimbleness to adapt to evolving dynamics of centralization and decentralization over the course of the pandemic. Secondly, the ability to integrate public health expertise was circumscribed at important phases. Thirdly, while coordination with external experts was utilized extensively, engagement with civil society groups was perceived as limited. Fourthly, the electoral cycle was perceived by some to have constrained governance capacity at a critical point in the pandemic. By analysing the dynamics of state-level capacity in Tamil Nadu during a complex emergency, this study provides important learnings for other contexts globally regarding the drivers shaping capacity to develop and implement policy responses to crises.
Keywords: Governance, capacity, policy, Tamil Nadu, crisis, COVID-19
Key messages.
Research on governance capacity in developing and managing the policy response to crises in the health sector is an important dimension of emergency management and health systems strengthening.
In Tamil Nadu, India, institutional frameworks for managing health emergencies enabled governance capacity, allowing for organizational flexibility that surfaced capacity through specialization, coordination and levels of centralization.
Organizational flexibility facilitated innovations that provided a boost to governance legitimacy, such as the formation of the War Room and the formation of various expert committees.
Political context was found to strongly shape governance capacity, with all forms of governance capacity influenced by the electoral cycle in Tamil Nadu.
Introduction
The coronavirus (COVID-19) pandemic presented national, state and local governments with the most complex set of public policy challenges in recent memory. In India, the health impacts of the pandemic have been extensive. Beyond the vast direct and indirect health impacts across the country, particularly during the second wave of COVID-19 from April to June 2021, there have been major societal and economic disruptions across different phases of the pandemic. The pandemic presented an array of governance and decision-making challenges across sectors and over multiple waves, which are made even more complex by India’s federal structure and the fact that the 28 states within the federal system have primary responsibility for health service delivery (Selvaraj et al., 2022). In this paper, we explore a crucial aspect of policy processes at the subnational level—capacity in developing and managing the policy response to crises in the health sector.
Defined as the ability to “function as a resilient, strategic, and autonomous entity”, capacity is a key determinant of health system performance (Kaplan, 1999). A growing body of empirical qualitative research focused on low- and middle-income countries has examined the complex interplay of individual, organizational and systemic factors in shaping processual aspects of state capacity and its outcomes in the context of routine health system functions (Mirzoev et al., 2015). The capacity of government agencies to perform their core functions and manage relationships while responding to external shocks has been a growing focus of public administration and public health scholarship (Christensen et al., 2016) and has increasingly been investigated in the health sector in the wake of myriad crises in the health sector, such as communicable disease outbreaks (Christensen and Lægreid, 2020; Christensen and Ma, 2021), climate-induced disasters (De Goyet, 2007) and conflicts (Douedari and Howard, 2019). Understanding the capacity of governments to develop a cohesive and coherent strategy, mobilize and coordinate actors within and outside of government and implement actions and decisions during crisis has been crucial to investigating multi-sectoral policy responses from the earliest days of the pandemic (Capano et al., 2020; Greer et al., 2020). An emerging body of work drawing on a diverse range of public policy and broader social science theory has illuminated antecedents to strengthened capacity to manage crises, such as experience with prior outbreaks (Woo, 2020; Sundararaman and Gaitonde, 2021), collaboration between national and subnational jurisdictions (Greer et al., 2022), the influence of politics (Cameron et al., 2023) and goal alignment between elected officials and bureaucrats (Askim and Christensen, 2022).
Tamil Nadu, a state in Southern India, provides a useful example for understanding subnational policy response and capacity to address crises in the health sector. The state is known to have a long public health history and strong capacity in public health and social sectors (Gupta et al., 2010; Muraleedharan et al., 2011), positioning it as a useful example in understanding how state capacity is mobilized during a complex global emergency with national and local implications. Tamil Nadu has also experienced previous disease outbreaks and natural disasters, which have strongly tested the public health response (Gupta et al., 2010; Gaitonde and Gopichandran, 2016). The application of learnings from previous emergencies has been previously documented in the case of Kerala (Sundararaman and Gaitonde, 2021) but has not yet been fully explored in Tamil Nadu. Major factors such as statewide elections in 2021 (Mahmood, 2022) and nationwide challenges in the procurement and distribution of medical oxygen and certain drugs (Economic Times, 2021) are also important to understand as influences on the capacity to develop and implement policy responses.
The ability of governments to coordinate and manage policy responses during crises is increasingly important given the growing complexity and scale of health and public policy decisions. As such, the experiences of developing and implementing policy responses during COVID-19 will yield important lessons for policy-making in the health sector (Hargovan et al., 2024). The purpose of this study is to examine the governance capacity to develop and implement a policy response to a major health emergency—COVID-19—in Tamil Nadu, India, and to understand the factors shaping governance capacity during the first and second waves (2020–21). By analysing the dynamics of state-level capacity in Tamil Nadu during those turbulent times, this study provides important learnings for other contexts globally regarding the drivers shaping the policy response to crises.
Theoretical framework
The abilities, competencies and capabilities of governments to perform their policy functions are a major influence on policy process dynamics (Wu et al., 2015). Capacity is a key determinant shaping health policy processes and has been referenced—through explicit references to capacity or through reference to quality, expertise and effectiveness—in several health policy frameworks, including the studies by Grindle and Thomas, (1989), Shiffman and Smith (2007) and Walt and Gilson, (1994). Several concepts have been used to describe and explain the capacity of the public sector, including state capacity, governance capacity, policy capacity, resilience and government effectiveness (Chae, 2023). In this paper, we draw on the public administration literature regarding governance capacity and governance legitimacy and the ways in which these dimensions impact crisis management. Examining governance response through the lenses of capacity and legitimacy surfaces processual dynamics, i.e. the individual, interpersonal, organizational and systemic factors that shape the policy response of governments to crisis (Christensen et al., 2016). Recent analyses have applied governance capacity and legitimacy to understanding the response to COVID-19 in contexts such as China and Norway (Christensen and Lægreid, 2020; Mao, 2023).
Governance concerns ‘a set of processes (customs, policies, laws) that are formally or informally applied to distribute responsibility or accountability among actors of a given [health] system’ (Barbazza and Tello, 2014). Crisis management is one among many governance functions held by governments in the event of major external shocks that are increasingly global and complex. However, crisis also upends routine governance processes and organizational responsibilities due to their unpredictable and dynamic nature, demanding different arrangements that facilitate timely action on a range of coordination, management and implementation functions (Christensen et al., 2016). In this way, crisis management demands a particular form of capacity focused not only on structures and resources but also on ‘professional communities of practice’ able to perform a diverse range of functions under pressures that are distinct across types of crises ( ‘t Hart and Sundelius, 2013).
Governance capacity is defined as ‘formal structural and procedural features of the governmental administrative apparatus but also informal elements, that is, how these features work in practice’ (Christensen et al., 2016). Governance capacity and performance during periods of crisis are also strongly influenced by context, particularly institutional, organizational and political (Christensen et al., 2016; Berman et al., 2023). Institutional context pertains to the formal and informal structures that guide actions and behaviours, with regime type, political institutions, laws, regulations and policies providing the formal framework or structure to act within, while values, norms and beliefs shape the informal dynamics undergirding these processes and structures (Greer et al., 2020). Organizational context provides an understanding of the types of units at different levels of government, the nature of their interactions, and its impact on crisis management (Christensen et al., 2016).
Embedded within this context are the governance capacities for organizations to respond to crisis, with two salient aspects—coordination and specialization (Christensen et al., 2016). Coordination concerns the act of bringing units within and outside of government together around a shared goal, heightened in times of crisis by time pressures, unpredictability and reordering in relationships and power dynamics (Christensen et al., 2016). Coordination can be conceptualized along two dimensions—vertical and horizontal (within the same sector line and between levels of government, such as central, state and local or at the same level of government but across sectors) and internal and external (within government and with organizations outside of government). From a capacity standpoint, coordination can emerge from ‘soft’ mechanisms, such as levels of trust and a sense of shared purpose, as well as ‘hard’ mechanisms, such as formal agreements and regulations (Turner et al., 2022).
Specialization refers to the types of responsibility and expertise that are distributed within and outside the institution, as well as the coordination of knowledge and skill (i.e. geography, clientele and process). In the context of health emergencies, diverse forms of expertise are required which can be grouped under the following domains: public health, clinical and other forms of public policy. Expertise where available may be located within or outside the government and drawn into policy processes based on the nature of the crisis. Studies on specialization and health policy processes during crisis have noted that the utilization or role of internal and external experts from within and outside government is strongly dependent on institutional and political factors (Cairney and Wellstead, 2021).
Impacting these capacities is the degree to which the responsibility for a particular crisis response is centralized or decentralized. Centralization here refers to the extent to which crisis management functions are held within a particular sector or level of government. Decentralization refers to the ways in which these responsibilities are then distributed to ‘lower’ levels of government or sectors. The literature on governance capacities and decentralization in the health sector suggests that capacities vary across subnational jurisdictions based on jurisdictional wealth and processual learning (Abimbola et al., 2019). Furthermore, capacities across multiple levels of governance perform a ‘backup’ or ‘shock absorber’ function in order to compensate for weaknesses at any level of governance (Abimbola et al., 2019).
While capacity concerns the internal functioning of government and its partners, consideration must also be given to how government actions and policies are perceived by the public. Governance legitimacy refers to ‘the relationship between government authorities and citizens’ (Christensen et al., 2016) and focuses on citizen perceptions of government actions.
Methods
We utilized a single case study approach to examining the response to COVID-19 by state authorities in Tamil Nadu from early 2020 to August 2021. We drew upon three sources of information: (1) a review of key policy documents (n = 164); (2) a review of English-language media articles in the Indian press (n = 336); and (3) in-depth interviews with senior decision makers, technical experts, civil society leaders and media representatives (n = 10). Our study team consisted of emerging and established researchers from India and Canada and also included individuals with experience in managing health crises with the Government of Tamil Nadu, including one team member involved in the COVID-19 response.
Document review
Two team members (S.B.T. and H.N.G.L.) identified and reviewed ∼164 policy documents, primarily from March 2020 to September 2021. These documents consisted of government orders, directives and other official notifications of policy. The majority of our documents explored policies at the state level, but we also included policies from the central level that were particularly relevant during the first and second waves. The document review was supplemented by other sources, such as PRS Legislative Research and peer-reviewed literature. Document review is available in Supplementary Appendix 1.
Media review
One team member (H.N.G.L.) analysed 336 media articles. The articles primarily explored governance updates (i.e. new orders, formation of taskforces, etc.), case numbers, lockdown policies, treatment guidelines and vaccination policies. The media articles were primarily from The Hindu’s English-language daily paper. Articles from The Hindu were supplemented by specific articles from The Indian Express and Economic Times. The review of media articles is available in Supplementary Appendix 2.
In-depth interviews
We prioritized a limited number of in-depth, high-quality interviews with very senior individuals within the response. From June 2022 to September 2022, we conducted 10 in-depth interviews with senior, highly ranked current and former decision makers in the Government of Tamil Nadu (n = 7), as well as representatives of research institutes (n = 1), civil society (n = 1) and the media (n = 1). These interviews were conducted in person by V.S. and G.V. (n = 3) or on Zoom (n = 7) by V.S., G.V., S.B.T., H.N.G.L. and S.H. Interviews were semi-structured and ranged from 45 min to 2 h. Some respondents were shown drafts of the organograms, based on which detailed feedback was provided. Two interviews were recorded, while eight were unrecorded but involved detailed note-taking by team members.
Analysis
The first stage of the analysis was to prepare detailed timelines of the policy response to COVID-19 in Tamil Nadu, drawing on the document review and analysis of news articles. The second stage was to prepare the draft of detailed organograms for each COVID-19 wave, drawing on existing data (Government of Tamil Nadu websites) and knowledge of the response by analysts within the team. Organograms were then repeatedly revised following respondent feedback, interview transcripts and document review and consolidated into one figure (Figure 1).
Figure 1.

Organizations involved in COVID-19 governance in Tamil Nadu (non-exhaustive and illustrative)
Recorded interviews were transcribed using otter.ai and cleaned and checked by H.N.G.L., S.H. and S.K. An initial draft of a codebook was developed using a combination of a priori concepts—institutions, politics, organizations and governance—and inductively through repeated review of the data. This codebook was applied to the same two transcripts by two analysts (S.H. and V.S.) after which modifications were made to the codebook. The final codebook was applied to the full set of 10 transcripts using NVivo v. 12. Initial themes were developed by the research team through the coding process and regular debriefing within the team. Themes continued to be iteratively developed through an application of theoretical concepts from governance capacity and legitimacy. Findings from the study were shared with three respondents; their feedback was incorporated based on the remit and scope of the research project.
Results
Institutional, organizational and epidemiological context
Tamil Nadu is a state in Southern India with a population of 72 147 030 as per the 2011 Government of India census. Public health has also long been part of the institutional framework in Tamil Nadu, in terms of both legislation and organizational capacity. The establishment of a sanitary department in the 1860s and—following several epidemics in the region—the establishment of a Department of Public Health and Preventative Medicine in 1923 (with a specialized techno-administrative public health cadre) are some milestones during the colonial-era Madras Presidency (Mushtaq, 2009). These were followed by the introduction of the Madras Public Health Act in 1939 (later changed to the Tamil Nadu Public Health Act). Tamil Nadu is also unique in that it did not amalgamate its medical and public health services, thereby building a strong public health management cadre at the district level (IDI1, IDI3 and IDI4).
…there is a public health way of doing things in Tamil Nadu, because of its legacy with the public health service… (Journalist, IDI4).
As described in Figure 1, in Tamil Nadu, the mandate and resources for addressing health emergencies, however, extend beyond public health and involve the Revenue Department, State and District Disaster Management Authorities, the Department of Municipal Administration and the health units of city corporations (IDI2).
Figures 2 and 3 provide an overview of key milestones in the response to COVID-19 in Tamil Nadu. In late 2019, public health officials in the state began to track developments emerging out of China and globally (PRS Legislative Research). Discussions at the cabinet level accelerated in early to mid-March 2020, followed by the declaration of COVID-19 as a notifiable disease under the Tamil Nadu Public Health Act on 13 March 2020. The first case had appeared a week earlier, on 7 March 2020 (Times of India, 2020).
Figure 2.
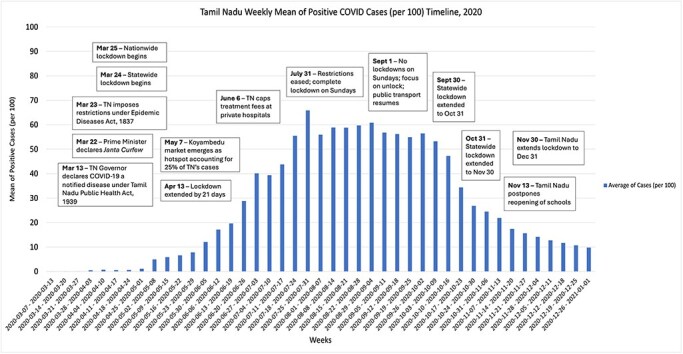
Key milestones in COVID-19 policy response in Tamil Nadu (2020) (weekly mean cases per 100)
Figure 3.

Key milestones in COVID-19 policy response in Tamil Nadu (2021) (weekly mean cases per 100)
Respondents noted that a vigorous response began to cohere at the level of the Chief Secretary, the leading Indian Administrative Services (IAS) bureaucrat in the state government, by late March (IDI1–IDI3, IDI5–IDI7 and IDI10; Government of Tamil Nadu, 2020b), particularly following lockdown orders from the central government (Government of Tamil Nadu, 2020a). The initial Janata Curfew (22 March 2020) was followed by a 3-week national lockdown that began on 25 March 2020. This was extended nationally until May 2020. The state government preceded this by 1 day (24 March 2020) and extended this lockdown by several months, until 31 August 2020, gradually relaxing the severity of the lockdown.
The first wave was marked by clusters of cases associated with national and international travel, as well as those associated with transmission at a major wholesale market in Chennai, Koyambedu Wholesale Market Complex. Public health measures were slowly relaxed from August 2020 onwards as the ‘unlock’ phases began, followed by steadier relaxation in measures towards the end of 2020 and into 2021. The months between January and March 2021 saw increased election-related activity (The Hindu, 17 March 2021c). Cases began to steadily increase in the first weeks of April 2021 (The Hindu, 2021f). The period of striking escalation in cases in Tamil Nadu coincided with a ‘lame duck’ government during statewide elections. The peak of the second wave in Tamil Nadu occurred on 21 May 2021 with 36,184 cases (The Indian Express, 2021), just 2 days after a new political party took charge of the state government. By this time, the crisis had become one of ‘supply and demand’, exemplified by the drastic shortage of not only medical oxygen but also hospital beds and pharmaceutical treatments.
If you look at it this way, the first wave was managed more from a public health point of view, the second wave was more from a therapeutic point of view (Senior government official, IDI2).
Public health measures were relaxed after the reduction in cases following the second wave (from approximately July 2021 onwards). Efforts to expand vaccination further accelerated in September 2021 (The Hindu, 2021e). As of November 2023, Tamil Nadu had witnessed 3.6 million cases of COVID-19, with ∼38 000 deaths (Statistica, 2023).
Influence of political processes and context on governance capacity
During the first wave, several respondents noted that the political executive also started to mobilize, after a period of uncertainty regarding the seriousness of the problem. One respondent noted that the political executive was convinced by bureaucrats that the pandemic was proceeding in this direction and that the reaction was like ‘stages of grief … denial, then acceptance’ (Senior government official, IDI5). In March 2020, political leaders began to mobilize in support of state action regarding COVID-19 and bureaucrats also worked to keep politicians from ruling and opposition parties informed of policy decisions.
Following the intensive policy response to the first wave, respondents noted a sense of complacency or a ‘lull’ in the months that followed due to declining case counts and mortality in the state and due to perceived successes with the first wave response (IDI5, IDI6, IDI7, IDI8 and IDI9). As noted by one respondent, ‘… there was this feeling that the problem has gone away, and they had managed very well … so I think they completely underestimated’ (Civil society representative, IDI8).
Preparatory work for statewide elections in April 2021 started in late January 2021. This period, which in retrospect was clearly a ‘calm before the storm’, was perceived differently by respondents. Public health experts within and outside government were warning of an impending increase in transmission (IDI9). Some bureaucrats similarly felt that the election was going to contribute to a rise in cases and were concerned about rising caseloads in other countries (IDI2, IDI5, IDI6 and IDI7). Moreover, one of the challenges faced by bureaucrats in the response was that the entire bureaucracy had to shift towards election-related activities (IDI2, IDI5, IDI7 and IDI10). As shared by one respondent, ‘[the] entire machinery goes into election mode’ (Senior government official, IDI5).
The period between late 2020 and March 2021 saw a confluence of two challenges. First, it was challenging to enforce public health measures, such as managing crowd size and mask usage, during the period of political campaigning (IDI7, The Hindu, 2021a). Challenges with public health measures were so stark that the Madras High Court issued a stern statement to the Election Commission regarding its role in disease transmission (Times of India, 2021; The Hindu, 2021d).
[Justices] said public health was of paramount importance and that it was distressing to note that Constitutional authorities had to be reminded of it. Only when a citizen survives, would he/she be able to enjoy the rights that a democratic republic guarantees to him/her, they said (The Hindu, 26 April 2021d).
The second challenge was that it was difficult to issue major policy decisions during the election period (IDI5 and IDI7), resulting in a decision-making vacuum during an important phase in the trajectory of the pandemic. These factors, coupled with the limited autonomy and authority of public health officials, resulted in a distressing scenario of rising caseloads but a limited response.
Specialization, coordination and the influence of centralization/decentralization processes
Across the first and second wave of COVID-19, governance capacities—as illustrated through trends in specialization and coordination—were strongly tested due to shifting patterns of centralization and decentralization.
Specialization
In January–February 2020, internal guidelines were introduced to address the growing concern of a pandemic from specialized state public health officials through specific public health measures (The Hindu, 2020a, The Hindu, 20 January 2020 IDI3). For example, routine screenings for respiratory illnesses were monitored, and border and surveillance teams were activated at airports and the state border with Kerala (The Hindu, 2020b).
With China reporting an outbreak of a novel coronavirus, the Directorate of Public Health and Preventive Medicine has instructed doctors to look out for symptoms of influenza-like illnesses, regardless of patient travel history to the affected country (The Hindu, 20 January 2020).
While the pandemic was truly an unprecedented crisis, respondents also described the Tamil Nadu bureaucratic cadre as being robust and with many experienced IAS bureaucrats (IDI1, IDI2, IDI5 and IDI6), drawing on learnings from recent experiences in managing diseases and outbreaks, such as chikungunya, dengue and H1N1, as well as complex emergencies, such as the Indian Ocean tsunami, recurrent cyclones and floods. Officials within the state learned many lessons from these experiences and applied them in the context of COVID-19, such as involvement of the Commissioner of Revenue Administration in order to strengthen coordination with District Collectors, the chief bureaucrat in each district (IDI1 and IDI3). A key learning was that intersectoral collaboration was critical, and as stated by one respondent ‘[the] disease is bigger than the department’ (IDI1, senior government official).
Specialized knowledge from within the public health team regarding the optimal approaches to limiting transmission was, however, not always heeded (IDI1, IDI3, IDI6 and IDI9). For example, one respondent noted that approaches such as lockdowns, quarantines, surveillance at ports of entry and contact tracing were not viewed as particularly effective in comparison to measures such as masking, ventilation and hospital preparedness (e.g. increasing bed and oxygen capacity) (IDI3). The overarching framework set down by the central government in the form of the lockdown, global uncertainty regarding best practices to manage the pandemic and limited authority given to public health officials due to the dominance of IAS bureaucrats in decision-making resulted in a lack of autonomy for public health officials (IDI1, IDI6 and IDI9).
Expertise was also periodically drawn from outside of the state government. The National Institute of Epidemiology (based in Chennai) was closely involved with state- and local-level public health officials in designing surveillance systems (Jagadeesan et al., 2022). State- and local-level committees were also frequently constituted, and experts within and outside of India were consulted, covering issues ranging from treatment protocols to economic recovery (The Hindu, 2020c).
Since the COVID-19 lockdown was announced 45 days ago, Tamil Nadu has formed 15 committees comprising senior civil servants, IPS officers and other experts to handle multiple issues arising out of the pandemic. The strategy has largely paid off. Civil servants, who are multitasking, have also used this as an opportunity to innovate, launching delivery apps and utility portals (The Hindu, 8 May 2020).
On Thursday, the Chief Minister had said that a decision on extending the lockdown depended on the advice of the 19-member committee of medical experts and the government’s 12 panels on tackling COVID-19 scenario (Times of India, 10 April 2020).
The periods in between the waves were marked by inaction, with different groups of officials taking different views of the pandemic’s trajectory (IDI5). Public health guidance from state and external experts regarding the potential for a devastating second wave was not heeded at this time (IDI9). The decision-making void during the transition phase between the elections and announcement of results also coincided with the marked escalation of cases. Upon taking office, the new government began to mobilize internally and with external experts.
Coordination
During the first wave, respondents noted that the Chief Secretary was the primary coordinator of the initial response, coordinating across departments and managing interactions with political leaders and the Government of India and also with District Collectors. Respondents were particularly appreciative of the culture facilitated by the Chief Secretary, such as allowing for debate among officers and the inclusion of junior officers in decision-making. As one respondent noted, ‘[there was an] initial phase of acting, reacting, little bit of fighting’ and that a ‘tug of war was there … very palpable’ (IDI5). The Chief Secretary also played a role in stepping in when various challenges were taking place in the wide range of departments, boards and other units involved in the response.
From an organizational standpoint, a wide variety of structural shifts (i.e. new committees, taskforces and control rooms) were initiated (Times of India, 2020). From a personal standpoint, officers were regularly shifted to address emerging challenges and nodal officers were utilized to oversee the response—an innovation from previous emergencies (IDI1).
A State Emergency Operations Centre (SEOC) was activated within the Directorate of Public Health Control Room. This was a refurbished physical space with support from the US Centers for Disease Control, Indian Council of Medical Research and the National Health Mission (“CDC and India”, 2021, IDI3). Officials, including bureaucrats, were brought in from different departments and with different levels of seniority to operationalize the SEOC. Respondents in this study held mixed views on the effectiveness of the SEOC, describing the platform as ‘adhoc’ and ‘[adding] to the confusion’ (Senior government official, IDI6).
Another key issue that the functioning of the SEOC illustrated was power dynamics ‘within’ the bureaucracy. For example, one issue that emerged in the response was the role of the Director, Public Health and Preventative Medicine (DPH), vis-à-vis the IAS officers who had been brought into managing the response (IDI2). The DPH typically plays a predominant role in managing health emergencies; however, given the complex nature of the growing crisis and the involvement of other officials, its role has diminished (IDI2). Furthermore, many agencies and branches, which had typically not worked closely together, as well as a mix of officers across departments, seniority and hierarchy, were working together for the first time (IDI5 and IDI6).
Efforts taken to coordinate and engage civil society groups were seemingly mixed. Civil society organizations played a critical role in supplementing the response, for example, by supporting migrant workers, providing food and other social assistance and conducting local monitoring (Firstpost, 2020; Arogya Iyakkam Resource Collective, 2021; Bandyopadhyay et al., 2021). During the first wave, there did not appear to be an official or periodic forum for engaging civil society at the state and local levels despite their major role (IDI8). However, efforts to engage non-governmental organizations began to occur more systematically through the formation of a committee in May 2021 to coordinate actions (Times of India, 2021).
During the second wave, one of the first government orders issued by the new government was the establishment of a newly constituted ‘War Room’ (building on a Unified Command Center that was announced on April 30), established on 8 May 2021. This innovation drew on examples from Kerala and Maharashtra. Although the SEOC continued, it was no longer the hub of decision-making. The aim of the War Room was to unify and coordinate the activities related to managing and controlling the spread of COVID-19 across the state. By this time, the crisis had become more one of ‘supply and demand’, i.e. the focus was on attending calls from the public, oxygen, beds and treatments (meeting the supply of these needs with demand from the public). The establishment of the War Room also seemingly aimed to improve public perception and confidence in the overall response. For example, the Chief Minister visited the War Room and participated in responding to calls from the public (India Today, 2021).
Impacts of centralization/decentralization
Centralization of the response in the context of Tamil Nadu involved dynamic shifts in the balance of power between central, state and local leaders. During the first wave, respondents noted that while the overall direction for the lockdown was provided by the central government, granular details and implementation needed to be worked out within the state. As stated by one senior-level government official, ‘the lockdown came as a shock. Nobody was prepared for such a big jolt to the system’ (Senior government official, IDI10). Despite the sudden nature of the lockdown, some respondents shared that the strength of the state bureaucracy and the pivotal role played by the Chief Secretary allowed the response to eventually settle and take a structured approach (IDI1–IDI3, IDI5–IDI7 and IDI10). Districts had fewer decision-making roles and were primarily involved in implementing orders from the state level.
In contrast to the first wave, the central government had almost largely delegated powers to the states during the second wave, including around lockdowns and movement restrictions (with some exceptions, e.g. certain aspects of oxygen supply and delivery and international travel). Allocation conflicts with the central government around liquid oxygen, vaccinations and other materials were also heightened at this time (Radhakrishnan, 2021; The Hindu, 2021a). Within the state, the level of crisis resulted in further decentralization, where District Collectors and other officials drove key aspects of the response, e.g. managing beds and oxygen. Procurement and regulation of pharmaceutical treatments, such as remdesivir and tocilizumab, were managed at the state level (IDI2).
The immense challenges of securing oxygen during the second wave exemplify many of these issues. Despite some efforts to expand the supply of liquid oxygen during the first wave, challenges began to rapidly escalate during the second wave when oxygen cylinders were insufficient to address the demand, and liquid oxygen was required. Respondents in our study as well as media reports described the harrowing experience of trying to rapidly and urgently locate sources of liquid oxygen, with hours to spare for certain facilities (The Hindu, 2021b,g).
There was no help coming from any side. I had to manage on my own using whatever jugaad (innovations) came to mind (State government official, IDI7).
While some District Collectors set up response mechanisms, such as effective war rooms and innovative approaches to oxygen and bed management, others were more dependent on the state-level War Room or external experts (IDI6 and IDI7). Furthermore, some respondents noted additional challenges regarding the capacity of officials at the district level. In some districts, there was limited institutional memory around pandemic preparedness and structures had to be developed de novo to address the emerging crisis. In other districts, bureaucratic demands resulted in immense pressure on health and other officials, such as data entry and analysis, limiting their ability to develop and implement responses to the crisis (IDI9). Civil registration systems (i.e., death registration) and transparency around these statistics were also raised as concerns (IDI4, IDI9).Public health officials were also perceived to have less power when compared to the District Collectors and were expected to adhere to their approach to the response, limiting their autonomy to shape the response (IDI3 and IDI9).
Discussion
Research and analysis examining the dynamics of national and subnational policy responses to COVID-19 remain limited, despite their immense value in surfacing lessons for future health emergencies (McKee et al., 2022). As health crises escalate and grow in complexity, there is an urgent need to understand ‘how’ governments develop and implement policy and what factors shape these capacities. These learnings are equally relevant for developing and extending our theoretical understanding of governance capacities and their role in shaping the policy process at the subnational level. Furthermore, they yield policy-relevant findings that can help improve governance in the health sector, not only in Indian states but also in other contexts.
We develop four key insights from this analysis. First, Tamil Nadu’s institutional framework—legislative foundations, institutional learnings and robust bureaucratic and technical capacity—facilitated governance capacity at the state level during an emergency of massive complexity. This framework allowed for organizational flexibility and nimbleness in adapting to evolving dynamics of centralization and decentralization over the course of the pandemic. Secondly, despite a strong basis of technical expertise within and outside government, the ability to integrate particular forms of expertise, such as public health, was constrained across both waves. Thirdly, while the government actively coordinated with external groups, particularly through expert committees, engagement with civil society groups was more limited. Fourthly, political processes, specifically the statewide election in 2021, were perceived to negatively influence governance capacity in responding to the second wave. Each of these findings help extend our understanding of governance capacities and their influence on policy processes during crisis and also provide the basis for policy and programme recommendations for future emergencies (Box 1).
Box 1. Recommendations and policy implications.
-
At the state level, need for strengthening capacities and structure to assess, manage and respond to health emergencies, including infectious diseases:
Emergency powers for the DPH and scaling up of public health cadre up to the block level
Strengthening alert and response system for outbreaks in the state and districts (and at the community level)
Independent structures that can be mobilized during emergencies without/with limited political involvement
Improving coordination within the health sector and with other departments
Further deliberation over roles and coordination between SEOC, War Room and SDMA
Improving routine surveillance and civil registration systems (e.g., Medical Certification of Cause of Death)
Adoption of a learning-focused approach to health system development
District- and block-level decision-making, implementation and institutional learning require more investment and attention
Political processes such as elections limit the potential of bureaucratic capacity to manage crises—consideration of policy solutions to address this
-
Expanding space for civil society engagement in crises:
Adopting a citizen-centric approach in public health surveillance
Developing community-based surveillance.
Institutional dynamics are at the core of understanding policy responses to crisis and provide a useful entry point for understanding how governance capacities shape the policy response to crisis. In our analysis, we find that capacities around specialization and coordination were bolstered by a robust institutional framework. The state’s strong bureaucratic and public health cadre, the existence of key legislative foundations (i.e. Tamil Nadu Public Health Act) and learnings over multiple health emergencies (i.e. chikungunya, dengue, H1N1 and cyclones) aided in navigating shifting dynamics of centralization and decentralization, similar determinants to effective crisis response in other jurisdictions (Woo, 2020; Sundararaman and Gaitonde, 2021). As the locus of initiative shifted across levels of government from central to state in the first wave, and from state to local in the second wave, strong capacity at the state level and in some cases at the local level was able to serve as ‘shock absorbers’ to handle gaps in the crisis response (Abimbola et al., 2019).
Thus, the state could navigate major gaps in the national framework for pandemic response. A critical aspect of the response was the presence of strong leaders with the ability to coalesce and organize diverse departments and agencies; to coordinate across national, state and local levels; and to take rapid decisions. The culture of bureaucracy in Tamil Nadu also allowed for internal debate, particularly during the first wave, further contributing to individual and organizational learning and ultimately systems learning (Sheikh et al., 2022). Organizational innovations, in the form of the use of nodal officers and the establishment of the War Room, were facilitated by this framework. Future research can examine whether organizational flexibility renders existing structures less effective (i.e. the SEOC, the DPH Control Room and State Disaster Management Authority committees in this example) and what the connections are between organizational innovation and governance legitimacy.
Despite these strengths in Tamil Nadu’s response, our findings indicate that specialization capacities in developing and implementing policy responses were not sufficiently integrated, notwithstanding the flexibility shown in other aspects of the response. The dominance of IAS officers over public health officers—drawing on the legacies of past emergencies—is one potential explanation. The complex administrative nature of the crisis is another reason. During the pandemic, inputs from public health experts regularly ran up against established knowledge and bureaucratic hierarchies (Singer et al., 2021; Donadelli and Gregory, 2022). Understanding the role of health expertise during complex emergencies is therefore an important area for future work. Questions to probe include the following: do public health experts have autonomy and authority within the institutional framework to provide independent advice and guidance? What are the authority and power relations between bureaucrats and public health technocrats during complex emergencies? What do public health officials perceive as the major barriers to having their viewpoints integrated into the policy response?
The presence of strong leaders and robust networks is a critical component of policy process theory (Shiffman and Smith, 2007), intensified during crisis. As noted, Tamil Nadu had strong leaders at the state and district level, but the presence of these individuals was also uneven, a pattern observed in health governance in India (Bhuputra and Thakur, 2016). Engagement with networks of civil society organizations outside the government system was similarly uneven although experts were engaged repeatedly in both waves. Limited formal participation of civil society organizations in policy processes also raises questions regarding governance legitimacy, an arguably challenging endeavour during periods of crisis, but one that has proven to be an asset in COVID-19 responses (Hanson et al., 2021; Levine et al., 2023).
Finally, a key contribution of our findings is bringing in the influence of political context and processes (e.g. elections) on governance capacity. Other studies have noted the strong influence of political and administrative context on shaping positive developments in health service delivery and health outcomes in Tamil Nadu (Smith, 2014). However, few studies have explored how political ‘processes’, capacity and crisis are connected. The engagement of political parties in managing the crisis was perceived positively by some respondents (with the exception of election-related rallies and activities). However, we found that the political process—in this case, statewide elections—constrained state-level officials, primarily due to the dominant focus on election-related processes within the bureaucracy in the lead-up to elections. Empowerment of public health officials in the response to public health emergencies would allow for additional capacity during periods of heightened political activity (Birch et al., 2020).
Limitations
This study had several limitations that must be considered when interpreting our findings. First, this study was conducted as an exploratory study regarding the response to COVID-19 in Tamil Nadu. A more comprehensive study involving a wider range of interviews at the state, district and block levels and from within and outside government should be undertaken to surface comparisons and learnings. Secondly, this study sought to provide a wide overview of the response, and as a result, we are unable to go into depth regarding particular areas of the response; each of these policy domains could in fact be the focus of an individual study going forward. Thirdly, there were several policy domains that were unfortunately not covered or covered minimally in this paper, such as routine medical care, private healthcare sector engagement, social security and border control. Finally, the analysis shared in this paper is largely based on the perspective of respondents involved in the response and through an analysis of policy and media documents; as such, we cannot make causal linkages between the decisions described here and the epidemiology of COVID-19 in Tamil Nadu.
Conclusion
The capacity to develop policy responses during crisis at the subnational level is an underdeveloped conceptual area of health policy process literature. The policy response to COVID-19 in Tamil Nadu as viewed through the lens of governance capacity is instructive in surfacing important conceptual and practical findings. While Tamil Nadu developed a robust institutional framework for developing policy responses to crisis, some areas of strengthening include the need to better integrate public health expertise into management of complex health emergencies, the importance of systematic engagement of non-state actors, including civil society organizations, institutional gaps in responding to crises during election cycles and further strengthening of leadership and coordination skills at the state and local levels. Key learnings from Tamil Nadu must be documented in order to ensure that such learnings are integrated into future pandemic preparedness planning in India and other contexts.
Supplementary Material
Acknowledgments
Our thanks to our respondents for their time and insight, and to Alessia Montecalvo for support in manuscript development.
Contributor Information
Veena Sriram, School of Population and Public Health, University of British Columbia, 2206 East Mall, Vancouver, BC V6T 1Z3, Canada; School of Public Policy and Global Affairs, University of British Columbia, 1855 West Mall, Vancouver, BC V6T 1Z2, Canada.
Girija Vaidyanathan, Department of Humanities and Social Sciences, Indian Institute of Technology—Madras, Chennai, Tamil Nadu 600036, India.
G S Adithyan, Department of Humanities and Social Sciences, Indian Institute of Technology—Madras, Chennai, Tamil Nadu 600036, India.
Shambo Basu Thakur, Department of Humanities and Social Sciences, Indian Institute of Technology—Madras, Chennai, Tamil Nadu 600036, India.
Simran Kaur, School of Public Policy and Global Affairs, University of British Columbia, 1855 West Mall, Vancouver, BC V6T 1Z2, Canada.
Hari Narayanan GL, School of Public Policy and Global Affairs, University of British Columbia, 1855 West Mall, Vancouver, BC V6T 1Z2, Canada.
Sabah Haque, School of Public Policy and Global Affairs, University of British Columbia, 1855 West Mall, Vancouver, BC V6T 1Z2, Canada.
V R Muraleedharan, Department of Humanities and Social Sciences, Indian Institute of Technology—Madras, Chennai, Tamil Nadu 600036, India.
Supplementary data
Supplementary data is available at Health Policy and Planning Journal online.
Author contributions
V.S., G.V. and V.R.M. were involved in the conception or design of the work. V.S., G.V., H.N.G.L., S.B.T., S.H., S.K. and A.G.S. were involved in data collection. V.S., G.V., H.N.G.L., S.B.T., S.H., S.K. A.G.S. and V.R.M. were involved in data analysis and interpretation. V.S. and G.V. were involved in drafting the article. V.S., G.V., S.K., H.N.G.L., S.B.T., S.H., A.G.S. and V.R.M. were involved in the critical revision of the article. V.S., G.V., S.K., H.N.G.L., S.B.T., S.H., A.G.S. and V.R.M. were involved in the final approval of the version to be submitted.
Reflexivity statement
Our research team consists of researchers who are all of Indian and South Asian origin. The team is a combination of researchers based at the Indian Institute of Technology—Madras (based in Chennai, India) and the University of British Columbia (Vancouver, BC, Canada). We are a mix of emerging researchers (S.K., S.H., H.N.G.L. and S.B.T.), mid-career researchers (V.S. and A.G.S.) and established researchers (G.V. and V.R.M.). Two team members had extensive experience in managing health crises with the Government of Tamil Nadu (G.V. and A.G.S.), including one team member involved in the COVID-19 response (A.G.S).
Ethical approval
Ethical approval was received by the University of British Columbia in Vancouver, BC (H22-00567).
Conflict of interest
A.G.S. served as a consultant in the National Health Mission in Tamil Nadu from 2017 to 2022. G.V. was a civil servant in the Government of Tamil Nadu until 2019.
Funding
This study was funded by the University of British Columbia (Health After 2020).
Data availability
Some of the data underlying this article are available in its online Supplementary data. Interview data underlying this article cannot be shared publicly in order to protect the privacy of individuals who participated in the study.
References
- Abimbola S, Baatiema L, Bigdeli M. 2019. The impacts of decentralization on health system equity, efficiency and resilience: a realist synthesis of the evidence. Health Policy & Planning 34: 605–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arogya Iyakkam Resource Collective . 2021. Learning from Tamil Nadu’s Response to COVID-19 Pandemic: Lessons for the Right to Health Agenda. Tamil Nadu Science Forum & Pondicherry Science Forum for the People’s Health Movement (Makkal Nalavazhvu Iyyakkam). https://aipsn.net/wp-content/uploads/2021/11/Learning-from-TN_29Nov2021.pdf (10 October 2023, date last accessed).
- Askim J, Christensen T. 2022. Crisis decision-making inside the core executive: rationality, bureaucratic politics, standard procedures and the COVID-19 lockdown. Public Policy and Administration 09520767221129676. [Google Scholar]
- Bandyopadhyay KK, Chawla M, Aravind SR, and Sharma Y. 2021. Civil Society Support to COVID-19 Affected Families: Outreach and Resourcing in the Second Wave. PRIA. https://www.pria.org/knowledge_resource/1625214248_Civil_Society_Support_to_C19_Affected_Families_During_2nd_wave.pdf (5 October 2023, date last accessed).
- Barbazza E, Tello JE. 2014. A review of health governance: definitions, dimensions and tools to govern. Health Policy 116: 1–11. [DOI] [PubMed] [Google Scholar]
- Berman P, Cameron MA, Gaurav S et al. 2023. Improving the response to future pandemics requires an improved understanding of the role played by institutions, politics, organization, and governance. PLoS Global Public Health 3: e0001501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birch S, Buril F, Cheeseman N et al. 2020. How to Hold Elections Safely and Democratically during the COVID-19 Pandemic. London: The British Academy. [Google Scholar]
- Cairney P, Wellstead A. 2021. COVID-19: effective policymaking depends on trust in experts, politicians, and the public. Policy Design and Practice 4: 1–14. [Google Scholar]
- Cameron MA, Hurtado V, Sosa Villagarcia P, Gombata M. 2023. A tale of two crashes: pandemic politics in Brazil and Peru. Latin American Perspectives 50: 248–67. [Google Scholar]
- Capano G, Howlett M, Jarvis DSL, Ramesh M, Goyal N. 2020. Mobilizing policy (in)capacity to fight COVID-19: understanding variations in state responses. Policy and Society 39: 285–308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC and India . 2021. CS322044-AU September 10, 2021. CDC India. https://stacks.cdc.gov/view/cdc/110337 (1 October 2023, date last accessed). [Google Scholar]
- Chae SH. 2023. State capacity and COVID-19: targeted versus population-wide restrictions. Journal of Health Politics, Policy and Law 48: 889–918. [DOI] [PubMed] [Google Scholar]
- Christensen T, Lægreid P. 2020. Balancing governance capacity and legitimacy: how the Norwegian government handled the COVID-19 crisis as a high performer. Public Administration Review 80: 774–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen T, Lægreid P, Rykkja LH. 2016. Organizing for crisis management: building governance capacity and legitimacy. Public Administration Review 76: 887–97. [Google Scholar]
- Christensen T, Ma L. 2021. Comparing SARS and COVID-19: challenges of governance capacity and legitimacy. Public Organization Review 21: 629–45. [Google Scholar]
- De Goyet CDV. 2007. Health lessons learned from the recent earthquakes and tsunami in Asia. Prehospital and Disaster Medicine 22: 15–21. [DOI] [PubMed] [Google Scholar]
- Donadelli F, Gregory R. 2022. Speaking truth to power and power to truth: reflections from the pandemic. Public Organization Review 22: 327–44. [Google Scholar]
- Douedari Y, Howard N. 2019. Perspectives on rebuilding health system governance in opposition-controlled Syria: a qualitative study. International Journal of Health Policy and Management 8: 233–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Economic Times . 2021. Tamil Nadu Battles Shortage of Beds, Oxygen and Vaccines. Economic Times. https://economictimes.indiatimes.com//news/india/tamil-nadu-battles-shortage-of-beds-oxygen-and-vaccines/articleshow/82809056.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst (1 September 2022, date last accessed).
- Firstpost . 2020. In Tamil Nadu, NGOs and Volunteers Pave Way for Migrant Workers as Govt Machinery Struggles to Cope with COVID-19 Crisis. https://www.firstpost.com/health/in-tamil-nadu-ngos-and-volunteers-pave-way-for-migrant-workers-as-govt-machinery-struggles-to-cope-with-covid-19-crisis-8415291.html. (1 September 2022, date last accessed).
- Gaitonde R, Gopichandran V. 2016. The Chennai floods of 2015 and the health system response. Indian Journal of Medical Ethics 1: 71–5. [DOI] [PubMed] [Google Scholar]
- Government of Tamil Nadu . 2020a. Disaster Management—Corona Virus Disease (COVID-19) —Infection Prevention and Control—The Disaster Management Act 2005—Notification Issued. Chennai: Revenue and Disaster Management Department. https://cms.tn.gov.in/sites/default/files/go/revenue_e_172_2020.pdf. (10 September 2022, date last accessed). [Google Scholar]
- Government of Tamil Nadu . 2020b. Infectious Diseases—Corona Virus Disease (COVID-19) Declared as a Notified Disease throughout the State of Tamil Nadu. Health and Family Welfare Department. https://cms.tn.gov.in/sites/default/files/go/hfw_e_95_2020.PDF (10 September 2022, date last accessed).
- Greer SL, da Fonseca EM, Raj M, and Willison C. 2022. Institutions and the politics of agency in COVID-19 response: federalism, executive power, and public health policy in Brazil, India, and the U.S. Journal of Social Policy 53: 1–19. [Google Scholar]
- Greer SL, King EJ, da Fonseca EM, Peralta-Santos A. 2020. The comparative politics of COVID-19: the need to understand government responses. Global Public Health 15: 1413–6. [DOI] [PubMed] [Google Scholar]
- Grindle MS, and Thomas JW. 1989. Policy makers, policy choices, and policy outcomes: The political economy of reform in developing countries. Policy Sci 22: 213–248. doi: 10.1007/BF00136320 [DOI] [Google Scholar]
- Gupta M, Desikachari BR, Shukla R et al. 2010. How might India’s public health systems be strengthened? Lessons from Tamil Nadu. Economic and Political Weekly 45: 46–60. [Google Scholar]
- Hanson C, Luedtke S, Spicer N et al. 2021. National health governance, science and the media: drivers of COVID-19 responses in Germany, Sweden and the UK in 2020. BMJ Global Health 6:e006691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hargovan M, London L, and Orgill M. 2024. The influence of crisis on policy formulation: the case of alcohol regulation in South Africa during COVID-19 (2020-2021). Health Policy & Planning 39: czae055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Hindu. 2020. Tapping expertise — how T.N. is handling the crisis. https://www.thehindu.com/news/national/tamil-nadu/tapping-expertise-how-tn-is-handling-the-crisis/article31538660.ece (15 September 2022, date last accessed)
- The Hindu. 2020. With coronavirus outbreak in China, TN asks doctors to look out for influenza-like illnesses. https://www.thehindu.com/news/national/tamil-nadu/with-coronavirus-outbreak-in-china-tn-asks-doctors-to-look-out-for-influenza-like-illnesses/article30605915.ece (17 September 2022, date last accessed).
- The Hindu . 2020a. City to Get Its Own Coronavirus Testing Centre at Guindy. The Hindu. https://www.thehindu.com/news/cities/chennai/city-to-get-its-own-coronavirus-testing-centre-at-guindy/article30696723.ece (12 September 2022, date last accessed).
- The Hindu . 2020b. Coronavirus: Tamil Nadu to Step up Surveillance along Kerala Border. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/coronavirus-state-to-step-up-surveillance-along-kerala-border/article30707078.ece (15 September 2022, date last accessed).
- The Hindu . 2020c. Expert Committee Set up to Tackle COVID-19. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/expert-committee-set-up-to-tackle-covid-19/article31195244.ece (15 September 2022, date last accessed).
- The Hindu. 2021. Facing the second wave of COVID-19. https://www.thehindu.com/news/national/tamil-nadu/facing-the-second-wave-of-covid-19/article38074727.ece (15 September 2022, date last accessed).
- The Hindu . 2021a. Coronavirus Updates|April 21, 2021. The Hindu. https://www.thehindu.com/news/national/coronavirus-live-april-21-2021-updates/article34372726.ece (15 September 2022, date last accessed).
- The Hindu . 2021b. COVID-19 Surge: First Tanker with 4.80 Tonne Oxygen Leaves Sterlite Copper’s Thoothukudi Plant. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/covid-19-surge-first-tanker-with-480-tonne-oxygen-leaves-sterlite-coppers-thoothukudi-plant/article34547789.ece (15 september 2022, date last accessed).
- The Hindu . 2021c. Increased Political Activity One of the Reasons for Rise in Fresh COVID-19 Cases, TN Health Secretary Says. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/increased-political-activity-one-of-the-reasons-for-rise-in-fresh-covid-19-cases-tn-health-secretary-says/article34090684.ece ( 15 September 2022, date last accessed).
- The Hindu . 2021d. Madras HC Blames ECI for Raging Second Wave of COVID-19 in T.N., Puducherry. The Hindu, https://www.thehindu.com/news/national/tamil-nadu/madras-hc-blames-eci-for-raging-second-wave-of-covid-19-in-tn-puducherry/article34413670.ece (15 September 2022, date last accessed).
- The Hindu . 2021e. Tamil Nadu Exceeds Target by over 9.85 Lakh COVID-19 Vaccine Doses at Mega Camp. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/tamil-nadu-exceeds-target-by-over-985-lakh-covid-19-vaccine-doses-at-mega-camp/article36687211.ece (15 September 2022, date last accessed).
- The Hindu . 2021f. Tamil Nadu Reintroduces Restrictions from April 10. The Hindu. https://www.thehindu.com/news/national/tamil-nadu/tamil-nadu-reintroduces-restrictions-from-april-10/article34276188.ece (15 September 2022, date last accessed).
- The Hindu . 2021g. TN Asks Oxygen Manufacturing Industries to Explore Ways to Increase Production. https://www.thehindu.com/news/national/tamil-nadu/tn-asks-oxygen-manufacturing-industries-to-explore-ways-to-increase-production/article34400308.ece (16 September 2022, date last accessed).
- India Today . 2021. Inside Tamil Nadu’s ‘Covid War Room’. India Today. https://www.indiatoday.in/india/story/inside-tamil-nadu-s-covid-war-room-1805283-2021-05-21 (16 September 2022, date last accessed).
- Jagadeesan M, Ganeshkumar P, Kaur P et al. 2022. Epidemiology of COVID-19 and effect of public health interventions, Chennai, India, March–October 2020: an analysis of COVID-19 surveillance system. BMJ Open 12: e052067doi: 10.1136/bmjopen-2021-052067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaplan A. (1999). The Developing of Capacity’, Community Development Resource Association. Cape Town: Centre for Developmental Practices. [Google Scholar]
- Levine AC, Park A, Adhikari A et al. 2023. The role of civil society organizations (CSOs) in the COVID-19 response across the Global South: a multinational, qualitative study. PLoS Global Public Health 3: e0002341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahmood Z. 2022. Elections during Covid-19: the Indian experience in 2020–2021. Case Study. International Institute for Democracy and Electoral Assistance. [Google Scholar]
- Mao Y. 2023. What accounts for the different regional responses to COVID-19 in China? Exploring the role of institutional environment, governance capacity and legitimacy. Health Policy & Planning 38: 552–66. [DOI] [PubMed] [Google Scholar]
- McKee M, Hanson K, and Abbasi K. 2022. Guided by the science? Questions for the UK’s Covid-19 public inquiry. BMJ 378: o2066. [Google Scholar]
- Mirzoev TN, Green A, Van Kalliecharan R. 2015. Framework for assessing the capacity of a health ministry to conduct health policy processes—a case study from Tajikistan. The International Journal of Health Planning and Management 30: 173–85. [DOI] [PubMed] [Google Scholar]
- Muraleedharan VR, Dash U, and Gilson L. 2011. Tamil Nadu 1980s–2005: a success story in India. In: Balabanova D, McKee M, Mills A (eds). Good Health at Low Cost 25 Years on. What Makes a Successful Health System?. London: The London School of Hygiene & Tropical Medicine, 159–192. [Google Scholar]
- Mushtaq MU. 2009. Public health in British India: a brief account of the history of medical services and disease prevention in Colonial India. Indian Journal of Community Medicine: Official Publication of Indian Association of Preventive & Social Medicine 34: 6–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Panda B, Thakur HP. 2016. Decentralization and health system performance—a focused review of dimensions, difficulties, and derivatives in India. BMC Health Services Research 16: 561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radhakrishnan RK. 2021. COVID Second Wave: Number of Worries for Tamil Nadu. Frontline. https://frontline.thehindu.com/the-nation/public-health/number-of-worries-tamil-nadu-second-wave-pandemic-handling/article34471049.ece (16 September 2022, date last accessed).
- Selvaraj S, Karan KA, Srivastava S, Bhan N, Mukhopadhyay I. 2022. India: Health System Review. Health Systems in Transition, Vol. 11. New Delhi: World Health Organization. Regional Office for South-East Asia. [Google Scholar]
- Sheikh K, Peters D, Akua Agyepong I et al. 2022. Learning is a means to progress and empowerment for health systems. BMJ Global Health 7: e010572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman J, Smith S. 2007. Generation of political priority for global health initiatives: a framework and case study of maternal mortality. Lancet 370: 1370–9. [DOI] [PubMed] [Google Scholar]
- Singer PM, Willison CE, Moore-Petinak N, and Greer SL. 2021. Anatomy of a failure COVID-19 in the United States. In: Greer S, King EL, da Fonseca EM, Peralta-Santos A (eds). Coronavirus Politics: The Comparative Politics and Policy of COVID-19. Ann Arbor, MI: University of Michigan Press, 478-493. [Google Scholar]
- Smith SL. 2014. Political contexts and maternal health policy: insights from a comparison of South Indian States. Social Science & Medicine (1982) 100: 46–53. [DOI] [PubMed] [Google Scholar]
- Statistica. 2023. Number of coronavirus (COVID-19) cases across Tamil Nadu. https://www.statista.com/statistics/1143336/india-tamil-nadu-covid-19-cases-by-type/ (30 October 2023, date last accessed).
- Sundararaman T, and Gaitonde R. 2021. India—learning from the Nipah virus outbreak to inform the COVID-19 response in Kerala. In: Sheikh K, Abimboka S (eds). Learning Health Systems: Pathways to Progress. Geneva: World Health Organization, 104-107. [Google Scholar]
- ‘t Hart PT, and Sundelius B. 2013. Crisis management revisited: a new agenda for research, training and capacity building within Europe. Cooperation and Conflict 48: 444–61. [Google Scholar]
- Times of India . 2020. Tamil Nadu Reports First Covid-19 Case; Man Tests +ve on Return from Oman. Times of India. https://timesofindia.indiatimes.com/city/chennai/tamil-nadu-reports-first-covid-19-case-man-tests-ve-on-return-from-oman/articleshow/74529856.cms (15 September 2022, date last accessed).
- Times of India . 2021. Election Commission Is Responsible for Covid-19 Surge, Must Face Murder Charges: Madras High Court. Times of India. https://timesofindia.indiatimes.com/city/chennai/election-commission-responsible-for-covid-19-surge-madras-high-court/articleshow/82254754.cms (16 September 2022, date last accessed).
- Turner S, Segura C, Niño N. 2022. Implementing COVID-19 surveillance through inter-organizational coordination: a qualitative study of three cities in Colombia. Health Policy & Planning 37:232–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walt G, and Gilson L.1994. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy Plan 9:353-70doi:doi: 10.1093/heapol/9.4.353. [DOI] [PubMed] [Google Scholar]
- Woo JJ. 2020. Policy capacity and Singapore’s response to the COVID-19 pandemic. Policy and Society 39: 345–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu X, Ramesh M, and Howlett M. 2015. Policy capacity: A conceptual framework for understanding policy competences and capabilities. Policy and Society 34:165–171. doi: 10.1016/j.polsoc.2015.09.001 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Some of the data underlying this article are available in its online Supplementary data. Interview data underlying this article cannot be shared publicly in order to protect the privacy of individuals who participated in the study.