

Abstract
Intrathoracic kidney is very rare and has the lowest prevalence among all renal ectopias. We report the case of a 70-year-old male who was referred for diethylenetriaminepentaacetic acid (DTPA) scan as a part of presurgical work-up for a right renal mass. PriorUltrasonography abdomen incorrectly reported left kidney as normal in location. 99mTc-DTPA renal scan combined with single-photon emission computed tomography – computed tomography revealed impaired global glomerular filtration rate with left kidney in ectopic (intrathoracic) location. 18-fluorodeoxyglucose positron emission tomography-computed tomography images revealed a soft tissue mass completely replacing the right kidney with metastases to bilateral lungs. This case reemphasizes the importance of nuclear medicine imaging in diagnosis and evaluation of the renal function of the intrathoracic kidney.
Keywords: Diethylenetriaminepentaacetic acid scan, ectopic kidney, fluorodeoxyglucose positron emission tomography-computed tomography, intrathoracic kidney, single-photon emission computed tomography – computed tomography
Introduction
Ectopic kidney refers to a kidney situated in any location other than the renal fossa. Ectopic kidneys occur in approximately 1 in 1000 births, but only about 1 in 10 are ever diagnosed. Intrathoracic kidneys are very rare and represent <5% of all renal ectopias.[1,2] Measurement of differential function is difficult in renal ectopias.[3] We describe a case of a 70-year-old male referred for 99mTc-diethylenetriaminepentaacetic acid (DTPA) renal scan to assess renal function as a part of presurgical work-up of right kidney mass. Prior ultrasonography (USG) incorrectly reported the left kidney as normal in location. However, a 99mTc-DTPA renal scan with single-photon emission computed tomography – computed tomography (SPECT-CT) identified the left kidney to be intrathoracic in location. This case highlights the importance of nuclear medicine imaging in not only diagnosis but also in the evaluation of the function of the intrathoracic ectopic kidney.
Case Report
A 70-year-old male presented with pain abdomen for 5 months. He underwent USG abdomen, which revealed a lobulated iso to a hypoechoic lesion in the right kidney measuring 10.6 cm × 7.1 cm × 11.6 cm, with no hydronephrosis or calculus. The left kidney was reported to be normal in location, size, outline, and echogenicity with maintained corticomedullary differentiation and no hydronephrosis or calculus. Serum creatinine was reported as 1.5 mg/dL (normal range: 0.7–1.3 mg/dL). The patient was planned for radical nephrectomy and was referred for Tc-99m DTPA renogram study for evaluation of renal function as a part of presurgical evaluation [Figure 1.] 99mTc-DTPA renal scan-dynamic (B) images show heterogeneous cortical uptake in the right kidney. However, the left kidney was not visualized in the left renal fossa. On further inspection of the dynamic images, a focal spot of tracer activity (arrow) was noted in the left upper aspect of the field of view (FOV). Hence, we took a static image to confirm the same. Static image in posterior view [Figure 2a] with increased FOV covering the thorax and the abdomen revealed an ectopic left kidney located in an intrathoracic location (arrow). SPECT-CT images [Figure 2b] revealed an elevated left hemi diaphragm with a malrotated ectopic left kidney lying completely above the diaphragm in the left hemi thorax. Herniation of the spleen and large bowel loop was also noted. The right kidney was normal in a location with evidence of a large lobulated mass almost completely replacing the right kidney. Hence, the renal dynamic study with 99mTc DTPA was repeated with corrected FOV. The study was acquired for 30 min in both anterior and posterior views after an intravenous injection of 5mCi of 99mTc-DTPA radiopharmaceutical. Adequate hydration was maintained before the scan. Injection frusemide (40 mg) was administered at the 10th min of the study. Processed 99mTc-DTPA renal scan images [Figure 3] showed elevated background tracer activity with a global glomerular filtration rate of 50.1 mL/min. The left kidney was ectopic (intrathoracic) in a location with nonobstructive drainage. The right kidney was normal in size and showed impaired cortical function and prompt drainage of radiotracer during the dynamic images; heterogeneous tracer uptake was noted in the right kidney mass. 18-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography images [Figure 4a] showed a large partially exophytic soft mass almost completely replacing the right kidney with infiltration of the renal pelvis. Coronal sections [Figure 4b and c] show defect in the left hemidiaphragm with herniation of the left kidney, spleen, and large bowel. Transaxial sections of lungs [Figure 4d] revealed FDG avid multiple soft tissue nodules in bilateral lungs with mild right pleural effusion, suggestive of metastases. The patient was referred to the Department of Medical Oncology for further management.
Figure 1.
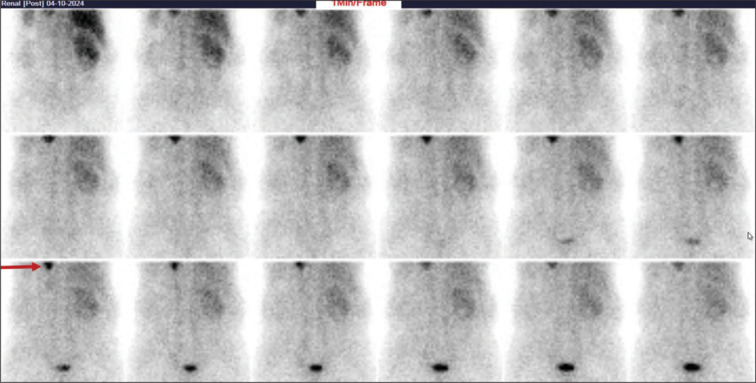
Renal dynamic images acquired in the posterior view after intravenous injection of 99m-Tcdiethylenetriaminepentaacetic acid shows heterogeneous cortical uptake in the right kidney. Left kidney is not visualized in the left renal fossa. However, a focal spot of tracer activity (arrow) is noted in the left upper aspect of the field of view
Figure 2.
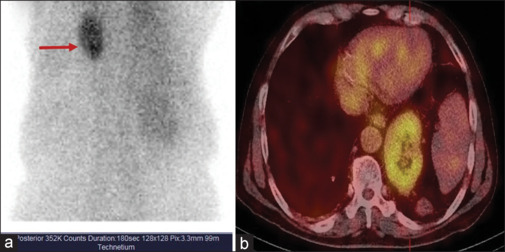
Static image in posterior view with increased field of view covering thorax and the abdomen (a) reveals an ectopic left kidney located in intrathoracic location (arrow). Single-photon emission computed tomography – computed tomography images (b) reveal elevated left hemi diaphragm with malrotated ectopic left kidney lying completely above the diaphragm in the left hemi thorax
Figure 3.

Repeat renal dynamic study processed images showed elevated background tracer activity. Left kidney is ectopic (intrathoracic) in location with non-obstructive drainage. Right kidney is normal in size with impaired cortical function and prompt drainage of radiotracer; heterogeneous tracer uptake noted in the right kidney mass
Figure 4.

18-Fluorodeoxyglucose positron emission tomography computed tomography images (a) shows a large partially exophytic soft mass almost completely replacing the right kidney with infiltration of the renal pelvis. Coronal sections (b and c) show defect in the left hemidiaphragm with herniation of left kidney, spleen and large bowel. Transaxial sections of lungs (d) reveals18 Fluorodeoxyglucose (FDG) avid multiple soft tissue nodules in bilateral lungs with mild right pleural effusion, suggestive of metastases
Discussion
Ectopic kidney in intra thoracic location is very rare and is one of the differential diagnoses for posterior mediastinal mass. Usually on conventional imaging such as USG abdomen, the kidney is not visualized. Dimercaptosuccinic acid (DMSA) renal scan is usually the first line of investigation in a case of a nonvisualized kidney on USG.[2] However, in our case, the USG abdomen incorrectly reported the left kidney as normal in location. The first case of the intrathoracic ectopic kidney was reported by Wolfromm using retrograde pyelography in the year 1940.[4] Upon thorough review of literature, only 200 cases have been published so far.[5,6] Possible etiologies for intrathoracic kidney include delayed closure or maldevelopment of the pleuroperitoneal membrane, accelerated ascent of the kidney, persistence of the nephrogenic cord, and effect of the developing liver and adrenal glands.[7] Pfister-Goedeke and Burnier classified four types of the intrathoracic kidney: (1) thoracic renal ectopia with eventration of the diaphragm (most common cause), (2) thoracic renal ectopia with diaphragmatic herniation, (3) traumatic rupture of the diaphragm with renal ectopia, and (4) thoracic renal ectopia with closed diaphragm.[8] Intrathoracic kidney shows male predominance and occurs on the left more commonly and in 10% of cases is bilateral.[9] The features of the thoracic kidney include a long ureter, rotational anomaly, medial deviation of the lower pole of the kidney, and anomalous high derivation of the renal vessel. However, the adrenal gland is located in a normal position in most cases. Intrathoracic kidneys are mostly reported to be functionally normal, with the stretched ureter providing good drainage, and unlike the low-lying kidney is less prone to infections.[2] In the majority of cases, treatment is not required, except in those associated with other anomalies such as vesicoureteric reflux and obstruction.[6] Ectopic intrathoracic kidney although an asymptomatic condition, requires a correct diagnosis as this information should be made available to the patient as well as the treating physician/surgeon to avoid unnecessary interventions. Nuclear medicine studies such as DMSA and 99mTc-DTPA renal scans play a crucial role in the diagnosis and evaluation of renal function in such cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflicts of interest
There are no conflicts of interest.
Funding Statement
Nil.
References
- 1.Donat SM, Donat PE. Intrathoracic kidney: A case report with a review of the world literature. J Urol. 1988;140:131–3. doi: 10.1016/s0022-5347(17)41506-0. [DOI] [PubMed] [Google Scholar]
- 2.Natarajan A, Agrawal A, Purandare N, Shah S, Rangarajan V. Rare case of thoracic kidney detected by renal scintigraphy. Indian J Nucl Med. 2016;31:219–21. doi: 10.4103/0972-3919.181863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ten Broek MR, Te Beek ET, Stuurman-Wieringa RE. 99mTc-MAG3 renography of intrathoracic renal ectopia. Clin Nucl Med. 2019;44:78–80. doi: 10.1097/RLU.0000000000002336. [DOI] [PubMed] [Google Scholar]
- 4.Wolfromm MG. Kidney position in right diaphragmatic eventration. Mem Acad Chirur. 1940;60:41–7. [Google Scholar]
- 5.Kian B, Kayedi M, Teimouri A. Intrathoracic kidney: A rare presentation of ectopic kidney. Radiol Case Rep. 2022;17:2795–7. doi: 10.1016/j.radcr.2022.05.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Navaratnarajah A, Barry V, Charif R. Bochdalek hernias associated with intrathoracic kidney: A case report and systematic review of outcomes including renal function. Clin Nephrol Case Stud. 2020;8:1–11. doi: 10.5414/CNCS109962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gupta A, Maheshwarappa RP, Jangid H, Meena ML. Ectopic intrathoracic kidney: A case report and literature review. Hong Kong J Nephrol. 2013;15:48–50. [Google Scholar]
- 8.Pfister-Goedeke L, Brunier E. Intrathoracic kidney in childhood with special reference to secondary renal transport in Bochdalek’s hernia. Helv Paediatr Acta. 1979;34:345–57. [PubMed] [Google Scholar]
- 9.Lee CH, Tsai LM, Lin LJ, Chen PS. Intrathoracic kidney and liver secondary to congenital diaphragmatic hernia recognized by transthoracic echocardiography. Int J Cardiol. 2006;113:E73–5. doi: 10.1016/j.ijcard.2006.04.021. [DOI] [PubMed] [Google Scholar]