

ABSTRACT
Fast food has become a common dietary choice worldwide, with significant health consequences. In low‐ and middle‐income countries (LMICs), particularly in Asia, the consumption of fast food has risen, yet research providing a comprehensive summary of fast food consumption patterns is limited. Therefore, this review consolidates evidence on the patterns and factors influencing fast food consumption in Asian LMICs. A comprehensive literature search was conducted using PubMed, Google Scholar, and references of relevant studies, covering peer‐reviewed articles published in English from January 1, 2011, to June 30, 2023. A total of 87 studies met the inclusion criteria, encompassing data from 178,554 individuals across 26 countries. The findings indicated a higher fast food consumption with a preference for Western fast food, such as pizza, burgers, fried chicken, French fries, and sandwiches, over local options. Key factors driving fast food consumption included taste, affordability, accessibility, mass media advertisement, restaurant environment, service quality, and family/peer influence. Furthermore, socioeconomic status, age, gender, and educational background influenced the consumption. For adults, factors like time constraints, lack of alternatives, employment status, health consciousness, stress, and food quality and hygiene were important. The increasing presence of fast food in the Asian diet highlights the need for comprehensive policies to curb this trend and protect public health.
Keywords: fast food, low‐ and middle‐income countries (LMICs), Asia
This review highlights the high prevalence and frequent consumption of fast food, particularly western items such as pizza, burgers, fried chicken, French fries, and sandwiches, among populations in Asian LMICs. Factors influencing fast‐food consumption include taste, affordability, availability, mass media advertising, restaurant environment, service quality, family and peer influence, socioeconomic status, demographic characteristics (age, gender, education, employment), limited time for cooking, lack of healthy alternatives, health consciousness, stress, and concerns about food quality and hygiene.

1. Introduction
The dietary landscape of Asian countries has undergone a remarkable transformation over recent decades, marked by a shift from traditional diets to the adoption of the Western diet. This transition is characterized by an increased consumption of fast food, animal products, oil, sugar‐sweetened and processed food, and ultra‐processed food [1, 2, 3]. Such dietary shifts are further reinforced by the rapid proliferation of fast food establishments across Asia [3], contributing significantly to the nutrition transition observed not only in developed nations but also in low‐ and middle‐income countries (LMICs) [4].
The term “fast food” is loosely defined, originating from its introduction by Merriam‐Webster, which defines it as food that can be swiftly prepared and served [5]. This category encompasses a range of mass‐produced food items tailored for rapid preparation and distribution, commonly retailed by restaurants, concession stands, and convenience stores [6]. According to the USDA, fast food restaurants are establishments where customers make payment for their food before it is served [7]. Furthermore, fast food is defined by the Foodbook study as food prepared in restaurants that do not offer table service but instead offer counter‐service, drive‐through, or carry‐out alternatives [7]. Fast food is one of the largest components of the food industry. The rapid growth of fast food in Asia can be attributed to various factors, such as unregulated food marketing, technological advancements in the food industry, globalization, urbanization, trade liberalization, and economic progress [3, 8, 9, 10, 11]. Originating from the United States, the fast food culture has transcended borders to become a global phenomenon, even reaching smaller towns in Asia. This expansion is not solely driven by multinational giants like McDonald's, KFC, and Pizza Hut, but also by domestic enterprises imitating the products and operational models of their foreign counterparts [3]. The international appeal of fast food is also evident in the success of chains like McDonald's and Yum!, which generate significant sales overseas, with 65% and 50% of their sales coming from international markets, respectively [5].
Fast food is characterized as larger in portion size, with palatability that typically contains higher levels of refined carbohydrates, sugars, fats, saturated fats, trans fats, cholesterol, and salt, along with a lower level of essential micronutrients and dietary fibers [12, 13, 14, 15]. Due to its high energy density and glycemic load, fast food consumption has been associated with weight gain and obesity [16]. Notably, overweight/obesity are key risk factors for a range of non‐communicable diseases (NCDs), including cardiovascular diseases, various metabolic syndromes, liver disease, osteoarthritis, sleeping disorders, certain types of cancers, and mental illness, contributing to a greater economic burden [17, 18]. The increasing trend of overweight/obesity has become a serious issue in LMICs [19]. This region contains about half of the world's stunted and overweight children, experiencing the double burden of malnutrition [20], and one out of every three LMICs is struggling with the double burden of malnutrition [21]. In Asia, the highest number of stunted and overweight children has been observed, exacerbating the situation [20]. Higher fast food consumption leads to a higher health burden. The consumption frequency can be a predictor of their diet and health status, as higher consumption of fast food is related to higher BMI [22] and lower diet quality [13].
In Asia, there is a scarcity of comprehensive reviews on fast food consumption. Although two reviews have covered certain Asian countries, none have specifically focused on LMICs in Asia, encompassing both children/adolescents and adults [23, 24]. Therefore, this review aims to gather scientific evidence to provide insights into fast food consumption patterns and their key driving factors in Asian LMICs.
2. Methods
2.1. Literature Search Approach
Fast food is defined differently by various sources. In Asia, although many street foods or junk foods are considered fast food, not all of them are classified as such [5]. Therefore, a comprehensive search was conducted in PubMed, which was chosen due to its extensive coverage of public health and nutrition‐related studies. To supplement this, Google Scholar was searched for gray literature, and the reference lists of relevant articles were screened to capture additional studies. The search strategy utilized a combination of MeSH and non‐MeSH terms, including fast food, junk food, Western food, ultra‐processed food, street food, unhealthy food, and unhealthy diet, as these terminologies were closely related to defining fast food (Table S1).
2.2. Inclusion and Exclusion Criteria
This review included original, peer‐reviewed, full‐text primary articles written in English and published between January 1, 2011, and June 30, 2023, focusing on LMICs in Asia. The studies included in this review met the following criteria based on the PECO framework:
Population (P): Individuals from LMICs in Asia;
Exposure (E): Consumption of fast food;
Comparison (C): Not applicable;
Outcome (O): Fast food consumption frequency or patterns, preferred or commonly consumed fast food items, and influential factors behind consumption.
Interventional studies, qualitative studies, and reviews were excluded. All identified studies were categorized into two groups based on age: children/adolescents and adults. Studies that did not specify the age or could not be categorized into either age group were excluded.
2.3. Data Extraction and Analysis
All records from the databases were downloaded and uploaded to EndNote for title and abstract screening. All selected abstracts were then evaluated for inclusion criteria, and key information from the included studies was extracted using an Excel data extraction table. The extracted data included author, publication year, location, participants, study design, sample size, gender, age, sample characteristics, fast food consumption frequency, influencing factors, and preferred fast food items.
2.4. Definitions
For the fiscal year 2023, the World Bank classified 33 countries as LMICs in Asia based on gross national income: Afghanistan, Bangladesh, Bhutan, Cambodia, China, India, Indonesia, Iran, Iraq, Jordan, Kazakhstan, Laos/Lao PDR, Lebanon, Malaysia, Maldives, Mongolia, Myanmar, Nepal, Pakistan, Philippines, Russian Federation, South Korea, Sri Lanka, Syria, Tajikistan, Thailand, Timor‐Leste, Turkey, Turkmenistan, Uzbekistan, Vietnam, West Bank, and Yemen [25].
3. Results
A total of 3338 potential studies were identified in the electronic databases. After screening titles and abstracts, a total of 180 studies were considered for full‐text review. However, 92 of these did not meet the inclusion criteria. Thus, a total of 87 studies were included in this review, among which two were multi‐country studies. A summary of the process is detailed in Figure 1, and an overview of the 87 identified studies can be found in Table S2. These studies covered 26 countries from 33 LMICs in Asia, extracting information for 178,554 individuals.
FIGURE 1.
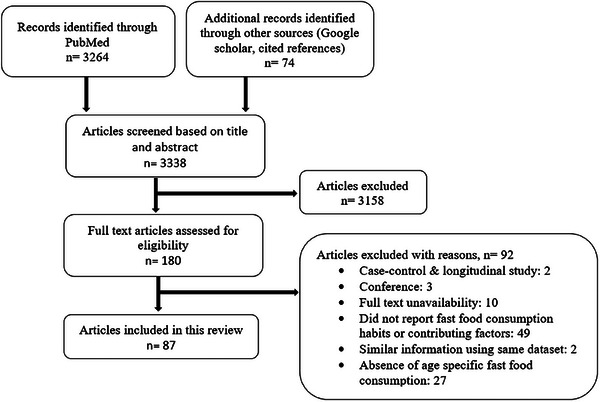
Flowchart of the study selection procedure.
3.1. Fast Food Consumption Frequency
The studies examined fast food consumption across various timeframes, including daily, weekly, and monthly intervals. The findings showed significant regional variations in consumption patterns, with frequent consumption reported.
3.1.1. Fast Food Consumption Frequency Among Children/Adolescents
Fast food consumption among children and adolescents was widespread across Asian LMICs, though the frequency varied significantly by country, age, gender, and socioeconomic status. Studies from India, Pakistan, Nepal, and Bhutan indicated particularly high consumption rates. In India, approximately 98% of school‐going students consumed fast food, with 85% doing so regularly and over 20% consuming it more than three times per week [26, 27, 28, 29, 30]. A similar trend was observed in Pakistan, where nearly 96% of school‐aged children consumed fast food weekly [31], and 54% were frequent consumers [32]. In Nepal, three‐fourths of adolescents consume fast food weekly, with one‐third consuming it daily [33], whereas in Bhutan, around 90% consume fast food weekly [34].
Fast food consumption appeared to increase with age in several countries, including Malaysia, Iraq, and Bangladesh. In Malaysia, fast food intake was significantly higher among adolescents, with rates ranging from 48% to 83%, whereas younger children consumed fast food far less frequently [35, 36, 37, 38]. In Iraq, half of the primary school students consumed fast food weekly [39], a figure that rose to 57% among adolescents [37]. A similar pattern was observed in Bangladesh, where 68% of college‐going adolescents consumed fast food weekly, compared to 54% among younger school‐aged adolescents [37, 40].
In Iran, fast food consumption varied widely depending on socio‐demographic factors. Although some studies reported consumption rates as high as 70% among adolescents [41], others found much lower rates (15%–27%) [42, 43, 44]. Interestingly, in some Iranian studies, sweet snacks were preferred over fast food, particularly among girls [43]. Westernization of dietary patterns shaped fast food consumption in China, where 52% of children and adolescents consumed Western fast food weekly, whereas 44% preferred local Chinese fast food options [45].
In other countries, weekly fast food consumption among school‐going adolescents was also high: Thailand (82%) [37], Sri Lanka (43%–80%) [46, 47], Lebanon (77%) [47], Timor‐Leste and Afghanistan (65%) [37], Indonesia (56%) [37], Mongolia (55%) [37], the Philippines (49%) [37], and Syria (43%) [37]. However, consumption was considerably lower in the Maldives, Yemen, and Vietnam, where weekly consumption was around 35% [37, 47].
Gender differences in fast food consumption varied across countries. In Pakistan, high school and college girls consume more frequently than boys [48], whereas among younger children, boys tend to have higher consumption [49]. Similar trends were observed in Iraq [50], China [45], Bangladesh [51], Syria [52], and Vietnam [53], where boys consumed more than girls. However, in Malaysia, girls consumed more fast food than boys [38] (Table 1). Deatils of the consumption patterns can be found in Table S3.
TABLE 1.
Fast food consumption frequency among children and adolescents.
| Country | Fast food consumption frequency |
|---|---|
| Afghanistan | 1–3 days/week: 52.2%, 4–7 days/week: 10.8%, ≥1 times/week: 65%, mean day/week: 2.4 [37] |
| Bangladesh | Once/week: 53.2%–68.3%, 1–2 days/week: 28%, 1–3 days/week: 35.9%–42.9%, ≥3 days/week: 26%–64.1%, mean day/week: 2.4, male consumed more than female [37, 40, 51] |
| Bhutan | Weekly consumption: 90.4% [34] |
| China | Weekly consumption: 32.4%, Western fast food/week: 51.9%, Chinese fast food/week: 43.6%, mean consumption/week: 0.6 to 1.5, male was frequent consumer than female [37, 54, 55, 56] |
| India | Once/week: 28.8%–62.7%, 1–2 times/week: 44.2%, 2 times/week: 15.4%–90%, 1–3 times/week: 62.6%, ≥2 times/week: 21.9%–57.5%, ≥3 times/week: 38.8%–90.4%, 4–7 times/week: 22.4%, occasionally: 17%, fast food preference and habit: 98% [26, 27, 28, 29, 30, 57, 58] |
| Indonesia | 1–3 days/week: 45.3%, 4–7 days/week: 10.5%, ≥1 times/week: 56.5%, mean day/week: 2.3 [37] |
| Iran | Daily: 2.4%–10.6%, once/week: 22.7%–69.8%, 1–2 items/week: 24.2%, 2 times/month: 26.9%, 1–3 times/week:12.5%, ≥3 times/week: 2.7%–10%, monthly: 26.3%–43.9%, seasonally: 13.8%, yearly: 10.8% [41, 42, 43, 44, 59] |
| Iraq | Once/week: 34.6%–56.5%, 1–3 days/week: 45.3%, 2–3 times/week: 12.3%, >3 days/week: 10.5%–37% (male: 37%, female: 25%), daily: 1.8%, mean day/week: 2.3–3 (male: 3, female: 2.4) [37, 39, 50] |
| Maldives | ≥1 times/week: 35.1% [47] |
| Mongolia | 1–3 days/week: 37.7%, 4–7 days/week: 17.4%, ≥1 times/week: 55.1%, mean day/week: 2.6 [37] |
| Nepal | Once/week: 22.2%, 2 times/week: 24.8%, >2 times: 19.3%–89.6%, ≥1 times/week: 75.3%, daily: 10.3%–33.8%, monthly junk foods: 60.3% [33, 47, 60] |
| Pakistan | 1–2 times/week: 29.5%–72.9%, 1–3 times/week: 44%–46%, ≥3 times/week: 13.4%–23.3%, daily: 5.4%–8%, frequent consumer: 54%, occasionally: 57%, mean consumption/week: 2.1 times for male and 2.5 times for female, everyone consumed fast food [31, 32, 48, 49, 61] |
| Philippines | 1–3 days/week: 47.8%, 4–7 days/week: 4.1%, ≥1 times/week: 49%, mean day/week: 1.9 [37] |
| Sri Lanka | ≥1 times/week: 42.8%, once/week: 60%,1–2 times/ month: 20%, daily: 20% [46, 47] |
| Syria | 1–3 times/week: 37.8%–85.8%, 4–7 days/week: 5%–14.2%, ≥1 times/week: 42.5%, mean day/week: 1.8, male consumed more frequently than female [37, 52] |
| Thailand | 1–3 days/week: 36.8, 4–7 days/week: 43.3, ≥1 times/week: 81.8%, mean day/week: 4.1 [37] |
| Timor‐Leste | 1–3 days/week: 55.4%, 4–7 days/week: 11.8%, ≥1 times/week: 64.9%, mean day/week: 2.4 [37] |
| Vietnam | 1–3 days/week: 24.4%, 2–6 times/week: 1.6%, 4–7 days/week: 5.3%, ≥1 times/week: 30.3%, mean day/week: 1.7, male consumed more than female [37, 53] |
| Yemen | ≥1 times/week: 34.5% [47] |
3.1.2. Fast Food Consumption Frequency Among Adults
The frequency of fast food consumption among adults varied widely across countries. Several studies reported high consumption frequencies in Southeast Asia, particularly among undergraduate students, with India, Bangladesh, Pakistan, Sri Lanka, Malaysia, and Vietnam showing strikingly high numbers. In India, university students reported higher consumption rates (81%–95%) weekly, with a significant proportion consuming it ≥3 times/week [62, 63, 64, 65, 66]. Similarly, in Bangladesh, 94% of university students preferred fast food and showed a clear preference for foreign fast food chains over local ones [67]. A wide variation in weekly fast food consumption among university students was also found, ranging from 54% to 98% in Bangladesh [68, 69, 70, 71]. Furthermore, social media users (e.g., Facebook) had higher fast food intake in Bangladesh [72]. Among Pakistan's university students, consumption rates range from 58% to 91%, with a significant portion of female students consuming fast food regularly [73, 74, 75, 76]. In Sri Lanka, 98% of university students consumed fast food weekly, and half of them consumed it daily [77]. In Malaysia, studies showed a wide range in consumption, from 23% to 99% [78, 79]. In Vietnam, 42% of university students consumed fast food 1–2 times/week [80].
Fast food consumption also followed a higher trend among university students in the Middle East, such as in Syria (74% weekly) [81], Jordan (59% ≥ 2 times/week) [82], Turkey [83], and the West Bank (83% ≥ 3 times/week) [84]. In Iran, weekly fast food consumption varied from 11% to 69% [85, 86, 87, 88, 89].
Among working adults, fast food consumption was generally lower compared to students. For example, in Cambodia, only 63% of working individuals reported consuming fast food in the past month [90], whereas in Malaysia, consumption was significantly lower in low‐income areas [91, 92]. South Korea showed the lowest fast food consumption rate, with only 10% consuming it regularly [93].
Gender disparities in fast food consumption were evident in several regions. In Bangladesh, Turkey, Iran, and the West Bank, males were more likely to consume fast food than females. However, in Malaysia, females tend to consume fast food more frequently than males (Table 2). Details of the consumption patterns are avialable in Table S4.
TABLE 2.
Fast food consumption frequency among adults.
| Country | Fast food consumption frequency |
|---|---|
| Bangladesh |
Once/week: 40.8%–50.5%, 1–2 times/week: 24%–27%, ≥4 times/week: 4.6%, ≥1 times/week: 54%–98.5% (male: 56% and female: 44%), daily: 15%, once/month: 20.1%–25.2%, 2–3 times/month: 29%, 1–3 times/month: 44.5%–48.1%, ≥3 times/month: 35.2%, ≥4 times/month: 14%–45.6% [67, 68, 69, 70, 71, 72, 94, 95]. Fast food preference: 71%–94.2%, preference of foreign fast food restaurants 60.3% vs. local fast food restaurants 39.7% [67], male preferred fast food over female [69] |
| Cambodia | Monthly fast food consumption: 62.7% [90] |
| India |
<1 time/week: 6.8%–10%, Once/week: 30.8%, 1–2 times/week: 42.8%–80%, 3–4 times/week: 13.3%–23.7%, ≥3 times/week: 19.6%–74.6%, daily: 19.1%–44.6%, occasionally: 18.1%–22.7% [62, 63, 64, 65, 66, 96]. |
| Iran | ≥1 times/week: 10.7%–31%, ≥2 times/week: 50%–52%, once/month: 8%–15.9%, 1–2 times/month: 20.9%, 2 times/month: 11.8%–25.6%, 1–3 times/month: 29.1%, monthly fast food consumption: 72.4% (males: 80.7% vs. females: 67.4%), mean consumption/month: 2.7 times [85, 86, 87, 88, 89, 97, 98] |
| Jordan | ≥2 times/week: 59.4% [82] |
| Malaysia |
≥1 times/week: 15%–34% (male: 23.5 vs. female: 34%), 1–5 times/week: 99%, ≥4 times/month: 24.3%, <4 times/month: 75.7% [78, 79, 91, 92]. 93% preferred fast food [79] |
| Pakistan | ≥1 times/week: 57.4%–91.2%, weekends: 26.7%, occasionally: 48.71% [74, 75, 76, 99], 64%–94% consumed fast food [73, 76] |
| South Korea | 10% habituated to fast food [93] |
| Sri Lanka | Once/week: 11%–16.7%, 2–3 times/week: 21%, 4–6 times/week: 12%, daily: 54%, 1–2 times/month: 66.7%–83.3% [46, 77] |
| Syria | Once/week: 44.5%, 2 times/week: 17.7%, ≥3 times/week: 11.4% [81] |
| Turkey | Female vs. male–once/15 days: 40.6% vs. 38.6%, 3 times/week: 19.8% vs. 28.4%, 5 times/week: 11.5% vs. 5.6%, once/month: 28.2% vs. 27.3% [83] |
| Vietnam | 1–2 times/week: 42%, 1–2 times/month: 27% [80] |
| West Bank | 12 times/week: 30.9%, 3 times/week: 52.4%, male consumed more fast food than female [84] |
3.1.3. Factors Influencing Fast Food Consumption Among Children/Adolescents
Table 3 describes the factors that influenced children and adolescents to consume fast food. Taste, convenience, availability, peer influence, and media exposure emerged as dominant factors influencing fast food consumption in this study. However, regional differences were evident, with parental control and family culture playing a stronger role in Asian countries like India [100], China [101], Indonesia [102], and Iran [41].
TABLE 3.
Factors influencing the consumption of fast food among children and adolescents.
| Factors | Country | References | Factors | Country | References |
|---|---|---|---|---|---|
| Taste | Bangladesh, India, Iran, Pakistan | [31, 44, 51, 57, 103] | Urbanization | India | [103] |
| Accessibility or convenience | Bangladesh, China, Iran, Pakistan | [32, 44, 51, 101] | Inexpensive | Iran | [44] |
| Advertisements and media influence | India, Indonesia, Iran, Pakistan | [31, 41, 102, 103] | Evening meals with family members | India | [100] |
| Availability | India, Nepal | [60, 100, 103] | Habit | Iran | [104] |
| Parental control or mediation | India, Indonesia, Pakistan | [31, 100, 102] | Past behavior | Iran | [104] |
| Family and peer influences | Iran, Nepal | [41, 60, 104] | Ethnicity | Malaysia | [38] |
| Proximity of fast food outlets | Iran, Sri Lanka | [41, 44, 46] | Location of schools | Malaysia | [38] |
| Educational qualification | Bangladesh, Sri Lanka | [46, 51] | Public school | Nepal | [60] |
| Gender | Bangladesh, Malaysia | [38, 51] | Nuclear family | Nepal | [60] |
| Socioeconomic circumstances | Bangladesh, Iran | [44, 51] | Living with parents | Nepal | [60] |
| Educational level of caregiver | China, India | [100, 101] | At the time of traveling, reading | Nepal | [60] |
| Variety or diversity | India | [57, 103] | Friends outgoing or gathering | Pakistan | [31] |
| Quick service | India | [57, 103] | Lack of time to cook | Pakistan | [31] |
| Income | India, Pakistan | [31, 100] | Social and environmental enjoyment | Pakistan | [32] |
| Age | Malaysia, Sri Lanka | [38, 46] | Hunger and satiety | Pakistan | [32] |
| Ideology of caregiver | China | [101] | Employment status | Sri Lanka | [46] |
| Brand value | India | [103] |
In India, the variety of fast food items, brand value, quick service, family income, and urbanization were driving forces to consume fast food [100, 103]. Children and adolescents in Nepal who studied in public schools and lived in small families with parents consumed more fast food. Furthermore, they consumed fast food while traveling, reading books, or staying in school [60]. Lack of parental involvement in cooking had an impact in Pakistan [31]. In Pakistan, some children and adolescents consumed fast food when they were hungry or going out with friends [31]. In Iran, adolescents’ behavior, habits, and lifestyle were responsible for their fast food consumption [104]. In Malaysia, the age of children and adolescents, their ethnicity, and the location of the educational institution played an important role in consuming fast food [38].
3.1.4. Factors Influencing Fast Food Consumption Among Adults
The key factors that explained the fast food consumption among adults were described in Table 4. In this study, taste, affordability, convenience, lack of time to cook, restaurant environment, and family/peer influences emerged as the most consistent drivers of fast food consumption. However, many other cultural, social, and economic factors influenced fast food consumption, which varied by region.
TABLE 4.
Factors influencing the consumption of fast food among adults.
| Factors | Country | References |
|---|---|---|
| Taste | Bangladesh, India, Indonesia, Iran, Sri Lanka, Turkey | [62, 65, 67, 69, 70, 77, 83, 88, 92, 95, 96] |
| Price | Bangladesh, Indonesia, Pakistan, Sri Lanka, Vietnam | [67, 70, 76, 77, 80, 92, 99] |
| Accessibility or convenience | Bangladesh, India, Pakistan, Sri Lanka, Thailand | [46, 62, 67, 70, 76, 106] |
| Lack of time to cook | India, Indonesia, Jordan, Pakistan, Turkey | [65, 78, 82, 83, 96, 99] |
| Environment of the restaurants | Bangladesh, Iraq, Pakistan | [67, 76, 99, 105] |
| Family and peer influences | Bangladesh, India | [69, 70, 95, 96] |
| Sociability | Bangladesh, Turkey | [70, 72, 83] |
| Food quality | Bangladesh, Iraq, Pakistan | [67, 99, 105] |
| Pocket‐friendly or inexpensive | Bangladesh, Iran, Turkey | [70, 83, 88] |
| Fun | Indonesia, Iran, Pakistan | [78, 87, 99] |
| Service quality | Bangladesh | [67, 72] |
| Availability | Bangladesh, Indonesia | [69, 92] |
| Quick service | Bangladesh, Iran | [70, 88] |
| Lack of alternatives | Bangladesh | [69, 70] |
| Habit | Bangladesh, Pakistan | [69, 99] |
| Friends outgoing or gathering | Bangladesh, Indonesia | [78, 95] |
| Recreational activity | Bangladesh, Iraq | [95, 105] |
| Stress relief | Bangladesh, India | [95, 96] |
| Family culture | Iran, Pakistan | [88, 99] |
| Advertisements and media influence | Iran, Iraq | [88, 105] |
| Health consciousness | Pakistan, Vietnam | [80, 99] |
| Income | Pakistan, Thailand | [99, 106] |
| Food safety and hygiene | Sri Lanka, Vietnam | [77, 80] |
| Age | Sri Lanka, Thailand | [46, 106] |
| Educational qualification | Sri Lanka, Thailand | [46, 106] |
| Employment status | Sri Lanka, Thailand | [46, 106] |
| Personal aspects | Bangladesh | [72] |
| Payment system | Bangladesh | [67] |
| Location | Bangladesh | [67] |
| Free Wi‐Fi facility | Bangladesh | [95]) |
| Emotion | India | [62] |
| Variety or diversity | India | [96] |
| Home delivery services | India | [96] |
| Decoration of fast food | India | [96] |
| Tasteless hostel meal | India | [65] |
| Knowledge | Iran | [97] |
| Subjective norms | Iran | [97] |
| Brand reputation | Pakistan | [99] |
| Hunger and satiety | Pakistan | [76] |
| Gender | Thailand | [106] |
In countries like Bangladesh and Pakistan, people consumed fast food out of habit or pleasure [69, 76, 78, 87, 99] and during social gatherings [70, 72, 78, 95]. Family culture played a role in developing fast food habits in regions like Iran, Malaysia, and Pakistan [78, 88, 99]. Furthermore, brand value and reputation were considerable reasons in Pakistan [99]. Among Bangladeshi adults, consumption was affected by a lack of alternatives to fast food [69, 70], availability of modern recreation facilities, Wi‐Fi, and mode of payment [95]. Some people consume fast food as a means of stress relief in India and Bangladesh [95, 96]. People living in Iran and Iraq were influenced by mass media advertisements [88, 105]. Besides, knowledge, subjective norms, perception of health benefits, and disorganized student life also played important roles in Iran [97]. People in Iraq were persuaded to take their kids to a fast food restaurant for entertainment. Playful surroundings and the availability of room for kids to play were therefore seen as important considerations [105]. Many Pakistanis ate fast food when they were hungry [76]. In Thailand, fast food consumption varied by age, educational level, and occupation type of the customer [106].
3.2. Commonly Consumed Fast Food Items in LMICs of Asia
Table 5 demonstrates the most commonly consumed fast food items in LMICs in Asia. Pizza, burgers, fried chicken, and sandwiches were widely consumed across most countries. Furthermore, biscuits, noodles, chips, cake, pastries, hotdogs, doughnuts, spaghetti, and sausages were frequently reported in India, Nepal, Cambodia, Vietnam, and Malaysia. Alongside these, country‐specific consumption patterns were also observed.
TABLE 5.
Variety of consumed fast food items in LMICs of Asia.
| Fast food items | Country | References |
|---|---|---|
| Pizza | India, Iran, Nepal, Pakistan, Bangladesh, Iraq, Malaysia, Turkey, Vietnam | [27, 30, 31, 44, 65, 66, 69, 76, 80, 83, 95, 96, 98, 100, 105, 107, 108, 109, 110, 111] |
| Burgers | India, Iran, Nepal, Pakistan, Bangladesh, Iraq, Malaysia, Turkey, Vietnam | [27, 30, 31, 65, 66, 69, 76, 80, 83, 88, 96, 100, 105, 109, 110, 111] |
| Fried chicken | India, Bangladesh, Pakistan, Iran, Malaysia, Vietnam | [30, 31, 69, 76, 80, 96, 98, 109] |
| Sandwiches | Iran, Pakistan, Malaysia, Vietnam | [31, 44, 76, 80, 88, 98, 109] |
| Noodles | India, Nepal, Bangladesh | [30, 33, 69, 100, 110] |
| Biscuits | India, Nepal, Cambodia | [33, 90, 100, 107, 110] |
| Chips | India, Nepal, Vietnam | [33, 80, 100, 110] |
| Momo | Nepal, India | [33, 65, 96, 110] |
| Chowmein | Nepal, India | [33, 65, 108, 110] |
| French fry | Pakistan, Malaysia | [32, 66, 76, 109] |
| Cake | India, Cambodia, Malaysia | [30, 90, 109] |
| Pastry | India, Malaysia, Sri Lanka | [77, 107, 109] |
| Samosa | India, Bangladesh | [27, 95, 100] |
| Hotdog | Iran, Cambodia, Malaysia | [44, 90, 109,] |
| Doughnut | Nepal, Malaysia, Cambodia | [90, 109, 110] |
| Sausage | Cambodia, Malaysia, Vietnam | [80, 90, 109,] |
| Spaghetti | Cambodia, Malaysia, Vietnam | [80, 90, 109] |
| Chocolate | India | [27, 107] |
| Cookies | India, Nepal | [100, 110] |
| Wafer | India, Bangladesh | [95, 100] |
| Pav bhaji | India | [100, 108] |
| Ice cream | Nepal, Malaysia | [109, 110] |
| Fries | Pakistan, Nepal | [109, 110] |
| Shawarma | Pakistan, Iraq | [31, 105] |
| Meat ball toast | Cambodia, Malaysia | [90, 109] |
| Patties | India, Sri Lanka | [77, 108] |
| Rolls | India, Sri Lanka | [77, 96] |
| Puffs | India | [30] |
| Indian sweet | India | [107] |
| Maggi | India | [107] |
| Kachori | India | [107] |
| Namkeen | India | [107] |
| Fried rice | India | [107] |
| Vada pav | India | [107] |
| Chinese bhel | India | [107] |
| Pakora | Nepal | [33] |
| Panipuri | Nepal | [33] |
| Candies | Nepal | [33] |
| Fried food | Nepal | [110] |
| Daalmoth | Nepal | [110] |
| Papad | Nepal | [110] |
| Grill | Cambodia | [90] |
| Roast | Cambodia | [90] |
| Steak | Cambodia | [90] |
| Pasta | Cambodia | [90] |
| Macaroni | Cambodia | [90] |
| Chole bhature | India | [108] |
| Golgappa | India | [108] |
| Biryani | India | [96] |
| Kebab | Iraq | [105] |
| Falafel | Iraq | [105] |
| Meat dough | Iraq | [105] |
| Nuggets | Malaysia | [109] |
| Waffle | Malaysia | [109] |
| Pie | Malaysia | [109] |
| Porridge | Malaysia | [109] |
| Wade | Sri Lanka | [77] |
| Fish bun | Sri Lanka | [77] |
| Lahmacun | Turkey | [83] |
In Bangladesh, adults consumed noodles most frequently [69]. Cambodian adults usually consumed grilled pork, bacon, ham, roast, steak, meat ball, toast, pasta, macaroni, or spaghetti [90]. In India, traditional items such as chole bhature, kachories, pakoras, pav bhaji, panipuri, golgappa, biryani, and namkeen were popular [96, 107, 108]. Furthermore, sweets, Maggi, patties, rolls, and puffs were commonly consumed in India [27, 30, 96, 107, 108]. The most consumed fast food items among Iraqi adults were kebabs, shawarma, falafel, and meat dough [105]. Among Malaysian adults, ice cream, nuggets, meat balls, waffles, pie, and porridge were popular [109]. Popular fast food items among children/adolescents in Nepal include pakora, panipuri, ice cream, fried food, daalmoth, and fries [33, 110]. Furthermore, rolls, wade, fish buns, and patties were frequently consumed in Sri Lanka [77]. Vietnamese people prefer salad [80]. In Nepal and India, noodles, chocolate and candies, momo, and chowmein were also popular fast food items [27, 30, 33, 65, 100, 107, 108, 110]. Several studies in Bangladesh and India reported the consumption of samosas and wafers [27, 95, 100].
4. Discussion
This review is the first to offer a comprehensive overview of fast food consumption patterns in Asian LMICs over the past decade. The findings revealed a substantial rise in fast food consumption across two different age groups, highlighting a significant dietary shift in the region. Furthermore, this review identified the key driving factors influencing fast food consumption and delineated the spectrum of preferred fast food items.
The review identified that more than three‐quarters of children/adolescents frequently consumed fast food (at least once a week) in India, Pakistan, Nepal, Bhutan, Thailand, Lebanon, Syria, and Malaysia. Furthermore, the fast food consumption rate was found to be higher in the rest of the countries. These findings were corroborated by a study among adolescent girls in LMICs, where 75% reported weekly consumption [112]. However, this rate was slightly lower compared to a study across 54 LMICs, where around 55% of adolescents consumed fast food weekly, with a pooled prevalence of 57% in the Southeast Asia region [37]. Among adults, fast food consumption varied from 42% to 100% weekly in countries like Bangladesh, India, Pakistan, Sri Lanka, Malaysia, Jordan, Vietnam, Syria, and the West Bank. Similarly, higher consumption was noted among young adults in Kuwait, where 82% consumed fast food two or more times weekly [113], and in Singapore, where 71% indulged in Western fast food weekly [114]. In South Korea and China, consumption rates were lower compared to other LMICs. Despite a general trend toward increasing fast food consumption in China, its expansion is still limited [115]. This might be due to the implementation of laws and regulations and parental concerns about a healthy diet in China [10, 38] as well as the promotion the traditional Korean diet in South Korea [116].
This review found that the prevalence of fast food consumption was more pronounced among adults than children/adolescents. Several studies conducted in European countries and Australia have identified comparable trends, where takeaway food consumption was found to be increased from adolescence to adulthood, with high fast food consumption observed between the ages of 18 and 45 years [117, 118, 119, 120, 121]. Adults typically possess greater autonomy and income sources, which are positively associated with fast food consumption. Furthermore, their engagement in income‐generating activities, coupled with time constraints, often compelled them to consume fast food [22].
Several studies suggested that the most preferred fast food items were pizza, burgers, French fries, sandwiches, shawarma, fried chicken, kebabs, sausages, and noodles [4, 113, 122, 123, 124], and the findings presented here agree with this review. Though local fast food constituted a larger share of fast food items in India, Nepal, Sri Lanka, and Turkey, Western fast food was consumed more frequently. The increased consumption of Western fast food can be attributed to the rapid rise of modern food retail outlets, including supermarkets, restaurants, and convenience stores. Over the past 15 years in Asia and the Pacific region, these modern outlets have experienced growth rates ranging from 14% to 1243% across various countries. This expansion has driven a significant rise in the sales of ultra‐processed food [125].
The unparalleled economic growth and urbanization in Asian countries have reshaped living patterns, with half of the population now residing in urban areas [125]. The concurrent trends of trade liberalization and open markets have made unhealthy fast food more accessible. Even a healthy diet is costlier than an unhealthy diet in Asia [4]. Nearly 1.9 billion people, constituting 44% of the population in Asia and the Pacific, struggle to afford a nutritious diet, with Southern Asia facing an even more substantial challenge, with 70% of the population unable to afford a healthy diet. Consequently, a large portion of people rely on processed or highly processed foods due to their ready availability and cheaper nature [125]. Besides, millions of dollars are invested in Asia to popularize fast food [37]. Many driving factors are responsible for this kind of popularity of fast food. With consistent results, the literature suggested its lucrative features, including taste, appearance, convenience, accessibility, availability, and inexpensiveness, for this fast food culture [113, 126]. More women are involved in economic activities, and long working hours compel them to consume this convenient fast food due to limited time to cook [127]. However, advertisements, food marketing, and discounts on price influenced people to consume [12]. Although many people visited fast food restaurants to socialize with friends and family members [126]. Family income, restaurant milieu, hygiene, and food safety were also some concerning issues in choosing fast food restaurants [128].
In this review, some studies suggested gender variation in fast food consumption, whereas others did not. In agreement with the literature, our review found that males consumed more fast food in Bangladesh, China, Iraq, India, Iran, Jordan, Malaysia, Pakistan, Syria, Turkey, Vietnam, and the West Bank [117, 120, 129]. However, findings from other studies in India, Pakistan, and Malaysia showed that females consumed more. Whether the consumption among females is more or less than that of males, they are more susceptible to overweight, obesity, and micronutrient deficiencies. The increased risk to females is likely due to a sedentary lifestyle and lower basal metabolic rate compared to males [22].
The findings of this review highlighted the urgent need for policy interventions to address the growing fast food culture in LMICs. Governments should implement public health campaigns to raise awareness about the health risks associated with fast food consumption. Additionally, regulatory measures such as taxation on unhealthy food, subsidies for nutritious alternatives, and stricter marketing restrictions—especially targeting children and adolescents—could help mitigate the rising prevalence of diet‐related diseases [11, 37, 130]. Policies should also encourage food reformulation to reduce harmful ingredients and improve the nutritional profile of fast food items. Strengthening food safety regulations and monitoring the nutritional composition of fast food products and front‐of‐pack labeling to highlight unhealthy nutrient content can further support healthier food environments [130]. Given the increasing role of modern retail outlets and fast food chains, it is essential for policymakers to collaborate with the food industry to foster healthier eating environments. Urban planning strategies should also be designed to enhance access to affordable and nutritious food options. At the same time, workplace and institutional policies should encourage the availability of healthier meal alternatives, aligning with broader public health goals.
Despite the growing body of research on fast food consumption in LMICs across Asia, significant gaps remain. Most available studies are cross‐sectional, limiting the ability to establish causality between fast food consumption and health outcomes. Future research should prioritize longitudinal studies to assess the long‐term effects of fast food consumption on obesity, NCDs, and overall dietary patterns. Moreover, qualitative research is needed to explore the socio‐cultural and psychological factors driving fast food consumption. Insights into consumer motivations, as well as the role of peer and family influences, will help to design more effective behavioral change interventions. There is a lack of research examining the impact of government regulations on fast food consumption patterns. More research is needed to determine the impact of these interventions on consumer behavior and health outcomes. Additionally, limited data exist on the nutritional quality of commonly consumed fast food. Future studies should assess levels of trans fats, sodium, and added sugars to guide policy efforts aimed at improving food quality and ensuring compliance with regulatory standards.
A key strength of this review was its use of comprehensive search criteria to maximize the identification of relevant publications. However, limitations include the failure to adhere strictly to systematic review standards. Nevertheless, this study provides valuable evidence to guide policymakers in implementing regulations to curb the rise of fast food consumption in the region. Furthermore, the findings lay the groundwork for future research focused on developing innovative, health‐conscious approaches to fast food, addressing the underlying factors driving its consumption.
5. Conclusion
This review revealed widespread consumption of fast food in LMICs across Asia, with Western fast food like pizza, burgers, fried chicken, French fries, and sandwiches being particularly popular. Several key factors driving this consumption included taste, affordability, availability, mass media influence, restaurant environment, service quality, family and peer influence, socioeconomic factors, age, gender, education, employment status, time constraints, stress, and health consciousness. The evidence underscores a critical situation, as fast food consumption is linked to overweight and obesity. This situation is concerning, especially in these economically vulnerable regions. To address these challenges, the implementation of targeted governmental policies is crucial. Such measures will help curb the expansion of unhealthy fast food practices and mitigate their adverse health effects in this region.
Author Contributions
Rafid Hassan: conceptualization (equal), data curation (equal), formal analysis (equal), methodology (equal), writing – original draft (equal), writing – review and editing (equal). Abu Ahmed Shamim: writing – review and editing (supporting). Masum Ali: writing – review and editing (supporting). Md. Ruhul Amin: conceptualization (equal), methodology (supporting), supervision (lead), writing– review, and editing (lead).
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Supporting File 1: puh270095‐sup‐0001‐Tables.docx
Funding: The authors received no specific funding for this work.
Data Availability Statement
Data sharing does not apply to this article, as no datasets were generated or analyzed during the current study.
References
- 1. Baker P. and Friel S., “Food Systems Transformations, Ultra‐Processed Food Markets and the Nutrition Transition in Asia,” Globalization and Health 12, no. 80 (2016): 1–15, 10.1186/s12992-016-0223-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Pan A., Malik V. S., and Hu F. B., “Exporting Diabetes Mellitus to Asia: The Impact of Western‐Style Fast Food,” Circulation 126, no. 2 (2012): 163–165, 10.1161/CIRCULATIONAHA.112.115923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Pingali P., “Westernization of Asian Diets and the Transformation of Food Systems: Implications for Research and Policy,” Food Policy 32, no. 3 (2007): 281–298, 10.1016/j.foodpol.2006.08.001. [DOI] [Google Scholar]
- 4. Thow A. M., Farrell P., Helble M., and Rachmi C. N., “Eating in Developing Asia: Trends, Consequences and Policies,” Background Paper for the Asian Development Outlook 2020 Update: Wellness in Worrying Times (Asian Development Bank, 2020). [Google Scholar]
- 5. Jahan I., Karmakar P., Hossain M. M., Jahan N., and Islam M. Z., “Fast Food Consumption and Its Impact on Health,” Eastern Medical College Journal 5, no. 1 (2020): 28–36. [Google Scholar]
- 6. Kendall E., “Fast Food,” Encyclopedia Britannica, published 2024, https://www.britannica.com/topic/fast‐food.
- 7. Ufholz K. and Werner J. J., “Social and Demographic Correlates of Fast Food Consumption: A Review of Recent Findings in the United States and Worldwide,” Current Cardiovascular Risk Reports 17, no. 12 (2023): 233–243, 10.1007/s12170-023-00730-5. [DOI] [Google Scholar]
- 8. Bishwajit G., “Nutrition Transition in South Asia: The Emergence of Non‐Communicable Chronic Diseases,” F1000Research 4, no. 8 (2015): 1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kelly M., “The Nutrition Transition in Developing Asia: Dietary Change, Drivers and Health Impacts,” in Eating, Drinking: Surviving. SpringerBriefs in Global Understanding, ed. Jackson P., Spiess W., and Sultana F. (Springer, 2016), 83–90, 10.1007/978-3-319-42468-2_9. [DOI] [Google Scholar]
- 10. Wang Y., Wang L., Xue H., and Qu W., “A Review of the Growth of the Fast Food Industry in China and Its Potential Impact on Obesity,” International Journal of Environmental Research and Public Health 13 (2016): 1112, 10.3390/ijerph13111112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Wu Y., Wang L., Zhu J., Gao L., and Wang Y., “Growing Fast Food Consumption and Obesity in Asia: Challenges and Implications,” Social Science and Medicine 269 (2021): 113601, 10.1016/j.socscimed.2020.113601. [DOI] [PubMed] [Google Scholar]
- 12. Bowman S. A. and Vinyard B. T., “Fast Food Consumption of U.S. Adults: Impact on Energy and Nutrient Intakes and Overweight Status,” Journal of the American College of Nutrition 23, no. 2 (2004): 163–168, 10.1080/07315724.2004.10719357. [DOI] [PubMed] [Google Scholar]
- 13. Ebbeling C. B., Sinclair K. B., Pereira M. A., Garcia‐lago E., Feldman H. A., and Ludwig D. S., “Compensation for Energy Intake From Fast Food Among Overweight and Lean Adolescents,” JAMA 291, no. 23 (2004): 2828–2833. [DOI] [PubMed] [Google Scholar]
- 14. French S. A., Harnack L., and Jeffery R. W., “Fast Food Restaurant Use Among Women in the Pound of Prevention Study: Dietary, Behavioral and Demographic Correlates,” International Journal of Obesity 24, no. 10 (2000): 1353–1359, 10.1038/sj.ijo.0801429. [DOI] [PubMed] [Google Scholar]
- 15. Pereira M. A., Kartashov A. I., Ebbeling C. B., et al., “Fast‐Food Habits, Weight Gain, and Insulin Resistance (the CARDIA Study): 15‐Year Prospective Analysis,” Lancet 365, no. 9453 (2005): 36–42, 10.1016/S0140-6736(04)17663-0. [DOI] [PubMed] [Google Scholar]
- 16. Rosenheck R., “Fast Food Consumption and Increased Caloric Intake: A Systematic Review of a Trajectory Towards Weight Gain and Obesity Risk,” Obesity Reviews 9, no. 6 (2008): 535–547, 10.1111/j.1467-789X.2008.00477.x. [DOI] [PubMed] [Google Scholar]
- 17. Williams E. P., Mesidor M., Winters K., Dubbert P. M., and Wyatt S. B., “Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem,” Current Obesity Reports 4, no. 3 (2015): 363–370, 10.1007/s13679-015-0169-4. [DOI] [PubMed] [Google Scholar]
- 18. Wyatt S. B., Winters K. P., and Dubbert P. M., “Overweight and Obesity: Prevalence, Consequences, and Causes of a Growing Public Health Problem,” American Journal of the Medical Sciences 331, no. 4 (2006): 166–174, 10.1097/00000441-200604000-00002. [DOI] [PubMed] [Google Scholar]
- 19. Haddad L., Cameron L., and Barnett I., “The Double Burden of Malnutrition in SE Asia and the Pacific: Priorities, Policies and Politics,” Health Policy and Planning 30, no. 9 (2015): 1193–1206, 10.1093/heapol/czu110. [DOI] [PubMed] [Google Scholar]
- 20. Winichagoon P. and Margetts B. M., “The Double Burden of Malnutrition in Low‐ and Middle‐Income Countries,” in Energy Balance and Obesity, ed. Romieu I., Dossus L., and Willett W. C. (International Agency for Research on Cancer, 2017), 9–15, https://www.ncbi.nlm.nih.gov/books/NBK565811/. [PubMed] [Google Scholar]
- 21. Estecha Querol S., Iqbal R., Kudrna L., Al‐Khudairy L., and Gill P., “The Double Burden of Malnutrition and Associated Factors Among South Asian Adolescents: Findings From the Global School‐Based Student Health Survey,” Nutrients 13, no. 8 (2021): 2867, 10.3390/nu13082867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Janssen H. G., Davies I. G., Richardson L. D., and Stevenson L., “Determinants of Takeaway and Fast Food Consumption: A Narrative Review,” Nutrition Research Reviews 31, no. 1 (2018): 16–34, 10.1017/S0954422417000178. [DOI] [PubMed] [Google Scholar]
- 23. Arya C. and Dubey N., “A Critical Review on Fast‐Food Consumption Pattern Among South Asian and Southeast Asian Young Adults,” International Journal of Community Medicine and Public Health 10, no. 6 (2023): 2282–2290, 10.18203/2394-6040.ijcmph20231717. [DOI] [Google Scholar]
- 24. Saha S., Al Mamun M. A., and Kabir M. R., “Factors Affecting Fast Food Consumption Among College Students in South Asia: A Systematic Review,” Journal of the American Nutrition Association 41, no. 6 (2022): 627–637, 10.1080/07315724.2021.1940354. [DOI] [PubMed] [Google Scholar]
- 25.“World Bank Country and Lending Groups,” World Bank, accessed November 27, 2023, https://datahelpdesk.worldbank.org/knowledgebase/articles/906519‐world‐bank‐country‐and‐lending‐groups. [Google Scholar]
- 26. Faizi N. and Mittal C., “Fast Food Is Not the Only Junk Food: Consumption Pattern of Different Types of Junk Food in Adolescents of Aligarh,” Indian Journal of Child Health 5, no. 11 (2018): 659–662. [Google Scholar]
- 27. Joseph N., Nelliyanil M., Rai S., et al., “Fast Food Consumption Pattern and Its Association With Overweight Among High School Boys in Mangalore City of Southern India,” Journal of Clinical and Diagnostic Research 9, no. 5 (2015): LC13–LC17, 10.7860/JCDR/2015/13103.5969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Khan M., Banerjee S., Bandyopadhyay K., et al., “Role of Dietary Habits and Personal Hygiene on Nutritional Status of School‐Going Adolescents: A Cross‐Sectional Study in Selected Schools Located in Slum Areas of Nagpur City, Maharashtra,” Annals of African Medicine 21, no. 3 (2022): 185–192, 10.4103/aam.aam_109_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Nawab T., Khan Z., Khan I., and Ansari M., “Is Small Town India Falling Into the Nutritional Trap of Metro Cities? A Study in School‐Going Adolescents,” Journal of Family Medicine and Primary Care 5, no. 3 (2016): 581–586, 10.4103/2249-4863.197296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Rani M. A. and Sathiyasekaran B. W. C., “Behavioural Determinants for Obesity: A Cross‐Sectional Study Among Urban Adolescents in India,” Journal of Preventive Medicine and Public Health 46, no. 4 (2013): 192–200, 10.3961/jpmph.2013.46.4.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hayyat M. U., Munir A., Shahzad L., Farhan M., and Ghafoor G. Z., “Assessing the Nexus of Fast Food Consumption and Childhood Obesity in Lahore Metropolitan City of Pakistan,” International Journal of Biosciences (IJB) 14, no. 04 (2019): 95–102, 10.12692/ijb/14.4.95-102. [DOI] [Google Scholar]
- 32. Shami Y. and Fatima F., “Trend of Fast Food Consumption Among College Girls,” International Journal of Scientific and Engineering Research 8, no. 2 (2017): 598–606. [Google Scholar]
- 33. Poudel P., “Junk Food Consumption and Its Association With Body Mass Index Among School Adolescents,” International Journal of Nutrition and Food Sciences 7, no. 3 (2018): 90–93, 10.11648/j.ijnfs.20180703.12. [DOI] [Google Scholar]
- 34. Choeda T., Jeyashree K., Kathirvel S., et al., “Dietary Behavior of School‐Going Adolescents in Bhutan: Findings From the Global School‐Based Student Health Survey in 2016,” Nutrition (Burbank, Los Angeles County, Calif.) 90 (2021): 111290, 10.1016/j.nut.2021.111290. [DOI] [PubMed] [Google Scholar]
- 35. Chong K. H., Wu S. K., Hafizah N., et al., “Eating Habits of Malaysian Children: Findings of the South East Asian Nutrition Surveys (SEANUTS),” Asia Pacific Journal of Public Health 28, no. S5 (2016): 59S–73S, 10.1177/1010539516654260. [DOI] [PubMed] [Google Scholar]
- 36. Gan W. Y., Mohamed S. F., and Law L. S., “Unhealthy Lifestyle Associated With Higher Intake of Sugar‐Sweetened Beverages Among Malaysian School‐Aged Adolescents,” International Journal of Environmental Research and Public Health 16, no. 15 (2019): 2785, 10.3390/ijerph16152785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Li L., Sun N., Zhang L., et al., “Fast Food Consumption Among Young Adolescents Aged 12–15 Years in 54 Low‐ and Middle‐Income Countries,” Global Health Action 13, no. 1 (2020): 1795438, 10.1080/16549716.2020.1795438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Man C. S., Hock L. K., Ying C. Y., et al., “Is Fast‐Food Consumption a Problem Among Adolescents in Malaysia? An Analysis of the National School‐Based Nutrition Survey, 2012,” Journal of Health, Population and Nutrition 40, no. 1 (2021): 1–10, 10.1186/s41043-021-00254-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Al‐Delaimy A. K., Al‐Taha M. A., and Al‐Samarraie M. A. M., “Prevalence and Predicting Risk Factors of Overweight and Obesity Among Primary School Pupils in Ramadi, Iraq,” Malaysian Journal of Public Health Medicine 20, no. 3 (2020): 20–26, 10.37268/MJPHM/VOL.20/NO.3/ART.544. [DOI] [Google Scholar]
- 40. Khan A. and Uddin R., “Is Consumption of Fast‐Food and Carbonated Soft Drink Associated With Anxiety‐Induced Sleep Disturbance Among Adolescents? A Population‐Based Study,” Clinical Nutrition ESPEN 36 (2020): 162–165, 10.1016/j.clnesp.2020.01.011. [DOI] [PubMed] [Google Scholar]
- 41. Alimoradi F., Jandaghi P., Khodabakhshi A., Javadi M., and Zehni Moghadam S. A. H., “Breakfast and Fast Food Eating Behavior in Relation to Socio‐Demographic Differences Among School Adolescents in Sanandaj Province, Iran,” Electronic Physician 9, no. 6 (2017): 4510–4515, 10.19082/4510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Rasouli A., Mohiti S., Javadi M., Panjeshahin A., Kazemi M., and Shiri‐Shahsavar M. R., “The Effect of Daily Fast Food Consumption, Family Size, Weight‐Caused Stress, and Sleep Quality on Eating Disorder Risk in Teenagers,” Sleep and Breathing 25, no. 3 (2021): 1527–1533, 10.1007/s11325-020-02189-9. [DOI] [PubMed] [Google Scholar]
- 43. Shayan‐Moghadam R., Heidari‐Beni M., Riahi R., et al., “Assessment of Lifestyle and Eating Habits Among a Nationally Representative Sample of Iranian Adolescent Girls: The CASPIAN‐V Study,” Archives of Iranian Medicine 23, no. 8 (2020): 522–529, 10.34172/aim.2020.54. [DOI] [PubMed] [Google Scholar]
- 44. Yarmohammadi P., Sharifirad G. R., and Azadbakht L., “The Association Between Socio‐Demographic Characteristics and Fast Food Consumption With in High School Students in Isfahan, Iran,” Journal of Community Health Research 4, no. 3 (2015): 194–202. [Google Scholar]
- 45. Li M., Xue H., Jia P., et al., “Pocket Money, Eating Behaviors, and Weight Status Among Chinese Children: The Childhood Obesity Study in China Mega‐Cities,” Preventive Medicine 100 (2017): 208–215, 10.1016/j.ypmed.2017.04.031. [DOI] [PubMed] [Google Scholar]
- 46. Aruppillai T. and Godwin Phillip P. M., “An Analysis of Consumers' Buying Behaviour and Its Determinants of Fast Food in Sri Lanka,” International Journal of Economics and Finance 7, no. 9 (2015): 112–119, 10.5539/ijef.v7n9p112. [DOI] [Google Scholar]
- 47. Smith L., Barnett Y., López‐Sánchez G. F., et al., “Food Insecurity (Hunger) and Fast‐Food Consumption Among 180,164 Adolescents Aged 12–15 Years From 68 Countries,” British Journal of Nutrition 127, no. 3 (2020): 470–477, 10.1017/S0007114521001173. [DOI] [PubMed] [Google Scholar]
- 48. Tariq S., Tariq S., and Tariq S., “Association of Perceived Stress With Healthy and Unhealthy Food Consumption Among Teenagers,” Journal of the Pakistan Medical Association 69, no. 12 (2019): 1817–1821, 10.5455/JPMA.302642278. [DOI] [PubMed] [Google Scholar]
- 49. Mushtaq M. U., Gull S., Mushtaq K., Shahid U., Shad M. A., and Akram J., “Dietary Behaviors, Physical Activity and Sedentary Lifestyle Associated With Overweight and Obesity, and Their Socio‐Demographic Correlates, Among Pakistani Primary School Children,” International Journal of Behavioral Nutrition and Physical Activity 8, no. 130 (2011): 1–13, 10.1186/1479-5868-8-130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Musaiger A. O., Al‐Mufty B. A., and Al‐Hazzaa H. M., “Eating Habits, Inactivity, and Sedentary Behavior Among Adolescents in Iraq: Sex Differences in the Hidden Risks of Noncommunicable Diseases,” Food and Nutrition Bulletin 35, no. 1 (2014): 12–19, 10.1177/156482651403500102. [DOI] [PubMed] [Google Scholar]
- 51. Banik R., Naher S., Pervez S., and Hossain M. M., “Fast Food Consumption and Obesity Among Urban College Going Adolescents in Bangladesh: A Cross‐Sectional Study,” Obesity Medicine 17 (2020): 100161, 10.1016/j.obmed.2019.100161. [DOI] [Google Scholar]
- 52. Musaiger A. O. and Kalam F., “Dietary Habits and Lifestyle Among Adolescents in Damascus, Syria,” Annals of Agricultural and Environmental Medicine 21, no. 2 (2014): 416–419, 10.5604/1232-1966.1108616. [DOI] [PubMed] [Google Scholar]
- 53. Nguyen N. M., Tang H. K., Dibley M. J., and Alam A., “Sugar‐Sweetened Beverage Consumption and Overweight and Obesity in Adolescents in Ho Chi Minh City, Vietnam: A Population‐Based Analysis,” Pediatrics International 64, no. 1 (2022): e14886, 10.1111/ped.14886. [DOI] [PubMed] [Google Scholar]
- 54. Ma R., Castellanos D. C., and Bachman J., “Identifying Factors Associated With Fast Food Consumption Among Adolescents in Beijing China Using a Theory‐Based Approach,” Public Health 136 (2016): 87–93, 10.1016/j.puhe.2016.03.019. [DOI] [PubMed] [Google Scholar]
- 55. Qin Z., Wang N., Ware R. S., Sha Y., and Xu F., “Lifestyle‐Related Behaviors and Health‐Related Quality of Life Among Children and Adolescents in China,” Health and Quality of Life Outcomes 19, no. 1 (2021): 1–9, 10.1186/s12955-020-01657-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Zhao Y., Wang L., Xue H., Wang H., and Wang Y., “Fast Food Consumption and Its Associations With Obesity and Hypertension Among Children: Results From the Baseline Data of the Childhood Obesity Study in China Mega‐Cities,” BMC Public Health [Electronic Resource] 17, no. 1 (2017): 933, 10.1186/s12889-017-4952-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Rojekar N. P., Sajjanar A., Chavan P., Shukla H., and Bhattad D., “Assessment of Knowledge, Attitude and Factors Affecting Consumption of Fast Food in 8–12 Years of Children: A Cross Sectional Study,” Journal of Advanced Medical and Dental Sciences Research 7, no. 8 (2019): 100–105. [Google Scholar]
- 58. Singh M. and Mishra S., “Fast Food Consumption Pattern and Obesity Among School Going (9‐13 Year) in Lucknow District,” International Journal of Science and Research (IJSR) 3, no. 6 (2014): 1672–1674. [Google Scholar]
- 59. Taghizadeh S., Abbasalizad‐Farhangi M., Pourali F., and Asghari‐Jafarabadi M., “Predictors of Childhood High Blood Pressure Among Overweight and Obese Children and Adolescents According to the Lifestyle‐Scoring Algorithm Using Data From Iranian Health Care Reform Plan,” Clinical Nutrition Research 10, no. 3 (2021): 243–256, 10.7762/cnr.2021.10.3.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Bohara S. S., Thapa K., Bhatt L. D., Dhami S. S., and Wagle S., “Determinants of Junk Food Consumption Among Adolescents in Pokhara Valley, Nepal,” Frontiers in Nutrition 8, no. 644650 (2021): 1–9, 10.3389/fnut.2021.644650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Ahmed J., Rehman S. U., and Mughal F., “Assessment of Dietary Behavior of High School Students of an Urban Setting in Pakistan,” International Journal of Health Science 10, no. 4 (2016): 549–555, 10.12816/0049658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Javalkar S., Akshaya K. M., and Nirgude A. S., “Food Habits and Fast Food Preferences Among Medical Students,” International Journal of Multidisciplinary Research and Development 2, no. 10 (2015): 556–559. [Google Scholar]
- 63. Mahajan S. A. and Gothankar J. S., “Fast Food Consumption Pattern Amongst Undergraduates of Various Disciplines of Private Colleges in Pune,” International Journal of Community Medicine And Public Health 7, no. 2 (2020): 505–511, 10.18203/2394-6040.ijcmph20196069. [DOI] [Google Scholar]
- 64. Rauf A., Dawood R., Chohan U., and Akhtar J., “Prevalence of Overweight Among Students of Sargodha Medical College Due To Increased Consumption of Fast Food,” Pak‐Euro Journal of Medical and Life Sciences 3, no. 1 (2020): 19–22, 10.31580/pjmls.v3i1.1240. [DOI] [Google Scholar]
- 65. Sharma S., Patnaik L., Pattnaik S., and Mohapatra G., “Study on Consumption of Fast Food and Its Association With BMI Among Medical Students in a Tertiary Care Center of Eastern India,” International Journal of Nutrition, Pharmacology, Neurological Diseases 13, no. 3 (2023): 140–144, 10.4103/ijnpnd.ijnpnd_2_23. [DOI] [Google Scholar]
- 66. Shree V., Prasad R. R., Kumar S., Sinha S., and Choudhary S. K., “Study on Consumption of Fast Food Among Medical Students of IGIMS, Patna,” International Journal of Community Medicine And Public Health 5, no. 7 (2018): 2750–2754, 10.18203/2394-6040.ijcmph20182416. [DOI] [Google Scholar]
- 67. Akhter M. M., “Consumer Attitude Toward Fast Food Consumption: A Study on University Students in Dhaka City,” Asian Journal of Humanity, Art and Literature 6, no. 1 (2019): 21–32, 10.18034/ajhal.v6i1.346. [DOI] [Google Scholar]
- 68. Al Muktadir M. H., Islam M. A., Amin M. N., et al., “Nutrition Transition – Pattern IV: Leads Bangladeshi Youth to the Increasing Prevalence of Overweight and Obesity,” Diabetes and Metabolic Syndrome: Clinical Research and Reviews 13, no. 3 (2019): 1943–1947, 10.1016/j.dsx.2019.04.034. [DOI] [PubMed] [Google Scholar]
- 69. Bipasha M. S. and Goon S., “Fast Food Preferences and Food Habits Among Students of Private Universities in Bangladesh,” South East Asia Journal of Public Health 3, no. 1 (2013): 61–64, 10.3329/seajph.v3i1.17713. [DOI] [Google Scholar]
- 70. Goon S., Bipasha M. S., and Islam M. S., “Fast Food Consumption and Obesity Risk Among University Students of Bangladesh,” European Journal of Preventive Medicine 2, no. 6 (2014): 99–104, 10.11648/j.ejpm.20140206.14. [DOI] [Google Scholar]
- 71. Karmakar P., Jahan N., Banik S., Das A., and Rahman K. A., “Food Habits, Obesity and Nutritional Knowledge Among the University Students in Noakhali Region of Bangladesh: A Cross Sectional Study,” Journal of Food and Nutritional Disorders 5, no. 4 (2016): 1–6, 10.4172/2324-9323.1000201. [DOI] [Google Scholar]
- 72. Shetu S. N., “Factors Influencing on Consumers' Fast‐Food Consumption Preferences: An Empirical Study on Facebook Users in Dhaka City, Bangladesh,” International Journal of Business and Technopreneurship 11, no. 1 (2021): 13–24. [Google Scholar]
- 73. Akhtar N., Zareen H., and Sarmad R., “Eating Habits and Nutritional Status of Female Students of a Medical College of Lahore,” Annals of King Edward Medical University 24, no. 1 (2018): 49–53, 10.21649/akemu.v24i1.2321. [DOI] [Google Scholar]
- 74. Asghar A., Shah A. M., Hussain A. A., Tahir A., and Asghar H., “Frequency of Pre‐Obesity and Obesity in Medical Students of Karachi and the Predisposing Lifestyle Habits,” Cureus 11, no. 1 (2019): e3948, 10.7759/cureus.3948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Irfan M., Jabbar M., and Hameed S., “Dietary Habits and Prevalence of Underweight /Obesity in Students of University of Gujrat, Pakistan,” Journal of Liaquat University of Medical and Health Sciences 18, no. 02 (2019): 175–180, 10.22442/jlumhs.191820623. [DOI] [Google Scholar]
- 76. Ismail I., “Trend of Fast Food Consumption Among University Girls in Karachi, Pakistan,” International Journal of Endorsing Health Science Research 4, no. 1 (2016): 32–38, 10.29052/ijehsr.v4.i1.2016.32-38. [DOI] [Google Scholar]
- 77. Jayasinghe J. M. J. K. and De Silva L. P. U., “Fast Food Consumption and Health Status of Students of a University in Sri Lanka,” Journal of Food and Agriculture 7, no. 1 and 2 (2014): 38–50, 10.4038/jfa.v7i1-2.5192. [DOI] [Google Scholar]
- 78. Mat R. C., Zulqernain N. S., and Zaid N. A. M., “Profiling of Malaysian Young Consumers Towards Fast Food Consumptions,” Journal of Applied Environmental and Biological Sciences 6, no. 7S (2016): 20–27. [Google Scholar]
- 79. Syafiqah I. N., Riza N., Chik A., et al., “Fast Food Consumption Behavior Among University Students,” International Journal of Research and Innovation in Social Science (IJRISS) II, no. XII (2018): 138–141. [Google Scholar]
- 80. Phan T. A. and Mai P. H., “Determinants Impacting Consumers' Purchase Intention: The Case of Fast Food in Vietnam,” International Journal of Marketing Studies 8, no. 5 (2016): 56–68, 10.5539/ijms.v8n5p56. [DOI] [Google Scholar]
- 81. Alhashemi M., Mayo W., Alshaghel M. M., Alsaman M. Z. B., and Kassem L. H., “Prevalence of Obesity and Its Association With Fast‐Food Consumption and Physical Activity: A Cross‐Sectional Study and Review of Medical Students' Obesity Rate,” Annals of Medicine and Surgery 79 (2022): 104007, 10.1016/j.amsu.2022.104007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Mwafi N. R., Al‐Rawashdeh I. M., Al‐Kubaisy W. A., Ezzat W. R., Al‐Qazaqi R. A., and Salameh M. H., “Prevalence and Factors Related to Obesity and Fast Food Consumption Among Mutah University Students, Jordan,” Journal of the Pakistan Medical Association 71, no. 6 (2021): 1608–1612, 10.47391/JPMA.274. [DOI] [PubMed] [Google Scholar]
- 83. Arslan N., Aslan Ceylan J., and Hatipoğlu A., “The Relationship of Fast Food Consumption With Sociodemographic Factors, Body Mass Index and Dietary Habits Among University Students,” Nutrition and Food Science 53, no. 1 (2023): 112–123, 10.1108/NFS-01-2022-0003. [DOI] [Google Scholar]
- 84. Tayem Y. I., Yaseen N. A., Khader W. T., Abu Rajab L. O., Ramahi A. B., and Saleh M. H., “Prevalence and Risk Factors of Obesity and Hypertension Among Students at a Central University in the West Bank,” Libyan Journal of Medicine 7, no. 1 (2012): 3–7, 10.3402/ljm.v7i0.19222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Azadbakht L. and Esmaillzadeh A., “Macro and Micro‐Nutrients Intake, Food Groups Consumption and Dietary Habits Among Female Students in Isfahan University of Medical Sciences,” Iranian Red Crescent Medical Journal 14, no. 4 (2012): 204–209. [PMC free article] [PubMed] [Google Scholar]
- 86. Jahanbakhsh E. and Mousanezhad Z., “Survey of Fast Food Consumption Status and Its Relationship With Personal‐Background Variables Among Students of Ilam Universities, Iran,” Archives of Hygiene Sciences 4, no. 3 (2015): 161–166. [Google Scholar]
- 87. Namdar A., Naghizadeh M. M., Zamani M., and Montazeri A., “Exploring the Relationship Between Health Literacy and Fast Food Consumption: A Population‐Based Study From Southern Iran,” BMC Public Health [Electronic Resource] 21, no. 1 (2021): 1–11, 10.1186/s12889-021-10763-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Rezaei S. M. A., “Frequency and Attitudes to Fast Food Consumption in Yasuj, Southwestern Iran,” International Journal of Nutrition Sciences 2, no. 2 (2017): 92–96. [Google Scholar]
- 89. Sangsefidi Z. S., Lorzadeh E., Hosseinzadeh M., and Mirzaei M., “Dietary Habits and Psychological Disorders in a Large Sample of Iranian Adults: A Population‐Based Study,” Annals of General Psychiatry 19, no. 1 (2020): 1–10, 10.1186/s12991-020-00263-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Sim S. and Laohasiriwong W., “Fast Food Consumption, Overweight and Obesity Among Working Age Persons in Cambodia,” Journal of Clinical and Diagnostic Research 13, no. 7 (2019): LC01–LC06, 10.7860/jcdr/2019/41892.12965. [DOI] [Google Scholar]
- 91. Azizan N. A., Thangiah N., Su T. T., and Majid H. A., “Does a Low‐Income Urban Population Practise Healthy Dietary Habits?,” International Health 10, no. 2 (2018): 108–115, 10.1093/inthealth/ihy001. [DOI] [PubMed] [Google Scholar]
- 92. Eng C. W., Lim S. C., Ngongo C., et al., “Dietary Practices, Food Purchasing, and Perceptions About Healthy Food Availability and Affordability: A Cross‐Sectional Study of Low‐Income Malaysian Adults,” BMC Public Health [Electronic Resource] 22, no. 1 (2022): 192, 10.1186/s12889-022-12598-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Kim D. Y., Ahn A., Lee H., Choi J., and Lim H., “Dietary Patterns Independent of Fast Food Are Associated With Obesity Among Korean Adults: Korea National Health and Nutrition Examination Survey 2010–2014,” Nutrients 11, no. 11 (2019): 2740, 10.3390/nu11112740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Chowdhury N. S., “Eating Habits and Nutritional Status Among the Bangladeshi Medical Students Depending Upon BMI,” Update Dental College Journal 4, no. 1 (2014): 10–14, 10.3329/updcj.v4i1.21159. [DOI] [Google Scholar]
- 95. Rizwan A, Hossain AA, Akhter S, et al., “Fast Food Consumption Pattern Among Students of a Private Medical College of Northern Bangladesh,” Dinajpur Medical College Journal 11, no. 2 (2018): 226–230. [Google Scholar]
- 96. Pushkar K., Kaushik S., Nagarjuna P., Mukherjee G., Teli P., and Yadav A., “Fast‐Food Culture – Prevalence, Pattern, and Preference Trends and Its Association With Body Mass Index of Medical Students,” Journal of Marine Medical Society 25, no. 1 (2023): 37–42, 10.4103/jmms.jmms_36_22. [DOI] [Google Scholar]
- 97. Didarloo A., Khalili S., Aghapour A. A., Moghaddam‐Tabrizi F., and Mousavi S. M., “Determining Intention, Fast Food Consumption and Their Related Factors Among University Students by Using a Behavior Change Theory,” BMC Public Health [Electronic Resource] 22 (2022): 314, 10.1186/s12889-022-12696-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Mohammadbeigi A., Asgarian A., Moshir E., et al., “Fast Food Consumption and Overweight/Obesity Prevalence in Students and Its Association With General and Abdominal Obesity,” Journal of Preventive Medicine and Hygiene 59, no. 3 (2018): E236–E240, 10.15167/2421-4248/jpmh2018.59.3.830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Ali A. and Lee J. I., “Determinants of Consumer Satisfaction in Fast Food Industry of Lahore Pakistan,” Journal of the Korean Society of Food Culture 34, no. 4 (2019): 424–431, 10.7318/KJFC/2019.34.4.424. [DOI] [Google Scholar]
- 100. Moitra P. and Madan J., “Socioeconomic, Intrapersonal and Food Environmental Correlates of Unhealthy Snack Consumption in School‐Going Adolescents in Mumbai,” BMC Public Health [Electronic Resource] 22, no. 1 (2022): 1129, 10.1186/s12889-022-13449-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Song C., Goto K., Hu M., and Wolff C., “The Impact of Social and Cultural Factors on the Consumption of Western Fast Food Among Chinese Children,” Community Development Journal 50, no. 4 (2015): 709–723, 10.1093/cdj/bsu067. [DOI] [Google Scholar]
- 102. Lwin M. O., Malik S., Ridwan H., and Au C. S. S., “Media Exposure and Parental Mediation on Fast‐Food Consumption Among Children in Metropolitan and Suburban Indonesian,” Asia Pacific Journal of Clinical Nutrition 26, no. 5 (2017): 899–905, 10.6133/apjcn.122016.04. [DOI] [PubMed] [Google Scholar]
- 103. Vaida N., “Prevalence of Fast Food Intake Among Urban Adolescent Students,” International Journal of Engineering And Science 2, no. 1 (2013): 353–359. [Google Scholar]
- 104. Sharifirad G., Yarmohammadi P., Azadbakht L., Morowatisharifabad M. A., and Hassanzadeh A., “Determinants of Fast Food Consumption Among Iranian High School Students Based on Planned Behavior Theory,” Journal of Obesity 2013 (2013): 1–7, 10.1155/2013/147589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Rasool Z. S. and Akbay C., “Fast Food Consumption Behavior of Consumers in the Northern Region of Iraq,” Eurasian Journal of Agricultural Economics (EJAE) 1, no. 1 (2021): 1–13. [Google Scholar]
- 106. Khaipetch J., “Factors Affecting Consumer Behavior of Fast Food in Pathum Thani,” RMUTT Global Business Accounting and Finance Review 1, no. 2 (2017): 50–62. [Google Scholar]
- 107. Meena M. and Varma K., “Fast Food Consumption Among Adolescent School Girls in Jaipur,” International Journal of Innovative Research and Review 3, no. 3 (2015): 38–42. [Google Scholar]
- 108. Monika B., Chishty S., and Verma K., “Fast Food Consumption Pattern Among Postgraduate Female Student Living in Hostel of University of Rajasthan, India,” Asian Journal of Dairy and Food Research 34, no. 4 (2015): 324–327, 10.18805/ajdfr.v34i4.6887. [DOI] [Google Scholar]
- 109. Hatta N. M., Ali A., Yusof A., Shukri W. H. W. Z., and Shazmikamarudin K., “Socio‐Demographic Determinants of Fast‐Food Consumption in Malaysian Young Adults,” Malaysian Applied Biology 51, no. 6 (2022): 65–72, 10.55230/mabjournal.v51i6.2392. [DOI] [Google Scholar]
- 110. Singh D. R., Sunuwar D. R., Dahal B., and Sah R. K., “The Association of Sleep Problem, Dietary Habits and Physical Activity With Weight Status of Adolescents in Nepal,” BMC Public Health [Electronic Resource] 21, no. 1 (2021): 1–17, 10.1186/s12889-021-10985-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Mirkarimi K., Mansourian M., Kabir M. J., et al., “Fast Food Consumption Behaviors in High‐School Students Based on the Theory of Planned Behavior (TPB),” International Journal of Pediatrics 4, no. 7 (2016): 2131–2142, 10.22038/ijp.2016.7011. [DOI] [Google Scholar]
- 112. Keats E. C., Rappaport A. I., Shah S., Oh C., Jain R., and Bhutta Z. A., “The Dietary Intake and Practices of Adolescent Girls in Low‐ and Middle‐Income Countries: A Systematic Review,” Nutrients 10, no. 12 (2018): 1978, 10.3390/nu10121978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Shaban L. and Alkazemi D., “Trends in Fast‑Food Consumption Among Kuwaiti Youth,” International Journal of Preventive Medicine 10, no. 44 (2019): 1–7, 10.4103/ijpvm.IJPVM. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Naidoo N., van Dam R. M., Ng S., et al., “Determinants of Eating at Local and Western Fast‐Food Venues in an Urban Asian Population: A Mixed Methods Approach,” International Journal of Behavioral Nutrition and Physical Activity 14, no. 1 (2017): 69, 10.1186/s12966-017-0515-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Lim H., Lee H. J., Choue R., and Wang Y., “Trends in Fast‐Food and Sugar‐Sweetened Beverage Consumption and Their Association With Social Environmental Status in South Korea,” Journal of the Academy of Nutrition and Dietetics 118, no. 7 (2018): 1228–1236, 10.1016/j.jand.2017.08.001. [DOI] [PubMed] [Google Scholar]
- 116. Popkin B. M., “Global Nutrition Dynamics: The World Is Shifting Rapidly Toward a Diet Linked With Noncommunicable Diseases,” American Journal of Clinical Nutrition 84, no. 2 (2006): 289–298, 10.1093/ajcn/84.2.289. [DOI] [PubMed] [Google Scholar]
- 117. Adams J., Goffe L., Brown T., et al., “Frequency and Socio‐Demographic Correlates of Eating Meals Out and Take‐Away Meals at Home: Cross‐Sectional Analysis of the UK National Diet and Nutrition Survey, Waves 1–4 (2008‐12),” International Journal of Behavioral Nutrition and Physical Activity 12, no. 1 (2015): 1–9, 10.1186/s12966-015-0210-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Dunn K. I., Mohr P. B., Wilson C. J., and Wittert G. A., “Beliefs About Fast Food in Australia: A Qualitative Analysis,” Appetite 51, no. 2 (2008): 331–334, 10.1016/j.appet.2008.03.003. [DOI] [PubMed] [Google Scholar]
- 119. Orfanos P., Naska A., Trichopoulos D., et al., “Eating Out of Home and Its Correlates in 10 European Countries. The European Prospective Investigation Into Cancer and Nutrition (EPIC) Study,” Public Health Nutrition 10, no. 12 (2007): 1515–1525, 10.1017/S1368980007000171. [DOI] [PubMed] [Google Scholar]
- 120. Smith K. J., McNaughton S. A., Gall S. L., Blizzard L., Dwyer T., and Venn A. J., “Takeaway Food Consumption and Its Associations With Diet Quality and Abdominal Obesity: A Cross‐Sectional Study of Young Adults,” International Journal of Behavioral Nutrition and Physical Activity 6 (2009): 1–13, 10.1186/1479-5868-6-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Vandevijvere S., Lachat C., Kolsteren P., and Van Oyen H., “Eating Out of Home in Belgium: Current Situation and Policy Implications,” British Journal of Nutrition 102, no. 6 (2009): 921–928, 10.1017/S0007114509311745. [DOI] [PubMed] [Google Scholar]
- 122. Ayo S., Bonabana‐Wabbi J., and Sserunkuuma D., “Determinants of Fast Food Consumption in Kampala, Uganda,” African Journal of Food, Agriculture, Nutrition and Development 12, no. 5 (2012): 6567–6581, 10.18697/ajfand.53.10775. [DOI] [Google Scholar]
- 123. Bîlbîie A., Druică E., Dumitrescu R., Aducovschi D., Sakizlian R., and Sakizlian M., “Determinants of Fast‐Food Consumption in Romania: An Application of the Theory of Planned Behavior,” Foods 10 (2021): 1877, 10.3390/foods10081877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Steyn N. P., Labadarios D., and Nel J. H., “Factors Which Influence the Consumption of Street Foods and Fast Foods in South Africa—A National Survey,” Nutrition Journal 10, no. 1 (2011): 1–10, 10.1186/1475-2891-10-104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. FAO, UNICEF, WFP & WHO , Asia and the Pacific – Regional Overview of Food Security and Nutrition 2022. Urban Food Security and Nutrition (FAO, 2023), 10.4060/cc3990en. [DOI] [Google Scholar]
- 126. Anderson B., Rafferty A. P., Lyon‐Callo S., Fussman C., and Imes G., “Fast‐Food Consumption and Obesity Among Michigan Adults,” Preventing Chronic Disease 8, no. 4 (2011): 1–11. [PMC free article] [PubMed] [Google Scholar]
- 127. Musaiger A., Food Consumption Patterns in the Eastern Mediterranean Region (Arab Center for Nutrition, 2011). [Google Scholar]
- 128. Mohr P., Wilson C., Dunn K., Brindal E., and Wittert G., “Personal and Lifestyle Characteristics Predictive of the Consumption of Fast Foods in Australia,” Public Health Nutrition 10, no. 12 (2007): 1456–1463, 10.1017/S1368980007000109. [DOI] [PubMed] [Google Scholar]
- 129. Denney‐Wilson E., Crawford D., Dobbins T., Hardy L., and Okely A. D., “Influences on Consumption of Soft Drinks and Fast Foods in Adolescents,” Asia Pacific Journal of Clinical Nutrition 18, no. 3 (2009): 447–452. [PubMed] [Google Scholar]
- 130. FAO, UNICEF, WFP & WHO , Asia and the Pacific Regional Overview of Food Security and Nutrition 2020: Maternal and Child Diets at the Heart of Improving Nutrition (FAO, 2021), 10.4060/cb2895en. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting File 1: puh270095‐sup‐0001‐Tables.docx
Data Availability Statement
Data sharing does not apply to this article, as no datasets were generated or analyzed during the current study.