

Abstract
Since 2014, the National Cancer Institute Affordable Cancer Technologies (ACTs) program has supported a broad research portfolio focused on the development and validation of new technologies for global cancer control. ACTs projects are conducted by international teams composed of investigators from the United States and low- and middle-income countries, spurring important contextually relevant innovations. During its first decade, the ACTs program ushered in new technology platforms, led to commercialized products, and affected health policies and programs worldwide including in the United States. It has allowed a new generation of investigators working across disciplines and national borders to pursue novel technological solutions and leverage new analytic methods to advance human health. This commentary lays out the scope and accomplishments of the ACTs program to date while considering possible future research directions.
INTRODUCTION
In 2014, after years of planning and competitive review of applications, the US National Cancer Institute (NCI) funded the first grants in the Affordable Cancer Technologies (ACTs) program, a new initiative that sought to spur innovative, technology-driven solutions to cancer control challenges in low-resource settings, globally.1,2 The genesis of the ACTs program coincided with a consensus across the global health community that noncommunicable diseases, including cancers, deserved greater attention. This had previously led to the establishment of the NCI Center for Global Health in 2011, charged with integrating cancer control into global health research.3 Cancer control depends on the availability of effective technologies, and many standard technologies are unavailable in low- and middle-income countries (LMICs) because of expense, dependency on extensive medical infrastructure, or both.1 These needs, combined with a dedicated center at the NCI focused on supporting and coordinating US engagement in global cancer research efforts, motivated NCI to launch the ACTs program to expand the toolkit of possible solutions while incorporating affordability and utility at the point of need as explicit design criteria.
The research objective of the ACTs program is to engineer, adapt, apply, and validate new technologies to prevent, detect, diagnose, or treat cancers in specific LMIC health care settings. In addition to affordability, ACTs investigators are asked to consider cultural, environmental, societal, and demographic issues. These include distance to care, urban versus rural contexts, local health care delivery models, availability of companion technologies, and issues related to patient contact and follow-up. To maximize uptake by target populations, many ACTs technologies are also designed for use at the community level and/or nontraditional health care settings. Although teams supported by the ACTs program include US and LMIC investigators working in LMICs, finding novel technological solutions to key cancer challenges in LMICs has relevance for many communities in the United States, as evidenced by specific examples described below.
Because the ACTs program covers many cancer sites and types of interventions, there is no ideal target product profile for all successful ACTs technologies. However, several desirable characteristics have emerged. ACTs technologies have typically been designed for use at the point of need with a focus on ease of use, to ensure the technology is suitable for the chosen setting by caregivers trained locally in operation and maintenance. Likewise, successful technologies have typically been operable in locations with infrastructure challenges (eg, limited access to electricity or refrigeration). Many successful ACTs projects have focused on delivering rapid or real-time results leveraging Internet or mobile networks to transmit results to relevant databases for follow-up. Modular designs are often coupled to standard, readily available, commercial, off-the-shelf components to improve reliability, ease of use, and maintenance.
OVERVIEW OF ACTs PROGRAM PORTFOLIO
There has historically been little support from the National Institutes of Health (NIH) or other biomedical research funders for translational technology research for global oncology. Support from the NCI through the ACTs program has therefore filled an essential research gap and catalyzed a community of investigators, entrepreneurs, and implementers working together to address global cancer control challenges. In response to significant interest from the research community as reflected by many meritorious applications received over six funding solicitations to date, 38 cooperative agreement research project grants have been funded (mobile health [mHealth] projects focused on cancer control in LMICs are separately supported through NCI participation in the NIH Fogarty International Center Mobile Health: Technology and Outcomes in Low and Middle Income Countries program).4
To provide an overview of the ACTs portfolio, cancer site and common scientific outline (CSO) codes for each project were sourced from Dimensions for NIH.5 CSO codes are defined by the International Cancer Research Partnership and are used to categorize research across the cancer continuum.6 These data are presented in Figure 1. Although cervical and oral cancers are highly prevalent in LMICs and make up many of the awards, the portfolio of ACTs-funded projects are distributed across many cancer types. Additionally, most ACTs projects focused on early detection, diagnosis, and prognosis. There have been fewer ACTs projects focused on treatment, which represents an important area for future research to improve outcome disparities between high-income countries (HICs) and LMICs.7
FIG 1.

ACTs awards by cancer site and CSO code. Note that some awards may have multiple CSO codes and/or cancer sites. ACTs, Affordable Cancer Technologies; CSO, common scientific outline.
Research, Condition, and Disease Categorization (RCDC) codes8 are used to categorize NIH funding and relevant codes were sourced from Dimensions for NIH.5 The RCDC codes shown in Figure 2 highlight the translational focus of the ACTs portfolio while also shedding light on several active areas for ACTs technology development (eg, biomedical imaging, machine learning, and artificial intelligence).
FIG 2.
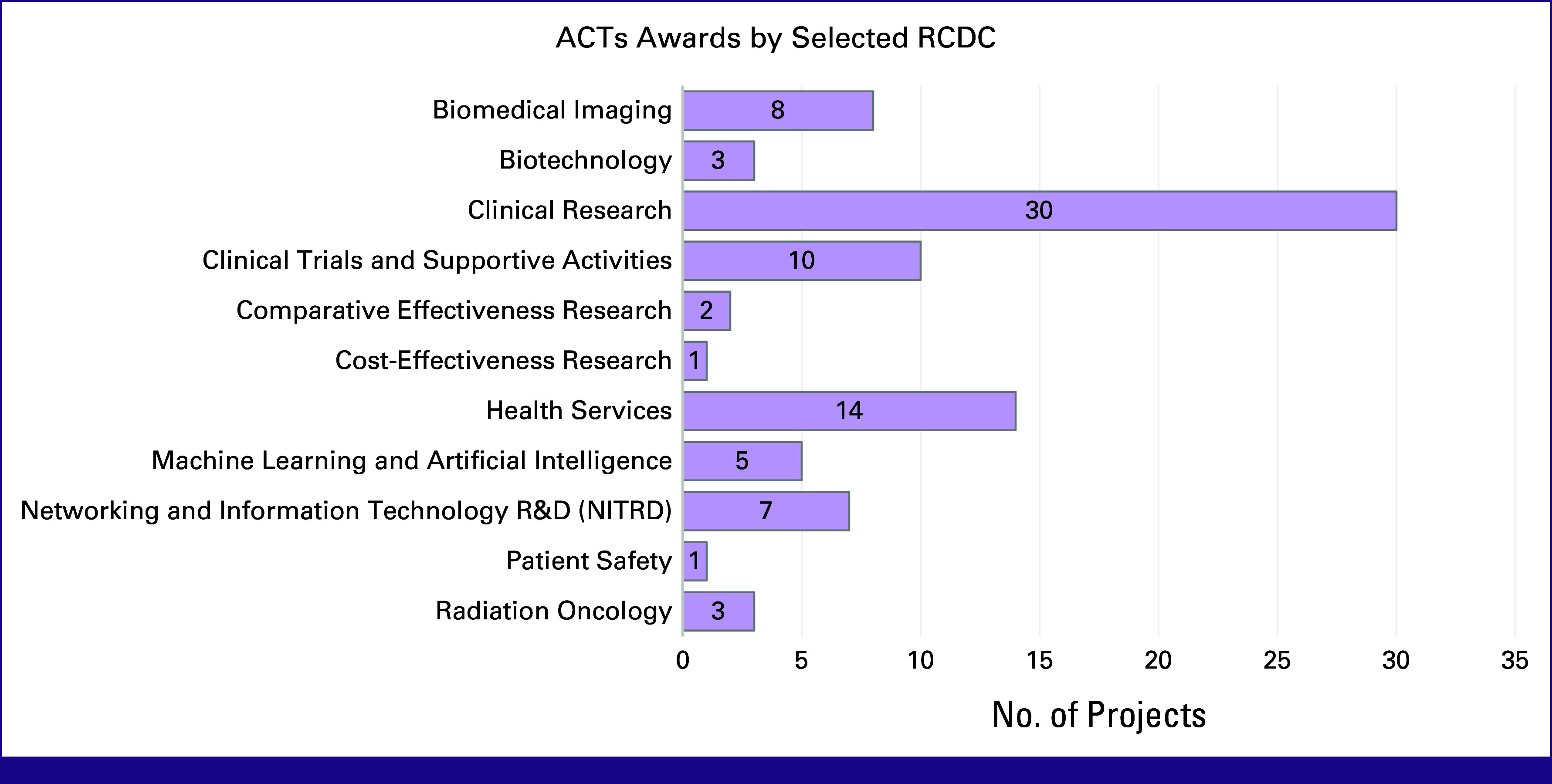
ACTs awards by RCDC codes. Note that some awards may have multiple RCDC codes. ACTs, Affordable Cancer Technologies; RCDC, Research, Condition, and Disease Categorization.
ACTs projects included principal investigators or collaborators in 39 countries, with the most frequent collaborators in India and Uganda (nine projects each). Collaborating countries represented all World Bank regions and four World Bank income groups, including 32 LMICs (Fig 3). This included 94 international collaborating institutions, 13 of which collaborated on multiple awards. Projects also included principal investigators at 25 institutions. To date, these projects have resulted in nine patents and 139 publications, which have been cited a total of 2,977 times (average of 21.42 citations per paper, mean relative citation ratio of 1.83, and mean Altmetric attention score of 12.58). Excluding the current 17 active awards, past ACTs investigators have gone on to successfully receive 71 additional NIH awards to further optimize and validate their technologies and expand their applications to other cancer sites.
FIG 3.
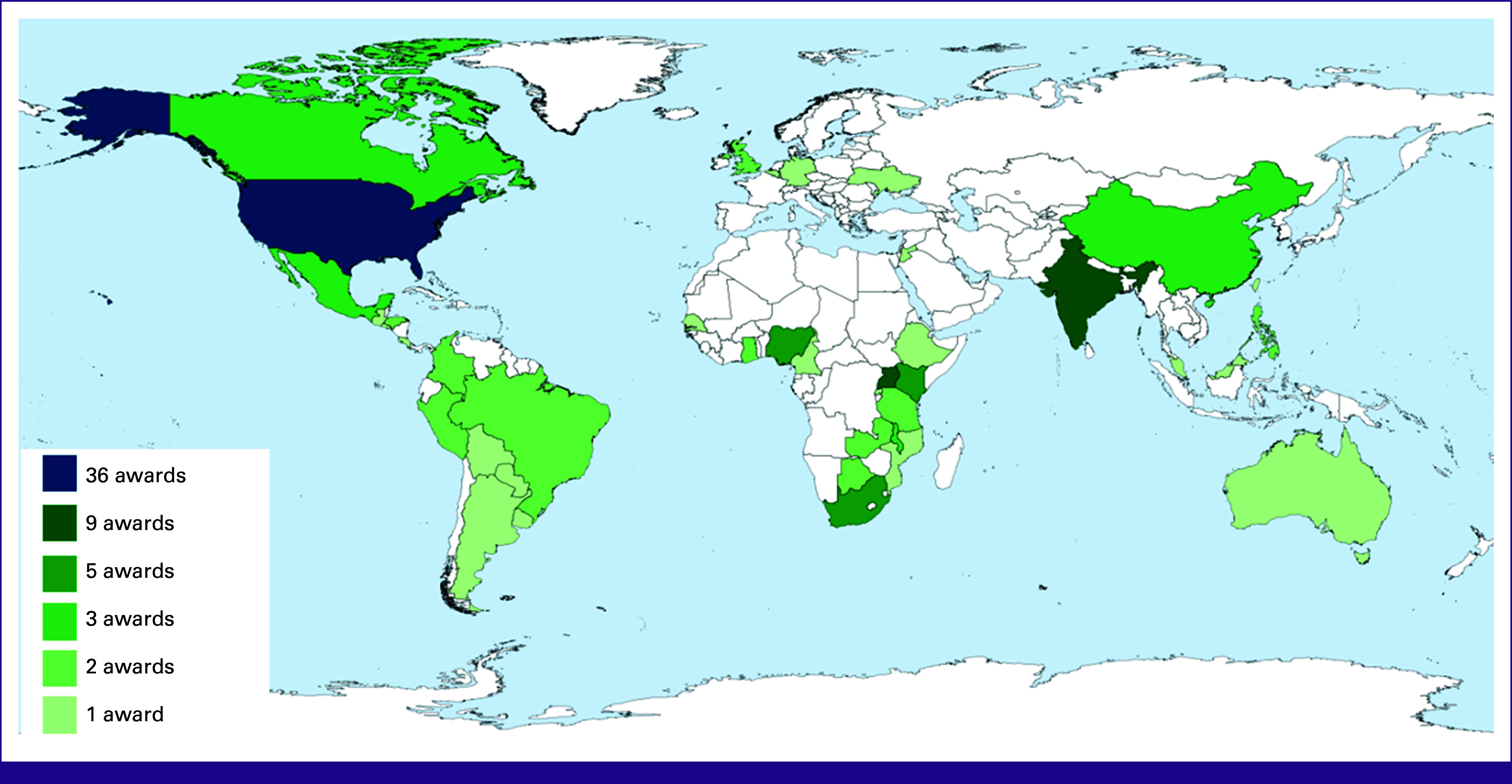
ACTs collaborator countries. Note that some projects have performance sites in several countries. ACTs, Affordable Cancer Technologies.
ACTs PROGRAM ACCOMPLISHMENTS
The remainder of this commentary will focus on specific examples from ACTs projects as well as perspectives on the evolution of the field and future research directions.
Cancer Screening and Early Detection
The ACTs program has supported 29 projects focused on early detection and diagnosis. Many projects leveraged the rapid development of low-cost consumer electronics, new and emerging biosensors, and advances in microfluidics to develop diagnostic platforms testing a variety of biomarkers and sample types at the point of care (POC). An example is a POC diagnostics for esophageal cancer developed at Johns Hopkins being studied in collaboration with investigators at Makerere University. This technology uses a retrievable swallowable sponge to gather esophageal specimens for molecular testing combined with a magnetofluidic chip for sample processing and detection of DNA methylation.9-12 In another ACTs project, investigators from Memorial Sloan Kettering Cancer Center, Obafemi Awolowo University, and the University of Alberta developed a colorimetric urine-based metabolomic screening test for colorectal cancer that, combined with clinical characteristics such as weight loss, showed promise for symptomatic individuals in Nigeria.13-15
Human Papillomavirus Diagnostics and Cervical Cancer Prevention
Several POC human papillomavirus (HPV) diagnostics have been developed and furthered. In a project coled by investigators from Becton Dickinson and Company and the University of North Carolina, a cytology-free assay was developed and adapted for lateral flow detection using two biomarkers, P16INK4A and KRT7. This project was ultimately part of an effort to implement self-collection for primary HPV testing in community health centers and has directly informed efforts to implement self-collection in the United States to improve cervical cancer screening rates especially for rural and underserved communities.16,17 HPV self-collection has major potential to improve cervical cancer screening and, coupled with an affordable, portable, and rapid diagnostic, such as a lateral flow test,2 could result in a significant improvement in early detection and diagnosis of cervical cancer in low-resource settings. ACTs likewise supported a partnership between New York University, the University of Cape Town, and Cepheid to advance and evaluate the Xpert HPV assay for use in a single-visit, screen-and-treat paradigm.18 This study further demonstrated the safety and feasibility of screen-and-treat as a strategy in low-resource, primary care settings. ACTs is also currently supporting the development of two HPV diagnostics that are leveraging clustered regularly interspaced short palindromic repeats to enable highly specific testing for multiple high-risk HPV types at the POC.19-22
To date, 14 ACTs projects have focused on cervical cancer. In addition to HPV diagnostics, ACTs has supported the development of several enabling technologies for treatment of cervical precancer, especially that rely on nonexcisional (ie, surgical removal of cervix) approaches. Using cold-based (cryotherapy) or heat-based (thermal ablation) nonsurgical approaches to destroy precancerous cells of the cervix offer significant advantages. These methods can be easier to task-shift to nonphysician health care providers including nurses and midwives, and can be performed in conjunction with POC screening methods as part of a see-and-treat paradigm for cervical cancer prevention. Although cryotherapy has been widely used, this approach has been associated with high rates of recurrence. Furthermore, traditional cryotherapy requires reliable supply of cryogenic gases (liquid nitrous oxide or liquid carbon dioxide), which can present significant logistical and procurement challenges in many settings. Alternatives that have been evaluated in the ACTs program include portable, low-cost cryotherapy devices that rely on battery power to achieve freezing temperatures, for example, CryoPop developed by Jhpiego that enhances the efficiency of CO2 use by reducing the amount needed for effective treatment and delivers comparable performance over the freeze cycle.23,24 Thermal ablation, which involves heat coagulation, has traditionally had better outcomes than cryotherapy, and the emergence of portable, battery-operated thermal ablation devices supported by the ACTs program represent a major advance, given that these devices overcome the logistical challenges of gas supply. An ACTs-supported randomized trial in Zambia evaluated safety and efficacy of a portable thermal ablation device (manufactured by Liger Medical, Lehi, UT) versus traditional cryotherapy or large loop electrosurgical excision of transformation zone.25,26 The study demonstrated that the portable thermal ablation device had an excellent safety profile and comparable efficacy to traditional cryotherapy and excision, although response rates were lower for women with HIV across all treatment modalities. ACTs studies on precancer treatment have bridged key gaps in evidence to directly inform international consensus guidelines and program implementation for cervical cancer prevention worldwide.27,28
HIV and HIV-Associated Malignancies
HIV and cancer have significant overlap in many LMIC settings, and even with advancements in antiretroviral therapy access, there is a persistent increase in cancer risk among people with HIV.29 To this end, in many contexts, it has been important to specifically focus on individuals with HIV, as in the Zambia studies evaluating thermal ablation for cervical precancer treatment cited above.25,26
ACTs has also supported several projects focused explicitly on HIV-associated malignancies. One such project, a collaboration of investigators from several US and Ugandan institutions, developed a POC diagnostic, known as the Tiny Isothermal Nucleic acid quantification sYstem (TINY), for loop-mediated isothermal amplification–based quantification of Kaposi sarcoma (KS)–associated herpesvirus from KS-suspected biopsies.30 Working at the point of need in Uganda led the engineering team to adapt their original platform so it could operate from a variety of power sources (electricity, sunlight, and open flame), allowing operability in and out of laboratory settings and the ability to store heat from intermittent energy sources to allow for operation when electricity is not readily available.31 The group has continued to adapt the device to simplify usability by integrating their SLICER system, which processes samples into microcores that can be directly used with TINY, as well as an optimized, equipment-free DNA extraction, allowing for a more streamlined test and has expanded study sites to include Kenya, Tanzania, Rwanda, Botswana, and Malawi.32,33
Other Novel Cancer Diagnostics
The rapid democratization of artificial intelligence (AI) models for image analysis has also driven the development of new, low-cost technologies for cancer diagnosis. For example, in collaboration with Tata Memorial Center, Investigators from Emory University are integrating AI-pathomic tools within PathPresenter,34 a global image sharing platform for pathology, to establish an AI-enabled Digital Pathology Platform for multicancer diagnosis, prognosis, and prediction of therapeutic benefit. ADAPT is being optimized and validated for breast cancer, oral cavity squamous cell carcinoma, and prostate cancer for (1) prognosticating recurrence, (2) predicting pathologic complete response to neoadjuvant chemotherapy, (3) predicting benefit of adjuvant chemotherapy and radiotherapy, and (4) identifying individuals in whom radiation therapy can be deintensified.35-38
ACTs investigators have likewise taken advantage of advances in optics to create POC imaging platforms for cancer detection and diagnosis. Further development of a high-resolution microendoscope (HRME) with subcellular resolution imaging capabilities was developed and tested for the detection of cervical and colorectal cancer. HRME consists of a thin-flexible fiber optic probe, with a light source and camera, and uses a laptop or tablet-based processor to display the image.39-41 HRME has also been deployed in a mobile unit, to provide access for cervical cancer screening in remote settings. ACTs supported groups from Massachusetts General Hospital, University of Massachusetts, and University of Arizona are developing an integrated Screen, Image and Treat Optical System (SITOS) for the screening and image-guided photodynamic therapy of premalignant and malignant oral lesions. SITOS, a low-cost device for intraoral imaging, includes a battery-operated light source for photodynamic therapy, integrated into a handheld mobile device, using a cloud-based AI approach for image classification to enable image-guided photodynamic therapy.42-45 SITOS is being tested in clinical trials to be conducted at various sites in India.
Cancer Treatment
Several enabling technologies for treatment have also been supported. ACTs supported the development of the Radiation Planning Assistant (RPA), a US Food and Drug Administration–cleared, web-based, deep learning tool codesigned and developed in the United States and South Africa to address critical workforce shortages in radiation oncology in LMICs, while similarly streamlining workflow and reducing costs of radiotherapy for patients with cancer in the United States.46-48 Recent studies of RPA output, reviewed by specialists from 16 institutions in six countries, showed that more than 90% of plans were clinically acceptable with minor edits and most plans were clinically acceptable without edits.49 The ACTs program is currently supporting a prospective evaluation of the RPA in four countries to assess the quality of plans, quantify time-savings, and determine how this translates into cost-savings. Another ACTs project is developing a ring compensator system leveraging 3D-printed molds and reusable tungsten beads as a cost-effective replacement for the costly and difficult-to-repair multileaf collimators typically used to shape the photon beam in intensity-modulated radiotherapy (IMRT).50-52 This technology offers the promise of enabling affordable, state-of-the-art IMRT in settings where it is currently out of reach.
Many LMICs face resource constraints that limit their ability to test the quality of chemotherapy medicines before administration. A team led by investigators at the University of Notre Dame are validating Chemotherapeutic Paper Analytical Device (ChemoPAD), which combines simple thin-layer chromatography on paper with a free phone app to detect quality of chemotherapy at the POC.53-55 ChemoPAD is currently being validated in Ethiopia, Malawi, Cameroon, and Kenya. Finally, ACTs is currently supporting the further development of the KeyScope for laparoscopic cancer surgery. KeyScope, developed as a collaboration between Duke University, University of Maryland, and Makerere University, is a single-unit system operable in settings with variable power and compatible with submersion sterilization that addresses the capital costs of equipment, maintenance and repair, as well as the disposable costs that keep laparoscopic surgery out of reach in most LMIC settings.56,57 The device is being developed and built in Uganda, ensuring sustainability and low cost. This project is a result of a multidisciplinary collaboration between surgeons, engineers, oncologists, and global health experts. Such collaborations are a hallmark of the ACTs program and essential for the development of devices that can be maintained and used in setting for which they have been developed.
DISCUSSION AND FUTURE DIRECTIONS
Addressing global cancer control extends beyond technological advancements; it also requires fostering trust and engagement within local populations. Historical mistrust of foreign-funded research can hinder the adoption of new medical interventions. Establishing robust partnerships with local communities, health care systems, and regulatory agencies is essential to ensure the successful implementation of novel cancer technologies. Strengthening research infrastructure and focusing on patient-centered outcomes can enhance the relevance and accessibility of new technologies.58 Over the 10 years of the ACTs program, there has been an increasing focus on explicitly requiring the kind of parity and shared leadership that has become an expectation in the global health community. This shift has resulted in LMIC investigators as key personnel on all projects, intellectual leadership from LMIC scientists at all levels of projects, and the technologies designed by engaging LMIC end-users at the earliest stages. A potential consequence of these strong partnerships is that, in the face of the COVID-19 pandemic and other large-scale disruptions, ACTs projects successfully met key milestones and delivered the results discussed in this paper. Nonetheless, there continues to be a tendency for technology development to flow from HIC settings to LMIC settings, offering room for growth and bidirectional learning in the next decade of the ACTs program.
There is a growing emphasis in both LMICs and the United States on decentralized, community-based health care models that leverage POC technologies to bring cancer detection and treatment closer to the populations in need.59 Strengthening health systems through digital health innovations, workforce training, and regulatory harmonization is crucial to ensuring access to quality cancer care. Public-private partnerships and international collaborations can accelerate the availability of proven cancer control technologies in underserved regions, ultimately reducing global disparities in cancer diagnosis, treatment, and survival outcomes.
ACTs investigators have faced some challenges advancing affordable and deployable technologies beyond the research stages. Market disincentives have made it challenging for investigators to commercialize and scale their technologies. Specifically, larger manufacturers have been hesitant to license and further develop these lower-cost technologies because of perceptions around potentially limited returns on investment. There is likewise limited venture capital in global health. Finally, a lack of consistent, harmonized regulatory pathways makes introducing technologies into LMIC markets challenging. As such, efforts beyond technology development and clinical validation are needed to ensure that technologies can be introduced successfully into the continuum of care in LMICs. There is a need for both creative financing and technology development approaches, including intentional codesign approaches with US health care centers, to garner interest from US and other HIC industry and venture funds.
Interventions developed in LMIC health settings have significant potential to increase access to quality cancer care in the United States and other HICs as well. Although ACTs have been developed for specific cancer control challenges in LMICs, scalability is key to broadening reach, impact, affordability, adoption, and sustainability. A variety of partnership models between researchers in HICs and LMICs have been adopted across the ACTs consortium to advance science and translation, as well as drive commercialization and adoption, including for many US small businesses seeking to develop products to address cancer control challenges in LMICs and access global markets. Understanding the enablers and facilitators of these successes will be a primary goal for the future. Moreover, reciprocal innovation has emerged in recent years as a formalized approach to research focused on translating innovations developed in LMICs to other settings, especially HICs. Rid et al60 suggest that such work involves two ethical commitments: (1) promoting work to adapt health innovations from LMICs for use in HICs or developing innovations in LMICs and HICs and (2) committing researchers from LMICs and HICs to work collaboratively on such work. Future work in the ACTs program should explicitly seek to build on these models. Although at times complex, such efforts to successfully codesign and develop new technologies can increase the potential market and impact for resultant technologies.
Supporting the next generation of global cancer control technologies represents a transformative opportunity to bridge gaps in cancer care. The ACTs program has fostered the development of innovative, affordable, and scalable solutions tailored for resource-limited settings worldwide. Emerging technologies are being designed to improve accessibility and enhance patient outcomes through cost-effective and user-friendly innovations.
Portable and battery-powered devices—Several ACTs projects supported ablative technologies, but the versatility of these advancements extends beyond cervical cancer. Their portability and ease of use make them well suited for decentralized cancer care, expanding their accessibility in diverse settings where conventional therapies are often unavailable. The development of battery-powered handheld thermal ablation units and non–gas cryotherapy devices is revolutionizing treatment methodologies through single-visit screen-and-treat approaches.25,61 Notably, devices powered by Stirling coolers and alternative energy sources bolster sustainability in remote health care settings, providing capabilities for immediate treatment after a diagnosis. This timely intervention reduces the likelihood of loss to follow-up, thereby significantly improving patient outcomes even in locales where surgical and radiation therapies are limited.
AI-driven solutions—As evidenced from several of the projects, AI-assisted tools are emerging as powerful assets in LMICs. Proposed applications span computer-aided detection/diagnosis, risk assessment, disease prediction, and surveillance. Given workforce and infrastructure limitations, AI tools are particularly poised to revolutionize and increase access to timely and accurate cancer diagnostics. Machine learning algorithms capable of automating cytology and histopathology play a critical role in bridging workforce shortages by empowering nonspecialist health care workers to conduct accurate and rapid diagnostics.62 AI-driven digital pathology platforms facilitate early detection and streamline decision-making processes, making cancer diagnostics more accessible in underserved regions.63 Enhanced imaging techniques using AI can improve the diagnosis and management of malignancies across multiple organ systems, thus offering scalable solutions for early cancer detection.
Point-of-care biomarker testing—Advancements in molecular diagnostics are paving the way for POC biomarker testing that can be deployed in resource-limited settings.64,65 Innovations such as portable HPV DNA testing present promising alternatives for early cancer detection, especially in regions where laboratory infrastructure is lacking. These diagnostic breakthroughs contribute to earlier interventions and significantly improve patient prognoses. The expansion of biomarker testing to include critical markers further enhances the potential for early detection and personalized treatment strategies in LMICs.
Digital and mHealth solutions—Digital platforms and mobile applications are transforming patient engagement, follow-up care, and remote consultations in cancer care.66,67 By leveraging telemedicine, LMICs can expand access to specialized oncologists and advance the decentralization of health services. mHealth solutions improve communication between patients and health care providers, ensuring continuity of care in resource-constrained environments. Remote monitoring and telepathology applications can complement cancer care pathways, thereby reducing delays in treatment initiation and promoting overall system efficiency while maintaining high-quality evidence-based care.
3D printing for medical devices and prosthetics—The emergence of 3D printing technologies is revolutionizing global cancer care. This innovative approach allows for low-cost production of medical devices, prosthetics, and surgical models tailored to individual patient needs.68,69 This capability is particularly advantageous in LMICs, where costs associated with traditional medical equipment procurement can be prohibitive. Applications in oncology include creating patient-specific implants and surgical guides for tumor resections.
Wearable and sensor-based technologies—Advancements in wearable health monitoring devices allow for continuous tracking of vital signs, early detection of complications, and personalized cancer treatment monitoring.70,71 These technologies improve treatment adherence and reduce the need for frequent hospital visits while providing real-time health insights for both patients and health care providers. Wearable biosensors and monitoring technologies have the potential to track biomarkers for the early detection of several cancers, thus enabling proactive cancer management in environments where routine screenings are often unavailable.
In conclusion, the ACTs program demonstrates US and NCI leadership in supporting a broad portfolio of technologies for cancer control in LMICs. It has ushered in new platforms for further research and development, led to commercial products, and directly affected health programming. Over the course of the intervening 10 years, new technologies have emerged, prompting a new generation of US and LMIC ACTs investigators to pursue more sophisticated targets and leveraging new analytic methods. As these technologies evolve, the focus must remain on ensuring their affordability, regulatory approval, and integration into existing health care systems worldwide, including the United States, where applicable. Collaborative efforts between researchers, policymakers, industry partners, and local stakeholders are essential for scaling these innovations and making them sustainable for long-term impact worldwide. The success of the ACTs program over the past decade showcases the potential of targeted investment in technology-driven solutions for global cancer control, setting the stage for continued progress in the coming years.
DISCLAIMER
This is a US Government work. There are no restrictions on its use. The opinions expressed by the authors are their own and this material should not be interpreted as representing the official viewpoint of the US Department of Health and Human Services, the National Institutes of Health, or the National Cancer Institute.
AUTHOR CONTRIBUTIONS
Conception and design: Paul C. Pearlman, Rao Divi, Rebecca Huppi, Srivatsan Kidambi, Pushpa Tandon, Miguel Ossandon, Ophira Ginsburg, Satish Gopal
Financial support: Satish Gopal
Administrative support: Satish Gopal
Provision of study materials or patients: Satish Gopal
Collection and assembly of data: Paul C. Pearlman, Elise Garton, Satish Gopal
Data analysis and interpretation: Paul C. Pearlman, Ophira Ginsburg, Satish Gopal
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/go/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
No potential conflicts of interest were reported.
REFERENCES
- 1. Pearlman PC, Divi R, Gwede M, et al. The National Institutes of Health affordable cancer technologies program: Improving access to resource-appropriate technologies for cancer detection, diagnosis, monitoring, and treatment in low- and middle-income countries. IEEE J Transl Eng Health Med. 2016;4:2800708. doi: 10.1109/JTEHM.2016.2604485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Haney K, Tandon P, Divi R, et al. The role of affordable, point-of-care technologies for cancer care in low- and middle-income countries: A review and commentary. IEEE J Transl Eng Health Med. 2017;5:2800514. doi: 10.1109/JTEHM.2017.2761764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Varmus H, Trimble EL. Integrating cancer control into global health. Sci Transl Med. 2011;3:101cm28. doi: 10.1126/scitranslmed.3002321. [DOI] [PubMed] [Google Scholar]
- 4.National Institutes of Health, Fogarty International Center . Mobile Health Technology and Outcomes in LMICs (R21 R33) Fogarty International Center; n.d.. https://www.fic.nih.gov/Programs/Pages/mhealth.aspx [Google Scholar]
- 5.Digital Science . Dimensions. 2018. https://app.dimensions.ai under licence agreement. [Google Scholar]
- 6.International Cancer Research Partnership . Common Scientific Outline (CSO) 2023. https://www.icrpartnership.org/cso [Google Scholar]
- 7. Pramesh CS, Badwe RA, Bhoo-Pathy N, et al. Priorities for cancer research in low- and middle-income countries: A global perspective. Nat Med. 2022;28:649–657. doi: 10.1038/s41591-022-01738-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.National Institutes of Health . RCDC: Categorization Process. NIH RePORT. n.d.. https://report.nih.gov/funding/categorical-spending/rcdc-process [Google Scholar]
- 9. Hasnain AC, Stark A, Trick AY, et al. Cancer methylation biomarker detection in an automated, portable, multichannel magnetofluidic platform. ACS Nano. 2024;18:12105–12116. doi: 10.1021/acsnano.3c10070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ma K, Kalra A, Tsai HL, et al. Accurate nonendoscopic detection of esophageal squamous cell carcinoma using methylated DNA biomarkers. Gastroenterology. 2022;163:507–509 e2. doi: 10.1053/j.gastro.2022.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Stark A, Shin DJ, Wang TH. A sample-to-answer droplet magnetofluidic assay platform for quantitative methylation-specific PCR. Biomed Microdevices. 2018;20:31. doi: 10.1007/s10544-018-0276-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Stark A, Trick A, Pisanic TR, II, et al. Droplet magnetofluidic assay platform for quantitative methylation-specific PCR. Methods Mol Biol. 2022;2394:199–209. doi: 10.1007/978-1-0716-1811-0_13. [DOI] [PubMed] [Google Scholar]
- 13. Deng L, Ismond K, Liu Z, et al. Urinary metabolomics to identify a unique biomarker panel for detecting colorectal cancer: A multicenter study. Cancer Epidemiol Biomarkers Prev. 2019;28:1283–1291. doi: 10.1158/1055-9965.EPI-18-1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhang L, Zheng J, Ismond KP, et al. Identification of urinary biomarkers of colorectal cancer: Towards the development of a colorectal screening test in limited resource settings. Cancer Biomark. 2023;36:17–30. doi: 10.3233/CBM-220034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bhattacharyya D, LeVatte MA, Wishart DS. A fast and accurate colorimetric assay for quantifying hippuric acid in human urine. Anal Biochem. 2023;680:115303. doi: 10.1016/j.ab.2023.115303. [DOI] [PubMed] [Google Scholar]
- 16. Le A, Rohweder C, Wheeler SB, et al. Self-collection for primary HPV testing: Perspectives on implementation from federally qualified health centers. Prev Chronic Dis. 2023;20:E93. doi: 10.5888/pcd20.230056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Le A, Wheeler SB, Lafata JE, et al. Self-collection for HPV testing: Potential issues related to performance measures and quality improvement among federally qualified health centers. J Public Health Manag Pract. 2024;30:688–700. doi: 10.1097/PHH.0000000000001913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Denny L, Saidu R, Boa R, et al. Point-of-care testing with Xpert HPV for single-visit, screen-and-treat for cervical cancer prevention: A demonstration study in South Africa. Sci Rep. 2023;13:16182. doi: 10.1038/s41598-023-43467-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Guan X, Yang R, Zhang J, et al. Programmable multiplexed nucleic acid detection by harnessing specificity defect of CRISPR-cas12a. Adv Sci (Weinh) 2025;12:e2411021. doi: 10.1002/advs.202411021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Yang R, Guan X, Zhang J, et al. Quencher-free CRISPR-based molecular detection using an amphiphilic DNA fluorescence probe. Biosens Bioelectron. 2025;271:117054. doi: 10.1016/j.bios.2024.117054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lee CY, Kim H, Degani I, et al. Empowering the on-site detection of nucleic acids by integrating CRISPR and digital signal processing. Nat Commun. 2024;15:6271. doi: 10.1038/s41467-024-50588-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Roh YH, Lee CY, Lee S, et al. CRISPR-enhanced hydrogel microparticles for multiplexed detection of nucleic acids. Adv Sci (Weinh) 2023;10:e2206872. doi: 10.1002/advs.202206872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Anderson JR, Yogeshkumar S, Lu E, et al. The CryoPop study: Screening for high-grade cervical dysplasia in Karnataka, India. BJOG. 2023;130(suppl 3):158–167. doi: 10.1111/1471-0528.17702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Yogeshkumar S, Anderson J, Lu E, et al. Safety and efficacy of the new CryoPop® cryotherapy device for cervical dysplasia in low- and middle-income countries: Study protocol for a multicenter open-label non-inferiority clinical trial with historical controls. Trials. 2021;22:915. doi: 10.1186/s13063-021-05802-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Basu P, Mwanahamuntu M, Pinder LF, et al. A portable thermal ablation device for cervical cancer prevention in a screen-and-treat setting: A randomized, noninferiority trial. Nat Med. 2024;30:2596–2604. doi: 10.1038/s41591-024-03080-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Pinder LF, Parham GP, Basu P, et al. Thermal ablation versus cryotherapy or loop excision to treat women positive for cervical precancer on visual inspection with acetic acid test: Pilot phase of a randomised controlled trial. Lancet Oncol. 2020;21:175–184. doi: 10.1016/S1470-2045(19)30635-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.WHO Guideline for Screening and Treatment of Cervical Pre-cancer Lesions for Cervical Cancer Prevention. Geneva: 2021. [PubMed] [Google Scholar]
- 28.WHO Guidelines for the Use of Thermal Ablation for Cervical Pre-cancer Lesions. Geneva: 2019. [PubMed] [Google Scholar]
- 29. Odeny TA, Fink V, Muchengeti M, et al. Cancer in people with HIV. Infect Dis Clin North Am. 2024;38:531–557. doi: 10.1016/j.idc.2024.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. McCloskey D, Semeere A, Ayanga R, et al. LAMP-enabled diagnosis of Kaposi's sarcoma for sub-Saharan Africa. Sci Adv. 2023;9:eadc8913. doi: 10.1126/sciadv.adc8913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Snodgrass R, Gardner A, Semeere A, et al. A portable device for nucleic acid quantification powered by sunlight, a flame or electricity. Nat Biomed Eng. 2018;2:657–665. doi: 10.1038/s41551-018-0286-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Manning JC, Boza JM, Cesarman E, et al. Rapid, equipment-free extraction of DNA from skin biopsies for point-of-care diagnostics. Sci Rep. 2024;14:13782. doi: 10.1038/s41598-024-64533-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nutt D. Portable Cancer Testing Expands in Sub-saharan Africa. Cornell Chronicle; 2022. https://news.cornell.edu/stories/2022/08/portable-cancer-testing-expands-sub-saharan-africa [Google Scholar]
- 34.PathPresenter n.d.. https://www.pathpresenter.com
- 35. Chen Y, Li H, Janowczyk A, et al. Computational pathology improves risk stratification of a multi-gene assay for early stage ER+ breast cancer. NPJ Breast Cancer. 2023;9:40. doi: 10.1038/s41523-023-00545-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Koyuncu CF, Frederick MJ, Thompson LDR, et al. Machine learning driven index of tumor multinucleation correlates with survival and suppressed anti-tumor immunity in head and neck squamous cell carcinoma patients. Oral Oncol. 2023;143:106459. doi: 10.1016/j.oraloncology.2023.106459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Wang X, Barrera C, Bera K, et al. Spatial interplay patterns of cancer nuclei and tumor-infiltrating lymphocytes (TILs) predict clinical benefit for immune checkpoint inhibitors. Sci Adv. 2022;8:eabn3966. doi: 10.1126/sciadv.abn3966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Serafin R, Koyuncu C, Xie W, et al. Nondestructive 3D pathology with analysis of nuclear features for prostate cancer risk assessment. J Pathol. 2023;260:390–401. doi: 10.1002/path.6090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Louie JS, Shukla R, Richards-Kortum R, et al. High-resolution microendoscopy in differentiating neoplastic from non-neoplastic colorectal polyps. Best Pract Res Clin Gastroenterol. 2015;29:663–673. doi: 10.1016/j.bpg.2015.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Grant BD, Fregnani JHTG, Possati Resende JC, et al. High-resolution microendoscopy: A point-of-care diagnostic for cervical dysplasia in low-resource settings. Eur J Cancer Prev. 2017;26:63–70. doi: 10.1097/CEJ.0000000000000219. [DOI] [PubMed] [Google Scholar]
- 41. Tang Y, Kortum A, Parra SG, et al. In vivo imaging of cervical precancer using a low-cost and easy-to-use confocal microendoscope. Biomed Opt Express. 2020;11:269–280. doi: 10.1364/BOE.381064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Song B, Sunny S, Uthoff RD, et al. Automatic classification of dual-modalilty, smartphone-based oral dysplasia and malignancy images using deep learning. Biomed Opt Express. 2018;9:5318–5329. doi: 10.1364/BOE.9.005318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Uthoff RD, Song B, Sunny S, et al. Point-of-care, smartphone-based, dual-modality, dual-view, oral cancer screening device with neural network classification for low-resource communities. PLoS One. 2018;13:e0207493. doi: 10.1371/journal.pone.0207493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Khan S, Song BF, Mallidi S, et al. Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic and Photobiomodulation Therapy, Volume 11940. 2022. Clinical assessment of a low-cost, hand-held, smartphone-attached intraoral imaging probe for ALA PDT monitoring and guidance. [DOI] [Google Scholar]
- 45. Siddiqui SA, Siddiqui S, Hussain MAB, et al. Clinical evaluation of a mobile, low-cost system for fluorescence guided photodynamic therapy of early oral cancer in India. Photodiagnosis Photodyn Ther. 2022;38:102843. doi: 10.1016/j.pdpdt.2022.102843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Court LE, Kisling K, McCarroll R, et al. Radiation planning assistant—A streamlined, fully automated radiotherapy treatment planning system. J Vis Exp. 2018;134:57411. doi: 10.3791/57411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Nealon KA, Balter PA, Douglas RJ, et al. Using failure mode and effects analysis to evaluate risk in the clinical adoption of automated contouring and treatment planning tools. Pract Radiat Oncol. 2022;12:e344–e353. doi: 10.1016/j.prro.2022.01.003. [DOI] [PubMed] [Google Scholar]
- 48. Court L, Aggarwal A, Burger H, et al. Addressing the global expertise gap in radiation oncology: The radiation planning assistant. JCO Glob Oncol. doi: 10.1200/GO.22.00431. 10.1200/GO.22.00431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Court LE, Aggarwal A, Jhingran A, et al. Artificial intelligence-based radiotherapy contouring and planning to improve global access to cancer care. JCO Glob Oncol. doi: 10.1200/GO.23.00376. 10.1200/GO.23.00376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ford E. Humanitarian Engineering for Global Oncology. Bristol England, United Kingdom: IOP Publishing; 2024. [Google Scholar]
- 51. Sengupta B, Oh K, Sponseller P, et al. Cobalt compensator-based IMRT device: A treatment planning study of head and neck cases. Phys Med. 2023;106:102526. doi: 10.1016/j.ejmp.2023.102526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Zaki P, Sengupta B, Oh K, et al. Cobalt compensator-based IMRT for gynecologic cancer treatment in low- and middle-income countries: Equivalence to LINAC-based IMRT. Int J Radiat Oncol Biol Phys. 2023;117:S81. [Google Scholar]
- 53. Roller RM, Rea A, Lieberman M. The air-gap PAD: A roll-to-roll-compatible fabrication method for paper microfluidics. Lab Chip. 2023;23:1918–1925. doi: 10.1039/d2lc01164f. [DOI] [PubMed] [Google Scholar]
- 54. Saidu Y, Nchinjoh SC, Adidja A, et al. Anticipating and strategizing to address potential bottlenecks during clinical research projects in sub-Saharan Africa: A case for adapting approaches and tools used in the entrepreneurial and development sectors. Trials. 2024;25:105. doi: 10.1186/s13063-023-07897-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Smith M, Ashenef A, Lieberman M. Paper analytic device to detect the presence of four chemotherapy drugs. JCO Glob Oncol. doi: 10.1200/JGO.18.00198. 10.1200/JGO.18.00198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Barnes AC, Kaluzienski ML, Chen J, et al. Improved performance and design of a low-cost laparoscope to enable laparoscopic surgery in low-income countries. Biophotonics Discov. 2025;2:022302. [Google Scholar]
- 57. Barnes AC, Kaluzienski M, Quang T, et al. Development of a portable testing chamber to assess imaging performance of laparoscopes in low- and middle-income countries. J Biomed Opt. 2025;30:016001. doi: 10.1117/1.JBO.30.1.016001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Monge C, Eldridge L, Pearlman PC, et al. Global perspectives on patient-centered outcomes: Advancing patient-centered cancer clinical trials globally. J Natl Cancer Inst Monogr. 2025;2025:35–41. doi: 10.1093/jncimonographs/lgae043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Romero Y, Tittenbrun Z, Trapani D, et al. The changing global landscape of national cancer control plans. Lancet Oncol. 2025;26:e46–e54. doi: 10.1016/S1470-2045(24)00405-4. [DOI] [PubMed] [Google Scholar]
- 60. Rid A, Aguilera B, Banda C, et al. Global health reciprocal innovation: Ethical, legal and regulatory considerations. BMJ Glob Health. 2024;8:e014693. doi: 10.1136/bmjgh-2023-014693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Selmouni F, Sauvaget C, Dangbemey DP, et al. Lessons learnt from pilot cervical cancer screening and treatment programmes integrated to routine primary health care services in Benin, Cote d'Ivoire, and Senegal. JCO Glob Oncol. doi: 10.1200/GO.22.00051. 10.1200/GO.22.00051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Aggarwal A, Bharadwaj S, Corredor G, et al. Artificial intelligence in digital pathology—Time for a reality check. Nat Rev Clin Oncol. 2025;22:283–291. doi: 10.1038/s41571-025-00991-6. [DOI] [PubMed] [Google Scholar]
- 63. Chen S, Ding P, Guo H, et al. Applications of artificial intelligence in digital pathology for gastric cancer. Front Oncol. 2024;14:1437252. doi: 10.3389/fonc.2024.1437252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Ng XJK, Mohd Khairuddin AS, Liu HC, et al. Artificial intelligence-assisted point-of-care devices for lung cancer. Clin Chim Acta. 2025;570:120191. doi: 10.1016/j.cca.2025.120191. [DOI] [PubMed] [Google Scholar]
- 65. Kalligosfyri PM, Lamprou E, Kalogianni DP. Emerging sensing technologies for liquid biopsy applications: Steps closer to personalized medicine. Sensors (Basel) 2024;24:7902. doi: 10.3390/s24247902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Moghul M, Cazzaniga W, Croft F, et al. Mobile health solutions for prostate cancer diagnostics—A systematic review. Clin Pract. 2023;13:863–872. doi: 10.3390/clinpract13040078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Bergerot CD, Bergerot PG, Philip EJ, et al. Enhancing cancer supportive care: Integrating psychosocial support, nutrition, and physical activity using telehealth solutions. JCO Glob Oncol. doi: 10.1200/GO-24-00333. 10.1200/GO-24-00333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. McGarry CK, Tonino Baldion A, Burnley J, et al. IPEM topical report: Guidance on 3D printing in radiotherapy. Phys Med Biol. 2025;70:04TR01. doi: 10.1088/1361-6560/ada518. [DOI] [PubMed] [Google Scholar]
- 69. Thacharodi A, Singh P, Meenatchi R, et al. Revolutionizing healthcare and medicine: The impact of modern technologies for a healthier future—A comprehensive review. Health Care Sci. 2024;3:329–349. doi: 10.1002/hcs2.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Goncalves Leite Rocco P, Reategui-Rivera CM, Finkelstein J. Telemedicine applications for cancer rehabilitation: Scoping review. JMIR Cancer. 2024;10:e56969. doi: 10.2196/56969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Lu T, Ji S, Jin W, et al. Biocompatible and long-term monitoring strategies of wearable, ingestible and implantable biosensors: Reform the next generation healthcare. Sensors (Basel) 2023;23:2991. doi: 10.3390/s23062991. [DOI] [PMC free article] [PubMed] [Google Scholar]