

Abstract
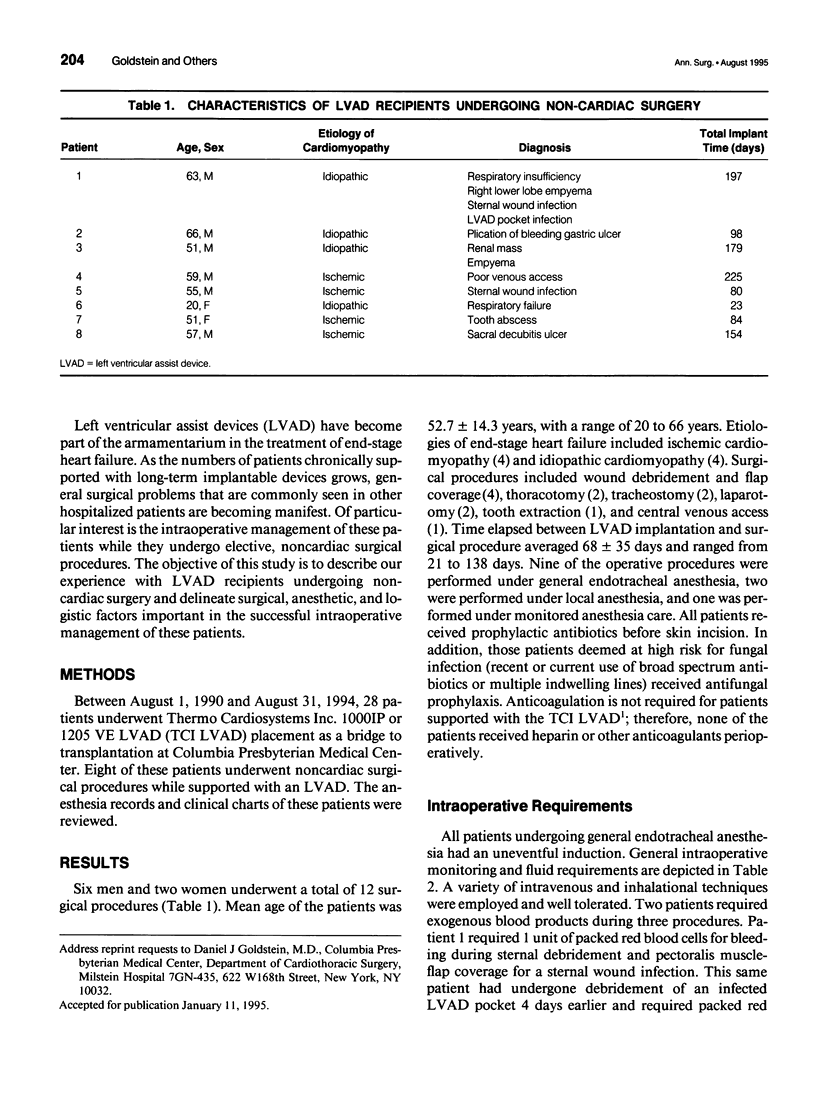
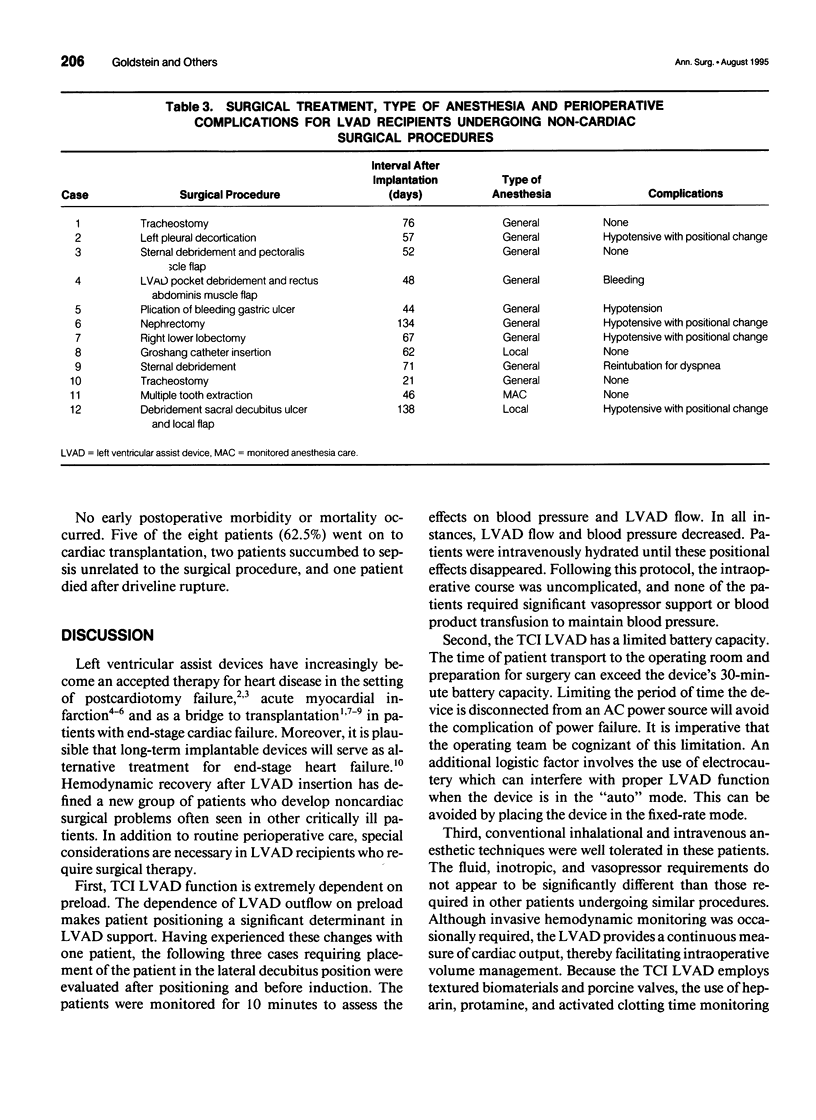
OBJECTIVE: The authors describe their experience with left ventricular assist-device (LVAD) recipients undergoing noncardiac surgery and delineate surgical, anesthetic, and logistic factors important in the successful intraoperative management of these patients. SUMMARY BACKGROUND DATA: Left ventricular assist-devices have become part of the armamentarium in the treatment of end-stage heart failure. As the numbers of patients chronically supported with long-term implantable devices grows, general surgical problems that are commonly seen in other hospitalized patients are becoming manifest. Of particular interest is the intraoperative management of patients undergoing elective noncardiac surgical procedures. METHODS: The anesthesia records and clinical charts were reviewed for eight ventricular assist-device recipients undergoing general surgical procedures between August 1, 1990 and August 31, 1994. RESULTS: A total of 12 procedures were performed in 6 men and 2 women averaging 52.7 years of age. Mean time elapsed from device implantation to operation was 68 +/- 35 days. Conventional inhalational and intravenous anesthetic techniques were well tolerated in these patients undergoing diverse surgical procedures. No perioperative mortality was observed. Five of eight patients went on to successful cardiac transplantation. CONCLUSIONS: Hemodynamic recovery after LVAD insertion has defined a new group of patients who develop noncardiac surgical problems often seen in other critically ill patients. Recognition of the unique potential problems that the LVAD recipient may encounter in the perioperative period--in particular patient positioning, device limitations, and fluid and inotropic management--will ensure an optimal surgical outcome for LVAD recipients undergoing noncardiac surgery.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Deeb G. M., Bolling S. F., Nicklas J., Walsh R. S., Steimle C. N., Shea M. J., Meagher J. S. Clinical experience with the Nimbus pump. ASAIO Trans. 1990 Jul-Sep;36(3):M632–M636. [PubMed] [Google Scholar]
- Frazier O. H., Rose E. A., Macmanus Q., Burton N. A., Lefrak E. A., Poirier V. L., Dasse K. A. Multicenter clinical evaluation of the HeartMate 1000 IP left ventricular assist device. Ann Thorac Surg. 1992 Jun;53(6):1080–1090. doi: 10.1016/0003-4975(92)90393-i. [DOI] [PubMed] [Google Scholar]
- Frazier O. H. The development of an implantable, portable, electrically powered left ventricular assist device. Semin Thorac Cardiovasc Surg. 1994 Jul;6(3):181–187. [PubMed] [Google Scholar]
- Jett G. K. Postcardiotomy support with ventricular assist devices: selection of recipients. Semin Thorac Cardiovasc Surg. 1994 Jul;6(3):136–139. [PubMed] [Google Scholar]
- McBride L. R. Bridging to cardiac transplantation with external ventricular assist devices. Semin Thorac Cardiovasc Surg. 1994 Jul;6(3):169–173. [PubMed] [Google Scholar]
- McGee M. G., Parnis S. M., Nakatani T., Myers T., Dasse K., Hare W. D., Duncan J. M., Poirier V. L., Frazier O. H. Extended clinical support with an implantable left ventricular assist device. ASAIO Trans. 1989 Jul-Sep;35(3):614–616. doi: 10.1097/00002480-198907000-00145. [DOI] [PubMed] [Google Scholar]
- Moritz A., Wolner E. Circulatory support with shock due to acute myocardial infarction. Ann Thorac Surg. 1993 Jan;55(1):238–244. doi: 10.1016/0003-4975(93)90530-u. [DOI] [PubMed] [Google Scholar]
- Pennington D. G., McBride L. R., Peigh P. S., Miller L. W., Swartz M. T. Eight years' experience with bridging to cardiac transplantation. J Thorac Cardiovasc Surg. 1994 Feb;107(2):472–481. [PubMed] [Google Scholar]
- Pennington D. G., Merjavy J. P., Swartz M. T., Codd J. E., Barner H. B., Lagunoff D., Bashiti H., Kaiser G. C., Willman V. L. The importance of biventricular failure in patients with postoperative cardiogenic shock. Ann Thorac Surg. 1985 Jan;39(1):16–26. doi: 10.1016/s0003-4975(10)62516-7. [DOI] [PubMed] [Google Scholar]
- Smalling R. W., Sweeney M., Lachterman B., Hess M. J., Morris R., Anderson H. V., Heibig J., Li G., Willerson J. T., Frazier H. Transvalvular left ventricular assistance in cardiogenic shock secondary to acute myocardial infarction. Evidence for recovery from near fatal myocardial stunning. J Am Coll Cardiol. 1994 Mar 1;23(3):637–644. doi: 10.1016/0735-1097(94)90748-x. [DOI] [PubMed] [Google Scholar]