

Abstract
OBJECTIVE: The authors review the Pennsylvania Health Care Cost Containment Council reports on coronary artery surgery and compare this reporting structure to others, including the Society for Thoracic Surgeons database, currently used by their own program. The authors review the growing likelihood of a need for outcome measures for all of the surgical subspecialties. SUMMARY AND BACKGROUND DATA: Pressure from consumers and insurers will require surgical specialties to be graded by objective outcome measures. Practitioners must be prepared and become involved in the process. METHODS: The authors reviewed the data, which grades all of Pennsylvania's hospitals at which coronary artery bypass is performed. Apparently, the major risk factors commonly employed in most other risk adjustment schemes for cardiac surgery have been deleted, and the practitioners might be judged unfairly. The Pennsylvania system appears to be insurance driven to reward low-cost providers who operate on patients with the lowest risk. RESULTS: Review of data suggests that the Pennsylvania Health Care Cost Containment Council's annual publication, A Consumer's Guide for Coronary Artery Bypass Surgery, misrepresents fair risk adjustment in favor of lower-risk patients, thereby encouraging better score cards for those institutions with patients who are less ill. Data regarding charges for the procedure have not been risk adjusted or related to a regional economic index. CONCLUSIONS: Surgeons must prepare to better understand relevant models that evaluate outcome. Cardiothoracic surgery is one of the first specialties to feel the pressures of mandated evaluations, and the lessons learned in Pennsylvania should be applicable to other states and their practitioners.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blumberg M. S. Biased estimates of expected acute myocardial infarction mortality using MedisGroups admission severity groups. JAMA. 1991 Jun 12;265(22):2965–2970. [PubMed] [Google Scholar]
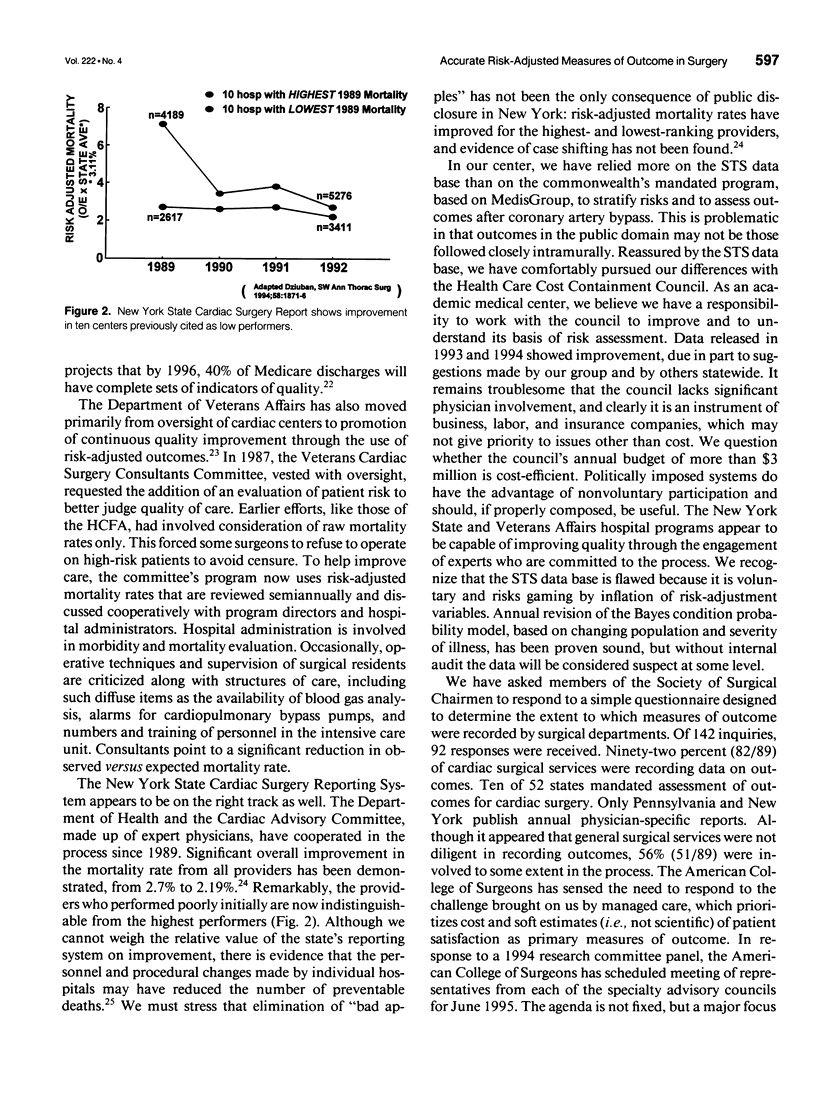
- Dziuban S. W., Jr, McIlduff J. B., Miller S. J., Dal Col R. H. How a New York cardiac surgery program uses outcomes data. Ann Thorac Surg. 1994 Dec;58(6):1871–1876. doi: 10.1016/0003-4975(94)91730-2. [DOI] [PubMed] [Google Scholar]
- Edwards F. H., Albus R. A., Zajtchuk R., Graeber G. M., Barry M. A quality assurance model of operative mortality in coronary artery surgery. Ann Thorac Surg. 1989 May;47(5):646–649. doi: 10.1016/0003-4975(89)90111-2. [DOI] [PubMed] [Google Scholar]
- Edwards F. H., Clark R. E., Schwartz M. Coronary artery bypass grafting: the Society of Thoracic Surgeons National Database experience. Ann Thorac Surg. 1994 Jan;57(1):12–19. doi: 10.1016/0003-4975(94)90358-1. [DOI] [PubMed] [Google Scholar]
- Edwards F. H., Graeber G. M. The theorem of Bayes as a clinical research tool. Surg Gynecol Obstet. 1987 Aug;165(2):127–129. [PubMed] [Google Scholar]
- Grover F. L., Johnson R. R., Shroyer A. L., Marshall G., Hammermeister K. E. The Veterans Affairs Continuous Improvement in Cardiac Surgery Study. Ann Thorac Surg. 1994 Dec;58(6):1845–1851. doi: 10.1016/0003-4975(94)91725-6. [DOI] [PubMed] [Google Scholar]
- Hannan E. L., Kumar D., Racz M., Siu A. L., Chassin M. R. New York State's Cardiac Surgery Reporting System: four years later. Ann Thorac Surg. 1994 Dec;58(6):1852–1857. doi: 10.1016/0003-4975(94)91726-4. [DOI] [PubMed] [Google Scholar]
- Hattler B. G., Madia C., Johnson C., Armitage J. M., Hardesty R. L., Kormos R. L., Pham S. M., Payne D. N., Griffith B. P. Risk stratification using the Society of Thoracic Surgeons Program. Ann Thorac Surg. 1994 Nov;58(5):1348–1352. doi: 10.1016/0003-4975(94)91911-9. [DOI] [PubMed] [Google Scholar]
- Iezzoni L. I., Moskowitz M. A. A clinical assessment of MedisGroups. JAMA. 1988 Dec 2;260(21):3159–3163. doi: 10.1001/jama.260.21.3159. [DOI] [PubMed] [Google Scholar]
- Jencks S. F. HCFA's Health Care Quality Improvement Program and the Cooperative Cardiovascular Project. Ann Thorac Surg. 1994 Dec;58(6):1858–1862. doi: 10.1016/0003-4975(94)91727-2. [DOI] [PubMed] [Google Scholar]
- Relman A. S. Assessment and accountability: the third revolution in medical care. N Engl J Med. 1988 Nov 3;319(18):1220–1222. doi: 10.1056/NEJM198811033191810. [DOI] [PubMed] [Google Scholar]
- Takaro T., Ankeney J. L., Laning R. C., Peduzzi P. N. Quality control for cardiac surgery in the Veterans Administration. Ann Thorac Surg. 1986 Jul;42(1):37–44. doi: 10.1016/s0003-4975(10)61833-4. [DOI] [PubMed] [Google Scholar]
- Topol E. J., Califf R. M. Scorecard cardiovascular medicine. Its impact and future directions. Ann Intern Med. 1994 Jan 1;120(1):65–70. doi: 10.7326/0003-4819-120-1-199401010-00011. [DOI] [PubMed] [Google Scholar]