

Abstract
Inflammatory hypothalamo-hypophyseal disorders are uncommon, representing only 1% of hypophyseal lesions. Among these, postpartum lymphocytic hypophysitis emerges as a particularly notable etiology. As a relatively recent entity, its recognition mandates a multidisciplinary approach to ensure preservation of compromised vital prognosis and amelioration of associated neuro-ophthalmologic and/or hypophyseal manifestations. We present a remarkable case of lymphocytic hypophysitis in a 32-year-old woman, unveiled during the postpartum period. Despite employing magnetic resonance imaging (MRI), preoperative diagnosis remained challenging. Surgical intervention became imperative due to progressive visual impairments. Postoperative course demonstrated favorable evolution, characterized by significant enhancement in visual acuity and normalization of cerebral MRI findings during follow-up.
Keywords: hypophysitis, pituitary gland, endonasal surgery
Introduction
Inflammatory hypothalamo-hypophysitis is rare and represents only 3% of pathologies affecting the pituitary gland. Among these conditions, lymphocytic hypophysitis holds significant etiological importance. The first documented case was reported by Goudie and Pinkerton in the early 1960s, 1 describing a patient who died from acute adrenal insufficiency. However, it was not until 1980 that the first case was authenticated through pituitary biopsy. Since then, nearly 500 cases have been documented in the medical literature. Autoimmune hypophysitis is characterized by lymphocytic infiltration of the pituitary gland. This condition primarily affects women and most commonly manifests during pregnancy and the postpartum period. However, cases have also been described before puberty and after menopause.
Observation
A 32-year-old patient, with no significant medical history, G2P2, presented during her 9th month of pregnancy with helmet-like headaches accompanied by food vomiting, attributed to pregnancy. The symptoms worsened postpartum with the sudden onset of bilateral visual acuity loss, associated with the absence of postpartum bleeding and lactation, amidst significant fatigue and notable weight loss. Initial clinical examination revealed left visual acuity of 2/10, right visual acuity of 4/10, bitemporal hemianopsia in the visual field, and a fundus without anomalies. Hormonal investigations concluded: corticotrope insufficiency (8-hour cortisol: 1.14 µg/dL), thyrotrope insufficiency (LT4: 6.60 μmol/L; TSH:1.2 mUI/L), prolactin at 19 ng/mL, and estradiol at 16 pg/mL. Hypothalamo-hypophyseal magnetic resonance imaging (MRI) showed an intrasellar and suprasellar mass measuring 2.5 × 2.4 cm, isointense in T1 ( Fig. 1 ), T2, and fluid-attenuated inversion recovery, enhancing intensely after contrast agent injection. This mass had a champagne cork appearance, displacing and elevating the optic chiasm upwards, with the pituitary parenchyma pressed against the sellar floor. It is noteworthy: a T2 halo seemed to separate the process from the sellar floor ( Fig. 2 ), with contrast enhancement of the sellar diaphragm on either side of the latter ( Fig. 3 ).
Fig. 1.
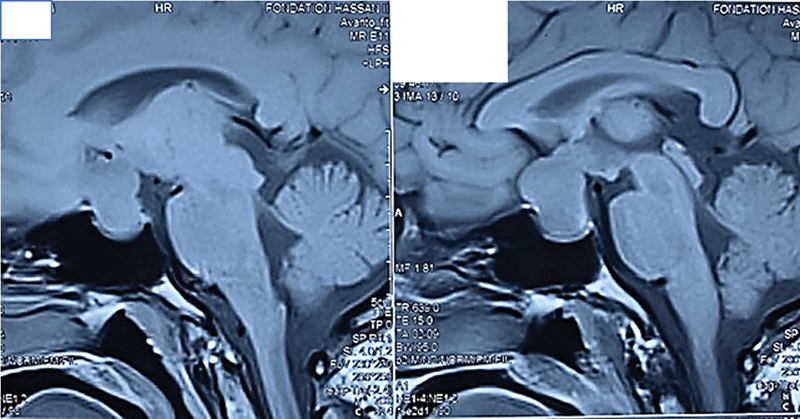
Intrasellar and suprasellar mass measuring 2.5 × 2.4 cm, isointense on T1.
Fig. 2.
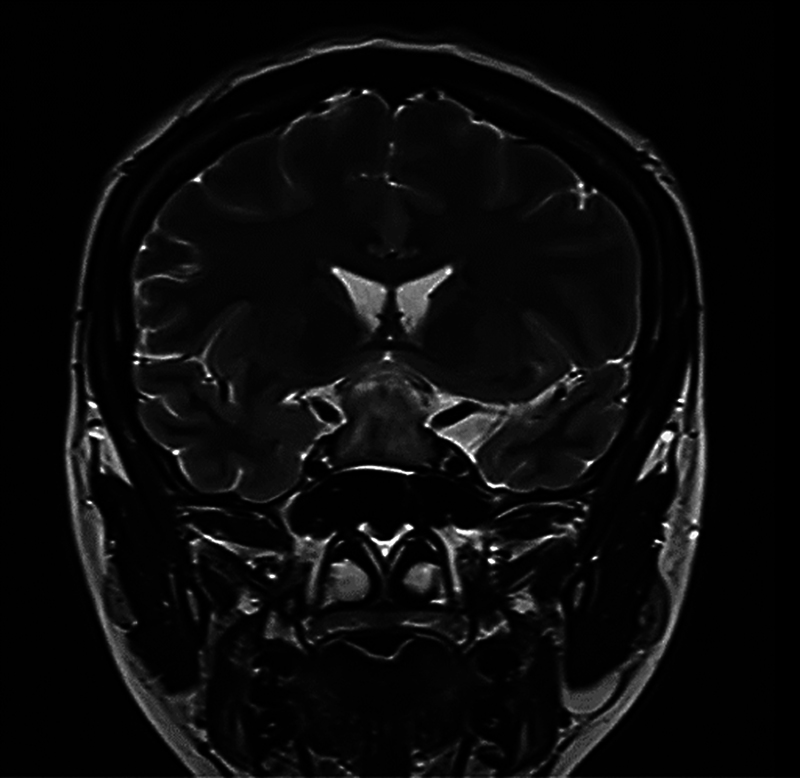
Intrasellar and suprasellar mass measuring 2.5 × 2.4 cm, isointense on T2 with a T2 halo that separate the process from the sellar floor.
Fig. 3.
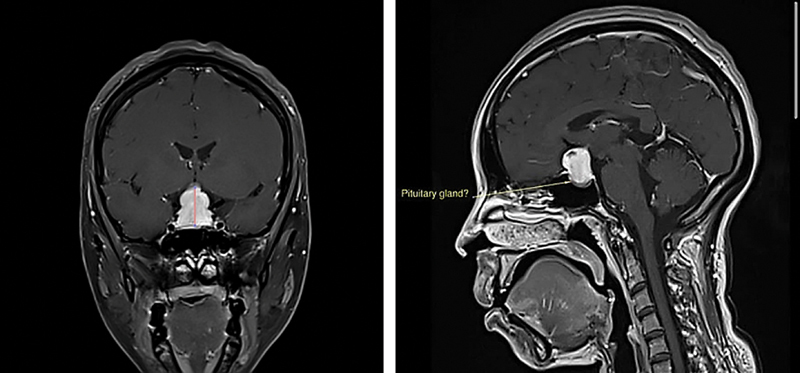
Intrasellar and suprasellar mass enhancing intensely after contrast injection, with a champagne cork appearance, displacing and elevating the optic chiasm upwards, with the pituitary parenchyma pressed against the sellar floor.
Based on clinical, biological, and radiological criteria, the diagnosis of pituitary adenoma, likely fibrous, was made. The patient was medically treated and hospitalized for decompressive surgery due to visual compromise. Exeresis was performed via transsphenoidal endoscopic approach, with almost monobloc exeresis of a process immediately found subdural upon dura mater opening. The intraoperative appearance rather suggested a meningioma of the sellar diaphragm, and samples were taken for histopathological studies. At the end of the excision, the optic chiasm was visualized, laminated by process pressure with the two anterior communicating arteries and the two carotids. The pituitary stalk also appeared discontinuous, and the pituitary parenchyma was not visualized in the residual sellar cavity ( Fig. 4 ). Immediate postoperative evolution was marked by the onset of diabetes insipidus requiring Minirin introduction. Histopathological examination revealed a homogeneous, whitish-yellow lesion with a smooth, multilobulated surface ( Fig. 5 ). Microscopically, the lesion was composed of a dense lymphoplasmacytic infiltrate with scattered eosinophils interspersed among large cells exhibiting vesicular nuclei and clear cytoplasm ( Fig. 6 ). Immunohistochemical analysis showed strong positivity for CD45 in numerous cells of varying sizes ( Fig. 7 ), while lymphocytic cells stained positive for CD5 and CD3. These findings were consistent with a diagnosis of postpartum lymphocytic hypophysitis.
Fig. 4.
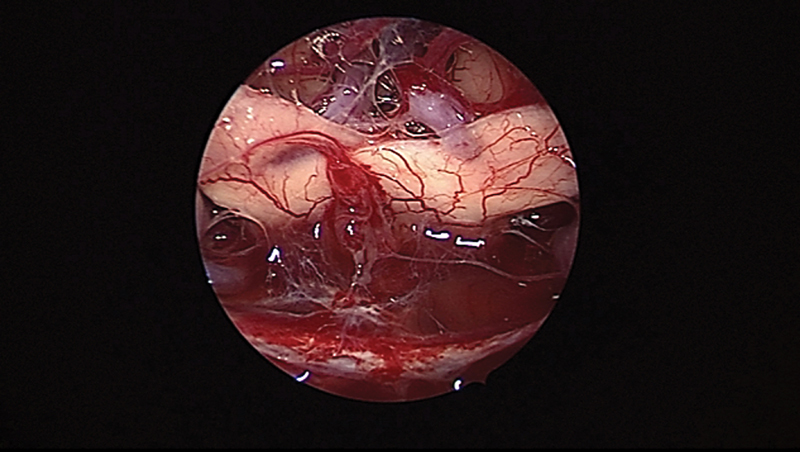
Peroperative image showing at the end of the excision: the optic chiasm, with anterior communicating arteries (ACAs) and the two carotids. The pituitary stalk appeared discontinuous, and the pituitary parenchyma was not visualized in the residual sellar cavity.
Fig. 5.
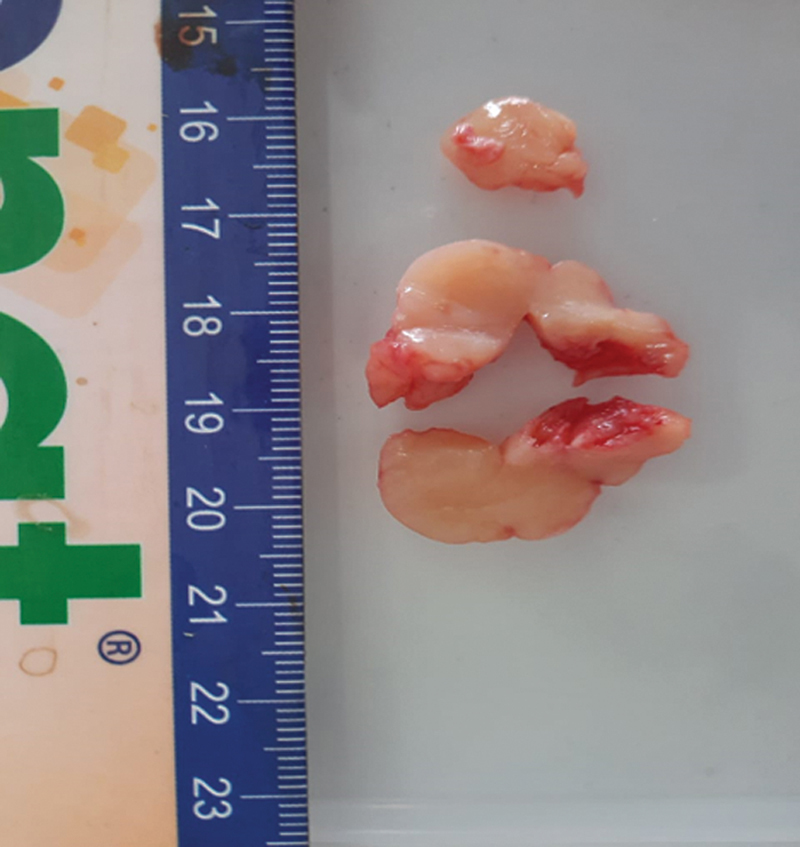
Macroscopic appearance: homogeneous, whitish-yellow lesion with a smooth, multilobulated surface.
Fig. 6.
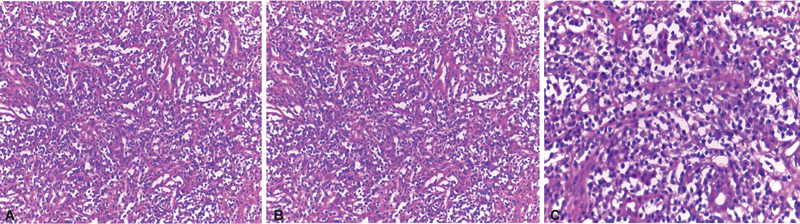
Microscopic appearance: lesion composed of a dense lymphoplasmacytic infiltrate with scattered eosinophils interspersed among large cells exhibiting vesicular nuclei and clear cytoplasm: ( A ) Gx10; ( B ) Gx20; ( C ) Gx40.
Fig. 7.
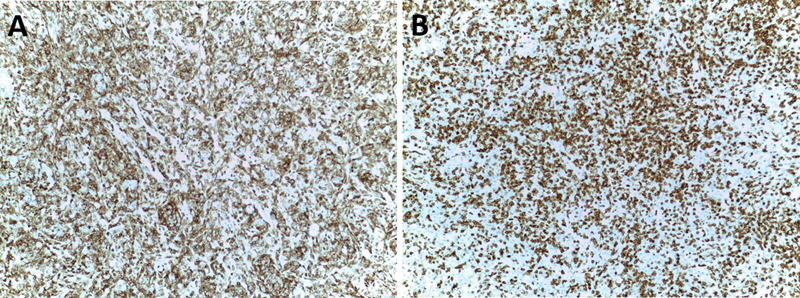
Immunohistochemical analysis: ( A ) showed strong positivity for CD45 in numerous cells of varying sizes, and ( B ) lymphocytic cells stained positive for CD5 and CD3.
The patient was referred to endocrinology for possible correction of hormonal disorders and for the investigation of other autoimmune diseases, which returned negative. She was seen in consultation 3 months later, with improved visual acuity (8/10 right and 6/10 left), but persistent hormonal deficits, particularly treated central diabetes insipidus with Minirin melt 60 (1 tablet twice a day). Control MRI performed at 1 year of follow-up revealed the disappearance of the pituitary pseudotumor and a reduction in the thickening of the pituitary stalk.
Discussion
Lymphocytic hypophysitis is a rare and recently described entity. Since the first autopsy case reported by Goudie and Pinkerton in 1962, 3 approximately 500 cases have been documented. This pathology is observed predominantly in pregnant or postpartum women (72% of cases), 1 4 5 7 8 14 15 16 but it has also been described in multiparous women outside of pregnancy, in menopausal women, 8 16 17 18 and in rare cases in men. 1 2 Additionally, three cases associated with craniopharyngiomas have been reported. 10
Clinically, the condition frequently manifests during the third trimester of pregnancy or in the immediate postpartum period with sudden onset of frontal or retro-orbital headaches (72%) and visual disturbances, including visual field defects and decreased visual acuity, suggesting optic chiasm involvement. 1 3 7 8 15 Less commonly, oculomotor palsy may also be present. 15 16 The acute presentation can mimic pituitary apoplexy of an undiagnosed pituitary adenoma, warranting urgent hypothalamo-hypophyseal imaging and, in some cases, neurosurgical decompression. In the postpartum period, anterior pituitary insufficiency is often predominant, with complete or partial hypopituitarism occurring in more than two-thirds of cases. 9 14 16 Adrenal insufficiency is particularly concerning, manifesting as weight loss, profound fatigue, hypotension, and even cardiovascular collapse. Combined somatotropic and corticotropic deficiencies may lead to hypoglycemic episodes. 19 Gonadotropic dysfunction may become apparent postpartum, presenting as secondary amenorrhea, hyperprolactinemia, or hypoprolactinemia. 17 Posterior pituitary involvement results in polyuria-polydipsia syndrome, suggestive of central diabetes insipidus.
Radiologically, a cerebral computed tomography scan typically reveals an intrasellar mass with suprasellar extension, demonstrating homogeneous contrast enhancement, which often mimics a pituitary macroadenoma. MRI remains the gold standard for imaging, typically showing a pseudotumoral lesion that is iso- to hypointense on T1-weighted images, with suprasellar extension and optic chiasm compression. On T2-weighted sequences, these lesions exhibit homogeneous hypersignal. A key radiological feature suggestive of hypophysitis is pituitary stalk thickening with strong contrast enhancement. 11 However, these findings often overlap with those of pituitary adenomas, complicating the preoperative diagnosis.
To aid differentiation, Gutenberg et al proposed a radiological scoring system ( Table 1 ) 12 incorporating factors such as patient age, pregnancy status, pituitary volume, contrast enhancement characteristics, lesion symmetry, neurohypophyseal bright spot presence, pituitary stalk size, and sphenoidal mucosa thickening. A score of > 1 favors an adenoma diagnosis, while ≤ 0 suggests hypophysitis, with a positive predictive value of 97% and a negative predictive value of 97%. Additionally, although the detection of antipituitary antibodies has been investigated, their low sensitivity and specificity limit their diagnostic utility.
Table 1. Gutenberg score 12 .
| Characteristic | Hypophysitis | Adenoma | Score if yes |
|---|---|---|---|
| Age < 30 | Yes | No | −1 |
| Pregnancy-related | Yes | No | −4 |
| Volume > 6 cm 3 | No | Yes | +2 |
| Intensity and homogeneity of enhancement | Yes | No | -Enhancement type (medium or high) −1 -Enhancement feature (heterogeneous) +1 |
| Asymmetry of lesion | Yes | No | +3 |
| Loss of posthypophyseal bright spot | Yes | No | −2 |
| Enlarged stalk size | Yes | No | −5 |
| Thickened pituitary stalk | Yes | No | +2 |
Despite these radiological advancements, distinguishing hypophysitis from a pituitary macroadenoma remains challenging, particularly in the context of an ophthalmologic emergency where urgent decompression is necessary. This underscores the critical role of intraoperative histological examination. Frozen section analysis, when available, is invaluable in guiding intraoperative decision-making. A diagnosis of hypophysitis on frozen section may prompt a more conservative surgical approach, minimizing the risk of postoperative hypopituitarism. Unfortunately, in our case, intraoperative frozen section analysis was unavailable, potentially contributing to postoperative endocrine disturbances.
Histologically, definitive diagnosis requires surgical biopsy, revealing dense lymphocytic and plasmacytic infiltration, often with lymphoid follicle formation and germinal centers. 1 3 6 8 9 14 15 17 18 The predominance of T lymphocytes in the infiltrate, along with polyclonal plasma cells favoring immunoglobulin G subclass, supports an autoimmune etiology, which is further reinforced by associations with other autoimmune disorders such as Hashimoto's thyroiditis, 18 pernicious anemia, and sarcoidosis. 9 The histological differential diagnosis includes granulomatous hypophysitis (which exhibits histiocytic infiltration), tuberculosis, sarcoidosis, and Langerhans cell histiocytosis. 17 20
Surgical management depends on the clinical presentation. In cases with significant visual impairment, urgent neurosurgical decompression is warranted. Transsphenoidal surgery remains the preferred approach, enabling biopsy and decompression while minimizing damage to normal pituitary tissue. When significant suprasellar extension is present, a transcranial approach may be considered. Subtotal resection with preservation of viable pituitary tissue is recommended to prevent permanent hypopituitarism.
If intraoperative frozen section analysis confirms lymphocytic hypophysitis, a conservative surgical strategy should be adopted to avoid unnecessary extensive resection. The goal should be limited decompression and biopsy, as complete tumor removal is not required in inflammatory conditions. Once hypophysitis is confirmed, corticosteroid therapy should be considered postoperatively to reduce inflammation and facilitate regression of residual tissue. Early endocrine assessment is crucial to determine the extent of hormonal deficits and initiate appropriate replacement therapy.
In cases where visual compromise is absent, high-dose corticosteroid therapy with close imaging and ophthalmologic monitoring is the preferred management strategy. 7 8 Spontaneous resolution of the lesion is observed in some cases, with subsequent development of an empty sella, confirming the diagnosis retrospectively. However, endocrine deficits often persist, necessitating long-term hormone replacement therapy.
Several comparative studies have evaluated the efficacy of different management approaches. A study by Faje et al compared surgical decompression versus corticosteroid therapy in patients with lymphocytic hypophysitis and found that while surgery provided immediate relief of compressive symptoms, it carried a higher risk of long-term hypopituitarism. Conversely, corticosteroid therapy was associated with lesion regression but required prolonged endocrine follow-up due to potential relapses. 21 Another study by Sato et al reviewed outcomes of patients managed conservatively versus those undergoing biopsy and demonstrated that patients with mild to moderate symptoms responded well to high-dose corticosteroids, whereas those with severe visual disturbances benefited more from early decompression. 22 These studies highlight the importance of individualized treatment planning based on clinical and radiological findings.
In conclusion, the diagnosis of lymphocytic hypophysitis relies on a combination of clinical, radiological, and histological findings. Given its potential to mimic pituitary adenomas, careful preoperative assessment is crucial to avoid unnecessary aggressive surgical interventions. Intraoperative frozen section analysis, when available, provides critical guidance in surgical decision-making, potentially reducing postoperative morbidity. Finally, lifelong endocrine follow-up remains essential due to the frequent persistence of hormonal deficiencies. Leporati et al proposed five diagnostic criteria for hypophysitis, further aiding in distinguishing this condition from other sellar pathologies ( Table 2 ).
Table 2. Leporati, 2011 13 .
| Criteria | Description |
|---|---|
| 1: Histology | Mononuclear infiltration of the pituitary gland, rich in lymphocytes and plasma cells |
| 2: Pituitary MRI | Sellar mass or thickening of the pituitary stalk |
| 3: Other organ involvement | Biopsy confirming involvement of another organ |
| 4: Serology | Plasma IgG4 levels > 140 mg/dL |
| 5: Response to treatment | Reduction in pituitary mass and improvement of symptoms with corticosteroid therapy |
| Diagnostic conclusion | Diagnosis confirmed if criterion 1 is present, or if criteria 2 + 3, or criteria 2 + 4 + 5 are met |
Abbreviations: IgG, immunoglobulin G; MRI, magnetic resonance imaging.
Conclusion
The possibility of a diagnosis of lymphocytic hypophysitis should be considered in pregnant and postpartum women. Surgical intervention pursues a dual objective: obtaining a definitive diagnosis and decompressive therapeutic aim, while avoiding complete excision. The increase in observed cases may lead to a revision of the anatomopathological classification of these hypothalamo-hypophyseal inflammatory phenomena.
Footnotes
Conflict of Interest None declared.
References
- 1.Goudie R B, Pinkerton P H. Anterior hypophysitis and Hashimoto's disease in a young woman. J Pathol Bacteriol. 1962;83:584–585. [PubMed] [Google Scholar]
- 2.Gossain V V, Rovner D R. Primary hypothyroidism, pituitary insufficiency and pregnancy. A case report. J Reprod Med. 1984;29(04):284–288. [PubMed] [Google Scholar]
- 3.Pholsena M, Young J, Couzinet B, Schaison G. Primary adrenal and thyroid insufficiencies associated with hypopituitarism: a diagnostic challenge. Clin Endocrinol (Oxf) 1994;40(05):693–695. doi: 10.1111/j.1365-2265.1994.tb03023.x. [DOI] [PubMed] [Google Scholar]
- 4.Beressi N, Cohen R, Beressi J Pet al. Pseudotumoral lymphocytic hypophysitis successfully treated by corticosteroid alone: first case report Neurosurgery 19943503505–508., discussion 508 [DOI] [PubMed] [Google Scholar]
- 5.Reusch J E, Kleinschmidt-DeMasters B K, Lillehei K O, Rappe D, Gutierrez-Hartmann A. Preoperative diagnosis of lymphocytic hypophysitis (adenohypophysitis) unresponsive to short course dexamethasone: case report. Neurosurgery. 1992;30(02):268–272. doi: 10.1227/00006123-199202000-00023. [DOI] [PubMed] [Google Scholar]
- 6.Pechner M JA, Ludecker D K, Salger W. The anterior pituitary lobe in patients with cyctic craniopharyngioma. Three cases of associate lymphocytic hypophysitis. Acta Neurochir (Wien) 1994;26:34–43. doi: 10.1007/BF01476492. [DOI] [PubMed] [Google Scholar]
- 7.Fedala N S, Chentli F, Meskine D, Haddam A EM. Les hypophysites: aspects cliniques et évolutifs. Ann Endocrinol (Paris) 2016;77(04):329–371. [Google Scholar]
- 8.Boudjeloud A, Sebti I, Bersali M, Saber K A. Hypophysite du post-partum: un piège diagnostic à propos d’un cas et revue de littérature. J Neurochir. 2012;15:57. [Google Scholar]
- 9.Hayashi H, Yamada K, Kuroki T et al. Lymphocytic hypophysitis and pulmonary sarcoidosis. Report of a case. Am J Clin Pathol. 1991;95(04):506–511. doi: 10.1093/ajcp/95.4.506. [DOI] [PubMed] [Google Scholar]
- 10.Stelmach M, O'Day J. Rapid change in visual fields associated with suprasellar lymphocytic hypophysitis. J Clin Neuroophthalmol. 1991;11(01):19–24. doi: 10.3109/01658109109009637. [DOI] [PubMed] [Google Scholar]
- 11.Ahmadi J, Meyers G S, Segall H D, Sharma O P, Hinton D R. Lymphocytic adenohypophysitis: contrast-enhanced MR imaging in five cases. Radiology. 1995;195(01):30–34. doi: 10.1148/radiology.195.1.7892490. [DOI] [PubMed] [Google Scholar]
- 12.Gutenberg A, Larsen J, Lupi I, Rohde V, Caturegli P. A radiologic score to distinguish autoimmune hypophysitis from nonsecreting pituitary adenoma preoperatively. AJNR Am J Neuroradiol. 2009;30(09):1766–1772. doi: 10.3174/ajnr.A1714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Leporati P, Landek-Salgado M A, Lupi I, Chiovato L, Caturegli P. IgG4-related hypophysitis: a new addition to the hypophysitis spectrum. J Clin Endocrinol Metab. 2011;96(07):1971–1980. doi: 10.1210/jc.2010-2970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cosman F, Post K D, Holub D A, Wardlaw S L. Lymphocytic hypophysitis. Report of 3 new cases and review of the literature. Medicine (Baltimore) 1989;68(04):240–256. doi: 10.1097/00005792-198907000-00006. [DOI] [PubMed] [Google Scholar]
- 15.Unlühizarci K, Bayram F, Colak R et al. Distinct radiological and clinical appearance of lymphocytic hypophysitis. J Clin Endocrinol Metab. 2001;86(05):1861–1864. doi: 10.1210/jcem.86.5.7440. [DOI] [PubMed] [Google Scholar]
- 16.Stelmach M, O'Day J. Rapid change in visual fields associated with suprasellar lymphocytic hypophysitis. J Clin Neuroophthalmol. 1991;11(01):19–24. doi: 10.3109/01658109109009637. [DOI] [PubMed] [Google Scholar]
- 17.Levine S N, Benzel E C, Fowler M R, Shroyer J V, III, Mirfakhraee M. Lymphocytic adenohypophysitis: clinical, radiological, and magnetic resonance imaging characterization. Neurosurgery. 1988;22(05):937–941. [PubMed] [Google Scholar]
- 18.Shimono T, Yamaoka T, Nishimura K et al. Lymphocytic hypophysitis presenting with diabetes insipidus: MR findings. Eur Radiol. 1999;9(07):1397–1400. doi: 10.1007/s003300050855. [DOI] [PubMed] [Google Scholar]
- 19.Wild R A, Kepley M. Lymphocytic hypophysitis in a patient with amenorrhea and hyperprolactinemia. A case report. J Reprod Med. 1986;31(03):211–216. [PubMed] [Google Scholar]
- 20.Mayfield R K, Levine J H, Gordon L, Powers J, Galbraith R M, Rawe S E. Lymphoid adenohypophysitis presenting as a pituitary tumor. Am J Med. 1980;69(04):619–623. [PubMed] [Google Scholar]
- 21.Faje A T et al. Comparing surgical decompression and corticosteroid therapy in lymphocytic hypophysitis: outcomes and long-term endocrine sequelae. J Clin Endocrinol Metab. 2018;103(02):567–575. [Google Scholar]
- 22.Sato N et al. Management of lymphocytic hypophysitis: a comparative study of surgical and conservative approaches. Pituitary. 2021;24(04):612–623. [Google Scholar]