

Abstract
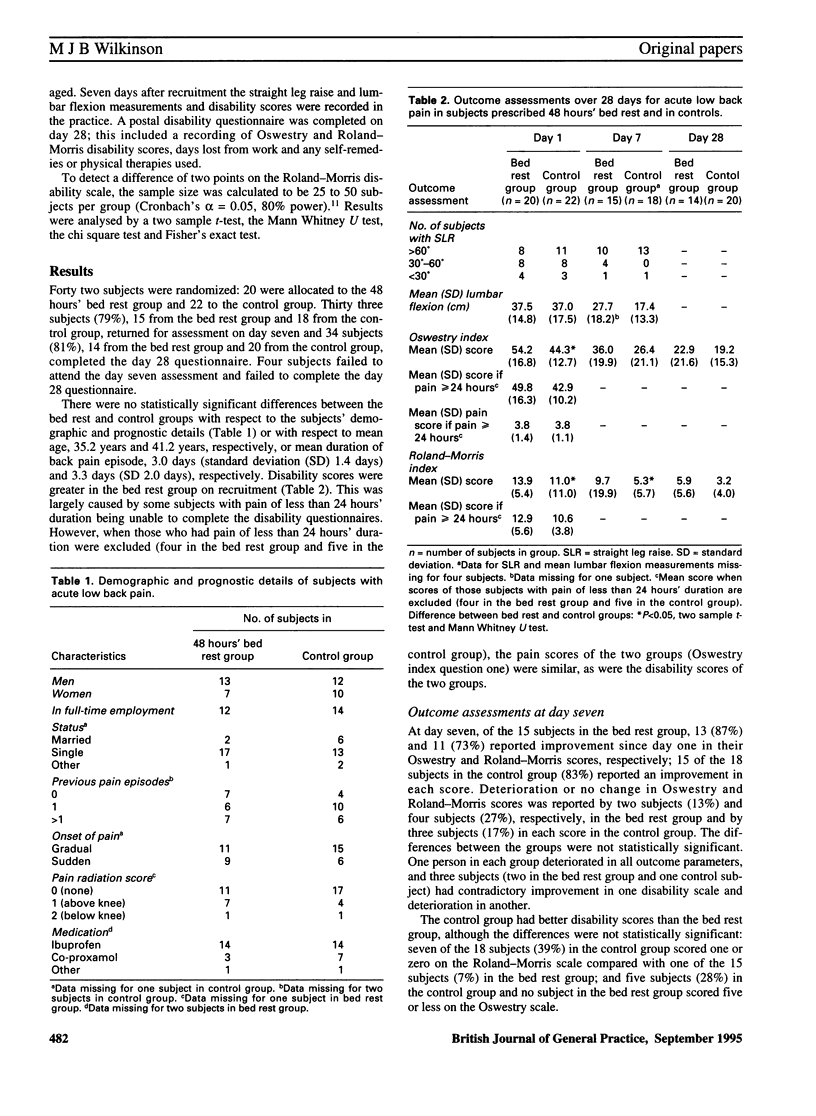
BACKGROUND. Bed rest is a traditional treatment for back pain, yet only in recent years has the therapeutic benefit of this been questioned. AIM. The aim of this pilot study was to ascertain whether or not 48 hours' bed rest had an effect on the outcome of acute low back pain. METHOD. The study was conducted as a randomized controlled trial to compare a prescription of 48 hours' strict bed rest with controls; the control subjects were encouraged to remain mobile and to have no daytime rest. Nine general practitioners from practices in the West Midlands recruited patients in the age range 16-60 years who presented with low back pain of less than seven days' duration, with or without pain radiation. The outcome measures assessed were: change in straight leg raise and lumbar flexion after seven days, Oswestry and Roland-Morris disability scores after seven days and 28 days, and time taken from work. RESULTS. Forty two patients were recruited: 20 were allocated to bed rest and 22 as controls. Compared with the bed rest group the control group had statistically better Roland-Morris scores at day seven (P < 0.05) but not at day 28. At day seven, there were no statistically significant differences between groups in straight leg raise or lumbar flexion measurements although the control group had a better mean lumbar flexion than the bed rest group. The improvement in disability scores at day seven compared with day one was similar for the two groups but more of the control group had fully recovered (defined as scores of one or zero on the Roland-Morris disability scale and five or less on the Oswestry disability scale) by day seven. Remaining mobile did not appear to cause any adverse effects. The number of days lost from work in both groups was equal. A large number of self-remedies and physical therapies were recorded by subjects from both groups. CONCLUSION. The results of this pilot study did not indicate whether bed rest or remaining mobile was superior for the treatment of acute low back pain; however, the study sample was small. Subjects in the control group possibly fared better as they appeared to have better lumbar flexion at day seven. It appears that 48 hours' bed rest cannot be recommended for the treatment of acute low back pain on the basis of this small study. Large-scale definitive trials are required to detect clinically significant differences.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Deyo R. A. Conservative therapy for low back pain. Distinguishing useful from useless therapy. JAMA. 1983 Aug 26;250(8):1057–1062. [PubMed] [Google Scholar]
- Deyo R. A., Diehl A. K., Rosenthal M. How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med. 1986 Oct 23;315(17):1064–1070. doi: 10.1056/NEJM198610233151705. [DOI] [PubMed] [Google Scholar]
- Florey C. D. Sample size for beginners. BMJ. 1993 May 1;306(6886):1181–1184. doi: 10.1136/bmj.306.6886.1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert J. R., Taylor D. W., Hildebrand A., Evans C. Clinical trial of common treatments for low back pain in family practice. Br Med J (Clin Res Ed) 1985 Sep 21;291(6498):791–794. doi: 10.1136/bmj.291.6498.791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nachemson A. Work for all. For those with low back pain as well. Clin Orthop Relat Res. 1983 Oct;(179):77–85. [PubMed] [Google Scholar]
- Roland M., Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine (Phila Pa 1976) 1983 Mar;8(2):141–144. doi: 10.1097/00007632-198303000-00004. [DOI] [PubMed] [Google Scholar]
- Roland M., Morris R. A study of the natural history of low-back pain. Part II: development of guidelines for trials of treatment in primary care. Spine (Phila Pa 1976) 1983 Mar;8(2):145–150. doi: 10.1097/00007632-198303000-00005. [DOI] [PubMed] [Google Scholar]
- Thomas K. B. General practice consultations: is there any point in being positive? Br Med J (Clin Res Ed) 1987 May 9;294(6581):1200–1202. doi: 10.1136/bmj.294.6581.1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiesel S. W., Cuckler J. M., Deluca F., Jones F., Zeide M. S., Rothman R. H. Acute low-back pain. An objective analysis of conservative therapy. Spine (Phila Pa 1976) 1980 Jul-Aug;5(4):324–330. doi: 10.1097/00007632-198007000-00006. [DOI] [PubMed] [Google Scholar]